
Abstract
We used Swedish national-register data (N = 2,828,777) to examine divorce and its associated patterns of family genetic-risk scores (FGRSs; personalized measures of genetic risk inferred from diagnoses in relatives) across 10 psychiatric disorders: major depression, anxiety disorders, obsessive compulsive disorder, bipolar disorder, schizophrenia, anorexia nervosa, alcohol use disorder, drug use disorder, attention-deficit/hyperactive disorder, and autism spectrum disorder. Individuals who divorced had elevated FGRSs across all disorders compared with individuals who were stably married or never married. FGRSs for all disorders were higher among divorced females compared with divorced males and among individuals who did not go on to have a stable second marriage compared with individuals who had a stable second marriage and increased as the cumulative number of divorces increased. In summary, genetic predispositions for psychiatric disorders are associated with the propensity to divorce and with several differences as a function of sex, remarriage, and the cumulative number of divorce transitions.
Divorce is common worldwide, and the divorce rate today is higher than it was in the 1970s in many countries (Organisation for Economic Co-operation and Development, 2021). Although the social acceptance of divorce is increasing (Treas et al., 2014), marital status continues to be a powerful sociodemographic correlate of a range of psychiatric morbidities (Metsa-Simola et al., 2018; WHO International Consortium in Psychiatric Epidemiology, 2000), including internalizing disorders (e.g., major depression [MD], anxiety disorders [ADs], and obsessive compulsive disorder [OCD]; Bromet et al., 2011; Kessler et al., 1998; Mojtabai et al., 2017), alcohol use disorder [AUD] and drug use disorder (DUD; Kessler et al., 1998; Mojtabai et al., 2017; Salvatore et al., 2017), neurodevelopmental disorders such as attention-deficit/hyperactivity disorder (ADHD; de Zwaan et al., 2012), psychotic disorders (e.g., bipolar disorders [BDs] and schizophrenia [SZ]; Agerbo et al., 2004; Mojtabai et al., 2017; Suppes et al., 2001), and eating disorders (e.g., bulimia and anorexia nervosa [ANO]; Andreeva et al., 2019).
Efforts to understand the nature of the associations between divorce and psychiatric disorders have largely focused on examining whether these disorders are likely to cause divorce or vice versa (South, 2021; Whisman et al., 2021). These studies have found some evidence that the onset of several disorders (e.g., BD, MD, generalized anxiety disorder, and drug or alcohol abuse) are prospectively associated with the risk of experiencing divorce (Kessler et al., 1998; Mojtabai et al., 2017). Likewise, divorce is associated with the onset of several disorders, including DUDs and AUDs (Edwards et al., 2018; Kendler et al., 2017) and the mood disorder dysthymia (Overbeek et al., 2006). As a set, the results emerging from this body of work suggest that the impairments associated with psychiatric disorders undermine key interpersonal processes that contribute to marital stability. Likewise, the stress associated with the process of divorce, which involves both interpersonal disruption and concomitant changes in living situation, child-rearing, and finances, can precipitate the onset of psychiatric disorders.
Another plausible explanation for these strong associations is that there is a set of confounding factors that contribute to both risk of divorce and risk of psychiatric morbidity (Whisman & South, 2017). Marital status and psychiatric disorders are multiply determined by social/cultural factors, interpersonal processes, and individual characteristics that may change across the life course. Genetic predispositions represent one key type of individual characteristic that contributes both to the likelihood of divorce (D’Onofrio et al., 2007; McGue & Lykken, 1992; Salvatore et al., 2018) and the propensity to develop a psychiatric disorder (Smoller et al., 2019). There is also evidence that the genetic propensity to develop several common psychiatric disorders overlaps with the genetic propensity to experience divorce and marital discord. For example, genetic factors account for more than 50% of the covariance between divorce and AUD (Salvatore et al., 2017) and for a substantial proportion of the covariance between marital quality and symptoms of internalizing disorders (South & Krueger, 2008; Spotts et al., 2004). Likewise, genetic factors account for approximately 40% of the covariance between divorce and a personality composite that includes traits implicated in a range of psychiatric and substance use disorders (e.g., low levels of constraint, high levels of negative emotionality; Jockin et al., 1996). Such findings underscore the complex nature of the associations between divorce and psychiatric disorders and the need for a fuller understanding of how genetic factors may be related to marital dissolution (Sbarra, 2015).
In view of theory and evidence that individual differences can contribute to stress generation in a relationship and the couple’s ability to navigate those challenges (Karney & Bradbury, 1995; Santee et al., 2023), we would expect genetic predispositions for a range of psychiatric disorders to be elevated among individuals who divorce compared with individuals who are stably married. We also expected genetic predispositions for psychiatric disorders to be elevated among individuals who never marry compared with individuals stably married in view of prior epidemiological evidence (Breslau et al., 2011).
Alongside characterizing these associations at the population level is the need to understand potential differences as a function of factors such as gender, remarriage, the cumulative number of divorce transitions, and characteristics of the spouse. With respect to potential gender differences, the association between divorce and mortality is higher in men compared with women (Shor et al., 2012). To the extent that psychiatric disorders contribute to this gender difference at the phenotypic level, we would also expect genetic predispositions for psychiatric disorders to be higher among divorced men than divorced women. However, there is not robust evidence for sex/gender differences in the psychiatric predictors and consequences of divorce (Bloom & Caldwell, 1981; Gove, 1972; Strizzi et al., 2022), and accordingly, hypotheses about gender differences should be considered tentative. Remarriage following divorce is also quite common (Bramlett & Mosher, 2002), and some individuals whose first marriages end in divorce go on to have stable second marriages. To the extent that a stable second marriage reflects fewer individual vulnerabilities, we hypothesize that individuals who go on to have a stable second marriage (vs. individuals who do not) would have lower genetic predispositions for psychiatric disorders. Conversely, and consistent with the idea that individual vulnerabilities can undermine relationship stability, we would expect that individuals who divorce multiple times will have higher genetic predispositions for psychiatric disorders.
Finally, we sought to examine whether the profile of genetic predispositions for psychiatric disorders differed based on the spouse’s history of psychiatric disorders. Vaillant (2015) posited that dissolving a marriage to a spouse with a substance use disorder could be a marker of psychological health. Consistent with this perspective, we and others previously found that the risk of developing problem drinking or an AUD following divorce was lower among individuals who divorced a spouse with (vs. without) a drinking problem (Kendler et al., 2017; Smith et al., 2012). We thus hypothesized that individuals who divorced a spouse with an AUD or other substance use disorder would have lower genetic predispositions for psychiatric disorders compared with individuals who divorced an unaffected spouse. In view of the evidence that spousal internalizing disorders are associated with lower relationship satisfaction (Whisman et al., 2004), we also examined whether the same pattern was observed for individuals who divorced a spouse with MD or an AD.
We used Swedish national data to examine patterns of family genetic-risk scores (FGRSs) across 10 mental- and behavioral-health conditions: MD, ADs, OCD, BD, SZ, ANO, AUD, DUD, ADHD, and autism spectrum disorder (ASD). FGRSs (Kendler et al., 2021b) are personalized measures of genetic risk for a disorder inferred from diagnoses (defined by codes from medical, legal, and pharmacy registries) in first- to fifth-degree relatives, weighted by degree of genetic relatedness and adjusted for cohabitation effects (i.e., shared environmental factors that contribute to familial resemblance). Thus, an individual from a densely affected family pedigree (e.g., multiple affected first-degree relatives) would have a higher FGRS compared with an individual from a sparsely affected pedigree (i.e., no or few affected distant relatives). A strength of the FGRS approach over other latent/inferred genetic approaches, such as twin-family studies, is the ability to capture genetic risk from extended pedigrees and the ability to calculate FGRSs for all individuals in a population. We examined the following questions:
Research Question 1: What is the pattern of FGRSs for our 10 disorders of interest among individuals divorced, individuals in stable marriages, and individuals never married?
Research Question 2: Do FGRS patterns differ between divorced males and females?
Research Question 3: Do FGRS patterns differ as the cumulative number of divorce transitions increases?
Research Question 4: Do FGRS patterns differ between individuals who divorced and had a stable second marriage and individuals who did not have a stable second marriage (divorced again or never remarried)?
Research Question 5: Do FGRS patterns differ between individuals who divorced a spouse who did not have a registration for any of the 10 disorders versus a spouse with a registration for (a) AUD/DUD or (b) MD/AD (in first divorces).
Transparency and Openness
Preregistration
This study was not preregistered; accordingly, results should be considered exploratory.
Data, materials, code, and online resources
Given the highly sensitive and confidential nature of the information as required by Swedish law, analyses by outside parties could take place in Sweden only under the supervision of J. Sundquist and/or K. Sundquist.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study (Simmons et al., 2011).
Ethical approval
The Regional Ethical Review Board of Lund (No. 2008/409 and later amendments/updates until 2018) approved this study.
Method
We collected information on individuals from Swedish population-based registers with national coverage linking each person’s unique personal identification number, which, for confidentiality, was replaced with a serial number by Statistics Sweden. Our database consisted of all individuals born in Sweden between 1950 and 1980 of parents themselves born in Sweden and followed through December 31, 2018. This cohort definition balances coverage of the relevant phenotypes in the registries, the mean ages at first marriage for men (36.4 years) and women (34.5 years; Statistics Sweden, 2023), and sufficient follow-up time for observing divorce, which was informed by prior evidence that relative risk for divorce peaks between the third and sixth years of marriage (Andersson, 1995; Kulu, 2014). The main cohort for these analyses included 2,828,777 individuals, with a mean age at end of follow-up of 51.7 years (SD = 11.2) and a range of 38 to 68 years.
In the database, we included date of registration for marriage(s) and divorce(s) and individual FGRSs for MD, AD, OCD, BD, SZ, AN, AUD, DUD, ADHD, and ASD. The FGRSs were based on selected first-, second-, third-, fourth-, and fifth-degree relatives to the probands; there was a mean of 40.1 relatives per proband. The logic of the FGRS approach is complementary to genome-wide polygenic-scoring approaches in which molecular genetic variants are weighted by their effect size from an external discovery sample to estimate one’s genetic risk for a disorder (Dudbridge, 2016; Wray et al., 2014). The key difference is that an FGRS is an inferred measure of genetic risk, estimated based on phenotypic information about the proband’s relatives, weighted by the degree of genetic similarity among different types of relatives (e.g., biological full siblings share 50% of their genetic variation identical by descent, whereas second cousins share 3.13%). FGRSs were based on lifetime diagnoses in relatives from medical, legal, and pharmacy registries; weighted by degree of genetic relatedness; and adjusted for age, sex, year of birth, area of residence, number of recorded relatives, and cohabitation effects. Support for the validity of this approach comes from studies showing that the patterns of FGRSs largely replicate previous findings about the genetic architecture of psychiatric disorders (Kendler et al., 2021b) and that FGRSs are associated with risk of disorder (Salvatore et al., 2023) and clinical features, such as age of onset, recurrence, and diagnostic transitions (Kendler et al., 2021a; Kendler, Ohlsson, Sundquist, & Sundquist, 2023). Furthermore, the results of a recent simulation study suggest that a modified version of FGRSs (i.e., the Pearson-Aitken FGRS; Dybdahl Krebs, Georgii Hellberg et al., 2023) and genome-wide polygenic scores index the same underlying genetic risk (Dybdahl Krebs, Appadurai et al., 2023). In addition, we included the date of first registration for each of the 10 phenotypes. For the full definitions of the FGRS and phenotypes, see the Supplemental Material available online.
For our first research question, we created a three-level variable: ever divorced, individuals in stable marriages (> 7 years with no divorce), and individuals never married (> 1 SD from sex-specific population average age at marriage). For our second research question, we examined FGRS patterns in divorced males and females separately. For our third research question, we created a three-level variable as a function of the cumulative number of divorces (one, two, three or more). For our fourth research question, we created a binary variable using individuals who divorced and had a stable second marriage and individuals who did not have a stable second marriage (defined as divorced again or never remarried). For our fifth research question, we created a three-level variable among individuals that were divorced: individuals who divorced a spouse who did not have a registration for any of the 10 disorders, individuals who divorced a spouse who had an AUD and/or a DUD registration, and individuals who divorced a spouse who had an MD and/or an AD registration. To reduce potential bias because of assortative mating, we limited these analyses to dyads in which neither partner was affected with AUD/DUD or MD/AD before marriage.
We first calculated the mean FGRS for individuals registered with each of the 10 disorders. Second, we calculated the ratio between the individual FGRS and the mean FGRS (e.g., individual FGRS for MD divided by the mean FGRS score for MD for individuals registered with MD). This ratio is what we present. We calculated the mean FGRS ratio for each of the 10 specific FGRSs among all the specific groups defined above. To test differences between groups, we used a t test and a corresponding 95% confidence interval. All analyses were done using SAS (Version 9.4).
Results
Characteristics of the study cohort are summarized in Table 1. In total, 592,232 individuals experienced divorce. The majority divorced once, but a sizable minority divorced twice or three or more times. The average length of first marriages that ended in divorce was 14.7 years (SD = 9.5). Among individuals who experienced divorce, the most common psychiatric disorders before divorce included MD (6.97%), AD (5.08%), AUD (4.71%), and DUD (1.70%). MD and AD were more prevalent among females who divorced, and AUD and DUD were more prevalent among males who divorced.
Descriptive Statistics for Study Sample
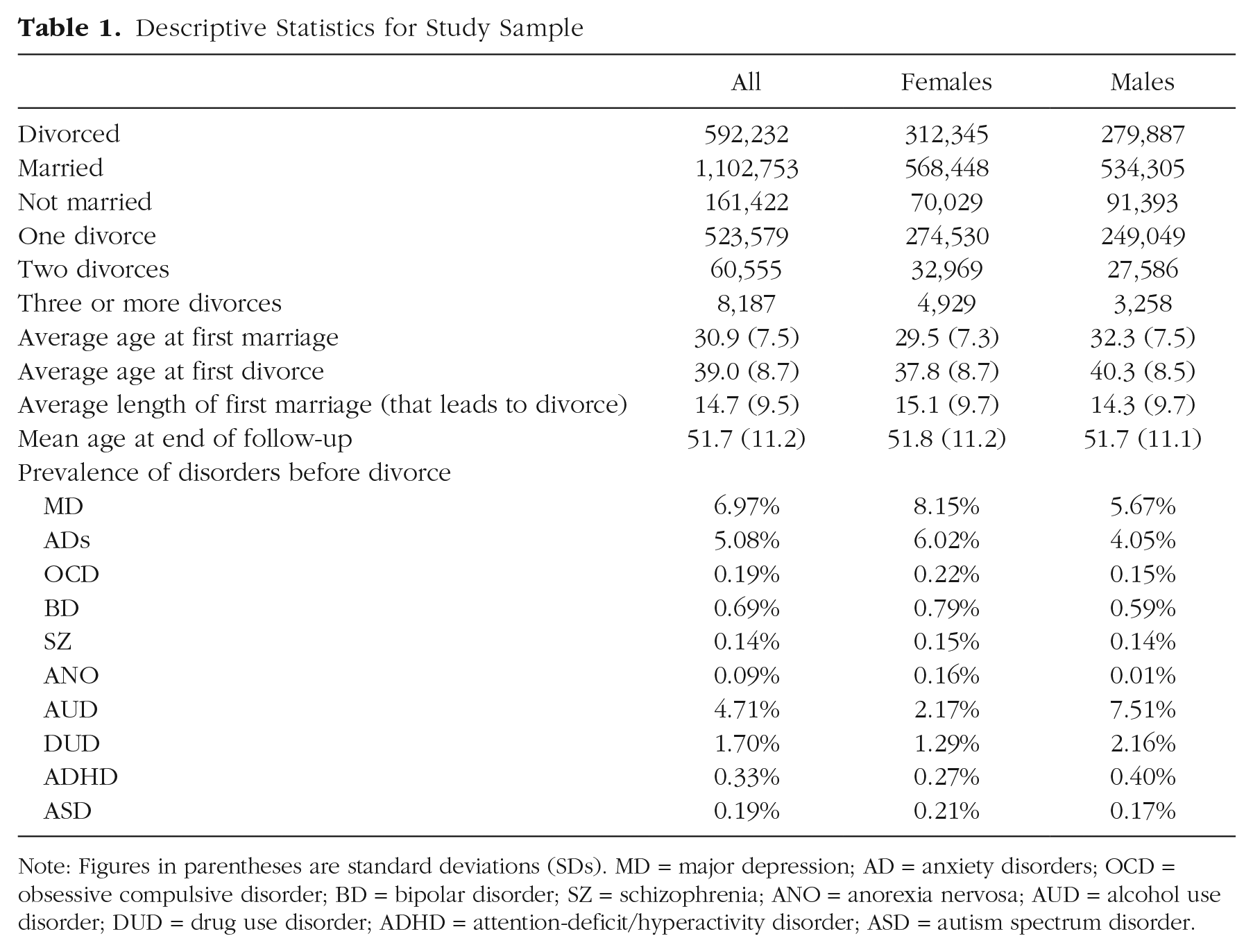
Note: Figures in parentheses are standard deviations (SDs). MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
Patterns of FGRSs among individuals divorced, individuals in stable marriages, and individuals never married are shown in Figures 1a through 1c. FGRSs are presented as a percentage relative to an affected proband, as previously reported in Kendler et al. (2021a, 2021b), in which a value of 100% represents an FGRS equal to the average affected individual and a value of 0% represents an FGRS equal to the average in the population. Negative values represent an FGRS lower than the average in the population. Several features merit comment. First, as shown in Figure 1a, individuals who experienced divorce had FGRSs higher than the respective population average for all disorders. Of particular note, individuals who experienced divorce had FGRSs for MD and AD that were nearly 45% that of MD- and AD-affected probands. Likewise, divorced individuals had FGRSs for AUD and DUD that were approximately 20% of the value of AUD- and DUD-affected probands. In contrast, individuals who were stably married (Fig. 1b) and never married (Fig. 1c) had FGRSs lower than the respective population average across all 10 disorders. The only exception to this was that in the stably married group, the FGRS for ANO did not differ from the population average. As shown in Figures S1a through S1c in the Supplemental Material, divorced individuals had significantly higher FGRSs across all disorders compared with individuals in stable marriages or never married. As shown in Figure S1b in the Supplemental Material, individuals in stable marriages had lower FGRSs across all disorders compared with individuals never married, with the exception that the FGRSs for OCD and ANO were higher among individuals in stable marriages.
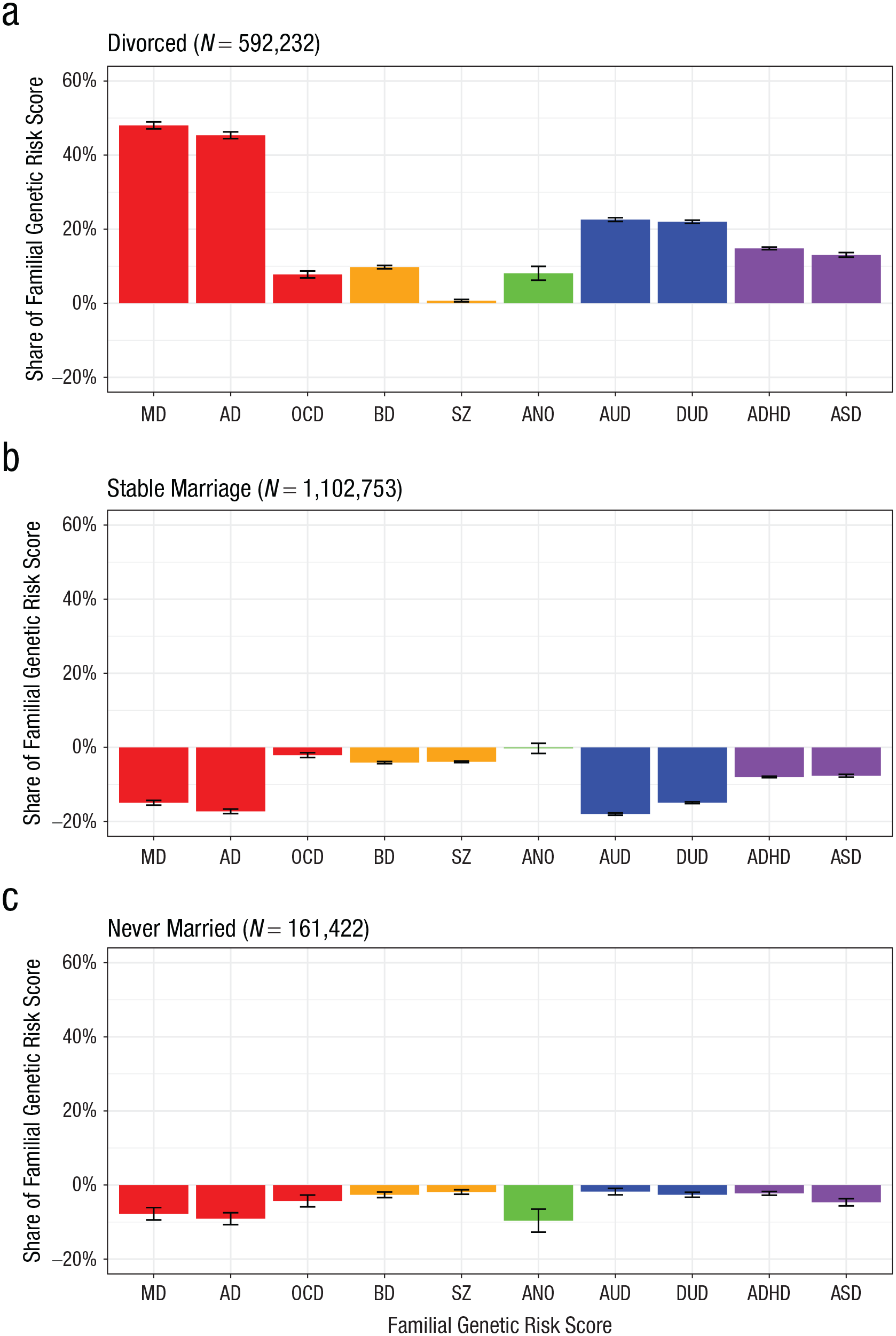
Family genetic-risk scores for 10 disorders among individuals who were (a) divorced, (b) in stable marriages, and (c) never married. MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
We then examined whether FGRS patterns differ between divorced females and divorced males. Patterns of FGRSs for females and males are shown in Figures 2a and 2b, respectively, and the differences between them are shown in Figure 2c. Consistent with what we observed in the total divorced population, FGRSs for the 10 disorders were elevated among both divorced females and divorced males. The exception to this pattern was that among divorced males, the FGRSs for SZ did not differ from the population average. Compared with divorced males, divorced females had significantly higher FGRSs such that divorced females had FGRSs that were closer to that of an affected proband than divorced males. This was observed for all disorders except ANO, for which there was no statistically significant difference between divorced males and females. The elevations in the FGRSs for MD and AD in divorced females compared with divorced males were particularly pronounced; AUD and DUD had more modest elevations.
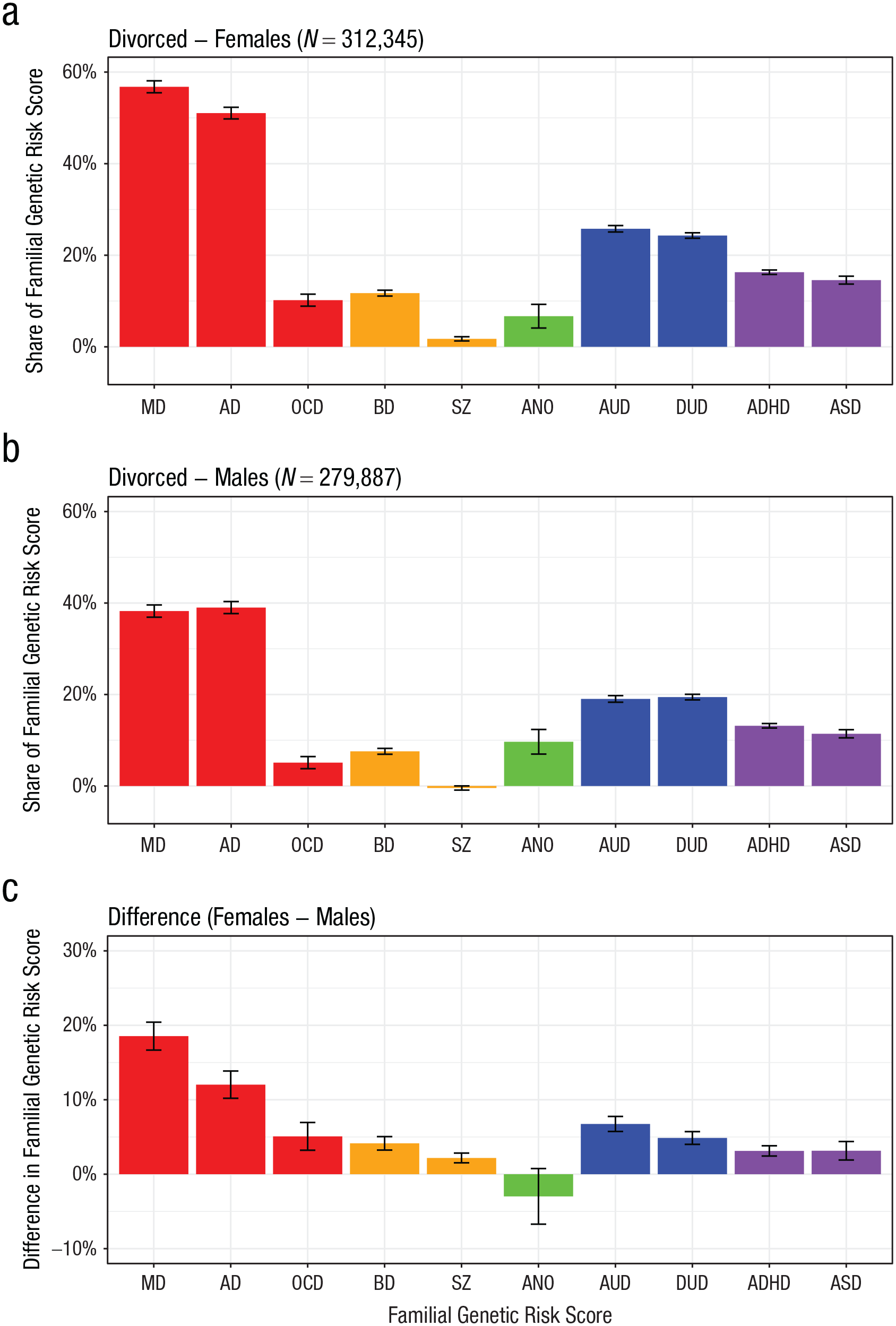
Family genetic-risk scores for 10 disorders among (a) divorced females and (b) divorced males and (c) differences between these two groups. MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
Next, we examined whether FGRS patterns differed as the cumulative number of divorce transitions increased. Patterns of FGRSs for one, two, and three or more divorces are shown in Figures 3a through 3c, respectively. The FGRS differences between individuals with two versus one divorce and three versus two divorces are shown in Supplemental Material Figures S2a and S2b, respectively. The FGRSs for most disorders increased as the number of divorce transitions increased and was especially pronounced for MD, AD, AUD, and DUD; ADHD and ASD had some elevation as well.
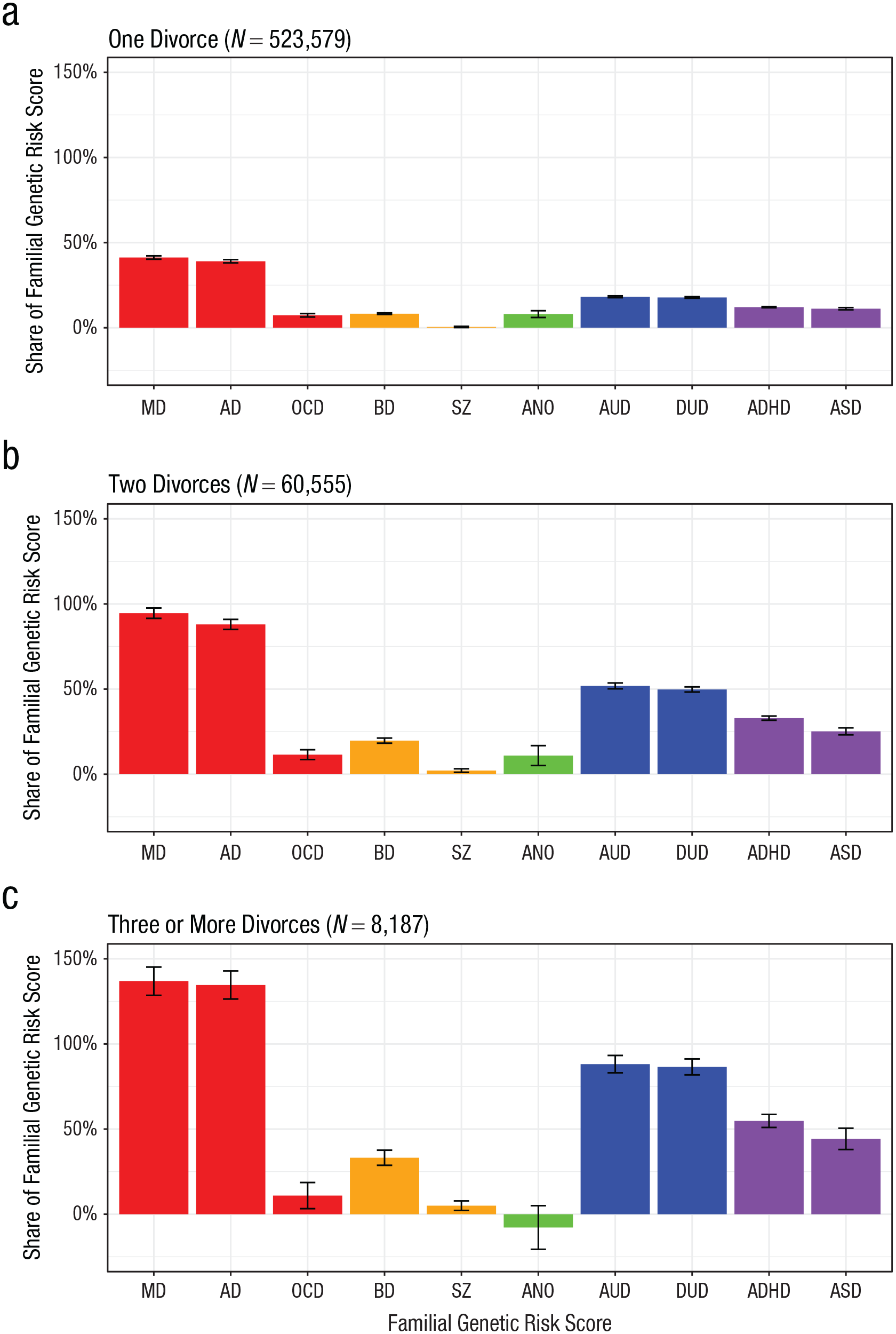
Patterns of family genetic-risk scores for 10 disorders across cumulative divorces. MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
Next, we examined whether FGRS patterns differed between individuals who divorced and had a stable second marriage and individuals who did not have a stable second marriage. Patterns of FGRSs for divorced individuals with and without stable second marriages are shown in Figures 4a and 4b, respectively. FGRSs for most disorders were elevated in both groups relative to the average FGRSs in the population. Individuals who went on to have a stable second marriage had FGRSs for MD and AD that were approximately 30% to 40% that of affected probands and FGRSs for AUD and DUD that were approximately 10% that of affected probands. As shown in Figure 4b, individuals who did not have a stable second marriage had FGRSs for MD and AD that were nearly 60% that of affected probands and FGRSs for AUD and DUD that were approximately 30% of affected probands. Differences in FGRSs between individuals with and without stable second marriages are shown in Figure 4c. Compared with individuals with stable second marriages, individuals without stable second marriages had higher FGRSs across all disorders except ANO, which did not significantly differ between the two groups. In particular, the FGRSs for MD, AD, AUD, and DUD were elevated among individuals without versus with a stable second marriage, corresponding to FGRSs equal to 15% to 22% that of affected probands.
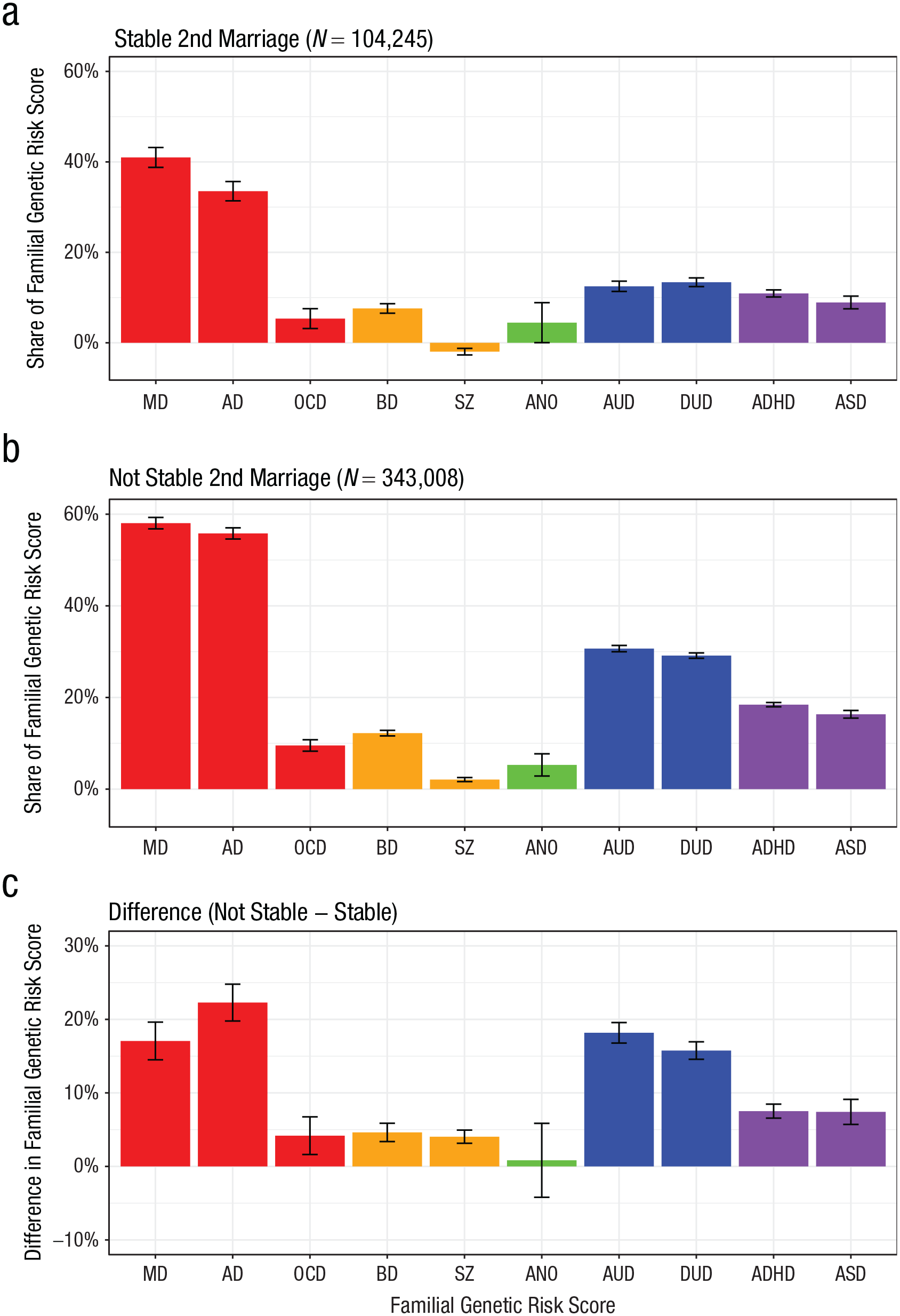
Family genetic-risk scores for 10 disorders among (a) divorced individuals who went on to have a stable second marriage and (b) divorced individuals who did not have a stable second marriage and (c) differences between these two groups. MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
Following this, we examined whether FGRS patterns differed between individuals who divorced a spouse who did not have a registration for any of the 10 disorders versus a spouse with a registration for AUD/DUD or MD/AD. Patterns of FGRSs for disorders among individuals who divorced a spouse with no registration for any of the 10 disorders, individuals who divorced a spouse with a registration for AUD and/or DUD, and individuals who divorced a spouse with a registration for MD and/or AD are shown in Figures 5a through 5c. Differences in FGRSs among individuals who divorced a spouse with versus without an AUD/DUD registration and in individuals who divorced a spouse with versus without an MD/AD registration are shown in Figures S3a and S3b, respectively, in the Supplemental Material. Individuals who divorced a spouse with an AUD/DUD registration had higher FGRSs across all disorders (except SZ and ANO) compared with individuals who divorced a spouse with no registration for any of the 10 disorders. Likewise, individuals who divorced a spouse with an MD/AD registration versus no registration for any of the 10 disorders had higher FGRSs across most disorders. There were three exceptions: FGRSs for AUD were lower among individuals who divorced a spouse with an MD/AD registration versus no registration for any of the 10 disorders. There was no statistically significant difference in FGRSs for SZ and DUD between individuals who divorced a spouse with an MD/AD registration versus no registration for any of the 10 disorders.
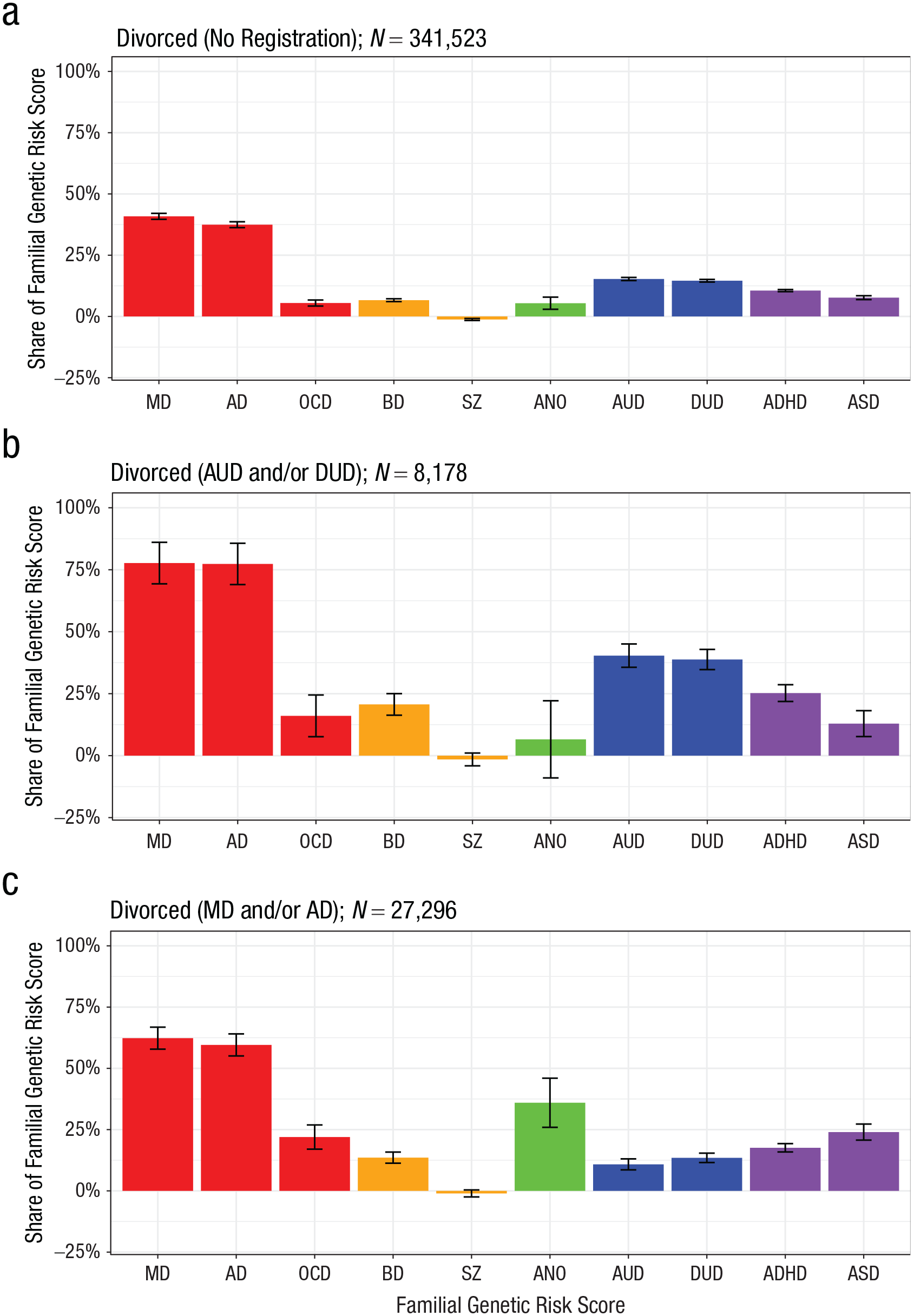
Family genetic-risk scores for 10 disorders among (a) individuals who divorced a spouse with no registration for any of the 10 disorders, (b) individuals who divorced a spouse with a registration for AUD and/or DUD, and (c) individuals who divorced a spouse with a registration for MD and/or AD. MD = major depression; AD = anxiety disorders; OCD = obsessive compulsive disorder; BD = bipolar disorder; SZ = schizophrenia; ANO = anorexia nervosa; AUD = alcohol use disorder; DUD = drug use disorder; ADHD = attention-deficit/hyperactivity disorder; ASD = autism spectrum disorder.
We also conducted a series of sensitivity analyses to evaluate the possibility that the pattern of FGRSs observed among divorced individuals was an artifact of including affected individuals in the analysis given that the rate of divorce is higher among individuals with (vs. without) a psychiatric disorder and that affected individuals are likely to have a higher disorder-specific FGRS. For this purpose, individuals with a registration for each of the 10 disorders were removed from the corresponding analysis (i.e., individuals with an MD registration before divorce were removed from the analysis of FGRSs for MD). As shown in Figures S4a and S4b in the Supplemental Material, even when affected individuals were removed from the like-kind analysis, the FGRS profile for divorce remained largely the same with only some attenuation in the effects. Likewise, as shown in Figures S5a through 5c in the Supplemental Material, the patterns of FGRSs among individuals who experienced one, two, and three or more divorces remained the same even when affected individuals were removed from the like-kind FGRS analysis. However, as shown in Figures S5d through S5f in the Supplemental Material, the reduction in the effects was more pronounced, particularly for the FGRSs for AUD, in individuals who experienced three or more divorces.
Discussion
We used national-registry data and examined the associations between divorce and genetic predispositions for a series of psychiatric disorders, as indexed using FGRSs. Three key findings emerged from our analysis. First, individuals who divorced had elevated FGRSs across all disorders compared with individuals who were stably married or never married, with particularly notable elevations for internalizing (MD, AD) and substance use (AUD, DUD) disorders. Never-married individuals also tended to have higher FGRSs than stably married individuals but lower than divorced individuals. These effects are consistent with the robust evidence that difficulty establishing harmonious and stable intimate relationships is a strong correlate of a range of psychiatric disorders (Whisman & Baucom, 2012; Whisman et al., 2021) and closely related heritable traits and behaviors such as neuroticism and impulsivity (Joel et al., 2020; Lavner et al., 2017; Tan et al., 2017; Tucker et al., 1998).
This pattern of effects maps onto prior evidence that these associations may be attributable, in part, to nonspecific genetic risk factors that contribute to both divorce and psychiatric disorders (Jockin et al., 1996; Salvatore et al., 2017; South & Krueger, 2008; Spotts et al., 2004). It is notable that the pattern of effects was robust when we removed affected individuals as part of sensitivity analyses. Thus, it does not appear that the presence of the disorder itself mediated the associations between FGRSs and divorce, although we acknowledge our registry-based definitions may not have identified more mild forms of these disorders. Likewise, we acknowledge that for AUD and DUD, even individuals with severe disorders may not be identified in the registries if they do not have police contact, a substance-related medical diagnosis, or symptoms that rise to a doctor’s attention. This suggests that a broad range of subclinical traits/behaviors associated with genetic predispositions for these disorders may be linked to marital outcomes. This interpretation is consistent with evidence that the genetic signal captured by FGRSs often crosses diagnostic boundaries (Kendler et al., 2021b) and theoretical perspectives and empirical evidence that boundaries between disorders are often arbitrary and that symptoms and maladaptive traits can be hierarchically organized into increasingly broad dimensions (Kotov et al., 2017, 2021).
Second, we observed several differences in FGRS profiles and divorce as a function of sex, remarriage, and the cumulative number of divorce transitions. Genetic predispositions for all disorders were higher among divorced females compared with divorce males, with particularly notable elevations for internalizing (MD, AD) and substance use (AUD, DUD) disorders. These sex differences suggest that the traits/behaviors and interpersonal stressors associated with genetic predispositions for these disorders (e.g., neuroticism and cognitive distortions that often characterize major depression and the high levels of impulsivity typically associated with substance use disorders) may be less well tolerated in wives than in husbands. Although others have posited that there are likely to be sex/gender-specific mental-health correlates of divorce (Sbarra & Whisman, 2021; Simon, 2002), the empirical evidence on this point is at present limited and mixed. For example, consistent with the pattern of effects found here, an integrative data analysis of four samples of divorcing couples found that women reported more psychological distress compared with men before separation (Bloom & Caldwell, 1981). Yet others have reported that rates of psychiatric disorders are elevated among divorced men compared with divorced women (Gove, 1972) or no gender differences in postdivorce adjustment (Strizzi et al., 2022). Our population-level data are uniquely well suited to overcome limitations from these prior studies (which included smaller and selected samples) and suggest that genetic predispositions for these major psychiatric disorders are higher among divorced females than divorced males.
There was also heterogeneity in FGRS profiles depending on whether individuals had a stable second marriage. As noted by others, the correlates of remarriage and stability of second marriages are not well known (Jensen & Sanner, 2021; Raley & Sweeney, 2020). The pattern of findings suggests that divorced individuals who go on to have a stable second marriage have lower genetic predispositions for nearly all of the major psychiatric disorders examined here, with the exception of ANO. The reductions in FGRSs for internalizing (MD, AD) and substance use (AUD, DUD) disorders among individuals with stable second marriages versus individuals without were particularly notable. Thus, even within a population of divorced individuals, genetic predispositions for psychiatric disorders are associated with the ability to form and maintain a second marriage. Genetic predispositions for most disorders also increased as the cumulative number of divorces increased. Individuals with two divorces had FGRSs for MD and AD that were as high as affected probands, and individuals with three divorces had FGRSs for MD, AD, AUD, and DUD that were as nearly as high (or higher) than affected probands. Although third and higher-order divorces are relatively uncommon (Brody et al., 1988), our findings here mirror earlier evidence that multiple marriages and divorces are associated with antisocial personality traits (McCranie & Kahan, 1986) and are more common among individuals with more severe psychiatric disturbance (Bloom et al., 1978).
Third, we found that individuals who divorced a spouse with MD/AD or AUD/DUD tended to have higher FGRSs across the 10 psychiatric disorders compared with individuals who divorced a spouse without a registration for any of the disorders. This pattern of effects ran counter to our hypothesis, inspired by Vaillant’s (2015) work on the natural history of physical and emotional well-being in men, that ending a marriage to a spouse with one of these common psychiatric disorders might not reflect liability to psychiatric illness. When bringing a genetic perspective to this question in a population-based sample, we instead found the opposite, whereby individuals who divorced a spouse affected by one of these common disorders during marriage had a profile of elevated genetic risk.
As with any genetic-epidemiological study, associations between FGRSs and marital status do not necessarily imply a causal effect, and complementary study designs are needed to understand the mechanisms underlying the patterns observed here. As illustrated in Figure 6, there are several possible pathways linking genetic predispositions and divorce. An FGRS may have pleiotropic effects on both disorder and divorce (Fig. 6a). Alternatively, active disorder or the subclinical traits/behaviors associated with a disorder may mediate the influence of genetic predispositions on divorce (Fig. 6b). Evocative genetic effects are also possible such that high-FGRS individuals may evoke unconstructive behaviors in their spouses that contribute to divorce (Fig. 6c). Social-relations modeling (Kenny et al., 2006; Rasbash et al., 2011), which can help disentangle active and evocative effects, could be used to test these possibilities. In view of evidence that spouses resemble one another in their psychiatric histories (Galbaud du Fort et al., 1998), it is also plausible that high-FGRS individuals may pair with partners who also have a high FGRS (i.e., assortative mating) and whose symptoms may increase risk of divorce (Fig. 6d). More broadly, the pattern of effects could be explained by active gene-environment correlation such that high-FGRS individuals seek out environments in which divorce is more common or socially acceptable. This would be consistent with evidence that predispositions for many traits and behaviors are geographically clustered (Abdellaoui et al., 2022) and urban–rural differences in risk of divorce (Zahl-Olsen, 2022). Tracing the pathways from these predispositions to divorce remains an important direction for future research.
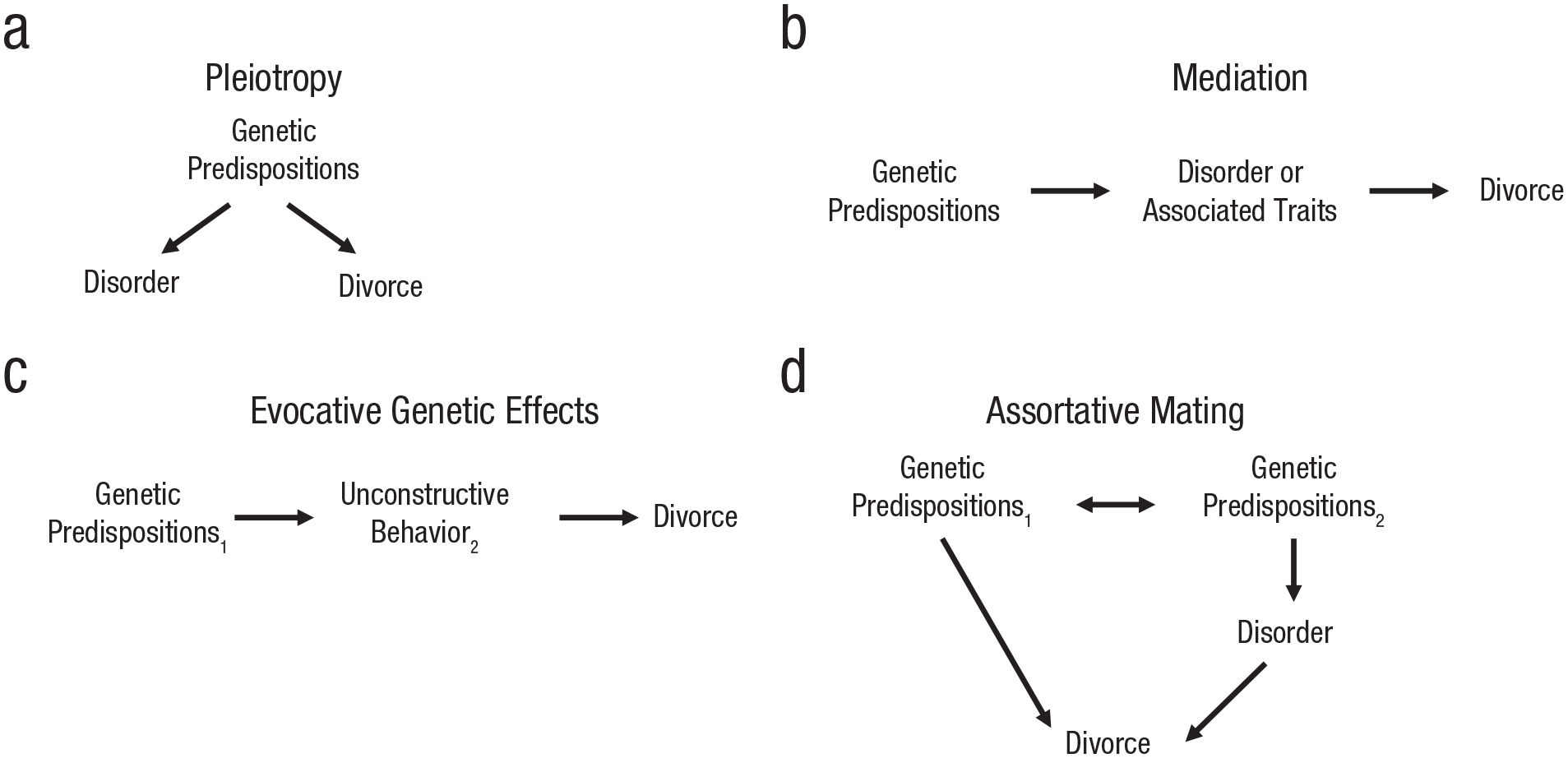
Schematic of selected mechanisms linking genetic predispositions for psychiatric disorders and divorce. Subscripts refer to Partner 1 and Partner 2 in marital dyads.
Our results should also be interpreted in the context of the study’s limitations. First, because the analyses were limited to the Swedish population, the potential generalizability to other populations is unknown. The crude annual divorce rate in Sweden is one of the highest in Europe, with 2.7 divorces per 1,000 inhabitants according 2014 data (Eurostat, 2016). Relatedly, although the cohort used for these analyses was selected to allow for a suitable follow-up period for observing marriage and divorce, we recognize that some unmarried individuals from the younger birth cohorts may in fact go on to marry and that some married individuals may go on to divorce. The consequence of these misclassifications on our inferences is that the differences between unmarried and married individuals and between married and divorced individuals are likely underestimated. Second, the FGRS approach depends on the accuracy of the diagnoses and the performance of the cohabitation correction. Diagnoses came from national registries and for this reason, generally capture the more severely affected individuals. Encouragingly, the rates of several disorders observed here closely parallel the rates observed in an epidemiological study in nearby Norway (Kringlen et al., 2001). Also tempering this concern, in previous work, we have demonstrated a high degree of concordance across our different methods of ascertainment for AUD and DUD diagnoses (Kendler et al., 2015) and the validity of psychiatric diagnoses from primary-care-register data (with primary care being the most common setting for common psychiatric disorders in Sweden; Sundquist et al., 2017). Furthermore, in simulations, we demonstrated that the correction for the shared environment performs as expected, suggesting that the FGRS largely captures genetic rather than shared environmental risk (Kendler, Ohlsson, Bacanu, et al., 2023). Third, divorce is by definition a dyadic rather than individual event. Accordingly, we recognize that the genetic makeup of both partners is likely to be important for whether a couple divorces or remains stably married, and a dyadic perspective represents an important future direction for this line of inquiry. This is particularly true in view of evidence that spousal concordance/discordance on genetically influenced traits such as neuroticism and conscientiousness predict relationship stability (Kurdek, 1993). Fourth, although divorce laws in Sweden are quite liberal, there are also cultural, social, and economic factors that influence whether an individual or couple will divorce. Accordingly, there may be subgroups for which the FGRS patterns associated with marital status differ, such as immigrants (whose marriages are more likely to dissolve compared with individuals born to Swedish-born parents; Andersson et al., 2015) or couples with young children (Andersson, 1997).
In the Swedish population, divorce is associated with elevated FGRSs for 10 major psychiatric disorders. These elevations were particularly pronounced among divorced females compared with divorced males, among individuals who did not go on to have a stable second marriage, and among individuals with multiple divorce transitions. There were particularly notable elevations in FGRSs for internalizing disorders and substance use disorders. As a set, the results from this study provide some of the most comprehensive evidence concerning the genetic landscape of psychiatric disorders related to divorce.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026231214204 – Supplemental material for Family Genetic-Risk Profiles Associated With Divorce
Supplemental material, sj-docx-1-cpx-10.1177_21677026231214204 for Family Genetic-Risk Profiles Associated With Divorce by Jessica E. Salvatore, Henrik Ohlsson, Jan Sundquist, Kristina Sundquist and Kenneth S. Kendler in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Jennifer Lau
Editor: Jennifer L. Tackett
Author Contribution(s)
K. Sundquist and K. S. Kendler share last authorship.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.