
Abstract
Air pollution is a leading threat to human health but has been largely overlooked in the study of psychopathology. As the burden of poor mental health grows, a consideration of new contributors to psychopathology is needed to identify novel prevention and intervention approaches. Consequently, collaboration between clinical-psychological scientists and experts in atmospheric research, pollution, and built environments holds great potential for advancing knowledge and addressing these threats. In the current project, we bring together a cross-disciplinary team to summarize the state of existing research linking air quality to the development and maintenance of psychopathology. We then identify some traditional challenges to collaboration across disciplines before identifying promising areas for future research and providing concrete advice to psychological scientists interested in similar collaborations, including recommendations for the measurement and application of outdoor and indoor air quality, ways to strengthen causal inference, and considerations for environmental justice.
Exposure to poor air quality is one of the greatest known threats to human health, causing the premature deaths of approximately 7 million people globally every year (World Health Organization [WHO], 2022). According to WHO (2022), nine out of every 10 people in the world breathe air that contains unacceptably high levels of pollutants, putting them at risk for physical illnesses, including cardiovascular disease, stroke, asthma, respiratory infections, cancer, and chronic obstructive pulmonary disease (e.g., Dominski et al., 2021; Landrigan, 2017). For example, even in economically wealthy regions, such as the European Union, 97% of urban populations breathe air with levels of particulate matter (PM) of aerodynamic diameter less than 2.5 µm (PM2.5) above the thresholds recommended by WHO (European Environmental Agency, 2021).
Recognizing the scope of the problem, many nations are attempting to implement policies explicitly designed to reduce air pollution by regulating human-generated contributors (e.g., Jonidi Jafari et al., 2021), such as fossil-fuel emissions and industrial practices, with varying success. The physical-health effects of select indoor and outdoor air pollution are well documented and robust (e.g., Sørensen et al., 2003) and include, among other consequences, effects on immune processes, the hypothalamic-pituitary-adrenal (HPA) axis, and central nervous systems—all of which are implicated in the development of mental-health disorders as well. However, despite these pathways, substantially less attention has been given to the mental-health effects of exposure to poor air quality to date, resulting in a potentially significant gap in knowledge and overlooked opportunity in clinical-psychological science.
Such an oversight is notable given that the global burden of psychopathology is growing (GBD Mental Disorders Collaborators, 2022). In the most recent worldwide estimate, 980 million people met criteria for a psychological disorder in 2019 (WHO, 2022). Consequently, the identification of novel contributors to mental disorders is of paramount importance to intervene, reduce risk transmission, and reduce suffering and economic burden caused by psychopathology. Collaboration between clinical-psychological scientists (i.e., scientists working to understand clinical-psychological problems and phenomena), epidemiologists, building engineers, air-quality researchers, and environmental, transportation, and energy regulators, therefore, holds great potential for advancing knowledge and addressing these threats. However, existing collaborations among these disciplines are rare for multiple reasons, including a lack of shared understanding between the professions.
The purpose of this consideration of mental health and air pollution is to promote new collaborative research by (a) describing the current state of the literature, (b) identifying historic challenges to research, and (c) providing recommendations and resources for multidisciplinary collaboration for clinical-psychological scientists drawing on insights from a team of clinical psychologists, atmospheric researchers, and building engineers. Through innovative collaboration, we believe science can better understand and address the role of air quality in contributing to the onset and maintenance of psychological disorders.
The State of Current Knowledge
Our supposition that exposure to poor air quality places individuals at risk for symptoms of psychopathology and poor mental health is guided by a theoretical model in which exposures to problematic levels of air pollutants induce a variety of biological responses that, in turn, increase the individual’s risk for psychopathology (see also Bhui et al., 2023; Reuben et al., 2022). Reflective of a developmental life-course perspective (e.g., Beauchaine et al., 2018; Evans et al., 2013; Vergunst & Berry, 2022), associations at each place in the model depend on the extent and type of the exposure, developmental stage of the individual, and interactions with a variety of other genetic and nongenetic risk and protective factors (as depicted in Fig. 1).
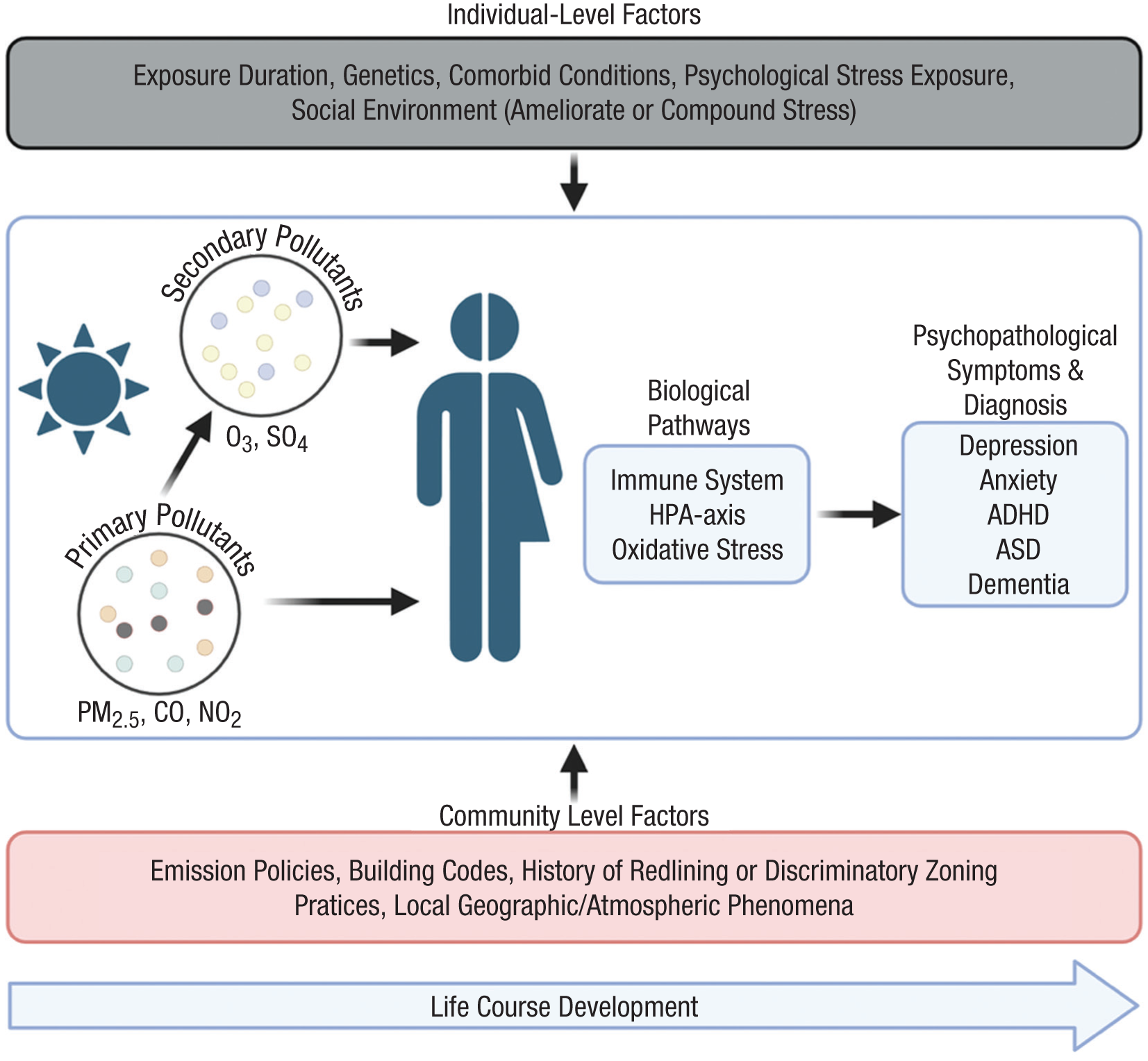
Schematic of theoretical model guiding possible associations between air pollution and psychopathology.
In support of this model, we summarize the current state of knowledge on air pollutants, observed associations with a variety of mental-health outcomes, and theorized biological mechanisms. What follows is not intended as an exhaustive systematic review but, rather, a synopsis of the most notable, rigorous, and/or consistent findings. When possible, we direct readers seeking more information to specific systematic reviews and meta-analyses on the relevant topics.
Overview of air pollutants
Air pollutants can be classified into two categories: primary pollutants and secondary pollutants. Primary pollutants (e.g., nitrogen dioxide [NO2], carbon monoxide [CO], black carbon) are atmospheric constituents that are directly emitted to the atmosphere through a variety of human activities, including industrial and agricultural practices, energy generation, transportation, mining, residential cooking and heating activities, wildfires, and so on. Secondary pollutants (e.g., ozone [O3], sulfate) form in the atmosphere because of reactions among primary pollutants in the presence of sunlight.
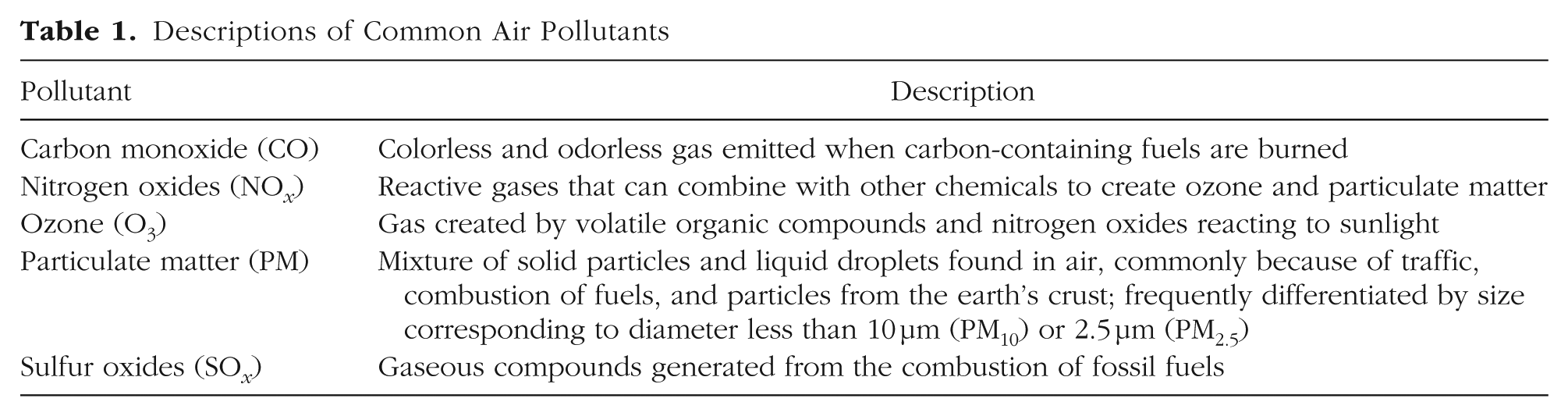
Research on air quality has identified a range of specific air pollutants that are relevant to human health. Common air pollutants include CO, NO x , O3, PM, and sulfur oxides (SO x ). These pollutants vary in both chemical structure and properties and their impacts on human health. As summarized in Table 1, O3 is a gas created by the photochemical reactions among pollutants (i.e., volatile organic compounds and NO x ) in the presence of sunlight. Exposure to O3 is linked to a variety of physical-health risks, including respiratory and cardiovascular diseases and premature mortality (Nuvolone et al., 2018). PM is a mixture of solid particles and liquid droplets found in the air, which can include metal air toxicants, inorganic components (e.g., sulfate, nitrate, and ammonium), black carbon, organic carbon, dust, or dirt. PM is often differentiated by its aerodynamic diameter to note PM smaller than 10 µm (PM10) or 2.5 µm (PM2.5), corresponding roughly to coarse- and fine-mode inhalable particles, respectively. Fine and ultrafine particles are seen as particularly hazardous because they can more deeply penetrate the lungs and enter the bloodstream. Primary contributors of PM pollution include road traffic, combustion of fuels, and particles from the earth’s crust (Mukherjee & Agrawal, 2017). Exposure to PM is associated with birth defects, cardiovascular and respiratory diseases, and inflammatory responses (Mukherjee & Agrawal, 2017). NO x are highly reactive gases that can combine with other chemicals in the air to produce O3 and PM. Health effects include increased rates of cancer, birth defects, respiratory-tract infections, diabetes, and impacts to the immune system (Hakeem et al., 2017). CO is a colorless and odorless gas emitted into the outdoor air when vehicles or other machinery burn fossil fuels. CO can be lethal in high concentrations and is associated with a variety of health concerns, including cardiovascular diseases and developmental effects (Raub, 1999). SO x are gaseous compounds generated from the combustion of fossil fuels at power plants and industrial facilities. SO x are associated with impacts to respiratory, cardiovascular, and nervous systems; diabetes; and mortality (Khalaf et al., 2024).
Descriptions of Common Air Pollutants
In addition to these common pollutants, there are additional pollutants known to have clear toxic effects (i.e., to cause cancer or other serious health problems) for living organisms, which are associated with additional levels of regulation by governing bodies. In the United States, the Environmental Protection Agency (EPA) has identified 188 hazardous pollutants that must be regulated under the Clean Air Act (U.S. EPA, 2015), including metallic compounds, such as lead, antimony, and arsenic. Furthermore, the EPA’s Air Toxics Screening Assessment, based on 2018 emission inventory data, identified the following 12 air toxicants as being most relevant to physical-health outcomes (contributing to 98.3% of estimated cancer risk associated with air pollution): formaldehyde, carbon tetrachloride, benzene, acetaldehyde, naphthalene, ethylene oxide, polycyclic aromatic hydrocarbons and polycyclic organic matter, 1,2-Butadiene, hexavalent chromium, ethylbenzene, inorganic arsenic compounds, and nickel compounds (U.S. EPA, 2022).
In sum, air pollutants may have a broad range of health impacts depending on the type of pollutant, form of exposure (e.g., inhaled or ingested), and quantity of exposure (Manisalidis et al., 2020). Here, short-term (acute) exposure generally refers to exposures that happen on the scale of hours, days, or weeks. In contrast, long-term (chronic) exposure generally refers to exposures that happen on the scale of months and years.
Despite previous research that has shown exposure to both common and/or toxic air pollutants are risk factors for negative physical-health outcomes, the extent to which these pollutants also relate to mental-health outcomes is less studied.
Mental health and air quality
Clinical-psychological scientists address the study of mental health and disorder both through diagnostic-level (categorical) and symptom-level (dimensional) approaches. The most common taxonomies are derived from the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2022) in the United States and the 11th edition of the International Classification of Diseases (ICD; WHO, 2019) outside of the United States. In both, disorders that share common features (e.g., those involving disturbances related to mood) are clustered together, resulting in categories such as mood disorders, anxiety disorders, schizophrenia spectrum disorders, and substance use disorders, among others. Higher-order categories of internalizing versus externalizing disorders are sometimes used to acknowledge similarities between disorders that largely manifest as distress and dysfunction experienced internally (e.g., worry) versus in ways that are outwardly visible (e.g., anger outbursts). Additional superorder structures, including the psychopathology or p-factor, have also been proposed to reflect an underlying susceptibility for any symptoms of psychopathology (Caspi et al., 2014).
The most recent global estimates of disease burden and prevalence for 12 common types of mental disorders across 204 countries notes that anxiety disorders are the most prevalent form of psychopathology, affecting an estimated 301.4 million people in 2019 (GBD Mental Disorders Collaborators, 2022). This is followed by depressive disorders (279.6 million), personality disorders (117.2 million), idiopathic developmental intellectual disability (107.6 million), attention-deficit/hyperactivity disorder (ADHD; 84.7 million), conduct disorder (40.1 million), bipolar disorders (39.5 million), autism spectrum disorders (28.3 million), schizophrenia (23.6 million), and eating disorders (13.6 million).
Below, we highlight some of the most consistent, notable, or rigorous findings related to associations between air quality and different forms of psychopathology.
Air quality and internalizing disorders
To date, a large portion of existing research on mental-health outcomes and air pollution has focused on associations with internalizing disorders, including depressive and anxiety disorders. For example, a systematic review and meta-analysis summarizing findings before 2019 found significantly increased risk of depression with long-term exposure to PM2.5 and short-term exposure to PM10, NO2, SO2, and CO (Zeng et al., 2019). An example of rigorous work in this area includes a study of nearly 16,000 midlife adults in China followed in three waves with satellite-derived estimates of PM2.5, which found that PM2.5 concentrations were associated with depressive-symptom scores (Xue et al., 2021). Recently, a representative study of more than 20,000 South Korean adults demonstrated associations between short-term (0–30 days) exposure to CO and medium-term (0–120 days) exposure to CO, SO2, PM2.5, and PM10 with likelihood of a depressive episode (Y. Lim et al., 2024).
Within this area of work, however, there is substantial variability in methodological approaches and quality of air-pollution measurements, resulting in some inconsistencies across findings. For example, a large cross-sectional study found no consistent evidence for associations between air pollutants, including NO2, PM2.5, and PM10, and depressed mood in adults (Zijlema et al., 2016). At the same time, different associations with depression may exist on the basis of the developmental period of the study sample, with unique patterns emerging for adolescents, adults, and the elderly. For example, a large cross-sectional study investigating links between depression risk and exposure to air pollutants found significantly elevated risk of developing major depressive disorder in adolescents with greater childhood exposure to NO x and PM2.5 (Latham et al., 2021). Other cross-sectional adolescent studies have found significant links between O3 and depressive symptoms, including that higher O3 concentrations were associated with greater percentages of adolescents experiencing depressive symptoms (Waxman & Manczak, 2024) and that higher O3 predicted steeper increases in depressive symptoms over time (Manczak et al., 2022). Similar associations have also been found in elderly populations—for example, in a nationally representative sample of older adults, increases in PM2.5 were significantly associated with greater depressive symptoms (Pun et al., 2017). Ultimately, understanding links between air pollutants and depressive symptoms across developmental periods may be particularly important in informing understanding of risk and preventive efforts.
Similar to depression, suicidal thoughts and behaviors have also been associated with air-pollutant exposure. Here, several systematic reviews have noted significant links between increased exposure to NO2, SO2, O3, CO, PM10, and PM2.5 and suicide risk (Braithwaite et al., 2019; Davoudi et al., 2021). An exemplar of this work is a large national-cohort study that found exposure to air pollution during childhood, including NO2 and PM2.5, to be associated with subsequent self-harm risk (Mok et al., 2021), pointing to significant associations with both suicide risk and self-harm behaviors. Several studies have also observed seasonal dependence of these associations; for example, one case-crossover study found significant associations between suicide risk and exposure to NO2 in the spring and fall and PM2.5 in the spring (Bakian et al., 2015), whereas another found significant associations of PM10 and O3 with suicide during the summer and O3 during the spring and fall (Casas et al., 2017). Other studies have had null findings or have found associations in the opposite direction such that death by suicide was related to lower levels of O3 (Davoudi et al., 2021). As with studies of depression, the timing of exposure and operationalization of outcomes vary widely across studies, potentially contributing to these inconsistencies.
Symptoms of anxiety have likewise been associated with air-pollution exposure, although this association has been less commonly studied than depression, and the associations found are not as consistent (Trushna et al., 2021). Nonetheless, a significant correlation between air-pollution exposure and anxiety symptoms has been observed across multiple developmental periods from childhood to older adulthood and with multiple pollutants, including PM2.5 (Power et al., 2015; Pun et al., 2017; T. Yang et al., 2023), airborne lead (Rasnick et al., 2021), and NO x (T. Yang et al., 2023). Indeed, several of these studies employed rigorous designs with large nationally representative samples (Power et al., 2015; Pun et al., 2017). Some studies have found these associations even when air-pollution levels are in compliance with air-quality standards (Rasnick et al., 2021; T. Yang et al., 2023), suggesting that current standards may not be strict enough to protect individuals from experiencing anxiety symptoms.
Taken together, growing evidence points to a significant relationship between internalizing disorders and pollutant exposure, with associations observed across a range of pollutants, internalizing symptoms, and developmental periods.
Air quality and externalizing disorders
Although evidence for the impact of air pollution on internalizing disorders has been steadily mounting, research investigating its effect on externalizing disorders has been more limited. A 2023 narrative review examined eight longitudinal and six cross-sectional studies from several countries regarding the impact of air-pollution exposure on externalizing symptoms in both neurodiverse and typically developing children in which authors noted inconsistency across findings and overwhelmingly low-quality evidence (Baird et al., 2023). When considering externalizing symptoms generally (e.g., aggression, rule-breaking), captured by broadband measures such as the Child Behavior Checklist, results seem to be influenced by timing and type of exposure. Loftus et al. (2020) found prenatal exposure to NO2 in the United States to be associated with higher rates of clinically significant externalizing behaviors in early childhood. In addition, a longitudinal study in South Africa found exposure to indoor PM10 during the prenatal period to likewise be linked with externalizing problems in early childhood (Christensen et al., 2024). Researchers examining PM2.5 exposure during middle childhood in the Adolescent Brain Cognitive Development Study cohort in the United States have uncovered more mixed results; one study found increased externalizing symptoms in females only (Smolker et al., 2024), and another found no associations at all (Campbell et al., 2024). A small body of research has examined the impact of air-pollution exposure on the development of conduct disorder specifically. One study in the United Kingdom did not find significant associations between conduct disorder and NO2 and PM2.5 exposure during birth and middle childhood (Bradley et al., 2024). Another UK-based study by Roberts et al. (2019) also found no significant associations when examining exposure during middle childhood, but other researchers using the same cohort have found significant findings when including exposure during adolescence and considering externalizing behaviors more broadly (Reuben et al., 2021). Karamanos et al. (2021) found that exposure to lower concentrations of PM2.5 and NO2 were linked with a decrease in reported conduct problems, and heightened exposure was linked with a flattened conduct problem trajectory in a UK-based longitudinal sample. Overall, this is an area that requires more exploration to truly understand the relationship between air pollution and externalizing symptoms and disorders.
Air quality and psychotic disorders
Air pollution, particularly exposure to PM and NO2, has been linked to the early development of psychotic symptoms in children and adolescents, severity of psychotic symptoms, and hospital admission and relapse rates. For example, individuals with schizophrenia who were exposed to higher levels of PM2.5 exhibited more severe psychotic symptoms, including delusions and hallucinations (Eguchi et al., 2018). As demonstrated in a case-crossover study conducted in Seoul, South Korea, even short-term (i.e., daily) increases in air-pollution levels were found to be significantly associated with heightened psychotic symptoms (W. Lee et al., 2022). Likewise, prior work has found that periods of elevated PM and NO2 were associated with increased hospital admissions for individuals with schizophrenia, suggesting that short-term spikes in air pollution contribute to acute exacerbations of symptoms that necessitate hospital care (Bai et al., 2019, 2020).
Longitudinal studies provide additional support for the role of air pollution in the development and exacerbation of psychotic disorders. A prospective population-based survey highlighted the link between long-term (i.e., yearly) exposure to air pollutants and the exacerbation of schizophrenia symptoms, noting that higher levels of PM2.5 and NO2 were associated with increased symptom severity, higher relapse rates, and more frequent hospital admissions and that individuals living in areas with higher levels of PM2.5 and NO2 were at a greater risk of developing psychiatric disorders, particularly psychosis and schizophrenia (Bakolis et al., 2021). Likewise, studies using high-resolution data have shown that increased exposure to NO2 and PM2.5 was significantly associated with the development of psychotic symptoms during adolescence (Newbury et al., 2019; Roberts et al., 2019).
Air quality and neurodevelopmental disorders
Regarding neurodevelopmental disorders, increased incidence of autism has been associated with air-pollution exposure. Beginning with the prenatal period, authors of a 2021 meta-analysis found that PM2.5 exposure during late pregnancy was associated with an increased risk of autism in offspring (Dutheil et al., 2021). Prenatal exposures to O3 and NO x have also been found to be associated with increased odds of autism (McGuinn et al., 2020; Oudin et al., 2019). In addition, the early postnatal period appears to be a sensitive window in which air-pollution exposure, particularly PM2.5 and O3, are associated with greater incidence of autism (Dutheil et al., 2021; Kaufman et al., 2019).
In contrast, the association between air-pollution exposure and ADHD is less robust. For example, a 2022 systematic review and meta-analysis of nine studies did not find a significant relationship between the two (Zhang et al., 2022). However, the meta-analysis authors cautioned that the number of available studies on this topic was limited and that more research is needed. Conversely, other studies have identified links between symptoms of ADHD and early life exposure to NO2 and PM2.5 (Thygesen et al., 2020) and long-term exposure to O3 (Zhou et al., 2023). The inconsistency across studies highlights the need for additional research to better understand links between air-pollution exposure and ADHD. Moreover, less attention has been paid to the associations between air-pollution exposure and intellectual disability; nonetheless, a recent study found that exceeding the 24-hr limits of PM2.5 exposure (based on WHO and EPA guidelines) during preconception and early pregnancy was associated with increased incidence of intellectual disability in a Utah-based sample of children (Grineski et al., 2024). Further study is needed to better understand the impact of air-pollution exposure on a variety of neurodevelopmental outcomes, including those already discussed, and specific learning disabilities, speech/language disorders, and motor disorders (for a systematic review of neuropsychological development and air pollution, see Suades-González et al., 2015).
Air quality and cognitive abilities/disorders
Research has demonstrated that air pollution may adversely affect human cognitive processes, resulting in negative mental-health outcomes. In studies beginning with prenatal exposure, previous research indicates a negative association between air-pollution exposure during pregnancy and subsequent offspring cognitive outcomes. Specifically, in a cohort study of 568 children (age: M = 10.52 years) in northern California, higher average PM2.5 exposure during pregnancy was associated with lower overall IQ and lower scores in working memory and processing-speed indices (Holm et al., 2023). Prenatal exposure has been likewise associated with adolescent academic achievement and inhibitory control (Margolis et al., 2021). Results of another cohort study (Loftus et al., 2019) demonstrated that higher average PM2.5 and NO2 exposure during the prenatal and postnatal periods was associated with lower offspring IQ during childhood (ages 4–6). Note, however, that a recent meta-analysis (Thompson et al., 2023) concluded that current evidence was not strong enough to definitively link air pollution to poorer cognitive outcomes in children and adolescents; consequently, more research is warranted.
For older adults, air quality has also been associated with cognitive decline and dementia. For example, in a large longitudinal sample of older adults in England, results indicated that increasing exposure to PM2.5, PM10, and NO2 were associated with decreasing scores on measures of memory and executive functioning over time (Wood et al., 2024). Likewise, in a study of older adults in France, greater PM2.5 exposure was linked to accelerated global cognitive decline (Duchesne et al., 2023); at the same time, the results for NO2 and black carbon were not significant. The results of a recent systematic review and meta-analysis of 86 studies on air pollution (i.e., PM, NO x , and O3) and cognitive abilities (e.g., global cognition, executive functioning, memory) across the life span concluded that air-pollution exposure was linked to worse cognitive outcomes in adults (Thompson et al., 2023). More specifically, NO2 was significantly associated with lower scores across cognitive batteries, and PM2.5 exposure was linked to worse general cognition, verbal fluency, and executive function in adults ages 40 and older.
Although these studies considered broad cognitive functioning, other studies similarly found associations between air pollution and clinical dementia. For instance, a national cohort study of 12 million older adults in the United States demonstrated a link between long-term PM2.5 exposure and elevated risk for incident dementia and Alzheimer’s disease (Shi et al., 2021). NO2 was also associated with elevated risk for incident dementia and Alzheimer’s disease in this sample, although the effect was smaller. The large sample size and measurement of air pollution and cognitive impairment across time provide compelling evidence that air pollution may be an overlooked risk factor for dementia and Alzheimer’s disease among older adults. Relatedly, a recent meta-analysis found an association between ambient air pollution, particularly PM2.5, and clinical dementia across 51 studies. (Wilker et al., 2023). Note that this was observed even in studies in which PM2.5 was below federal National Ambient Air Quality Standards, indicating that chronic low levels of pollutant exposure can predict adverse cognitive outcomes. In addition, in a review of air pollutants and risk for dementia in North America and Europe, greater exposure to NO2 and NO x were also associated with increased dementia risk (Peters et al., 2019). Taken together, research suggests that air pollution may exert negative impacts on cognition and increase risk for cognitive disorders later in life. However, more work is needed to understand which pollutants may be most salient for cognitive functioning across the life span.
Air quality and eating disorders
To our knowledge, only one published article to date has examined associations between air quality and eating disorders; however, the rigor of the study was commendable. Specifically, a large-scale sample of children under 15 in Catalonia were assessed with ICD-10 diagnoses, which were related to air-pollution metrics derived from spatiotemporal models, Bayesian inferences, and compositional data (Mota-Bertran et al., 2024). The authors found that overall pollution was significantly associated with receiving an eating-disorder diagnosis.
Although not specific to eating disorders, there also exist studies that suggest air-pollution exposure is related to appetite and obesity in children and adults. For example, a cross-sectional study of preschoolers in China found that higher levels of O3 and PM2.5 were associated with greater likelihood of having obesity or being overweight (Su et al., 2022). Among adults, a study of outdoor workers in Malaysia found that higher levels of PM2.5 were associated with more calories consumed and greater appetite (Sundram et al., 2022). A systematic review in 2018 examining 66 reported associations between air pollution and obesity found that 29 involved positive associations, 29 involved null findings, and eight involved negative associations (An et al., 2018); further research is necessary to better understand associations between air pollution, eating disorders, and eating behaviors.
Air quality and substance use disorders
Several large-scale studies have begun investigationing associations between pollutants and substance use disorders. For example, using a case-crossover design, one study of adults in Taipei found that a 35% rise in O3 on cool days and a 12% rise in O3 on warm days were associated with mental-health hospitalizations for substance use, which were not accounted for by changes in other pollutants (S.-S. Tsai et al., 2022). Likewise, a study of emergency-department visits for abuse of psychoactive substances among Canadian adults found significant lagged associations between exposure to CO, PM10, and NO2, although the specific durations of lagging differed (Szyszkowicz, 2022). Among children, a study of black-smoke air-pollution exposure from the prenatal period to age 10 demonstrated that high prenatal, postnatal, preschool, and childhood exposures were significantly associated with substance use in adolescence (Hobbs et al., 2025). Although the aforementioned studies all evince rigorous designs, there have been inconsistent and mixed findings in other work in this area. For example, an 8-year study of more than a million residents of Rome, Italy, did not find significant associations between long-term air-pollution exposure and first incidents of hospitalizations or doctor visits for substance use (Nobile et al., 2023). Earlier work has suggested that inconsistent findings on the topic of smoking and alcohol consumption with air pollution may be due to failure to account for socioeconomic and neighborhood factors (Strak et al., 2017). More research in this area is warranted.
Air quality and other conceptualizations of psychopathology
In addition to research examining specific types of psychopathologies, summarized above, occasional studies have adopted broadband conceptualizations of mental-health dysfunction. In one of the more rigorous examples of this, using data from the ERISK study in England and Wales, NO x exposures at ages 10 and 18 were found to be associated with general psychopathology scores at age 18 (Reuben et al., 2021). Other studies have examined air pollution in relation to emotional distress rather than psychopathology per se. A longitudinal study of older women over 12 years found that PM2.5 and NO x were associated with greater emotional distress in U.S. women (Petkus et al., 2021). Smaller studies involving 59 children (Taylor et al., 2024) and 102 adults (S. Chen et al., 2018) have likewise linked radon and smog exposure, respectively, to measures of emotional distress.
In sum, compelling evidence is emerging that links air-pollutant exposure to a variety of forms of psychopathology; however, there remains substantial need for further rigorous research to clarify and extend these findings.
Theorized biological mechanisms
Although research to date has begun identifying associations between pollutants and mental health, little research has directly tested biological mechanisms for these connections. Nevertheless, a variety of biological mechanisms are plausibly implicated in how exposure to air pollutants can influence social and emotional outcomes throughout the life span, including neuroendocrine and HPA-axis dysregulation, inflammation, structural brain changes, and oxidative stress, briefly reviewed here.
A growing body of research has found that environmental pollutants (e.g., OM and O3) act as physical stressors that can activate the HPA axis. Although acute activation of the HPA axis is necessary for survival, chronic, dysregulated HPA-axis functioning is associated with a host of psychopathology symptoms and disorders across the life span (Faravelli et al., 2012; Juruena et al., 2020; Watson & Mackin, 2006). For example, research has found links between dysregulated HPA-axis functioning and posttraumatic stress disorder (PTSD), generalized anxiety disorder, panic disorder, obsessive compulsive disorder (OCD), and social anxiety disorder (also known as social phobia) both concurrently and longitudinally (Daskalakis et al., 2013; Faravelli et al., 2012). Dysregulated HPA-axis functioning (e.g., HPA hyperactivity) has also been observed in depressive disorders (Bertollo et al., 2020; Nandam et al., 2020; Stetler & Miller, 2011) and schizophrenia (Ji et al., 2021; F. Yang et al., 2020). Several studies evince a link between early life stress (e.g., adverse childhood experiences, having a caregiver/parent with psychopathology) and HPA-axis dysfunction, such as cortisol hypersecretion, slower return to homeostasis following a stressor, and lower cortisol-awakening response (Schumacher et al., 2019; Stetler & Miller, 2011; Yehuda & LeDoux, 2007), which may subsequently increase risk for psychopathology. Poor air quality has been suggested to be akin to chronic low-level exposure to physical stress or early life adversity that can contribute to abnormal and prolonged HPA-axis activation (Thomson, 2019).
Inflammation is another crucial biological process that may underlie the links between air quality and mental-health risk. Briefly, when the immune system detects a pathogen, it signals a cascade of inflammatory processes known as “inflammation” (Barton, 2008). Similar to HPA-axis functioning, inflammation is necessary in the short-term; however, chronic inflammation is associated with psychopathology onset, course, and maintenance (Mac Giollabhui et al., 2021; Renna et al., 2018; Slavich & Irwin, 2014). For example, a strong body of research has found evidence for bidirectional associations between inflammation and depression (Kim et al., 2022; Milaneschi et al., 2021; Slavich & Irwin, 2014). Previous studies also indicate associations between inflammation and anxiety disorders (Hou et al., 2017; Michopoulos et al., 2017; Salim et al., 2012), PTSD (Michopoulos et al., 2017; Speer et al., 2018), OCD (Attwells et al., 2017; Meyer, 2021), and schizophrenia (Kirkpatrick & Miller, 2013; Miller et al., 2011). Research suggests that environmental pollutants may act as “inhaled pathogens” that contribute to altered or prolonged inflammation (Snow et al., 2018). For example, in a meta-analysis of the effects of household air pollutants on immune functioning (A. Lee et al., 2015), results indicated that PM induces a prolonged proinflammatory state.
A growing body of research demonstrates that air pollutants may also affect the central nervous system via neuroinflammatory processes, resulting in profound changes in frontolimbic brain regions, such as the hippocampus, amygdala, and prefrontal cortex (PFC; for a review, see Zundel et al., 2022). For instance, a review of neuroimaging studies found that air pollutants (i.e., elemental carbon, PM2.5, and PM10) were associated with reduced gray-matter volume (Herting et al., 2019), which has been linked to depression, conduct problems, ADHD symptoms, and general psychopathology in other studies (Durham et al., 2021; Vasic et al., 2008). Greater exposure to NO x and PM during pregnancy and childhood is linked to altered white-matter tracts in preadolescence (Lubczyńska et al., 2020). These white-matter tracts connect frontolimbic brain regions (e.g., hippocampus, amygdala, and PFC) that play a key role in emotion regulation and stress responding (e.g., Janiri et al., 2020). Specifically, the PFC cognitively controls the amygdala, which is responsible for processing emotions and identifying the valence and salience of emotional stimuli (Adolphs, 2002; Ochsner et al., 2012). The amygdala triggers the fight-or-flight response and plays a crucial role in emotional conditioning and memory (LeDoux, 1994). The amygdala works collaboratively with the hippocampus, which is necessary for emotional processing and memory and responding to stress (Herman & Cullinan, 1997; Teicher et al., 2003). Thus, the frontolimbic brain regions are crucial for emotion and stress regulation; alterations to this network (e.g., amygdala hyperreactivity) are often implicated in the course and maintenance of psychological disorders in which emotion dysregulation is core feature, such as depression, bipolar disorder, externalizing disorders, borderline personality disorder, anxiety disorders, PTSD, and schizophrenia (Eack et al., 2016; Helm et al., 2018; Herringa, 2017; Kenwood et al., 2022).
Finally, oxidative stress may be another biological mechanism through which air pollutants exert adverse mental-health effects. Briefly, oxidative stress is a complex phenomenon that occurs when there is an imbalance between the production of reactive oxygen species (ROS) and the body’s capacity to detoxify chemicals and repair cellular damage (Mecocci et al., 2018). Research suggests that pollutants contribute to overgeneration of ROS and oxidative stress, resulting in damage to cellular macromolecules (Al-Gubory, 2014), and a recent meta-analysis concluded that short-term exposure to PM was associated with increased oxidative stress (Li et al., 2020). In turn, oxidative stress has been found to predict externalizing behaviors and social difficulties in early childhood (Rommel et al., 2020).
Although research on these and other plausible biological pathways (e.g., sleep, transcriptional changes) is still emerging (e.g., J. Liu et al., 2020; O’Beirne et al., 2018), we note that these processes are likely interconnected and largely transdiagnostic. For example, activity in the HPA axis regulates and responds to systemic inflammation (Chrousos, 1995); inflammation in the periphery can influence (and be influenced by) neuroinflammation (Sun et al., 2022). Further work is needed, therefore, to identify both shared and unique components of risk for both psychological and physical disorders.
Remaining gaps in the literature
Despite emerging evidence of associations between air pollutants and a variety of mental-health outcomes, there remain several gaps in the literature. First, as noted above, several mental-health outcomes have been largely overlooked and remain understudied (e.g., externalizing disorders, certain neurodevelopmental disorders). Existing research also focuses primarily on adult populations, warranting further investigation of associations between a broader range of pollutants and mental health among children and adolescents. Second, there exists significant inconsistency in findings, which can make it difficult to interpret specific results. Much of this inconsistency is likely due to the significant variation in methodological choices that exist across and even within disciplines. For example, there is little consensus or standardization around how pollutant exposure is measured in terms of commonly studied pollutants, data sources, spatial resolution (e.g., at residential addresses vs. census-tract averages), and time frames (e.g., daily exposure vs. aggregates across a year). Thus, work that systematically considers differences in pollution measurement and/or estimation approaches is needed to illuminate best practices and drive future work. Third, relatively little research has directly examined possible mechanisms that might explain associations between air pollution and mental health, leading to substantial gaps in the biologically plausible pathways of risk and challenges with strengthening causal interpretations. Fourth, there has not been consistent acknowledgment of the disproportionate burden of pollution exposure on historically marginalized communities within the context of research on air pollution of dimensions of health; consequently, culturally sensitive research that partners with members of these communities will be critical for advancing more complete understandings of the impacts of air pollution.
Taken together, these findings point to substantial promise in investigating the role of air pollution but evince the need for additional high-quality research to comprehensively capture and understand associations between air-pollution exposure and psychopathology.
Challenges to Collaboration
For clinical-psychological scientists interested in advancing knowledge around mental health and air quality, collaboration with experts in air pollution affords unparalleled opportunities. However, there are several challenges to collaboration that may hinder the formation of multidisciplinary teams. To start, there are notable differences in terminology that can obstruct understanding. For example, in the field of psychology, “environment” or “environmental effects” are often used to refer to the social forces affecting an individual or to any nongenetic processes that might govern particular outcomes (e.g., family environment, genetic vs. environmental effects). In natural-science fields, these terms instead primarily refer to physical environmental factors (e.g., built and natural environments). Consequently, greater precision of terminology within each discipline is necessary for clarity.
An additional challenge to multidisciplinary collaboration is a lack of familiarity with central constructs belonging to other fields. For example, clinical-psychological scientists often have little prior knowledge of common air pollutants and few accessible resources for learning basics. Likewise, atmospheric scientists and building engineers are often unfamiliar with psychological diagnostic systems, leading to confusion about primary mental-health outcomes. In each instance, this lack of knowledge likely impedes motivation for incorporating these constructs into current projects or forging connections across disciplines.
A final challenge to collaboration involves disciplinary differences in methodological approaches. For example, clinical-psychological science often relies on intensive study of relatively small samples of participants (hundreds). In contrast, atmospheric science related to physical diseases frequently employs a public-health approach, using less detailed assessments of relatively large samples of participants (thousands), or maps global air pollution without respect to specific individuals. Adjusting the scale and scope of collaborative studies is therefore necessary for aligning across disciplines.
Solutions and Recommendations
Considerations and recommendations for measuring outdoor air quality
Measurement approaches for outdoor air quality
Data sets for outdoor air quality often incorporate a range of data sources, including observations, atmospheric-model data, and data-fusion products that combine several different data sets. Each of these sources has distinct uses for applications at the intersection of mental health and air quality, briefly described below.
The first common source for air-quality data is from observational data sets, which use instruments to measure trace constituents in the atmosphere. These can include anything from low-cost optical sensors for bulk measurements of pollutants such as PM2.5 or NO2 to research-grade instruments that differentiate between thousands of chemicals at high temporal resolution based on observed wavelengths and other parameters. Furthermore, these instruments can be ground-based for continuous measurements at a particular point, mobile or flight-based for observation for a time period in a given trajectory, or even include remote-sensing platforms, such as satellites, that provide observations with varied spatiotemporal coverage. Observational data sets therefore vary considerably in their spatial and temporal resolution depending on the placement and type of sensors. When located in proximity to populations of interest, these data sources can be well-tuned to their specific communities; in locations without sufficient coverage by observational instruments, such approaches may be imprecise.
Another source for air-quality data is atmospheric models, which use parameterizations of physical and chemical processes in the atmosphere to calculate the formation and fate of health-relevant pollutants. These methods range in complexity and their uses, although ones that are most useful for the study of trace pollutants in the atmosphere include representations of chemical mechanisms in the atmosphere and account for transport from wind and other processes. These can either be added as model variables or estimated simultaneously within the predictive model. Strengths of atmospheric models include that they estimate pollutant concentrations throughout large spatial and temporal domains and that they can also be used to estimate air quality in cases in which observations are lacking in both space and time; drawbacks include the lack of accessibility to create these models for psychological scientists who are not directly collaborating with atmospheric scientists.
Data-fusion products are statistical frameworks that combine observations with model outputs and other relevant geophysical data sets to estimate air quality over domains similar to those found in atmospheric models. In regions in which high-resolution input data are widely available, data-fusion products will commonly use machine-learning methods to distill large amounts of data into tractable representations of historical air quality at high resolution. Complex data-fusion products will also leverage satellite observations and models to provide spatial coverage of air quality in regions that have limited ground-based observations or air-quality gradients based on emissions sources such as roads and industrial sources.
The use of air-quality data from one of these sources is largely determined by the scope and purpose of the desired research outcomes. Although localized observations will tend to give the most accurate and comprehensive measures of atmospheric pollutants, studies are limited to the areas with existing high-quality observations, which limits cohort selection. For studies involving large areas and long periods of time, both data-fusion products and atmospheric models can be used to effectively classify air-pollution exposures, and both are often validated with respect to ground-based observations. The choice of approach in this case should be determined by which one has the best accuracy in the research locality and pollutant of interest. One particular case in which atmospheric models excel is air-quality forecasting and future climate and air-quality scenarios because the lack of observations for these periods can limit the efficacy of data-fusion products.
Another important consideration for outdoor air-quality data is the temporal resolution of exposure and the behavior of the pollutant of interest in the atmosphere. Many trace gases and aerosols undergo important reactions in the atmosphere and thus will have varying concentrations throughout the day (e.g., O3 and NO2) based on several factors (e.g., Bloomer et al., 2010). In these cases, using concentrations that are averaged on a daily or less frequent timescale may not provide an accurate representation of their exposure for humans. In addition, some mental-health responses may plausibly be affected by the peak concentrations or trajectory of exposure over time and therefore would need to be evaluated differently from the commonly used annual or daily averaged metrics. Consequently, the level of temporal and spatial resolution for air pollution necessary within a given study should be thoughtfully considered in the context of participant locations, behavior of specific pollutants, and theorized links to psychological outcomes.
Publicly available resources for assessing outdoor air quality
In addition to collecting and building unique air-quality exposure models, there are a variety of publicly available data sets providing localized air-pollution estimates that are easily accessible and offer opportunities for multidisciplinary research. First, the EPA has historically provided downloadable data sets with both annual and daily summaries for a variety of pollutants, including PM, air toxicants, and O3 estimates (U.S. EPA, 2024). Daily air-quality estimates for O3 and PM in the United States, Mexico, and Canada can also be accessed using the AirNow Air Quality Index tool (EPA, 2024). In the United States, several states have created environmental-justice mapping tools that provide neighborhood-level estimates of air-pollutant exposures in addition to other environmental measures that are relevant to human health (e.g., proximity to oil and gas facilities). For example, the Colorado Enviroscreen (Colorado Department of Public Health and Environment, 2025), the California Enviroscreen (California Office of Environmental Health Hazard Assessment, 2023), MiEJScreen (Michigan Department of Environment, Great Lakes, and Energy, 2018), and PennEnviroScreen (Pennsylvania Department of Environmental Protection, 2023) map environmental, health, and demographic characteristics across Colorado, California, Michigan, and Pennsylvania neighborhoods, respectively, at the census-tract level. In addition, although less reliable in quality, local citizen-science projects that collect and publish data from personal air monitors are also available as sources of data.
Regarding global air-pollution data, WHO (2024) provides information on air-pollution trends and concentrations worldwide. The State of Global Air (2024) is an additional resource that provides global estimates of air-pollutant concentrations at the country and city levels. For more precise air-pollutant measurements, the Atmospheric Science Data Center (ASDC) is a NASA center that provides a wide range of publicly available atmospheric data (ASDC Science Data Center, 2024). ASDC has multiple projects and data collections available for public access, including the Tropospheric Emissions: Monitoring of Pollution instrument, a newly developed tool that provides near real-time measurements of O3, NO2, and other atmospheric composition measurements (Smithsonian Astrophysical Observatory & NASA, 2024).
In sum, there are many publicly available data sets indexing outdoor air pollution in the United States and globally. These data can be easily accessed and combined with other data sets (e.g., psychosocial, policy, public-health data), providing exciting opportunities for multidisciplinary research. However, these tools may lack temporal and spatial precision, often providing yearly averages rather than daily or hourly estimates and data at the census tract, county, city, state, or country levels rather than residential addresses. Thus, it will be important for these tools to continue to refine their air-pollution measurements to enhance the accuracy and utility of available data.
Considerations and recommendations for measuring indoor air quality
Unique contributions of indoor air quality
Individuals in the United States spend nearly 90% of their time indoors (Klepeis et al., 2001). The built environment has dramatically changed in the last few generations with advancements (e.g., central heating/air conditioning, subdivisions, high-rises) and new indoor anthropogenic sources of pollution (e.g., cleaning products, formaldehyde and other chemicals in furnishings, gas appliances; Basile, 2014; Sundell, 2004). Concurrently, engineers have diligently developed new processes and buildings that are more efficient to reduce rising energy costs (Ionescu et al., 2015). In some cases, efficient construction results in a built environment that is more isolated from the outdoors (e.g., “tighter”), affecting the relationship between indoor and outdoor pollution levels (Colbeck et al., 2010). Although the impacts of building ventilation on the physical health and cognitive function of occupants have been studied (e.g., Carrer et al., 2015), the impacts of ventilation on mental health are nascent. In a recent review of literature evaluating the relationship between air pollution and mental health, researchers concluded that there is a paucity of ongoing research (epidemiologic, preclinical, or clinical) evaluating indoor air pollution for mental-health impacts (Hoisington et al., 2024).
Key metrics for measuring indoor air quality
Air quality in the built environment is influenced by the type of ventilation (e.g., mechanical, natural, mixture of both), design of the building, and occupants’ behavior. A key parameter for indoor air pollution is in supplied outdoor-ventilation rates. For air pollutants that are primarily sourced from the indoors, low outdoor-ventilation rates can increase indoor concentrations. Common airborne pollutants that have indoor sources include PM, human or pet bioaerosols, fungal spores, volatile organic compounds, and semivolatile organic compounds. Low ventilation rates have been associated with mold growth and elevated levels of carbon dioxide. In contrast, air pollutants that are primarily sourced in the outdoors can be reduced indoors with low outdoor-ventilation rates. Outdoor-sourced pollutants can include PM, CO, NO x , SO x , and O3.
Traditional ventilation-rate measurements are conducted in computation simulations, dedicate tracer gas decay (e.g., sulfur hexafluoride), or pressure-based methods that are difficult to perform in large-scale studies and need specific expertise (Persily, 2016). Recent advancements in technology led to an expanse of portable and inexpensive carbon-dioxide sensors that can detect occupant-generated gas (e.g., carbon dioxide). Although not as robust or reliable as the traditional methods (Persily, 2016; Sundell et al., 2011), carbon-dioxide measurements may provide an approximation of outdoor ventilation when assessed properly (e.g., single zone, well-mixed air, information on occupants; Persily, 2022; Persily et al., 2022).
Additional factors in the built environment should be considered when engaging in airborne-pollutant and mental-health studies. Buildings are dynamic environments with indoor-pollution levels that can vary within a building, across seasons (Abdel-Salam, 2021), and between buildings with similar designs (J. Chen et al., 2020). In addition, the indoor air quality is dependent on dynamic occupant behaviors (Ibrahim et al., 2022). Location, even within the same city, can dramatically alter spatially heterogeneous outdoor-air-pollutant concentrations that, in turn, result in nonstandard indoor air concentrations (Sarnat et al., 2010). Finally, socioeconomics should be considered alongside indoor air quality because they can alter building performance and occupant usage. Neighborhood socioeconomic characteristics, such as poor housing quality, have been shown to result in negative mental-health outcomes from overcrowding (Rollings et al., 2017), housing disarray (Suglia et al., 2011), and pest infestations (Shah et al., 2018; Zahner et al., 1985). Low-income neighborhoods are also more likely to impair mental health through noise exposure from roadways (Stansfeld et al., 2005), airports (Baudin et al., 2018), heat (Chakraborty et al., 2019), and high-density residential units (Jensen et al., 2018), making it critical to assess and account for these factors as well.
Future directions for indoor-air-quality research and mental health
Future studies would be enhanced with partnerships between social scientists, built environmental researchers, and indoor-air specialists (Corsi, 2015). The availability of low-cost sensors has the possibility to actively increase the variety of airborne pollutants for study using spatial and temporal scales not even considered a decade ago. The impact of using more sensors indoors is vital to understanding a field that—with the exception of workplaces—is unregulated. Social-scientist researchers with a broad and firm understanding of interventional studies have the skills to change the current trend of investigating associations between air pollutants and mental health to discovering causal links that can lead to interventions for psychological benefits. Finally, although regulations of the indoor environment might not happen soon, several positive developments are currently occurring that may draw attention to indoor air pollution and mental-health research, such as the increased use of external certifications of buildings based on occupant health and well-being (e.g., LEED, WELL Building Standards) and amplified public awareness to indoor air quality related to the COVID-19 pandemic.
Opportunities to strengthen causal interpretations
Increasing the rigor of study design
For ethical reasons, direct experimental manipulation of air-pollution exposure in relation to psychopathology in humans is not possible; consequently, existing research relies on observational studies. Of course, this leaves work vulnerable to unmeasured confounding factors and incorrect directional interpretations, especially for research that is cross-sectional. To be sure, some studies do leverage natural experiments and other quasi-experimental designs, such as case-crossover paradigms, to increase the plausibility of causal interpretations. When such approaches are not possible, however, additional design considerations can increase rigor. For example, repeated measures of both pollution exposure and mental-health outcomes and potentially confounding factors, such as demographic characteristics and socioeconomic resources, can allow for lagged modeling to disentangle sequencing of associations. Moreover, research that directly tests theorized pathways connecting air pollution to mental health, such as biological changes, can strengthen causal interpretations by identifying temporally sensitive mediators and complement experimental work in animal models. Randomized clinical trials that target reducing indoor or outdoor pollution and assessments before and after policy changes that affect exposure will also be valuable for deepening causal understanding.
Disentangling physical exposure from anticipated exposure
Another important step in establishing causal pathways between air-pollution exposure and psychopathology is understanding how the impacts of physical exposure to pollution differ from the impacts of psychological processes of anticipating detrimental exposure, such as the impacts of climate change on future air quality. As the threat of climate change looms larger in the public consciousness, uncertainty and worry about how it will affect quality of life is on the rise (Leiserowitz et al., 2024).
Negative emotional responses to climate change are relevant in the discussion of air pollution and psychopathology because air quality and climate change bidirectionally influence one another (Orru et al., 2017). Specifically, climate change produces hotter and dryer conditions, increasing the likelihood of wildfires, which increases concentrations of certain air pollutants, such as PM2.5 (Y. Liu et al., 2010). In addition, ground-level O3 is the product of volatile organic compounds, NO x , and sunlight; therefore, fewer cloudy days and more high-temperature days will likely result in increased concentrations of ground-level O3, especially if unaccompanied by emissions reductions (Bloomer et al., 2009). Moreover, the burning of fossil fuels both produces air pollutants and contributes to the accumulation of carbon dioxide in the atmosphere, further warming the planet (Ramanathan & Feng, 2009).
Given the connection between air quality and climate change, it is possible that exposure to air pollution may elicit heightened fears and anxieties surrounding the threat of climate change, further exacerbating the relationship between air pollution and psychopathology. Although very little attention has been paid to threat of exposure’s differential effect on the relationship between air-pollution exposure and psychopathology thus far, there is preliminary evidence to suggest its validity. For example, a qualitative analysis of community reactions to the 2019–2020 Australian bushfires highlighted how the persistent visibility of wildfire smoke and its health repercussions elicited feelings of depression and anxiety among residents (Williamson et al., 2022). Overall, because air-pollution exposure and threat of future exposure are related yet distinct constructs that are both associated with psychopathology symptoms, it will be important to incorporate measurements of both in research studies to disentangle their unique and potentially interactive effects on mental health.
Consideration of historically marginalized communities
To comprehensively examine the relationship between air pollution and psychopathology, it is imperative to discuss the inequitable rates of air-pollution exposure experienced by historically marginalized communities. It is well established that communities of color in the United States are disproportionately exposed to greater air pollutants compared with communities in predominantly White and affluent areas (L. P. Clark et al., 2014; Collins et al., 2022; Pope et al., 2016; Woo et al., 2019). Moreover, individuals who reside in low- and middle-income countries (LMICs) are exposed to higher rates of air pollution compared with individuals residing in high-income countries (HICs; Rentschler & Leonova, 2023).
Evidence points to the discriminatory practice of “redlining” as potentially contributing to these inequities in air-pollution exposure in the United States (Bramble et al., 2023; Collins et al., 2022; Hwa Jung et al., 2022; Motairek et al., 2023). In the 1930s, the United States government created the Home Owners’ Loan Corporation (HOLC), which assigned neighborhoods “grades” ranging from A (“best”) to D (“hazardous”) to indicate the security of mortgage investments during the country’s financial crisis (Mitchell & Franco, 2018). Predominantly Black, Asian, and Latine neighborhoods were considered hazardous investments and systematically received D grades. These neighborhoods were shaded red on HOLC maps, hence the term “redlined” (Hillier, 2003). Consequently, residents of these neighborhoods were systematically denied opportunities to build generational wealth and saw little investment in neighborhood infrastructure (Mitchell & Franco, 2018). Furthermore, these redlined neighborhoods were more frequently chosen as sites for heavy industry and highway construction, contributing to disparate exposure to air pollutants for residents of these communities (Lane et al., 2022; Mohai et al., 2009; Shkembi et al., 2024).
Burgeoning research has begun to associate the health disparities experienced by communities in historically redlined neighborhoods to inequitable air-pollution exposure (E. K. Lee et al., 2022). For example, there is evidence that there is an increase in mortality related to air-pollution exposure in census tracts with more Black residents, lower home values, or residents with lower median incomes (Y. Wang et al., 2016). Although mental-health outcomes have mostly been overlooked in this area of research, there is preliminary evidence to suggest that this is a fruitful area for further investigation. Indeed, a recent study found that air-pollution exposure in historically redlined neighborhoods in New York State was associated with increased emergency-department visits for mental-health concerns compared with neighborhoods with higher HOLC grades (Yoo & Roberts, 2024). Very few other studies have looked at the relationship between air pollution and mental health specifically in the context of redlining; however, other research supports the notion that individuals with minoritized identities experience worse mental-health outcomes associated with air-pollution exposure. For example, one study of an urban, U.S.-based sample of pregnant women found that the association between PM2.5 exposure and postpartum-depression symptoms was most severe for Black women (Sheffield et al., 2018).
Moreover, it is likely that the unequal air-pollution exposure in these communities interacts with psychosocial stressors, such as discrimination, to exacerbate mental-health outcomes. There is evidence that environmental exposures and psychosocial stressors have a cumulative and adverse effect on physical health (Clougherty & Kubzansky, 2009; Hicken et al., 2014; Morello-Frosch et al., 2011; Padula et al., 2020), and it is possible this includes mental health. Indeed, one study found that experiences of racism moderated the association between air pollution and conduct problems in children in a UK-based sample (Karamanos et al., 2021). Furthermore, these communities also bear the burden of additional forms of structural oppression, such as disparities in the built and natural environments (Adamkiewicz et al., 2011; Nardone et al., 2021). These disparities may serve as another potential moderator of the relationship between unequal air-pollution exposure and psychopathology (Rollings et al., 2017; W.-L. Tsai et al., 2023; H. Wang & Li, 2023). Although the specific interactions between air-pollution exposure, psychosocial stressors, structural oppression, and mental health have yet to be extensively evaluated, preliminary evidence suggests this is a worthy area of inquiry, especially with minoritized groups.
In addition to individuals who hold minoritized ethnic and racial identities, members of the LGBTQ+ community may also experience disproportionate air-pollution exposure, which may negatively influence their mental health. Although research in this area is scarce, one study found that individuals who lived in same-sex-couple enclaves in the Greater Houston, Texas, area experienced greater exposure to hazardous air pollutants associated with increased cancer risk (Collins et al., 2017). Moreover, unhoused individuals also bear the brunt of increased exposure to outdoor air pollution. Unhoused populations commonly spend a substantial proportion of their time outdoors, often by major roadways and other major sources of pollution (MacMurdo et al., 2022), making them particularly vulnerable to the effects of air pollution. Indeed, one study found that 31% of unhoused individuals in their sample reported emotional distress related to air pollution, and 89% reported seeking out medical services for a mental- or physical-health condition related to air pollution (DeMarco et al., 2020).
Looking beyond the United States, there is preliminary evidence that populations minoritized by race and/or ethnicity residing in other HICs (e.g., UK, the Netherlands) may also experience disparate air-pollution exposures because of living in closer proximity to sources of pollution (Abed Al Ahad et al., 2022; Fecht et al., 2015; Karamanos et al., 2021; Pasetto et al., 2019). However, very few studies of this nature have been conducted thus far; therefore, understanding disproportionate air-pollution exposure within HICs outside the United States remains an important area of research (Mustansar et al., 2025).
It is well established that individuals who reside in LMICs are exposed to increasingly hazardous concentrations of air pollutants compared with individuals who reside in HICs. According to a study conducted by Rentschler and Leonova (2023), 7.3 billion people are exposed to unsafe annual concentrations of PM2.5 globally, and 80% of these individuals reside in LMICs (Rentschler & Leonova, 2023). It is thought that factors such as rapid industrialization, reliance on fossil fuels, and densely populated urban centers contribute to such inequities (McDuffie et al., 2021). Moreover, a systematic review of personal monitoring of PM2.5 exposure found that individuals living in rural communities in non-HICs experienced high levels of exposure from indoor sources, such as use of coal as a heating source (S. Lim et al., 2022). Consequently, individuals residing in middle-income countries (e.g., India and China) are most affected by unsafe PM2.5 concentrations given the industrialized nature of their economies (Rentschler & Leonova, 2023). In turn, unsafe exposure levels are associated with increased cardiovascular and respiratory mortality in LMICs (Newell et al., 2017). Additional research that considers mental-health impacts in such communities is needed.
Recommendations for attending to inequity in research design
Based on these pervasive and long-standing inequities, it is paramount that future work examining this topic focuses on marginalized populations who are disproportionately exposed to air pollution. To do this, one must be mindful of the research methods employed. Psychological research has long struggled with creating inclusive samples that truly represent larger populations. Furthermore, the scientific-research community has a long and enduring history of actively exploiting and harming minoritized populations that persists to this day (P. A. Clark, 1998; Washington, 2006). Therefore, employing anti-racist, community-centered research methods in this area is critical. One example of this approach is community-based participatory research (CBPR), in which researchers establish community partnerships and engage in ongoing dialogues with community members surrounding community needs and interests (Minkler & Wallerstein, 2008). Consequently, community members serve an active and vital role in the development, implementation, and dissemination of findings of CBPR projects. Another consideration is to ensure that the psychopathological tools used are culturally informed and validated in diverse samples to ensure accurate measurement of symptoms. Furthermore, one must be mindful of hesitancy in reporting mental-health symptoms because of either cultural stigma or fraught racial relationships with research and mental-health systems, which can threaten internal validity. Aside from psychological measurement, methods for collecting air-pollution data should also be designed with care. If using publicly available data, consider whether these data have equivalent accuracy for more diverse and/or more socioeconomically disadvantaged areas (e.g., sufficient sensor coverage). In addition, researchers should consider how policies in a given country affect air-quality data collection, measurement, and interpretation given that many countries operate on vastly different standards and air-quality indexes, which may make cross-country cohort comparisons more challenging. Being familiar with local environmental policy can ensure that conclusions are accurately informed by the data and that recommendations provided by researchers are relevant and realistically implementable. Moreover, given the multiple simultaneous exposures many marginalized communities face (e.g., heat, proximity to industrial sites), careful measurement of multiple aspects of the built and natural environments will be important for clarifying unique risk. In summary, at its most basic level, designing research with diverse populations at the forefront can make progress in improving inclusivity and garnering a more robust understanding of how air pollution affects psychopathology in these communities.
Conclusion
Taken together, there is promising research suggesting that exposure to outdoor and indoor air pollution is associated with a variety of mental-health outcomes. However, significant gaps in knowledge remain, and existing research frequently employs inconsistent methodologies, which may account for mixed findings. Multidisciplinary collaboration between clinical scientists and experts in atmospheric research, pollution, and built environments holds tremendous potential for significantly advancing the field of psychological research by addressing these gaps and increasing methodological rigor.
In the current article, we sought to identify and address potential hurdles to such collaborations by providing information on common air-pollution constructs and recommendations and resources for outdoor- and indoor-air-quality assessment. We also highlighted important opportunities for future research, including approaches that strengthen causal interpretations of associations between air quality and psychopathology and that attend to inequity and disproportionate burden experienced by historically marginalized communities. Through multidisciplinary collaboration that incorporates physical environmental exposures, clinical-psychological science can expand knowledge on contributors to psychopathology and identify new targets for intervention and prevention efforts.
Footnotes
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contributions