
Abstract
Sexual- and gender-minority (SGM) individuals experience higher rates of depression compared with their non-SGM peers. Little is known about the day-to-day processes linking SGM experiences to depression. In responses from SGM young adults (N = 252)—predominantly self-identified as bi+ (sexual/romantic interest in multiple genders) cisgender women and nonbinary individuals assigned female at birth—we used multilevel structural equation modeling to investigate whether affective reactivity to SGM concealment and outness over an 8-day ambulatory assessment period (N = 4,342 observations) was associated with depression symptoms and whether momentary identity dysfunction accounted for this association. Concealment and outness were differentially associated with self-concept clarity and SGM-identity positivity. We did not find a direct association between depression and affective reactivity, although higher mean negative affect indirectly linked depression and affective reactivity to concealment. This study indicates that momentary identity and affective processes play an important role in the daily experiences of visibility for bi+ individuals.
Young adults with minority sexual and gender identities (e.g., lesbian, gay, bisexual, transgender, and gender nonbinary) tend to report higher prevalence of depression and suicidality than their cisgender, heterosexual peers (Pakula & Shoveller, 2013). They also tend to report greater identity dysfunction, including difficulty maintaining a coherent, stable, and positive self-schema (Rodriguez-Seijas et al., 2021). Individuals who sexually identify as bi, pan, or fluid and/or gender-identify as trans or nonbinary tend to additionally report greater depression, identity impairment, and identity invalidation (Feinstein & Dyar, 2017; Garr-Schultz & Gardner, 2021; Johnson et al., 2024; Price-Feeney et al., 2020; Ross et al., 2018). Developing and maintaining a stable identity is considered a crucial task of young adulthood (Arnett, 2015), associated with foundational personality processes, such as emotion regulation and interpersonal functioning (Nielsen & Wright, 2025). Social environments in adolescence and young adulthood are thought to shape identity development; affirming environments foster stable identity functioning, and hostile environments hinder stable identity functioning and contribute to psychopathology (Klimstra & van Doeselaar, 2017). Psychotherapy treatments adapted for sexual- and gender-minority (SGM) individuals suggest that repeated identity-threatening experiences are often the root of both identity dysfunction and psychopathology experienced by SGM individuals (Pachankis et al., 2023).
Minority-stress theory and identity-threat theory both suggest that increased risk of psychopathology in SGM individuals is caused by minority-specific stressors, such as active or anticipated discrimination or invalidation (Hossain & Ferreira, 2019; Meyer, 2003; Pachankis et al., 2024; Parr & Howe, 2019; Reyes et al., 2020). According to these theories, minority stressors threaten social identity and challenge the maintenance of a coherent and positive self-schema (Branscombe et al., 1999). Minority stressors therefore function as identity-threatening events, contributing higher momentary identity dysfunction and negative affect in response to the minority stressor. Identity dysfunction in this context includes lower positive attitudes about SGM identity (lower SGM positivity) and a lower overall sense of one’s identity as coherent and stable (lower self-concept clarity). Minority-stress theories additionally suggest that repeated exposure to identity-threatening situations may lead to depression.
A growing body of research investigates the relation between minority-stress experiences and health outcomes (Nicholas & Bresin, 2024). However, few studies have investigated the indirect role of identity dysfunction in the association between SGM identity-threatening experiences and affect in daily life. In the present project, we use ecological momentary assessment (EMA) to examine two primary aims. In Aim 1, we examine within-person associations between SGM-specific stressors (SGM-identity concealment and low outness), two components of identity functioning (SGM positivity and self-concept clarity), and negative affect. We particularly aim to investigate the role of identity functioning in the relation between depression symptoms and negative affective reactivity to SGM-specific stressors. In Aim 2, we examine the relation between increases in depression symptoms and individual differences in reactivity to SGM-specific stressors. We aim to clarify the relation between identity dysfunction and depression for SGM young adults.
Momentary Associations: Minority Stress, Identity Dysfunction, and Negative Affect
Exposure to identity-threatening environments is thought to contribute to identity dysfunction and negative affect in SGM individuals. In a world of increasing anti-SGM legislation in the United States (American Civil Liberties Union, 2026), prejudice, violence, and the threat of discrimination disrupt the maintenance of a stable, positive, and coherent SGM identity (Meyer, 2003). Research indicates exposure to identity-threatening contexts impedes SGM individuals’ self-concept development (Hossain & Ferreira, 2019). According to minority-stress theories, exposure to negative societal attitudes about SGM identity contributes to internalized SGM negativity and lower overall self-concept clarity. Actively hiding or concealing SGM status to manage stigma may reduce the immediate risk of harm while also threatening self-concept clarity, SGM-identity positivity, and sense of belonging in the moment (Bosson et al., 2012; Kiekens & Mereish, 2022; Newheiser et al., 2017).
Prior research has linked higher SGM-identity concealment with greater negative affect and identity dysfunction. In prior research, greater internalized SGM negativity on one day was associated with increases in depressed and anxious mood the following day in a 30-day EMA study (Dyar, 2024), and greater SGM negativity in response to discrimination was associated with greater negative affect in a 28-day daily diary study (Feinstein et al., 2022). In EMA research, SGM outness, or the degree to which others know about one’s SGM status, has been associated with greater identity affirmation and lower negative affect in daily life (Dyar et al., 2022), and greater concealment has been associated with higher negative affect (Kiekens & Mereish, 2022) and suicidal ideation.
Prior research indicates minority stressors are associated with greater momentary negative affect. In 14-day EMA daily diary studies, SGM individuals reported higher ratings of depressed mood (Livingston et al., 2020) and lower positive mood (Newberger et al., 2022) on days they experienced identity-based discrimination. Over 3 weeks, SGM individuals reported higher negative affect following experiences of identity concealment at work (Mohr et al., 2019). Over 30 days, internalized SGM negativity was associated with depressed and anxious mood (Dyar, 2024). Although this body of research indicates that minority stressors are associated with negative affect and identity dysfunction, no singular study investigates the unique associations between minority stressors, momentary identity dysfunction, and negative affect.
Theory further suggests that the strength of the association between minority stress and affect depends on the degree to which the minority stressor is associated with identity dysfunction (Branscombe et al., 1999; Emerson & Murphy, 2014). However, there is a dearth of empirical research on the relation between minority stressors, identity dysfunction, and affect. Still, extant research suggests that greater momentary identity dysfunction is associated with greater negative affect. For example, momentary decreases in self-concept clarity have been associated with momentary increases in negative affect and depression symptoms, such as feeling sad and nervous (Ellison et al., 2022), and intent to self-harm (Scala et al., 2018). However, this research has neither focused on SGM individuals nor directly included the impact of minority-stress processes in understanding these associations. Further investigation is needed to assess the theorized role of identity dysfunction in the relation between minority stressors and negative affect in daily life.
Depression Severity and Reactivity to Identity Threats
Depression symptoms have been associated with cumulative identity-threat exposure (e.g., an additive effect of repeated minority stressors) in prior research. This research demonstrates that individuals with higher depression severity also report more frequency and/or intensity of minority stressors. For example, gay men in China who reported concealing their sexual identity more often also reported higher depression severity and lower self-concept clarity (Li et al., 2022). Bisexual individuals reporting more identity-denial experiences, in which their bisexual identity was questioned or invalidated, reported higher depression severity and lower self-concept clarity and self-esteem (Garr-Schultz & Gardner, 2021). Gay and bisexual men indicating higher discrimination frequency in the prior 6 months also reported lower self-esteem and higher rates of suicidal ideation (Huebner et al., 2004). Furthermore, SGM individuals with higher internalized SGM negativity, lower self-concept clarity, and higher ambiguity about their sexual identity report more severe depression symptoms (Feinstein et al., 2012). However, the nature of the relation between depression symptoms and minority stress is unclear: Does minority-stress exposure contribute to increases in depression symptoms, and/or do individuals with higher depression severity react more strongly to minority stressors?
Individual differences in reactions to minority stressors may be associated with depression severity through (a) depression severity predicting individual differences in reactivity to identity threats and (b) reactivity to identity threats predicting increasing depression severity over time. Individuals reporting higher depression symptoms may be more reactive to stressful identity-threatening situations. Given that depression has been linked to greater affective and self-esteem reactivity to negative events (Clasen et al., 2015; Cohen et al., 2005; Parrish et al., 2011), we would expect individuals with higher depression severity to experience greater dips in self-esteem and self-concept clarity and greater increases in negative affect in reaction to identity-threatening events.
Identity Threats and Increasing Depression Severity
Identity-threatening events may also contribute to worsening depression symptoms over time. Individuals who experience greater identity dysfunction in reaction to identity-threatening events may be more likely to develop depression symptoms. Prior longitudinal research suggests that reactivity to stressors precedes an increase in depression severity, establishing that reactivity to stressors may be an important predictor for the course of depression (Cohen et al., 2005; Parrish et al., 2011). In addition, longitudinal research links identity dysfunction to increasing depression progression such that identity dysfunction in adolescence predicts an increase in depression symptoms 3 years later (Bogaerts et al., 2023). It is unclear whether a greater impact of stressors on identity functioning is associated with increasing depression symptoms. Given that reactivity to stressful events and greater identity dysfunction have been associated with worsening depression symptoms, we would expect that greater reactivity in identity dysfunction and affect to identity-threatening situations may be associated with increases in depression symptoms over time. Understanding the relation between identity threats and depression progression may help identify individuals at increased risk for depression.
Study Aims
SGM young adults are at increased risk for depression. Although there are many theories regarding the role of minority-specific events in depression for SGM individuals, the relation between depression and reactivity to minority-stress events in daily life has not been assessed. We explore the relation between SGM-specific stressors (e.g., number of discrimination events and low SGM visibility), identity functioning (self-concept clarity and SGM-identity positivity), negative affect, and depression symptoms (Fig. 1). We focus on SGM individuals ages 18 to 29 because of prior research highlighting identity development and manifestation of psychopathology during this period (Arnett, 2015). Preregistered SGM-specific stressors included a checklist of SGM-specific invalidating events and ratings of SGM-identity visibility—concealment and outness. Concealment and outness are considered distinct—yet related—aspects of SGM visibility; concealment represents active efforts to hide SGM status, and outness represents the extent to which one’s SGM status is known by the people around them (Jackson & Mohr, 2016). SGM individuals may report low outness when reporting high efforts to conceal SGM status. SGM individuals may also report low outness and low concealment when they are not expressing SGM status but are not actively hiding SGM status.
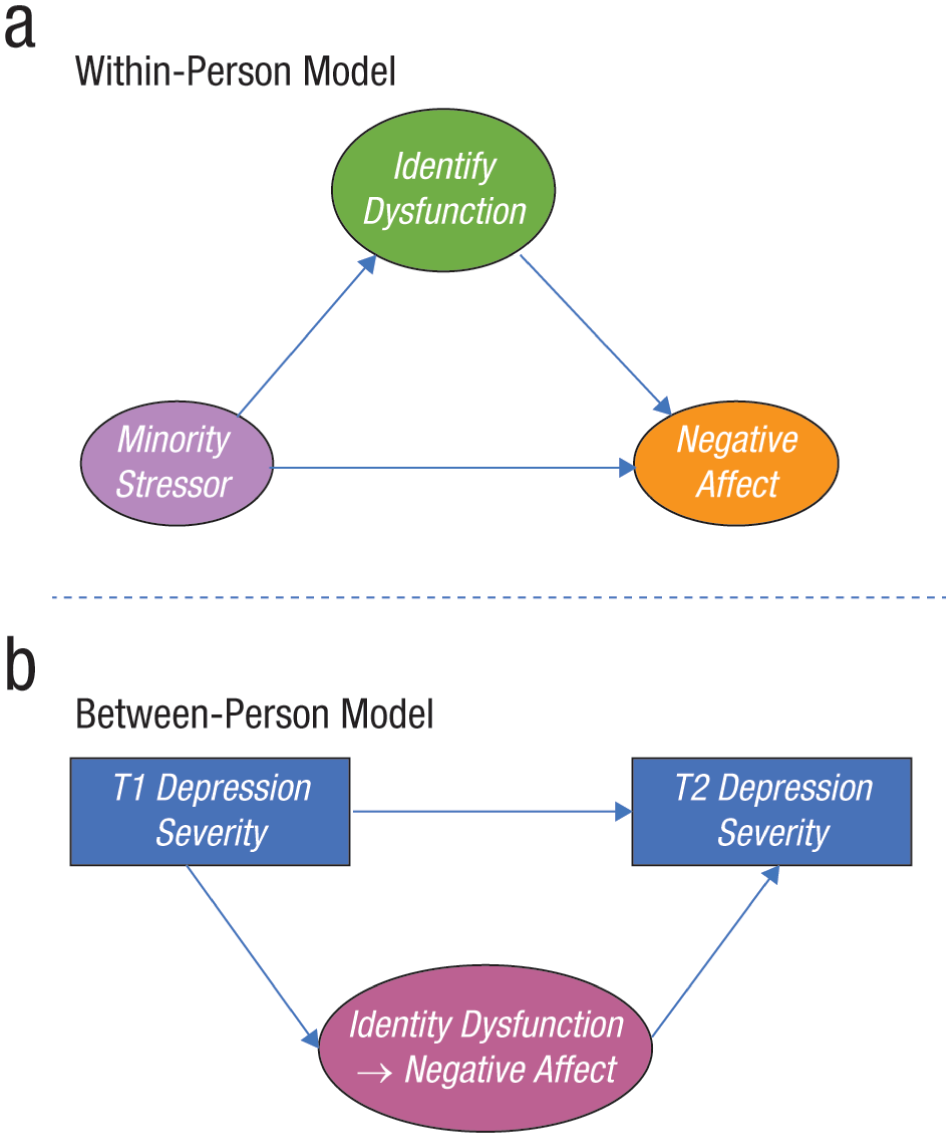
Diagram of the general multilevel structural equation model estimated for our main aims. Single-headed arrows represent regression paths. All random intercepts and slopes at the between-person level were allowed to freely covary. (a) The within-person model, which investigates the role of identity functioning in the relation between depression and negative affective reactivity to SGM-specific stressors. (b) The between-person model, which explores whether within-person increases in depression symptoms between the beginning and end of the EMA protocol are related to the average levels and within-person associations of negative affect and identity functioning. Covariates (sexual self-concept ambiguity and SGM-identity centrality) are not depicted. Identity Dysfunction → Negative Affect = individual difference variable representing negative-affect reactivity to identity dysfunction; minority stressor = SGM-specific minority stressor, assessed through level of SGM-identity concealment and SGM-identity outness; identity dysfunction = momentary identity dysfunction, assessed through lower self-concept clarity and lower SGM-positivity; negative affect = momentary negative affect; EMA = ecological momentary assessment; SGM = sexual and gender minority.
For clarity in the article as recommended from our reviewers, we consolidated our preregistered aims into the following two aims.
In Aim 1, we sought to investigate the role of identity functioning in the relation between depression and negative affective reactivity to SGM-specific stressors (Fig. 1a). At the within-person level, we predicted that SGM-specific stressors would be associated with identity dysfunction (lower momentary self-concept clarity and SGM-identity self-esteem relative to an individual’s average). We further anticipated that the momentary association between SGM-specific stressors and momentary identity functioning will partially account for the momentary association between SGM-specific stressors and negative affect. We hypothesized that greater decreases in identity functioning and greater increases in negative affect would partially account for the relation between SGM-specific stressors and depression severity. We also hypothesized that average level of self-concept clarity and SGM-identity positivity would relate to the within-person association between SGM-specific stressors and negative affect. Given that prior research has linked other SGM-identity variables to well-being, such as level of ambiguity about sexual orientation (Talley et al., 2015), we additionally hypothesized that sexual self-concept ambiguity and identity centrality (i.e., the degree to which SGM status is central to one’s self-concept) would be related to a stronger association between SGM-specific stressors and negative affect.
In Aim 2, we also explored whether within-person increases in depression symptoms between the beginning and end of the EMA protocol are related to the average levels and within-person associations of negative affect and identity functioning (Fig. 1b). We hypothesized that greater negative affective reactivity to low SGM visibility would predict increases in depression symptoms from Time 1 to Time 2. In addition, we predicted that greater reactivity to low SGM visibility (i.e., greater decreases in momentary identity functioning and greater increases in negative affect) would predict increases in depression symptoms from Time 1 to Time 2, controlling for the number of SGM-specific stressors and average negative affect.
Given that these relations between affect, SGM-specific stressors, and identity may represent generalizable social and identity processes in young adulthood, we chose to open our sampling to all SGM young adults ages 18 to 29 years. As detailed in the method section, our sample ultimately consisted of primarily White cisgender women and nonbinary individuals assigned female at birth who indicated sexual/romantic interest in multiple genders. Our results are considered in relation to this group.
Method
Transparency and openness
Preregistration
The analytic plan for the current study was preregistered after data collection and before any data analysis. The preregistration can be found at https://osf.io/cmjaz. All deviations from preregistered procedures are noted in this article.
Data, materials, code, and online resources
All data, code, and output of the models estimated as part of this study and the supplemental material are available at https://osf.io/ngq7p/. Note that Mplus input and output files can be opened with any text-editing program; Mplus is not required.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. Between-person sample size was determined by prior work indicating that correlation coefficients tend to stabilize at sample sizes around N = 250 (Schönbrodt & Perugini, 2013). A within-person sampling rate of 10 times per day was designed to achieve the maximal number of observations over an 8-day study duration without overburdening participants. To ensure reliable estimates of within-person associations, participants who provided fewer than 10 momentary observations over the 8-day period were excluded from analyses. Power was estimated at both the within- and between-persons levels using Monte Carlo simulations in Mplus using close approximations to the observed sample sizes (persons: N = 252; observations: N = 4,284). Assuming an intraclass correlation of .5, we have > .80 power to detect effects at α = .05 for standardized regression coefficients as small as .05 at the within-person level and .20 at the between-person level. This includes cross-level interactions.
Ethical approval
Study procedures were approved by the University of Pittsburgh Institutional Review Board (22080183).
Participants
Participants were two hundred fifty-two 18- to 29-year-old (M = 23.32 years, SD = 3.13) SGM young adults recruited in the Pittsburgh, Pennsylvania, area from December 2022 to June 2023. Recruitment sources included Pitt+Me (the University of Pittsburgh community research-recruitment source), flyers, and social media advertisements by the University of Pittsburgh Clinical and Translational Science Institute. Individuals were considered sexual-minority individuals if they indicated a sexual identity other than exclusively heterosexual (i.e., gay, lesbian, bisexual, pansexual, queer, questioning/I am still figuring out who I am attracted to, and/or other), indicated same-gender attraction, or indicated same-gender sexual experiences. Individuals were considered gender-minority individuals if they indicated a noncisgender identity by indicating a gender identity differing from their sex assigned at birth and/or a minority-gender identity (i.e., transmasculine, transfeminine, genderqueer, gender fluid, nonbinary, and/or another identity). All participants indicated residence in the United States and ownership of a smartphone compatible with the MetricWire survey app used for the EMA surveys.
Inclusion criteria for analyses involved completion of baseline questionnaires and at least 10 EMA survey responses over the EMA period in which participants reported they were around other people. This was a more burdensome sampling procedure than is typical (Wrzus & Neubauer, 2023) and included both randomly delivered prompts and event-contingent surveys regarding social interactions. We opted for this sampling procedure in an effort to capture as many assessments in social situations as possible. Participants reported their level of outness and concealment only when around others; therefore, we used only the observations that included these levels from randomly delivered prompts. Thus, our analyses used only the subset of survey responses in which others were present. The initial EMA sample included 285 participants, 33 of which were excluded for completing fewer than 10 random surveys while around other people. Final sample size was 252 participants with a total of 4,393 observations, or 22% of total randomly delivered surveys (17.43/participant). We expected that only a portion of randomly delivered surveys would involve others present as required by our analyses. Therefore, the relatively modest response rate on the random prompts is understandable in the context of larger number of surveys responded to each day. Sample demographics are provided in Tables 1 and 2. Participants were primarily White (84%) and assigned female sex at birth (86%). The sample varied in sexual and gender identity: Bisexual (45%) and queer (43%) were the most frequently endorsed sexualities, and cisgender woman (63%) and nonbinary (31%) were the most frequently endorsed gender identities. Note that the sample majority were not current students (60%). Given that participants were largely White, bi+, and assigned female at birth, results are discussed primarily as they relate to this group.
Sexual- and Gender-Minority Categories
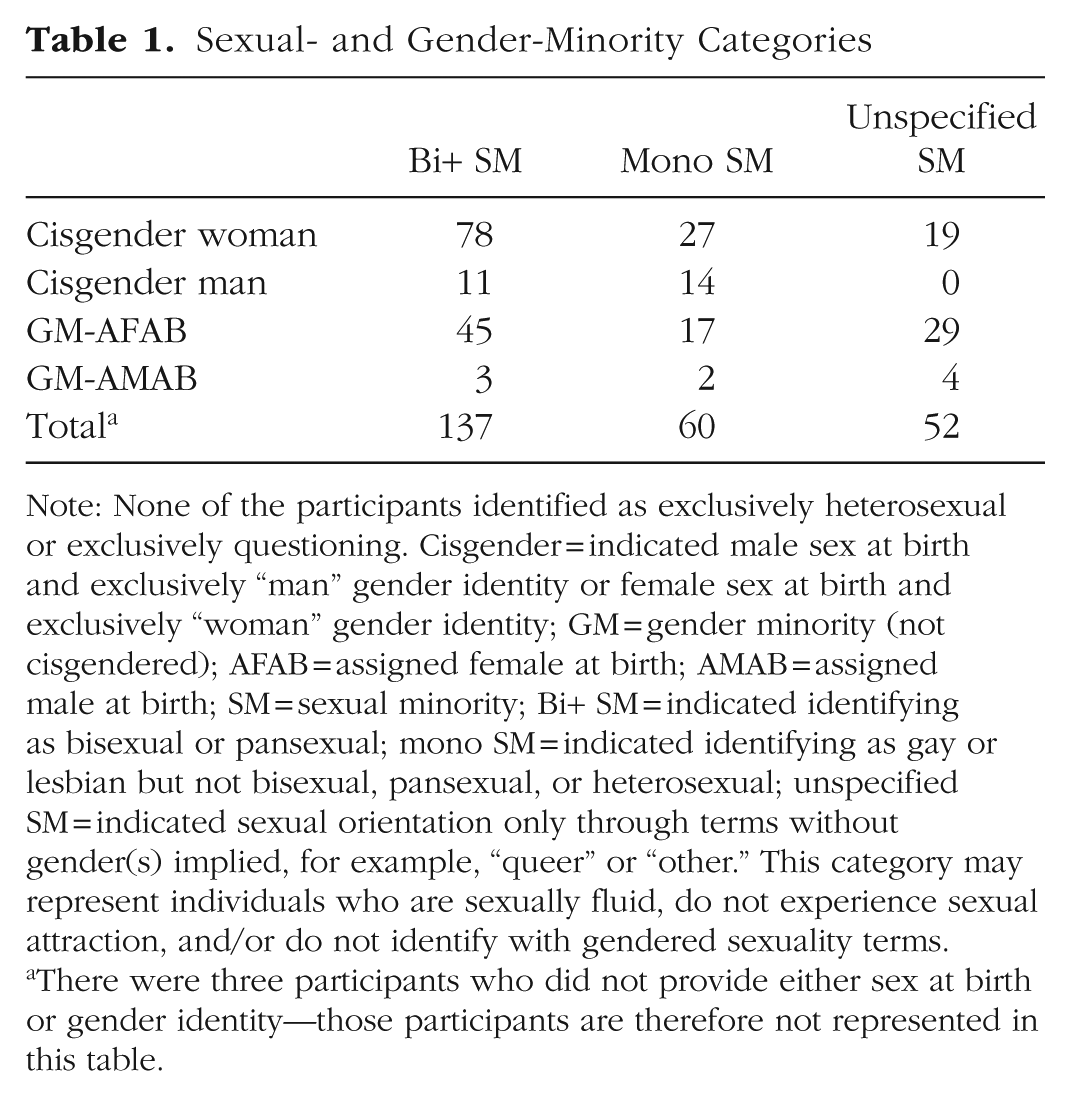
Note: None of the participants identified as exclusively heterosexual or exclusively questioning. Cisgender = indicated male sex at birth and exclusively “man” gender identity or female sex at birth and exclusively “woman” gender identity; GM = gender minority (not cisgendered); AFAB = assigned female at birth; AMAB = assigned male at birth; SM = sexual minority; Bi+ SM = indicated identifying as bisexual or pansexual; mono SM = indicated identifying as gay or lesbian but not bisexual, pansexual, or heterosexual; unspecified SM = indicated sexual orientation only through terms without gender(s) implied, for example, “queer” or “other.” This category may represent individuals who are sexually fluid, do not experience sexual attraction, and/or do not identify with gendered sexuality terms.
There were three participants who did not provide either sex at birth or gender identity—those participants are therefore not represented in this table.
Demographics
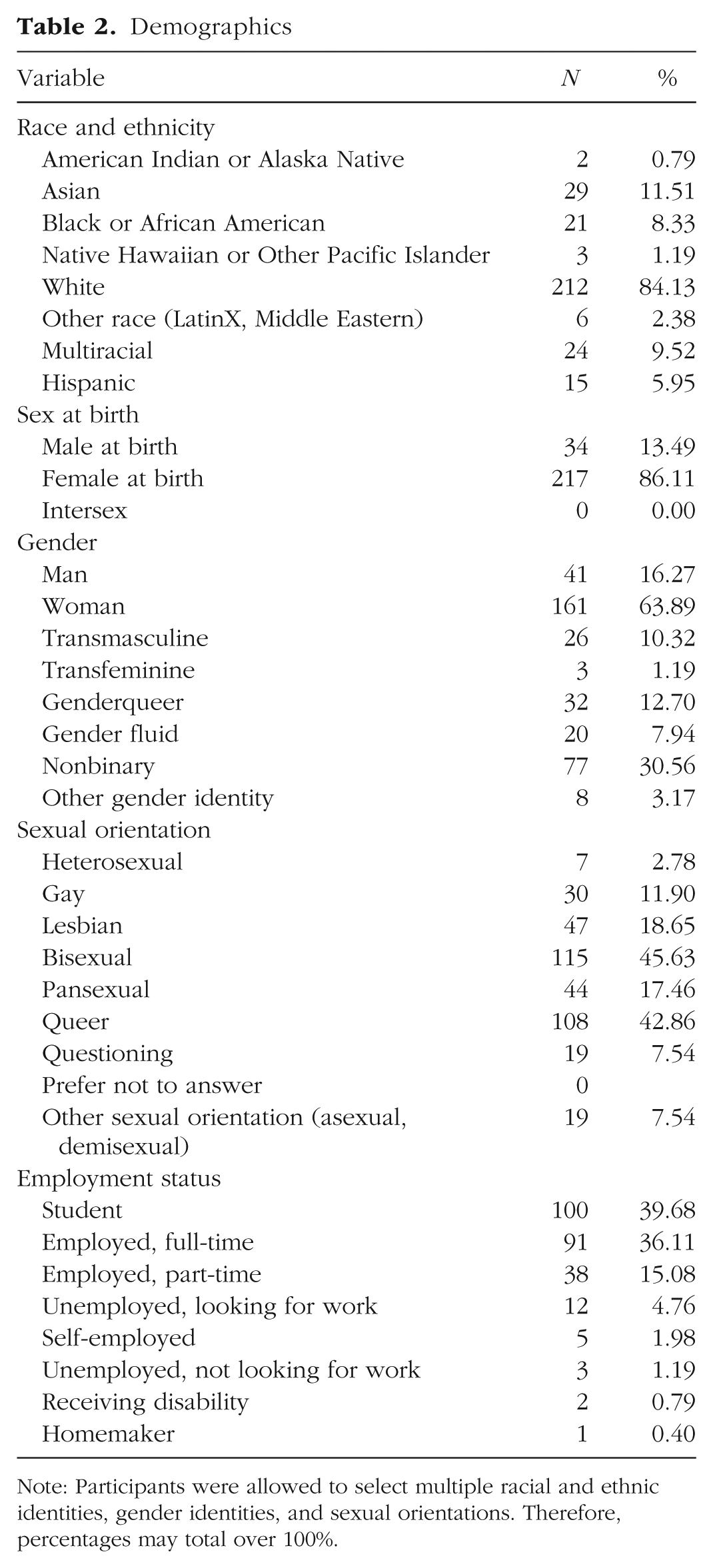
Note: Participants were allowed to select multiple racial and ethnic identities, gender identities, and sexual orientations. Therefore, percentages may total over 100%.
Study procedures
All study procedures were approved by the University of Pittsburgh Institutional Review Board. Participants were screened to determine eligibility before they were invited to review additional study information. Enrolled participants completed baseline questionnaires about SGM experiences, depression, and personality. Participants who opted into the EMA portion of the study viewed a training video about the EMA protocol and completed a comprehension quiz before beginning the EMA period via the MetricWire app lasting 8 days and consisting of (a) 10/day semirandomly delivered prompts and (b) a survey on the last day assessing depression symptoms over the past week. Compensation was proportional to the number of surveys completed, and the maximum was $100.
Measures
Momentary negative affect
Using a modified Positive and Negative Affect Schedule (PANAS) approach to measuring negative affect (e.g., Hall et al., 2021), an overall momentary negative-affect score was calculated as the mean of all assessed negative affects. Rather than using all 10 negative-affect words from the PANAS, negative affect was assessed in EMA surveys with the following terms on a sliding scale of 0 (not at all) to 100 (extremely): nervous, depressed, rejected, ashamed, guilty. Between-person reliability was good in our sample (α = .83). Negative affect was measured as a momentary construct and is treated as a momentary construct in this article unless specified otherwise.
SGM-specific invalidating events and other stressors
EMA surveys assessed past-hour discriminatory experiences via a checklist including nine items from the Everyday Discrimination Scale (e.g., “You were treated with less respect than other people are”; Williams et al., 1997) and the following items of SGM-specific experiences informed by previous research created for this study: “People denied or invalidated your LGBTQ+ identity,” “People expressed discomfort or disapproval of the LGBTQ+ experience,” and “People made jokes that involved microaggressions against the LGBTQ+ community.” Participants then attributed the source of the discrimination to aspects of their identity (e.g., race/ethnicity, disability, mental health, gender, sexual orientation, transgender identity, or other). Instances of discrimination attributed to sexual orientation or transgender experience were coded as SGM-specific invalidating events. Discrimination experiences in EMA surveys attributed exclusively to other identities besides SGM identity were coded as an “other stressor.”
Momentary SGM outness and concealment
Prior research suggests that concealment and outness, or visibility, are distinct processes (Jackson & Mohr, 2016). If participants indicated that they were around other people at the time of the EMA survey, they were asked about their levels of SGM-identity concealment and outness separately. Single items were developed for this study. SGM-identity concealment was assessed in EMA surveys with “I hid part of my LGBTQ+ identity from another person or other people” on a scale of 0 (not at all) to 10 (very much). SGM-identity outness was assessed with “The other person was aware of my LGBTQ+ identity” on a scale of 0 (not at all) to 10 (it was openly acknowledged). SGM visibility was measured as a momentary construct and is treated as a momentary construct in this article unless specified otherwise.
Momentary identity functioning
Identity functioning was assessed as self-concept clarity and SGM-identity positivity via the semirandomly delivered EMA surveys. Self-concept clarity was assessed using the four-item Momentary Self-Concept Clarity Scale (MSCCS; which includes items such as “Right now, I am wondering about what kind of person I really am” and “Right now, I’m not sure what I really believe in” (Ellison et al., 2022). Items are rated on a 4-point Likert scale from strongly disagree to strongly agree. Because three of the four MSCCS items are keyed toward identity dysfunction (rather than clarity), the one clarity item (“Right now, I have a clear sense of who I am”) was reverse-scored when calculating the MSCCS score, and the scale is considered a measure of identity dysfunction. Therefore, a lower MSCCS score reflects higher momentary self-concept clarity, and a higher score reflects higher momentary identity dysfunction. Between-person reliability in our sample for the MSCCS was good (α = .88). SGM-identity positivity was assessed with the item “I like my LGBTQ+ identity” on a sliding scale of 0 (not at all) to 10 (very much). This SGM-positivity item was developed for this study. Identity functioning was measured as a momentary construct and is treated as a momentary construct in this article unless specified otherwise.
Depression
Depression symptoms were assessed using the Patient Health Questionnaire (PHQ), which asks frequency of depression symptoms over the past week on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). Depression symptoms were first assessed at baseline, before the EMA period, using the nine-item PHQ (PHQ-9; Kroenke et al., 2001) and additionally assessed 9 days later at the end of the EMA period via MetricWire survey using the 8-item version (PHQ-8; Kroenke et al., 2009), which omits the question about suicidal ideation. Reliability in our sample was good for the PHQ-8 at Time 2 (α = .81) and the PHQ-9 at Time 1 (α = .86).
Trait SGM-identity functioning
We hypothesized that reactivity to SGM-specific stressors may be associated with characteristics of SGM identity, such as uncertainty about one’s sexual orientation, or sexual self-concept ambiguity (SSCA). We preregistered assessing SSCA at baseline using the Sexual Self-Concept Ambiguity Scale (SSAS; Talley & Stevens, 2017). As we prepared our data for analyses, we also thought to analyze the relation between reactivity and SGM-identity centrality given that centrality of SGM identity has been indicated as another influential identity characteristic (Hinton et al., 2022). We assessed SGM-identity centrality using four items from the Identity Centrality subscale of the Lesbian, Gay, and Bisexual Identity Scale (Mohr & Kendra, 2011), modified to be inclusive of gender-minority individuals. Items were rated on a 6-point Likert scale from 1 (disagree strongly) to 6 (agree strongly) and included “My LGBTQ+ identity is a central part of my identity” and “Being an LGBTQ+ person is a very important aspect of my life.” Reliability in our sample was good for the SSAS (α = .92) and the centrality subscale (α = .92).
Analyses
All analyses for the main aims were conducted in R studio (Version 4.2.2; RStudio Team, 2020), using the tidyverse package (Wickham et al., 2019), and Mplus (Version 8.6; Muthén & Muthén, 2017). Statistical models were preregistered on OSF with the intention of investigating the relation between depression and daily life reactivity to two types of minority-stress experiences: (a) SGM-specific invalidating events, such as discrimination or identity-invalidating jokes about the LGBTQ+ experience, and (b) actively hiding SGM identity (higher concealment) or limiting open expression of SGM identity (lower outness). However, our sample reported very low rates of SGM-specific invalidating events over the 8-day EMA period; only 67 participants out of 252 reported at least one event (M = 3.49, SD = 5.03 for those 67 participants). Potential reasons for this low endorsement rate are described further in the discussion section. Given that we did not have the statistical power to conduct our preregistered analyses on reactivity to SGM-specific events, we focus here on analyses involving reactivity to situations involving modulating SGM concealment and outness.
Analyses involved momentary negative affect, self-concept clarity, SGM-identity positivity, concealment, outness, baseline depression severity, SSCA, and SGM-identity centrality. We used multilevel structural equation models (MSEMs) with Bayesian estimation for primary models, nesting momentary assessments within individuals to investigate within- and between-person associations among depression, outness and concealment, affect, and identity functioning (Fig. 1). For variables measured during momentary assessments, which vary both within and between persons, MSEMs perform a latent partitioning of the total variance in observed variables into their within-person and between-person portions of variance (e.g., Lüdtke et al., 2008). The between-person variance reflects the average or individual differences in the endorsement of momentary variables, whereas the within-person variance reflects momentary deviations from an individual’s average. Thus, the within-person variance effectively person-centers the variables, allowing for estimation of associations among momentary fluctuations in variables relative to the individual’s average levels. All within-person effects were estimated as random, allowing for the strength of within-person associations to vary across individuals. In MSEMs, random effects of within-person associations are treated as between-person latent variables (e.g., individual differences in the strength of association among outness and affect in the moment) and can be associated with other between-person variables. In addition, variables sampled at the between-person level only (e.g., PHQ-9 in these data) can be included in these models at the between-person level.
In our primary model for Aim 1, at the within-person level, we entered both identity-functioning variables (self-concept clarity and SGM-identity positivity) into one model to examine their simultaneous roles in accounting for the association between concealment and outness and negative affect (Fig. 2), and the between-person level baseline variables of PHQ-9, SSCA, and SGM-identity centrality were included as correlates of the random effects. Toward Aim 2, we investigated whether within-person increases in depression symptoms between the beginning (Time 1) and end of the EMA protocol (Time 2) were related to the levels and within-person associations of momentarily assessed negative affective reactivity to concealment and outness.
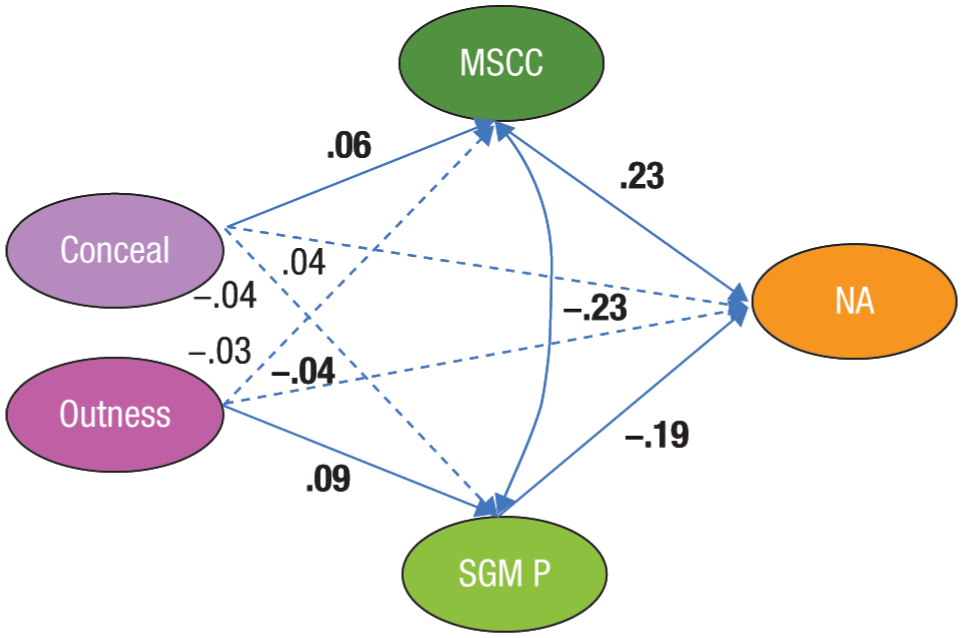
Diagram of the within-person associations in the combined multilevel structural equation model. Conceal = momentary concealment; outness = momentary outness; MSCC = momentary self-concept clarity; SGM = sexual and genderminority; SGM P = SGM-identity positivity; NA = negative affect. Single-headed arrows represent regression paths. Solid arrows represent significant associations (based on 95% credibility intervals). Dashed lines represent nonsignificant associations. Estimates are provided for significant associations. Covariates included for between-person associations (sexual self-concept ambiguity, depression, and SGM-identity centrality) are not depicted in this figure but were included in the model this figure represents.
All models were estimated with 10,000 iterations, and the first 5,000 were discarded as burn-in. We have found that 10,000 iterations typically work well with models similar to these in other data sets. Model convergence was determined using the potential scale-reduction factor value of < 1.1 (Gelman & Rubin, 1992) in addition to evaluation of the plots of the parameters’ posterior distributions, trace plots, and plots of the autocorrelations. Coefficients are presented along with their 95% credibility intervals (CIs), which were used to determine parameter significance.
Results
Descriptive statistics and bivariate correlations for within- and between-person effects are reported in Table 3. We first investigated associations between components of our main model in a series of multilevel models (see supplemental material on OSF). Table 4 reports between-person associations from our primary MSEM including baseline variables of centrality, depression, SSCA, negative affect, concealment, outness, self-concept clarity, and SGM positivity in daily life.
Between-Person Correlations and Means for Baseline Variables and Person-Centered 8-Day Averages for Momentary Variables and Within-Person Correlations for Momentary Variables
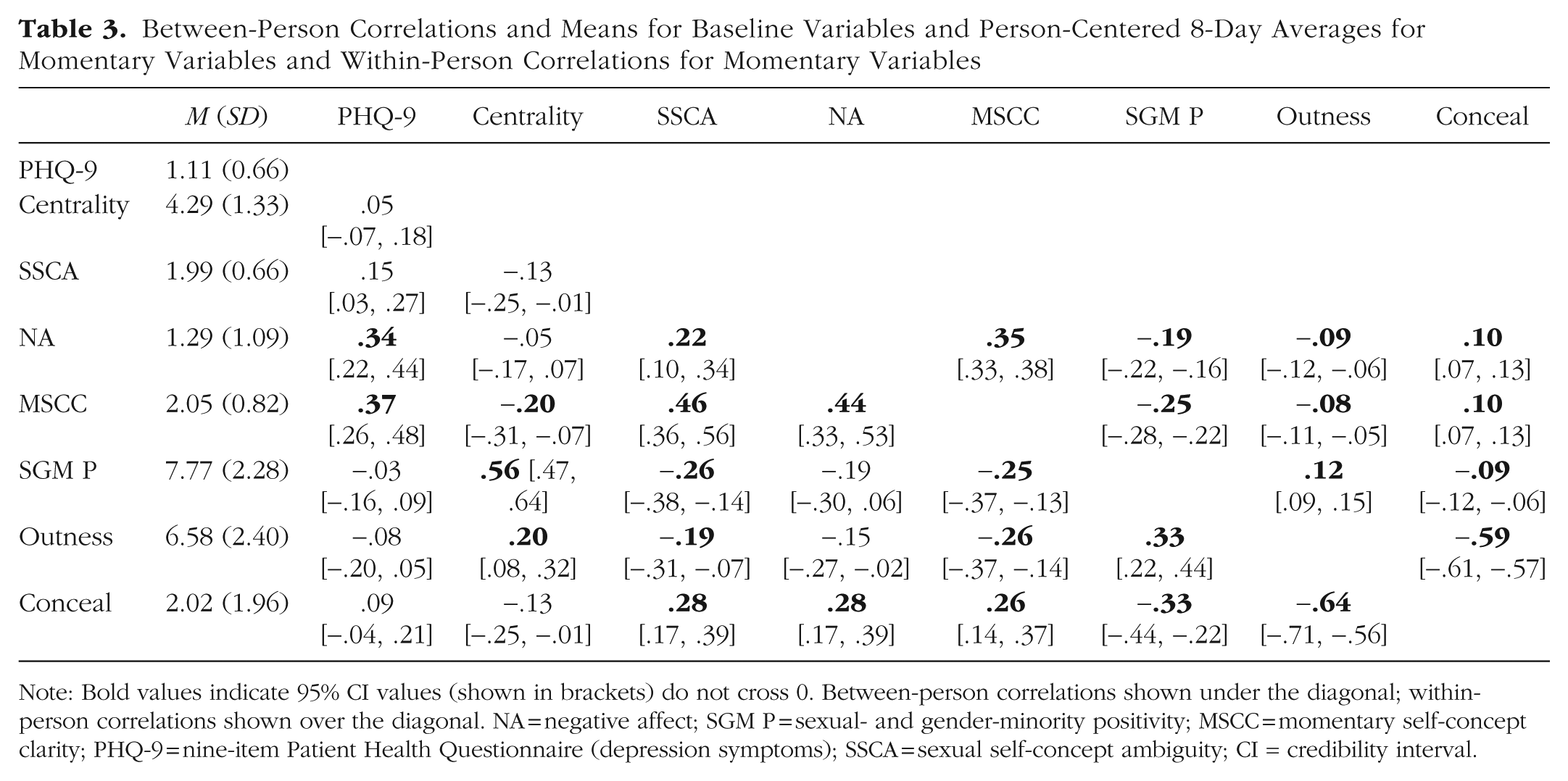
Note: Bold values indicate 95% CI values (shown in brackets) do not cross 0. Between-person correlations shown under the diagonal; within-person correlations shown over the diagonal. NA = negative affect; SGM P = sexual- and gender-minority positivity; MSCC = momentary self-concept clarity; PHQ-9 = nine-item Patient Health Questionnaire (depression symptoms); SSCA = sexual self-concept ambiguity; CI = credibility interval.
Between-Person Associations From the Combined Model Including Baseline Variables and Negative Affect, Identity, and Concealment and Outness in Daily Life
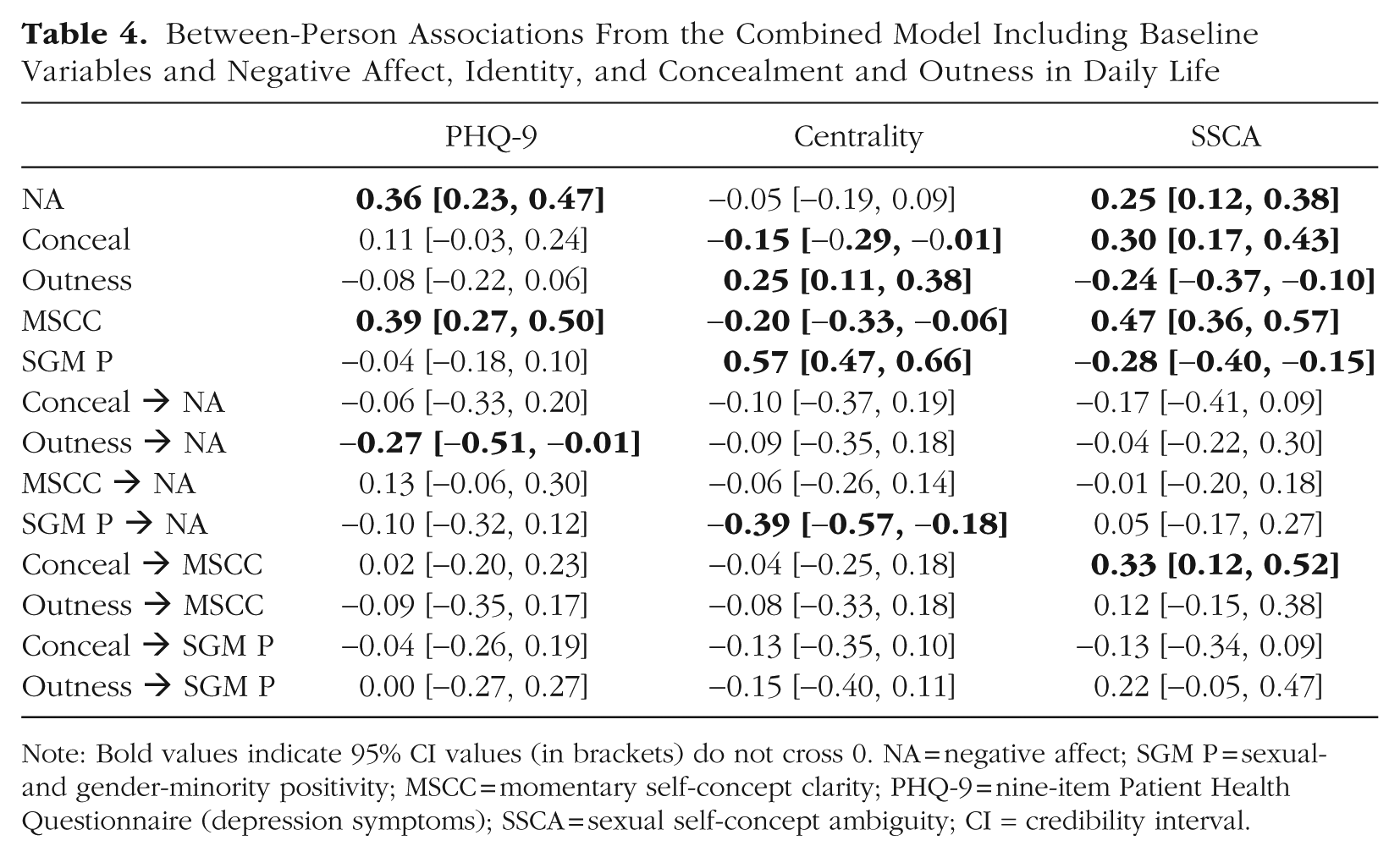
Note: Bold values indicate 95% CI values (in brackets) do not cross 0. NA = negative affect; SGM P = sexual- and gender-minority positivity; MSCC = momentary self-concept clarity; PHQ-9 = nine-item Patient Health Questionnaire (depression symptoms); SSCA = sexual self-concept ambiguity; CI = credibility interval.
Aim 1: SGM visibility, identity functioning, and negative affect
For our primary MSEM, at the within-person level, we entered both identity-functioning variables (self-concept clarity and SGM-identity positivity) into one model to examine their simultaneous roles in accounting for the association between concealment and outness and negative affect (Fig. 2), and the between-person level baseline variables of PHQ-9, SSCA, and SGM-identity centrality were included as covariates of the random effects. In this model, all within-person associations were significant except the relation between momentary negative affect and momentary concealment, suggesting that identity functioning partially accounted for the relation between negative affect and concealment in daily life (Table 4). In the within-person part of the model, momentary negative affect was significantly associated with lower momentary outness (β = −0.04, 95% CI = [−0.08, −0.00]). Higher momentary negative affect remained significantly associated with lower momentary self-concept clarity (β = 0.23, 95% CI = [0.19, 0.27]) and lower momentary SGM-identity positivity (β = −0.19, 95% CI = [−0.23, −0.14]). Momentary SGM positivity remained significantly associated with momentary outness (β = 0.09, 95% CI = [0.04, 0.13]), and momentary self-concept clarity remained significantly associated with momentary concealment (β = 0.06, 95% CI = [0.02, 0.11]). At the between-person level, higher average negative affect was associated with higher average concealment (r = .32, 95% CI = [.18, .45]), lower SGM-identity positivity (r = −.21, 95% CI = [−.34, −.07]), lower self-concept clarity (r = .46, 95% CI = [.34, .56]), and higher self-concept clarity reactivity to concealment (r = .28, 95% CI = [.07, .48]). These results suggest that both self-concept clarity and SGM-identity positivity are associated with modulating SGM social identity in daily life.
Baseline depression severity was not associated with reactivity in negative affect or identity functioning to concealment or outness (Table 4). Higher baseline SGM-identity centrality was associated with greater negative affective reactivity to SGM-identity positivity such that for individuals with higher SGM-identity centrality, decreases in SGM positivity were associated with greater increases in negative affect (r = −.39, 95% CI = [−.57, −.18]). Higher baseline SSCA was associated with greater momentary self-concept clarity reactivity to concealment such that increases in concealment were associated with greater decreases in self-concept clarity (r = .33, 95% CI = [.12, .52]) for individuals with higher baseline SSCA. Therefore, individuals who considered their SGM status as more central to their identity reported more negative affect with decreased SGM positivity, and individuals who were more uncertain about their sexual orientation reported less self-concept clarity with increased concealment.
Aim 2: change in depression severity and reactivity to minority stress
As part of our preregistered exploratory analyses, we investigated whether within-person increases in depression symptoms between the beginning (Time 1) and end of the EMA protocol (Time 2) are related to the levels and within-person associations of momentarily assessed negative affective reactivity to concealment and outness. Past-week PHQ-8 scores from both time points were used for comparison (i.e., the suicide question from PHQ-9 was not collected at follow-up). Time 1 depression severity was strongly associated with Time 2 depression (β = 0.52, 95% CI = [0.44, 0.59]). PHQ at Time 2 was significantly associated with average levels of negative affect during the EMA period (r = .26, 95% CI = [.11, .40]). However, depression at neither Time 1 nor Time 2 was associated with negative affective reactivity to concealment or outness.
We then included self-concept clarity in the model to explore whether changes in depression severity are associated with self-concept clarity reactivity to concealment and outness. Time 2 depression scores were associated with lower average self-concept clarity (r = .34, 95% CI = [.20, .47]). However, depression at neither Time 1 nor Time 2 was associated with self-concept clarity reactivity to concealment or outness. When estimating the model with SGM-identity positivity, average level of SGM-identity positivity was not associated with Time 2 depression severity. Given that depression levels at Time 1 and Time 2 were not significantly associated with reactivity in negative affect or identity functioning to concealment or outness, we did not run models exploring change scores in depression severity.
Discussion
SGM individuals report higher rates of depression and identity dysfunction compared with their cisgender, heterosexual peers (Pakula & Shoveller, 2013). Given that situations that threaten or invalidate SGM identity may contribute to depression in SGM individuals, we investigated the relations among depression symptoms and the reactions of identity dysfunction and negative affect to daily life SGM experiences of modulating outness. In 8 days of smartphone survey responses from a sample of SGM emerging adults (primarily bi+ individuals assigned female at birth), we found that negative affect reported in situations of higher concealment and lower outness was associated with momentary identity dysfunction. Specifically, momentary higher concealment (compared with the individual’s average) was associated with momentary lower self-concept clarity, and lower outness was associated with lower SGM-identity positivity. These results suggest that situations eliciting SGM-identity concealment and discouraging outness limit identity functioning and promote negative affect. We did not find direct links between depression symptoms and reactivity to modulating SGM social identity. However, we did find a significant indirect association such that depression symptoms and negative affective reactivity were associated with concealment only for individuals with higher average levels of negative affect. Given that greater negative affect is a core feature of many forms of psychopathology, this process of identity threats contributing to negative affect through identity dysfunction may partially explain higher rates of depression and other forms of psychopathology among SGM young adults.
Our findings generally support our hypothesis that situations threatening SGM identity tend to promote negative affect by disrupting identity functioning. However, we did not anticipate that SGM experiences of concealment and outness would be differentially associated with two types of identity dysfunction. Higher levels of concealment were associated with lower momentary general self-concept clarity but not lower SGM-identity positivity. Lower levels of outness were associated with lower SGM-identity self-esteem but not lower self-concept clarity. Therefore, concealment and outness may be associated with negative affect through different identity processes.
Given that prior research indicates processes of concealment and outness may be particularly multifaceted in bi+ populations and gender-nonbinary populations (Feinstein et al., 2019; Johnson et al., 2024), our results may indicate processes specific to this sample and may not be fully generalizable to exclusively gay/lesbian sexual-minority individuals, cisgender male sexual-minority individuals, or binary, transgender gender-minority individuals. As we discuss the relations between outness, identity dysfunction, and affect, we also consider the potential influence of experiences specific to bi+ individuals assigned female at birth investigated in prior research.
Concealment
We found that higher momentary concealment was associated with lower momentary self-concept clarity but not lower SGM-identity positivity. Prior research supports the link between concealment and lower self-concept clarity. Self-concept clarity involves a sense of consistency in self-concept over time and across situations. Concealing one’s identity may cause an inconsistency in the self-concept, a discrepancy between one’s internal self-concept and social representation of the self-concept. Prior research suggests that highlighting inconsistencies in the self-concept reduces self-concept clarity (Boucher et al., 2016). Therefore, conflicting internal and social self-concepts may leave individuals feeling fragmented when concealing their SGM status, contributing to an overall decreased sense of self-concept clarity.
Although the link between inconsistency and self-concept clarity may be a more general process, prior research suggests that concealment may not be consistently associated with SGM-identity positivity. Rather, one’s motivation for concealment may indirectly link concealment and SGM positivity. SGM individuals report many motivations for concealment, sometimes concealing out of fear for their own safety and sometimes concealing out of their own uncertainty or discomfort regarding their identity (Feinstein et al., 2020). Although we do not assess outness motivations in this study, these prior findings suggest that whether an association is observed between concealment and SGM positivity may be a function of the motivation for concealment in the moment. For instance, concealing because of internalized negative attitudes might be associated with SGM positivity, but concealing to minimize negative social consequences would not. Concealment motivation may also explain links between concealment and negative affect. For example, Feinstein et al. (2020) found that concealing bi+ identity because of concerns about judgment or victimization was associated with higher levels of depression and anxiety but concealing because of uncertainty about bi+ identity was not. Further research is needed to investigate the role of concealment motivation in the link between concealment and SGM-identity positivity.
Outness
SGM-identity outness was associated with SGM-identity positivity such that less momentary outness was associated with lower SGM-identity positivity but outness was not associated with self-concept clarity. It may be that choosing not to express SGM social identity creates less dissonance between the internal and social self-concepts than choosing to actively conceal identity such that lower outness is not associated with lower self-concept clarity. Lower outness may instead be in line with the individual’s preference in the moment to limit self-expression and/or contextual factors discussed more below.
The relation between outness and SGM-identity positivity could be explained by several processes described in prior literature on SGM outness. First, how one feels about one’s SGM identity in the moment contributes to level of outness. The role of internal attitudes about SGM identity in outness is supported by prior research on bi+ women, which also found that greater outness was associated with higher SGM-identity centrality and lower SGM-identity ambiguity (Dyar et al., 2015). Individuals may choose to disclose less when they are already experiencing lower SGM-identity positivity and disclose more when they are experiencing higher SGM positivity. Second, the link between outness and SGM-identity positivity may indicate the influence of social situations on both self-expression and positivity. Outness may occur less in social situations in which personal self-expression is less comfortable (e.g., with strangers or acquaintances) or perceived as not immediately relevant (e.g., at work). Higher levels of outness may occur in instances in which self-expression is more comfortable (e.g., with close friends) or perceived as immediately relevant (e.g., around a potential romantic partner). Prior research on bi+ visibility suggests that although outness is generally associated with positive affect and identity affirmation, these positive outcomes were dependent on a supportive social context (Dyar et al., 2022). The social context may be particularly relevant to bi+ individuals, who report difficulty expressing their sexual-minority status through appearance (Hayfield et al., 2013) and may need to express verbally. Furthermore, the strategy for bi+-identity visibility (e.g., direct communication, indirect communication, visual displays) may influence visibility outcomes (Feinstein et al., 2021). Given that we assessed momentary SGM-identity outness with “The other person was aware of my LGTBQ+ identity,” our largely bi+ sample may be indicating outness primarily in contexts in which verbal self-expression is comfortable and SGM positivity may be higher (e.g., with close others). Therefore, it is impossible to determine from our findings whether the link between momentary outness and SGM-identity positivity may be better explained by internal attitudes about SGM identity or the interpersonal situation. We recommend that further EMA research includes additional contextual variables that are likely to affect outness, such as level of SGM-identity expression, salience or centrality of SGM status in the moment, and perceived SGM status of other people in the interaction.
Depression
We aimed to investigate the relation between depression symptoms and SGM concealment and outness processes in daily life. Although we did not find a direct association between depression and reactivity to concealment and outness, we did find a significant indirect effect between the two with average negative affect such that individuals with higher average negative affect had greater negative affective reactivity to concealment and higher depression severity. However, the reason for this effect is unclear. Negative affect may be a more proximal outcome to identity threats in daily life, whereas heightened depression symptoms are more distally related to identity threats. The depression symptoms may be an outcome and/or risk factor for the negative affect associated with identity threats. Alternatively, there may be a methods effect such that a true direct link between depression symptoms and affective reactivity to concealment and outness could not be detected when depression was assessed at baseline and concealment, outness, and negative affect were assessed through EMA surveys. Further research using different assessments for negative affect and depression symptoms over different timescales is needed to assess the link between outness and depression.
Another possibility is that identity threats are associated with other forms of psychopathology besides depression. Although low mood is a core feature of depression, negative affect is also a feature or outcome of many other psychiatric disorders (Stanton, 2020). There may be a direct link between reactivity to concealment and other disorders with higher prevalence among SGM individuals, such as substance use disorders and personality disorders. Further research investigating the relation between concealment, outness, and other forms of psychopathology may help elucidate the role of identity threats in the manifestation and maintenance of different disorders in SGM individuals.
SGM experiences of our sample: bi+, assigned female at birth
The identities represented in our SGM sample may influence these results. Our sample primarily identified sexually as bi+, meaning they experience sexual/romantic interest in more than one gender. Bi+ individuals report more concealment and less outness than gay and lesbian individuals (Mohr et al., 2017; van der Star et al., 2019) and report identity invalidation from both heterosexual and gay/lesbian individuals (Feinstein & Dyar, 2017), suggesting that the situations and processes of modulating outness in our sample may differ from those observed in a predominantly gay/lesbian sample. Bi+ individuals also report higher levels of general identity dysfunction (Talley et al., 2011) and sexual-identity uncertainty (Talley & Stevens, 2017) compared with other sexual minorities and more exposure to stereotypes about their identities being unstable and phasic from heterosexual individuals and other sexual-minority groups (Feinstein & Dyar, 2017). Furthermore, outness may be associated with different health outcomes for bi+ individuals compared with gay/lesbian individuals (Feinstein et al., 2019). Therefore, the relation between outness and identity functioning observed in our sample may represent bi+-specific processes or processes amplified among bi+ individuals.
The gender makeup of our sample may also restrict interpretation of our results. Our sample was also predominantly assigned female at birth, and participants largely identified as exclusively cisgender women or as gender-nonbinary individuals. Concealment and outness processes may be different for gender-minority individuals compared with cisgender sexual-minority individuals. There may be a greater risk of victimization for gender-minority individuals, with more immediate negative physical and social consequences when one is open about gender-minority identity, making outness a potentially riskier process than concealment in certain contexts (Flynn & Smith, 2021). Identity threats affecting mental health for gender-minority individuals may often take the form of identity invalidation, in which one’s gender identity is directly challenged or ignored. For example, the process of “passing” as binary-gendered has been associated with distress for nonbinary individuals, suggesting that lower outness may be particularly associated with momentary identity dysfunction and negative affect for nonbinary individuals (Flynn & Smith, 2021). Nonbinary individuals report more frequent exposure to identity invalidation compared with binary-trans individuals, with identity invalidation partially explaining variance in psychopathology severity (Johnson et al., 2024). Therefore, the nonbinary individuals in our sample may experience more identity threats primarily involving identity invalidation than other SGM groups. Further research is needed to investigate differences in the impact of identity-invalidating events compared with other types of identity threats in different SGM populations.
Further research is needed to apply our findings in the conceptualization or treatment of depression in bi+ individuals. However, our findings support conceptualization of low mood and identity dysfunction in this population as related to minority-stress exposure—specifically, situations of low SGM visibility. Treatments for depression in bi+ young adults may benefit from addressing SGM visibility, including validating the potential impact of low SGM visibility on self-concept clarity, SGM positivity, and mood. In addition, our findings suggest that individual differences in how SGM individuals relate to their SGM identity may inform their responses to minority stressors. For example, patients who see their SGM status as more central to their overall self-concept may derive greater benefit from a treatment acknowledging the role of SGM visibility than patients who are more uncertain about their SGM status or do not see it as central to their overall self-concept.
Limitations
Given that our sample is primarily bi+ 18- to 29-year-old individuals assigned female at birth, with a mix of cisgender and nonbinary gender identities, our results are contextualized in the experiences of women and nonbinary bi+ individuals. To meet demands of statistical power for our analyses, we were unable to separate our sample into groups based on sexual orientation or gender identity. Further studies are needed to investigate whether these findings replicate in samples of other SGM groups across age cohorts. Given that racial and ethnic experiences may influence reactions to SGM-specific experiences, further research is needed to examine the role of intersectionality across racial and ethnic groups for SGM individuals (Fox et al., 2020; Jardas et al., 2023; Mereish et al., 2021).
Because of low frequency of identity-invalidating events, we were unable to test our hypotheses about the relation between depression and discrimination. The low frequency in reporting may be a result of the sociopolitical climate in Pittsburgh, Pennsylvania, a city with several large universities and a more liberal climate than the surrounding area. Furthermore, individuals may have been uncomfortable responding about an adverse event related to their identity such that responses may be missing not at random. We attempted to reduce barriers to completing the surveys in situations participants may be concealing their sexual or gender status by using the study name “Experiences in Daily Life” in survey prompts rather than explicitly referencing SGM status. However, it is possible some participants did not engage with the app when experiencing stressful events. In addition, our assessment of events may have been lacking important manifestations of identity-invalidating contexts or behavior, leaving participants without the ability to share all they experienced. Our events were typically direct and in person. However, future studies may benefit from including vicariously experienced events both in person and via media (e.g., “I saw a negative social media comment about my identity”) to better capture the types of identity invalidation faced by SGM young adults today (Marciano & Antebi-Gruszka, 2022) and expand the sampling period beyond 8 days. Inclusion of events specific to the SGM sample may also be beneficial. For example, bi+ samples and nonbinary samples may be more likely to endorse identity-threatening events characterized by invalidation rather than discrimination in a more liberal area.
Although theory suggests a causal link between minority stressors, identity dysfunction, and negative affect, we were able to investigate only contemporaneous associations given our study design. Participants tended to complete few surveys per day, with hours between survey completion, making it impossible to detect lagged effects in our data for a process occurring on a short timescale. For rapid processes like these, potential causal associations are expected to be reflected in contemporaneous associations (Granger, 1969). In our within-person analyses, we were able to demonstrate that situations of lower SGM visibility are associated with greater identity dysfunction and negative affect, finding that identity dysfunction moderates the association between SGM visibility and negative affect and an indirect effect of identity functioning on the association between SGM visibility and negative affect. These findings lend support to theory that minority stressors contribute to negative affect at least partially because of their effect on identity functioning. However, we are unable to claim causal mediation from our analyses. To better investigate causation, we suggest that future ambulatory-assessment studies collect more survey data on a shorter timescale around a minority-stress event. One method for this may be combining randomly delivered prompts with bursts of follow-up, event-contingent surveys when a minority stressor has been reported (Kaurin et al., 2026). We also recommend that future studies with a shorter timescale around minority-stress events investigate potential autoregressive effects given the potential carryover effects of one time point to another.
Our assessment of depression symptoms was also limited. Although we found an indirect link between depression and negative affective reactivity to concealment through average levels of negative affect during the EMA period, we did not find a direct link between depression and negative affective reactivity to concealment or outness. Additional research is needed to further investigate the relation between depression and identity threats for SGM individuals. Future research may investigate this process in a sample with higher depression severity and assess the relation between depression, concealment, and outness over a longer timescale.
Note that the depression severity for this sample was relatively mild. This is likely contributing to lack of variability in depression symptoms between participants and lack of variability in changes to depression severity over time. The reactivity to low SGM visibility described in this study may therefore be more representative of general minority-stress processes rather than reactivity associated with depression. Depression severity may be relatively low in our sample because of our recruitment method or study protocol. We recruited from the general community with flyers rather than from hospitals or mental-health clinics. Our study protocol may have been too demanding for individuals experiencing depression. Given the elevated prevalence of depression among SGM individuals compared with cisgender, heterosexual peers, we encourage future research to sample for depression severity and consider less burdensome sampling methods to better understand minority-stress processes in the context of depression.
Although our project focused on depression, further research is needed to investigate associations between minority stressors and other aspects of psychopathology, including other internalizing symptoms, such as anxiety, and externalizing symptoms, such as impulsivity. Given the high rates of depression in SGM young adults, we primarily focused on depression severity and momentary negative affect for this initial study. However, future studies may investigate the role of minority stressors and identity dysfunction in other features of psychopathology. Prior EMA research suggests that minority stressors may be similarly associated with momentary anxiety (Livingston et al., 2020), and further research is necessary to investigate whether identity dysfunction plays a role in the association between minority stress and anxiety.
Conclusion
Minority-stress theory and identity-threat theory both suggest that experiences with concealing SGM status are associated with momentary identity dysfunction and negative affect, although few empirical studies have investigated these associations. In this project, we investigated whether day-to-day processes of reactivity to concealment and outness explain individual differences in depression severity. We found that concealment and outness were differentially associated with self-concept clarity and SGM-identity positivity. Our results support that situations promoting concealment and limiting outness relate to negative affect through identity processes, functioning as identity threats. Furthermore, concealment and outness may relate to negative affect through different identity processes. Contrary to our hypotheses, we did not find a direct link between depression symptoms and reactivity to modulating concealment and outness over 8 days. Further research is needed to explore the relation between concealment, identity dysfunction, and depression across different SGM groups and age cohorts and SGM social identity expression and other forms of psychopathology. This project provides a potential framework for the relation between SGM-specific experiences, identity dysfunction, and negative affect in daily life.
Supplemental Material
sj-xlsx-1-cpx-10.1177_21677026261417349 – Supplemental material for Depression, Identity Functioning, and Negative Affective Reactivity to Sexual- and Gender-Minority Concealment and Outness in Daily Life in a Predominantly Female Bi+ Sample
Supplemental material, sj-xlsx-1-cpx-10.1177_21677026261417349 for Depression, Identity Functioning, and Negative Affective Reactivity to Sexual- and Gender-Minority Concealment and Outness in Daily Life in a Predominantly Female Bi+ Sample by Sienna R. Nielsen, Craig Rodriguez-Seijas, Sophia Choukas-Bradley and Aidan G. C. Wright in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Chelsea Boccagno
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.