
Abstract
Although Native (American Indian [AI] and Alaska Native [AN]) populations have high rates of abstinence from alcohol, health problems associated with substance use remain a pressing concern in many AI/AN communities. As part of a longstanding community-based participatory research project involving 5 years of relationship building and three preliminary studies, our team of academic and community coresearchers developed a culturally grounded intervention to facilitate recovery from substance use disorders among tribal members from a rural AI reservation. Our Indigenous Recovery Planning (IRP) intervention consists of six weekly sessions and is designed to provide inroads to existing resources in the community, affirm and enhance Native identity, address culturally relevant risk factors, and build on strengths. Results from a feasibility pilot study (N = 15) suggest that IRP is feasible to implement and acceptable to the community. Although there was insufficient statistical power to conduct hypothesis testing, there were changes between pretest and posttest scores in the expected directions. Future directions and limitations of this research are discussed.
American Indian (AI) and Alaska Native (AN) peoples have high rates of current and lifetime abstinence from alcohol relative to other racial groups in the United States (Cunningham et al., 2016). However, the legacies of settler colonialism continue to negatively affect Native communities (Tuck & Yang, 2012), manifesting in greater rates of substance use disorders (SUDs) among AI/ANs who do use alcohol or drugs (Grant et al., 2015, 2016). Historical factors contributing to substance use among AI/ANs include the geographic, economic, political, social, and cultural impacts of forced removal from traditional lands and placement on reservations (Nutton & Fast, 2015; Warne & Frizzell, 2014); ongoing discrimination and racism (Brave Heart et al., 2016; Skewes & Blume, 2019; Whitesell et al., 2012); and the effects of historical trauma (Brave Heart, 2003; Brave Heart & DeBruyn, 1998; Gameon & Skewes, 2020, 2021). Despite high rates of alcohol abstinence, health problems associated with substance use remain a pressing public health concern in many Native communities.
Factors that help account for disproportionately high rates of SUD among AI/ANs include inequities in the social determinants of health, such as greater poverty and unemployment, lower attainment of formal education, greater exposure to trauma, limited access to health care, and underfunding of health care services (Brave Heart et al., 2016; Castor et al., 2006; Davis et al., 2016; Vaeth et al., 2017; Whitesell et al., 2012). All of these factors can be linked to colonization. For example, the U.S. government’s efforts to eradicate Native cultures through forced removal of children from their families and placement in residential schools exposed AI/AN children to physical and sexual abuse and disrupted protective factors such as family bonds, traditional parenting practices, and spirituality (Brave Heart & DeBruyn, 1998; Lajimodiere, 2014; Zephier Olson & Dombrowski, 2020). Research has shown that residential school survivors and their descendants experience greater mental health problems, including addiction (Evans-Campbell et al., 2012; Hahmann et al., 2022; Zephier Olson & Dombrowski, 2020). In addition, centuries of governmental policies aimed at removing AI/AN peoples from their traditional lands have contributed to both historical trauma and persistent socioeconomic inequities affecting Native communities (Bombay et al., 2014; Davis et al., 2016; Keating, 2020; Warne & Frizzell, 2014). Although these factors are widely recognized as contributors to SUD and other health concerns, there are few culturally congruent, evidence-based SUD treatments designed or tested with AI/AN populations (Skewes et al., 2019, 2020; Venner et al., 2021).
Effective SUD treatments are critically needed for improving health equity in AI/AN communities (Etz et al., 2012). Although there are empirically supported behavioral and pharmacological treatments for SUD, AI/ANs have been vastly underrepresented in the clinical trials of these treatments (Greenfield & Venner, 2012). Insufficient opportunity to participate in clinical trials is compounded by distrust resulting from colonization and a history of research ethics violations in Native communities (Foulks, 1989; Skewes & Lewis, 2016). There also is evidence of strong resistance to the idea of evidence-based treatments developed by non-Native researchers for non-Native clients being used in AI/AN communities (Calabrese, 2008; Gone, 2007; Greenfield & Venner, 2012; Novins et al., 2011; Skewes & Lewis, 2016; Venner et al., 2016). Respect for culture and tribal sovereignty is perceived to be at odds with mandates to use evidence-based treatments, and aspects of some efficacious treatments are at odds with Native culture (Gone, 2007, 2008; Larios et al., 2011; Novins et al., 2011; Venner et al., 2016). With the greatest need for SUD treatment among all racial groups in the nation (Chartier & Caetano, 2010), AI/AN communities are calling for new approaches that center Native culture, traditions, knowledge, and values (Calabrese, 2008; Gone & Trimble, 2012; Novins et al., 2011; Skewes et al., 2019, 2021). To address the need for effective, culturally congruent SUD interventions, academic partners from Montana State University and community partners from a rural AI reservation have collaborated on a series of community-based participatory research (CBPR) studies since 2014.
Community-Based Participatory Research
CBPR is considered a best practice for research with AI/AN communities, and many tribes prefer or require CBPR for studies conducted with their people (Burhansstipanov et al., 2005; Malerba et al., 2018). The CBPR framework is a partnership approach to research that emphasizes equitable relationships between academic and community co-researchers; it involves community participation at every step in the research process, from study design and implementation to interpretation and dissemination of findings (Wallerstein & Duran, 2006). Researchers engaged in CBPR aim to develop trusting, long-term relationships with community members, study topics that matter to the community, and acknowledge that solutions to problems reside within the community. Tribal ownership of data and oversight of research dissemination are key components of CBPR with Native communities (Fisher & Ball, 2003). The goal of CBPR is to identify and build on existing strengths, empowering the community to effect change (Wallerstein & Duran, 2010). We used a CBPR framework throughout this project, including the pilot studies that informed the development of our intervention and the feasibility study discussed in this article. Our ongoing efficacy trial uses a CBPR framework as well.
Partnership to Address SUD in a Reservation Community
Our partnership came together in 2014 to discuss ways that research can help address SUD in a rural reservation community. Academic researchers were invited to visit the reservation to meet with stakeholders, including health care professionals, Tribal Council members, cultural leaders, and community members in recovery from SUD. After a series of initial visits, the academic partners were invited to participate in community events and attend local recovery support groups at the on-reservation SUD treatment center. Through these activities, we developed the groundwork for a trusting CBPR partnership. We then established a subaward to the local tribal college, hired a local project manager and community research associates, and recruited community leaders to serve on the project’s community advisory board (CAB). The CAB, which remains active today, included the director of the local SUD treatment center, cultural leaders, Elders, people in recovery from SUD, and family members affected by their relatives’ substance use. We focused on relationship building during monthly visits for 1 year prior to embarking on our first research study together. Through regular meetings (about six per year), the CAB collaborated on all of the preliminary studies described below.
Preliminary Study 1: Key Informant Interviews
After developing our CBPR partnership, our team collaboratively began our empirical work with a qualitative interview study designed to understand the needs, priorities, and preferences of the community with regard to SUD treatment (Skewes & Blume, 2019; Skewes et al., 2019). Through regular CAB meetings, we developed an interview protocol and assembled a list of potential key informants from the reservation. After receiving approval for the study from the Tribal Institutional Review Board (IRB), we recruited key informants and conducted the interviews (detailed methods and findings can be found in Skewes & Blume, 2019, and Skewes et al., 2019). This qualitative study helped the academic partners better understand the nature of substance use, addiction, and recovery on the reservation and also helped build trust with the community. Findings from the key informant interviews were presented to the community in an interactive findings gathering, where we organized a community feed, led a data-sharing presentation with opportunity for feedback, and recruited a spiritual leader to conduct a healing ceremony. This findings gathering was well attended, and many attendees provided valuable feedback, which we used to guide the next phase of the project.
Preliminary Study 2: Substance Use and Resilience Survey
After disseminating the findings from our key informant interview study, the academic partners, local research staff, and CAB held a series of meetings to discuss the findings and community feedback and outline the next steps for the project. Our partnership decided to proceed with a quantitative study to examine hypothesized risk and protective factors for SUD recovery identified in the key informant interviews. We collaboratively designed the study, which included developing the sampling strategy, selecting the measurement instruments, and designing the study procedure and dissemination plan. Approval for the study was then obtained from the Tribal IRB, which also approved all presentations and publications disseminating the findings. Our Substance Use and Resilience Survey was conducted with 198 adult tribal members who self-identified as having a current substance use problem (detailed methods and findings can be found in Skewes et al., 2020; Gameon & Skewes, 2021; and Gonzalez & Skewes, 2021). This study helped us establish rapport with the population we aim to serve, identify intervention needs and potential challenges and barriers to participation, and evaluate data collection procedures and measurement instruments. After disseminating the results to the community through research summaries written in plain language, our partnership again conducted a series of meetings to discuss future directions for this research. Ultimately, we decided that relapse prevention support was the most pressing need in this community.
Relapse Prevention
In our preliminary research, community members identified relapse as a key barrier to recovery from SUD (Skewes et al., 2019). Changing one’s substance use was seen as manageable in the short term or while away from the community, but long-term maintenance of behavior change was seen as exceedingly difficult when residing on the reservation. The availability of drugs and alcohol, social pressure to use substances, insufficient opportunities for treatment, and few occupational and recreational opportunities to keep busy were identified as barriers to recovery (Skewes et al., 2019, 2020). These barriers were compounded by stress due to poverty, discrimination, and frequent reminders of losses, both personal and historical. Considering these needs, we selected group-based relapse prevention, an established treatment with demonstrated efficacy for reducing substance use and associated consequences (Hendershot et al., 2011; Larimer et al., 1999; Marlatt & Donovan, 2007; Marlatt & George, 1984; Witkiewitz & Marlatt, 2004), as a promising candidate for cultural adaptation. This pragmatic and compassionate approach is congruent with Native cultural values and appealed to the community partners. However, relapse prevention has not been empirically evaluated for use with AI/ANs—a notable gap in the evidence base considering the existing health disparities—and does not account for cultural aspects of SUD recovery in any meaningful way. Therefore, we decided to culturally adapt relapse prevention before implementing it in this community.
The Need for Cultural Adaptation
Cultural adaptation is “the systematic modification of an evidence-based treatment . . . or intervention protocol to consider language, culture, and context in such a way that it is compatible with the client’s cultural patterns, meaning, and values,” while retaining the active ingredients of an intervention (Bernal et al., 2009, p. 362). Meta-analyses and systematic reviews have found that culturally adapted interventions are more effective than standard interventions and that interventions having the greatest effectiveness incorporated the most adaptations (Benish et al., 2011; Griner & Smith, 2006; Huey et al., 2014). With regard to SUD interventions, a recent meta-analysis suggests that cultural adaptation may help reduce substance use and associated consequences for people of color, although more high-quality clinical trials of culturally adapted SUD interventions are needed (Hai et al., 2021). Cultural adaptation is recommended whenever (a) the existing intervention would be unacceptable to the community, (b) adaptation would increase participation and retention, (c) adaptation would improve an intervention’s palatability or acceptability, or (d) cultural factors are known to affect the target behavior or concern (Burlew et al., 2013). These recommendations support the need for culturally adapted relapse prevention in tribal communities.
Preliminary Study 3: Focus Groups
As part of our cultural adaptation process, we conducted a third preliminary study to understand perspectives on relapse among different groups of stakeholders from the reservation. After collaboratively developing the study methods and securing Tribal IRB approval, we conducted a series of focus groups to discuss relapse, relapse prevention, and cultural adaptations that may be needed to improve the effectiveness of relapse prevention in this community. Separate focus groups were held with cultural leaders, SUD treatment providers, people with SUD, and affected family members (detailed methods and findings can be found in Skewes et al., 2021).
Participants identified many reasons for relapse, including culturally specific risk factors that are not included in current models of relapse or addressed in existing treatments. These included grief and loss reminders, historical trauma, racism and unfair treatment, and lateral oppression—locally defined as lack of social support, peer pressure to use substances, and undermining or sabotaging of recovery efforts by one’s social network (Skewes et al., 2021). Participants also noted cultural strengths that promote recovery that are absent from existing interventions, such as ethnic identity, spirituality, and communal mastery—defined as problem-solving through reliance on an interconnected social network (Fok et al., 2012). They emphasized the need for alternatives to the behavioral health services offered in the community, which can be difficult to access because of limited resources and long waiting lists. Following completion of the focus group study, we engaged in a series of meetings to review the standard relapse prevention content and discuss ways in which it might be improved through cultural adaptation.
From Relapse Prevention to Indigenous Recovery Planning
Considering findings from these preliminary studies, our partnership discussed ways to merge relapse prevention strategies (e.g., identifying triggers and planning for them, addressing the abstinence violation effect, learning new coping skills, reinstating sobriety quickly following a lapse; e.g., Larimer et al., 1999) with cultural lessons and activities to increase engagement and improve cultural fit for tribal members. We also aimed to address the locally relevant risk and protective factors that emerged from our preliminary data. Our approach to cultural adaptation was consistent with the formative method for adapting psychotherapy framework developed by Hwang (2009). This bottom-up, community-based approach involves five phases: (a) working with community stakeholders to generate knowledge and ideas; (b) merging community-derived knowledge with theory, clinical, and empirical knowledge; (c) reviewing initial intervention content with community stakeholders and making appropriate revisions; (d) testing the modified treatment in the community; and (e) finalizing the intervention (Hwang, 2009). We accomplished the first three phases through the preliminary studies and collaboration with the CAB described above, resulting in a culturally modified curriculum consisting of six manualized sessions. The adaptation goals were to (a) improve acceptability and desirability of the intervention, (b) enhance focus on strengths and address culturally specific relapse triggers, and (c) circumvent logistical barriers to participation and increase community capacity. See Table 1 for a summary of the adaptations made.
Cultural Adaptations Informed by Preliminary Studies
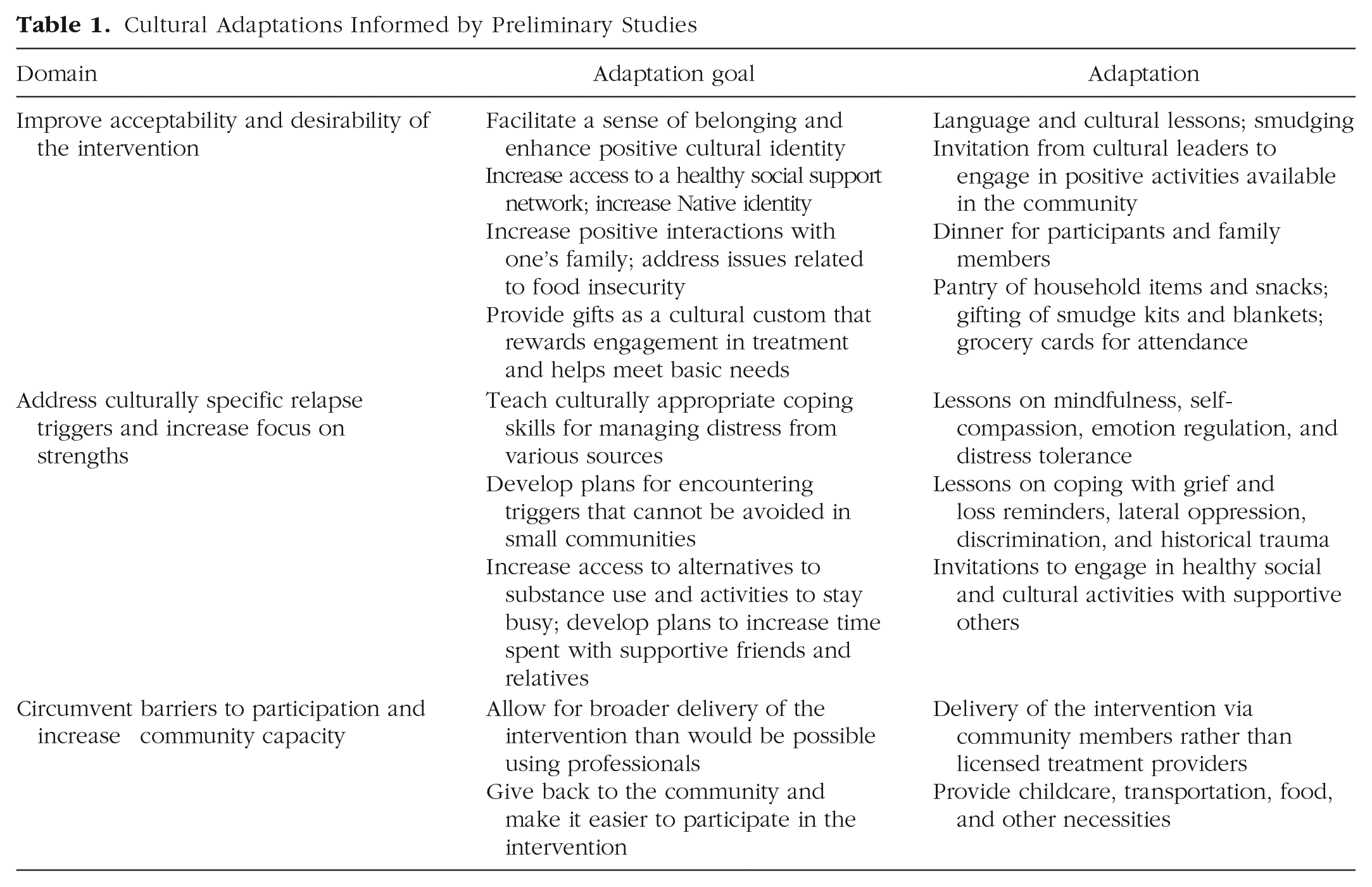
A key adaptation was to create a strengths-based intervention by shifting the focus from preventing relapse to planning for recovery. Community members preferred to focus on taking steps toward achieving a healthy, balanced future as opposed to focusing on relapse. This simple but important adaptation helped garner enthusiasm for the intervention among the community partners. We also aimed to improve the effectiveness of the intervention by training community members to deliver Indigenous Recovery Planning (IRP). Community-based facilitators bring special cultural and local ecological knowledge to the intervention, are well-equipped to respond to participant needs, and have a unique understanding of the challenges participants face, as well as their strengths (O’Keefe et al., 2021). As community members first, the IRP facilitators are able to connect with participants and explain the intervention goals and strategies in accessible ways. As a secondary benefit, community-based facilitators increase the sustainability of the intervention by circumventing the need for licensed professionals to deliver it.
We incorporated cultural lessons, stories, and locally relevant metaphors and examples into IRP to increase social validity (Lau, 2006) and to enhance and affirm Native cultural identity. For example, IRP includes language lessons, stories from community and cultural leaders, ceremonial smudging with sage, and invitations for participants to engage in healthy sober activities available on the reservation. Although the specific cultural lessons, metaphors, stories, ceremonies, language lessons, and invitations may be unique to this community, these elements are common to many reservations and may be tailored by other tribal communities to meet their needs, enhancing the transferability of IRP to other locations.
Additional adaptations were made to address culturally specific relapse triggers identified through our preliminary studies. For example, we added emphasis on staying busy, coping with grief and reminders of personal and historical losses, coping with discrimination and unfair treatment, navigating lateral oppression, increasing social support, and learning to forgive oneself and others to release anger and shame. Although these components emerged from preliminary studies with this particular community, they are relevant to other tribal communities as well (i.e., all AI/AN tribes have experienced events leading to historical trauma, and addressing historical trauma is likely important for SUD recovery across Native cultural groups). Adaptations were also made to circumvent logistical barriers to treatment, such as providing food, transportation, and childcare services at intervention sessions. These adaptations may improve treatment adherence and retention among any population of people with SUD.
IRP Procedure and Content
IRP was designed to be delivered in a group format. Six weekly sessions take place at the reservation’s tribal college, with transportation provided if needed. Family members are vital to tribal members’ recovery efforts, and participants are encouraged to invite their relatives to support their efforts to change. Before each IRP session, participants, their families, and the facilitators share an evening meal. Families are seated together and served dinner while engaging in an activity intended to build family cohesion. Following dinner, children remain in the large meeting room to be supervised by childcare providers, while participants move to a nearby classroom for the intervention session. Adult relatives have the option to stay with the children or to leave after dinner. The IRP facilitators open the session with a check-in, inquire about any issues that have arisen since the previous session, and then introduce the week’s guest speaker.
Guest speakers are cultural and community leaders who provide culture and language lessons and invite participants to engage in healthy activities available in the community. These activities may include, for example, attending a cultural event or traditional ceremony, signing up for classes at the tribal college, or attending a recovery support group at the local SUD treatment center. To increase participation in these activities, the guest speakers not only extend invitations but also explain what the activity will be like and what will be involved in attending. Further, the guest speakers share their contact information with participants and offer to meet them at these activities and help them overcome any logistical barriers. The goal is to make it as welcoming and comfortable as possible for participants to try something new that helps them stay busy and introduces them to new skills and social supports, and to provide opportunities to reintegrate with the community.
After the guest speaker leaves, the group then focuses on the IRP content areas, with exercises and discussions led by the community member facilitators. Focus areas for each of the six sessions are as follows. The first session covers psychoeducation about addiction and recovery, building motivation to change, and eliciting social support for change. The second session involves identifying triggers and high-risk situations that led to substance use in the past, identifying coping strategies and creating a recovery plan for times when triggers are likely to be encountered, discussing harm reduction strategies to stay safe in case of lapses, and planning to reinstate recovery as soon as possible following a lapse. In the third session, the group discusses managing cravings through mindfulness and distress tolerance skills as well as practicing self-compassion and forgiveness. The focus of the fourth session is understanding personal and historical trauma, coping with grief and loss reminders, and learning stress management and problem-solving skills. The fifth session covers identifying social support needs and asking for help from relatives; learning to cope with discrimination, lateral oppression, and lack of support from important others; and identifying pleasurable activities and making a plan to schedule substance-free activities with supportive others. In the sixth and final session, the group discusses making a plan to carry recovery into the future by preparing for bumps in the road and asking for support; reorganizing one’s lifestyle to restore balance in body, mind, emotions, and spirit; envisioning a healthy future for oneself, one’s family, and the community; getting involved in the community as a way of helping others; and celebrating successes. See Table 2 for a summary of the IRP content.
Indigenous Recovery Planning Content Areas
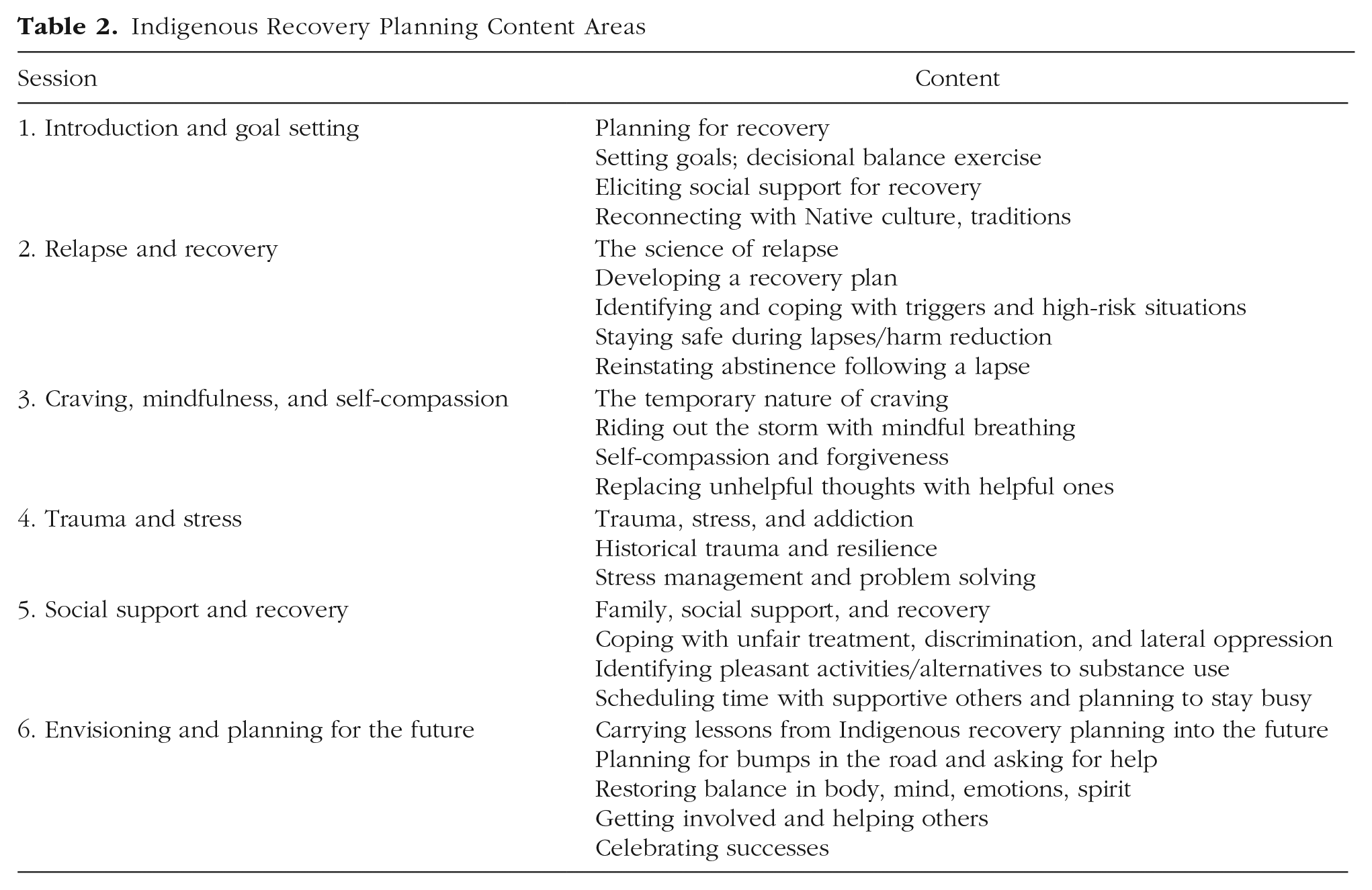
Group discussions and writing exercises take place at each session, and practice exercises are assigned between sessions. Importantly, participants are celebrated for each session they attend, regardless of whether they have experienced a lapse. The intervention is designed to reward participation and all efforts toward recovery. It also is intended to help address basic needs as a way to facilitate participation. For example, providing a meal is not only culturally congruent, but it also helps alleviate food insecurity and allows participants to focus on the intervention content. Participants also receive a $15 grocery card for each session they attend to help alleviate the stress of poverty, which may contribute to relapse. In addition, the IRP facilitators maintain a pantry of household goods such as personal hygiene items, canned goods, and prepackaged snacks at the tribal college where IRP takes place. At the end of each session, participants receive items from the pantry to help meet their needs. Participants also receive materials to smudge with sage, a traditional energy healing practice, and are taught how to smudge by cultural leaders. Finally, at the end of the sixth IRP session, each “graduate” is gifted a blanket, a cultural way of honoring someone, to celebrate their efforts at recovery. At this time, individuals who do not have a traditional Indian name and desire one are offered the opportunity to be named by a cultural leader who conducts the naming ceremony.
Current Study: Feasibility Pilot
After developing our CBPR partnership, conducting preliminary studies 1 to 3, and collaboratively developing the IRP curriculum, our team of academic and community researchers decided to proceed with a pilot feasibility study to identify issues to be addressed before planning a clinical trial and applying for external funding from the National Institutes of Health. Specifically, we were interested in gathering information about recruitment and retention, reactions to the IRP content and assessment instruments, and any procedures that may need adjustment. As in the previous preliminary studies, the CAB and research team discussed and collaboratively developed the research methods, including participant recruitment, assessment instruments, and study procedures. After designing the study, we obtained approval from the Tribal IRB to implement it. We also secured a Tribal Resolution—an act of law approving this research—from the reservation’s Tribal Council.
The IRP feasibility pilot study took place at the local tribal college with 15 adult tribal members desiring recovery from substance use problems. Participants completed self-report assessments before the first IRP session and after the last. Because IRP is focused on changing substance use, participants completed assessments of their alcohol and drug use as well as assessments of craving, readiness to change, and self-efficacy at pretest and posttest. To examine the potential effects of the intervention more holistically (Laudet, 2011), we also asked participants to complete measures of quality of life and psychological distress (i.e., anxiety and depression symptoms). In addition, our previous research identified potentially important factors that could impact treatment outcomes, including childhood adversity and historical trauma, as well as protective factors, such as social support for change, AI identity, spirituality, and self-compassion (Skewes et al., 2019, 2020, 2021). These factors also were assessed. All measurement instruments were reviewed and approved by the CAB and Tribal IRB.
Because of the small sample size and aims of this pilot feasibility study, we did not conduct hypothesis testing; however, descriptive statistics for pretest and posttest scores are shown in Table 3 along with accompanying effect sizes. Feedback on the intervention from facilitators is summarized below.
Summary of Feasibility Pilot Study Findings
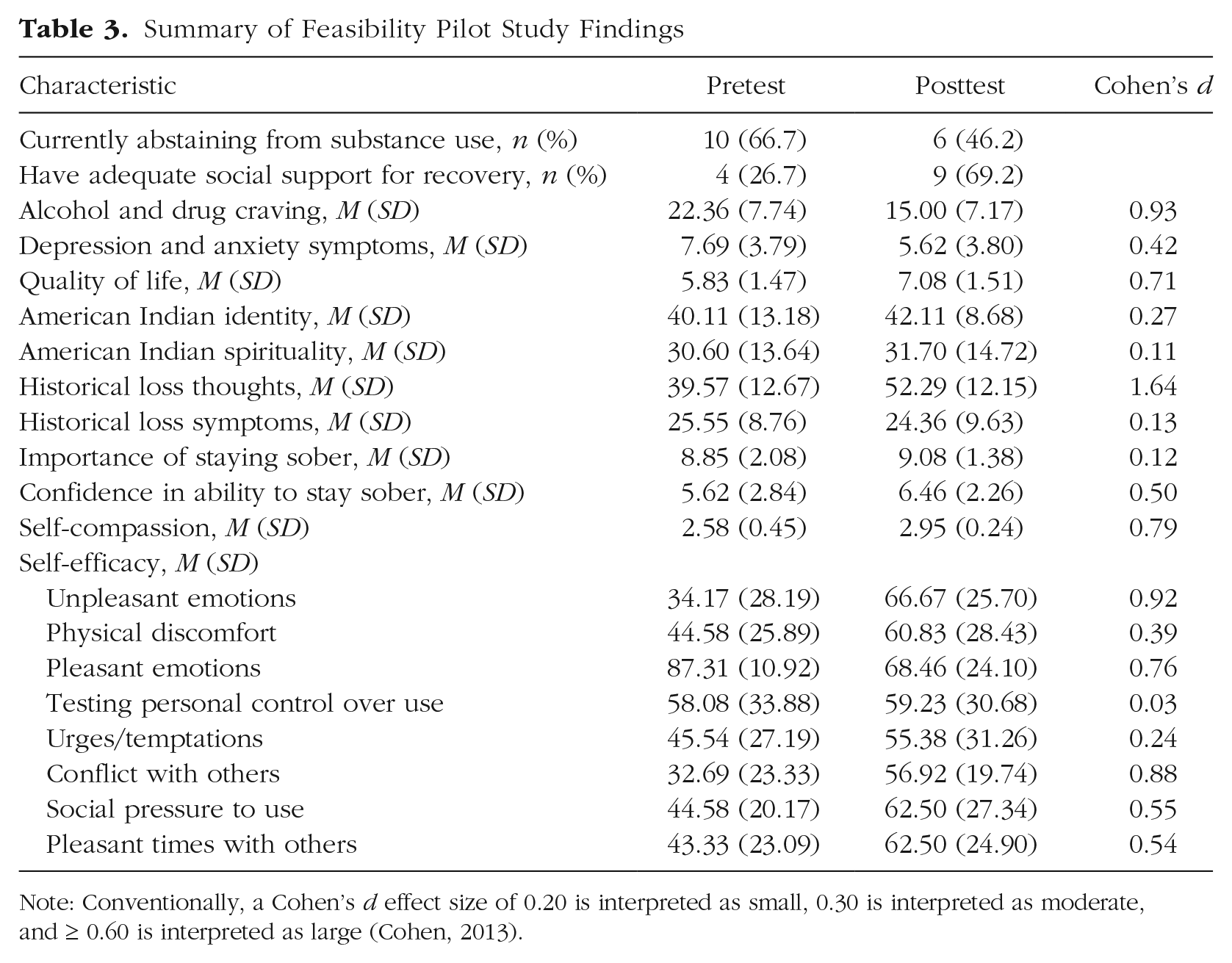
Note: Conventionally, a Cohen’s d effect size of 0.20 is interpreted as small, 0.30 is interpreted as moderate, and ≥ 0.60 is interpreted as large (Cohen, 2013).
Method
Facilitators and participants
Two AI women from the community served as facilitators in the feasibility study. The facilitators were CAB members who had been involved in the development of the intervention. One facilitator had an associate’s degree in nutrition, and the other had a master’s degree in public health. Both facilitators had extensive work and volunteer experience in the community, including serving as research assistants on other health-related projects. Because the facilitators had been closely involved with the development of the intervention, they had a deep understanding of the content and rationale for each IRP session. The facilitators participated in a day of training to review and discuss the IRP curriculum prior to beginning the feasibility pilot study.
Participants were 15 AI adults between the ages of 20 and 58 years old (M = 35.53, SD = 10.25) who identified as women (n = 9, 60%) and men (n = 6, 40%). Nine participants had completed high school, whereas six had not, and their median monthly income was $192. Alcohol and methamphetamine were the primary substances used. Six participants had previously received inpatient treatment for SUD (40%), five had completed the intensive outpatient program at the reservation’s treatment center (33.33%), nine had attended Alcoholics Anonymous meetings (60%), four had attended Narcotics Anonymous meetings (26.67%), and two had participated in a recovery-focused sweat lodge ceremony (13.33%). The mean number of adverse childhood experiences was 5.58 (out of 10 possible), with nine reporting an Adverse Childhood Experiences score of 4 or higher (60%). At pretest, only four (26.67%) reported that they had enough social support for recovery.
Measures
Background, substance use, and treatment history
Participants responded to open-ended questions about their age, gender, education, and monthly income. Participants also reported their primary substance of choice; whether they were abstaining from substance use at the time of the assessment, and if so, for how long; whether they felt they had adequate social support for recovery; and whether they had ever received inpatient or outpatient treatment, attended 12-step meetings, or participated in other recovery activities (i.e., recovery sweat lodge) in the past.
Childhood trauma
Childhood trauma was measured at pretest using the Adverse Childhood Experiences questionnaire (Felitti et al., 1998). This 10-item questionnaire assesses various forms of trauma (e.g., physical abuse, neglect, household dysfunction) experienced before age 18, with each item scored dichotomously (yes/no). Total Adverse Childhood Experiences scores were calculated by summing all “yes” responses; higher scores indicated greater childhood adversity. Scores of four or higher have been shown to predict greater physical and mental health problems in adulthood (Felitti et al., 1998). In this sample, the Adverse Childhood Experiences questionnaire demonstrated good internal consistency (α = .84).
Alcohol and drug craving
Craving was assessed at pretest and posttest using the five-item Penn Alcohol Craving Scale (Flannery et al., 1999), modified to refer to craving drugs or alcohol. Items assess the frequency, intensity, and duration of cravings; how difficult cravings were to resist; and a global rating of craving experienced in the previous week. Items are scored on a scale from 0 to 6, and responses are summed to yield a total score, with higher scores indicating greater craving. In the present sample, the Penn Alcohol Craving Scale demonstrated good internal consistency at pretest (α = .94) and at posttest (α = .95).
Anxiety and depression symptoms
The four-item Patient Health Questionnaire (Kroenke et al., 2009) was used to assess anxiety and depression symptoms experienced in the previous 2 weeks. Participants reported whether they had experienced each of four symptoms (e.g., feeling nervous, anxious, or on edge; having little interest or pleasure in doing things) on a 4-point scale from 0 (not at all) to 3 (nearly every day). Items were summed to yield a total score, with scores of 6 or greater suggesting clinically significant anxiety and depression symptoms. The Patient Health Questionnaire had good internal consistency in the present sample at pretest (α = .88) and at posttest (α = .87).
Quality of life
The 26-item brief World Health Organization Quality of Life assessment (The WHOQOL Group, 1998) was used to assess quality of life across four domains: physical health (e.g., “Do you have enough energy for everyday life?”), social relationships (e.g., “Do you get the kind of support from others that you need?”), environment (e.g., “How healthy is your physical environment?”), and psychological well-being (e.g., “How much do you enjoy life?”). Participants respond to each item on a scale from 1 to 5; response options differ depending on the question. Negatively phrased items are reverse scored, and then responses are summed to yield four subscale scores, which in turn are summed to yield a total quality of life score. Higher scores indicate greater quality of life. Internal consistency estimates in the present sample were good at pretest (α = .89) and adequate at posttest (α = .74).
AI identity and cultural connection
The 29-item Cultural Connectedness Scale (Snowshoe et al., 2015) was used to assess AI identity and connection with Native culture. This scale was developed through a community partnership with Canadian First Nations Elders to assess various aspects of cultural identity among Indigenous respondents. Sample items include “When I am in need of guidance, I look to my Native culture for help” and “I have a traditional person, Elder, or Clan mother who I can talk to.” The Cultural Connectedness Scale includes 11 dichotomous items (yes/no) and 18 items scored on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree). Item responses are summed to yield a total score, with higher scores indicating greater identification and affiliation with Native culture. In the present sample, the Cultural Connectedness Scale showed good internal consistency at pretest (α = .96) and at posttest (α = .94).
AI spirituality
Spirituality was assessed using the Native American Spirituality Scale (Greenfield et al., 2015). Participants are asked to respond to 12 items (e.g., “I believe everything is alive with a spirit,” “I wake up early and pray to Creator/ancestors”) on a 6-point scale from 0 (never or almost never) to 5 (every day). Item responses are summed to yield a total score, with higher scores indicating greater Native spirituality. In the present sample, the Native American Spirituality Scale demonstrated good internal consistency at pretest (α = .90) and at posttest (α = .92).
Historical trauma thoughts and symptoms
The 12-item Historical Loss Scale (Whitbeck et al., 2004) measures the frequency of thoughts related to experiences of traumatic historical losses experienced by AI/AN Peoples. Participants report how often they think about different historical losses (e.g., loss of culture, land, traditions, and community and family connections) on a scale from 1 (never) to 6 (several times a day). Responses are summed to yield a total score, with higher scores indicating greater historical trauma thoughts. In the present sample, the Historical Loss Scale had good internal consistency at pretest (α = .91) and at posttest (α = .97).
The 12-item Historical Loss Associated Symptoms Scale (Whitbeck et al., 2004) is a companion measure to the Historical Loss Scale that assesses distress associated with thinking about historical losses. Participants are asked to rate how often they experience various emotions (e.g., anger, depression, and fear) when thinking about the historical losses specified in the Historical Loss Scale on a scale from 1 (never) to 5 (always). Responses are summed to yield a total score, with higher scores indicating greater historical trauma symptoms. In the present sample, the Historical Loss Associated Symptoms Scale had good internal consistency at pretest (α = .89) and at posttest (α = .91).
Readiness to change
The two-item Readiness Ruler (Rollnick et al., 1992) was used to assess readiness to change. Participants are asked to rate the importance of changing their substance use and their confidence in their ability to do so on a scale from 0 (not at all important/confident) to 10 (extremely important/confident). Higher scores indicate greater importance or confidence.
Self-efficacy
Self-efficacy was assessed with the eight-item Brief Situational Confidence Questionnaire (Breslin et al., 2000), modified to refer to drinking or drug use. This questionnaire assesses confidence in one’s ability to avoid substance use across a variety of tempting situations (i.e., when experiencing unpleasant emotions, physical discomfort, pleasant emotions, desire to test personal control over substance use, urges and temptations, conflict with others, social pressure to use substances, or pleasant times with others). Participants are asked to indicate their current level of confidence in their ability to avoid substance use in each situation on a scale from 0% (not at all confident) to 100% (totally confident). Item scores are examined separately to identify situations in which participants are more or less confident in their ability to avoid substance use.
Self-compassion
The 12-item Self-Compassion Scale–Short Form (Raes et al., 2011) was used to assess self-compassion, or how participants treat themselves when faced with difficulty. Sample items include “When I’m going through a very hard time, I give myself the caring and tenderness I need,” and “When I fail at something that’s important to me, I tend to feel alone in my failure.” Response options range from 1 (almost never) to 5 (almost always). Following reverse scoring of negatively phrased items, responses are averaged to yield a total score, with higher scores indicating greater self-compassion. In the present sample, internal consistency for the Self-Compassion Scale-Short Form was questionable at pretest (α = .65) and at posttest (α = .64).
Procedure
A flyer advertising the study was disseminated through social media, with prospective participants instructed to contact the local project manager for more information and to determine eligibility for the study. Inclusion criteria included being a tribal member aged 18 or older, living on the reservation, self-identifying as having a substance use problem, and desiring treatment. Interested participants met with the project manager in a private location at the tribal college to discuss the study and provide informed consent, complete the pretest assessment, and receive the schedule for the IRP sessions. Following the last intervention session, participants completed the posttest assessments. Each assessment took approximately 1 hr, and each IRP session took approximately 2 hr, not including transportation or dinner. Participants received gift cards in the amount of $30 for the pretest assessment and $40 for the posttest assessment. They also received a resource list with contact information for mental health and SUD treatment agencies available on the reservation.
Results
Recruitment and retention
It took less than 1 week for reservation-based research team members to recruit 15 participants for the feasibility study. Of these participants, 13 remained in the study and completed both assessments (86.67%). Two participants withdrew from the study because of loss of housing and illness that precluded study completion.
Reactions to assessments
Participants responded well to the assessments, informally sharing that it was helpful to consider various aspects of their substance use behavior in a safe, private environment. Although there was a safety protocol in place in the event that a participant became distressed and needed care, the protocol was not used. No participants demonstrated distress during the assessments, nor did they report having difficulty with the questions asked.
Pretest and posttest scores
Given the aim of assessing feasibility, we did not conduct hypothesis testing, but we noted moderate to large increases between pretest and posttest scores in quality of life, confidence in one’s ability to change, self-compassion, and self-efficacy in many tempting situations, as well as a small increase in AI identity (see Table 3). At pretest, only four participants (26.7%) reported having adequate social support for recovery; at posttest, nine reported having adequate support (69.2%). This was encouraging, as increasing social support was an important goal of the intervention. There also were moderate to large decreases in anxiety and depression symptoms between assessments.
Regarding historical trauma, we noticed a large increase in thoughts about historical losses, which was expected given the IRP content on historical trauma, but not in historical loss symptoms (i.e., distress associated with thoughts about historical losses). Interestingly, self-efficacy scores increased in some domains (i.e., when experiencing unpleasant emotions, physical discomfort, urges/temptations, conflict with others, social pressure to use substances, and pleasant times with others), but self-efficacy when experiencing positive emotions decreased between pretest and posttest. The importance of changing substance use and AI spirituality appeared to be stable from pretest to posttest. Although fewer participants reported abstinence at posttest relative to pretest, there were moderate to large decreases in alcohol and drug cravings.
Facilitator feedback
The intervention was enthusiastically received by the community member facilitators. They especially valued the opportunity to share cultural lessons and to provide pantry items, meals, and gifts to participants. The facilitators selected and purchased items they knew community members needed, and they believed this to be important for the intervention’s success. Sharing food and gifts is a traditional cultural practice in this community, and people with SUD often miss the opportunity to be included in this practice. Facilitators viewed rewarding participants for efforts to change as a culturally grounded way to help them reconnect with Native traditions while simultaneously helping to meet participants’ basic needs. They also viewed the rewards as key to the desirability and acceptability of the intervention.
In addition, the facilitators valued spending time with participants while providing transportation, sharing that this time together involved further discussions of the IRP content and was therapeutic. They also reported that transportation and childcare were critical supports that enabled participation and increased the intervention’s desirability. Facilitators viewed IRP as a way to embrace, celebrate, and reward tribal members for taking a step toward recovery, which was seen as a novel approach in a community where treatment is often a punitive consequence for addiction-related legal trouble. They shared that focusing on positive reinforcement, nonjudgmental acceptance, and compassion was more aligned with their cultural values.
Regarding advice for conducting future iterations of the intervention, facilitators emphasized the crucial importance of a substantial food budget. Participants arrived hungry, and all food went quickly. At some sessions, the number of family members in attendance brought the head count to 50 or more. Food was a significant motivator to bring people to the intervention, as food insecurity is high in the community. Related to this, at first the facilitators had the guest speakers present during dinner so they could transition to the IRP content immediately following the meal. However, many participants were unable to pay attention during dinner. After the first session, the guest speakers met with participants after dinner was finished, and they were much better able to attend to the invitations. Of the pantry items available, food items were selected first, again indicating the extent of food insecurity. Facilitators viewed childcare as important for assuaging concerns about children’s safety, enabling participants to focus on the intervention. Finally, facilitators noticed that many participants appeared restless during the first IRP session and needed a way to occupy their hands. For the remaining sessions, the facilitators purchased fidget toys, clay, adult coloring books, and colored pencils to address this concern, and they reported that participants were better able to focus on the intervention with these supplies available.
The intervention also appeared to be well received by participants. Although we did not conduct a formal process evaluation, the facilitators reported having informal discussions with participants about their reactions to the intervention. According to facilitators, the cultural components of the intervention especially resonated with participants, as did the opportunity to discuss substance use in a nonjudgmental, supportive environment. Following completion of the intervention, facilitators reported that four participants enrolled in classes at the tribal college as a way to stay busy and focus their minds toward recovery. Furthermore, several participants have remained in touch with the facilitators since completing the intervention, suggesting that the IRP’s goal of expanding participants’ social networks was successful.
Discussion
Through a long-term CBPR partnership, our team of academic and community co-researchers developed a culturally adapted relapse prevention intervention to facilitate recovery from SUD among tribal members. Using data from a series of mixed-methods preliminary studies, we identified culturally specific risk and protective factors that study participants and community partners deemed important to address in SUD treatment. Our IRP intervention addresses these factors through a strengths-based group intervention that is grounded in Native culture, traditions, and values. We aimed to create an accessible, desirable, and sustainable intervention that circumvents barriers to treatment in this community. We then conducted a feasibility pilot study to gather information about recruitment and retention, reactions to the intervention content developed for the pilot study, and any procedures that may need adjustment before initiating a clinical trial.
The findings suggest that IRP is feasible to implement, acceptable, and desirable to the community. It took less than 1 week to recruit 15 participants by sharing a flyer on social media, and 13 (86.67%) of these participants completed the study. Although the sample size and study goals precluded hypothesis testing, several variables showed changes in the expected direction between pretest and posttest. For example, there were increases in social support for recovery, quality of life, AI identity, confidence in one’s ability to change, self-compassion, and self-efficacy in most tempting situations, as well as decreases in alcohol and drug craving and anxiety and depression symptoms between assessments. We were encouraged to see that the observed increase in historical trauma thoughts was not accompanied by increased historical trauma symptoms, suggesting that the resilience frame of Native peoples as survivors of historical trauma was successfully conveyed.
Although many changes in scores between pretest and posttest were encouraging, they also suggested a need for improvement in some content areas. For example, although self-efficacy scores increased in most types of tempting situations, there was a decrease in self-efficacy to avoid alcohol or drugs when experiencing positive emotions. This change may be related to decreases in depression and anxiety symptoms over the course of the pilot study and, potentially, to increases in positive emotions. The IRP lessons on coping with distress, cravings, and social pressure to use substances may need to be augmented with skills training to enable new ways of celebrating and experiencing positive emotions without using substances.
Notably, there was a decrease in the number of participants who reported abstinence from alcohol and drugs between pretest (n = 10) and posttest (n = 6). This may reflect the nature of SUD as a chronic health problem characterized by relapse (Connors et al., 1996; McLellan et al., 2000). Relapse prevention encourages participants to report lapses, which are framed as learning opportunities rather than signs of failure. It may be that participants were more forthcoming about their substance use at posttest relative to pretest, having experienced the nonjudgmental tone of the intervention and developed trust in the research team. Moreover, we do not know whether all participants had an abstinence goal, so abstinence may not have been an appropriate outcome to examine. Although some participants may have experienced a lapse, there also may have been positive changes in the quantity or frequency of use, which we did not examine. This finding indicates the need for a more comprehensive assessment of substance use as well as the inclusion of other outcome variables, such as substance use consequences and SUD severity, in future research.
The importance of community involvement in this research cannot be overstated. Community partners recommended using a strengths-based approach by framing the intervention as recovery planning rather than relapse prevention. They also suggested cultural lessons, stories, and practices that were incorporated into the intervention as a means of enhancing and affirming AI identity. They suggested that community and cultural leaders be invited to share opportunities to engage with positive activities available on the reservation to help participants reintegrate with the community and build a sense of belonging. They recommended that community members deliver the intervention to increase a sense of ownership and trust and suggested inviting participants’ families to pre-session meals as a way of increasing family cohesion and involving relatives in recovery efforts. Community partners shaped the sessions on culturally specific risk factors that tribal members often face (e.g., lateral oppression, historical trauma) and recommended strategies for coping with triggers that cannot be avoided in small reservation communities. Furthermore, they emphasized the importance and cultural relevance of providing food, pantry items, and gifts as a means of increasing recruitment and retention, enabling participants to focus on the IRP content, and reinforcing efforts to change. Rewarding tribal members for changing their substance use has empirical support, as contingency management has been shown to increase abstinence among AI people (McDonell et al., 2021). In addition, community partners emphasized food insecurity as a notable barrier to recovery and recommended budget increases for food and grocery cards to help address basic needs.
Limitations and future directions
Although we cannot determine whether the intervention caused the observed changes in scores from pretest to posttest, this pilot feasibility study helped us identify strengths and areas of improvement for future research. We believe that the cultural adaptations and procedures suggested by the community partners were successful at improving the acceptability, desirability, and sustainability of the intervention. Although the pretest–posttest design and sample size were appropriate for the goals of this study, future research is needed to determine whether IRP changes substance use among tribal members with SUD. Following modifications and enhancements to the IRP manual and study procedures informed by the present research, we will test the efficacy of the intervention in an adequately powered randomized controlled trial (RCT). We have secured funding for this research and are now preparing to launch the efficacy trial.
A key limitation of the present study is the assessment of abstinence at pretest and posttest using one dichotomously rated item. In the RCT, we will use the Timeline Follow back technique (Sobell & Sobell, 1992) to assess quantity and frequency of alcohol and drug use at each assessment, and measures of substance use consequences and SUD severity will be included as well. We will also assess participants’ treatment goals at baseline, engagement in other SUD treatments and mutual support groups at each assessment period, and reactions to the intervention content following each session. Working with the CAB, we have made revisions to the assessment battery to be used in the RCT, including replacing the measures of self-efficacy, spirituality, and AI identity with newer and/or simpler assessments of the same constructs. Also, there will be repeated posttest assessments in the efficacy trial, with follow-up assessments taking place immediately following the intervention, at 6 weeks after the intervention, and at 12 weeks after the intervention. This will allow us to examine whether treatment effects are maintained over time. The RCT also will include additional training for facilitators, detailed treatment fidelity assessments, and a formal process evaluation.
Another limitation of this feasibility pilot study pertains to our participant recruitment strategy. Recruitment took place solely through social media, which may have affected the sample characteristics. For the RCT, social media is but one of several planned recruitment strategies. We will also recruit participants from the waiting list at the reservation’s outpatient SUD treatment center, from wellness court, the tribal college, and the Indian Health Service clinic, and through newspaper and radio ads. Furthermore, the ease of recruiting 15 participants for this study may reflect greater motivation to change among these participants relative to that of participants in the larger RCT.
Finally, we acknowledge that future facilitators will require enhanced training relative to those in this feasibility pilot, who had been closely involved in the development of the intervention and had an in-depth understanding of the curriculum. We are in the process of developing a standardized facilitator training curriculum that will involve enhanced training as well as an opportunity to practice through serving as a co-facilitator prior to leading sessions independently. While the facilitators in the RCT all have experience in social work, substance use treatment, and/or mental health services, our team is engaging in ongoing discussions about the educational and background requirements for facilitators who may come on board in the future. We are working to develop a set of criteria that considers experience in the community, particularly with individuals with substance use problems, as well as educational background when selecting new facilitators to deliver the intervention.
It is important to note that the results of this feasibility study may not generalize to other AI/AN communities. There are 574 federally recognized AI/AN tribes in the United States (USA.gov, 2022), representing distinct cultural groups with different languages, cultures, and histories. As noted previously, the preliminary studies, cultural adaptation, and resulting intervention described in this article were designed by, with, and for this particular AI reservation. It is unknown whether other Native communities would desire IRP or whether it would be feasible to implement in other settings. However, many core components of IRP, if adapted, may be transferable to other communities. Although each tribe has a unique history and culture, there are commonalities among many AI/AN cultural groups, including the history of colonization that gave rise to historical trauma and disproportionately high rates of SUD (Nutton & Fast, 2015; Pride et al., 2021; Spillane et al., 2022), inadequate funding of the Indian Health Service (Joseph et al., 2019; Whitesell et al., 2012), and a preference for culturally grounded interventions (Walters et al., 2020; Wendt et al., 2022). Many Native cultures share common values regarding the importance of family, language, spirituality, and cultural identity (Dickerson et al., 2020; Walters et al., 2020) and may find elements of IRP to be well-suited to their communities. Although the specific cultural lessons, languages, and ceremonies may require tailoring for each community, these elements may be desirable to other AI/AN communities and are easily customizable. The elements of IRP designed to reduce barriers to treatment in rural areas with low resources (e.g., using trained community member facilitators and providing transportation, childcare, and meals) may also be transferable to other underserved communities. After the RCT is complete, we intend to create a template for tailoring the IRP materials for use in other communities and will work with other reservations interested in customizing IRP to meet their needs.
Although IRP may require tailoring before being used in other communities, our CBPR process and approach to cultural adaptation are transportable. Working in partnership to achieve the goals of the overarching project, we have created a desirable, culturally grounded, and potentially effective intervention that addresses the needs of this reservation. The process of working together on a series of preliminary studies has resulted in an intervention that none of us could have imagined at the onset of our work together and, we contend, is a best practice for intervention development in any minoritized community. Throughout our preliminary research, we not only gained a deeper understanding of the community and the topic at hand but also strengthened our relationships with one another and built trust with community members that has been crucial for the success of our research. This project represents a true partnership, with important contributions made by all partners, and has resulted in multifaceted benefits to the community—including financial benefits and employment opportunities associated with a large grant to test the intervention’s efficacy. Furthermore, our CBPR approach has enhanced the transparency and trustworthiness of our research findings through vetting by the CAB, Tribal IRB, and Tribal Council.
Conclusion
In many Native communities, SUDs are an important health concern and a priority area for research. As part of a longstanding CBPR project, our team of academic and community co-researchers has developed a culturally grounded intervention to facilitate recovery among tribal members from a rural AI reservation. Our IRP intervention is designed to provide inroads to existing resources in the community, affirm and enhance Native identity, address culturally relevant risk factors, and support participants in reconnecting with their families, community, and culture while learning evidence-based strategies to change their substance use. Results from a pilot feasibility study suggest that IRP is feasible to implement, acceptable, and desirable to the community. Next, our team will conduct an RCT to test the efficacy of the intervention and will disseminate IRP to other tribal communities to adapt according to their needs.
Footnotes
Acknowledgements
The authors express sincere gratitude to the Community Advisory Board for their guidance and feedback on this project and to the participants who generously shared their time and experiences. We also thank Arthur Blume, Dennis Donovan, and Joseph Gone for their guidance on earlier phases of the project described in this article. The findings of this study should be interpreted with consideration of the authors’ positionality. The authors include female descendants of European (M. C. Skewes, J. A. Gameon, and S. Holder) and Cuban (V. M. Gonzalez) immigrants, and American Indian male (M. Reum) and female (A. Ricker and S. Martell) community members.
Transparency
Action Editor: Patricia Lui
Editor: Jennifer L. Tackett
Author Contributions