
Abstract
In the United States, there are persistent disparities in mental-health services for linguistically and culturally minoritized groups. We examined whether bilinguals reported psychological symptoms differently when assessed across their two languages. Japanese-English bilinguals completed anxiety-symptom (State-Trait Anxiety Inventory [STAI]) and depression-symptom (Beck Depression Inventory [BDI-II]) scales in Japanese and English, counterbalanced across 2 days. Bilinguals reported higher total anxiety scores but not total depression scores in first-language Japanese than in second-language English. Suicidal thoughts (BDI-II Item 9) were rated higher in Japanese. Bicultural bilinguals who lived in balanced language environments had greater cross-linguistic differences in anxiety and depression symptoms compared with bilinguals who lived in Japanese-dominant environments. Bilinguals may express symptoms differently as a function of language because of varying degrees of emotional reactivity across their first and second languages and associated cultural norms. We conclude that clinicians must consider multilingual assessments to implement equitable and effective mental-health services.
Bilingual speakers face linguistic and cultural barriers to psychological care at each step of access (Ohtani et al., 2015; Sentell et al., 2007), assessment (Leong et al., 2003), treatment (Aggarwal et al., 2016; Kim et al., 2011), and outcomes (Miteva et al., 2022) despite federal mandates to implement linguistically appropriate mental-health services (U.S. Department of Health and Human Services & Office of Minority Health, 2016). In the present study, we integrate research on cultural conceptualization of mental health (e.g., illness narratives; Kleinman, 2020), experiences of racial minorities (e.g., minority-stress theory; Frost & Meyer, 2023), cognitive models of bilingual language processing (e.g., foreign-language effect; Hayakawa et al., 2021), and frameworks of bilingual general function (e.g., consequences of bilingualism for cognition and emotion; Marian, 2023) to study how bilinguals use each of their languages to express psychological distress, or “language-dependent symptom expression.”
We examined clinical-symptom rating scales that have been translated across languages and implemented across cultural groups (Beck et al., 1996; Iwata, Mishima, et al., 1998, 2000; Kojima et al., 2002; Spielberger et al., 1970). Drawing on prior research showing how bilingual speakers recount personal memories (Marian & Kaushanskaya, 2004), activate cultural selves (Y. Hong et al., 2000), and make decisions differently in their first language (L1) and second language (L2; Keysar et al., 2012), we tested whether bilinguals reported their psychological symptoms differently based on the language of assessment (L1 or L2). Our findings have direct implications for the assessment and diagnoses of approximately 12 million individuals who speak multiple languages in the United States and are treated in mental-health-service settings (Martin et al., 2020; United States Census Bureau, 2022).
Bilingualism in Mental-Health-Service Settings
Psychological-health services for minoritized populations—across race (Atdjian & Vega, 2005; Trinh et al., 2019), culture (Jimenez et al., 2022), income (Patel, 2007), gender (Plöderl & Tremblay, 2015), and faith traditions (Gonçalves et al., 2015)—require attention from researchers, clinicians, and government agencies. National mandates established by the National Culturally and Linguistically Appropriate Services Standards focus on communication and language assistance (U.S. Department of Health and Human Services & Office of Minority Health, 2013), including the provision of mental-health services in patients’ native and heritage languages. For example, translated symptom-rating scales are recommended in the patient’s L1 at intake and treatment visits (Campos & Gonçalves, 2011; García-Batista et al., 2018; González et al., 2015). Integrating medical interpreters on the service-provider team has been increasingly adopted and implemented as best practice in many psychiatric and behavioral-health settings (Karliner et al., 2007; Paone & Malott, 2008). The dominant assumption in these L1-focused approaches is that limited L2 English proficiency constitutes a barrier to effective communication, assessment, and intervention (Karliner et al., 2007; Yeheskel & Rawal, 2019).
Despite the recent shift from a bilingual-deficit perspective (e.g., speakers of multiple languages have limited abilities to express themselves in English) to a bilingual-asset perspective (e.g., speakers of multiple languages have abilities to express themselves in Japanese and English; Marian, 2023), studies that focus on bilingual mental-health services (i.e., in L1 and L2) remain sparse (Altarriba & Morier, 2006; Altarriba & Santiago-Rivera, 1994; Ateş-Barlas, 2023; Bamford, 1991; W. L. Cho et al., 2025; Costa & Dewaele, 2014; Dewaele & Costa, 2013; Miteva et al., 2022; Putzu-Williams, 2023; Santiago-Rivera & Altarriba, 2002; Santiago-Rivera et al., 2009; Sentell et al., 2007; Zamani & Kim, 2021). A limited number of studies using clinical-case vignettes, personal anecdotes, and qualitative interviews have demonstrated effects of multiple languages on emotion expression, patient-clinician relationship, and trauma (see reviews by Seto & Forth, 2020; Verkerk et al., 2023). A few culturally responsive interventions have been developed in L1 (e.g., bilingual case managers and patient materials) and used to augment treatment-as-usual practices (Haack et al., 2025; Yeung et al., 2010). When multiple languages are integrated in psychological assessment and intervention, benefits in treatment alliance, engagement (e.g., increased emotional expression and disclosure), and outcomes are observed (Dewaele & Costa, 2013; Santiago-Rivera et al., 2009; Verkerk et al., 2023).
Bilingualism, Emotion, and Symptoms: Integrating Psycholinguistic Perspectives
In the present study, we integrate psycholinguistic theories on bilingualism and emotion to inform clinical assessments. Emotions can change as a function of language. That is, language can shape emotional expression, retrieval of memories, and communication (Marian & Kaushanskaya, 2004). Psycholinguistic experimental studies have documented language-dependent emotions across various methodologies, including electrodermal activity (Caldwell-Harris & Ayçiçeği-Dinn, 2009; Harris et al., 2003), pupillometry (Iacozza et al., 2017; Thoma, 2024), event-related potential (ERP; Jończyk et al., 2016; Opitz & Degner, 2012), Stroop tasks (Sutton et al., 2007), decision-making (Hayakawa et al., 2017; Keysar et al., 2012), and self-reports (Dewaele & Costa, 2013; Pavlenko, 2012). However, some aspects of emotion, for example, emotion perception (as opposed to emotion expression), are not always found to differ across languages in bilinguals who are highly proficient in both L1 and L2 (Champoux-Larsson & Nook, 2024), suggesting that unbalanced sequential bilinguals may be more susceptible to language-dependent emotion effects. In addition to language proficiency and dominance, factors that can influence emotion perception in bilinguals include modality of emotional input (auditory or visual), input familiarity (same or different race), and cultural background and experience (P. Chen et al., 2022, 2024; Chung-Fat-Yim et al., 2022). Previous studies have generally pointed to a pattern of increased emotional reactivity and automaticity in L1 in contrast to reduced emotional reactivity and automaticity in L2 (known as the “foreign-language effect”; Hayakawa et al., 2021) for sequential bilinguals and to amplified emotional expression when speaking in the preferred language (Marian & Kaushanskaya, 2008).
A therapeutic strategy of affect labeling is commonly used in clinical practice whereby putting feelings into words can help regulate emotional reactivity (Lindquist, 2017; Torre & Lieberman, 2018). Across qualitative studies and clinical observations, higher emotional expressivity during psychotherapy in bilingual patients’ L1 has been found compared with L2 (for reviews, see Dewaele & Costa, 2013; Verkerk et al., 2023). Studies have also documented bilingual clinicians’ use of code-switching as a psychotherapeutic technique to facilitate disclosure of feelings in L1 and to avoid or distance oneself from feelings in L2 (Santiago-Rivera et al., 2009).
Several nonmutually exclusive accounts have been proposed as mechanisms for language effects on emotion in bilinguals, including language-dependent memory (Marian & Fausey, 2006; Marian & Kaushanskaya, 2004; Marian & Neisser, 2000), psychological distancing (Kross & Ayduk, 2011), emotional dampening (Caldwell-Harris & Ayçiçeği-Dinn, 2009), and cultural-frame switching (Geipel et al., 2015; Y. Hong et al., 2000). These explanations may be organized into two types: processing accounts (i.e., automaticity, accessibility, and cognitive resources needed for L1 and L2 use) and association accounts (i.e., frequency of using L1 and L2 words in specific emotional contexts over time; Thoma, 2024; Williams et al., 2020). In a study on medical decision-making, Hayakawa et al. (2022) tested both mechanisms in Chinese-English bilingual speakers with balanced language proficiency. The participants perceived medical conditions to be less physically painful and less emotionally distressing in L2 (language-processing effect; Hayakawa et al., 2017) and endorsed cultural beliefs about doctors and treatments consistent with each language and cultural frame (cultural-association effect; Y. Hong et al., 2000). Multiple and overlapping mechanisms, including the interplay between linguistic and cultural factors, influence symptom expression and medical decision-making.
Symptom-rating scales are designed to quantify the severity of a psychological condition and used to assist diagnosis, treatment planning, and progress monitoring of intervention (Baer & Blais, 2010). Although clinical scales have been normed in multiple languages (Campos & Gonçalves, 2011; García-Batista et al., 2018; González et al., 2015), few studies have tested language effects in bilingual populations. In a study with sequential Spanish-English bilinguals, language effects were observed such that greater symptoms of anxiety were reported in L1 Spanish than in L2 English on the State-Trait Anxiety Inventory (STAI; Spielberger et al., 1970) measure of anxiety (Guttfreund, 1990). Sequential Spanish-English bilingual patients with a history of childhood trauma also reported more intense symptoms of posttraumatic stress disorder in L1 Spanish compared with L2 English (Schwanberg, 2010). In a validation study of the Spanish Beck Depression Inventory (BDI-II; Birnbaum et al., 2020), Penley et al. (2003) conducted a post hoc analysis on a subset of Spanish-English-speaking adult patients. Five patients were placed into more severe depressive categories on their English BDI-II, and two patients were placed into more severe depressive categories on their Spanish BDI-II (Penley et al., 2003). In a follow-up study of Spanish-English bilingual students with balanced proficiency, however, no differences in total depression scores were found (Wiebe & Penley, 2005). Such mixed evidence across type of psychopathology (anxiety-related disorders vs. depressive mood disorder), bilingual populations (simultaneous vs. sequential), and age groups (young adulthood vs. middle to late adulthood) suggests a need for continued and careful examination of how language might alter the expression of psychological symptoms in speakers of more than one language.
Cultural Differences in Prevalence, Perception, and Symptoms
Because language and culture are intertwined, researchers and clinicians are faced with multiple cultural beliefs and practices related to psychopathology. Previous cross-cultural and cross-national studies have examined the prevalence, perception, and symptoms of psychological stress. Anxiety prevalence was found to be highest in North America and lowest in East Asia (Baxter et al. 2014). Likewise, prevalence rates of major depression in the United States and Canada were consistently higher than rates of depression in East Asian countries, including Japan (Kawakami et al., 2005). Such underestimation is in part due to higher stigma surrounding mental illness in Japan relative to Western countries (Griffiths et al., 2006). The Japanese public was found to be more reluctant to use psychiatric labels, particularly for depression, and was less likely to disclose psychological disorders with others outside the family (Jorm et al., 2005). Among individuals diagnosed with depression, patients reported varying symptom severity based on cultural group. Data from three nationwide surveys in the United States, Japan, and Taiwan revealed that the lowest overall levels of depressive symptoms were found among Japanese elderly, followed by Taiwanese, White Americans, and Black Americans (Krause & Liang, 1992). Furthermore, Japanese American elderly who identified more with the Japanese culture reported lower depressive symptoms than individuals who identified more with the American culture (Harada et al., 2012). Endorsement of anxiety symptoms also varied across racial groups in the United States such that Asian Americans consistently reported anxiety symptoms less frequently than other groups, including White Americans (Asnaani et al., 2010).
In addition to expression of symptoms, beliefs about psychological distress and well-being differ across Japanese and American cultural contexts (Ryff et al., 2014). Medical anthropologists have documented somatization of psychological symptoms in East Asian groups (Kleinman, 1982). More recent work has suggested that such somatization could be understood as a cultural script, and critically, the Eastern cultural emphasis on somatization contrasts the Western cultural emphasis on psychologization (Ryder & Chentsova-Dutton, 2012).
Moreover, treatment preferences and selections differ across health-care systems and cultural contexts (e.g., psychotherapy and behavioral activation as first-line treatment in the United States in contrast to pharmacotherapy and physical rest in Japan; Nakagawa et al., 2015; Williams et al., 2016). Psychological-treatment approaches in the United States highlight the experience of emotional distress and how it is influenced by patterns of thoughts and behaviors (Ryff et al., 2014), as exemplified by Beck’s cognitive model (Beck & Haigh, 2014). Japanese psychological-treatment approaches, in contrast, teach patients to accept emotions and thoughts as transitory and not conducive to conscious control (Ryff et al., 2014). For instance, silent (i.e., nonverbal) introspection and physical rest are important components of healing in Morita’s (1998) therapy, Naikan therapy (Kawahara, 2005), and Kasahara’s (2007) psychotherapy practiced in Japan. The cross-cultural and cross-national studies conducted to date suggest that in Eastern and Western societies, particularly Japanese and American, anxiety and depression may be conceptualized differently and likely require culturally responsive approaches to care.
The Present Study
In the present study, we examined how languages influence expression of anxiety and depression symptoms in sequential Japanese-English bilinguals. Specifically, we tested whether and how the L1 Japanese and L2 English influenced symptom expression using a widely adopted clinical rating scale (STAI and BDI-II). Building on previous studies (Guttfreund, 1990; Penley et al., 2003; Schwanberg, 2010; Wiebe & Penley, 2005), we used a within-persons design in which each participant completed the rating scale in both L1 Japanese and L2 English across two online sessions in counterbalanced order. Middle- and older-age bilingual adults (i.e., 40 years and older) were selected because they are more likely to separate their L1 and L2 use across contexts (Schrauf, 2009). Moreover, the middle- to older-age Japanese-speaking community in the United States is critically underrepresented in clinical research and practice. Asian American Pacific Islander (AAPI) communities show persistently low mental-health-service utilization even among racial and ethnic minorities (Chung et al., 2024; Cook et al., 2017; Đoàn et al., 2019). Our study focused on a single ethnic group (i.e., Japanese) to reduce the bias that the AAPI community is monolithic and document the heterogeneity within AAPI subgroups (Gong & Xu, 2021).
We empirically tested the hypothesis of language-dependent symptom expression in Japanese-English bilinguals. Given the literature demonstrating increased emotional reactivity in L1 and decreased emotional reactivity in L2, we predicted a difference in L1 and L2 reporting of symptoms such that symptoms will be reported as greater in L1 than in L2. That is, total anxiety- and depression-symptoms scores would be higher in L1 Japanese than in L2 English for Japanese-English bilinguals. Considering that Japanese cultural norms and values emphasize moderation of independent expression (Kitayama et al., 2010; Markus & Kitayama, 2010), we also tested the moderating effects of Japanese and American cultural contexts.
Transparency and Openness
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. The data code is available on OSF at https://osf.io/2kjtm/?view_only=89d5b1950e654214b85c6e331a95caf7. The protocol was approved by the Institutional Review Board and carried out in accordance with the provisions of the World Medical Association Declaration of Helsinki.
Method
Participants
Various recruitment methods were used to increase participation and engagement among older AAPI communities (Cook et al., 2017; Đoàn et al., 2019). We contacted and distributed recruitment emails and fliers through listservs and webpages of Japanese community centers (65 community centers across 35 states), Japanese heritage language schools (66 schools across 32 states), programs for Japanese seniors (e.g., Kimochi, Inc.; Keiro), Japanese grocery stores (e.g., Mitsuwa Marketplace, Nijiya Market, Weee!), health-advocacy groups (e.g., FLAT JP, Center for Japanese Mental Health), and faith-based organizations (e.g., Japanese Christian churches). A national registry, the University of California San Francisco Collaborative Approach for Asian Americans, Native Hawaiians, & Pacific Islanders Research & Education, was also used. All recruitment materials were provided in Japanese and English.
Participants completed the experiment online using Qualtrics and were prescreened to ensure that they (a) were 40 years and older, (b) learned Japanese as a first language, (c) learned English as a second language, and (d) were residing in the United States at the time of the study. Only participants who rated their overall proficiency in both Japanese and English as 3 (fair) or greater on a scale from 0 (none) to 10 (perfect) on the Language Experience and Proficiency Questionnaire (LEAP-Q; Marian et al., 2007) were included. A total of 249 participants were prescreened, and 60 did not meet the above criteria (six participants were under age 40, two did not live in the United States, 16 did not select speaking both Japanese and English, five did not pass cutoff score for self-reported proficiency in English, nine did not complete prescreening survey, 21 did not provide consent, and one declined consent).
A total of 189 Japanese-English sequential bilingual speakers (female: n = 167; male: n = 20; nonbinary: n = 2; age: M = 54.83 years, SD = 10.42, range = 40–91; education: M = 16.74 years, SD = 3.40) ages 40 and older completed the initial screening and consent in Japanese or English. Each participant completed the anxiety- and depression-symptom rating scales in Japanese and English across two consecutive days; order of testing language was counterbalanced across participants. The STAI and BDI-II were presented in Japanese or English via visual and audio modalities depending on the language condition (i.e., participants read items in Japanese and listened to Japanese narration of the items in the Japanese condition; participants read items in English and listened to English narration of the items in the English condition). Online text-to-speech software TTSMaker was used to standardize the audio recordings. The first and second surveys were completed in approximately 35 to 45 minutes and 18 to 28 minutes, respectively. The study protocol was approved by the Northwestern University Institutional Review Board.
The final sample consisted of 164 Japanese-English sequential bilingual speakers (female: n = 144; male: n = 18; nonbinary: n = 2; age: M = 55.15 years, SD = 10.55, range = 40–91; education: M = 16.72 years, SD = 3.41). Out of the 189 participants who completed the prescreening and consent process, 25 were removed from data analyses (one participant completed the survey twice, one reported Japanese as their fourth language on the LEAP-Q, and 23 did not start the mental-health survey). Relatively high rates of dropout (13.2%) in this group reflected the low mental-health-service utilization among minoritized AAPI individuals (Olfson et al., 2009; Presley & Day, 2019). For the language characteristics of study participants, see Table 1. Participants acquired Japanese first (around 6 months of age) and English second (around age 12; i.e., sequential bilinguals) and reported higher proficiency in Japanese than in English. Participants had comparable exposure to Japanese and English across all contexts (i.e., family, reading, language apps, TV) except friends and radio/music, for which, participants had higher exposure to English. Participants overall had spent more years immersed in Japanese-language environments (i.e., country, family, school/work) compared with English-language environments.
Linguistic Profile of Japanese-English Sequential Bilinguals
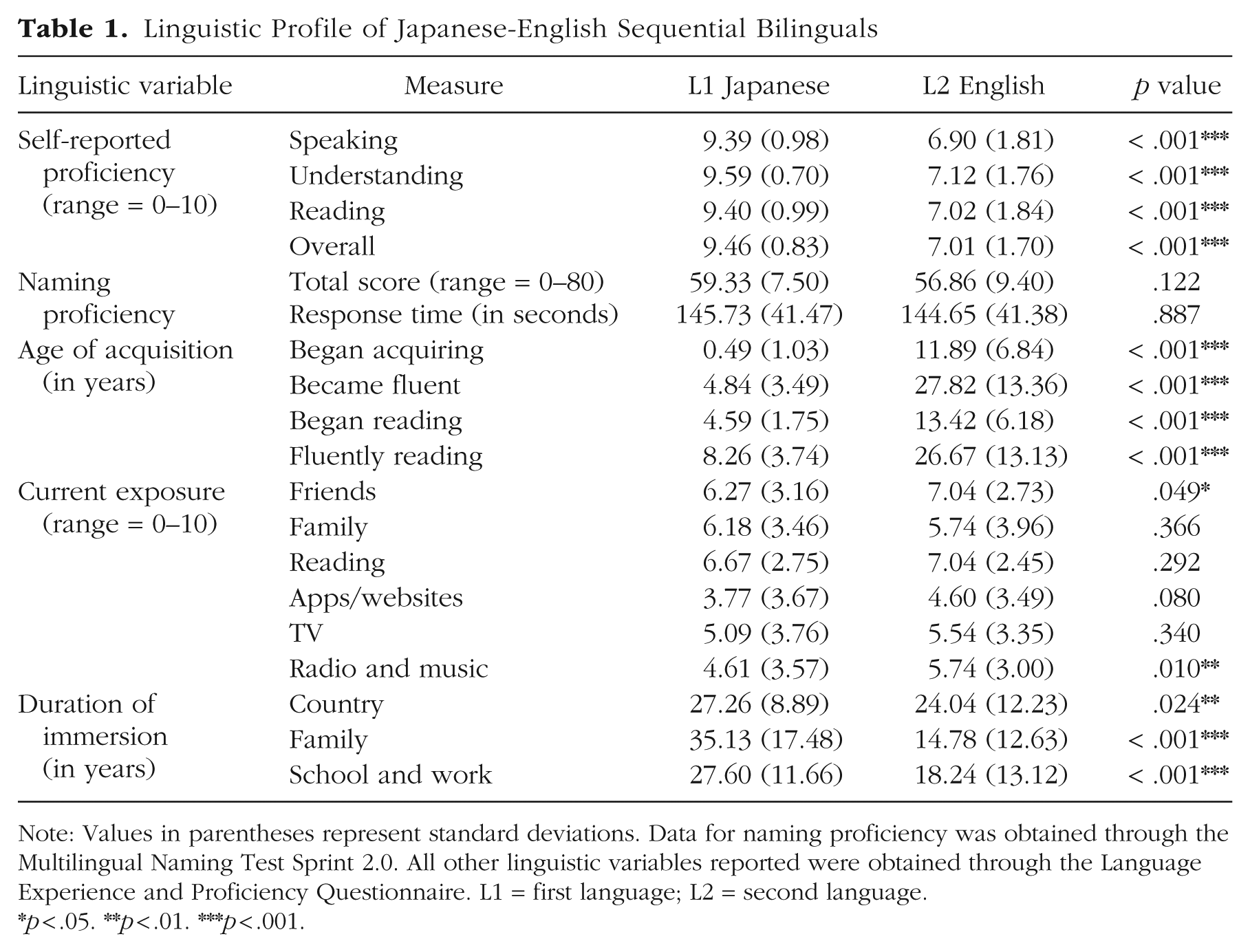
Note: Values in parentheses represent standard deviations. Data for naming proficiency was obtained through the Multilingual Naming Test Sprint 2.0. All other linguistic variables reported were obtained through the Language Experience and Proficiency Questionnaire. L1 = first language; L2 = second language.
p < .05. **p < .01. ***p < .001.
Measures
Anxiety symptoms
The Spielberger STAI for Adults (Spielberger et al., 1970) is a 20-item self-report scale of state- and trait-level anxiety. In the present study, we focused on state-level anxiety (i.e., how one is feeling right now). This measure is often administered in outpatient clinic settings and takes approximately 5 min to complete. Each STAI item (e.g., tense, calm, upset, worried, nervous, pleasant) is given a weighted score of 1 to 4. The total anxiety score ranges from 0 to 80. The Japanese version of the STAI has been translated by clinical researchers and used in clinical and nonclinical populations (Iwata, Mishima, et al., 1998, 2000). The correlation coefficients for the STAI in the current sample indicated excellent consistency (STAI Japanese version: Cronbach’s α = .93; STAI English version: Cronbach’s α = .94).
Depression symptoms
The BDI-II (Beck et al., 1996) is a 21-item self-report inventory used to measure depression severity and symptoms. The measure is often administered in outpatient clinic settings and takes approximately 5 to 10 min to complete. Each item is scored on a scale from 0 to 3. The total score ranges from 0 to 63, indicating four levels of depression severity (0–13 = minimal, 14–19 = mild, 20–28 = moderate, 29–63 = severe). The Japanese version of the BDI-II has been validated and used in Japan (Kojima et al., 2002). The correlation coefficients for the BDI-II in the current sample demonstrated excellent consistency (BDI-II Japanese version: Cronbach’s α = .89; BDI-II English version: Cronbach’s α = .89).
Depression is a major risk factor for suicide. BDI-II Item 9 assesses the severity of suicidal thoughts (0 = I don’t have any thoughts of killing myself; 1 = I have thoughts of killing myself, but I would not carry them out; 2 = I would like to kill myself; 3 = I would kill myself if I had the chance); higher scores indicate greater suicidal intent. The BDI-II suicide item has been found to significantly predict both deaths by suicide and repeated attempts; each successive cutoff score confers greater risk (K. L. Green et al., 2015). In clinical practice, it is recommended that a cutoff score of 1 or above triggers suicide-risk assessment and that careful attention be given to patients who endorse at or above a 2 on the item. All study participants who endorsed 1 or higher on BDI-II Item 9 received a phone or email contact within 24 hr, and individuals who were reached completed suicide-risk-assessment interviews in Japanese and English with a bilingual clinical psychologist.
LEAP-Q
The LEAP-Q is a validated questionnaire used to collect information about self-reported proficiency and experience from bilingual speakers (Marian et al., 2007). The questionnaire measures multiple facets of bilingual status, including language competence (proficiency, dominance, preference), age and modes of language acquisition, language exposure, current language use, and cultural identity. In addition, demographic information is collected from each participant, including their age, race, gender, and educational levels.
Multilingual Naming Test Sprint 2.0
Bilingual language proficiency was assessed using the Multilingual Naming Test Sprint 2.0 (MINT Sprint 2.0), which has been adapted in multiple languages, including Spanish, Chinese, and Hebrew (Gollan et al., 2024). Participants are presented with eight rows of 10 colored pictures of objects in order of increasing difficulty and instructed to name as many pictures as possible in 3 min. Scores for the MINT Sprint 2.0 are obtained by computing the number of correct responses and the total time to name all the items. We adapted the Japanese version of the MINT Sprint 2.0 for the present study. All English instructions were translated into Japanese and back-translated. A total of 15 items that were cognates or English loanwords (e.g., ドア, pronounced do-ah for door) was replaced with Japanese items of similar frequency (NINJAL-LWP, National Institute for Japanese Language and Linguistics, 2021; SUBTLEXUS, Brysbaert & New, 2009), concreteness (Scott et al., 2019), and phonetic length (e.g., 門, or gate). The Japanese version of the MINT Sprint 2.0 was piloted online with 10 Japanese-English bilingual speakers living in the United States. The pilot test was found to be feasible (i.e., all participants were able to complete the Japanese version of the MINT Sprint 2.0 within 3 min, as instructed) and acceptable (i.e., first pass score was on average 72 points, comparable with the 74 points in control subjects on the English version of MINT Sprint 2.0; Gollan et al., 2024).
Data analysis
Based on recommended cutoffs of 2 and 7 for skewness and kurtosis, all main variables from the STAI and BDI-II were tested for normality (West et al., 1995). Positive skews were found on total symptoms of anxiety and depression, which were expected given that assessments were conducted on a healthy population. Residuals of linear mixed-effects models were found to be normally distributed. To test the hypothesis that language predicts symptom expression, multilevel modeling was conducted considering the nested effects of repeated measures (i.e., first and second surveys). Random intercepts were used for the within-persons analysis. Order effects were treated as a covariate. The false-discovery-rate corrections were used to account for multiple comparisons. All analyses were conducted using the linear and nonlinear mixed effects models package (nlme; Pinheiro et al., 2023) and linear mixed effects models using Eigen and SE packages (lme4; Bates et al., 2015) in R (R Core Team, 2023).
In the first level (Level 1) within-persons analysis, we predicted that language (L1 Japanese or L2 English) would influence psychological symptoms while controlling for order effects. In the second level (Level 2) between-persons analysis, we tested whether the effect of language was moderated by language characteristics. The models are specified as follows:
Level 1:

Level 2:

where SYMPTOMij is the observed total symptom score at survey-response i for person j. β0j is the intercept, β1j is the effect of L1 or L2 on symptoms, and β2j is the ordering effect of first and second surveys. γ 10 is the effect of a given participant’s language characteristic reported on the first survey. γ00 is the main effect of L1 or L2 on symptoms. γ0m is the effect of language characteristics that influence the effect of language on symptoms (i.e., moderator).
In addition, a person-centered latent-profile-analysis (LPA) approach was used to identify language profiles in bilinguals (Su et al., 2022; Yang et al., 2024). Capturing language heterogeneity in bilingual groups is important (Marian & Hayakawa, 2021), and LPA is especially suitable for testing the presence of latent subgroups or profiles. Duration of immersion in various language environments was selected for analysis because of greatest variability in the current sample (Table 1).
Results
Bilingual-language effects on anxiety
Japanese-English bilinguals showed a cross-linguistic difference in the expression of anxiety symptoms. Specifically, bilinguals reported higher total symptoms of state-level anxiety in L1 Japanese than in L2 English, B = −2.37, SE = 0.72, β = −0.23, t(103.08) = −3.29, p = .001, with survey order and nested effects accounted for. For the box plot and the paired-scores plot of the STAI total scores in Japanese and English, see Figure 1.
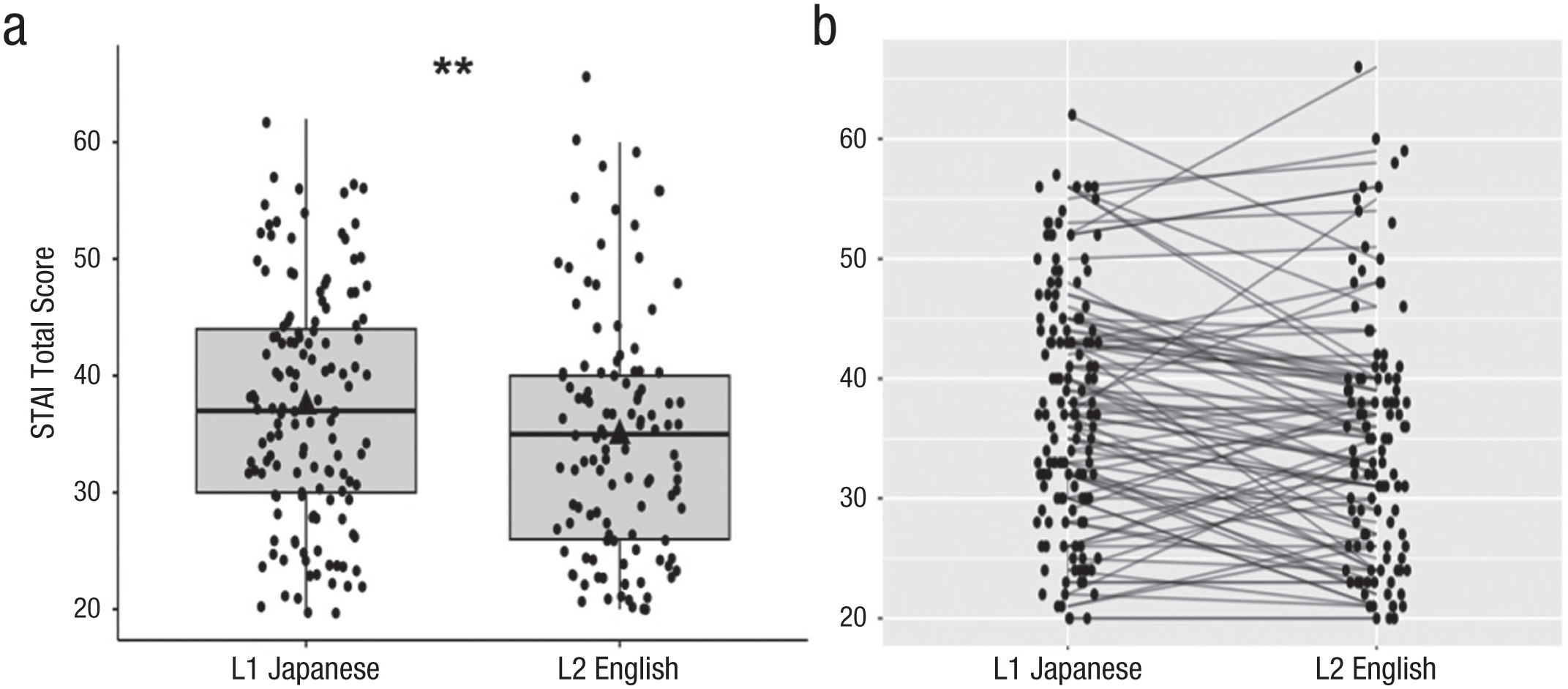
State Trait Anxiety Inventory (STAI) total score showing higher anxiety symptoms in L1 Japanese than in L2 English. (a) Each box represents the interquartile range for that condition; the horizontal line in each box represents the median. Dots represent individual participants. The black triangle represents the mean total score for each condition. (b) Each horizontal line connects each individual participant’s STAI total score in L1 Japanese and L2 English. L1 = first language; L2 = second language. Asterisks represent significance at p < .01.
Item-level analyses using linear mixed-effects models controlling for survey order and nested effects (see Table 2) revealed that the following symptoms were rated higher in L1 Japanese than in L2 English on the STAI: calm (Item 1), secure (Item 2), at ease (Item 5), frightened (Item 9), comfortable (Item 10), self-confident (Item 11), relaxed (Item 15), content (Item 16), steady (Item 19), and pleasant (Item 20). On the other hand, the following symptoms were higher in L2 English than in L1 Japanese: tense (Item 3), upset (Item 6), indecisive (Item 14), and confused (Item 18). For corrected and uncorrected p values based on group-mean comparisons, see the Supplemental Material available online.
State Trait Anxiety Inventory Responses of Japanese-English Sequential Bilinguals
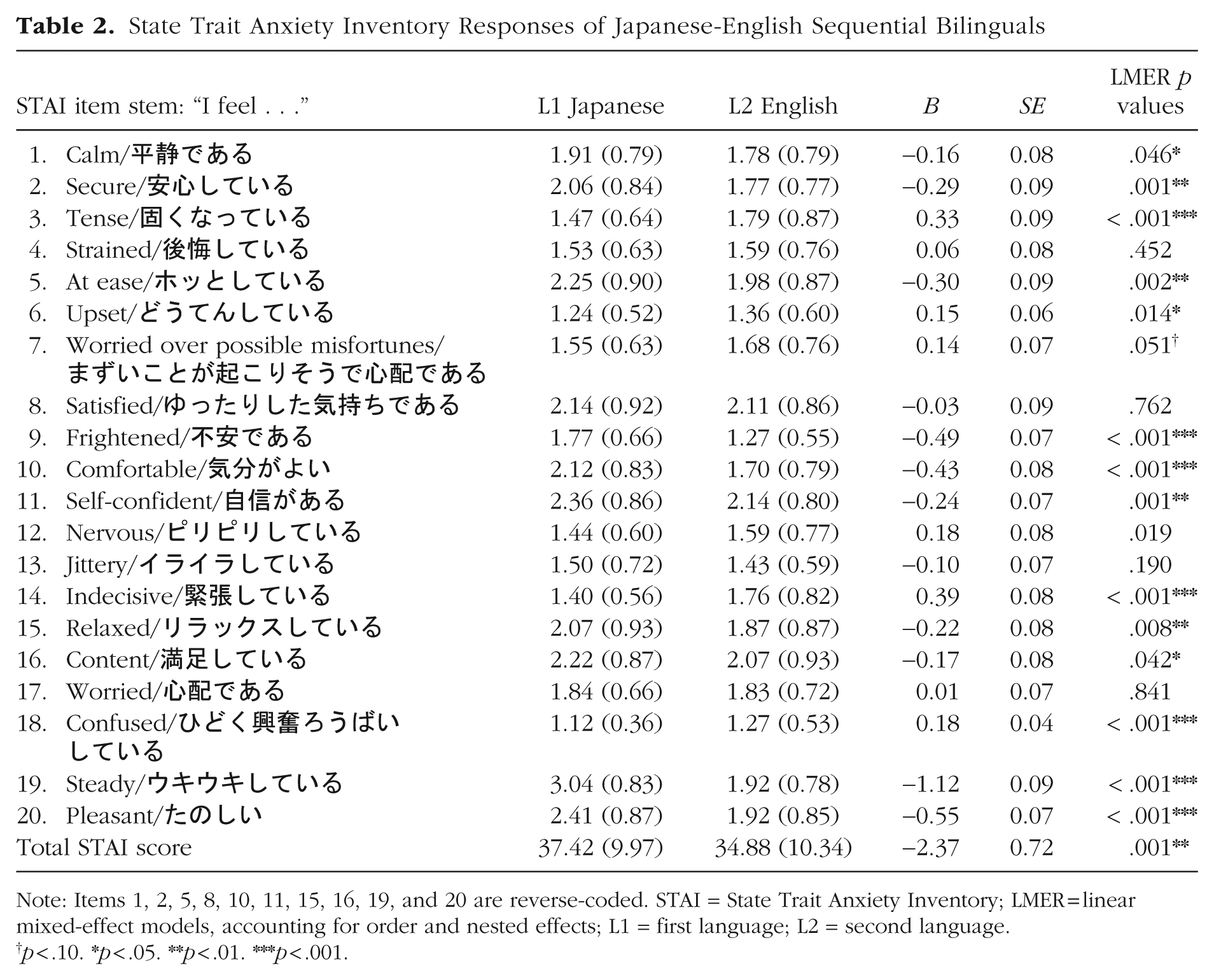
Note: Items 1, 2, 5, 8, 10, 11, 15, 16, 19, and 20 are reverse-coded. STAI = State Trait Anxiety Inventory; LMER = linear mixed-effect models, accounting for order and nested effects; L1 = first language; L2 = second language.
p < .10. *p < .05. **p < .01. ***p < .001.
Bilingual-language effects on depression and suicidal thoughts
BDI-II total scores were found to be similar across L1 Japanese and L2 English, B = −0.34, SE = 0.44, β = −0.04, t(95.85) = −0.77, p = .44. Two-factor approaches to BDI-II used in previous studies (Steer et al., 1999) have yielded two symptom clusters: cognitive and somatic-affective. The cognitive items include sadness (Item 1), pessimism (Item 2), guilty feelings (Item 5), punishment feelings (Item 6), self-criticalness (Item 8), and worthlessness (Item 14). The somatic-affective items include loss of energy (Item 15), changes in appetite (Item 18), tiredness and fatigue (Item 20), and loss of interest in sex (Item 21). Cognitive symptoms of depression (Cronbach’s α = .83) were significantly higher in L1 Japanese than in L2 English, B = −0.65, SE = 0.25, β = −0.17, t(100.57) = −2.60, p = .011. On the other hand, somatic-affective symptoms (Cronbach’s α = .79) did not differ by language, p = .23.
There was a cross-linguistic difference in the severity of suicidal thoughts as measured by BDI-II Item 9. The severity of suicidal thoughts was positively predicted by BDI-II total scores, B = 0.03, SE = 0.004, t(201.22) = 7.41, p < .001. Bilingual participants reported higher severity of suicidal thoughts in L1 Japanese than in L2 English, B = −0.14, β = −0.27, SE = 0.04, t(95.12) = −3.25, p = .002.
Additional item-level analyses using linear mixed-effects models accounting for survey order and nested effects (see Table 3) showed that feelings of sadness (e.g., “I feel sad much of the time”), B = −0.27, SE = 0.05, β = −0.47, t(119.03) = −4.95, p < .001; crying (e.g., “I feel like crying, but I can’t”), B = −0.32, SE = 0.06, β = −0.44, t(116.95) = −5.01, p < .001; and loss of interest in sex (e.g., “I am less interested in sex than I used to be”), B = −0.14, SE = 0.07, β = −0.13, t(99.14) = −2.07, p = .04, were expressed as higher in L1 Japanese than in L2 English. Past failure (e.g., “As I look back on my life, all I can see is a lot of failures”), B = 0.18, SE = .07, β = 0.26, t(115.40) = 2.63, p = .01, and changes in sleeping pattern (e.g., “I wake up 1–2 hours earlier than usual and find it hard to get back to sleep”), B = 0.61, SE = .13, β = 0.47, t(126.08) = 4.68, p < .001, were reported higher in L2 English than in L1 Japanese. For corrected and uncorrected p values based on group-mean comparisons, see the Supplemental Material.
Beck Depression Inventory Responses of Japanese-English Sequential Bilinguals
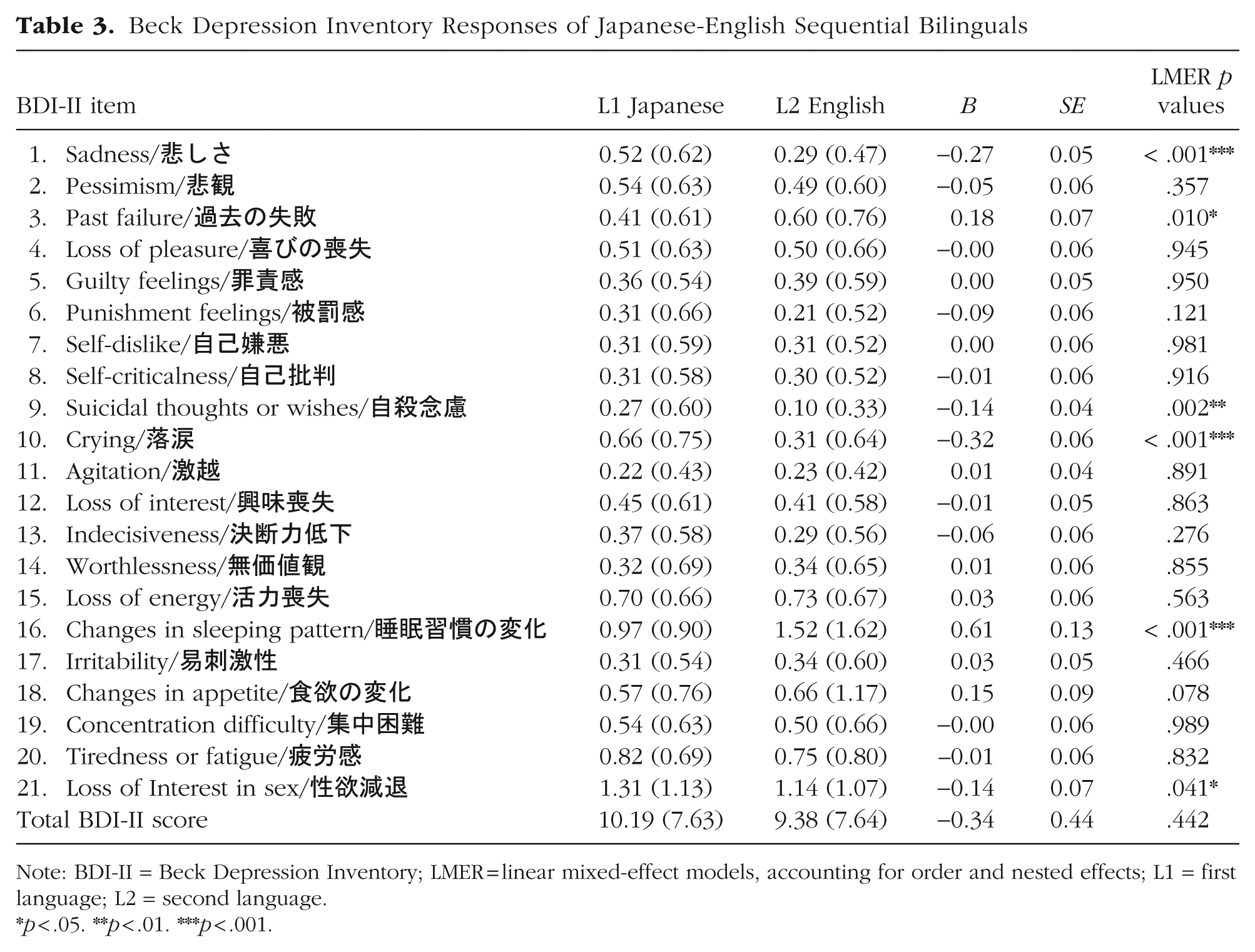
Note: BDI-II = Beck Depression Inventory; LMER = linear mixed-effect models, accounting for order and nested effects; L1 = first language; L2 = second language.
p < .05. **p < .01. ***p < .001.
LPAs of anxiety and depression symptoms in bilinguals
To account for within-groups heterogeneity, LPAs were conducted to understand the presence of subgroups or profiles in our bilingual population. The LPA revealed a two-profile solution in the current sample of Japanese-English bilinguals based on the Sample-Size Adjusted Bayseian Information Criterion (SABIC) and Lo-Mendell-Rubin Likelihood Ratio Test (LMR-LRT) model-fit summary (SABIC = −280.54, entropy = .87, LMR-LRT = .016; Fig. 2). The entropy value (.87) indicated good confidence in group classification. A three-profile solution was not selected because it included a profile that comprised 11 individuals (10%), which may be underpowered for subsequent analysis. The nonsignificant value from the LMR-LRT suggests that the three-profile solution does not provide significantly better fit than the two-profile solution (for model-fit comparisons, see the Supplemental Material).
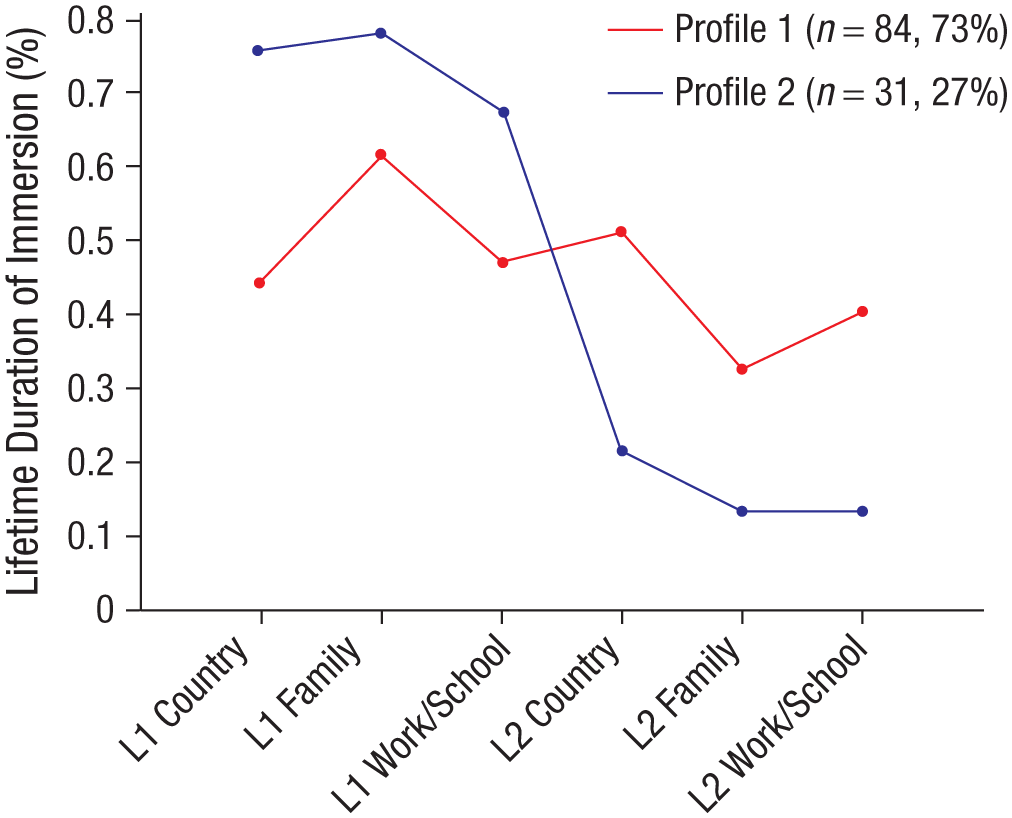
Latent-profile analyses of bilingual participants showing distinct balanced (Japanese and English) and Japanese-dominant language-environment profiles. Proportion of lifetime years immersed in L1 Japanese and L2 English environments. L1 = first language; L2 = second language.
Profile 1, “balanced language environment,” included 84 bilinguals (73%) who have spent approximately half of their life in Japanese-speaking (see Fig. 2, 0.44) and English-speaking (0.51) countries. These bilinguals have a relatively balanced proportion of their lifetime spent in Japanese-speaking (family: 0.62; school or work: 0.47) and English-speaking (family: 0.32; school or work: 0.40) settings. Profile 2, “Japanese-dominant language environment,” included 31 bilinguals (27%) who have spent a greater proportion of their lifetime in Japanese-speaking country (0.76), family (0.78), and school or work (0.67) settings than in English-speaking country (0.21), family (0.14), and school or work (0.14) settings.
Bilinguals typed as Profile 1, balanced language environment, endorsed more bicultural or multicultural identity compared with bilinguals typed as Profile 2, Japanese-dominant language environment (Profile 1: M = 1.71; Profile 2: M = 1.25), t(67.85) = 4.19, p < .001. Correspondingly, bilinguals typed as Profile 1, balanced language environment, were older (Profile 1: M = 56.43 years; Profile 2: M = 47.68 years), t(63.55) = 5.06, p < .001, and had higher self-reported English proficiency (Profile 1: M = 7.33; Profile 2: M = 6.29), t(54.89) = 3.06, p < .01, and lower self-reported Japanese proficiency (Profile 1: M = 9.39; Profile 2: M = 9.77), t(107.07) = −3.23, p < .01, compared with bilinguals in Profile 2, Japanese-dominant language environment. Differences across profiles were not found on the age of Japanese and English acquisition, ps > .08. The bicultural bilinguals who have lived in relatively more balanced Japanese and English language environments (Profile 1) had higher STAI total-difference scores (Fig. 3a) and higher BDI-II total-difference scores (Fig. 3b) than the monocultural bilinguals who have lived in a relatively more Japanese-dominant environment throughout their life (Profile 2). Subgroup membership predicted total-score differences between Japanese and English scales for anxiety symptoms, B = −2.54, SE = 1.05, β = −0.27, t(78) = −2.45, p = .017, and depression symptoms, B = −1.54, SE = 0.76, β = −0.23, t(78) = −2.04, p = .045.
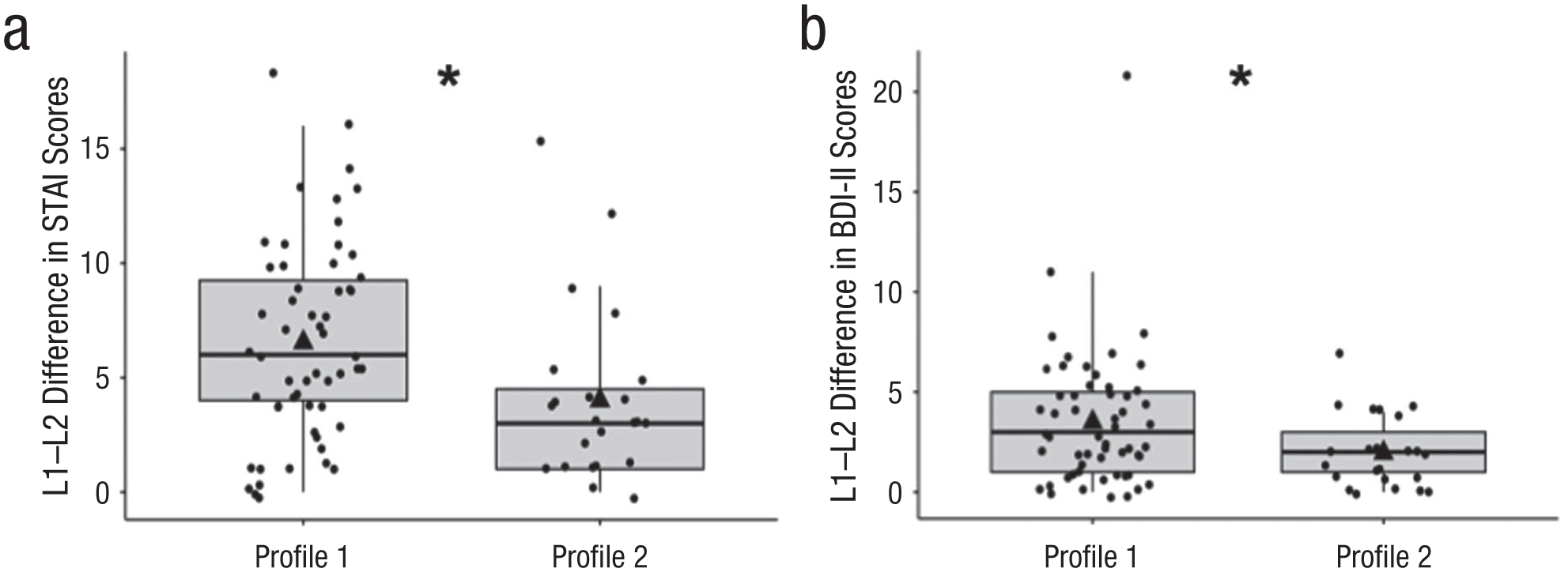
Total difference scores on the STAI and BDI-II showing higher total difference scores for balanced bilinguals (Profile 1) than Japanese-dominant bilinguals (Profile 2). (a) Cross-linguistic differences in STAI total state-anxiety scores. (b) Cross-linguistic differences in BDI-II total depression scores across Profile 1, balanced language environment, and Profile 2, Japanese-dominant language environment profiles. Each box represents the interquartile range for that profile; the horizontal line in each box represents the median. Dots represent individual participants. The black triangle represents the mean total-difference score for each profile. STAI = State-Trait Anxiety Inventory; BID-II = Beck Depression Inventory. Asterisk indicates significance at p < .05.
Qualitative-content analysis
Of the 32 participants who scored 1 or higher on the Japanese or English BDI-II suicide item, 8 individuals completed risk-assessment phone interviews (range = 20 min–1 hr) with a Japanese-English bilingual clinical psychologist. The participants varied in age (50s, 60s, and 70s), gender (female-identifying: n = 7; male-identifying: n = 1), geographical location in the United States (Connecticut, Illinois, New York, North Carolina, Virginia), occupation (homemaker, self-employed business owner, translator, school superintendent, neuroscientist, airlines executive secretary, babysitter, retiree), and mental-health history (anxiety, depression, obsessive compulsive disorder, attempted suicide, or no psychiatric history). This subgroup did not differ from the full sample in age, gender, levels of language proficiency, or age of acquisition (p > .40).
We identified five overarching themes capturing Japanese-English bilinguals’ experiences with language, emotion, and mental-health services. The themes derived from conventional content analysis (Hsieh & Shannon, 2005) are as follows: (a) bilingual emotion and symptom expression, (b) limits of English-only mental-health services, (c) need to integrate Japanese in mental-health services, (d) aging and end-of-life concerns, and (e) immigrant experience. We discuss the themes and subthemes below and include direct quotes.
Theme 1: bilingual emotion and symptom expression
Although participants were invited to conduct the interview in Japanese, English, or both, almost all interviews were carried out in Japanese with some code-switches into English. Japanese emotion words that involved the body part heart were frequently used (“my heart is not sunny”「心が晴れない」; “echoed in my heart”「心に響く」; “my heart felt strong”「心強い」). Suicidal expressions were described in Japanese (“I hate everything”「全てが嫌になる」; “I hate everything. Let’s quit.「全てが嫌、もうやめちゃお」). A few participants code-switched between Japanese and English as if strategically using each language and associated cultural rules about emotion to manage their symptoms: Maybe it’s cultural? In Japanese, it’s not rude to say negative things, like “Did you get skinnier? Did you gain weight?” or “I am just so tired of all of this” as a way to vent and empathize or connect with each other. When I feel depressed, I try to look at the “bright side.” In English, it’s all positive thinking for me. Basically, I don’t find negatives in myself.
It is possible that bilinguals may more easily access their emotional distress in L1 Japanese and deliberately process the emotional experience in L2 English to reduce negative thought patterns or feelings that contribute to psychological distress.
Theme 2: limits of English-only mental-health services
Participants unanimously described language barriers when facing English-only mental-health services. Many individuals noted the difficulty of communicating their feelings in L2 English, as described below: Despite my profession as a translator and my proficiency in English, I feel that it’s a high hurdle to describe my own depression in English [italics added]. I have never sought therapy or mental health providers before. I wonder, “How much can I communicate?” “Will they understand what I am feeling?” I would continue to experience doki-doki [sound of heart palpitations] along with dizziness, resulting in inability to get in a car or stand on some days. I was recommended therapy and I attended one or two sessions. American therapists were validating and good at listening, but offered no practical, concrete solutions. I also felt a language barrier, it felt difficult to communicate nuanced feelings in English. I felt that it would be especially hard to communicate my feelings or reach out in English when I am feeling down [italics added]. I experienced a dip in mood 4–5 years ago and started having suicidal thoughts. I hated all of it and wanted to quit on life. I was alarmed and went to 10 free sessions provided by work in English. It was nice to have a social worker draw out stories and difficult feelings that I can’t share with people who are close to me. But maybe it’s a fit or time or something, there’s always a stopper. It’s almost like there is a plug when speaking in English and I cannot bare my heart open [italics added].
Emotional symptoms may be muted in L2 because cognitive processing is less automatic and more effortful, particularly under the conditions of anxiety or depressive mood. The Japanese-English bilinguals described translation nonequivalence and limits of articulating their feelings and symptoms in English, and this was true even for individuals who were highly proficient in English (e.g., professional translator). The barriers that result from limited ability to express one’s full range of emotions in a monolingual health-service context appear to reduce help-seeking behaviors and lead to early dropout from treatment.
Theme 3: need to integrate Japanese into mental-health services
Across acculturative levels and varied mental-health-service-use history, all bilingual participants voiced a need to integrate the Japanese language into their psychological care. One participant described the acceptance and understanding of a diagnosis when described in L1 Japanese in contrast to L2 English: Though my obsessive compulsive disorder diagnosis has been explained to me in English, the English description of “perfection” never matched my experiences. Only 3 years ago, when I received treatment in Japanese through telehealth services, I fully understood my diagnosis. It was as if someone opened my eyes, it was a big step forward for me. . . . I felt lighter. To be able to express myself in Japanese, and to have another person listen.
The use of one’s first language appears to foster emotional processing and social connection that increases coping and reduces psychological distress: A few years ago, I participated in a research study that focused on talking about mental health challenges in Japanese communities. The theme was “while we work hard to live this positive American lifestyle and appear well, our mental health are suffering.” Though the staff abruptly discontinued after two to three sessions, our group of three to four Japanese women continued to meet weekly on our own. This saved my life. During my depression, my coping is to shut out English. I immerse myself in Japanese language—like watching owarai comedy on YouTube—to survive. It creates distance from my English-speaking husband and children, but it makes my heart lighter and gradually lifts me out of my depression.
Even for individuals who are highly acculturated and have high English abilities, speaking in their first language, Japanese, is closely related to expressions of bicultural identity and belonging: Of course there is a language handicap, but even more so, though I have been living in the US for 30 years, it made me realize that I am Japanese. I am adjusted to both Japanese and American cultures, and need both. But there are times when I hate America and I hate Japan and I don’t belong to either. When I am feeling good, it’s like having two swords.
Theme 4: bilingual immigrant experiences
These language-emotion links and their applications to mental-health services are further contextualized by the bilingual participants’ immigrant experiences. Minority stress, mistrust of medical mental-health providers, and missing their home country were subthemes that contribute to the psychological health of these older Japanese-English bilingual women: Ever since immigrating to the US about 25 years ago, I have experienced bouts of depression every 2–3 years. I do not talk about or share these concerns with others. I have never sought mental health support. I lost my niece to suicide after years of my sister taking her to psychiatrists and counselors here. My beloved niece always told me that counseling never helped. I like to figure things out on my own. I worry a lot about the future of Japan and the young people there. I feel that I may be more helpful returning to Japan, maybe I can teach or something, or contribute to society. I might be selfish or lacking confidence in my life decisions [spoken in Japanese], but I also enjoy my freedom and peaceful life in the US [spoken in English].
Theme 5: aging and end-of-life concerns
Finally, Japanese-English bilingual participants who are in their 70s described how the comforts and discomforts of language and cultural practices shaped their daily living, including housing, food, and declining physical health: I am currently separated from my spouse, who did not want to be at an English-only senior living home. So, I am on my own. There are many seniors around me who struggle with language and food as they get older, you know, in their 70s and 80s. These are folks who have lived in America for decades. But you start to forget your English, and it becomes easier to speak Japanese and you just want to eat your miso-soup and rice, isn’t that funny?
Subthemes of both ikigai (a purpose for living) and suicide (intentionally causing one’s own death) were found: I am grateful; I have lived doing the things that I like. Of course, I have had failures—separation from my spouse, and another divorce—but I am at peace with these things. I am thankful for my life and want to end it that way. I would like to have the option of suicide when the time comes. I try very hard to lead an active lifestyle and think about how best to live a meaningful life. But I know my mind and body are deteriorating and want to accept the reality of death. I’ve experienced a few disappointments since retiring. . . . I would like to live with ikigai [purpose], but I feel that my activities might be a burden to the younger generation. I wish for pin pin korori [live fully and go quickly when it is time].
These Japanese-English bilingual seniors appeared to be balancing their declining physical and cognitive health, postretirement challenges, past failures, and sense of burden to society along with respect for family, gratitude, and how to live and die well with dignity.
Discussion
In the present study, we examined the influence of bilingualism on symptom expression in middle- to older-age Japanese-English speakers living in the United States. Expression of anxiety and depression symptoms differed as a function of language. Specifically, Japanese-English bilinguals reported higher anxiety symptoms in their L1 Japanese compared with L2 English. Similar cross-linguistic differences were found in cognitive but not somatic-affective symptoms of depression and in suicidal thoughts. Furthermore, bicultural identity, as shaped by years of language immersion throughout life, moderated the effect of language on anxiety and depression. These results suggest language-dependent symptom expression in bilinguals and demonstrate the linguistic and cultural influences on psychological health.
In our study, we applied theories and experimental paradigms from laboratory-based psycholinguistic studies in a mental-health-assessment context. Previous research has shown that negative emotion words (e.g., “sadness,” “shame”) elicited different emotional responses in bilingual speakers depending on whether the words were presented in one’s L1 or L2 (Caldwell-Harris & Ayçiçeği-Dinn, 2009). Congruent with this pattern, the language of assessment in the present work affected bilinguals’ expression of anxiety symptoms, particularly their total anxiety scores and ratings on items that included words related to feelings (e.g., “frightened,” “relaxed,” and “content”). However, also consistent with previous findings (Wiebe & Penley, 2005), we did not observe cross-linguistic differences in the total depression scores on the BDI-II, which measures depressive moods. Because anxiety and depression differ in time course (e.g., Larson et al., 2007), it may be that language affects expression of psychological conditions and symptoms that unfold over shorter time spans (e.g., state anxiety) more than expression of prolonged moods (e.g., depression). Although there was no cross-linguistic difference in total depression scores, cross-linguistic differences were found on the BDI-II cognitive factor, which consists of emotion words (e.g., “guilty feelings,” “punishment feelings,” “worthlessness”) that refer to internal feeling states (e.g., “I feel utterly worthless”). Opposite effects (i.e., higher symptom expression in L2 English) were found for BDI-II items that reference a time frame in the past (e.g., “I sleep a lot more than usual”) or trait-level characteristics (e.g., “I feel I am a total failure as a person”). These item-specific patterns suggest that linguistic influences on expression of psychological distress may be greater for state-level symptoms than persistent mood or trait-level characteristics in bilingual individuals.
Our findings also suggest the role of cultural frame switching in bilingual mental health (Y. Hong et al., 2000) in which different languages prime and activate distinct cultural expressions of symptoms. Western cultures, such as the United States, value autonomy and independence, whereas Eastern cultures, such as Japan, value interpersonal relationships, group conformity, and moderation of self-expression—especially for women (Kitayama et al., 2000, 2010; Markus & Kitayama, 2010). These cultural perspectives of the self can result in distinct emotion-regulation goals (Mauss & Butler, 2010; J. L. Tsai, 2007). In English, bilinguals may be more likely to maximize or savor positive emotions—a tendency known as “hedonic emotion regulation” (Miyamoto et al., 2014). In contrast, in Japanese, bilinguals may be more likely to suppress or dampen positive emotions, reflecting their dialectical beliefs about emotion (Miyamoto & Ma, 2011). The greatest cross-linguistic differences on the STAI were found on positive-valence or “anxiety-absent” items (e.g., calm, relaxed, at ease, content). Our findings replicate a previous study that compared the STAI in Japanese and American university students in which Japanese students demonstrated a tendency to inhibit positive feelings, resulting in higher symptoms of anxiety (Iwata & Higuchi, 2000). Relatedly, a previous study also suggested that positive-affect items may not be an adequate assessment of depression in the Japanese population (Iwata, Umesue, et al., 1998). Thus, these cultural scripts about positive emotion may be reflected in bilingual symptom expression. It is also plausible that symptoms reported in clinical settings are more contextually grounded than use of emotion words in laboratory-based paradigms and are therefore more susceptible to the influence of cultural associations and cues.
Furthermore, results from the content analysis and the LPA provide evidence for the perspective that language and culture are highly interconnected (Y. Hong et al., 2000). Bicultural identity as described in the content analysis and more balanced immersion in Japanese- and English-language environments predicted greater cross-linguistic differences in symptom expression. Despite the availability of psychological assessments in multiple languages, emotion words are not universal across languages or cultures. Translation nonequivalence (Lindquist et al., 2018; Wierzbicka, 2005) may cause bilinguals to choose one language as more suitable than another language for conveying their emotions in culturally appropriate ways. Our bicultural bilingual participants had strong connections to both their Japanese and American identities and were able to shift between their cultural selves, activating distinct norms and values based on the language they were using. In contrast, the monocultural bilinguals who have been predominantly immersed in Japanese-language environments did not show large cross-linguistic differences in their symptom expression. For bicultural bilinguals, code-switching may thus change their patterns of psychological-symptom expressions based on the language and associated cultural norms.
Integrating emotion socialization as a mechanism for language-dependent symptom expression adds nuance to the previously observed language-dependent emotion effects—that is, that L1 tends to be more emotionally charged, whereas L2 and later-learned languages may be less so (Dewaele & Costa, 2013; Verkerk et al., 2023). Although emotions may be more readily accessed and automatically processed in L1, certain emotions and mental-health symptoms may also be more stigmatized or avoided in the L1 linguistic and cultural context (Heller et al., 2023), making these symptoms less likely to be explicitly expressed and possibly dampened. To better understand language-dependent expression of mental-health symptoms, future research may need to integrate developmental and socialization perspectives on mental-health assessments.
We found that bilinguals reported higher severity of suicidal thoughts on the BDI-II Item 9 in L1 Japanese than in L2 English. Historically, in Japan, choosing one’s death has been viewed as an esteemed action that protects one’s family name and honor in the face of personal struggles or failures (Fusé, 1980). More recent studies have shown that mild depression predicted suicide among Japanese individuals in contrast to more severe depression in Western individuals (Y. Cho, 2021). Japan’s high prevalence of suicide relative to other industrialized nations has been robustly documented (J. Chen et al., 2009; Motohashi, 2012). Globally, the suicide rate of persons over 65 is nearly 3 times higher than the suicide mortality across ages (He et al., 2021), and Asian countries have a higher older adult to general population suicide ratio compared with Western countries (J. Chen et al., 2009). Our interviews and qualitative content analysis of Japanese adults over age 70 illustrated themes of declining physical health, separation from family (i.e., many Japanese live on their own in the United States with relatives and extended family in Japan), and the burden of aging on younger generation and family. Consistent with findings on late-life suicide in Asian populations, participants discussed the cultural value of maintaining self-dignity by choosing to end one’s life (for a review, see Christensen et al., 2023).
Our findings may offer several clinical recommendations for providing more equitable mental-health services for bilinguals. First, contrasting the dominant view that clinical services must include languages other than English for individuals who have limited proficiency in English, the present work provided evidence that including L1 in assessment and intervention may be beneficial for bilingual individuals at all levels of L2 proficiency. Standardized symptom-rating scales available in multiple languages may be an accessible means to understanding bilinguals’ range of emotions and symptoms in clinical settings, even when the provider may not be proficient in the patient’s languages (J. J. Hong, 2013). This may be especially important for monitoring day-to-day or weekly changes of state-level emotions (e.g., anxiety) during treatment. Second, the inclusion of multiple languages in clinical assessment and interviews might be especially important for bilinguals who identify as bicultural. Although these highly acculturated individuals often receive psychological services in a monolingual-English context, the present findings showed that bilinguals activate their cultural selves through language and suggested that bilingual mental-health services are necessary for patients’ multicultural expression. Third, our findings demonstrated higher severity of suicidal thoughts in the participants’ L1, suggesting the importance of risk assessments that integrate one’s first or native language, especially in suicide screening among older adults from Asian and Asian American communities. Finally, for Japanese-English bilinguals, the cultural concept of uchi-soto (Doi, 1971) is relevant for mental-health treatment. Although epidemiological studies in Japan documented the underestimation of psychological disorders because of stigma, in the current study, we captured the utility of using the Japanese language to express distress. Several participants noted that they could not discuss these sensitive topics with family, friends, or acquaintances (i.e., individuals who are uchi, or inside their social networks) but could share with strangers (i.e., individuals who are soto, or outside their social networks). Some participants specifically requested counseling via telehealth with clinicians who lived outside of their neighborhoods or communities. Technology, including telehealth services and language translations, can extend the reach of mental-health assessments and interventions. The use of online bilingual symptom-rating scales coupled with a clinical phone interview and followed by a referral to an in-state Japanese-speaking telehealth clinician may be a viable service model to improve mental-health services for Japanese-English bilinguals living in the United States.
Beyond the present study, recent rapid developments in the use of natural language processing (Malgaroli et al., 2023) and machine-facilitated (e.g., artificial intelligence [AI]) translation technologies (Genovese et al., 2024) could improve the ease of integrating multiple languages in mental-health services. For example, providers may translate clinical handouts and materials more easily (e.g., via Canva’s AI online translator). Augmented reality glasses (e.g., Ray-Ban Meta glasses) with live translation using mixed modalities (i.e., audio and visual) may also support interpreter services in the near future. With a cautionary note that large language models include systemic biases against minoritized individuals (Wenzel et al., 2023), these technologies may help promote linguistic diversity in mental-health services.
Several limitations of the present study require further attention by future research. First, our sample is sufficiently powered to detect differences on the STAI but may be limited in power to detect differences on the BDI-II because of varying effect sizes (Brysbaert & Stevens, 2018; P. Green & MacLeod, 2016). Therefore, future studies may need to recruit larger samples to detect differences on both anxiety- and depression-symptom rating scales. Second, our sample is biased toward Japanese female-identifying individuals (88.5%). Despite the within-persons approach, in which symptom expression was examined as a function of each bilingual individual’s two languages, our findings may not generalize broadly across the gender spectrum given the role of gender in emotion and symptom expression (Glenberg et al., 2009; Newman et al., 2008). The attrition rate also highlights the stigma and challenges in recruiting middle- to older-age Japanese-English-speaking male-identifying individuals for whom age, race, gender, ethnicity, and immigration status intersect (Kalibatseva & Leon, 2011; Morrow et al., 2020), and reiterates the need for greater future efforts to represent this population in mental-health research and practice. Third, there are inherent limitations to using scales for measuring psychological symptoms. Although we used the same analytic approach for both scales, the STAI and BDI-II differ in their range (i.e., 80 points on the STAI vs. 63 points on the BDI-II) and type of anchors (e.g., “not at all” vs. “I do not feel like a failure”). The use of emotional verbal anchors on the BDI-II may have introduced a response bias—specifically, the anchor-contraction effect (De Langhe et al., 2011)—in which emotion-related words in L2 are perceived as less emotional than in L1, potentially inflating the responses in L2 and counteracting the hypothesized effects on this scale. Future studies will therefore need to consider the use of nonverbal anchors for the development and implementation of a more linguistically equitable psychological assessment in clinical practice. Nevertheless, despite the limitations and need for further research, the present study constitutes a valuable starting point for studying the experience, expression, and assessment of symptoms of anxiety and depression in Japanese-English bilinguals, with possible implications and likely relevance for the experience, expression, and assessment of mental health in Asian American populations and bilingual groups more generally.
To conclude, the current findings provided initial evidence for language-dependent symptom expression in bilinguals. The integration of psycholinguistic research with clinical science in our work illustrated that use of English-only psychological assessments with linguistically diverse populations could result in an incomplete and inaccurate understanding of individuals’ mental health. Language must be considered to prevent overestimation or underestimation of mental-health symptoms. Clinical researchers and practitioners must prioritize a patient-centered approach in which bilinguals can draw on their diverse linguistic and cultural repertoires for expressing symptoms. In mental-health-service settings where individuals regularly communicate through language, an inclusive and responsive clinical model that accounts for a person’s multilingual background will contribute to more equitable and effective care.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251385547 – Supplemental material for Language-Dependent Expression of Anxiety and Depression Symptoms in Japanese-English Bilinguals
Supplemental material, sj-docx-1-cpx-10.1177_21677026251385547 for Language-Dependent Expression of Anxiety and Depression Symptoms in Japanese-English Bilinguals by Aya Inamori Williams, Sirada Rochanavibhata and Viorica Marian in Clinical Psychological Science
Footnotes
Acknowledgements
We thank the members of the Bilingualism and Psycholinguistics Research Group for their feedback in developing the study. We thank Atsuo Nakagawa, Yuka Kudo, Taisei Wake, and Mayu Lindblad for assisting with the selection and translation of study instruments in Japanese. We extend special thanks to Emi Sakai, Junko Johnson, Tomoya Hirota, and Takeo Toyoshima for assisting with recruitment. We thank our community partners at FLAT JP; Kimochi, Inc.; and the University of California San Francisco Collaborative Approach for Asian Americans, Native Hawaiians, and Pacific Islanders Research and Education for their generous and instrumental support.
Transparency
Action Editor: Shirley Wang
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.