
Abstract
Asian Americans/Pacific Islanders (AAPIs) are the fastest growing ethnic/racial group in the United States but experience difficulties accessing and engaging in mental-health care. Limited clarity around applied cultural adaptations for evidence-based psychotherapies (EBPs) and biases in the psychological field may hinder innovations in care. In this qualitative study, we explore adaptations to existing EBP intervention frameworks by synthesizing perspectives of experts in AAPI issues from both mental-health and non-mental-health fields. In-depth interviews were conducted with mental-health researchers and clinicians who focus on AAPI issues (N = 24) and nonpsychology experts (N = 12) in Asian and AAPI issues, drawing from fields including ethnic studies, history, diaspora studies, cultural sociology, political science, literature, and film studies. Thematic analyses yielded eight key themes that informed peripheral and core modifications and goals to existing EBPs. This expanded EBP psychotherapeutic framework may improve clinical applications of cultural adaptations.
Between 2000 and 2019, Asian Americans and Pacific Islanders (AAPIs) grew by 81%, making them the fastest growing ethnic-racial group in the United States (Pew Research Center, 2021). Although nearly 20% of AAPIs will experience a lifetime mental disorder (Takeuchi et al., 2007), they underuse mental-health treatment relative to other ethnic/racial groups, and individuals who do seek services tend to delay initiating care, present with higher symptom severity, and be more likely to drop out of treatment than their White counterparts (M. Lee et al., 2020; S. Sue et al., 2012). Most of this research has focused on reducing stigma and increasing access; relatively few have articulated practical, clinical modifications to frameworks for evidence-based psychotherapy (EBP) or critically examined the content of the psychotherapy itself.
There is, however, a growing literature for cultural adaptations of EBPs, specifically for AAPIs. Many are creative, such as running a youth essay contest and community partnerships to deliver a parent-training intervention (Wang et al., 2021) and using Korean dramas to shift mental attitudes and stigma (Ta-Park et al., 2019). Nevertheless, several unresolved issues remain in the translation of these adaptations into everyday clinical practice. First, the AAPI umbrella category is known to be notoriously problematic yet persists in group-focused diversity research. Clinically, this can overlook risk because data disaggregation reveals unique youth-suicide profiles among AAPI subgroups (C. K. Lui et al., 2024). Second, results from cultural adaptations are rarely actionable for direct uptake by clinicians. For example, adaptations appear most effective when culturally tailored for specific AAPI subgroups (e.g., adapted for Chinese Americans; Huey & Tilley, 2018), but few practical details about individual-specific tailoring for clients exist, running the risk of microaggressions (D. W. Sue et al., 2007) and cultural-misattribution biases (Causadias et al., 2018; Liu & Herndon, 2022). Few EBP frameworks adequately integrate heterogeneity among AAPIs in socio-historical-political contexts, family-immigration trajectories, socioeconomic class, and intergenerational culture conflicts (P. P. Lui, 2015), among others. The cultural-treatment-adaptation framework (CTAF; Chu & Leino, 2017, see Figure 1) is one model that seeks to categorize the primary targets of adaptation, which can fall into two categories: (a) peripheral or surface-structure treatment components focused on engagement (e.g., language, framing, aligning with values, provider/client relationship) and (b) core treatment components that include changing deep elements of treatment that affect clinical outcomes. Core treatment adaptations can include a complete change, core addition (e.g., additional module), or core modification (e.g., component is changed or deleted). Therefore, identifying specific peripheral and core cultural modifications to existing EBPs would help guide practitioners toward greater individualization. Third, many culturally responsive treatments are often piecemeal, focusing on a single aspect of adaptation. For example, ethnic/racial socialization appears beneficial for the mental health of specific subgroups (e.g., Vietnamese American adolescents, as in Yu et al., 2022), and interventions that directly address racial stress are available (e.g., Hwang & Chan, 2019); however, rarely do clients show up to psychotherapy for racial stress alone. Integration of cultural adaptations wi a well-practiced EBP intervention framework, such as the cognitive-behavioral-therapy (CBT) case-formulation approach (Persons, 2012), would allow for a culturally nuanced working model and understanding of clinical problems. This would inform an individually tailored, culturally resonant intervention plan with core and peripheral modifications as outlined by J. Chu and Leino (2017). An exemplar is the cultural assessment of risk for suicide (CARS; J. Chu et al., 2013), which integrates cultural models of suicide risk with person-specific assessment of domains, such as family conflict, social support, minority stress, and acculturative stress.
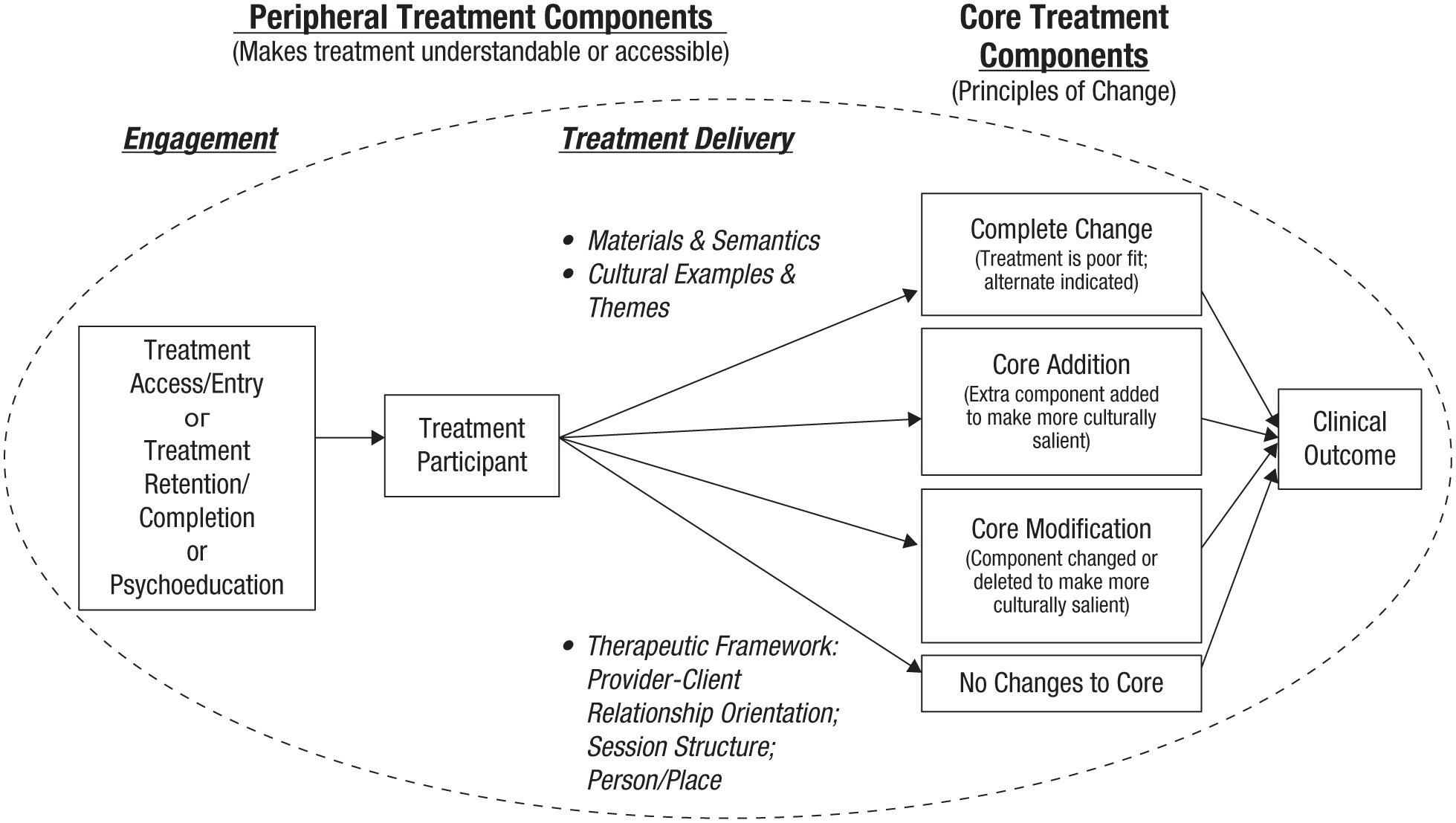
The cultural treatment adaptation framework for cultural adaptation of evidence-based interventions components from J. Chu and Leino (2017).
Beyond cultural adaptations, biases in psychology might inhibit innovation. D. W. Sue et al. (2024) recently named the “White epistemology” (p. 595) that remains entrenched in psychotherapy theory and practice. This criticism is not new—it is well recognized that psychology has overlooked diverse, global populations (e.g., Bradford et al, 2024; Henrich et al., 2010) and oversamples from White, middle-class, college-educated people (e.g., Thalmayer et al., 2021). When culture is addressed, it risks the misattribution biases described above. Furthermore, the clinician workforce lacks diversity (APA, 2020). EBPs themselves have been called “inherently ethnocentric” (Wendt et al., 2015, p. 334) and “a form of social control toward majority norms” (Hall & Malony, 1983, p. 139) by overemphasizing individualism (Chen et al., 2006; Markus & Kitayama, 1991; Markus & Kitayama, 2010), devaluing racial/ethnic identity (Chou & Feagin, 2015), and overlooking contextual and societal factors (Neblett, 2023).
Cultural psychologists have also cast a critical gaze on the ways psychology as a field operates from a culture of neoliberalism. As a result, it tends to radically abstract persons from socio-historical-political and interpersonal contexts, promote an entrepreneurial self, overvalue high-arousal positive emotions, and emphasize personal autonomy, fulfillment, and growth (Adams et al., 2019). Cultural adaptations for EBPs also rarely question psychotherapy content, its assumptions about well-being, or the potential harm that can result from interventions, particularly on interpersonal relationships (Wendt et al., 2015). One popular media piece described psychotherapy as “bound by many Western ideas and rooted in whiteness” (White, 2024). Biases have also been identified among mental-health clinicians embedded in an organizational culture. Even individuals trained in cultural competency and EBPs still have implicit biases that create an “invisible architecture” in mental-health-care systems (Desai et al., 2021, p. 86) such that clinicians prefer clients who are verbal, emotionally aware, and individually oriented—individuals without these characteristics can be pathologized or viewed as deficient. Therefore, in addition to understanding applied best practices from mental-health experts, advances in diversity science can benefit from integrating the perspectives of individuals outside of psychology.
Purpose of the Present Study
Given both the complexity of addressing AAPI mental health in practice and the biases inherent in the field, we explore ways to expand an EBP intervention framework. In this two-group qualitative study, we integrate the perspectives of mental-health experts and experts from disciplines outside of psychology, including the social sciences and humanities, to develop an expanded psychotherapeutic intervention framework for AAPIs. The goal of this study is twofold: to (a) build on the existing knowledge base of AAPI mental experts and practitioners who already engage in the EBP practice of cultural adaptations and (b) pull from a broader nonpsychology evidence base to explore additional considerations that can be integrated into a case-formulation framework to inform mental-health interventions for AAPI populations.
Transparency and Openness
Preregistration
This study was not preregistered.
Data, materials, code, and online resources
Privacy concerns restrict the availability of interview transcripts for open data. The interview guide used in this study is available in the Supplemental Material. MAXQDA24 was used to assist with storage, searching, and coding. Interrater coding was calculated using the irrCAC package (Gwet & Gwet, 2019) in R.
Reporting
We follow the journal-article reporting standards for qualitative data as outlined by Levitt et al. (2018).
Ethical approval
The study was approved by the Institutional Review Board of the University of California, Berkeley.
Method
Positionality
N. H. Liu and S. Chen are both second-generation Taiwanese American psychologists whose clinical and research training were completed in the United States in primarily positivist frameworks. N. H. Liu is a clinician educator, primarily engaged in clinical training with a particular emphasis on diversity, whose perspective is informed by time as a researcher in China and Argentina. S. Chen is a researcher and educator whose perspective is informed by his applied experience as a school counselor and educator in China.
Sample
Purposive sampling methods (Patton, 1990), specifically, criterion sampling, was used to gather information-rich cases, and individuals were recruited by email. All experts received a $150 gift card to compensate for their time. All interviews were face-to-face using Zoom and completed by N. H. Liu.
Group 1: mental-health experts
Group 1 inclusion criteria included expertise as a mental-health clinician and/or researcher specializing in AAPI populations and 18 years of age or older. Participants were identified by N. H. Liu, who is familiar with this content area. As described in Table 1, mental-health experts (N = 24) drew from a wide variety of mental-health backgrounds, including affective science, developmental psychopathology, clinical psychology, counseling psychology, psychiatry, and marriage and family therapy.
Demographic Characteristics of Group 1 and Group 2 Experts
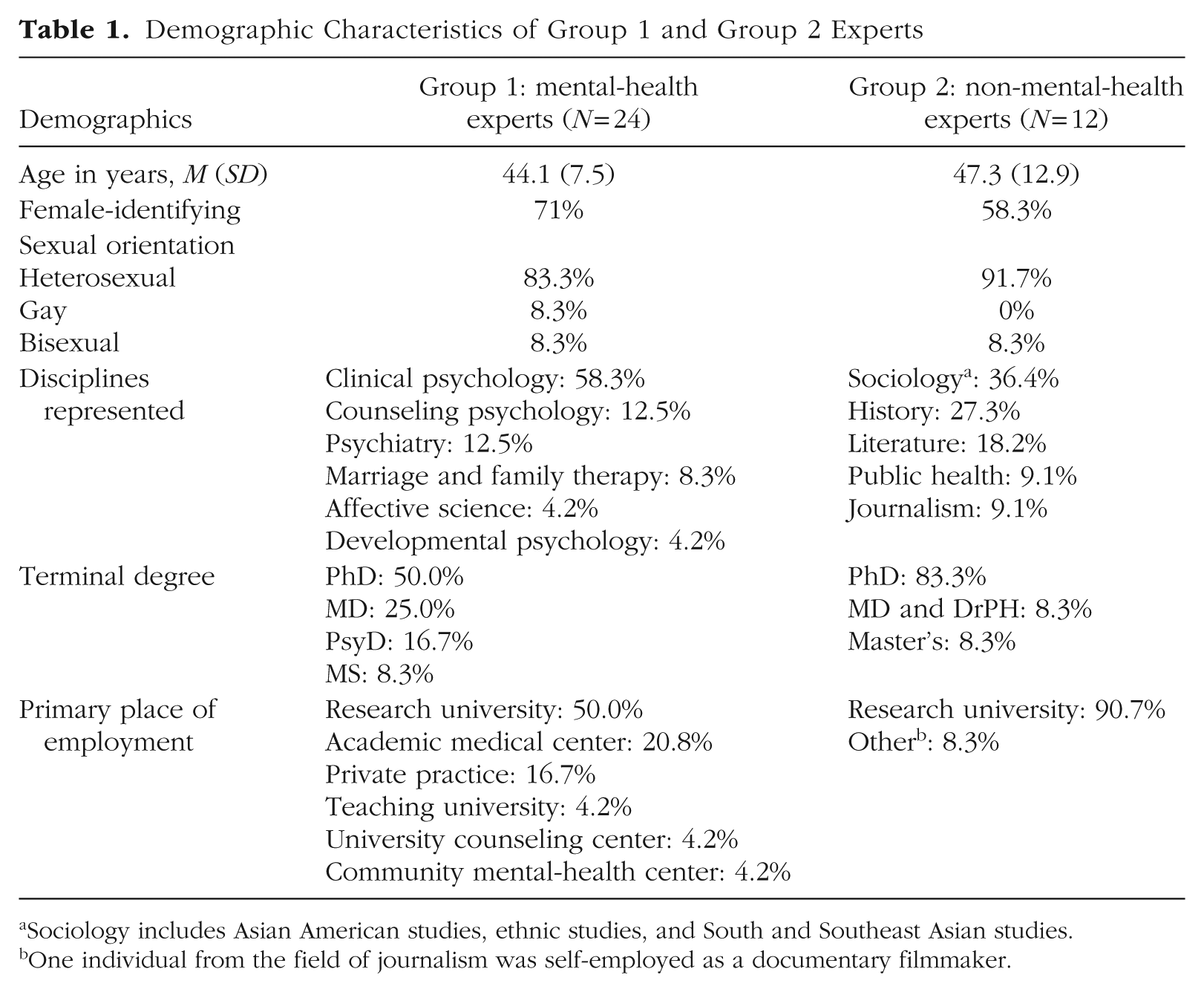
Sociology includes Asian American studies, ethnic studies, and South and Southeast Asian studies.
One individual from the field of journalism was self-employed as a documentary filmmaker.
Group 2: non-mental health interdisciplinary experts
Group 2 comprised non-mental-health experts (N = 12). Similar to Group 1, they drew from a range of nonpsychology backgrounds, including social sciences (e.g., sociology, ethnic studies, public health) and humanities (e.g., history, diaspora studies, literature, film studies, and journalism), as summarized in Table 1. Many also drew from their experiences as educators of college-age students. Inclusion criteria included being researchers with expertise in Asian and/or AAPI populations outside of mental-health fields and being 18 years of age or older. Participants were identified by N. H. Liu and S. Chen, who are familiar with this content area, and invited to participate through email.
Procedure
For both groups, following informed consent, participants completed a brief demographics and background questionnaire. Virtual, 2-hr, in-depth interviews were conducted by N. H. Liu using the same semistructured guide. Interview questions were derived from the N. H. Liu’s engagement in clinical training, practice, and supervision and focused on common challenges in psychotherapy among AAPI clients and how these were or should be addressed in current practice; the limitations of extant psychotherapies to address these challenges; advances in their areas of expertise to address these challenges; current approaches, solutions, and scientific findings that can improve psychotherapy; and adapted definitions of well-being among AAPIs. Specific questions focused on socio-emotional-cultural-linguistic development and expression, interdependence/independence in relationships, racial identity and racism, socioeconomic class, subgroups in the AAPI umbrella, and intergenerational experiences and socio-politico-historical factors, among others. A case-study prompt was included in the interview to prompt practical, illustrative strategies in treatment. A total of 24 interviews were completed with Group 1; 20 interviews were completed individually, and two group interviews composed of two individuals each (n = 4) were completed. For Group 2, 12 interviews were completed individually. All interviews were recorded and transcribed.
Ethics
Informed consent was obtained from all participants included in the study. To ensure participants’ confidentiality, we removed all identifying information from transcripts, and participants were referred to with identification codes.
Data analysis
Thematic analysis was the primary interpretative framework to guide our analyses and derive themes (Braun & Clarke, 2006, 2019). This focused on treatment adaptations and approaches to an existing framework to address existing challenges and associated clinical approaches. Initial coding was completed by N. H. Liu, and an interim voluntary session was held with participants on the research findings with opportunities for feedback to ensure that participants’ own meaning and perspectives were represented. For analysis, transcripts were coded line by line. Codes were created for each segment of data representing a new idea (total segments = 1,103). Segments conceptually similar in nature or related in meaning were grouped together into concepts. These concepts were developed through constant comparison, and the most relevant concepts were integrated into eight themes that formed the larger framework.
Following O’Connor and Joffe’s (2020) guidelines for intercoder reliability with qualitative data, S. Chen was trained on 10 randomly selected segments from the full data set, which were coded into the eight key themes. Discrepancies from the N. H. Liu’s codes were resolved through consensus. S. Chen then independently coded approximately 10% of the total segments. Given low base rates of references to each theme, Gwet’s agreement coefficient (AC1) was used to calculate intercoder reliability (Gwet & Gwet, 2019) in R. Gwet’s AC1 has been shown to effectively address limitations of Cohen’s kappa when applied to criteria with low prevalence rates and high agreement between coders (Gwet, 2008; Padilla-Iglesias et al., 2024; Wongpakaran et al., 2013). AC1 values indicated good intercoder reliabilities across all eight themes (range = 0.87–0.97).
Results
Thematic analysis revealed eight key themes across both groups with applied, practical recommendations for modifications to case formulations and interventions. These modifications are further categorized into peripheral and core modifications, in line with the CTAF by J. Chu and Leino (2017), and are illustrated in Table 2.
Group 1 and Group 2 Themes and Subthemes With Case Formulation and Intervention Modifications
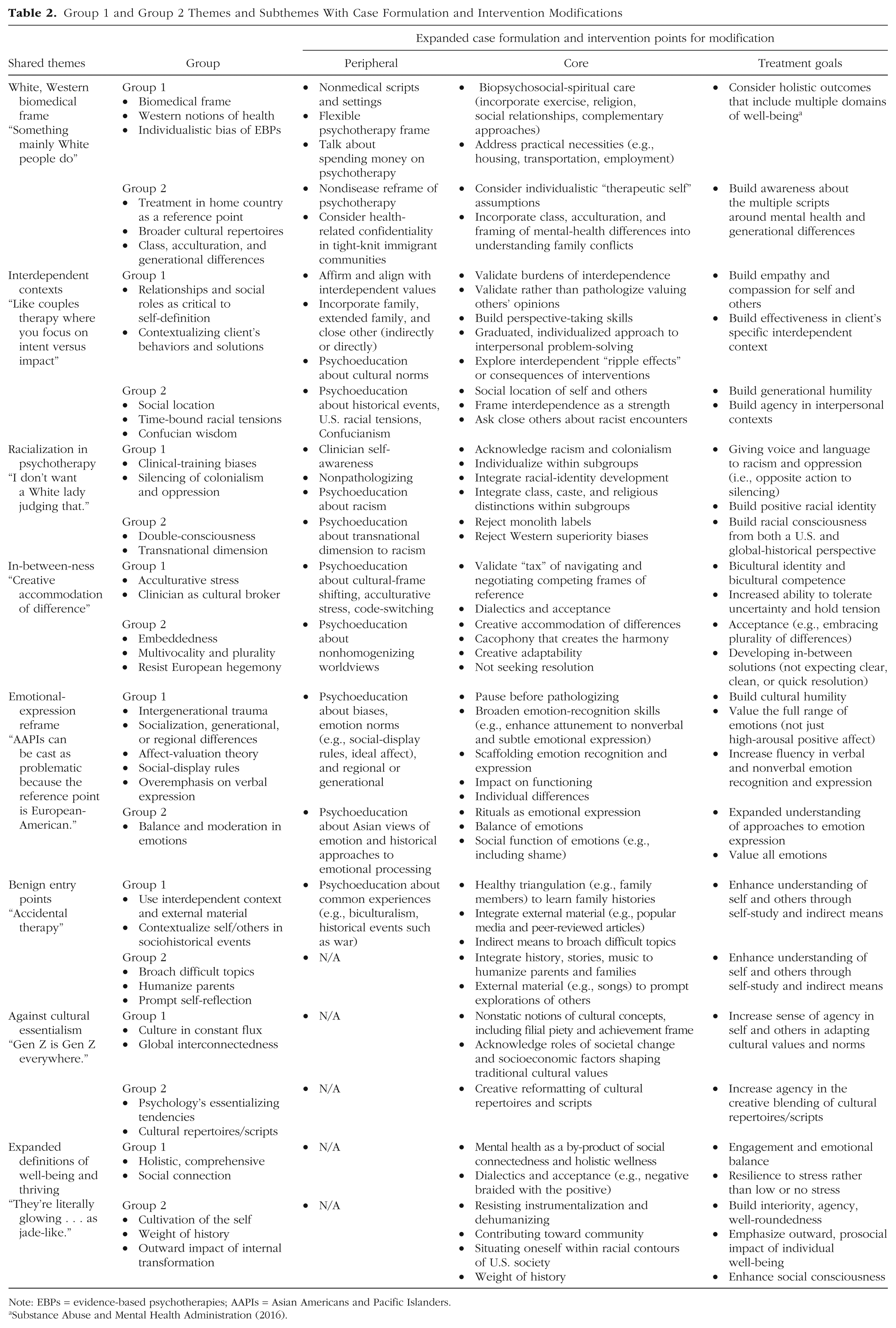
Note: EBPs = evidence-based psychotherapies; AAPIs = Asian Americans and Pacific Islanders.
White, Western biomedical frame
This theme (Table 2 shared theme: White Western biomedical frame) highlighted cultural assumptions in “therapy as usual.” Individuals more acculturated to White, Western norms and with higher socioeconomic status (SES) were viewed as more likely to benefit and feel comfortable with therapy. By extension, normative psychotherapy practices were culturally dissonant with AAPIs from lower SES, who are less acculturated, and from an older generation. One Group 2 expert noted that this could be due to mental-health-care norms in the country of origin (e.g., treatment being reserved for severe mental illness). Most Group 1 experts highlighted cultural norms around holistic and nonmedical approaches to mental health.
Experts (Table 2, Group 1) highlighted, based on their training, professional experiences, and direct clinical work with clients, the ways that psychotherapy and the larger mental-health-care system “lac[k] face validity.” The health-care framing of mental health, professionalized jargon, diagnostic labels, and “aggressive” treatments, such as medication, were viewed with skepticism, inconsistent with a broader holistic worldview that incorporated a biopsychosocial-spiritual understanding of health and well-being. Emotional distress was not the purview of health care. This Western view of health implied mind-body dualism, which excluded, implicitly and explicitly, alternative or nonmedical approaches to emotional well-being, such as exercise, herbal remedies, acupuncture, and tai chi. Group 1 reported that professionally, although they learned these practices, their peers rarely integrated these into clinical practice and that these practices were often seen as adjunctive, unnecessary, or “less valid” and not part of “real” EBPs. Group 1 also described how biomedical frames did not address the full range of clients’ needs that affected mental health (e.g., housing, transportation, employment). In training, they learned that this was “not the role of the therapist,” which left these problems unaddressed, leaving many clinicians feeling helpless about client dropout or treatment failure. They noted this further added to clients’ skepticism about EBPs. Mistrust of the larger mental-health-care system was common among specific subgroups, including beliefs about child removal from homes and its association with colonialism for PIs.
This biomedical framing or cultural script was also culturally discordant, requiring individuals to come into a professional office on a weekly basis, pay expensive fees despite ambivalence about therapy, and engage in intimate “confessional” conversations about family members, all usually with limited ethnic and linguistic matching. When matching was available, health-care confidentiality went against norms in tight-knit immigrant communities. One Group 2 public-health expert noted: I have to reassure [them] that we won’t disclose anything they say . . . in small communities where most people know each other, especially for the Vietnamese community, like you do a nail business, so a lot of them are just in a small community.
To adapt, Group 1 experts admitted to stretching the “psychotherapy frame,” which they said went against their professional training. They flexibly accommodated client schedules (e.g., individuals working in restaurants) with occasionally briefer (e.g., 30 min) or longer sessions. One marriage and family therapist (MFT) had session in client homes, which might include sharing food, if offered. Clinicians also encouraged directly talking about spending money on psychotherapy, especially how this might conflict with immigrant values. One clinical psychologist described Pacific-Islander (PI) clients in treatment: They’re not knowledgeable [about] this different way of approaching help . . . this idea that things . . . need to be disease-focused, tied to a diagnosis . . . in like a for-profit, health care world . . . and [even though] there’s . . . talk of . . . understanding that everything is interconnected . . . we still operate very siloed in our thinking about . . . mental health and well-being.
Group 1 described an expanded biopsychosocial-spiritual case formulation informing treatment. Modifications included encouraging clients to exercise, readily having “local acupuncture referrals on-hand,” and consulting regularly with these practitioners as a part of their professional network. This also included integrating interpersonal contexts and engaging informal supports, including family, friends, and community elders. Both groups highlighted significant religiosity among AAPIs and the need to incorporate spirituality and religious supports and leaders, such as Catholic priests, Protestant pastors, or temple resources.
For Group 1, the White, Western biomedical frame contributed to perceptions of psychotherapy by their clients as “something mainly White people do” (Table 2, shared theme). Its concepts were viewed as based on “White notions of personhood,” which overemphasized the individual. EBPs emphasized “declarative” approaches to managing interpersonal conflicts, which could be viewed as “selfish” and conflicting with interdependent values. There was also criticism by Group 1 that training was primarily focused on “training White people” to become culturally competent. Although many were experts in cultural adaptations, they acknowledged these were insufficient for real-world issues and described instead “making it up as I go along,” particularly in managing intergenerational culture and family conflicts.
Experts from outside of psychology (Table 2, Group 2) named broader, relevant cultural scripts among young generations—that of “therapeutic culture,” which emphasizes self-care and finding the “authentic or true self” and includes a class dimension. As one cultural sociologist noted, With the . . . therapeutic culture that has become increasingly salient among the upper middle class . . . there’s a lot of sociological studies now that show how broadly diffuse it’s become . . . it’s not only in people’s head, it’s part of the scripts that surround us. . . . It’s an objective reality . . . part of the cultural structures that surround us . . . people being in touch with their emotional needs and putting a personal balance above the pursuit of social mobility and . . . the idea of living in an authentic way . . . [and] be your full self. Maybe this therapeutic culture is . . . unevenly distributed across classes . . . class differences are often not discussed as much as they should in terms of how people relate to this therapeutic culture and the obligations that people have toward their families.
This broader cultural script may contribute toward intergenerational culture conflict (Lui, 2015), given different mental-health framing across generations (i.e., from medical model to therapeutic culture) and may be especially salient in families marked by upward social mobility, with its class and acculturative-stress implications. Therapeutic culture reflects hyper-individualistic values, which may exacerbate interpersonal conflicts, a focus of the next theme.
Interdependent contexts
Relationships were viewed as critical to one’s self-definition, based on social roles and interdependent values (Table 2 shared theme: interdependent contexts). Group 1 described modifying EBPs and incorporating significant interpersonal components even if family members or close others were not physically there. Family included extended family and close others (e.g., aunties, uncles, cousins, grandparents). These relationships were framed as that “lifelong thing [the client will need to] navigate.” Interdependence was viewed as something to affirm, a source of strength and support, and conflicts should be directly addressed in EBPs even without those individuals in session. When interdependence was stressful or burdensome, an MFT described giving language to and validating these experiences as common in immigrant families without culturally laden terms (Table 2, interdependent contexts, Group 1 core modification): It’s unspoken, it’s this felt sense of family responsibility . . . yes, you can call it “filial piety” . . . but why the person is in their career working so hard is that they saw the sacrifice of their parents, significant loss . . . parents who don’t know what self-care is, never engaged in wellness practices, no modeling for that. . . . All of this is playing out in a society where Asian Americans are largely invisible to the larger community, just working hard . . . simply a burden that they carry. When parents are older, they don’t have to work so hard. What’s carried inside, there’s no language for it.
Group 1 highlighted how most of their clients’ presenting problems were interdependent in nature. With individual EBPs, the focus and ultimate goal were framed as “like couples or family therapy with one person.” This meant creatively bringing in these close others and building up perspective-taking skills even if those people never made their way into the therapy room. Sometimes, this included assessing problems through the eyes of another to better situate presenting problems in a client’s interdependent context. As described by one psychiatrist, I would ask, “How would your childhood friend describe what’s going on with you? How would your grandfather describe it when you say, ‘I don’t want to live anymore?’ What would your childhood friends, what would your grandfather think about this . . . what would your grandmother have said?”
It also included conversations with close others through role-plays or chair-work techniques (Perls et al., 1951). As described by one MFT, “I would have [the client] have a conversation with the family member [in the therapy room] pretending they’re right there. Or ask them to do letter writing.” This also included deepening understanding of older generations (e.g., parents, grandparents) according to cultural norms and immigration experiences. Goals included perspective-taking, building empathy, and expanded ways of giving and receiving affection. Cultural brokering, psychoeducation, and guided discovery were used to explore attributions of others to build curiosity rather than judgment. Criticism was reframed as an expression of love, as described by one affective scientist: “Anyone can say positive things. Only the people who love you will tell you what you do not want to hear, something critical, that I think you can improve.” As one psychiatrist noted, I think it gets down to the intention versus impact conversation. I would be curious about the experience rather than immediately jumping to labeling. I do think that jumping to labeling is really problematic. I do like that [couples therapy] frame because it also humanizes each side for the other. . . . [One] person is so sure they’re right and . . . [instead, they learn to] mentalize and give the other [understanding], what might that person have [meant] . . . also love languages, right? I think for the classic example, Asian parents . . . wanting to do acts of service and the American-born, wanting words of affirmation. Explaining that concept [to clients can be helpful].
Communication and enforcement of boundaries were more nuanced than standard approaches. Group 1 noted how most EBP assertiveness-training approaches could “absolutely backfire.” Instead, experts gave clients agency to make decisions and thought through interdependent “ripple effects” (Table 2, interdependent context, Group 1 core modification). They emphasized letting the client lead, respecting the client’s understanding of what would be most effective with specific family members, and refraining from trying to resolve issues immediately. Group 1 explored the impact of interventions on clients’ close others, especially how decisions (e.g., around boundaries, elder care, marriage partners) would be received and how others’ opinions weigh heavily on clients with interdependent values. Communication was less confrontational and direct; instead, a continuum of options, ranging from email and texts to voice memos, were considered to express needs and soften their impact. Flexibility around determining steps forward included greater trial and error, more “wait and see” messaging about tapering up or down frequency of communication, an extended timescale for assessing and reassessing the effectiveness of solutions, and adapting solutions to understand its impact and to “set the yardstick” with clients about what would be effective in the client’s specific context.
Both groups highlighted family roles and structures, such as being an only daughter or eldest son and associated roles and responsibilities and/or inherent hierarchies. Group 2 drew on early sources of ancient Confucian wisdom about how to navigate individual agency in social interconnectedness (Table 2, interdependent context, Group 2 peripheral modification). One historian described the following: When you read a lot of early Confucian texts, they are about attaining independence from circumstances and . . . that’s definitely one way of defining freedom . . . fostering agency and self-sufficiency in the context of interdependence in the roles and responsibilities we each have.
Goals of therapy included fostering a contextualized understanding of self and others that would yield greater understanding and compassion. Contextualizing others meant understanding family histories, immigration trajectories, and timelines of migrations while acknowledging the impacts of different decades of racial tensions, tenuous citizenship status, and other elements of the context of reception, which is defined as “the ways in which the receiving society constrains and directs the acculturation options” Schwartz et al., 2010, p. 238). An unfavorable context of reception may include systemic barriers, such as discrimination, unsafe neighborhoods, and limited access to resources, including jobs and promotions (Schwartz et al., 2010). For example, parents might have faced frequent racism because of limited English fluency or anti-Asian hate in the 1980s following Vincent Chin’s murder. One clinical psychologist echoed the importance of not pathologizing individual family members but understanding them within their historical context: “Without understanding parents’ history . . . they literally seem crazy. . . . It has required [that clients] lean into their own history and learn about their family’s cultural history.”
Group 2 deepened this contextualization through the concept of social location (i.e., situating oneself and others within specific familial, cultural, social, historical, and political contexts and related power structures). Social location recognizes an individual’s “location” as embedded within a hierarchy stratified at various levels (e.g., local, national, transnational) and within a chronological and wider context, allowing for the integration of intersectionality (e.g., gender, race, class), and protects against essentializing tendencies that might be presumed in group-based categorization (Anthias, 2012). Group 2 acknowledged how the silencing of family histories and intergenerational trauma could be situated within a social location and reframed as the “the best they could do,” citing a popular graphic-novel memoir. Understanding social location had as its goal the building of greater empathy in clients and the way they understood others—in fact, greater empathy was named as an explicit treatment goal, in contrast to standard EBP outcomes. This was described as moving beyond seeing parents as “one-dimensional” but rather “in all of their complexity . . . as people.” As one ethnic studies scholar described it, That kind of consciousness can help them understand their situation as opposed to thinking, “I’m just inherently a bad person” or “the father’s just inherently a bad person.” There’s a story behind his own behavior and I think it helps them have a broader appreciation and understanding of where this may be coming from. But also it helps you feel better in knowing that [this] situation is not just one that’s involving your relationship to your father, but in fact, involves this . . . broader context and history to understand how you guys got to this point. It would help to be able to make that connection, ’cause I think it’s a powerful connection.
Time-bound racialized experiences or stressors faced by immigrants could also deepen empathy, including understanding tenuous citizenship status, anxiety about deportation, and experiences of discrimination (e.g., because of accents). For example, parents may have felt a sense of inadequacy navigating a new country in a foreign language and relied on their native-English-speaking children to help with interpretation or filling out important paperwork.
Group 2 encouraged clients to directly ask immigrant parents about racist encounters across decades and its gendered dimensions. One sociologist shared discovering only as an adult that his father was spat on in the 1970s. Another historian shared how her South Asian father-in-law immigrated in the 1970s and Americanized his name because of a fear of rejection and hypervigilance about “being too Indian.” In contrast, as part of a younger cohort, she had significant pride about her heritage, could comfortably go by her Indian name, and boldly corrected others’ mispronunciations without fear of repercussion.
Racialization in psychotherapy
Experts highlighted the way AAPI stereotypes and misperceptions (e.g., monolith, model minority, the “racial construction” of AAPIs, assumptions about family) can be imposed in psychotherapy, the larger mental-health field (e.g., health-care settings, cultural competency training), and societal structures (Table 2 shared theme: racialization in psychotherapy). Group 2 articulated reasons behind these tendencies, including histories of colonialism, racialization in the United States, and Western superiority biases, leading to perceptions of AAPIs as racially inferior, exhibiting pathological behaviors, and from a deficit model. Group 1 experts reported clients’ frequent experiences of racialization in psychotherapy, including feeling stereotyped, looked down on, labeled, or judged. One psychologist noted, You hear complaints about other clinicians, other experiences. . . . A lot of people don’t want to be seen by a White therapist. They’ll say, “No, she was just like a nice White lady.” They’re like, “I don’t want a White lady judging that.” And like the White lady saying, “Oh, you know, draw boundaries with her, tell her to stop that shaming you” or things like that.
They focused on racialization across many layers, from clinical training, in psychotherapy sessions, and client life experiences. One psychiatrist described the following: [Clients are] expecting the Western-trained clinician to look down on you. . . . Sometimes they can be embarrassed to bring it up . . . if part of them is worried, “Maybe I’m cursed, maybe this is karma, payback for something my ancestors did.” A part of them knows that talking about that can seem . . . backwards.
A counseling psychologist described a similar experience: If I talk about this part of my family experience, will this person judge me or think it’s crazy or think it’s too much and not understand the depth of connection that’s completely unspoken, generations of ambiguous loss that shows up in the tension that we feel, generational experiences, loss and grief and disconnection that are present and not anything can be done about it? Many live with that tension every day and learned to thrive despite it.
Modifications included directly acknowledging racism. Clinicians described client relief about “shortcutting, short-handing” experiences of racism in psychotherapy but attributed this to foundational clinical skills of attunement rather than ethnic-matching alone. As one South Asian clinical psychologist described, People feel as though they don’t have to explain how the color of your skin, how you look, affects your everyday life. And I try to be very like, “Hey, just ’cause I have experiences with how I look and how I was raised and what identities and cultures we’re involved in, it doesn’t mean even a person with matching identities is going to have the same opinion or the same experience but at least they won’t have to tell people, ‘No, Pakistan is not in Africa.’ Or, you know, ‘It’s not like Pakistan’s just like India,’ that kind of thing.” So not having to explain things . . . [In] best case scenarios, there’s shared language, acknowledgment, attunement . . . due to not just ethnicity/race.
Racialization was framed as silencing, and oppression was framed as taking away one’s voice. In response, Group 1 experts focused on psychoeducation about racism, giving language to and validating common experiences. As described by an MFT, Many didn’t realize that was part of their experience, wouldn’t have said, “Oh yeah, my whole life I’ve lived out the model minority stereotype and here I am.” It was my parents lost everything coming here . . . emphasized education. They were allowed to come to the United States only because of pursuing an education, so that’s all we know. And so we keep running.
Giving voice and empowerment was further identified as treatment goals, acknowledging histories of colonialism and oppression: “It’s really hard when people come here [to] Hawaii . . . there’s a lot of Pacific Islander folks that come because America has done some pretty awful things to islands near us.”
Group 2 extended this silencing to wider geopolitical history, particularly the violent political histories of some countries of origin that have been erased or are now unknown because as noted by one political scientist and historian, the United States “does not see itself as an imperialist, an empire.” Treatment goals included developing a racial consciousness and “decolonizing” one’s worldview. Modifications included psychoeducation about racialization within society, the imposition of a single identity (i.e., monolith), and the historical bias of being viewed as racially inferior. One sociologist cited data from the Pew Research Center, noting that “most Asian American groups don’t define themselves as ‘Asian-American.’”
Individualization was a key theme from both groups, although many acknowledged this was difficult. As one clinical psychologist noted, “Stereotypes about Indians tend to be even—I just did it, right? I immediately went to Indians when there [are] a lot of different identities in South Asia.”
Subgroups provided a “certain profile,” but within-groups heterogeneity could be understood through assessing individual sociopolitical histories, including understanding forced versus voluntary migration, different waves of immigration, and various AAPI diaspora communities in France, Australia, the Caribbean, Africa, and South America, through which many families came to places like the United States. Postmigration experiences with ethnic enclaves or White-majority areas also contributed to postadjustment well-being and affected racialization. Racial-identity development was acknowledged as a source of individualization. The act of going to psychotherapy itself was viewed as having “echoes” of racial identity, a social signaling of “what kind of AAPI” you are. Class, caste, and religious distinctions were also noted.
Group 2 experts identified racial consciousness as a treatment goal (Table 2, racialization in psychotherapy, Group 2 subthemes). An ethnic-studies scholar cited the W.E.B. DuBois idea of “double consciousness,” always seeing oneself through the eyes of another: There are norms of [how] you present yourself in different settings. For folks of color, for women, for other folks who are much more marginalized social groups, you’re always kind of conscious of that, like how to read the room. [It’s] a variation of that W.E.B. DuBois thing about double consciousness. You’re seeing yourself through the eyes of the other. You think about these even in everyday encounters. People read you as Asian. And then an interaction [is] contingent upon, do you speak English well or not, as to how they’re gonna read you.
This was further deepened by acknowledging racialization’s “transnational dimension”: There’s always that . . . transnational dimension . . . of immigrants coming from one sending country to the United States. [It’s] varied but . . . whatever the . . . prevailing tenor of U.S.-Asia relations is has a profound effect on what happens to Asians here. . . . We go to war with Japan, Japanese-Americans are incarcerated . . . anti-Chinese-rhetoric affects what happens with Chinese here. . . . [That’s] part of that unique racialization of Asian Americans . . . [they are] embedded in homeland politics . . . are always . . . seen in the popular consciousness as being tethered to . . . the country abroad.
This global dimension to racialization was further elaborated historically by more long-standing “Western superiority biases” that imposed labels such as “heathen” and deemed Asians as racially inferior: “Modern Chinese writers [from around 1895–1911] were full of self-loathing and a lot of that loathing came from the sense of being [deemed as] racially inferior [by the West in that time period].”
In-between-ness
This theme addresses cultural-frame shifting (CFS; Hong et al., 2000), which is shifting between two or more cultural scripts and applying different cultural interpretive frames and meaning systems to respond and react to everyday situations (Benet-Martinez et al., 2006). Experts from both groups focused on CFS at multiple levels: the individual, interpersonal, group, generational, historical, and clinician-client levels (Table 2, in-between-ness, groupsub themes). This recognizes how AAPIs (i.e., clients, clinicians, clients’ close others) are constantly frame shifting between various cultural norms and learning how to competently and effectively navigate and negotiate these differences: “How confusing it is to bring [hierarchical cultural norms that were passed down] into an egalitarian culture where people call their parents by their first name.”
This also intersected with gender norms and expectations across settings, such as at home (e.g., “don’t come across as brash”) versus a corporate setting (e.g., needing to “prove oneself”). Mental-health experts described how “code-switching” conflicted with the “authentic self” dialogue of therapeutic culture, leading to distress and self-questioning (“Who am I really?”) and that clients benefited from validation. As described by one clinical psychologist, The client said, “I’m a totally different person with my White friends and with my family, hard to navigate where everyone is together.” [He] started to feel like something is wrong that he can have such a different version of himself in two different places, “Am I not integrated? This is a problem.” He felt flipped, stressed out, imagining that he should be a single coherent self at all times, in all places.
Group 2 highlighted the universalism of this “in-between-ness” as a fundamental part of the human experience—that people always feel “out of place,” in exile, never fully belonging, and are constantly experiencing the self as suspended in tension between various value systems. This theme also addresses acceptance, dialectics, and embracing differences. It values multivocality and the coexistence rather than resolution of conflicting beliefs and is situated within the wider historical “homogenizing push” of the European worldview. Treatment goals included EBP concepts of dialectics and acceptance, rejecting binaries, and recognizing one’s “embeddedness” within a multilayered context.
For navigating this in-between, Group 1 described serving as cultural broker between cultures through curiosity and psychoeducation. Interventions drew beyond mainstream EBPs and focused on harmony rather than confrontation. As described by one psychiatrist, “The ‘coming out’ story is a very White phenomenon. Sometimes it’s OK to be quiet about it. . . . There can be a creative adaptability about it.”
Group 2 expanded potential interventions, indicating that “the solution is also proposed as something in-between,” consistent with EBP concepts of dialectics and holding things in tension. A scholar of modern Chinese literature noted acceptance through embracing: “Lu Xun [modern Chinese author] has this famous quote, ‘I am an in-between.’ . . . He basically rejects all labels that have been placed on him, and said, ‘The only thing I embrace is that I am an in-between.’”
Group 1 noted how third-wave CBT drew from Asian philosophies, such as Daoism, and influenced common EBP concepts, such as building tolerance of uncertainty, dialectics, and acceptance, but noted that this is typically attributed only to Buddhism. Practically, this meant guiding clients flexibly with interventions, sometimes requiring the “snail’s pace” of navigating and holding tensions. One psychiatrist described it in the following way: Being there to support the client as they’re testing out new things while being true to what it means to honor their parents . . . a gradual moving and practicing within a collectivist framework . . . there is too much potential of a relational rupture that becomes hard to repair . . . but holding the balance and tension of the bicultural values of your client, and having them remain as congruent to themselves while they’re playing out new behaviors . . . with their parents and relationships.
Another clinical psychologist who uses dialectical-behavior therapy shared a similar approach: I’ll [say], “Oh, actually 20% of this is . . . really good. It’s just . . . the other 80% . . . guilt and obligation . . . OK, 20% of that is good—that’s your wise mind telling you, don’t forget about family. They’re super important to you . . . let’s figure out . . . where does it go off the rails [where] you feel stressed all the time . . . let’s figure out where we went from ‘family is very important’ . . . to I’m stressed for a month before I have to see someone in my family,” so being able to find . . . a sweet spot . . . and not being too quick to be dichotomous or black-and-white.
Group 2 deepened these ideas by placing them within an historical context that rejected the “homogenizing push of the European worldview from the 19th century” that was “intolerant [of] anything different.” As described by an historian of AAPI diasporas, Asia and also Africa has been particularly resistant to any kind of homogenizing. . . . It has been deeply skeptical often . . . [to] not let any kind of homogenizing factor take over. . . . You may have communism and you may have all of these plans, but ultimately there are different languages . . . across China. There are different languages spoken in India, even if you think of Islam and perhaps you can say, okay, for much of at least Central Asia, there is . . . Islam, but the kind of Islam that is practiced . . . and the languages are all different. . . . [T]here is something inherent in that sense about [the acceptance of the] plurality of differences.
Group 2 elaborated on not always needing to seek resolution (Table 2, in-between-ness theme, Group 2 core modification). The same historian described different worldviews: Rather than finding a resolution where everyone is going to be the same . . . that is . . . the great divergence historically between European forms. . . . There is a creative accommodation of differences where resolutions are . . . understanding that you will never be the same as me, but you and I have to work together in this moment . . . for this reason. . . . [T]hat I think is the root of pluralism versus the Western Modern Post-Renaissance moment. . . . The whole point of 19th century imperialism was to bring that level of civilization to the rest of the world . . . so it was racism of a different sort, existed earlier . . . there was only a singular idea of how to be, so it was a single value system, it was a single idea of politics, a single idea of economics and free trade. And that’s singularity, right? The universalism of that singularity. . . . That’s the great divergence between the European mood. . . . The Asian, African . . . is cacophonous, right? And I would actually, include—I don’t know anything about Latin America, but—from what little I know it’s similar, like there’s the cacophony that creates the harmony versus the singularity of . . . we are all the same and the homogeneity.
Emotional-expression reframe
This theme addresses common attributions for AAPI patterns of emotional expression and how to reframe these to counter deficit-based models (e.g., as hypo-emotional or restricted). These attributions include essentialist stereotypes that these qualities are intrinsic to AAPIs, such as the robotic or “inscrutable” Asian, and reflect reified distinctions between independent and interdependent cultures. It also addresses nonverbal emotional expression (e.g., food, rituals to guide emotional processing) and social factors that can contribute to restrained emotional expressions, such as social-display rules. It reframes emotional-expression patterns through a strengths-based and culturally humble lens.
Mental-health experts (Table 2, emotional-expression reframe, Group 1 subtheme) highlighted a Eurocentric overemphasis on specific patterns of emotional experience and expressiveness in relationships, such as overvaluing verbal rather than nonverbal expression and the pursuit of high-arousal positive emotions (e.g., happiness, enthusiasm, pride) rather than low-arousal positive emotions (e.g., calm, peace, contentment). Low-arousal positive emotional states and fewer displays of high-arousal emotions led to AAPIs being misperceived as unemotional (e.g., “a robot”). This was often racialized and pathologized—sometimes dehumanized—by being viewed as unfeeling, stoic, or robotic. A clinical psychologist emphasized how these differences in emotion valuation can be reflected when clients are asked to verbalize emotions: You are going to be inarticulate when you’re asked to [verbalize emotions] or fill out questionnaires . . . if you haven’t been taught to focus on your internal state. You’re coming from a place that’s telling you [your internal state is] important, but it’s not the most important thing.
An affective scientist used a description of suffering following a major earthquake in Japan to highlight essentialist misattributions of AAPI emotion: [Japanese people were] not broadcasting their suffering into high-arousal negative affect . . . [it] can be read as disengagement. . . . East Asians get seen as robotic, because [they are] not broadcasting, [and this] is misattributed to no emotion. . . . There’s an emotional hierarchy in the US: If there’s not high-arousal positive affect . . . then you’re not emotional.
Both groups discussed experiences of war, trauma, and survivorship and how a need to focus on concrete, practical matters rather than internal states was adaptive in context. These responses affirm what Causadias et al. (2018) identified as a cultural-misattribution bias in American psychology in which “culture” is overemphasized in explaining the behaviors of members of ethnic/racial minorities but underemphasized in explaining the behavior of White Americans.
One way to address these misattributions was to broaden conceptualizations of culture beyond ethnicity/race or country of origin (e.g., Cohen & Varnum, 2016) and to understand how these emotion-expression patterns are also common in majority populations. One clinician described how her older White clients also had difficulty recognizing and expressing emotions and that there were regional variations, such as individuals from rural areas or Midwest, and even variability in families. This insight complements research highlighting substantial variability in patterns of emotional expression in AAPI groups even among members of the same subgroup (S. Y. Kim et al., 2013) and immigrant generation (Chen et al., 2015; Williams et al., 2024).
Core modifications include teaching both clinicians and clients to broaden what they are looking for, including understanding biases, valuing low-arousal positive emotions, and recognizing nonverbal expressions of emotion. For helping individuals less familiar with but finding value in verbal emotional expression, core modifications included not pathologizing and instead “scaffolding,” that is, giving language to and guiding the process of emotional expressions. Group 1 experts also highlighted the social-display rules of emotions, such as dampening high-arousal positive emotions (e.g., pride, confidence, or happiness) to avoid inviting envy or jealousy from others. Interdependent “social finesse” was contrasted with U.S. norms, which “requires [one] to be loud and rock the boat, ’cause you get rewarded [for] being squeaky.” These responses align with seminal concepts in cultural psychology, such as contrasts between independent and interdependent self-construals (e.g., Markus & Kitayama, 2010). At the same time, they counter deficit-based perceptions of these emotional displays by emphasizing their social function. For example, affect-valuation theory (Tsai et al., 2006, 2007) indicates that low-arousal emotions facilitate goals of adjusting to rather than influencing others. In this way, low-arousal emotion can be reframed as a strategic means of achieving one’s interpersonal goals.
Likewise, Group 1 reframed restricted emotional expression as containing more nuance, subtlety, and sophistication, given these interpersonal goals. This included recognizing nonverbal emotional expressions, such as “a sound, a look to indicate annoyance,” or their expansion to include behaviors, such as preparing food to express love and affection. One clinical psychologist described being deeply impressed while observing the “nonverbal choreography” of an older Asian couple as they displayed their care. In fact, overemphasis on verbal expression could lead to an “emotionally empty string of words,” as a psychiatrist described: “[It’s like] how people say, ‘Thank you’ and ‘Sorry.’ You said the word but the emotion is clearly not there . . . words [are] only a part of communication . . . it’s very different in different cultures.”
Both groups highlighted how differences in emotional expression should be viewed in terms of impairment on functioning rather than discrepancy with mainstream culture given how “the reference point is European-American” (Table 2, emotional-expression reframe shared theme). Group 2 further extended the social function and value of emotions by emphasizing the role of balance and moderation with the full range of emotional experiences and expressions, including shame (Table 2, emotional-expression reframe, Group 2 core modification). As one Confucian/Daoist scholar described, “Shame [is] a sign that we have [an] ability to tell good from bad. . . . A way to think about this concept . . . already exists. They . . . actually use the term ‘name’ or ‘fame.’ Like they are all the same word.”
Beyond verbal emotional expressions, an historian acknowledged Asian rituals (i.e., dance celebrations, wailing at weddings) and how they facilitated emotional processing and expression. Funeral ceremonies, instead of verbal expression, contained ritualized, social (i.e., ceremonial), and daily behavioral actions to process grief: These ritual ceremonies are about creating this gradual separation between the living and the dead . . . a concern . . . that you need the proper amount of time to process this emotion . . . the emotion as something that needs to be processed and . . . change[s] in daily routine [i]s a way of helping that process. And then . . . you can transition back to normal life, after a given period of time.
Benign entry points
Both groups described ways to foster deepened connections with—and understandings of—self and others through indirect means. This goes against the more “direct” approaches of EBPs, which assumes that clients can report accurately and exhaustively about themselves and their family history. Experts described how for many AAPIs, family histories are silenced or remain unknown (e.g., about intergenerational trauma, poverty, older generations’ experiences of racism). An indirect approach, described as “healthy triangulation,” used extended family (e.g., aunties, uncles, cousins), close others, and popular media to broach difficult topics or provide psychoeducation (Table 2, benign entry points, Group 1 core modification): “They have to ask somebody else if they can . . . [the] family story doesn’t just come from one person.”
Both groups emphasized how popular media, including books, film, and articles—even peer-reviewed academic articles—could provide psychoeducation, common language, a sense of connection, and self-reflection when family stories or historical narratives are unavailable (Table 2, benign entry points, Groups 1 and 2 core modifications). As two clinicians described, “Parents are not talking about this history and so [clients] have to learn about it on their own” and “Psychoeducation around a meta issue that parents don’t communicate a lot. . . . [There’s] no guidance around being bicultural.”
One clinical psychologist shared peer-reviewed articles, such as Markus and Kitayama (2010) article describing interdependence. Group 2 extended this to the use of literature and history: “It opens up a different way of looking at your parents, communicating outside of just the parent-child bond. . . . [They’re not] people who are just holding you back or want you to live a certain way.”
Both groups often used external material in sessions and coursework for powerful, indirect ways of communicating about racism and trauma, and learning about historical events, including memoirs such as The Best We Could Do (Bui, 2017), the Pixar-animated short Bao, a questions-focused card game (Visram, 2021), and a Filipino disco band called The Boyfriends. This was recommended as a way to broach difficult topics, such as sexual orientation. As described by one MFT, “Maybe there are informal ways that [the client] can introduce the topic, right? Like, watch an LGBTQ movie with your parents [as a way to] broach the topic.” Group 2 also described using external material to open up conversations about topics that otherwise would have been difficult. As described by one historian, “It can start with just reading the history and historical circumstances and those topics allow certain conversations to begin . . . oftentimes people don’t know how to start a conversation [about their parents’ history].”
Group 2 experts noted the “accidental therapy” that occurred in their college teaching, particularly how material helped students understand their parents, humanizing them. As one political scientist described, I might say . . . I’ll introduce you to a couple of disco songs that your dad might have heard growing up . . . because I do believe that . . . pop culture is so democratizing, especially the Filipino pop culture of the ’70s and the ’90s, for these two decades in the Philippines, people listened to the same stuff . . . which is very rare in Filipino culture, where people, where the elite . . . listen to the same stuff. . . . So I would just say, let’s go through this really democratic music and this is a way to connect with someone. And, in fact, this is how I end my class . . . “I gave you all this pop culture. What are you gonna do with it? Connect with the Philippines, and see where it takes you . . . let’s not get into the dicey [political, dictator] stuff. Just listen to this disco [music]. Just tell your dad that you learned about this in my class and see where that takes you.”
Another literature scholar described a similar approach: One thing I always tell students is that they should talk to their parents . . . because oftentimes . . . you don’t know about your own family history, right? Your parent is just that parent you’re rebelling against, and then, once the conversation opens up, and they find that the parents actually have these interesting and sometimes very traumatic life stories, that opens up a different way of looking at your parent. . . . These were works of literature that their parents read, but they would never have access to these works had they never taken a class . . . [they develop a] different way of seeing oneself and seeing one’s parents and relate in a different way that can create certain kinds of breakthroughs.
Against cultural essentialism
Long-standing emphases on so-called cultural pillars of AAPI worldviews (e.g., Confucianism, collectivism) have contributed to cultural essentialization and the reification of differences between AAPIs and other ethnic/racial groups (Okazaki, 2018). An essentialist view sees culture as “a core set of unchanging values, behaviors, practices, and norms that are immune to structural changes” (J. Lee & Zhou, 2014, p. 41). These processes were captured in the theme against cultural essentialism (Table 2), in which respondents emphasized the dynamic nature of cultural forces and a broader conceptualization of culture itself. Group 1 experts noted shifting norms both in the United States and sending countries, including socioeconomic changes, urbanization, “Gen Z culture,” and social media, which have expanded what has traditionally been identified as “cultural” forces shaping psychological understandings of AAPIs (Table 2, against cultural essentialism, Group 1 subtheme).
In addition to resisting attempts to essentialize ethnicity/race as culture, both groups highlighted its nonstatic aspects—that is, that culture is always in a state of flux. Clinicians noted how acculturation concepts presume a distance from the home country, but with increasing globalization and contemporaneous connections through social media and messaging platforms (e.g., Line, WhatsApp, WeChat), AAPIs and their families are constantly responding to changes and negotiating or even updating identities through connections between home and host countries. Countries of origin were described as “dynamic and messy places.”
Generational differences were also salient. Emphases on self-esteem and emotional intelligence were viewed as relatively recent phenomena globally, especially in urban areas and with high rates of social media use. One clinical psychologist described South Korea’s Generation Z as more individualistic “than even Americans” and how economic factors and housing availability primarily drove decisions to live with parents as adults. A cultural sociologist noted how “Gen Z is Gen Z everywhere,” with its own cultural script that transcends geographical location. Both groups also acknowledged societal change and socioeconomic factors shaping traditional ideas about family responsibility. As one historian noted, My generation, my parents’ generation, we are . . . one of these first generations of people . . . growing up in the urban context . . . after 50 years . . . so everyone is . . . figuring [it] out. . . . The reality of urban life is that . . . you might not live in the same city as your parents . . . the social expectation is that people take care of their parents when they’re old, but . . . there’s also a recognition that this is not always the option and . . . [some] senior citizens are also starting to think that maybe it’s not, the most enjoyable thing to live [with their adult children] . . . they also want their freedom.
Experts from Group 2 pointed out cultural essentializing tendencies in psychology, as viewed from outside disciplines (Table 2, against cultural essentialism, Group 2 subtheme) Socioeconomic factors and urbanization affected family conflicts and challenged the “achievement frame” typically used to describe AAPIs. As one cultural sociologist described, To a large degree it’s always been a tug of war between generations but now . . . Gen Z is feeling more economically precarious. . . . The structure of the economy has made it much more difficult . . . to attain that kind of economic mobility. . . . Even in academia, it’s not such a secure job anymore for everybody . . . with that in mind . . . [many] young Asian Americans are . . . willing to just sort of opt out of the rat race.
Likewise, Group 2 experts questioned static notions of Confucian filial piety. An historian described how filial piety has become an overemphasized notion partly because of political appropriation by the state: You’ll hear that a lot . . . like there was Confucius like 2,000 years ago and . . . everything’s been unchanged since then and . . . everyone’s still Confucian. I don’t believe that at all. I do think that that paradigm of the social role is . . . your main identity . . . you have to act like an ideal father and child . . . but . . . you do have to bring in the socialist context because that structure is still in place.
Group 2 provided alternatives to cultural essentializing, that is, the use of cultural scripts: I’m very, very attuned to the internal differentiation of the tools that people have access to. So that’s really a very important difference [between cultural sociology and cultural psychology]. . . . It’s more of these internal threads that maybe transcend multiple cultures. It’s not this group versus that group. But . . . finding unwinding and adding some of those common threads. . . . Instead, you say the environment offers tools that people can . . . draw on to make sense of situations. So it involves a concept of agency that’s much more active and the two societies have elements of individualism and interdependency but maybe in one context one set of tools is more present than another . . . instead of emphasizing a clear distinction between societies, it’s more you have a number of tools that are available, but more or less available. . . . And some ways that approach makes it more malleable too. There’s a little bit more room than to change.
Group 2 focused on integrating multiple cultural scripts. For example, a political scientist described the “multiple discourses” of Filipinos as being English-speaking (which allowed easy access to U.S. culture), “Confucian but less Confucian” than Asians, Catholic, and more Western than other Asian countries given their colonial history. This resulted in strong family ties—a kind of filial piety but different—and strong values of Western political liberalism and U.S. patriotism, which could lead to intergenerational conflict related to political views.
Having these multiple scripts allows for the creative “reformatting” of cultural scripts that contributes toward the individuality in AAPI subgroups. One diaspora studies scholar noted the following: What constitutes a diaspora . . . ultimately, is a group that has a homeland, a place they or their ancestors came to and that place continues to . . . frame their being, either in terms of actual physical contacts and going back and forth . . . geographical, rooted territory . . . that’s one aspect of it. But not the only one, ’cause . . . what they do carry with them are their names. They carry with them their religion. And they carry with them their food, which again gets sort of reformatted [as they adapt and acculturate]. . . . There’s also the emotion in the memories . . . language that continues, the songs, festivals . . . a history that sort of remains . . . a memory, a collective memory, which continues to make them South Asian and then . . . the external factor . . . a colonial state . . . in the Caribbean that really did racially demarcate you for everything.
Taken together, this theme allows clients to view themselves and their close others with flexible notions of culture rather than an intrinsic, static, or unchanging quality inherent to AAPIs (e.g., filial piety, gender norms). It allows for more possibilities of what culture can mean and its associated actions or responsibilities through the mixing and matching or “reformatting” of cultural repertoires. It provides room for how individuals and their close others might change over time. It also centers SES, social media, and global interconnectedness, which significantly shape cultural scripts and are often overlooked in EBPs.
Expanded definitions of well-being and thriving
This theme described expanded definitions of well-being for AAPIs that went beyond goals of symptom reduction that are typical of empirically supported treatments (ESTs). In contrast to ESTs, goals emphasized balancing the three components of EBPs (i.e., best available research evidence, clinical expertise, and client characteristics, culture, contexts, and preferences; APA Presidential Task Force on Evidence Based Practice, 2006) and broadening outcomes to include real-world functioning, quality of life, recovery, and patient-centered outcomes based on lived experiences (Fusar-Poli et al., 2022; Kazdin, 2000; Kilbourne et al., 2018; McKnight & Kashdan, 2009).
Group 1 experts described well-being as a “by-product” of engagement with others and being resilient through challenges. There was significant emphasis on family and social connectedness, viewing these as a source of pride and meaning: “It’s social relationships, it’s connection with families, participating and figuring things out. There are obstacles and they’re overcoming them . . . a high level of engagement . . . not taking themselves out [of the situation].”
Dialectics also informed these definitions, as described by one affective scientist: “It’s more of an understanding that the negative is braided in with the positive . . . it’s unrealistic to have only positive emotions. Negative emotions give meaning to the positive one . . . tolerance of negative emotions.” It was also holistic, with an emphasis on being multidimensional and comprehensive, inclusive of functioning across many domains, and some experts cited the eight domains of well-being described by the Substance Abuse and Mental Health Administration (2016).
Group 2 highlighted how historically, this holistic emphasis was described as the Confucian ideal of the “gentleman, 君子” which valued rich “interiority” and individual agency and freedom. The gentleman was characterized by being moral and well-rounded, demonstrating excellence in the arts, music, poetry, education, and physical competence: What’s nice about these early texts is their notion of [wellness] is very relatable. Our [current] value system tends to emphasize wealth and power. [But in these texts] . . . it’s really more about your individual perception, how you govern yourself and your emotional equilibrium . . . your sense of this upward trail towards moral development, regardless of circumstances. . . . As a result of this cultivation . . . [there’s] a charisma. These people . . . you meet them and you just have a sense that they’re different . . . they’re literally glowing, they’re described in one text as “jade-like.” Confucius is portrayed emphasizing enjoyment. [He] was able to enjoy studying ancient classics, enjoying music, ritual dance performance, and there is that sense of joy in that conception of a person doing well.
This was contrasted with the “dehumanizing view of personhood of Western science,” which was associated with objectification, that is, humans being useful and for only practical purposes. As an historian described, “When Western science was introduced to China . . . there’s always . . . in Chinese discourses, a distinction between . . . the opposite of ‘the Way’ . . . is . . . a ‘vessel’ or ‘instrument.’ A gentleman cannot be instrumentalized.”
Group 2 also highlighted the outward impact of individual wellness. This went beyond “just individual skills” but had a wider impact on society and the community (Table 2, expanded definitions of health and well-being, Group 2 core modification and treatment goals). A similar idea of wellness was situating oneself within the ethnic/racial “contours of U.S. society,” which included “enhancing [one’s] social consciousness” by understanding the “weight of history” and knowing how to contribute or pay it forward. Daoism similarly assumed that individual transformation affected those around them: [T]he Daoists are . . . similar in essence . . . its portrayal of these ideal figures or people who find joy . . . they just see it as part of a natural transformation of the world . . . and yourself, you transform the people around you . . . one possibility is . . . the daughter can . . . change . . . her family . . . by doing well herself, and have this influence on her family. That in turn, has influence on the neighbors, so it’s like this . . . butterfly effect.
Discussion
This qualitative synthesis from mental-health experts and nonpsychology experts highlights several areas for EBP modifications. We situate these themes within the CTAF (J. Chu & Leino, 2017) and identify core and peripheral modifications that can be incorporated into an individualized case formulation (Persons, 2012). Modifications had overlap with culturally adapted approaches, such as the CARS model (J. Chu et al., 2013), with its emphases on acculturative stress, interpersonal relationships, and discrimination. We summarize a few applied takeaways.
Interdependent Values, Social Location, and the Contextualization of Self and Others
First, the emphasis on bringing in wider interdependent contexts, such as family, into EBPs is not new, especially for AAPIs (e.g., S. B. Kim & Lee, 2021). But our results highlight how interdependence should be integrated at a more fundamental level, as both peripheral and core modifications. In addition to bringing in the perspectives of important others, the very notion of selfhood had interpersonal dimensions (e.g., social roles). In this light, caring much about the opinions of and feeling responsible for others might be viewed as normative rather than pathological. For clients with these interdependent values, EBPs can focus more on strengthening interpersonal ties and addressing interpersonal conflicts in direct and indirect ways even if the focus of psychotherapy is primarily individual. Our results provide alternatives to the more direct, confrontational approaches for dealing with interpersonal conflicts in mainstream EBPs, which may, in turn, provide greater opportunities for corrective emotional experiences and improved relationships.
Our results also shift the goals for interpersonal conflicts. Rather than the typical EBP focus on individual happiness, asserting needs, or conflict resolution, adaptations had a slower, more indirect approach, characterized by holding tension between protecting “lifelong” relationships, embedded within a larger interpersonal context of family and extended family, while maintaining individual agency. Concepts of dialectics, acceptance, balance, and tolerating tension are familiar CBT concepts but also consistent with Confucian/Daoist values and further echoed in themes related to the creative accommodation of differences. Moreover, these familiar third-wave CBT concepts are applied to the interpersonal domain: that of the incremental, ongoing, skillful navigation of relationship issues, with careful attention to repercussions in the self and wider interdependent contexts. This was likened to couples or family therapy with one person in which a therapist brings these relationships directly into the therapy room. There is some limited research on the effectiveness of family therapy with one person, focusing on Cuban American families, and this work redefined family therapy as a “treatment modality in which the therapist’s interventions target on changing family systems, regardless of who is present at a particular therapy session,” noting that this can include a single individual (Szapocznik et al., 1983, p. 890). When interdependent values are viewed as fundamental, treatment goals are expanded to include deepened empathy and building a sense of agency amid deep interconnectedness. Rather than individual well-being, there is recognition that an individual who remains deeply interconnected will need greater empathy, more tolerance of tension, a process for working out differences, perspective-taking, and a greater capacity to accept and embrace differences. Relational ruptures are still possible, but they are ones whose consequences have been carefully thought through.
To provide a case illustration of modifications, imagine a second-generation, Muslim, heterosexual AAPI woman who is experiencing depression and anxiety as a result of family tension because of dating a nonreligious, non-AAPI partner whom she is seriously considering marrying. Receiving standard EBP, she might (a) learn that she has a medical diagnosis; (b) explore in therapy what she really wants, understanding that she needs to be true to and take care of herself; (c) pathologize her parents for being too strict, religious, and racist; (d) blame them for not truly loving her because they undervalue her individual happiness; and (e) learn to assertively communicate her needs by expressing her decision to marry. Although an oversimplified case scenario, it is easy to see how this could lead to relational ruptures in the family and beyond in the short-term and perhaps even poor mental health in the long-term.
Instead, modifications related to interdependent contexts, in-between-ness, against cultural essentialism, and benign entry points instead provide alternative paths and greater creativity in options than a standard EBP might suggest. With this modified EBP, she might instead (a) learn about acculturative stress and intergenerational cultural conflicts; (b) situate her parents in their social location, as religious minorities who fled violence in their country of origin, with limited English fluency; and (c) situate herself as a second-generation adult child of immigrants growing up in multicultural society characterized by religious freedom and emphasizing personal fulfillment and autonomy. For dealing with this interpersonal conflict, a clinician might use benign entry points to guide the client toward confiding in a trusted relative of the same generational status (e.g., an aunt or uncle), who might then start to bring up similar topics to her parents indirectly (e.g., “Your daughter is getting older and should get married soon. What if she decided to marry someone who is not Muslim?”), understanding that cultural scripts are flexible, malleable, and open to influence. She might reach out to a trusted imam or acquaintance at her mosque who married a non-Muslim. The clinician might guide her in considering a range of graduated, individually specific solutions, such as keeping the relationship a secret for some time; slowly inviting her partner under the guise of “a friend, an old classmate” to various family or religious gatherings; watching a movie with her parents about interracial dating; and also considering marrying him anyway, although now only after careful consideration about the interpersonal repercussions and personal consequences of this decision over the short-term and long-term. All solutions are collaboratively considered, developed, and vetted by the client, who understands her interpersonal context best.
Second, the sociological concept of social location of self and others appears especially important because it addresses several acculturative-stress and intergenerational cultural-conflict issues that are known to affect psychopathology (e.g., P. P. Lui, 2015). Although similar concepts are discussed in health-equity research (e.g., Ford & Harawa, 2010), this is rarely integrated into applications for EBPs and much less often directly applied toward clients’ interpersonal relationships. Relatedly, although acculturative stress has been in the psychological literature for some time, it is not well integrated into EBPs. In some ways, EBPs do the opposite of what the acculturation literature might show—drawing from a single cultural reference point, especially when it comes to norms around emotional expression and relationships. Our results incorporate into EBPs acculturative-stress-resilience concepts of bicultural identity and bicultural competence (Ferguson et al., 2023). Themes around reframing emotional expression, racialization, and in-between-ness highlight the multiple frames of reference from which AAPI clients draw and also help with pinpointing the social location of self and others. The theme of racialization in therapy further adds the dimension of code-shifting and discrimination, concepts not well integrated into cultural-competency trainings (W. Chu et al., 2022).
Clinically, adult AAPI clients often present with “unfinished business” related to interpersonal cultural conflicts (e.g., with a traditional, less acculturated parent), leading to stress in the family and larger interpersonal system. As a first step, enhancing the clients’ ability to consider additional perspectives, shift their cultural frame of reference, and socially locate their parent through history and immigration experiences may help to deepen understanding. It may also help with attributing problems to external factors (cultural differences, societal racism, intergenerational trauma) rather than to the internal attributes of the parent (e.g., “he is too strict”). Common childhood experiences, such as low perceived warmth from parents (e.g., “she never said, ‘I love you’”), having significant responsibility (e.g., language translation for parents, caring for younger siblings), emphases on academic achievement, or addiction problems, often lead to feelings of resentment as an adult. Humanization of others might occur when contextualized in the light of immigration stories, discrimination, socioeconomic precarity, tenuous citizenship status, academic norms in the sending country, and intergenerational trauma. This shift is consistent with bicultural-effectiveness training approaches (e.g., Szapocznik & Williams, 2000) that seek to attribute stressors to external, acculturation-related factors (e.g., Hispanicism vs. Americanism) rather than dyadic factors (e.g., parent vs. child). That is, it shifts problems from personal blame (i.e., parents, client) to external and situational attributions (i.e., acculturative stress, racism/discrimination, poverty, war).
Third, several of the themes cast a critical gaze on assumptions within EBPs. Although stigma and mental-health literacy are cited as barriers to engagement with mental-health services among AAPIs, it is worth considering the value of nonbiomedical framing of mental health as a peripheral modification to EBPs. Cultural anthropologists have long criticized biomedical models, sometimes described as the medicalization of suffering (e.g., Kleinman, 1997). Increasingly, mental-health experts are valuing the lived experiences of consumers to improve treatments, using bottom-up approaches to capture the subjective suffering of psychosis (Fusar-Poli et al., 2022), depression (Fusar-Poli et al., 2023), and adolescent mental health (Fusar-Poli et al., 2024). Given what is known about equifinality and nature and nurture for mental disorders, clinicians might benefit from integrating nonbiomedical scripts. This might include embracing explanatory concepts such as “thinking too much” (Yang et al., 2010) while understanding their impacts (e.g., social inclusion, whereas a diagnostic label might lead to social exclusion; engagement in therapy as a way change unhelpful “thinking too much”). This could also include stretching the setting and frame of therapy beyond clinics, integrating community-based and nonspecialist approaches, such as a church-based suicide program (Molock et al., 2008), the friendship-bench intervention in Zimbabwe (Chibanda et al., 2016), and barber-shop studies in the United Kingdom (Ogborn et al., 2022).
Likewise, cultural-essentializing tendencies in psychology were named explicitly. This perspective is supported by research indicating that differences in psychological processes in AAPI groups can be attributed to variations in income, education, and other indicators of social status (Chaudhry & Chen, 2019; Chen & Zhou, 2019; Tao et al., 2013). An alternative approach may be drawn from cultural sociology through its use of cultural scripts or repertoires. This core modification to EBPs may help with individualizing AAPIs and provide a more granular way for integrating fluid notions of culture, different experiences of acculturation, and an individual’s adaptability within a given context. Furthermore, it allows for the creative malleability and “reformatting” of cultural identities, especially with mixed-race individuals who are increasingly common among AAPIs (Pew Research Center, 2021). Relatedly, racialization of AAPIs in psychotherapy occurred in explicit and sometimes implicit ways, such as through its deficit model of emotion expression. Recognition of these tendencies in the field and providing education and awareness to clinicians and clinical training programs are peripheral modifications that will ultimately benefit clients and reduce the number of these experiences. Reframing emotion-expression differences and emphasizing the fluidity of cultural scripts (e.g., around filial piety) and direct conversations about racism in session may also create greater freedom and possibilities for individual clients and protect against static notions of culture that both clients and clinicians may hold.
Fourth, nonpsychology experts shed a global, historical, and class dimension to potential biases in mainstream EBPs, such as the “homogenizing push” of a Western worldview, Western superiority biases, and the “therapeutic culture” zeitgeist and related cultural scripts of Gen Z (e.g., Zilberstein et al., 2023). Our results suggest that mainstream EBPs are developed in a particular context and may offer some practical steps toward “decolonizing” biases. This emphasis on contextualization also appears helpful for more precisely individualizing EBPs.
It also reflects a key distinction between two understandings of Bronfenbrenner’s bioecological model: an earlier versus a more mature version—the former is limited to describing contextual influences, and the latter highlights interactive components of the person who is in the process of developing and making “sense of the world and their place in it” (Tudge et al., 2009, p. 200). As described by Tudge et al. (2009, p. 199), Bronfenbrenner “later engaged in self-criticism for discounting the role the person plays in his or her own development and for focusing too much on context.” The mature Bronfenbrenner model is described as the process-person-context-time model and stresses person-context interactions and the processes of a developing person contextualized by time. This conceptualization appears to be reflected in the ways experts described clients navigating and negotiating their in-between-ness, clinicians recognizing the larger Western and White biomedical frame of psychotherapy, and family members being contextualized within their specific histories, immigration trajectories, and time frames (e.g., racism in the 1980s). In all of these, interactions among personal characteristics, proximal processes, contexts, and time yielded a unique, present individual still actively navigating and negotiating. This mature Bronfenbrenner model also incorporates wider “Gen Z” tendencies and global diffusion of “therapeutic culture” and makes space for the digital or virtual contexts in which influence also occurs, another area in which EBPs have had little to say. The process emphasis of this mature model allows for the malleability of cultural scripts and constant state of flux of concepts such as “filial piety” as it is subject to economic, urbanization, generational, and similar pressures.
Finally, the expanded treatment goals and definitions of well-being had a wider contextual dimension. These goals were interdependent in nature, including deepened empathy and compassion for self and others, cultural humility, heightened social consciousness, and tolerance of tension, dialectics, and acceptance of differences. As the world becomes increasingly interconnected, such skills may be especially adaptive for navigating one’s current context.
Limitations and future directions
Although we sought representation among AAPI subgroups among our experts, the majority of our experts were from East Asian backgrounds. For mental-health experts, we did not gather information about the AAPI subgroups with whom they work primarily and instead relied on their expertise with the larger AAPI category; however, we did include expertise specifically for PI and Southeast Asian refugees, who can be underrepresented in AAPI research. We also sought diversity in severity of the clinical populations treated, ranging from common mental disorders to suicide and severe mental illness. Likewise, for participants from nonpsychology backgrounds, we sought representation among Asian and AAPI issues, including Southeast Asian refugees, South Asian, and PI groups; however, the majority similarly studied East Asian issues. Given the importance of subgroup differences, some of the adaptations in Table 2 may not be applicable to all subgroups. Future studies should explore subgroup-specific adaptations and oversample from those subgroups and experts from underrepresented groups in AAPI studies. Given the growing importance of data disaggregation in AAPI mental health, future research should clarify subgroup-based nuances and contextualize these group-based differences.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251392853 – Supplemental material for Expanding Psychotherapeutic Intervention Frameworks for Asian American and Pacific Islander Mental Health: Qualitative Synthesis of Multidisciplinary Perspectives
Supplemental material, sj-docx-1-cpx-10.1177_21677026251392853 for Expanding Psychotherapeutic Intervention Frameworks for Asian American and Pacific Islander Mental Health: Qualitative Synthesis of Multidisciplinary Perspectives by Nancy H. Liu and Stephen Chen in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Shirley Wang
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.