
Abstract
Gambling disorder is associated with suicidal behaviors, but it is not clear whether the association is due to common etiologic factors or to gambling disorder being causally related to suicidality. This question was examined from the perspective of epidemiologic, longitudinal, and discordant-twin studies. The results suggested that the causes of the association with disordered gambling differed for suicidal ideation, plan, and attempt and differed for men and women. The association of suicidal thoughts with disordered gambling was noncausally explained by common genetic influences among women but not men. Conversely, there was evidence consistent with a potentially causal influence of disordered gambling on suicide attempt among men but not women, which might have been related to gambling-related financial problems. The use of monetary data to identify individuals experiencing financial harms associated with their gambling may represent a more practicable target for screening, intervention, and prevention and may reduce gambling-related financial crises, thereby warding off a potential gambling-related suicide attempt.
Gambling disorder is a pattern of gambling behavior, sometimes recurrent or persistent (Slutske, 2006), that is associated with substantial distress or impairment and that affects about 1% of the population (Potenza et al., 2019). Individuals with gambling disorder experience higher rates of nearly every other psychiatric disorder relative to people without a gambling disorder (Petry et al., 2005). Especially alarming is the elevated rate of suicide. For example, in a comprehensive national Swedish study of 2,099 individuals who had received treatment for gambling disorder between 2005 and 2016, 22 of 67 deaths (31%) were due to suicide. Suicide was the leading cause of death in this population-based sample of individuals who had received treatment for a gambling disorder (Karlsson & Håkansson, 2018).
It may be tempting to draw a causal link between gambling disorder and suicide. Individuals with a gambling disorder may accumulate unmanageable financial debt or be forced to face dire legal consequences—both factors that may lead some people to consider suicide (Blaszczynski & Farrell, 1998; Chen et al., 2006; Wong et al., 2010). Although there is the necessary temporal order between gambling disorder and suicide mortality consistent with causality, suicides are often preceded by thoughts about suicide, plans to commit suicide, and previous attempts (Kessler et al., 1999; Wong et al., 2010).
The focus of the current investigation was on the relation between gambling disorder and these nonfatal potential precursors to suicide, that is, suicidal thoughts, plans, and attempts. To our knowledge, there have been only five previous general-population surveys that focused on the association between gambling disorder and suicidal behaviors. 1 Only three assessed suicidal thoughts (Meltzer et al., 2011; Moghaddam et al., 2015; Park et al., 2010), one assessed suicidal plans (Park et al., 2010), and four assessed suicide attempts (Moghaddam et al., 2015; Newman & Thompson, 2003, 2007; Park et al., 2010). Unfortunately, three of the five studies did not assess suicidal behaviors outside of the context of a screening for major depression (Moghaddam et al., 2015; Newman & Thompson, 2003, 2007). That is, suicidal behaviors were assessed only among participants who reported a 2-week period of depressed mood or anhedonia. This leads to measures of suicidal behaviors that are confounded with depressed mood/anhedonia and excludes suicidal behaviors that occur outside of the context of depression. 2 Other than the present study, the only study that examined the relation between gambling disorder and suicidal thoughts, plans, and attempts assessed outside of the context of a depression screening in a representative sample of the general population was a study of 5,333 Korean individuals (Park et al., 2010) in which there were significant associations of gambling disorder with suicidal thoughts and plans but not attempts. This counterintuitive result can probably be explained by the lower prevalence of suicide attempt and the small number of individuals (n = 43) with gambling disorder.
Although cross-sectional studies have documented substantial associations between gambling disorder and suicidal behaviors, they cannot tell the temporal relation between the two. There are no longitudinal studies that have tracked the occurrence of suicidal behaviors and disordered gambling over time. In the absence of longitudinal data, researchers have used retrospectively recalled ages of onset obtained in a cross-sectional study to examine the temporal priority of cooccurring disorders. For example, in the National Comorbidity Survey Replication, gambling disorder had a later onset than did the co-occurring disorder (including mood, anxiety, impulse-control, and substance use disorders) 74% of the time, had an earlier onset 24% of the time, and first occurred in the same year 2% of the time (Kessler et al., 2008). In a small sample of 35 individuals with co-occurring gambling disorder and suicidal behaviors selected from a Swedish population-based study, gambling disorder had a later onset than did suicidal behaviors 63% of the time, had an earlier onset 31% of the time, and first occurred in the same year 6% of the time (Sundqvist & Rosendahl, 2019). However, even these data on the relative timing of the onsets of gambling disorder and suicidal behaviors are unsatisfactory because later emerging gambling disorder could still precipitate a subsequent suicidal event among individuals with a preexisting history of suicidal behavior. The existing epidemiologic evidence is insufficient to rule in or rule out a potential causal relation between gambling disorder and suicidal behavior.
An alternate explanation for the relation between gambling disorder and suicidal behavior is that they have a shared etiology. For example, Hodgins et al. (2006) proposed that a common factor shared between gambling, substance use, and mood disorders was related to the propensity to attempt and, ultimately, to commit suicide. This is supported by the results of an epidemiologic survey demonstrating that a significant relation between gambling disorder and suicidal behavior was substantially reduced after controlling for substance use disorders, major depression, phobia, and antisocial personality disorder (Newman & Thompson, 2003). Other evidence comes from a family study in which there was a significantly higher rate of suicide attempts (9% vs. 1%; odds ratio [OR] = 12.35) among 103 offspring of 95 parents affected with a gambling disorder compared with 130 offspring of 91 unaffected control parents (Black et al., 2015), which suggests that there is a shared familial risk (that may include genetic and shared family environmental factors) common to gambling disorder and suicidal behavior.
Multilevel discordant-twin modeling can provide insight into whether the association between gambling disorder and suicidal behavior is potentially causal or due to common genetic and family environmental risk factors. The discordant-twin design is a natural experiment in which a twin unaffected by a gambling disorder serves as the control subject for the co-twin affected by a gambling disorder (McGue et al., 2010). This individual-level effect controls for genetic and shared environmental factors and therefore can be attributed to the unique or individual-specific environment; it is consistent with a possible causal influence of gambling disorder on suicidal behaviors. Multilevel discordant-twin modeling (Turkheimer & Harden, 2014) also allows one to model effects at the familial (between twin pairs) and the individual (within twin pairs) levels. This familial-level effect represents a noncausal influence of systematic genetic or environmental differences between families that are related to both gambling disorder and suicidal behaviors. The inclusion of psychiatric covariates of interest in the model also can test whether this familial-level effect can be explained by comorbid psychiatric disorders.
The current study was based on data from a large, national, community-based sample of adult Australian twins that was used to explore the reasons for the elevated rates of suicidal behaviors (thoughts, plan, and attempt) among individuals with a gambling disorder. We examined cross-sectional and longitudinal epidemiologic associations between gambling disorder and suicidal behaviors and conducted multilevel discordant-twin modeling predicting suicidal behaviors from gambling disorder. Significant between-twin-pairs associations would provide support for a familial influence shared with gambling disorder and suicidal behavior, whereas significant within-twin-pairs associations would be consistent with an individual level and a potentially causal relation. Indicators of socioeconomic status and comorbid psychiatric disorders were covaried to eliminate alternate explanations for between-twin-pairs and within-twin-pairs associations.
Method
Participants
Participants were 8,327 members of the Australian Twin Registry (ATR) Cohort II (ATR-II) and Cohort III (ATR-III). They represented a broad cross-section of the general population of Australia. Similar to most community-based twin cohorts, however, the sample was relatively socioeconomically advantaged and had an average yearly income of AU$87,066 (SD = AU$40,804; equivalent to about $56,853 in the United States in 2006).
ATR-II
ATR-II members included adult twins (n = 4,542) born between 1964 and 1971; 57.8% of the participants were female. Nearly all the participants were of European (mostly Northern European) ancestry; 2.0% of the participants had at least one grandparent of indigenous Australian or New Zealand ancestry, and 2.7% reported Asian or Pacific Islander ancestry. For additional details, see Slutske et al. (2009).
ATR-III
The ATR-III members included adult twins (n = 3,298) and siblings (n = 487) born between 1972 and 1979; 63.9% of the participants were female. Nearly all the participants were of European (mostly Northern European) ancestry; slightly less than 2% of the participants had at least one grandparent of indigenous Australian ancestry, and less than 1% reported Asian ancestry. For additional details, see Lynskey et al. (2012).
ATR-II and ATR-III combined twin sample
The combined sample included 2,995 complete twin pairs (1,403 monozygotic [MZ]: 903 female, 500 male; 1,592 dizygotic [DZ]: 647 female–female, 327 male–male, and 618 female–male), 1,844 individual twins from incomplete pairs (608 MZ: 324 female, 284 male; 1,236 DZ: 309 females and 345 males from same-sex pairs, 409 females and 173 males from opposite-sex pairs), and six individual twins of unknown zygosity.
Procedure
In both cohorts, interviews were administered by trained lay interviewers who were supervised by project editors. All interviews were tape-recorded, and a random sample of 5% of the interview tapes was reviewed for quality control.
ATR-II
Two phases of assessment were conducted with ATR-II (see Table 1). At the Phase 1 assessment, participants reported on suicidal behaviors, and at the Phase 2 assessment, an in-depth assessment of gambling behaviors and a brief assessment of suicidal behaviors were conducted. The mean age was 29.9 years (range = 24–36) at Phase 1 and 37.7 years (range = 32–43) at Phase 2. The average time interval between the Phase 1 and Phase 2 interviews was 7.8 years (SD = 1.4, range = 4–11). The ATR-II studies were approved by the institutional review boards at Washington University, the University of Missouri, and QIMR Berghofer. All participants provided informed consent.
Overview of Assessments in the Two Twin Cohorts
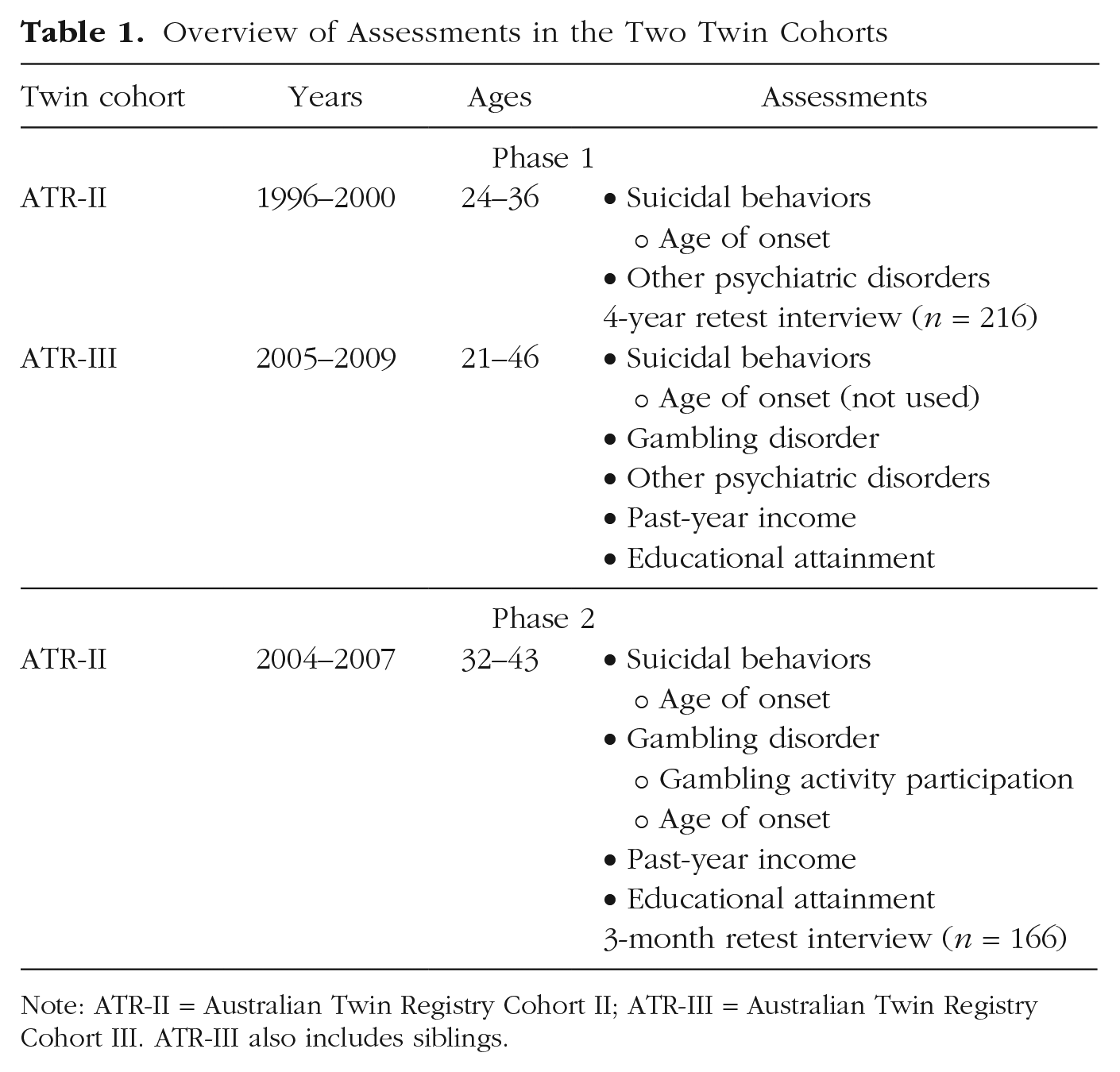
Note: ATR-II = Australian Twin Registry Cohort II; ATR-III = Australian Twin Registry Cohort III. ATR-III also includes siblings.
ATR-III
Gambling and suicidal behaviors were assessed via computer-assisted telephone interviews conducted between 2005 and 2009 (see Table 1). The mean age at assessment was 32.1 years (range = 21–46). The ATR-III study was approved by the institutional review boards at Washington University and QIMR Berghofer, and secondary analysis of the data was approved by the University of Missouri. All participants provided informed consent.
Measures
Gambling disorder
The nine lifetime symptoms of gambling disorder defined in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013) were assessed using the National Opinion Research Center DSM Screen for Gambling Problems (Gerstein et al., 1999) in both cohorts. From these symptoms, two categorical phenotypes were created: a diagnosis of DSM-5 gambling disorder 3 and having at least one symptom of gambling disorder (“disordered gambling”). 4 In ATR-II, the age of onset of each symptom of disordered gambling was also ascertained. Age of onset of gambling disorders was the age at which the first symptom occurred. Age of onset of gambling disorder symptoms was not queried in ATR-III. The internal consistency reliability of the nine-item gambling disorder symptom count was excellent: α = .86. The 3-month test–retest reliabilities among 166 participants from ATR-II were also very good: gambling disorder, r = .95; disordered gambling, r = .95 (tetrachoric correlations); and age of onset of gambling disorders, r = .63 (Pearson correlation).
Suicidal behaviors
At Phase 1, the assessment of suicidal behaviors was the same in both cohorts. Suicidal thoughts (ideation) were assessed with the question, “Have you ever thought about taking your own life?” Participants who reported suicidal thoughts were asked about plans of suicide with the question, “Did you ever have a [suicide] plan?” Suicide attempts were assessed for all participants, even participants without suicidal thoughts or plans, by asking, “Have you ever tried to take your own life?” Participants who reported suicidal thoughts or attempts were also asked to indicate the ages when each of these experiences first and last occurred (the age of first suicide plan was not queried). The 4-year test–retest reliabilities among 216 participants from ATR-II were generally very good: suicidal thoughts, r = .85; suicidal plans, r = .56; suicide attempt, r = .97 (tetrachoric correlations); age of first suicidal thought, r = .67; and age of first suicide attempt, r = .96 (Pearson correlations).
At Phase 2, ATR-II participants were asked, “Have you ever tried to or made a plan to take your own life?” Participants who reported this symptom were asked to indicate the ages at which this behavior first and last occurred and whether it was “ever related to your gambling.” A composite variable for age of suicidality onset was created according to the earliest age reported for the three items of suicidal thoughts, suicide attempts (both from Phase 1), or suicide plans/attempts (from Phase 2).
Other psychiatric disorders
Interviews with both cohorts were based on the Australian version of the Semi-Structured Assessment for the Genetics of Alcoholism (Bucholz et al., 1994) and the diagnostic criteria from the fourth edition of the DSM (APA, 2000). The following psychiatric disorders were included: major depression, alcohol use disorder, cannabis use disorder, nicotine dependence, and conduct disorder. The diagnosis of alcohol use disorder combined abuse and dependence in accordance with changes in the DSM-5 (APA, 2013; because craving was not assessed, it could not be included). The diagnosis of cannabis use disorder was based on an abbreviated six-item assessment that was included in the ATR-II study (Lynskey et al., 2006) and used in the ATR-III study to harmonize the assessments in the two samples (Richmond-Rakerd et al., 2016). The 4-year test–retest reliabilities (tetrachoric correlations) among 216 participants from ATR-II were very good: major depression, r = .81; alcohol use disorder, r = .72; cannabis use disorder, r = .93; nicotine dependence, r = .91; and conduct disorder, r = .84.
Socioeconomic status
Participants were asked to report their current combined household gross income before taxes using a respondent booklet with a list of 12 (ATR-II) or 11 (ATR-III) income ranges to use as response options. These were harmonized across the two cohorts into 11 ordered categories that were used as an ordinal income variable in analyses. Participants also reported the highest educational level attained with a list of five (ATR-II) or 10 (ATR-III) response options that were harmonized across the two cohorts into the five ordered categories of 8 to 10 years schooling (coded as 1); matriculation/year 12 (coded as 2); technical, teachers’ college, technical and further education (TAFE), business or secretarial college (coded as 3); university undergraduate training (coded as 4); and university postgraduate training (coded as 5). These ordered categories were treated as an ordinal educational attainment variable in analyses. Childhood socioeconomic status was based on the response to a question regarding perceived relative financial stability compared with the average family in the community (better off, about average, or worse off) when the participants were 6 to 13 years old.
Data analysis
Cross-sectional phenotypic analyses
Prevalence of gambling disorder and suicidal behaviors was evaluated. Mixed-effects logistic regression was conducted within SAS (Version 9.4) to account for the clustering of data within families. To test whether the effects differed for men and women, interaction terms between sex and gambling disorders were included. We tested whether the cross-sectional phenotypic associations between gambling disorders and suicidal behaviors remained after accounting for other frequently comorbid disorders (major depression, nicotine dependence, alcohol use disorder, cannabis use disorder, and conduct disorder). In addition, given the differing timing of assessments across cohorts, we tested whether the effects of gambling disorders on suicidal behaviors were moderated by cohort.
Longitudinal phenotypic analyses
Longitudinal phenotypic analyses were based on data from ATR-II. The mean ages of onset of suicidal behaviors and gambling behavior and disorder were examined, and the relative temporal precedence of onsets of suicidal behaviors and gambling disorder were compared with a χ2 test for equality of proportions. The prospective effects of suicidal thoughts, plans, and attempts on later gambling disorder were evaluated with mixed-effects logistic regression.
Multilevel discordant-twin analyses
Two-level generalized mixed-effects logistic regression was conducted using SAS PROC GLIMMIX. Mixed-effects logistic regression is used for analyzing clustered binary response data, such as the occurrence of at least one suicide attempt (Hedeker, 2003). With twin data, mixed-effects models are appropriate given the inherent clustering of individual twins (Level 1) within twin pairs (Level 2). Level 1 and Level 2 variances and a random intercept were estimated. Model-estimated coefficients were exponentiated to yield ORs.
A series of three (for suicidal thoughts) or four (for suicidal plans and attempts) models was fit for each suicidal behavior. First, models were run at the individual level that accounted for the nonindependence of twin-pair observations. These analyses examine evidence for an overall effect of disordered gambling on each suicide outcome and approximate analyses conducted with unrelated individuals. Minimally adjusted base models were fit predicting each suicide outcome from the presence or absence of disordered gambling and included age, sex, zygosity, childhood socioeconomic status, adult household income, and educational attainment as covariates. Potential sex and zygosity differences in the effect of disordered gambling were evaluated by including interaction terms. If significant, they were carried forward into fully adjusted analyses. Fully adjusted models were fit including all covariates from the minimally adjusted models and psychiatric conditions (major depression, alcohol use disorder, cannabis use disorder, nicotine dependence, and conduct disorder).
Second, discordant-twin models among MZ and DZ same-sex twin pairs were fit to remove potential sources of confounding that may contribute to the overall effect observed in individual-level models (McGue et al., 2010). Compared with the analysis of unrelated individuals, discordant-twin modeling controls for the shared family environment and genetic factors. Because of this, the approach is uniquely suited to parsing familial effects from possible causal effects of a predictor. Discordant-twin models were represented by the following equation:

in which Yij is the presence or absence of suicidal thoughts, plans, or attempts (depending on the model) for each twin; Xij indicates whether the twin has disordered gambling (0 indicates no symptoms, 1 indicates at least one symptom); and
Third, a set of models that were limited to MZ twins was conducted as a more stringent control for genetic confounding. Fourth, to differentiate the predictors of suicide plans and attempts from suicidal thoughts (May & Klonsky, 2016), individual-level and discordant-twin models that were limited to participants who reported suicidal thoughts were fit to predict suicide plan and attempt.
Biometric twin analyses
Although not the main focus of this study, biometric twin analyses were conducted, using Mplus (Version 8; Muthén & Muthén, 2017), to provide insight into any significant between-families effects observed in the multilevel discordant-twin analyses. In particular, bivariate twin analyses were employed to determine the extent to which any between-families influences of disordered gambling on suicidal behavior were explained by genetic or shared environmental influences. The logic behind univariate twin modeling is presented in the Supplemental Material available online. Below we describe the logic behind bivariate twin modeling.
The logic of bivariate twin modeling is similar to univariate twin modeling (the analysis of a single trait). With bivariate twin modeling, one is interested in the cross-trait and the within-trait similarity. For example, one examines the similarity of disordered gambling in one twin with suicidal thoughts in the other twin. If the MZ cross-trait, cross-twin similarity is greater than the DZ cross-trait, cross-twin similarity, then one infers that genetic factors are contributing to the association between disordered gambling and suicidal thoughts. In other words, there is at least one gene that is a risk factor for both disordered gambling and suicidal thoughts. If the DZ cross-trait, cross-twin similarity is greater than half the MZ cross-trait, cross-twin similarity, then one infers that shared environmental factors are contributing to the association between disordered gambling and suicidal thoughts. Unique environmental factors are implicated when the MZ cross-trait, cross-twin similarity is substantially less than the cross-trait, within-twins correlation between disordered gambling and suicidal thoughts. This represents the correlation between disordered gambling and suicidal thoughts that remains after controlling for genetic and shared environmental influences, that is, the factors that are not shared between twins. The unique environmental correlation represents the within-twin-pair association between disordered gambling and suicidal thoughts and is consistent with a potentially causal association (Turkheimer & Harden, 2014).
Results
Cross-sectional phenotypic analyses in ATR-II and ATR-III
Prevalence
About one quarter of participants (26.05%) reported having had suicidal thoughts, 6.77% reported having made a suicide plan, and 4.04% had attempted suicide. Men and women were equally likely to report having had suicidal thoughts or making a suicide plan, but men were significantly less likely to report having made a suicide attempt (OR = 0.59, 95% confidence interval [CI] = [0.47, 0.76]). Among participants who had made a suicide attempt, 61.86% had made a single attempt, and this did not differ for men and women (men = 61.96%; women = 61.83%); the average number of attempts was 2.09 (SD = 2.47, maximum = 20), and this also did not differ for men (M = 1.92, SD = 2.41) and women (M = 2.15, SD = 2.50). As expected, suicide attempt was strongly correlated with having had suicidal thoughts and having made a plan (Table 2), and it was exceedingly rare to report a suicide attempt without also reporting having had suicidal thoughts (0.89%). On the other hand, suicide attempt was frequently reported in the absence of ever having made a plan (38.39%).
Correlations Between Study Variables Among Men (n = 3,281) and Women (n = 5,046)
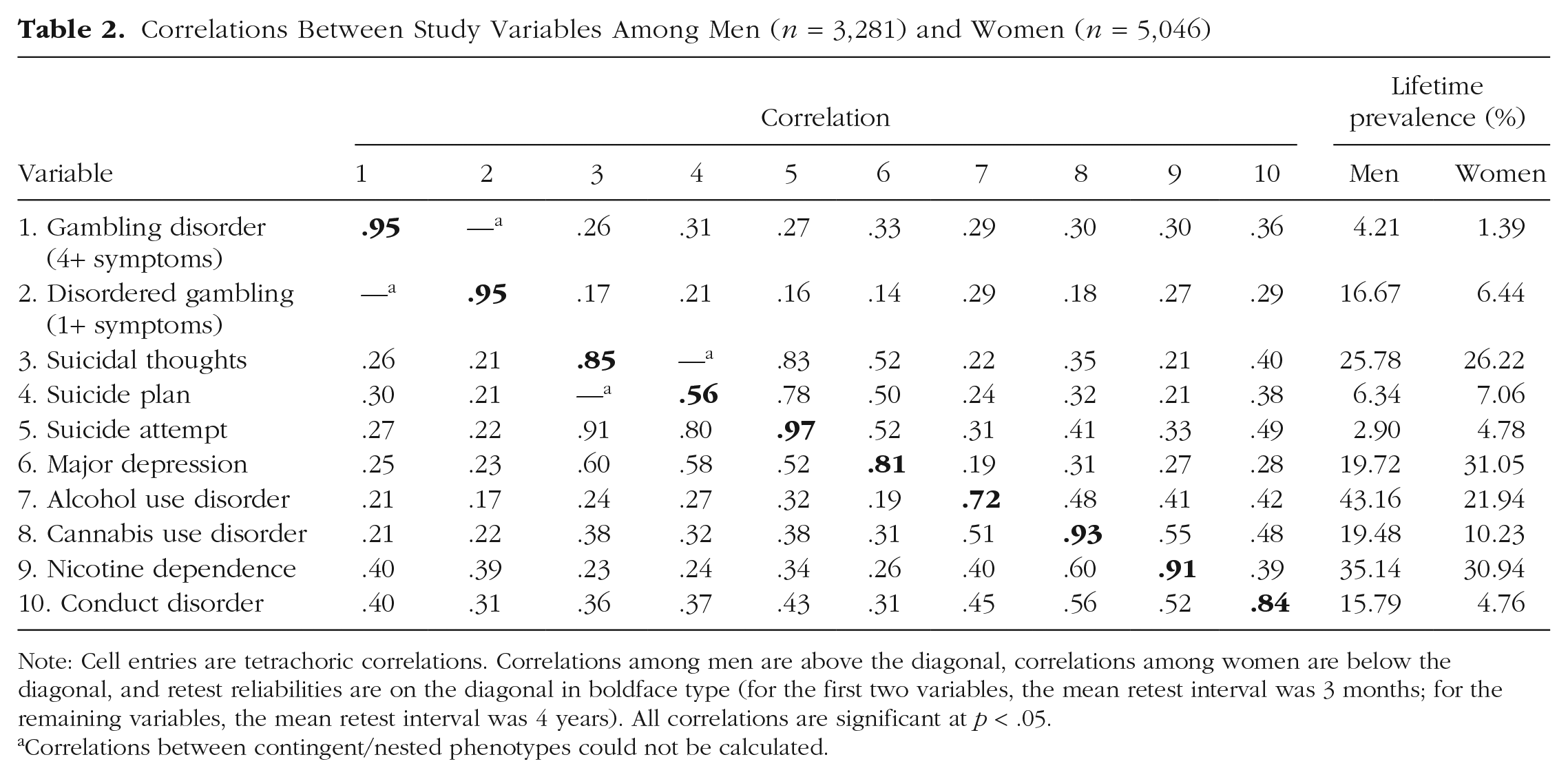
Note: Cell entries are tetrachoric correlations. Correlations among men are above the diagonal, correlations among women are below the diagonal, and retest reliabilities are on the diagonal in boldface type (for the first two variables, the mean retest interval was 3 months; for the remaining variables, the mean retest interval was 4 years). All correlations are significant at p < .05.
Correlations between contingent/nested phenotypes could not be calculated.
Regarding gambling disorder, 2.50% met the criteria for a lifetime diagnosis of DSM-5 (APA, 2013) gambling disorder (4.21% of men and 1.39% of women), and 10.47% (16.67% of men and 6.44% of women) met the criteria for disordered gambling. The prevalence of the nine individual symptoms of DSM-5 (APA, 2013) gambling disorder is presented in Table S1 in the Supplemental Material, the prevalence of participation in 11 different gambling activities is presented in Table S2 in the Supplemental Material, and the amounts of time and money spent on gambling are presented in Table S3 in the Supplemental Material. Of particular interest is the costliness of gambling disorder and disordered gambling in terms of the time and money spent; during the year of peak gambling involvement, individuals with gambling disorder and disordered gambling had spent 105% and 40%, respectively, of their yearly annual household income on gambling (see Table S3 in the Supplemental Material).
Associations between gambling disorder and suicidal behaviors
Individuals with gambling disorder were about 3 times as likely as individuals without a diagnosis to report suicidal thoughts (OR = 2.62, 95% CI = [1.95, 3.51]), plans (OR = 3.48, 95% CI = [2.39, 5.05]), and attempts (OR = 3.05, 95% CI = [1.91, 4.87]); 47.60% of individuals with gambling disorder reported having suicidal thoughts, 19.71% reported having made a suicide plan, and 11.06% had made a suicide attempt. The magnitude of the associations between gambling disorder and suicidal behaviors did not differ for men and women: thoughts, F(1, 3386) = 0.17, p = .68; plans, F(1, 3386) = 0.02, p = .89; attempts, F(1, 3386) = 0.00, p = .96. They also did not differ between the ATR-II and ATR-III cohorts: thoughts, F(1, 3386) = 0.16, p = .69; plans, F(1, 3386) = 0.14, p = .71; attempts, F(1, 3386) = 1.34, p = .25, which suggests that the different timing of assessments for the two cohorts did not affect the results. The associations between the nine individual symptoms of DSM-5 (APA, 2013) gambling disorder and suicidal thoughts (mean OR = 2.33), plans (mean OR = 3.10), and attempts (mean OR = 2.81) are presented in Table S1 in the Supplemental Material, and the association of specific gambling activities with suicide plans or attempts is presented in Table S2 in the Supplemental Material. Although all the gambling disorder symptoms were associated with all three suicidal behaviors, the association between the symptom of borrowing money to relieve a desperate financial situation (i.e., “bail out”) was especially strongly associated with suicide attempt (OR = 4.60, 95% CI = [2.64, 7.99]; see Table S1 in the Supplemental Material). Of the 11 gambling activities, the only one that was associated with suicidal behaviors was participation in electronic gambling machines (OR = 1.66, 95% CI = [1.20, 2.29]; see Table S2 in the Supplemental Material).
Associations between disordered gambling and suicidal behaviors
Participants with at least one symptom of gambling disorder were about twice as likely as participants without any symptoms to report suicidal thoughts (OR = 1.78, 95% CI = [1.52, 2.08]), plans (OR = 2.08, 95% CI = [1.65, 2.63]), and attempts (OR = 1.89, 95% CI = [1.41, 2.55]). 6 These associations also did not differ in magnitude for men and women: thoughts, F(1, 3386) = 1.57, p = .21; plans, F(1, 3386) = 0.06, p = .81; attempts, F(1, 3386) = 0.58, p = .44. They also did not differ across the two cohorts: thoughts, F(1, 3386) = 0.38, p = .54; plans, F(1, 3386) = 0.03, p = 087; attempts, F(1, 3386) = 0.33, p = .57, which, again, supports the decision to combine the two cohorts.
Role of psychiatric comorbidity
There were significant associations between suicidal thoughts, plans, and attempts and psychiatric disorders (see Table 2). There were also significant associations between gambling disorder and psychiatric disorders (see Table 2). After accounting for psychiatric comorbidity, the associations between gambling disorder and suicidal thoughts and attempt became nonsignificant (thoughts: OR = 1.37, 95% CI = [0.99, 1.90]; attempt: OR = 1.22, 95% CI = [0.74, 2.01]), and the association with suicidal plan remained significant but was attenuated (OR = 1.70, 95% CI = [1.13, 2.55]). On average, the ORs of the associations between gambling disorder and the three suicidal behaviors were attenuated by 79.40%, and this did not substantially differ for men (80.87%) and women (68.57%). Among participants with a history of gambling disorder, suicidal thoughts (5%), plan (2%), and attempt (0%) never or rarely occurred in the absence of a history of major depression, alcohol use disorder, cannabis use disorder, or conduct disorder (nicotine dependence was not included in this analysis).
Compared with gambling disorder, the magnitudes of the associations between disordered gambling and psychiatric disorders were somewhat weaker (Table 2). As with gambling disorder, the associations between disordered gambling and suicidal thoughts and plans remained but were attenuated (thoughts: OR = 1.28, 95% CI = [1.08, 1.53]; plans: OR = 1.42, 95% CI = [1.10, 1.83]), and the association of disordered gambling with suicide attempt became nonsignificant (OR = 1.11, 95% CI = [0.80, 1.53]) after accounting for history of major depression, alcohol use disorder, cannabis use disorder, nicotine dependence, and conduct disorder. On average, the ORs of the associations between disordered gambling and the three suicidal behaviors were attenuated by 70.95%, and this did not substantially differ for men (68.41%) and women (68.85%). Among participants with a history of disordered gambling, suicidal thoughts (13%), plan (5%), and attempt (3%) rarely occurred in the absence of a history of comorbid major depression, alcohol use disorder, cannabis use disorder, or conduct disorder.
Longitudinal phenotypic analyses in ATR-II
Ages of onset of gambling disorder and suicidal behaviors
There were 1,251 (27.54%) individuals in ATR-II with a history of any suicidal behavior. The mean age of onset of suicidal behavior was 20.40 years (SD = 6.4), and this did not differ for men and women (men: M = 20.77 years; women: M = 20.14 years; t = 1.72, p = .09). There were 125 individuals (2.75%) with a history of gambling disorder. The mean age of onset of gambling disorder was 24.40 years (SD = 6.39), which differed for men and women (men: M = 22.87 years; women: M = 27.14 years; t = −3.74, p = .0003).
Temporal precedence of gambling disorder and suicidal behavior
Among 66 individuals with co-occurring gambling disorder and suicidal behavior, 61% (n = 40) of the time, gambling disorder had a later onset than did suicidal behavior; 29% (n = 19) of the time, it had an earlier onset; and 11% (n = 7) of the time, gambling disorder and suicidal behavior first occurred in the same year. The result of the test of unequal proportions of later onset compared with onset was χ2(1) = 7.47, p < .006. These proportions differed between men and women (men: later = .54, earlier = .38, same year = .10; women: later = .75, earlier = .13, same year = .13). The difference between later and earlier was χ2(1) = 4.79, p = .03.
Gambling disorder also had a later offset than suicidal behavior 86% (n = 55) of the time. The result of the test of unequal proportions of later compared with earlier offset was χ2(1) = 48.50, p < .0001. 7 In addition, 30% (n = 20) of the time, the first gambling disorder symptom had occurred 2 to 17 years (M = 10.11 years) after the last suicidal behavior had occurred. Gambling disorder was also more persistent than suicidal behaviors; mean durations from onset to recency were 10.23 years (SD = 6.99) and 6.48 years (SD = 7.10), respectively. The average age of the 66 participants with co-occurring gambling disorder and suicidal behavior was 38.03 years; 32 (48.48%) of these participants had experienced symptoms of disordered gambling within the past year, whereas none had experienced a suicidal thought, plan, or attempt within the past year. The average number of years since the last gambling disorder symptom and suicidal behavior were 2.36 years (SD = 3.34) and 10.57 years (SD = 5.65), respectively.
A small fraction of individuals attributed their suicidal behavior to gambling. At the Phase 2 interview, eight of 424 participants who reported a suicide plan or attempt acknowledged that it was related to their gambling. Seven had a lifetime history of gambling disorder, which represented 20.00% of participants with co-occurring gambling disorder and suicidal behavior (according to this single question about suicide plans or attempts).
Longitudinal associations between suicidal behaviors and gambling disorder
Participants who reported suicidal thoughts (OR = 2.58, 95% CI = [1.79, 3.71]), plans (OR = 3.74, 95% CI = [2.36, 5.94]), and attempts (OR = 2.41, 95% CI = [1.23, 4.72]) at Phase 1 were more likely to meet the lifetime criteria for gambling disorder nearly 8 years later at Phase 2, 8 and this did not significantly differ for men and women (all ps > .36). After accounting for psychiatric comorbidity, the prospective association between suicidal plans and gambling disorder remained significant but was attenuated (OR = 1.83, 95% CI = [1.10, 3.04]), and the prospective associations between suicidal thoughts and attempt and gambling disorder became nonsignificant (thoughts: OR = 1.36, 95% CI = [0.91, 2.03]); attempt: OR = 0.89, 95% CI = [0.41, 1.92]). Note that these results are very similar to the cross-sectional phenotypic associations reported above, which again suggests that the different timing of assessments for the two cohorts did not affect the results and supports combining them in the cross-sectional phenotypic and multilevel discordant-twin-modeling analyses.
Multilevel discordant-twin analyses in ATR-II and ATR-III
Despite the large sample size of more than 2,300 complete same-sex twin pairs, there were only 75 pairs discordant for gambling disorder. Therefore, the multilevel discordant-twin analyses were based on the broader disordered gambling phenotype. There were 307 same-sex twin pairs discordant for disordered gambling in the full sample, 170 discordant MZ pairs (76 female, 94 male), and 137 discordant DZ pairs (59 female, 78 male). The affected twin in the discordant pairs usually had a single symptom of disordered gambling (59.28%), and the average number of symptoms was 2.23 (SD = 2.05).
Preliminary descriptive analyses of the association between suicidal behaviors and disordered gambling in discordant-twin pairs are presented in Table 3. Among disordered gambling discordant-twin pairs, the affected twin was significantly more likely to have experienced suicidal thoughts than the unaffected cotwin (35.50% vs. 26.71%); was more likely to have made a suicide plan than the unaffected cotwin, although this difference was not significant (9.45% vs. 7.82%); and was more likely to have made a suicide attempt than the unaffected cotwin, although this difference was also not significant (6.51% vs. 4.56%). For all three suicidal behaviors, the within-twin pair association with disordered gambling was stronger among men than women. These associations and potential sex differences were more rigorously examined in the multilevel models.
Suicidal Thoughts, Plan, and Attempt Among Twin Pairs Discordant for Disordered Gambling
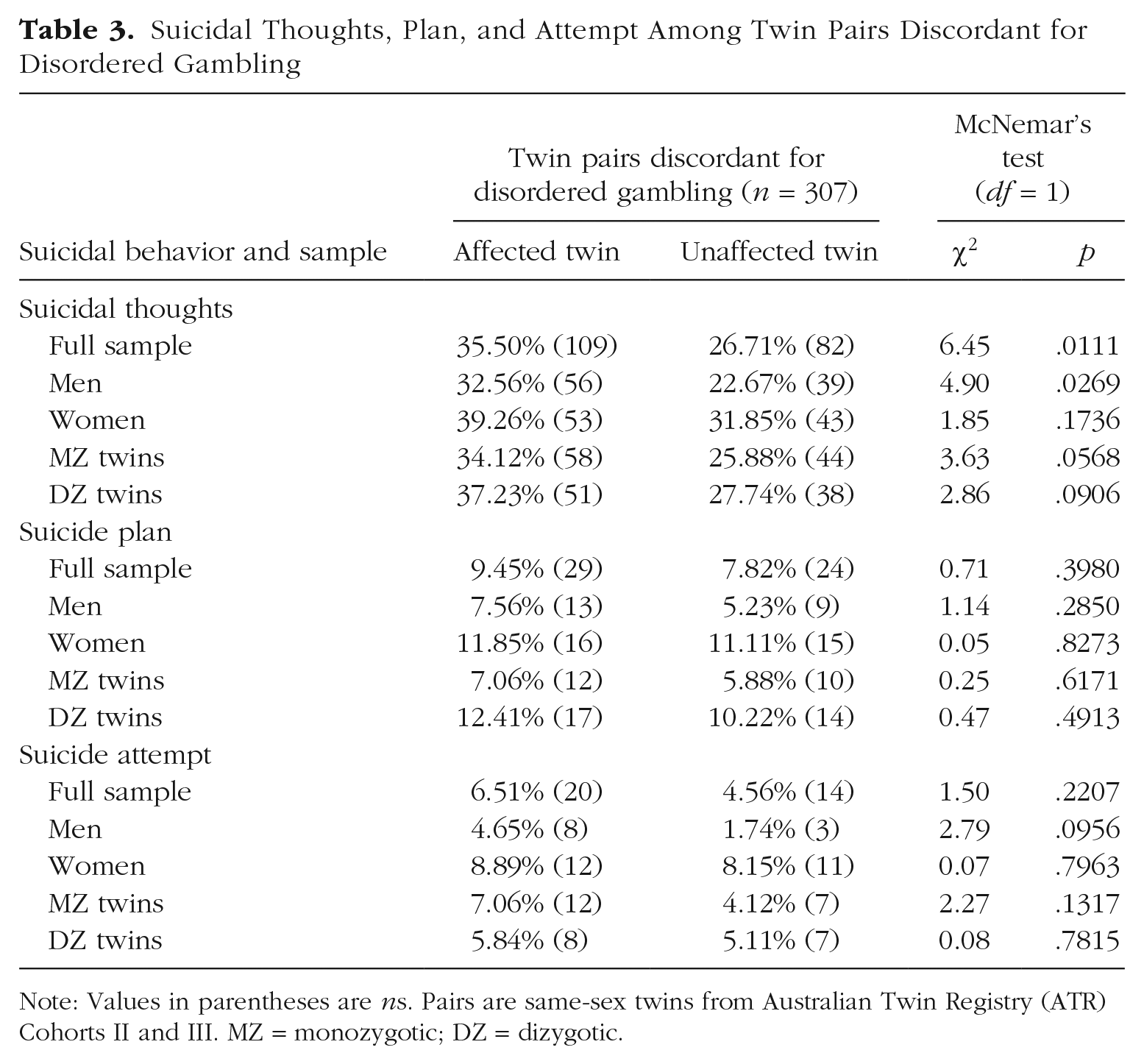
Note: Values in parentheses are ns. Pairs are same-sex twins from Australian Twin Registry (ATR) Cohorts II and III. MZ = monozygotic; DZ = dizygotic.
Suicidal thoughts
Individual-level model
Disordered gambling was associated with increased odds of having suicidal thoughts (OR = 2.00, 95% CI = [1.65, 2.41]). This association was attenuated but remained significant after accounting for comorbid psychopathology (OR = 1.37, 95% CI = [1.12, 1.68]; see Fig. 1). Several covariates also showed significant associations with suicidal thoughts (see Table 4, top).
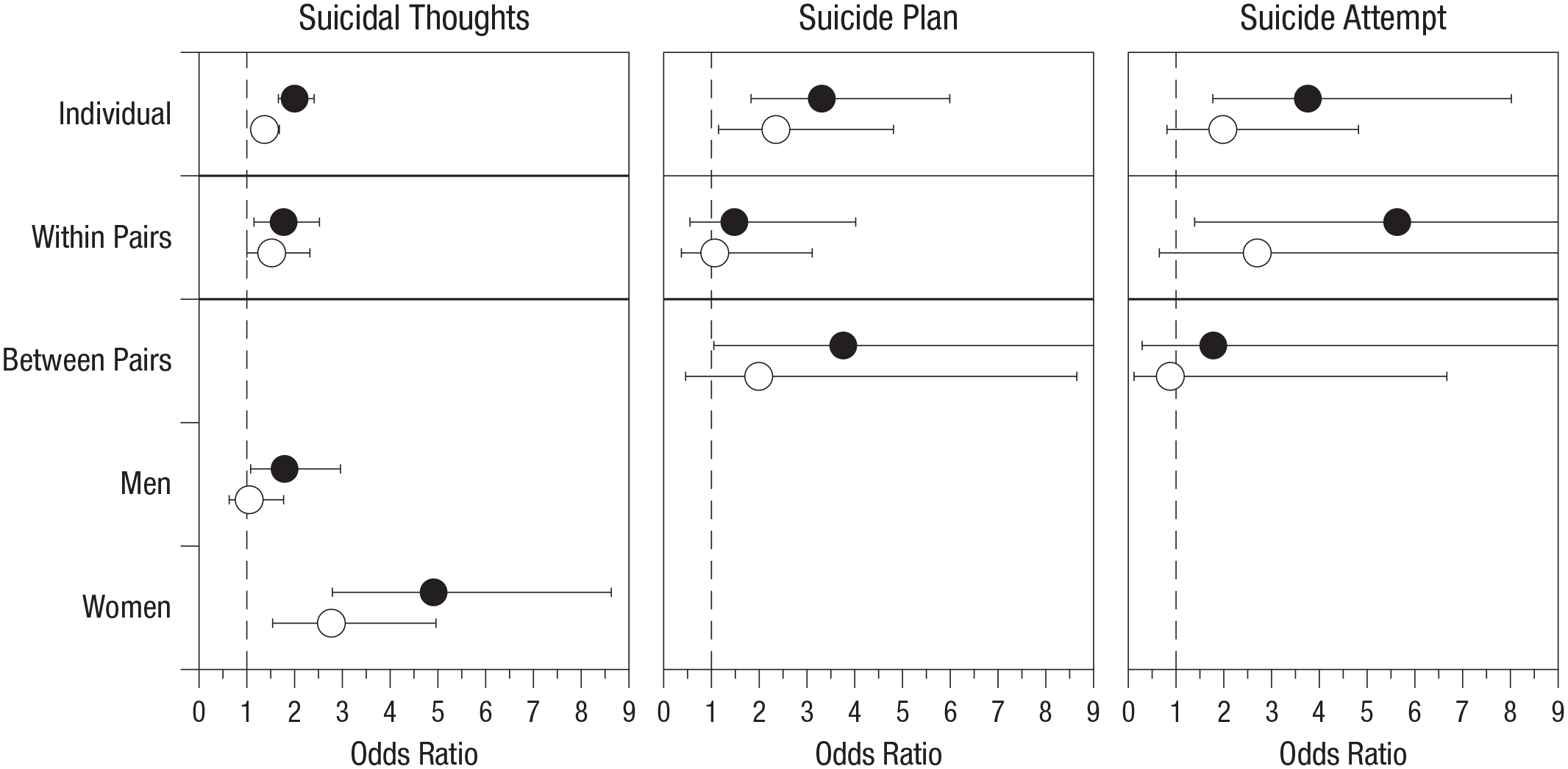
Estimates (and 95% confidence intervals) from multilevel models predicting suicidal thoughts, plan, and attempt from disordered gambling. Individual-level effects are in the top row, within-twin-pairs effects (that include potentially causal effects) are in the middle row, and between-twin-pairs effects (that include genetic and shared environmental influences) are in the bottom row; see Table 4 for a list of the covariates included in the base and adjusted models. The filled and open circles represent estimates from the base and adjusted models, respectively. Because there was a significant sex difference for the between-pairs effects for suicidal thoughts, the effects are plotted separately for men and women. Not shown in the figure is the significant sex difference for the unadjusted within-twin-pairs effect for suicide attempt (unadjusted: men odds ratio [OR] = 136.74, women OR = 1.89; adjusted: men OR = 23.13, women OR = 1.38). The upper bounds for the four confidence intervals that exceeded the chart boundaries were: suicide plan, between-pairs base model: 13.47; suicide attempt, within-pairs base model: 22.78; suicide attempt, within-pairs adjusted model: 11.17; suicide attempt, between-pairs base model: 11.05.
Results of Individual-Level and Multilevel Discordant-Twin Analyses Predicting Suicidal Thoughts, Plan, and Attempt From Disordered Gambling
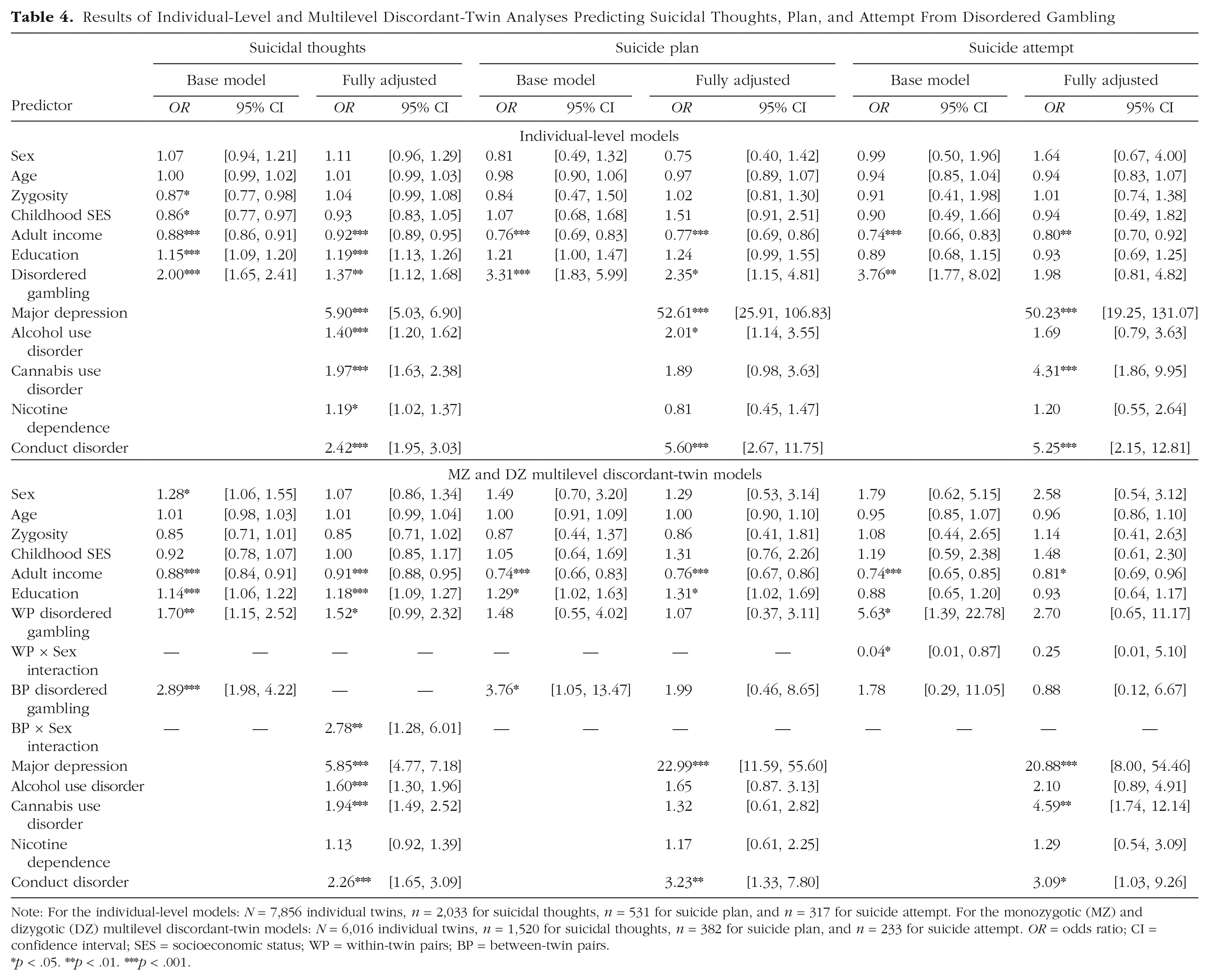
Note: For the individual-level models: N = 7,856 individual twins, n = 2,033 for suicidal thoughts, n = 531 for suicide plan, and n = 317 for suicide attempt. For the monozygotic (MZ) and dizygotic (DZ) multilevel discordant-twin models: N = 6,016 individual twins, n = 1,520 for suicidal thoughts, n = 382 for suicide plan, and n = 233 for suicide attempt. OR = odds ratio; CI = confidence interval; SES = socioeconomic status; WP = within-twin pairs; BP = between-twin pairs.
p < .05. **p < .01. ***p < .001.
MZ and DZ discordant-twin model
In the base model, significant associations with suicidal thoughts were observed at both the within-pairs and between-pairs levels (within pairs: OR = 1.70, 95% CI = [1.15, 2.52]; between pairs: OR = 2.89, 95% CI = [1.98, 4.22]). This means that within discordant-twin pairs, the twin who reported disordered gambling had 70% greater odds of having suicidal thoughts than the unaffected co-twin; compared with pairs in which neither twin reported disordered gambling, members of twin pairs in which at least one twin engaged in disordered gambling had almost 3 times the odds of suicidal thoughts. The effect of disordered gambling between twin pairs differed for men and women (interaction OR = 2.56, 95% CI = [1.21, 5.41]) such that there was a significantly greater effect in women than men (see Fig. 1). The effect within twin pairs did not significantly differ for MZ and DZ twins (OR = 0.76, 95% CI = [0.34, 1.66]).
Once comorbid psychopathology was included in the model, the within-twin-pairs effect became nonsignificant (OR = 1.52, 95% CI = [1.00, 2.32]), but the interaction of between-twin pairs and sex remained significant (interaction OR = 2.78, 95% CI = [1.28, 6.01]). Exploring this interaction further, we found that there was a significant between-pairs effect for women (OR = 2.77, 95% CI = [1.54, 4.96]) but not men (OR = 1.05, 95% CI = [0.63, 1.77]; see Fig. 1). The inclusion of comorbid psychopathology in the models attenuated the between-pairs effect by 55% in women and 94% in men; there were significant effects of major depression, alcohol use disorder, cannabis use disorder, and conduct disorder in both sexes (see Table 4, bottom). The results of the discordant-twin model restricted to MZ twins were consistent with those from the MZ and DZ models (see Table S5 in the Supplemental Material).
Suicide plan
Individual-level model
In the minimally adjusted individual-level model, disordered gambling was associated with more than 3 times the odds of reporting a suicide plan in one’s lifetime (OR = 3.31, 95% CI = [1.83, 5.99]). The inclusion of comorbid psychopathology reduced this association, but it remained significant (OR = 2.35, 95% CI = [1.15, 4.81]; see Table 4, top).
MZ and DZ discordant-twin model
In the minimally adjusted model including only demographic covariates, the between-pairs effect of disordered gambling was significant (OR = 3.76, 95% CI = [1.05, 13.47]), but the within-twin-pairs effect was not (OR = 1.48, 95% CI = [0.55, 4.02]). This means there was no evidence for a potentially causal effect of disordered gambling on suicidal plan, but being a member of a twin pair in which at least one twin reported disordered gambling was associated with almost 4 times the odds of having made a suicide plan. There was no evidence for sex differences in these effects. The within-twin-pairs effect did not significantly differ for MZ and DZ twins (OR = 0.58, 95% CI = [0.08, 4.29]). Comorbid psychopathology, primarily major depression and conduct disorder, appeared to largely explain the between-pairs effect of disordered gambling given that this association became nonsignificant and was attenuated by 64% with the inclusion of these covariates (OR = 1.99, 95% CI = [0.46, 8.65]; see Table 4, bottom). The results of the discordant-twin model restricted to MZ twins was consistent with those from the MZ and DZ models (see Table S5 in the Supplemental Material).
Restricting analyses to participants with suicidal thoughts
Analyses predicting suicidal plan were conducted in the subset of participants who reported having suicidal thoughts. Of primary interest was the extent to which the original effect sizes from the full samples were attenuated or amplified once suicidal thoughts were held constant. For a comparison of the results of the two sets of models, see Table S6 in the Supplemental Material.
The results of the individual-level analyses of suicide plan controlling for suicidal thoughts were similar to the original analyses. Disordered gambling remained a significant predictor of suicide plan in the minimally and fully adjusted models but with effect sizes attenuated by 79% and 93%, respectively (see Table S6 in the Supplemental Material).
The results of the discordant-twin analyses of suicide plan controlling for suicidal thoughts were similar to the original analyses. The between-twin-pairs effect of disordered gambling remained a significant predictor of suicide plan in the minimally adjusted model but with the effect size attenuated by 60% (see Table S6 in the Supplemental Material).
Suicide attempt
Individual-level model
In the minimally adjusted individual-level model, disordered gambling was associated with almost 4 times the odds of having made a suicide attempt (OR = 3.76, 95% CI = [1.77, 8.02]). After comorbid psychopathology was included in the model, the association between disordered gambling and suicide attempt was attenuated and nonsignificant (OR = 1.98, 95% CI = [0.81, 4.82]).
MZ and DZ discordant-twin model
In the minimally adjusted discordant-twin model, there was not a significant between-pairs effect (OR = 1.78, 95% CI = [0.29, 11.05]), but there was a significant within-twin-pairs effect of disordered gambling on lifetime suicide attempt (OR = 5.63, 95% CI = [1.39, 22.78]). Compared with a co-twin without disordered gambling, the twin with disordered gambling had more than 5 times the odds of having made a suicide attempt. There was a significant sex difference in the within-pairs effect (interaction OR = 0.04, 95% CI = [0.002, 0.87]) such that the effect was far greater for men than women (men: OR = 136.74, 95% CI = [6.35, 2944.22]; women: OR = 1.89, 95% CI = [0.36, 9.87]). The within-twin-pairs effect did not significantly differ for MZ and DZ twins (ORs = 2.60, 95% CI = [0.18, 38.25]).
With the inclusion of comorbid psychopathology in the model, the interaction of within-twin pairs and sex became nonsignificant, although the effect size was still large (OR = 0.25, 95% CI = [0.01, 5.10]). The within-twin-pairs effect was much larger among men (OR = 23.13, 95% CI = [0.55, 967.87]) than among women (OR = 1.38, 95% CI = [0.25, 7.75]), although both effects were not significant. The results of the discordant-twin model restricted to MZ twins were consistent with those from the MZ and DZ model (see Table S5 in the Supplemental Material).
Restricting analyses to participants with a history of suicidal thoughts
As was done for suicidal plans, analyses predicting suicide attempt were conducted among the subset of participants who reported experiencing suicidal thoughts. For a comparison of the original results and the results after controlling for suicidal thoughts, see Table S6 in the Supplemental Material.
The results of the individual-level analyses of suicide attempt controlling for suicidal thoughts were similar to the original analyses. Disordered gambling remained a significant predictor of suicide attempt in the minimally adjusted model but with the effect size attenuated by 53% (see Table S6 in the Supplemental Material).
The results of the discordant-twin analyses of suicide attempt controlling for suicidal thoughts were similar to the original analyses. The within-twin-pairs effect of disordered gambling remained a significant predictor of suicide attempt in the minimally adjusted model; the effect size increased by 178%. This effect was substantially larger and significant among men but not women. In the fully adjusted model, the within-twin-pairs effect was still nonsignificant, although the effect size increased by 575% (see Table S6 in the Supplemental Material).
Biometric twin analyses of disordered gambling and suicidal thoughts
Biometric twin modeling was conducted to follow up on the between-twin-pairs association between disordered gambling and suicidal thoughts that was significant among women but not men. Twin correlations for disordered gambling and suicidal thoughts (see Table S7 in the Supplemental Material) and the results of univariate twin modeling (see Table S8 in the Supplemental Material) are presented in the Supplemental Material. The relative contributions of genetic, shared environmental, and unique environmental influences to disordered gambling liability were 0.54, 0, and 0.46, respectively, and were 0.51, 0, and 0.49, respectively, for the propensity to experience suicidal thoughts. The estimates for men and women did not significantly differ (see Table S8 in the Supplemental Material).
The MZ cross-trait twin correlation for disordered gambling and suicidal thoughts was significant among women (r = .25) but not among men (r = .09; see Table S7 in the Supplemental Material). When a bivariate biometric twin model was fit to the data allowing the parameter estimates to differ for men and women, there was not a significant reduction in model fit when the contributions of shared environmental influences were dropped: χ2(6) = 0.92, p = .99, and a model that included genetic and unique environmental influences provided an adequate fit to the data: χ2(24) = 28.87, p = .23. The genetic contributions to disordered gambling and suicidal thoughts were significantly correlated in women (r = .42, 95% CI = [.26, .63]), but not in men (r = .15, 95% CI = [–.15, .45]), and the unique environmental contributions to disordered gambling and suicidal thoughts were significantly correlated in men (r = .26, 95% CI = [.03, .48],) but not in women (r = −.04, 95% CI = [–.42, .17]); these estimates were relatively unchanged when shared environmental influences were included in the model. These results are consistent with the multilevel discordant-twin model showing that the between-twin-pairs effects of disordered gambling were associated with suicidal thoughts among women but not among men and extends these findings by demonstrating that the between-twin-pairs effects were due to common genetic influences.
Discussion
The present study establishes significant associations between gambling disorders and suicidal thoughts, plan, and attempt in a general population sample for the first time. It also is the first study to dissect these associations into family-level components (including genetic and shared environmental factors) and individual-level components (including a potentially causal relation).
Differences between suicidal thoughts, plan, and attempt
The causes of the associations with disordered gambling differed for suicidal thoughts, plan, and attempt. In the multilevel discordant-twin models, the between-twin-pairs associations between disordered gambling and suicidal thoughts and plan were larger than the within-twin-pairs associations. The opposite was true for suicide attempt, in which the within-twin-pairs association was larger than the between-twin-pairs association. This means that the associations of disordered gambling with suicidal ideation or plan were due mainly to genetic or shared environmental influences that differed between families, whereas the association with suicide attempt was due mainly to unique environmental influences that varied within twin pairs. Combining suicidal behaviors together into an overall “suicidality” measure may obscure important differences.
There were also important sex differences in these associations. The between-twin-pairs association of disordered gambling with suicidal thoughts differed among men and women such that the association was larger and significant only among women; follow-up biometric analyses narrowed down the source of the between-families effect to shared genes. The within-twin-pairs association of disordered gambling with suicide attempt was larger and significant only among men. This means that there is something that differs within male twin pairs discordant for disordered gambling that contributes to the association with suicide attempt and is consistent with a potentially causal relation.
From suicidal thoughts to suicide plan and attempt
There is a concern that much of the extant suicidality literature has conflated the correlates of suicide attempt with the correlates of suicidal thoughts given convincing evidence that many of the correlates of suicide attempt disappear or are substantially reduced after accounting for the presence of suicidal ideation (Klonsky et al., 2016; May & Klonsky, 2016). Therefore, we revisited the multilevel analyses of suicide plan and attempt restricted to participants with a history of suicidal thoughts.
At the individual and the between-twin-pairs levels, the associations of disordered gambling with suicide plan remained significant but were substantially attenuated, which suggests that much of the association was with suicidal thinking. Nonetheless, a significant association of disordered gambling with suicide plan remained after accounting for suicidal thoughts. This residual association suggests that disordered gambling may also be related to the progression from suicidal thinking to forming a suicide plan.
The association of disordered gambling with suicide attempt at the individual level was substantially attenuated and no longer significant after accounting for a history of suicidal thoughts. At the within-twin-pairs level, however, the association between disordered gambling and suicide attempt was substantially amplified, with the sex difference intact. This suggests that not only is the within-twin-pairs difference in disordered gambling associated with suicide attempt among men but also that by stripping away the influence on suicidal thinking, an even stronger association was revealed. This intriguing and novel (yet unpredicted) finding requires replication.
Role of psychiatric comorbidity
The cross-sectional associations between gambling disorders and the three suicidal behaviors were attenuated by more than 70% after accounting for comorbid psychopathology, but the magnitude of the contribution of psychiatric comorbidity to the associations between disordered gambling and suicide plan and attempt were substantially reduced when analyses were restricted to participants with a history of suicidal thoughts. This is consistent with the results of a massive international survey of 11 nations (Nock, Borges, Bromet, Alonso, et al., 2008) and a large U.S. national survey (Hoertel et al., 2015). Comorbid psychopathology is primarily associated with suicidal thoughts but may also play a role in the progression to suicide plan and attempt.
Temporal relation between gambling disorder and suicidal behaviors
The ability to draw causal inferences from the multilevel discordant-twin analyses was hampered by the reliance on cross-sectional data. We attempted to discern the temporal relation between gambling disorder and suicidal behaviors from retrospectively reported ages of onset and recency. The mean age of onset of suicidal behaviors (20.40 years) was earlier than the mean age of onset of gambling disorder (24.40 years), and for the majority of participants who experienced both, the onset of suicidal behaviors was more likely to precede the onset of gambling disorder (61%), the offset of suicidal behaviors was more likely to precede the resolution of gambling disorder (86%), and there was a substantial percentage (30%) whose first symptom of gambling disorder postdated the last suicidal behavior by many years. This suggests that gambling disorder was unlikely to be a predominant cause of suicidal behavior. This is consistent with the finding that only a minority of participants with co-occurring gambling disorder and suicidal behavior (20%) attributed the suicidal behavior to gambling. Although this was based on a small number of individuals, it is strikingly similar to the rate observed among individuals with co-occurring gambling disorder and suicide attempt (21%) in a Canadian study (Hodgins et al., 2006).
Both the present Australian study and a previous Swedish study suggest that there might be important differences between men and women in the sequence of gambling disorder and suicidal behavior. In the present study, men were significantly more likely than women to experience an onset of gambling disorder that preceded the onset of suicidal behavior (38% vs. 13%). Although the differences were not statistically significant, the Swedish study (Sundqvist & Rosendahl, 2019) also found that suicidal behavior onset more often came after or in the same year as the onset of gambling disorder among men (42%) than among women (27%). These data raise the possibility that gambling disorder may be more likely to be a cause of suicidal behavior among men than among women, which is consistent with the results of the discordant-twin analyses of suicide attempt.
Potentially causal effect of disordered gambling on suicide attempt among men
The processes by which disordered gambling may potentially cause a suicide attempt particularly among men remain unclear. We hypothesize that this may have to do with the uniquely life-altering financial toll that disordered gambling can exact. Historically, population rates of suicide have been associated with major economic downturns. The highest rate of suicide in the last 100 years in the United States and Australia occurred during the Great Depression of 1929–1933 (Morrell et al., 1993; Tapia Granados & Diez Roux, 2009), and all the excess suicides occurred among men (Macmahon et al., 1963; Morrell et al., 1993). The more recent Great Recession of 2008 similarly led to an uptick in “economic suicides,” with a fourfold greater increase among men than among women (Reeves et al., 2014). 9 A psychological autopsy study conducted in Hong Kong of 150 completed suicides, compared with 150 matched living control participants, demonstrated that suicides were more likely to be preceded by unmanageable debt or unemployment (Chen et al., 2006), and of the 17 gambling-related suicides, all were characterized by unmanageable debt (Wong et al., 2010). These financial crises may pose a greater suicide risk among men than women because they may threaten the traditional primary role identities of men as being financially stable and competitive in the labor force (Girard, 1993; Stack, 2000), which may lead to feelings of burdensomeness and hopelessness (Klonsky & May, 2015; Van Orden et al., 2010).
Limitations
There were at least five limitations of the current study. First, the sex-specific multilevel discordant-twin models of suicide attempt were underpowered, which makes it difficult to interrogate the significant difference observed between men and women. Second, potentially important psychiatric disorders, such as bipolar disorder, posttraumatic stress disorder, panic disorder, and generalized anxiety disorder, and traits such as impulsivity were not included. These might have contributed to the between-twin-pairs effect of disordered gambling on suicidal thoughts among women or to the progression to suicide plan or attempt in either sex. Third, although there was adequate test–retest reliability of the measures, they were all based on retrospective reports, which have known weaknesses (e.g., Henry et al., 1994), especially assessments of ages of onset (e.g., Prusoff et al., 1988). Fourth, given the dearth of longitudinal data on suicidal behaviors, the availability of assessments at two time points was a strength of the study. However, the longitudinal nature of the study was extremely limited. The study would have been strengthened by assessing suicidal and gambling behaviors at multiple time points, and this should be a priority for future research. Fifth, the participants represented a narrow age range (27–43), were primarily of Northern European ancestry, and resided in Australia. In addition, the data were collected more than a decade ago. Thus, it is not clear the extent to which the results of this study can be generalized to other ages, ethnicities, racial groups, countries, or the current milieu. Moving forward, the inclusion of more diverse and contemporary samples will also be an important priority for research.
Conclusions and future directions
This study represents the largest and most comprehensive epidemiologic study and the only genetically informed study of the relation between gambling disorders and suicidal behaviors. The significant association of disordered gambling with suicidal thoughts appeared to be due primarily to common genetic factors (especially among women), and the association of disordered gambling with suicide attempt was potentially due to a causal relation (especially among men).
Great progress had been made in the past decade in elucidating the genetic overlap between different psychiatric disorders by interrogating the results of genome-wide association studies (GWASs; Harden & Koellinger, 2020). Note that the genotype–phenotype associations of interest (e.g., for gambling disorder and suicidal behavior) do not have to come from the same study. There have now been a handful of large-scale GWASs of suicidality (e.g., Erlangsen et al., 2020; Mullins et al., 2019); a top priority will be to conduct a large-scale GWAS of gambling disorder so that the genetic overlap with suicidal behaviors (and other disorders and traits) can be more thoroughly probed.
In previous research, we demonstrated using a discordant-twin design that there was a potentially causal relation between neighborhood disadvantage and disordered gambling (Slutske et al., 2019) and that genetic variation in the frequency of gambling was associated with exposure to neighborhood disadvantage (Slutske et al., 2015). Exposure to neighborhood disadvantage has also been associated with suicidal behaviors (Wardle et al., 2019). This emerging evidence suggests that disordered gambling and genetic risk for disordered gambling might shape the environment, for example, in the quality of the neighborhood in which one lives and whether one has experienced homelessness and severe financial problems (Roberts et al., 2017; Wong et al., 2010), that might precipitate suicidal behaviors. It remains an important question for future genetically informed research to determine which aspects of the environment might be critical in explaining the potentially causal and noncausal links between gambling disorders and suicidal behaviors.
Implications for prevention and intervention
The results of this study are inconsistent with a causal influence of disordered gambling on thoughts about suicide or plans to commit suicide. Rather, there were noncausal associations between disordered gambling and suicidal thoughts and plans that were explained by common familial influences shared with major depression and conduct disorder. A potentially effective route for preventing disordered gambling and suicidal ideation and the escalation to suicide attempt may be via pharmacological or psychological treatments for depression (Abbott, 2020; Zalsman et al., 2016).
On the other hand, after removing the influence of shared genetic and environmental risk factors, there was evidence consistent with a potentially causal influence of disordered gambling on suicide attempt, especially among men. We speculated that this causal influence may be related to financial problems. There were several clues consistent with this—household income was inversely related, the percentage of household income spent on gambling was positively related to the severity of gambling problems, and the DSM-5 (APA, 2013) gambling disorder symptom of borrowing money to relieve a desperate financial situation (i.e., bail out) was the symptom most strongly associated with suicide attempt. These clues are buttressed by findings from studies of individuals who have sought treatment for their disordered gambling (Swanton & Gainsbury, 2020). For example, in a study of 202 callers to a state-funded gambling helpline, the best predictor of suicidal ideation or attempt was financial problems (Carr et al., 2018). A massive study using financial transaction data from the United Kingdom’s largest retail bank demonstrated that the percentage of financial transactions that were devoted to gambling were significantly associated with a wide range of adverse financial, lifestyle, and health outcomes, including mortality (Muggleton et al., 2021).
Most people struggling with gambling disorders do not seek treatment (Slutske, 2006). Financial problems are often the impetus when help is sought (Swanton & Gainsbury, 2020). Given the difficulties inherent in screening for a disorder that is relatively rare, coupled with the unwillingness of affected individuals to seek treatment, focusing on the monetary aspect of disordered gambling may represent a more practicable target for screening, intervention, and prevention. The use of monetary data to identify individuals experiencing financial harms associated with their gambling is exemplified by the UK study described above (Muggleton et al., 2021). The proliferation of online gambling activities (Gainsbury, 2015) simplifies the identification of individuals who have incurred substantial financial losses because of their gambling (e.g., Gray et al., 2012) and can also make it possible to follow up with a tailored intervention to modify gambling behavior to forestall a financial crisis (e.g., Wohl et al., 2017). This would not only reduce gambling-related financial crises but also might ward off a potential gambling-related suicide attempt.
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026211062599 – Supplemental material for An Epidemiologic, Longitudinal, and Discordant-Twin Study of the Association Between Gambling Disorder and Suicidal Behaviors
Supplemental material, sj-pdf-1-cpx-10.1177_21677026211062599 for An Epidemiologic, Longitudinal, and Discordant-Twin Study of the Association Between Gambling Disorder and Suicidal Behaviors by Wendy S. Slutske, Christal N. Davis, Michael T. Lynskey, Andrew C. Heath and Nicholas G. Martin in Clinical Psychological Science
Footnotes
Acknowledgements
We thank Dixie Statham, Bronwyn Morris, Megan Fergusson, and Richard Parker for coordinating the data collection for the twins and David Smyth, Olivia Zheng, Anthony Conciatore, and Harry Beeby for data management. We are grateful for the participation of the Australian Twin Registry twins.
Transparency
Action Editor: Kelly L. Klump
Editor: Kenneth J. Sher
Author Contributions
W. S. Slutske developed the study concept and the study design. Testing and data collection were performed by W. S. Slutske, A. C. Heath, M. T. Lynskey, and N. G. Martin. C. N. Davis and W. S. Slutske performed the data analysis and interpretation. W. S. Slutske and C. N. Davis drafted the manuscript, and A. C. Heath, M. T. Lynskey, and N. G. Martin provided critical revisions. All of the authors approved the final manuscript for submission.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.