
Abstract
Although obsessive compulsive disorder (OCD) features maladaptive decision-making, previous research that examined economic decision-making in OCD has yielded inconsistent results. Here, we examined whether unmedicated adults with OCD (n = 268) differ from healthy control subjects (HCSs; n = 256) on two measures of decision-making about potential rewards: (a) delay discounting, the tendency to prefer rewards sooner rather than later, even if the delayed reward is larger, and (b) risk tolerance, the willingness to gamble for uncertain rewards when the risk is known. Data were collected in Brazil, India, the Netherlands, South Africa, and the United States as part of the Global OCD study. After controlling for age, sex, education, socioeconomic status, IQ, and site, individuals with OCD did not differ from HCSs in either delay discounting or risk tolerance. However, patients with OCD who reported more anxiety and depression showed higher delay discounting, or a relative preference for immediate rewards.
Obsessive compulsive disorder (OCD) is one of the most common and debilitating psychiatric disorders, with a lifetime prevalence of about 2% (Fontenelle et al., 2006; Ruscio et al., 2010). OCD is marked by the presence of obsessions (i.e., distressing, unwanted thoughts) and/or compulsions (i.e., repetitive behaviors that individuals feel driven to perform, often to get temporary relief from obsessions). It is a chronic disorder and a leading cause of disability worldwide (Baxter et al., 2014). OCD is associated with lower quality of life (Remmerswaal et al., 2016; Rosa et al., 2012), less educational attainment (Pérez-Vigil et al., 2018), and an increased risk of suicide (Torres et al., 2011). Thus, understanding the neurocognitive mechanisms that are disrupted in OCD is of critical importance. The Global OCD study was designed to identify robust, generalizable brain and behavioral signatures of OCD with the goal of better conceptualizing OCD to improve diagnosis and treatment (Simpson et al., 2020).
One domain in which people with OCD may show systematic impairments is in value-based decision-making (Cavedini et al., 2006; Sachdev & Malhi, 2005). For example, they perform compulsive activities (e.g., checking, hand washing) that provide immediate relief but negative consequences in the long term. There is research showing that people with OCD make less advantageous choices (Cavedini et al., 2002; Starcke et al., 2010; Zhang et al., 2015). However, the findings of this research have been mixed, and some tasks that have been used in the past (e.g., Iowa gambling task) are not optimized for teasing apart different decision variables. Here, we analyzed Global OCD study data to examine differences between patients with OCD and healthy control subjects (HCSs) on two distinct aspects of value-based decision-making: delay discounting and risk tolerance.
Delay discounting is the extent to which the subjective value of a delayed reward decreases as the delay to receiving it increases (Mazur, 1987; Strotz, 1956). Although everyone discounts delayed rewards to some degree, people vary widely in their rate of delay discounting (Keidel et al., 2021; Peters & Büchel, 2011). Delay-discounting rates can be measured in the lab by having participants make a series of choices between smaller, sooner monetary rewards (e.g., $10 today) and larger, later monetary rewards (e.g., $20 in 30 days). Higher discount rates measured in the lab are associated with real-world harmful behaviors, including substance abuse and other addictive behaviors, physical inactivity, overspending, and overeating (Amlung et al., 2017; Bartels et al., 2023; MacKillop et al., 2011; McClelland et al., 2016). Delay discounting is also elevated in several psychiatric conditions (e.g., substance use disorder, attention-deficit/hyperactivity disorder, schizophrenia, and depression), suggesting that it may be a critical trans-disease process in psychopathology (Amlung et al., 2019; Lempert et al., 2019). Delay discounting has often been considered a measure of impulsive choice, so it is fitting that those disorders in which impulsive behavior is observed, such as in behavioral addictions or substance use disorders, are the ones in which the highest discount rates are observed.
Given that OCD is characterized by compulsive and impulsive behavior, previous research has investigated whether individuals with OCD have higher discount rates than HCSs. Perhaps surprisingly, there is little evidence that discount rates in individuals with OCD are higher than those of HCSs (Norman et al., 2017; Pinto et al., 2014; Steinglass et al., 2017). Only one study found higher discount rates in OCD, but that study included medicated individuals and did not control for comorbidities (Sohn et al., 2014). In fact, people with obsessive compulsive personality disorder (OCPD) have been shown to have lower discount rates, or more patience, compared with HCSs (Pinto et al., 2014). There are a few possible reasons for this lack of an association. First, previous studies may have been underpowered to detect this difference. Second, heterogeneity in the symptoms of OCD may have masked that some OCD symptoms are positively associated with discounting, whereas others are negatively associated with discounting. Third, people with OCD simply may not discount delayed rewards at a higher rate than HCSs do. Here, we conducted the highest powered study of delay discounting in OCD to date and preregistered the hypothesis that individuals with OCD will show higher delay discounting (i.e., more myopic choice) than healthy participants.
If there are no overall differences in discounting between OCD and HCS groups, it may be because some symptoms of OCD, such as impulsive behaviors (e.g., aggression; Guo et al., 2017), are associated with higher discounting, whereas other symptoms, such as anxiety, are associated with lower discounting. This latter hypothesis is based on one previous study (Steinglass et al., 2017), in which trait anxiety (as measured by the Spielberger trait anxiety inventory; Spielberger, 1983) was associated with lower discounting across individuals with anxiety disorders, including OCD, social anxiety disorder, and anorexia nervosa, and HCSs. Even in just the OCD subgroup (n = 50) in that study, the extent to which those individuals endorsed feeling generally anxious was associated with being more willing to wait for future rewards (Steinglass et al., 2017). Thus, here we planned to examine continuous associations between anxiety (measured using the Hamilton Anxiety Inventory; Maier et al., 1988) and discounting within the OCD group and between impulsivity (measured using the Compulsive-Impulsions subscale of the Impulsive-Compulsive Behaviors checklist [ICBC]; Guo et al., 2017) and discounting within the OCD group. We preregistered the hypotheses that anxiety would be negatively associated with discounting and that impulsivity would be positively associated with discounting.
Although the primary focus of our study was on delay discounting, we also included a measure of risky choice to assess risk tolerance. Decisions with risky, or uncertain, outcomes might differ between individuals with OCD and HCSs as well. This idea has some support from studies that have examined self-reported intolerance of uncertainty (Tolin et al., 2003) and from cognitive-neuroscience research that implicates structures such as the orbitofrontal cortex and amygdala in both OCD and decision-making under uncertainty (Admon et al., 2012; Bragdon et al., 2023). Previous research has shown that individuals with OCD are more avoidant of risky options (Pushkarskaya et al., 2017; Sip et al., 2016; Sohn et al., 2014) but usually only when the probabilities of those options are unknown or ambiguous (Kim et al., 2015; Pushkarskaya et al., 2015; Starcke et al., 2010; Zhang et al., 2015). However, this literature is inconclusive, mostly because many different risky decision-making tasks have been used, and not all of them can quantify risk tolerance unconfounded by other variables. For example, even the studies that have asked participants to make choices between certain options and gambles vary the probability that is associated with the risky option, thus making it impossible to know whether people with OCD vary with respect to perceptions of risk or attitudes toward risk. Here, we used a well-validated task in which people choose between certain options and gambles and the gamble probabilities are always fixed at 50% (Lempert et al., 2020; Yu et al., 2017). From these choices, we can derive a risk-tolerance parameter that captures risk attitudes (specifically in the domain of potential monetary gains) unconfounded by other factors. We preregistered the hypothesis that participants with OCD would show reduced risk tolerance (i.e., increased risk aversion) relative to HCSs.
Transparency and Openness
This study involved an analysis of existing data from the Global OCD study (Simpson et al., 2020). The analyses and hypotheses were preregistered on OSF (https://osf.io/u62m9), and we note below instances in which analyses deviated from preregistration. In addition to testing the preregistered hypotheses mentioned in the introduction, we also preregistered our expectation that our results would be consistent across sites. In other words, we did not expect to see a group (OCD vs. HCS) by site interaction when examining risk tolerance or delay discounting, and we did not expect to see either an anxiety by site interaction or an impulsivity by site interaction when examining the relationships between those variables and delay discounting within the OCD group. Upon completion of the studies outlined in the Global OCD study grant, all data will be submitted to the National Institute of Mental Health Data Archive, a data repository funded by the National Institutes of Health. All the data, analysis code, and research materials pertaining to this article are also available on request from H. B. Simpson.
Ethical Approval
Experimenters from all sites completed online training on ethics in research and were certified after completing this course. The following institutional ethics boards reviewed and approved the study: Brazil, National Committee of Ethics in Research, Ministry of Health, Federal Government of Brazil (Reference 2.447.060); India, National Institute of Mental Health and NeuroSciences; Netherlands, Medisch Ethische Toetsingscommissie at Vrije Universiteit medisch centrum (Reference 2017.296–NL61982.029.17); South Africa, the Stellenbosch University’s Health Research Ethics Committee (Reference N17/05/053) and the University of Cape Town’s Human Research Ethics Committee (Reference 358/2017); and United States, the Institutional Review Board at the New York State Psychiatric Institute (Reference 7471). Written informed consent was obtained from all study participants.
Method
Overview
In the current study, we used a cross-sectional global sample of unmedicated individuals with OCD and HCSs from five different countries (Brazil, India, South Africa, the Netherlands, and the United States) located on five different continents (Simpson et al., 2020). As was detailed in a previous article (Batistuzzo et al., 2023), the delay-discounting and risk-tolerance measures were harmonized; this included not only currency conversion but also matching monetary amounts based on purchasing power. This harmonization was generally successful because site differences in delay discounting and risk tolerance were small in the HCS sample. Only India differed from the other sites in risk tolerance (less risk tolerance was observed in Indian participants), and only the Netherlands differed from the other sites on delay discounting (lower discounting rates were seen in that group). We controlled for site in all analyses in this article. We also controlled for important covariates that have been linked with these decision-making measures before: socioeconomic status (SES), age, sex, education, and intelligence.
Inclusion and exclusion criteria
To be included, participants with OCD had to be between 18 and 50 years old and had to have OCD as their principal diagnosis with at least moderate severity (Yale-Brown Obsessive-Compulsive Scale [Y-BOCS] score > 16). They were excluded if they had (a) lifetime diagnosis of psychosis, bipolar disorder, anorexia, autism, or Tourette disorder; (b) a current chronic tic disorder, substance use disorder, binge-eating disorder, bulimia, or suicidality; (c) current use of psychotropic medications or cognitive-behavioral therapy for OCD; (d) major medical or neurological disorders; (e) IQ < 80; or (f) contraindications to MRI (because the larger study included a neuroimaging component; Simpson et al., 2020).
HCSs were between 18 and 50 years old and were excluded if they had (a) a current or lifetime psychiatric disorder other than major depressive disorder or anxiety disorders (if not in the past year), (b) current or past use of psychotropic medications, (c) a first-degree relative with OCD or tic disorder, (d) major medical or neurological disorders, (e) IQ < 80, or (6) contraindications to MRI.
A total of 268 medication-free patients with OCD and 256 HCSs completed the study across all five sites: Brazil, n = 111 (OCD: n = 58; HCS: n = 53; 67% White, 21% mixed race, 9.9% Black, 2.7% East Asian); India, n = 107 (OCD: n = 57; HCS: n = 50; 100% South Asian); the Netherlands, n = 100 (OCD: n = 50; HCS: n = 50; 97% White, 2% mixed race, 1% Black); South Africa, n = 104 (OCD: n = 52; HCS: n = 52; 62% White, 29% mixed race, 1% South Asian, 8.7% Black); United States, n = 102 (OCD: n = 51; HCS: n = 50; 53% White, 16% Black, 12% East Asian, 11% mixed race, 6.9% South Asian, 1% American Indian). Demographic characteristics of both groups are shown in Table 1.
Demographic Characteristics of Patients With OCD and Healthy Control Subjects

Note: HCS = healthy control subject; OCD = obsessive compulsive disorder; CI = confidence interval; IQR = interquartile range; 8WAMI = Water and sanitation, Assets and household wealth, Maternal education, and Income.
Adjusted for site.
Standardized mean difference.
Clinical and demographic measures
A standardized protocol was used at all sites to clinically assess subjects in their respective language (i.e., Portuguese, Kannada, Dutch, Afrikaans, or English). This protocol included measures of total OCD severity, dimension severity, insight, sensory phenomena, age of onset, depression, anxiety, functioning, and other clinical profiles (Simpson et al., 2020).
In addition to age, sex, years of education, and site, we also included measures of SES and IQ as covariates in our primary analyses. To evaluate SES, the WAMI was administered. The WAMI generates an index based on access to improved water and sanitation (W), assets and household wealth (A), maternal education (M), and income (I). Each domain was measured using a scale from 0 to 8, and the total number of points was divided by 32 to get the index from 0 to 1 (Psaki et al., 2014). Given that no single IQ measure had been validated across all five countries and languages, each site selected its own measure of IQ. This IQ measure had to have been validated in the appropriate language for its respective country and had to yield a general IQ score and an estimate of performance in verbal domains (Brazil: first edition of the Wechsler Abbreviated Scale of Intelligence, Wechsler, 1999; India: Binet Kamat Test, Kamat, 1968; Netherlands: selected subscales from the fourth edition of the Wechsler Adult Intelligence Scale, Wechsler, 1997; South Africa and United States: second edition of the Wechsler Abbreviated Scale of Intelligence, Wechsler, 2011). The general IQ score was used as the measure of IQ in this study.
A few clinical measures were of interest to the current study as well. To test our hypothesis about the association between anxiety and delay discounting, the Hamilton Anxiety Rating Scale (HAM-A; Hamilton, 1959) served as our measure of anxiety. This 14-item self-report questionnaire measures both psychic anxiety (mental agitation and psychological distress) and somatic anxiety (physical complaints related to anxiety). To test our hypothesis about the association between impulsive behavior and delay discounting, we examined data obtained with the ICBC (Guo et al., 2017). The ICBC assesses the extent to which people with OCD display impulsive behaviors (i.e., smoking, betting, swearing, tattooing, and drug and alcohol use) and compulsive behaviors (i.e., washing, collecting, counting, and grooming). Note that although the authors of the ICBC (Guo et al., 2017) referred to these as “compulsive-impulsions” and “impulsive-compulsions,” respectively, we use the terms “impulsive behaviors” and “compulsive behaviors” for these subscales here for clarity. The impulsive-behaviors-subscale score served as our measure of impulsive behavior, although we also examined compulsive behaviors in exploratory analyses.
In additional exploratory analyses, we examined relationships between decision-making measures and the following: (a) Hamilton Depression Rating Scale (HAM-D; Hamilton, 1960); (b) age of OCD onset (categorically defined as early onset = 1–10 years old, intermediate onset = 11–17 years old, or late onset = 18+ years old); (c) the Y-BOCS total score (Goodman et al., 1989), a measure of OCD severity; (d) OCPD severity; and (e) the dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS; Rosario-Campos et al., 2006). The DY-BOCS contains the following dimensions: aggression, sexual/religious, symmetry, contamination, hoarding, and miscellaneous. The OCPD-severity measure represents the number of clinically significant OCPD criteria from the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders met by the participant, as assessed with questions from the Diagnostic Interview of Personality Disorders (Zanarini et al., 1987). One previous study (Pinto et al., 2014) found that people who had comorbid OCD and OCPD had significantly lower discount rates than HCSs. To see if this finding would replicate here, we compared participants with OCD who also met criteria for OCPD to HCSs who did not meet criteria for OCPD on the delay-discounting measure. We also examined the relationship between OCPD symptoms and delay discounting continuously within the OCD sample. For comparison between participants with OCD and HCSs on relevant clinical variables, see Table 2.
Summary of Select Clinical Measures for Patients With OCD and Healthy Control Subjects

Note: HCS = healthy control subject; OCD = obsessive compulsive disorder; Y-BOCS = Yale-Brown Obsessive-Compulsive Scale; ICBC = Impulsive-Compulsive Behaviors checklist; OCPD = obsessive compulsive personality disorder (number of diagnostic criteria endorsed).
Wilcoxon rank sum test, Fisher’s exact test, or Pearson chi square test.
n = 2 missing data from OCD group.
n = 4 missing data from HCS group, n = 3 missing data from OCD group.
n = 1 missing data from HCS group, n = 2 missing data from OCD group.
Decision-making tasks
Participants completed an intertemporal-choice task to assess delay discounting and a risky-choice task to assess risk tolerance.
On each of the 51 trials in the intertemporal-choice task (Fig. 1a), participants chose between a small amount of money available immediately and a larger amount of money available at a specified delay (Lempert et al., 2020; Pehlivanova et al., 2018; Senecal et al., 2012; Yu et al., 2017). The delayed outcome was always one of three amounts: $25, $30, or $35. Immediate reward amounts varied from $10 to $34, and delays ranged from 1 to 180 days. The immediate and delayed options alternated sides of the screen randomly from trial to trial. After participants selected their choice, a checkmark appeared on the screen indicating which side they had pressed.
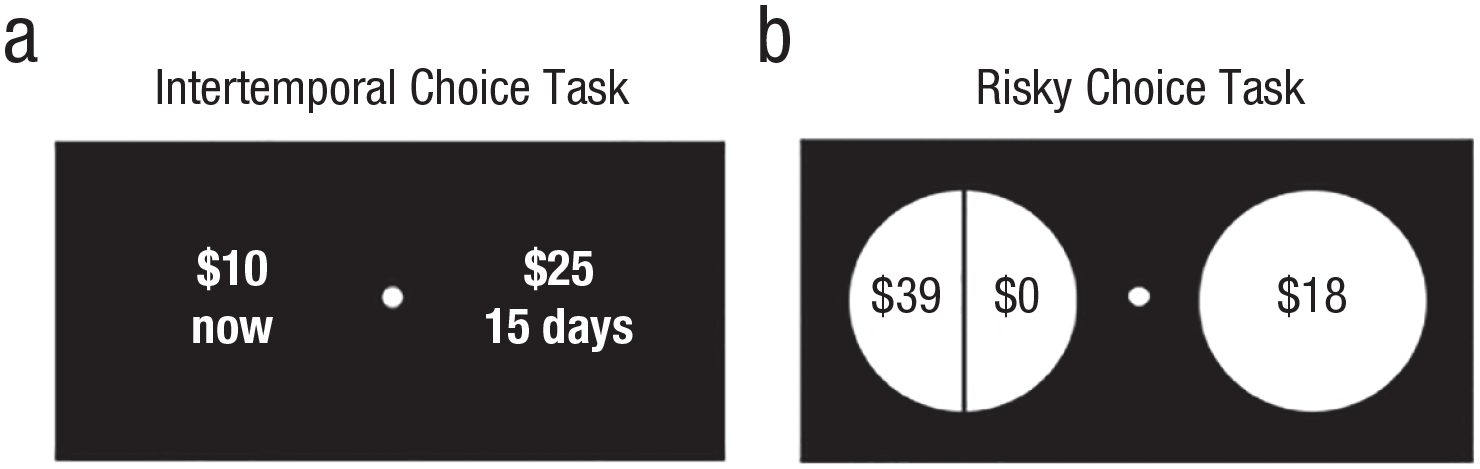
Sample choice screens from (a) the intertemporal-choice task and (b) the risky-choice task. Amounts were converted as appropriate for each site.
The goal of this task was to capture 17 hyperbolic discount rates, ranging from 0.0001 to 0.2525, equally distant in log-space (Senecal et al., 2012). For each of these discount rates, three trials were drawn from its “indifference curve”—one for each of the future amounts: $25, $30, and $35. Delays were quasirandomly generated with the constraints that the immediate amounts were integers and that delays did not exceed 180 days. Like the well-validated Kirby monetary-choice questionnaire (Kirby et al., 1999), this task can capture a wide range of discount rates but with even finer gradations (Lempert et al., 2019).
On each trial of the 60 choices in the risky-choice task (Lempert et al., 2020; Yu et al., 2017), participants chose between a small amount of money ($1–$63) available for certain and a larger amount of money ($10–$100) available with some risk. All risky options entailed a 50% chance of the larger amount and a 50% chance of $0. We used a 50% probability for all trials to minimize the confounding factor of probability distortion, which might also vary among individuals. Probabilities (either 100% or 50%/50%) were displayed graphically using pie charts (Fig. 1b). The risky and safe options alternated sides of the screen randomly from trial to trial. As with the intertemporal-choice task above, the monetary amounts were selected to sample a range of risk-tolerance parameters with the constraint that amounts were always integers and did not exceed $100.
In both decision-making tasks, participants used their left and right index fingers to press “f” or “j” on the keyboard to select their preferred option. Moreover, in both tasks, the order of the trials was randomized. After participants made their choice, a checkmark appeared on the screen for 500 ms, confirming their choice, followed by an intertrial interval of 1 s before the subsequent trial was presented. Both tasks had two training trials for the individuals to practice before data collection started. Before both tasks, participants were informed that (a) there were no right or wrong answers, (b) they should choose what they preferred, and (c) they would receive real money from one of the trials depending on their choice. In reality, all participants received the same amount ($24 in U.S. currency) that day after all tasks were finished. Although it is more typical to select a trial at random, it was more important in our case to standardize the protocol and subject compensation as much as possible across sites. Note that participants did not know which trial would be chosen, though, so at the time that they did the tasks, they believed that each trial was equally likely to be selected for payment. Moreover, $24 was offered in both decision-making tasks, so it was an amount that was likely to have been chosen by the participant.
One of the challenges of studying choices related to financial rewards is the fact that the same amount of money could vary in its purchasing power across countries. Because the currency of monetary reward differed across the sites, a suitable conversion formula based on purchasing power parities (PPPs) was calculated to ensure the monetary rewards were appropriately rewarding across currencies and countries. PPPs are the rates of currency conversion that try to equalize the purchasing power of different currencies by eliminating the differences in price levels between countries (Organisation for Economic Co-Operation and Development, 2017). This correction is particularly important given that lower SES has been linked with increased risk aversion and higher delay discounting (Haushofer & Fehr, 2014). For the precise amounts that were used at each site in this study, see Batistuzzo et al. (2023).
Data analysis
Participants’ individual choice data for the intertemporal- and risky-choice tasks were fit with the following logistic function using maximum likelihood estimation:

where P1 refers to the probability that the participant chose Option 1 and P2 refers to the probability that the participant chose Option 2. SV1 and SV2 refer to the participant’s estimated subjective value of Option 1 and Option 2, respectively. The scaling factor β was fitted for each individual task. In a set of exploratory analyses, we examined whether there were group differences (OCD vs. HCS) in this scaling factor for either task. We did not find any differences (all ps > .05), so we did not consider this parameter further.
In the risky-choice task, P1 was the probability of choosing the risky option. SV1 and SV2 (for the risky option and safe option, respectively) were estimated using a power utility function:

Here, A is the amount that could be received, p is the probability of receipt (p = .5 for the risky option, p = 1 for the certain option), and α is a risk-tolerance parameter that varies across subjects. Higher α indicates greater risk tolerance (less risk aversion).
In the intertemporal-choice task, P1 was the probability of choosing the delayed option, and the subjective values of the options were estimated using a hyperbolic discounting function (Green & Myerson, 2004; Mazur, 1987):

Here, A is the amount received, D is the delay until receipt (for immediate rewards, D = 0), and k is a discount-rate parameter that varies across subjects. Higher k indicates higher discounting (less tolerance of delay). Because k and α were not normally distributed, these values were natural log-transformed before conducting statistical analyses.
We performed quality control to ensure that participants were not responding randomly in the delay-discounting and risk-tolerance tasks by verifying that their responses were a function of task variables that should be relevant to the choice (Pehlivanova et al., 2018). For each task, participants’ responses were fit using a multinomial logistic regression model in which predictors for the risk-tolerance task included the certain and risky amounts and their squared terms and predictors for the delay-discounting task included the immediate amount, delayed amount, delay, and their squared terms. We assessed the goodness of fit of these regression models using the coefficient of discrimination (Tjur, 2009) and discarded data from participants who had a Tjur coefficient value < 0.20.
We used multiple linear regression to test our hypotheses that individuals with OCD would have increased delay discounting and reduced risk tolerance. Two separate linear regression models, one predicting delay discounting and one predicting risk tolerance, were run with OCD diagnosis as the independent variable of interest. All models were adjusted for covariates, including site, age, sex, years of education, SES, IQ, and the interaction of site with each of the other covariates. Note that our preregistration document did not explicitly mention the interaction terms between site and the other covariates. To test for OCD–HCS group differences by site, we fit separate models that included a group by site interaction term. This is also a slight deviation from our preregistration, which implied that the group by site interaction term would be included in the main model rather than tested in a separate model.
We also hypothesized that within the OCD group, the impulsive-behaviors subscale of the ICBC would be positively associated with delay discounting and that anxiety (HAM-A) would be negatively associated with delay discounting. Once again, we ran two multiple linear regressions. Delay discounting was the dependent variable in both regressions, but in one, the impulsive-behaviors subscale was the independent variable of interest, and in the other, the HAM-A score was the independent variable of interest. For these analyses, the HCSs were excluded, and group was removed as a predictor. Otherwise, all covariates were the same as above (age, sex, education, WAMI, IQ, site, and the interaction of site with the other covariates). Interaction terms between site and the independent variable of interest (HAM-A or impulsive behaviors) were also included in separate models. The significance level was set at α = .05 for all analyses. In a deviation from our preregistration, we did not perform any secondary sensitivity analyses.
Results
Preregistered analyses
The OCD (n = 268) and HCS (n = 256) samples were matched on age and sex, although they did significantly differ with respect to education, SES, and IQ (Table 1). Eleven patients with OCD and 11 HCSs did not complete the intertemporal-choice task, and two HCSs did not complete the risky-choice task. Of the participants who did complete the decision-making tasks, 34 were excluded because of poor-quality data (i.e., Tjur coefficient value < 0.20) in the risky-choice task (OCD: n = 19; HCS: n = 15), and three were excluded in the intertemporal-choice task (OCD: n = 2; HCS: n = 1). Therefore, in all delay-discounting analyses below, the total number of participants is 499 (OCD: n = 255; HCS: n = 244), and in all risk-tolerance analyses below, the number of participants is 488 (OCD: n = 249; HCS: n = 239).
Contrary to our first hypothesis, the OCD and HCS groups did not differ in their delay discounting (β = −0.006, p = .964; Table 3; for full regression output, see Table S1 in the Supplemental Material available online). Participants with OCD did not prefer smaller, sooner rewards more than HCSs did. Given that we obtained a null result, we calculated a Bayes factor post hoc to quantify the strength of evidence for the null hypothesis relative to the alternative hypothesis. According to standard cutoffs (Andraszewicz et al., 2015), the Bayes factor for this effect indicated that there was moderate evidence for the null hypothesis that discounting did not differ between groups (BF10 = 0.110, 95% confidence interval [CI] = [0.098, 0.121]). We also planned to see if there was a significant group by site interaction because it is possible that effects of OCD diagnosis might differ between sites. There was no significant group by site interaction in the delay-discounting model (F = 0.641, df = 4, p = .634).
Decision-Making Measures in OCD and HCS Samples

Note: HCS = healthy control subject; OCD = obsessive compulsive disorder.
Adjusted for site, age, sex, education, socioeconomic status, and IQ. Includes an interaction between all covariates and site.
Participants with OCD were also not more risk averse than HCSs were (β = 0.006, p = .888; Table 3; Table S2 in the Supplemental Material). Here, the Bayes factor suggested that there was strong evidence for the null hypothesis (BF10 = 0.090, 95% CI = [0.075, 0.105]). There was a significant group by site interaction in the risk-tolerance model (F = 2.48, df = 4, p = .043), however. In a post hoc analysis, we found that this interaction was driven by a significant difference in risk aversion between patients with OCD and HCSs at the site in India (β = 0.113, p = .034) but none of the other sites (Brazil: β = 0.062, p = .195; United States: β = −0.027, p = .567; Netherlands: β = −0.020, p = .687; South Africa: β = −0.087, p = .061). Given that the participants in India had, on average, lower risk-aversion parameters than participants at other sites (Batistuzzo et al., 2023), we reasoned that this group effect may be driven by HCSs in India who never selected a risky option. Indeed, when removing these “floor” subjects (n = 18), the group by site interaction was no longer significant (F = 1.37, df = 4, p = .245), and the effect of group on risk tolerance remained null (β = 0.033, p = .392).
Next, we examined whether impulsivity and anxiety within the OCD group were associated with delay discounting. Contrary to our hypothesis that impulsivity would be positively associated with delay discounting, there was no relationship between impulsivity (as measured by the ICBC impulsive-behaviors subscale) and delay discounting (β = 0.068, p = .335; Table S3 in the Supplemental Material). There was also no significant group by site interaction (F = 0.14, df = 4, p = .968). Regarding anxiety, we expected to see a negative association between HAM-A scores and delay discounting within the OCD group. However, we found that there was a significant association between anxiety and discounting in the opposite direction such that the OCD patients who reported more anxiety symptoms were more likely to select immediate rewards in the intertemporal-choice task (β = 0.042, p = .004; Fig. 2a; Table S4 in the Supplemental Material). We also found a significant anxiety by site interaction (F = 2.78, df = 4, p = .028), which was driven by there being a large effect size in the sample from the U.S. site (β = 0.145, p < .001) but none of the other sites (Brazil: β = 0.033, p = .172; India: β = 0.039, p = .465; Netherlands: β = 0.043, p = .246; South Africa: β = 0.010, p = .679; Fig. S1 in the Supplemental Material).
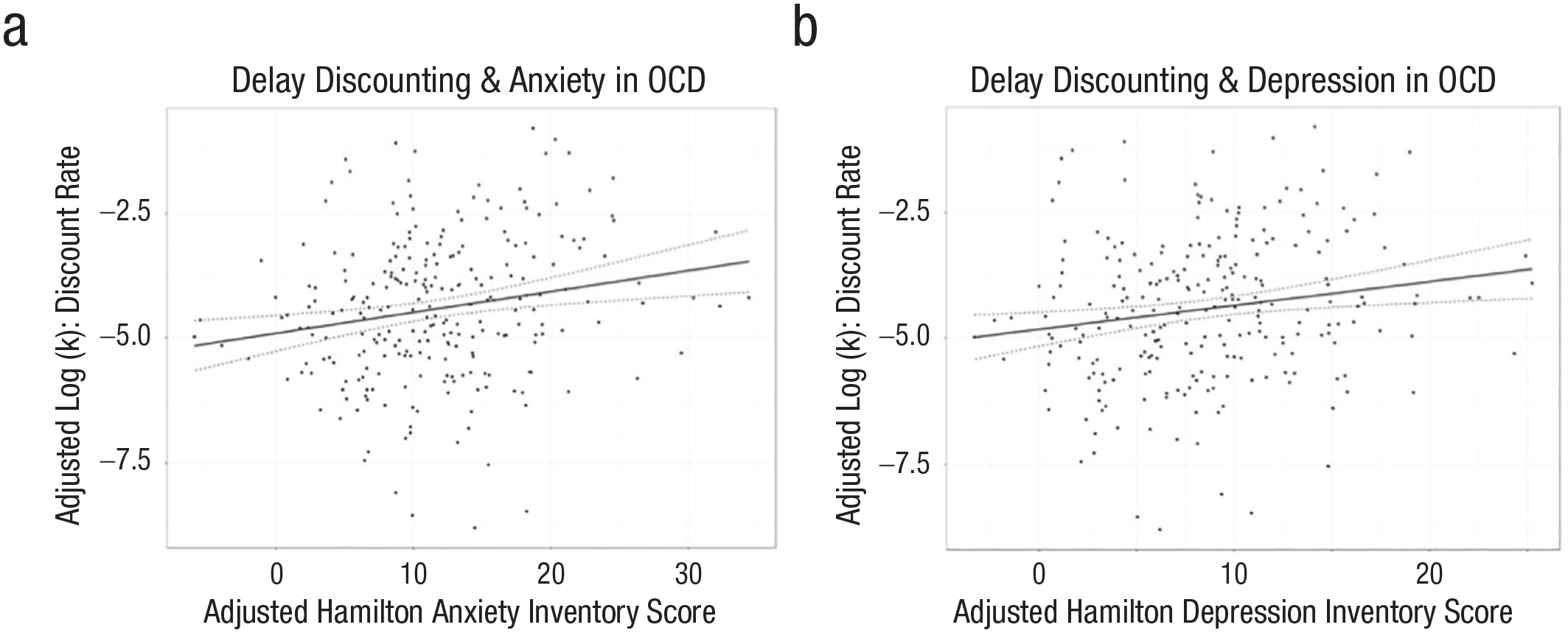
Associations between delay discounting and (a) anxiety and (b) depression in the obsessive-compulsive-disorder (OCD) group. Partial regression plots are shown after adjusting for covariates (site, sex, age, education, socioeconomic status, IQ, and interactions between all covariates and site). Within the OCD group (n = 268), increased Hamilton Anxiety Rating Scale (anxiety) and Hamilton Depression Rating Scale (depression) scores were associated with higher delay discounting such that people who were more depressed and anxious were more likely to choose smaller, immediate rewards over larger, delayed rewards.
Exploratory analyses
Next, we conducted a series of exploratory regressions to see if other clinical variables—compulsive behaviors (as measured by the ICBC compulsive-behaviors subscale), Y-BOCS scores, DY-BOCS dimensions, age of OCD onset, OCPD-severity scores, and HAM-D depression scores—were associated with delay discounting or risk tolerance within the OCD group. For risk tolerance, there were no significant associations found (all ps > .05). For delay discounting, however, depression symptoms (HAM-D scores) were positively associated with delay discounting such that patients who were more depressed were more likely to prefer smaller, sooner rewards (β = 0.048, p = .010; Fig. 2b; Table S5 in the Supplemental Material). Furthermore, just as was the case for anxiety symptoms, this effect was largest in the sample from the U.S. site (interaction: F = 3.58, df = 4, p = .008; United States: β = 0.148, p < .001; Brazil: β = 0.034, p = .273; India: β = −0.057, p = .314; Netherlands: β = 0.052, p = .250; South Africa: β = 0.025, p = .516; Fig. S2 in the Supplemental Material). Unfortunately, because of the high collinearity between HAM-A and HAM-D scores (r = .9), we could not determine whether depression or anxiety was a better predictor of delay discounting in OCD.
Given these significant findings, we next examined whether HAM-A and HAM-D scores were associated with delay discounting across both groups or within the HCS group only. When the two groups were combined, HAM-A and HAM-D remained significant predictors of delay discounting (HAM-A: β = 0.018, p = .044; HAM-D: β = 0.024, p = .045). However, neither of these associations were significant when restricting analyses to the HCS group (HAM-A: β = 0.016, p = .729; HAM-D: β = 0.053, p = .328).
Although we found no association between OCPD severity and delay discounting within the OCD group (β = 0.009, p = .879), we performed an additional analysis to examine if individuals who fulfilled diagnostic criteria for OCPD (n = 61 within the OCD group) differed from HCSs in delay discounting. Although we did not preregister this hypothesis, a previous study (Pinto et al., 2014) found that people who have comorbid OCD and OCPD have significantly lower discount rates compared with HCSs. In the current study, however, discount rates did not differ significantly between participants with comorbid OCD and OCPD and HCSs (β = −0.023, p = .913).
Discussion
In this study, we examined two distinct forms of value-based decision-making in a large, global, multisite study of unmedicated individuals with OCD and HCSs. Contrary to our preregistered hypotheses, we found that neither delay discounting (the tendency to prefer smaller, sooner rewards over larger, later rewards) nor risk tolerance (the tendency to prefer larger, uncertain rewards over smaller, certain rewards) were altered in the OCD group compared with the HCS group. We also did not find evidence of an association between impulsive behaviors and delay discounting in the OCD group. However, symptoms of anxiety within the OCD group were positively associated with delay discounting such that more anxious individuals were more likely to select immediate rewards at their long-term expense. In an exploratory analysis, we found that symptoms of depression were also positively associated with delay discounting in the OCD group.
Although null results may be difficult to interpret, we believe that our study provides the most compelling support to date that delay discounting is not elevated in OCD. Our sample size was large, so we can be confident that even if there is an effect, it is likely to be small and not clinically meaningful. This finding is important for a few reasons. First, most previous studies on this topic also found no differences in delay discounting between OCD and HCSs (Norman et al., 2017; Pinto et al., 2014; Steinglass et al., 2017), but those studies were small, so researchers have continued to investigate this question. Our result will thus encourage OCD researchers to focus on other cognitive processes that might be implicated in this disorder. Second, delay discounting has recently been criticized for lacking clinical utility, partly on the grounds that it is not sufficiently sensitive or disorder-specific (Bailey et al., 2021). Bailey and colleagues (2021) argued that if increased delay discounting is observed in most psychiatric disorders, it is not a useful marker for any disorder or dimension of psychopathology. However, the fact that discounting is elevated in some disorders (e.g., substance use disorder; Amlung et al., 2017; MacKillop et al., 2011) but not in OCD suggests that delay discounting might be helpful for differentiating between disorders that otherwise share features. Finally, our null finding is important because it adds to a growing body of evidence that shows that steep delay discounting does not reflect a lack of inhibitory control (Berkman et al., 2017; Jauregi et al., 2018; Lempert et al., 2020; Urošević et al., 2016). A lack of inhibitory control is a prominent feature in OCD; people with OCD often feel compelled to perform actions that they know they should resist performing (Chamberlain et al., 2005; Norman et al., 2019). If high delay discounting resulted from an inability to control one’s actions in the face of temptation, then we probably would have found increased delay discounting in the OCD group. We also would have observed an association between impulsive behaviors in OCD and delay discounting, but that was not the case. Therefore, our study sheds more light not only on the neurocognitive mechanisms that are disrupted in OCD but also on what the delay-discounting paradigm is actually measuring.
Our study is not the first to suggest that delay discounting captures something other than the inability to control impulses. Not only do discount rates correlate very weakly with questionnaire measures of impulsivity (Eisenberg et al., 2019; Murphy & Mackillop, 2012; Reynolds et al., 2006), but they may even have a distinct genetic basis (Gustavson et al., 2020). If delay discounting does not measure inhibitory control, then what does it measure? One possibility is that delay discounting assesses the extent to which someone has positive expectations about their future. Consistent with this idea, people with addictions, who tend to have high discount rates (Amlung et al., 2017; MacKillop et al., 2011), also have shortened time horizons (Bickel et al., 2008; Petry et al., 1998) such that they have trouble evaluating outcomes in the far future. Another disorder that is marked by both negative thoughts about the future (Roepke & Seligman, 2016) and high delay discounting (Amlung et al., 2019; Levitt et al., 2023; Pulcu et al., 2014) is major depressive disorder, which usually features symptoms of both anxiety and depression (Hopwood, 2023). People with anxious depression may have difficulty prospectively placing value on delayed rewards. One recent study found that across several psychiatric disorders, increased anhedonia was associated with a decreased valuation signal in the ventromedial prefrontal cortex when people were evaluating delayed rewards during intertemporal choice (Souther et al., 2022). Here, we found that both anxiety and depression were positively associated with delay discounting in the OCD group and in the entire sample; this finding converges nicely with the growing literature that suggests that delay discounting is capturing the nature of attitudes toward the future. However, a limitation of our study is that we were unable to disambiguate whether anxiety or depression explained more variance in delay discounting because the HAM-A and HAM-D measures were highly correlated. More research, perhaps using additional questionnaires or other diagnostic groups, is necessary to delineate the unique roles of anxiety and depression in delay discounting.
Although our result that anxiety is positively associated with discounting is consistent with some previous research in anxiety disorders (Bryan & Bryan, 2021; Hurlemann et al., 2019; Rounds et al., 2007), it contradicts other research. Specifically, one previous study found that trait anxiety in OCD was negatively associated with delay discounting (Steinglass et al., 2017). This discrepancy cannot be explained by the fact that the sample here was larger and global because the positive association between anxiety and discounting was actually strongest in the U.S. sample, which is where the Steinglass et al. (2017) study was done. There are two other differences between this study and that one that might explain this discrepancy, though. First, the two studies used different anxiety measures. Here, we used the HAM-A, which assesses symptoms of pathological anxiety, including somatic symptoms (e.g., tension, insomnia, gastrointestinal symptoms). In the Steinglass et al. study, anxiety was assessed with the Spielberger trait anxiety inventory and the neuroticism subscale of the NEO-Five Factor Inventory. These measures are more subjective and more likely reflect normal variations in the tendency to feel anxious (e.g., “I see myself as someone who worries a lot”). The HAM-A may be better able to capture the pathological anxiety that affects decisions about the future. Another major difference is that the Steinglass et al. study did not control for important covariates, such as SES. It is now widely accepted that especially when using monetary rewards as stimuli, lower SES is associated with higher delay discounting (Bickel et al., 2016; Carvalho et al., 2016; Haushofer & Fehr, 2014; Najdzionek et al., 2023). If the more anxious individuals in the previous study also happened to have higher SES, then this might have manifested as a negative association between trait anxiety and delay discounting in that sample. Overall, the current study has many strengths, so we are confident that the association between anxiety and delay discounting is, in fact, positive.
It is noteworthy, however, that there was no significant association between discounting and anxiety (or depression) in the HCS group in either the current study or the Steinglass et al. (2017) study. Indeed, most studies have shown null results when examining the relationship between anxiety or depression and delay discounting in HCSs (Augustine & Larsen, 2011; Olson et al., 2024). This lack of a significant association could be due to the restricted range of anxiety and depression scores in healthy participants in these studies; with increased variability in these measures, a statistically significant effect might emerge. Alternatively, it is possible that a linear relationship between anxiety or depression and delay discounting emerges only when a certain threshold is reached. Future studies in healthy participants with much larger sample sizes could resolve this question.
Another intriguing observation was that when examining the different sites separately, the associations between anxiety/depression and delay discounting in OCD were strongest in and only reached significance in the U.S. sample. It is unclear why this is the case. More research is needed to see if this relationship is present universally but just happens to be strongest in the U.S. sample or if the positive association between delay discounting and anxiety/depression is unique to Americans with OCD. Based on visual inspection of the site-specific scatterplots (Figs. S1 and S2 in the Supplemental Material), the former explanation seems more likely.
With the exception of anxiety and depression symptoms, no other clinical variables (e.g., age of onset of OCD, dimensions assessed by the DY-BOCS) were associated with delay discounting in the OCD group. Most notably, we did not replicate the finding that OCPD severity is negatively associated with delay discounting (Pinto et al., 2014). The relationship between OCPD severity and delay discounting here was null, and individuals who met criteria for OCPD did not differ from HCSs in delay discounting. This nonreplication should be interpreted with caution, however, because our study was not designed to replicate the association between OCPD severity and delay discounting. For one, we did not recruit individuals who had OCPD only, without comorbid OCD. In the study from Pinto and colleagues (2014), the individuals with OCPD only had the lowest discount rates. Therefore, delay discounting might still be reduced in people who have personality traits associated with OCPD who do not also have OCD. Second, here we used a different discounting task from the one used in the Pinto et al. study, and it is possible that OCPD-related traits have an impact on decision-making in some experimental settings but not others. Future research in individuals who meet criteria for OCPD and do not have significant comorbidities will help determine whether delay discounting is altered in that personality disorder.
A secondary aim of the study was to see if patients with OCD and HCSs differed in their risk tolerance. We found no difference between patients with OCD and HCSs in this measure. Furthermore, none of the clinical variables that we examined in OCD were associated with risk tolerance. This null result is consistent with previous research that has shown people with OCD are intolerant of uncertainty only when risks are unknown or ambiguous (Kim et al., 2015; Pushkarskaya et al., 2017; Starcke et al., 2010; Zhang et al., 2015). In the risky-choice task that we used here, we ensured that the risk was always known and always the same (50%). This was an advantage in one sense because it allowed us to measure attitudes toward risk unconfounded by perceptions of risk. People are known to distort probabilities when making decisions (Kahneman & Tversky, 1979), so if we had included a few levels of risk, then we would have had to model probability distortion and risk aversion separately, which would have required additional data. Keeping the level of risk static throughout the task is also a limitation, however, because we cannot generalize our results to situations in which probabilities are very low or very high. Therefore, although we can be confident that people with OCD do not differ from HCSs in their risk attitudes when the risk is moderate (50%), it remains to be seen whether people with OCD differ in their risky decision-making when probabilities are much higher or lower.
In sum, adults with OCD do not show steeper delay discounting or more risk aversion than HCSs do. Our conclusions are bolstered by the fact that (a) our study was sufficiently powered to detect even small differences, (b) our sample was diverse, (c) all of the patients with OCD were unmedicated, and (d) we controlled for important covariates. Our study adds not only to the understanding of OCD, but it also adds to the understanding of delay discounting. Although this construct has traditionally been considered a measure of impulsive choice, it might be better thought of as a measure of pessimism about the future—an interpretation that is supported by our findings that anxiety and depression scores are associated with higher delay discounting in OCD patients.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026241289927 – Supplemental material for Delay Discounting and Risk Tolerance in Obsessive Compulsive Disorder: Results From the Global OCD Study
Supplemental material, sj-docx-1-cpx-10.1177_21677026241289927 for Delay Discounting and Risk Tolerance in Obsessive Compulsive Disorder: Results From the Global OCD Study by Karolina M. Lempert, Benjamin Huber, Marcelo C. Batistuzzo, Karthik Sheshachala, Dianne M. Hezel, Niels T. de Joode, Clara Marincowitz, Christine Lochner, Dan J. Stein, Janardhanan C. Narayanaswamy, Odile A. van den Heuvel, Melanie Wall and Helen Blair Simpson in Clinical Psychological Science
Footnotes
Acknowledgements
We thank the following study team members for help with collecting the data across sites: Jamila Rocha (Brazil), Deise Palermo Ruiz (Brazil), Marines Alves Joaquim (Brazil), Rachel Middleton (United States), Gabrielle R. Messner (United States), Gabriella Restrifo-Bernstein (United States), Sarah Rose (United States), and Yael R. Stovetsky (United States). We also thank Page Van Meter (United States) for data curation and assistance. Finally, we thank the participants for their essential collaboration in this study.
Transparency
Action Editor: DeMond M. Grant
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.