
Abstract
The biopsychosocial model is perhaps the most widely accepted model of mental health. Yet the model is also surprisingly limited, failing to provide clear guidance for clinical research. In this article, we join recent efforts to chart a path forward for the biopsychosocial model, arguing that the success of this framework will hinge on the ability to engage in transdisciplinary collaboration. We begin by showing that the biopsychosocial model is a systems model and that collaboration with researchers studying systems in other disciplines will therefore afford insight into the nature, etiology, and treatment of mental disorders. We then illustrate how biological, psychological, social, and environmental systems all contribute to mental health and argue that advancing the understanding of mental health will therefore require collaborative integration of work from across domains of science. We conclude with three concrete steps that can help move the field toward a transdisciplinary systems science of mental health.
Keywords
If and when a general-systems approach becomes part of the basic scientific and philosophic education of future physicians and medical scientists, a greater readiness to encompass a biopsychosocial perspective of disease may be anticipated.
Nearly half a century ago, Engel (1977) proposed that medicine needed a new framework for understanding disease. Engel argued that the dominant model of that time, the biomedical model, was untenably reductionist, assuming disease “to be fully accounted for by deviations from the norm of measurable biological (somatic) variables” (Engel, 1977, p. 130). This reductionism, he argued, was dehumanizing, did not do justice to the complex landscape of issues that patients face, and impeded the ability to understand and treat disease. To better account for, prevent, and treat disease would require a model that considers not only the biological but also the “social, psychological, and behavioral dimensions of illness” (Engel, 1977, p. 135).
In some respects, it is difficult to overstate the impact of Engel’s work (Engel, 1977). His initial proposal has accumulated more than 21,000 citations, and the biopsychosocial model is now arguably “the most widely accepted model of health and disease in contemporary medicine” (Maung, 2021, p. 6). It is a fixture of clinical training, and there is an enormous body of empirical work supporting the position that biological, psychological, and social factors all play a role in the development and treatment of disease. Perhaps nowhere has the influence of this model been stronger than in the context of mental-health research and practice, in which few researchers or clinicians today would dispute the notion that factors across levels of analysis play important roles in the development and treatment of psychopathology (Pilgrim, 2002). The biopsychosocial model, it seems, is everywhere (Davies & Roache, 2017).
Yet Engel’s legacy is not unequivocally positive. Critics have argued that the biopsychosocial model is not really a model at all but rather something more akin to a slogan: a call to arms that implores one to look beyond biological factors alone but fails to provide concrete guidance for clinical research or practice (Ghaemi, 2010, 2011; McLaren, 1998). From this perspective, the popularity of the biopsychosocial model is not because it provided a paradigm shift in the understanding of disease but because of its diffuse permissibility: a framework from which researchers of all stripes are free to carry out their research. As noted by Davies and Roache (2017), the biopsychosocial model may be everywhere, but it is also nowhere.
In recent years, considerable efforts have been made to strengthen the biopsychosocial model and lay a path for its future (e.g., Aftab & Nielsen, 2021; Bolton & Gillett, 2019; Davies & Roache, 2017; Maung, 2021). For this special issue on interdisciplinary collaboration and clinical psychology, we aim to make a small contribution to these efforts, arguing that the success of the biopsychosocial model will rely on transdisciplinary collaboration: work that transcends traditional disciplinary boundaries and is unified by its focus on understanding and promoting mental health. Drawing on insights from our multidisciplinary authorship team, we begin by arguing that the biopsychosocial model is a systems model and that as such, the transdisciplinary field of systems science has a great deal to offer mental-health researchers. We then illustrate how systems across domains of analysis affect mental-health phenomena and argue that genuine progress in the understanding of mental disorders will therefore require an integration of work carried out by researchers working across domains of science. Given this need for collaboration across disciplines, we conclude with a discussion of three steps psychologists can take to move toward a transdisciplinary systems science of mental health.
Systems Science and Mental Health
A central criticism of Engel’s proposal is that he focused much more on the limits of the biomedical model than he did on the specifics of the new model he was proposing (Ghaemi, 2010; McLaren, 1998). However, Engel did provide one significant theoretical pillar for the biopsychosocial model, arguing that it “is based on a systems approach” (Engel, 1980, p. 535), specifically, the biologist Ludwig von Bertalanffy’s (2009) general system theory.
The core premise of von Bertalanffy’s (2009) theory was that there is consistency in the structure and dynamics of systems across levels of analysis and across substantive domains. Because of this consistency, the principles governing the behavior of a system in one scientific domain can provide insight into how a system in another scientific domain may operate. Although cursory, Engel’s incorporation of this framework seems increasingly prescient. In the years since Engel’s proposal, general system theory and cybernetics, information theory, chaos theory, network science, and other pioneering ideas of the 20th century have blossomed into the innovative and deeply impactful transdisciplinary field of systems science (Barabási, 2012; Mobus & Kalton, 2014). Moreover, in recent years, the notion that mental disorders emerge from complex systems of interacting components has seen a resurgence of interest (e.g., Borsboom, 2017; Hayes & Andrews, 2020; Nelson et al., 2017; Olthof et al., 2023; Schiepek & Pincus, 2023), and researchers collaborating across ecology, psychiatry, and psychology have used the consistency of system behavior across substantive domains to glean insights into the systems that may underlie mental health (e.g., Lunansky et al., 2021; Scheffer et al., 2024a, 2024b; Van De Leemput et al., 2014). In this section, we draw from these and other insights to illustrate how collaboration with systems-focused researchers across disciplines can advance the understanding of (a) the nature, (b) the development, and (c) the treatment of mental-health problems.
Ecology and the nature of mental disorders
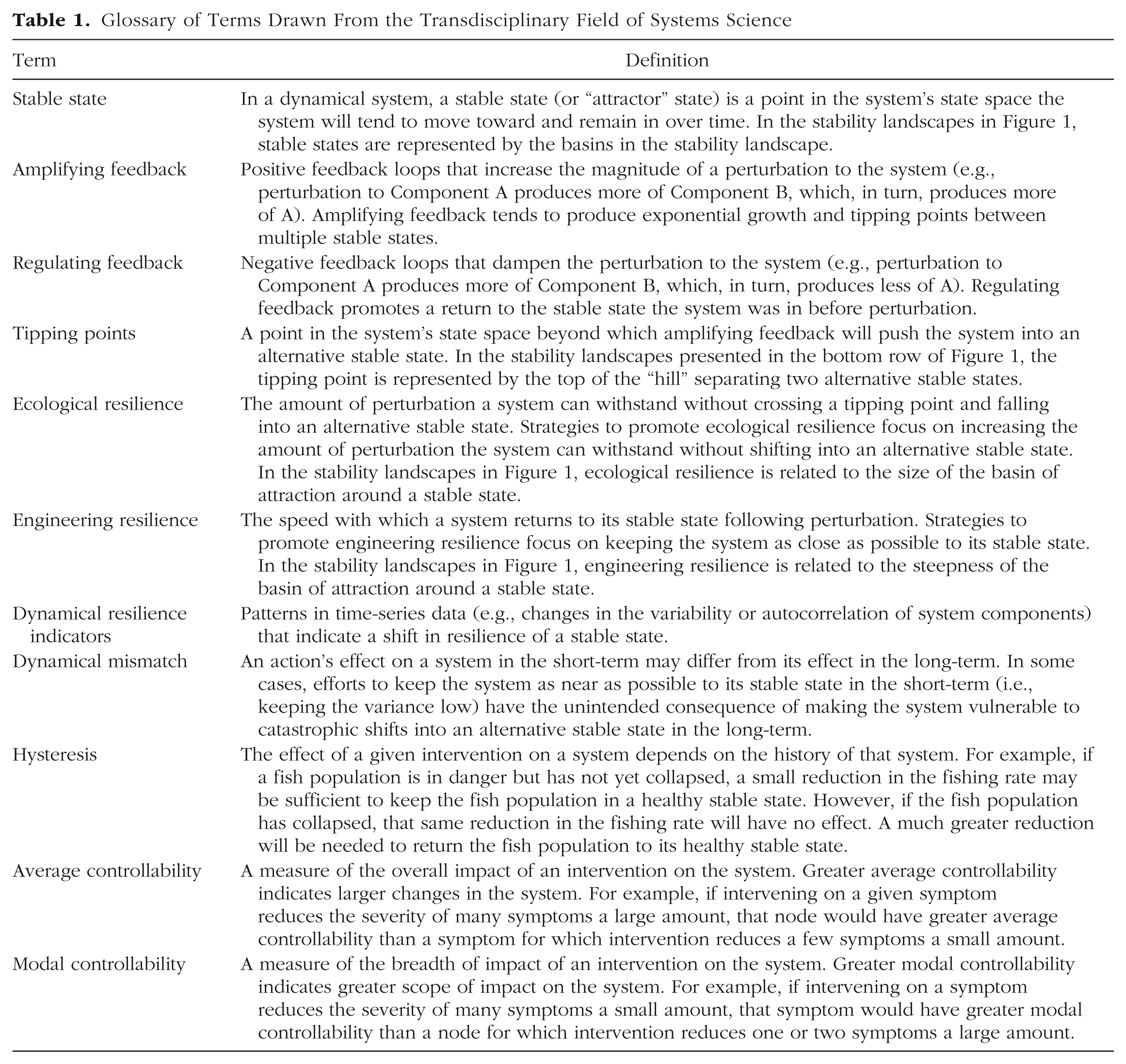
Some of the most valuable contributions to the understanding of how systems operate have come from the study of ecosystems. Ecosystems typically comprise a community of species in a physical environment. To understand these systems, ecologists investigate the interactions among species and their environment and the phenomena that emerge from these interactions. In doing so, ecologists have learned that in some ecosystems, the interactions among system components can produce alternative stable states (or “attractors”): two or more clearly different states that can exist under the same set of external conditions (for a glossary of terms from systems science relevant to mental health, see Table 1). Once an ecosystem has moved into a stable state, it is often difficult to move the system away from that state. A classic example is shallow lakes in which water tends to be either clear (because of water plants that suppress algae) or turbid (i.e., filled with algae and suspended matter; Scheffer & Van Nes, 2007). Once a lake moves into a stable state of high turbidity, it is difficult to shift the lake back into a state in which the water is clear and dominated by water plants. The extent of this difficulty is referred to as the stable state’s resilience. The more resilient the stable state is, the more difficult the shift becomes.
Glossary of Terms Drawn From the Transdisciplinary Field of Systems Science
The surprising insight at the heart of von Bertalanffy’s (2009) general system theory is that a shallow-lake ecosystem can provide considerable insight into the understanding of substantively very distinct phenomena, including mental health (Scheffer et al., 2024b). Just as an ecosystem is the product of complex interactions among species and their environments, the biopsychosocial model posits that mental health is the product of complex interactions among biological, psychological, social, and environmental components. Mental disorder is analogous to the state of turbidity in shallow lakes: a harmful stable state in the dynamical landscape produced by the biopsychosocial system (see Fig. 1). This conceptualization aligns well with Engel’s (1980) reflections on the nature of systems in the biopsychosocial model: “a stable configuration . . . that is maintained not only by the coordination of component parts in some kind of internal dynamic network but also by the characteristics of the larger system of which it is a component” (p. 537). Moreover, this conceptualization sets the stage to learn from the insights ecologists have gained into how these stable states operate. We focus on three such insights here.
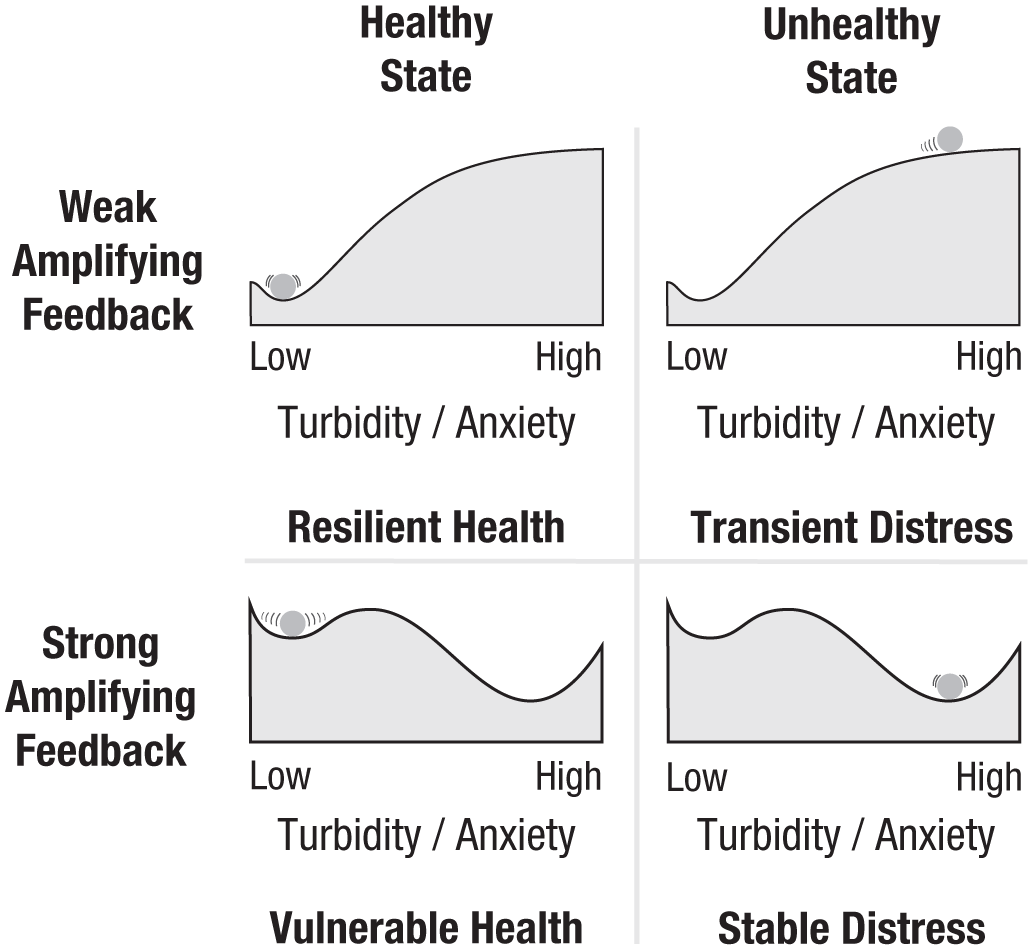
Stability landscapes to depict the dynamics that emerge from interactions among components within a system (Meyer, 2016). The lateral position of a “ball” on the landscape represents the system’s current state (e.g., a state of turbidity in a shallow-lake ecosystem or of anxiety in a system underlying one’s mental health). Movement along the landscape occurs under negative gradient flow: That is, a ball placed on a slope will roll downhill. In cases in which slopes are steep, the system changes quickly. In cases in which the slope is flat, the system will not change. The topography of the landscape thus represents how the state of the system will evolve over time from its current position. When amplifying feedback in the system is weak, the system has a single stable state, in this case, a state characterized by health (e.g., low turbidity or low anxiety). If perturbed, the system will quickly recover to its stable healthy state. However, when amplifying feedback is strong, an alternative stable state emerges. Here, the system is slow to recover from even minor perturbations, and significant perturbations are sufficient to push the system past a tipping point (i.e., the peak of the landscapes depicted in the bottom) and into a self-maintaining state of stable distress.
First, amplifying feedback loops are critical to formation of alternative stable states (see Table 1). For instance, small increases in turbidity in a clear shallow lake dominated by water plants can lead to increasing algal growth and, in turn, a loss of water plants and even more turbidity, thereby initiating a vicious cycle that pushes the system away from an intermediary state of semiturbidity and into a stable state of high turbidity (Van Nes et al., 2016). Because of these self-propelling processes, systems may have tipping points (see Table 1 and Fig. 1, bottom). Beyond these tipping points, amplifying feedback among system components will drive the system into a new stable state. Accordingly, if mental disorders are indeed harmful stable states, one should expect that amplifying feedback loops will be critical to the understanding of psychopathology. There are many examples of amplifying feedback loops already in the mental-health literature, such as between mood and physical activity, in which lower mood reduces the likelihood of engaging in physical activity and reductions in physical activity worsen mood (Giurgiu et al., 2020; Pemberton & Fuller Tyszkiewicz, 2016; Pham et al., 2023; Roman et al., 2023); or between autonomic arousal and perceived threat, in which increases in somatic sensations of arousal (e.g., heart rate) elicit perceived threat (e.g., the thought that one is having a heart attack), which, in turn, elicits more autonomic arousal, culminating in a panic attack (Clark, 1986). However, if one is to understand mental disorders from a systems framework, it will be critical to further investigate these and the many other feedback loops likely to drive the emergence of stable states of psychopathology.
Second, resilience is dynamic. In fact, the resilience of a stable state may rise or fall because of changing conditions even as the state of the system remains the same (Scheffer, 2020). In the domain of mental health, this means that a person’s vulnerability to a given mental disorder—or a person’s potential for recovery—may shift even as the person’s own internal experiences and behaviors may appear largely unchanged. The dynamic nature of resilience provides an opportunity to reorient thinking about prevention and treatment, placing an emphasis not only on changes in the state of the system (e.g., reducing symptom severity) but also on destabilizing the resilience of the harmful stable state and strengthening the resilience of a healthy stable state (Hayes et al., 2015; Olthof et al., 2023). Dynamical resilience indicators—a collection of statistics derived from time-series data that indicate a potential shift in the resilience of a stable state—provide tools by which one might identify changes in the resilience of a stable state of mental health or mental disorder (Scheffer et al., 2018, 2024a; Van De Leemput et al., 2014). Although the barriers to their practical application in the context of mental-health research are likely to be considerable (Dablander et al., 2023; Helmich et al., 2024), these tools nonetheless hold the promise of providing deeper insight into a person’s mental health by shifting focus from the immediate presence of symptoms to the resilience of the person’s healthy and harmful stable states.
Finally, systems exhibit a phenomenon known as “hysteresis”: Once a system has tipped to a new state, it is often much more difficult to shift the system back to its earlier state than it would have been to prevent that shift in the first place (see Table 1). It is therefore much more efficient to prevent a shift into a harmful stable state than it is to facilitate the recovery from a harmful stable state. In the domain of mental health, the concept of hysteresis sheds light on the dynamics underlying the familiar adage that “an ounce of prevention is worth a pound of cure” and argues for the importance of systems-oriented prevention strategies in the effort to reduce the global burden of mental illness (Fried et al., 2023; Lich et al., 2013).
Engineering and the development of mental disorders
The concept of stable states has implications for understanding not only the nature of mental disorders but also how mental disorders develop. As noted, the amount of perturbation a system can tolerate without shifting into an alternative stable state provides an index of that state’s resilience. This index has been referred to as “ecological resilience” because of the focus in ecology on understanding catastrophic shifts from one state to another (e.g., from savannah to desert; see Table 1). Another index of resilience is the speed by which a system returns to its stable state following perturbation, an index termed “engineering resilience” because engineered systems are often designed to remain close to a precise stable state (Holling, 1996; see Table 1).
Although engineering and ecological resilience are often highly correlated, efforts to promote these distinct types of resilience can be at odds with one another. Steps taken to promote engineering resilience are often successful in keeping a system close to the desired state but at the long-term cost of diminishing the system’s ecological resilience, leaving it vulnerable to catastrophic shifts into an alternative stable state (Holling, 1996). For example, fish hatcheries produce more stable and predictable fish populations (i.e., greater engineering resilience), but that stability encourages commercial fishing, depletes natural stocks, and makes the system dependent on a limited number of hatcheries, rendering the system more vulnerable to catastrophic shifts in the fish population if those hatcheries fail (i.e., reduced ecological resilience; Holling, 1996). Analogously, in anxiety disorders, avoidance and escape behavior can be understood as an effort to promote the system’s engineering resilience, keeping the system as near as possible to its desired equilibrium (i.e., a state without fear). Although often effective in promoting engineering resilience in that moment (e.g., preventing or reducing fear), escape and avoidance behaviors come at considerable cost to ecological resilience: shifting the stability landscape and leaving individuals vulnerable to falling into stable states of elevated fear and anxiety over time (for an illustration, see Robinaugh et al., 2024).
The unintended consequences of short-term engineering-resilience strategies provide an important lesson for understanding how mental disorders develop: Shifts into a harmful stable state are sometimes attributable to a dynamical mismatch in which actions with short-term benefits have unintended long-term costs (Mobus & Kalton, 2014, p. 25). In the short-term, escape and avoidance behavior prevent or reduce fear. However, in the long-term, these behaviors have the unintended cost of heightening vulnerability to persistent fear and anxiety. Another salient example of this dynamical mismatch in the domain of mental health is substance use disorder, in which substances sate cravings or regulate aversive emotions in the short-term but do so at considerable long-term cost, leading individuals to fall into a stable state of persistent use, craving, and aversive emotion. As both of these examples illustrate, regulating feedback loops may play an especially important role in these dynamical mismatches and therefore, in the development of psychopathology (see Table 1). For cases in which amplifying feedback loops are necessary for the emergence of alternative stable states, regulating feedback loops that are effective in the short-term (e.g., reducing cravings or anxiety) may play a critical role in creating or strengthening amplifying feedback loops that play out over longer periods of time, thereby heightening vulnerability to mental disorder in the long-term. This possibility of dynamical mismatch illustrates one reason why understanding processes and dynamics at distinct timescales is a core principle of systems science (Mobus & Kalton, 2014) and is therefore an area in need of much greater focus if the mental-health field is to understand the processes that give rise to persistent mental-health challenges.
Control theory and the treatment of mental disorders
One of the most challenging aspects of studying complex systems is that their behavior is exceedingly difficult to anticipate using intuition alone. In dynamical systems, changes in one component can have causal consequences that compound over time across the system, often in unexpected ways. In a treatment context, this complexity presents a considerable challenge. For example, if an intervention that targets fatigue in depressed individuals (e.g., a psychostimulant) also has the side effect of increasing anxiety, it may have iatrogenic impacts on the rest of the system, including, ironically, exacerbating the fatigue that was the original point of intervention. Because of this, it is typically far from trivial to determine precisely how one should intervene to affect change in a complex system. Fortunately, there is an entire discipline devoted to precisely this challenge, known as “control theory.”
Control theory can be traced back to the development of centrifugal regulators for steam engines in the 18th century, carefully engineered systems that use regulating feedback loops to control the engine’s speed, keeping that speed as close as possible to a desired stable state. Modern control theory underpins vast swaths of the technology people use every day, from the operation of thermostats to controlling planes in flight. To achieve these aims, control theorists start with a representation of the system of interest: specifically, a mathematical description, such as a formal theory of the causal mechanisms at play in the system, or a statistical model estimated from data. With this representation, control theory then allows one to quantify the impacts of an intervention on the system as a whole and on specific subcomponents.
One set of tools that may be of particular interest in the domain of mental health is measures of controllability centrality, which allow researchers to precisely quantify the magnitude and scope of an intervention’s impact (Henry et al., 2022). Average controllability directly measures the overall impact on the system while also accounting for the likelihood that reductions in some components of the system will lead to reductions in other components over time (see Table 1). Higher average controllability of an intervention indicates larger changes to the system. By contrast, modal controllability focuses on the scope of an intervention: for example, the number of components affected rather than the magnitude of those effects (see Table 1). Here, higher controllability corresponds to greater reach of the intervention. For example, a treatment that only mildly reduces the severity of all symptoms will have higher modal controllability than a treatment that greatly reduces the severity of a small set of symptoms. Together, these measures can therefore inform understanding of how impactful it would be to intervene on a specific system component (see Fig. 2).
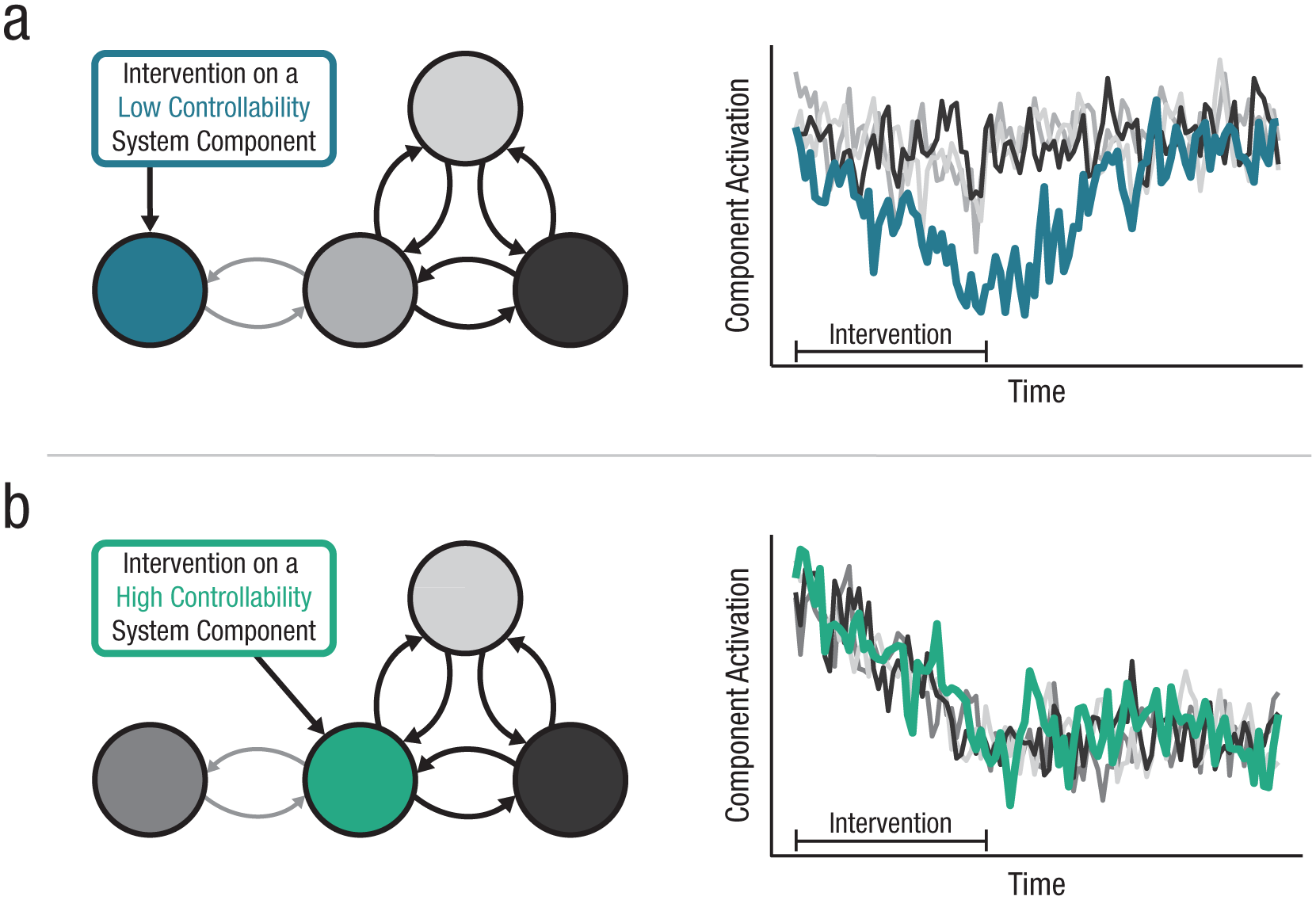
An illustration of controllability measures. (a) An imagined intervention on a system component with low average and modal controllability. Although the initial intervention lowers the severity of that component (e.g., a symptom), it has minimal impact on the broader system. Moreover, once the intervention concludes, the targeted component returns to a state of elevated severity because of the effects of the broader system. (b) An intervention on a system component with high average and modal controllability. Here, the impact of intervening on this one component has an impact throughout the system, causing a sustained reduction in the severity of all symptoms. Importantly, although controllability measures are illustrated here using relatively simple interventions on a single node, control theory can be more fruitfully applied to address significantly more complicated interventions, including the effect of targeting multiple nodes or the appropriate sequencing of distinct interventions (for an illustration, see Henry et al., 2022).
We see at least two core use cases for control theory in the context of mental health. First, control theory can be used for treatment discovery. As depicted in Figure 2, controllability centrality can be understood as a measure of component importance, and thereby, a measure that allows one to determine which component (e.g., symptoms) would in principle be the most impactful on which to intervene. With this insight, one can consider whether there are new interventions that would allow better targeting these highly impactful components and thereby improve gains made during treatment. Second, control theory can be used for treatment planning. In this case, control-theory metrics, such as controllability centrality or model predictive control (Schwenzer et al., 2021), can be used to estimate the impact of different existing interventions on the system, thereby allowing one to determine what treatment may work best for a given individual. Moreover, these methods can help in evaluating treatment plans that include distinct interventions delivered either simultaneously or serially (e.g., considering different sequences of modules in the Unified Protocol or determining whether to augment prolonged exposure therapy for posttraumatic stress disorder with interoceptive exposures or dialectical-behavior therapy) and dynamic interventions that target system elements based on ongoing changes (e.g., a just-in-time intervention, in which control-theory methods can respond dynamically to a shift in mood by identifying the most effective means of intervening among a menu of potential interventions). In these ways, control theory has the potential to identify the optimal timing and sequencing of intervention components for a given individual and the most effective intervention given the current state of the system.
As these use cases make clear, greater collaboration with control theorists holds enormous promise for mental-health research and practice, but considerable work remains to be done to realize this promise. One core challenge is that the understanding of psychological interventions can only be as strong as the understanding of the systems on which researchers and practitioners are intervening, including the relevant causal components of the system, the structure and strength of their interactions, and the timescales on which they interact. For most mental disorders, this information remains largely unknown. Accordingly, it will be critical that the mental-health field advance its understanding of the systems underlying mental-health problems if control theory is to be effectively used to make progress in the understanding of psychological treatments.
Conclusion
Engel argued that the biopsychosocial model should root itself in general system theory: a framework whose premise is that there is consistency in the principles that govern system behavior across substantive domains. In the decades since Engel’s proposal, general system theory helped stimulate the flourishing transdisciplinary field of systems science. As reviewed here, the lessons from this work have already begun to provide insight into the understanding of the nature of mental disorders, how they arise, and how they might be treated. To grapple with the enormous complexity of the systems underlying mental health, psychologists must further participate in this transdisciplinary community, collaborating across disciplines and drawing on the insights and tools that have been developed in the field of systems science.
Mental Health as a Transdisciplinary Phenomenon
The name “biopsychosocial model” implies three broad domains of analysis and is commonly interpreted simply to mean that biological, psychological, and social factors may affect mental health. However, Engel’s vision was broader than just these three levels of analysis, and his focus was not on individual factors within these levels but rather, on a “hierarchy of systems,” ranging from subatomic particles to the biosphere. Engel organized his hierarchy not by the importance of a given level of analysis for understanding disease but by the nested structure of systems operating across levels of analysis: with systems at one level (e.g., people) embedded within the systems of another (e.g., families), which themselves are embedded in other systems (e.g., communities). In this section, we discuss psychological, biological, social, and environmental systems that bear on mental-health phenomena and how systems science can provide guidance for integrating insights from across these levels of analysis. In doing so, we draw especially on the example of one symptom (fatigue) of one disorder (major depressive disorder) to illustrate the transdisciplinary and systemic nature of mental health.
Psychological systems
Engel (1980) argued that researchers aiming to study a phenomenon must choose a systems level at which to begin their effort and that any effort to understand health and disorder should begin at the level of the person: particularly, the person’s experiences and behavior. Consistent with this position, in recent years, there has been a renewed and growing interest in conceptualizing mental disorders as systems of interacting thoughts, emotions, behaviors, and other psychological components. Interest in this approach grew substantially following work in psychometrics (Borsboom, 2008) and the philosophy of psychiatry (Kendler et al., 2011) that reconceptualized the relationship between symptom and disorder as one of mereology rather than one of measurement (Cramer et al., 2010). Symptoms do not measure mental disorders, this position holds; they constitute them.
In this framework, commonly referred to as the “network approach” to psychopathology, symptoms take on new importance. Rather than merely indicating the presence of an underlying disease entity, symptoms are agents in a causal system. Consider fatigue. Rather than merely serving as a passive indicator of major depressive disorder, there is good reason to think that fatigue may cause other symptoms to arise. For example, fatigue may cause an individual to have difficulty concentrating, which may then interfere with productivity, which, in turn, may lead to job-related worry when laying down in bed, sleep problems, and consequently, yet more fatigue the next day (fatigue → concentration problems → worry → sleep problems → fatigue). In this way, the interactions among symptoms can create the kinds of amplifying feedback loops that are necessary to produce the harmful stable state that, we have argued, characterizes psychopathology.
Motivated by this conceptual framework, numerous exploratory studies have used psychometric-network analyses to gain insight into the structure of the relationships among symptoms of mental disorders, including many studies focused on depression (Malgaroli et al., 2021). In these studies, fatigue often exhibits strong conditional dependence relationships with other symptoms of depression, suggesting that fatigue may play an important role in this system. This possibility is supported by work outside of the psychometric-network literature. For example, fatigue is among the symptoms most commonly reported by individuals with depression (Buchwald & Rudick-Davis, 1993) and has consistently been identified as a prodromal symptom; individuals reporting persistent unexplained fatigue are as much as 28 times more likely to develop major depressive disorder (Addington et al., 2001). Likewise, residual fatigue is a strong predictor of relapse following treatment for depression (Fava et al., 2014). Together, these studies suggest that to understand depression, it will be critical to understand fatigue and how it relates to and potentially affects other symptoms.
In one especially insightful investigation of the depression-symptom network, Cramer et al. (2016) not only estimated the structure of relationships among symptoms but also investigated the system-level behavior that would follow if that network was assumed to represent the structure of a causal system. By simulating from this empirically derived model, they demonstrated that a system of causally interacting symptoms was capable of producing many of the core phenomena observed in ecological systems described in the previous section. To illustrate, we present a similar simulation in Figure 3. 1 For this simulation, we use an Ising model—a model adopted from statistical physics—to represent the network of relationships among depression symptoms (Haslbeck et al., 2021). In this network, symptoms are represented by nodes (i.e., the circles in the network), and the relationships among them are represented by edges or links (i.e., the lines in the network). Recently, Cui and colleagues (2023) developed procedures for estimating stability landscapes from the Ising model that are akin to the landscapes introduced in Figure 1, providing us with an opportunity to examine the dynamics that can follow from different symptom networks (for extended discussions, see Cui et al., 2023; Hoekstra et al., 2024). Here, we used these stability landscapes to examine how the behavior of the system differs as a function of the system’s connectivity.
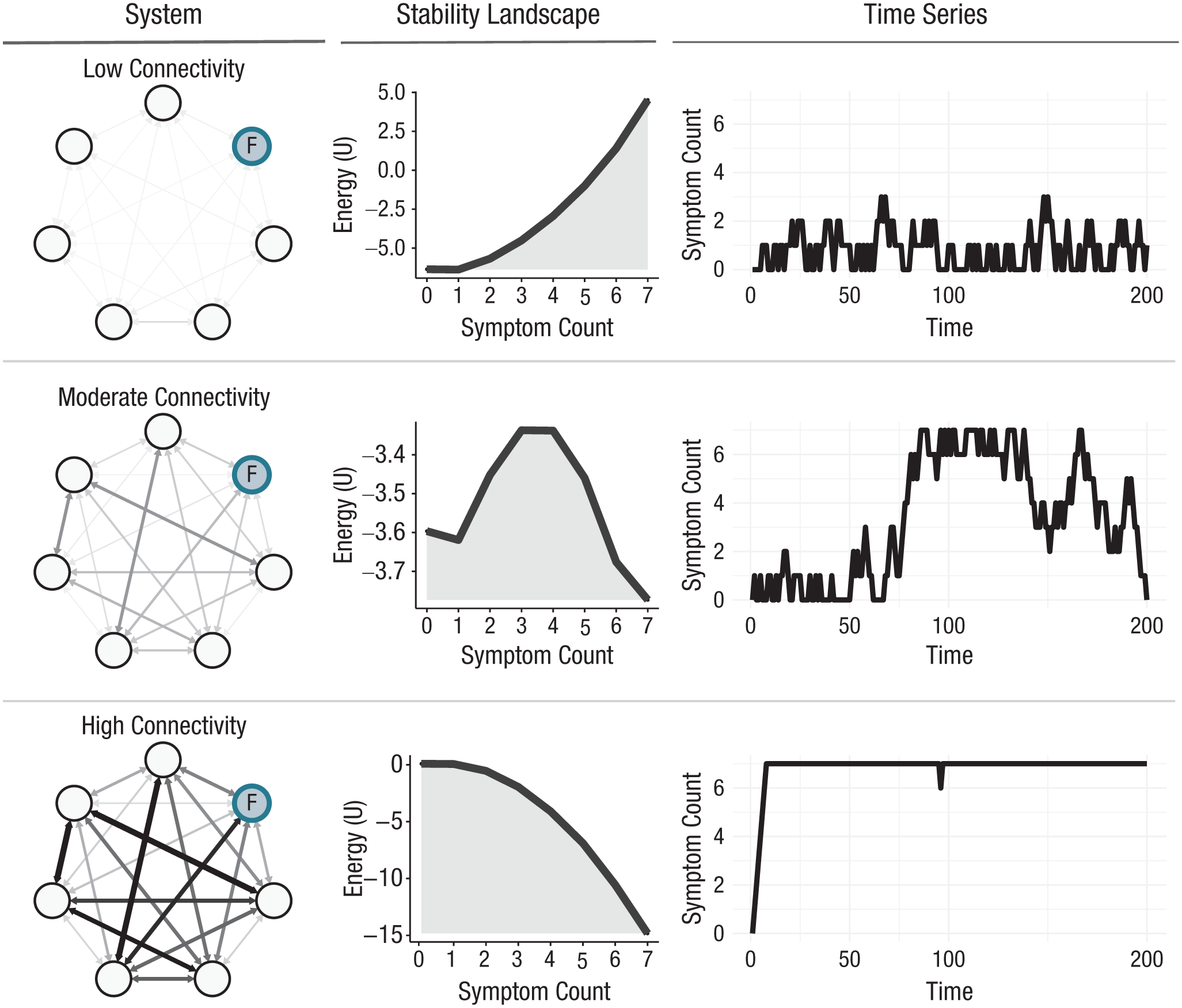
An illustration of the dynamics that can follow from a psychological system of interacting symptoms. In the left column, we use an Ising model in the {0,1} domain to represent a system of interacting symptoms of depression (for further details, see the Supplemental Material available online). Symptoms are represented by nodes in this model. The symptom “fatigue” is labeled “F.” The strength of association between symptoms is represented by the lines—or “edges”—between them. Thicker lines represent stronger associations. The central column depicts the stability landscapes that follow from these systems. The right column depicts time-series data simulated from these models for overall depression-symptom severity. The stability landscapes and, in turn, the behavior of the system depend heavily on the strength of associations among symptoms. If these mutually reinforcing associations are sufficiently high, the system will have a single stable state characterized by persistently elevated symptoms of depression, including persistent fatigue. Code used to produce this figure is available at https://osf.io/yp7zc/files/tvbue.
As depicted in Figure 3, when the strength of associations among symptoms is low, the system has a single healthy stable state characterized by an absence of symptoms; if symptoms do arise, they are transient and isolated. When the association among symptoms is moderate, there are two stable states, and the system fluctuates between states of low and high symptom severity. When symptoms are strongly interrelated, the system has a single harmful stable state of elevated depression symptoms. These simulations thus illustrate how a system of mutually reinforcing symptoms could give rise to a self-sustaining stable state of depression, including the experience of persistent fatigue.
The network approach to psychopathology has provided valuable initial insight into how disorders such as depression may arise from a system of interacting symptoms and highlighted the importance of the psychological level of analysis to the understanding of mental disorders. In addition, this framework provides insight into how factors across levels of analysis may interact with these psychological factors to give rise to psychopathology. From the perspective of network theory, biological, social, and environmental factors may interact with a symptom network in at least three ways (Borsboom, 2017).
First, systems at other levels of analysis may constitute features of the symptom network. For example, the symptom depressed mood represents the persistent experience of intense negative affect, emotional experiences that themselves can be understood as emergent features of a system with biological and psychological components. The stable behavior of this affective system may thus constitute the symptom depressed mood in the symptom network. Likewise, an amplifying feedback loop between autonomic arousal and perceived threat may constitute the symptom panic attack in the panic disorder symptom network. We suspect this form of integration with the symptom network may be especially relevant for incorporating factors that operate on a faster timescale than the weeks- or months-long timescale typical of symptoms such that the components of the symptom network can be understood as the stable behavior of a more rapidly operating system at another level of analysis.
Second, factors across different levels of analysis may directly interact with symptoms, thereby expanding the network to include biological, social, and environmental factors. Adopting this position, researchers have recently incorporated variables from across levels of analysis into psychometric-network analyses involving the statistical relationships among symptoms (Blanken et al., 2021). For example, a recent investigation of brain structural correlates and depression symptoms identified many robust cross-level biological–psychological associations, links that were obscured when investigating the associations between brain structural correlates and overall depression severity (Freichel et al., 2024). This cross-level interaction may be especially important for capturing biological, social, and environmental factors that operate on the same timescale as symptoms and form feedback relationships with factors at other levels of analysis (e.g., persistent fatigue deteriorating physical strength and, in turn, exacerbating fatigue).
Third, external factors may constrain or amplify features of the network, including the relationships among symptoms (therefore controlling how easily a given symptom affects another) or the symptom thresholds (i.e., the propensity of a symptom to be activated). For example, the availability of financial resources may influence how readily difficulty concentrating elicits worry about work performance (and, in turn, difficulty sleeping and ultimately, more fatigue). In other words, financial resources may play an important role in determining whether the amplifying feedback loop involving fatigue and worry is sufficiently strong that it generates an alternative stable state. Likewise, living in an environment with high light or noise pollution may influence the threshold at which sleep difficulty arises, rendering it susceptible to emerging even in the absence of other symptoms. Although less discussed in the network literature than the relationships among symptoms, thresholds have a large effect on the system’s stability landscape and thus the vulnerability or resilience to harmful stable states of distress (Hoekstra et al., 2024). We suspect that this form of integration with the psychological network in which factors at other levels of analysis constrain or amplify features of the symptom network may be especially relevant for incorporating factors that are static on the timescale on which the psychological-network dynamics play out, such as stable genetic, neurobiological, or environmental factors.
Overall, the network theory of psychopathology provides one framework through which researchers may go beyond merely noting the importance of biological, psychological, and social factors to tackle the challenge of determining how factors across these levels of analysis interact with the symptom network and thereby contribute to the development and persistence of mental-health challenges. We explore each of these possibilities in more detail below as we consider the contributions of biological, social, and environmental systems to mental health.
Biological systems
Depression is not the only health condition in which fatigue plays an important role. Fatigue is one of the most prevalent and debilitating symptoms across neurological, psychiatric, and other chronic illnesses and is a key focus of research in numerous health-science domains (Raizen et al., 2023). One such domain is physiology. Beginning with the pioneering work of Angelo Mosso on muscular fatigue in the late 1800s, physiologists have spent more than a century studying fatigue. This work has provided considerable insight into the physiological and neurobiological underpinnings of fatigue; research has demonstrated that both central (i.e., neurobiological, spinal, and supraspinal) and peripheral (i.e., muscular) mechanisms can lead to and compensate for fatigue (Barry & Enoka, 2007; Enoka & Duchateau, 2008; Gandevia, 2001). However, far from being reducible to these biological mechanisms, physiologists have found that fatigue itself turns out to be enormously complex.
One of the earliest insights from Mosso’s (1904) seminal work was that fatigue is not one thing but rather a collection of things that commonly hang together. In recent years, researchers have placed renewed emphasis on characterizing the distinct behavioral components of fatigue (Casamento-Moran et al., 2023; Kluger et al., 2013). For example, fatigue may include a subjective feeling of tiredness, a perception of effort expended, a reduced willingness to exert effort, and altered motor performance in an assigned task (Casamento-Moran et al., 2025). In most day-to-day activities, exerting sufficient effort may elicit each of these components of fatigue, and their tendency to arise together is why it is easy to think of them as a cohesive experience. However, in experimental paradigms, these factors often exhibit surprisingly low correlations with one another (Kluger et al., 2013; Raizen et al., 2023), and there is some evidence that these experiences can be experimentally dissociated (Casamento-Moran et al., 2025).
To better understand how fatigue arises, researchers have increasingly adopted a systems framework, positing that fatigue emerges from an allostatic system aimed at anticipating the demands of the environment and proactively maintaining a state of physiological equilibrium, including maintenance of the body’s energetic resources (Noakes et al., 2005; Shaffer et al., 2022; Stephan et al., 2016). For a diagram depicting such a system, see Figure 4. In this system, an individual’s generative model of the world and of the individual’s internal state is used for both perceptual inference (producing a perception of the current state the individual is in) and for anticipating the state the individual’s bodily system will need to be in to meet the upcoming demands of the individual’s internal and external environments. For example, if completing an experimental task in which the individual is asked to squeeze a force sensor, an individual’s generative model would produce both a perception of the individual’s current state (e.g., an absence of neuromuscular activity) and an anticipation of the state needed to meet current demands (e.g., sufficient neuromuscular activity to apply appropriate force). If there is a discrepancy between the individual’s current state and the state needed to meet these demands, a decision must be made about how to reduce this discrepancy (e.g., a decision to exert effort in the experimental task), which, in turn, may entail execution of a specific bodily activity (e.g., neuromuscular activity) that is then translated into an action in the environment (e.g., compressing a force sensor). In other words, the difference between one’s current state and one’s anticipated needs is used to determine which action the body should take to resolve this discrepancy, a regulatory feedback loop akin to those that lay the foundation for the control theory, as described in the previous section, but with an emphasis on anticipating rather than only responding to potential discrepancies between one’s current state and the state needed to support one’s bodily needs.
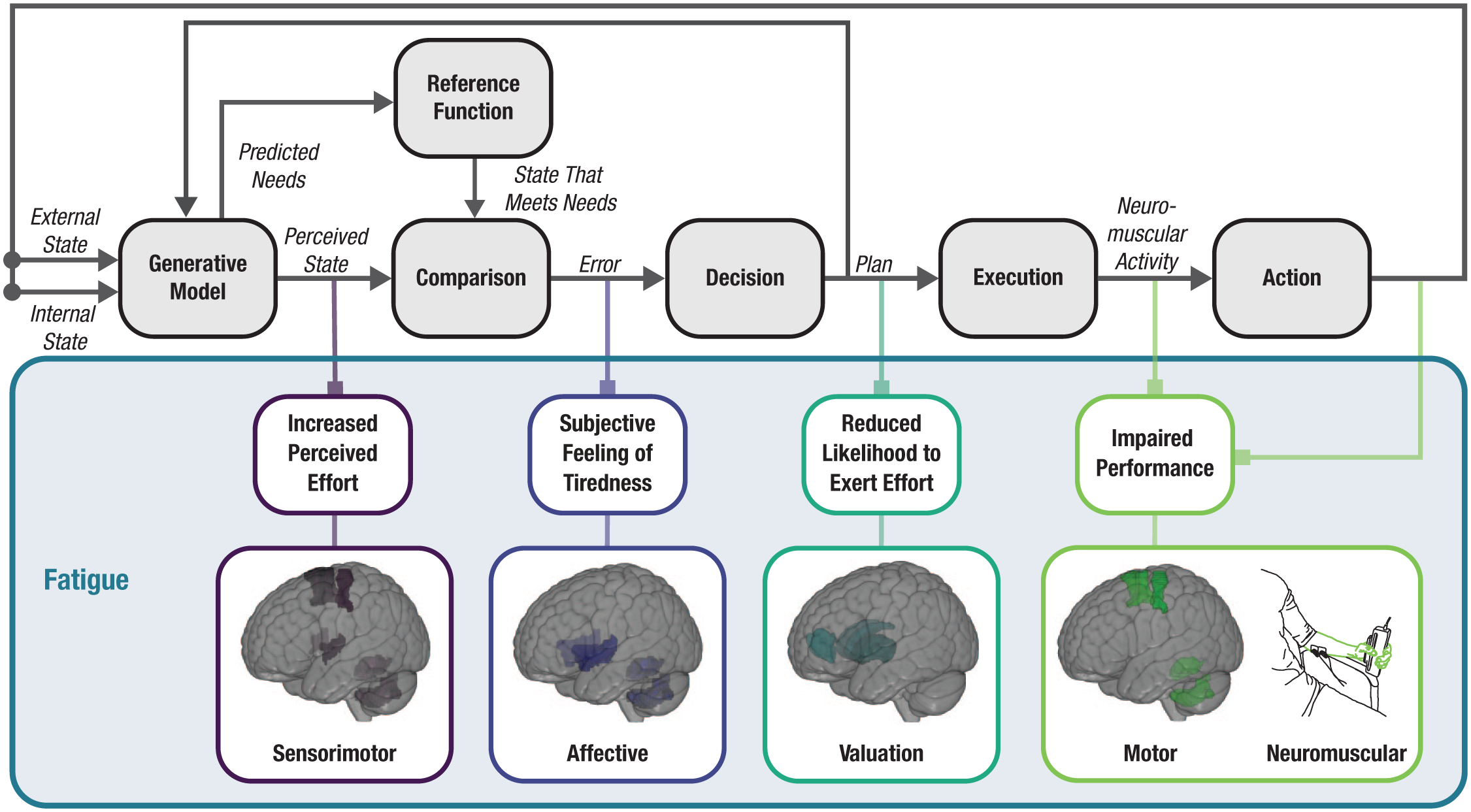
A causal diagram positing a toy allostatic system at play during an experimental task in which participants are asked to repeatedly squeeze a force sensor. This system gives rise to distinct features of fatigue, including increased perceived effort, a subjective feeling of tiredness, reduced likelihood to exert effort, and impaired performance. In this model, subjective tiredness, the felt component of fatigue, emerges when there is a discrepancy between one’s current internal state and the state needed to maintain bodily integrity. Subjective tiredness is thus an alarm that signals the need to refrain from any behavior that would further deplete the system’s resources.
In this toy allostatic system (Fig. 4), we show how different components of fatigue may arise together under specific task demands. As our imagined participant repeatedly squeezes the force sensor, the participant’s perception of expended effort increases. As energetic resources are expended, a discrepancy grows between the participant’s current state and the state needed to maintain adequate energetic resources, producing a subjective sense of tiredness. Furthermore, in anticipation of the energetic depletion that would occur with continued exertion, there is a reduction in the likelihood of exerting further effort. If effort continues and the system exhausts compensatory resources, neuromuscular activity will be insufficient for the task, and performance will be increasingly impaired even when deciding to exert effort. From this perspective, a subjective feeling of tiredness in the experimental task is a signal: a subjective experience that arises from the discrepancy between a feature of one’s internal biological state and the state needed to maintain bodily integrity, flagging the need for rest and recovery before the muscle itself begins to fail.
For depression researchers, this systems-focused work on the physiology of fatigue has several implications. First, the systemic and multidimensional nature of fatigue suggests it will be valuable to investigate which components of fatigue are most implicated in depression. Such findings would shed insight into the range of component- and system-level processes that may lead to fatigue in individuals with depression, the biological correlates of such processes, and how clinicians might intervene to reduce fatigue.
Second, as depicted in Figure 4, a range of neurobiological regions is likely to be at play in the experience of fatigue, including sensorimotor regions, affective regions, and regions implicated in valuation and decision-making. Because the processes supported by these regions are interconnected components of a system, dysfunction in any one area may have system-wide effects, and any system-level behavior (e.g., persistent fatigue) may arise from a variety of component-level dysfunctions. This equifinality is a general principle of systems and suggests that fatigue in depression may not have a consistent pattern of neurobiological correlates across all individuals (e.g., impairments in performance may arise from sensitivity to perceptions of fatigue in one individual but altered valuation of effort in another). Together with this equifinality, degeneracy in neurobiological systems (i.e., the fact that structurally different neural regions or circuits can support the same process and that these regions or circuits may differ across individuals) and the observation that systems may behave maladaptively even in the absence of component-level dysfunction (Robinaugh et al., 2024) all argue for considerable care when investigating the neurobiological underpinnings of fatigue in depression.
Third, the allostatic system posited to give rise to fatigue is a regulatory feedback loop constantly engaged in an effort to keep the body in a desired state of equilibrium. The presence of such regulatory feedback is critical for survival but also flags the possibility of the kind of dynamical mismatch sometimes seen in systems science in which short-term efforts to regulate the system have unintended long-term consequences (see the Engineering and the Development of Mental Disorders section above). Recently, several researchers have posited that the allostatic system responsible for energy regulation may play a central role in depression (Barrett et al. 2016; Shaffer et al., 2022; Stephan et al., 2016). The lessons from systems science would suggest that if this is the case, it may be because efforts that effectively regulate energy stores in the short-term are producing unintended long-term consequences for mood, fatigue, and the rest of the depression syndrome.
Finally, the allostatic framework underscores that subjective fatigue is a signal: an alert that there is a discrepancy between a system’s current state and desired state. For depression researchers, it will then be important to understand the nature of this signal (e.g., whether the discrepancy is emerging from a misinterpretation of the current state or from a genuine depletion of internal resources) and the factors driving the emergence of this signal, potentially including both social and environmental factors.
Social systems
In his biopsychosocial model, Engel made clear that a systems-level approach to mental health must encompass not only the constellation of processes occurring within the individual but also the broader external factors that drive and constrain those processes. Among these external influences, social networks are especially impactful. From the moment people are born, they are embedded in reciprocal social relationships that shape the way they think, feel, and behave (Wheatley et al., 2024). Perhaps not surprisingly then, individuals’ mental health is intricately tied to their social network, including how central they are within that network, how many connections they have, and even the emotional states of the people around them (Rosenquist et al., 2011). Indeed, the quality and accessibility of support within social networks—whether through family, friends, or community—play a crucial role in mental health throughout the life span. Strong and supportive ties within one’s social network promote resilience, help individuals cope more effectively with stress and emotional challenges, and are associated with neural responses to external stimuli that are more similar to one’s peers, which helps individuals remain attuned to the broader community (Baek et al., 2022).
The protective effects of social support extend beyond providing material assistance. Expressions of warmth, understanding, and validation foster a sense of belonging, security, and resource availability (Thoits, 2011). For example, health-care providers’ level of empathy predicts the efficacy of medical treatments they provide (Hojat et al., 2011; Mercer et al., 2012). Patients who report feeling heard and understood by their physician are more likely to engage in shared decision-making and have higher quality of life (Gramling et al., 2022). Even the placebo effects of medicine can be transmitted socially: The same placebo treatment is more efficacious if provided by someone who believes in its efficacy than someone who does not (Chen et al., 2019). When individuals feel genuinely cared for, their mental and emotional states improve, which can significantly reduce the risk of depression (Kahlon et al., 2021). Collectively, this research strongly supports Engel’s position that the clinical outcomes of an individual are not determined solely by that individual or the care the individual receives but also by the interpersonal context through which that care is delivered.
Expressions of care include the vital role of touch in regulating stress. Recent discoveries surrounding c-tactile fibers—a type of nerve fiber found in hair-covered skin—show how gentle stroking can activate pathways directly linked to emotional well-being. These fibers stimulate the release of oxytocin, a hormone associated with feelings of trust, safety, and bonding (Walker & McGlone, 2013). Oxytocin, in turn, down-regulates the hypothalamic-pituitary-adrenal axis, reducing cortisol levels and mitigating stress (Morrison, 2016). This physiological response to touch has profound implications for relationships, particularly in parent-child bonding, in which gentle touch and nurturing reinforce emotional security and resilience in children with consequences that stretch far into adulthood (Shaw et al., 2004). This growing neurobiological evidence that touch is central to psychological well-being powerfully illustrates the deep interactions among the social, psychological, and biological systems that affect mental health and has clear implications for a world in which interpersonal touch is often discouraged (e.g., in schools and hospitals) or absent altogether (e.g., in the proliferation of virtual environments).
Social connection and social touch have enormous implications for understanding fatigue and depression. Although the allostatic system depicted in Figure 4 is represented as operating exclusively within an individual, there is substantial evidence that others in one’s social environments play a critical role in this system (Atzil et al., 2018; Burleson & Quigley, 2021). Indeed, during infancy, humans are fully dependent on others to meet their physiological needs, and throughout much of people’s early lives, caregivers are active features of the allostatic feedback loop, anticipating needs and responding to calls of distress by satiating hunger, regulating temperature, and supporting the regulation of bodies in countless other ways (Atzil & Barrett, 2017; Zoltowski et al., 2022). As people age, social touch and social communication continue to signal the availability of resources needed to meet allostatic needs (Fotopoulou et al., 2022), and people learn social norms that guide their effort expenditure when working toward common goals in group settings (Karau & Williams, 1993), allowing people to cooperatively meet the enormous metabolic demands of their bodily systems.
The literature on social allostasis makes clear that the effective regulation of one’s physiological needs is intimately bound up with the social systems in which one is embedded. Perhaps not surprisingly then, disruption within these social systems presents a considerable challenge to one’s well-being. Social relationships that are unsupportive and conflict-prone are strongly associated with depressive symptoms, especially in adolescents (Sheeber et al., 2007). Even in the absence of outright conflict, simply bearing the responsibility for others’ well-being—as seen in caregiving roles—can divert vital internal resources. When external support is perceived to be unavailable (e.g., through an absence of social touch or communication) or cannot be trusted, individuals are left with no choice but to rely solely on their internal reserves. This ongoing self-reliance risks depleting these resources, potentially leading to the subjective experience of fatigue. In other words, fatigue may arise not only because of changes in one’s own biological and psychological systems but also because of changes that occur in individuals to whom one is socially connected (see Fig. 5).
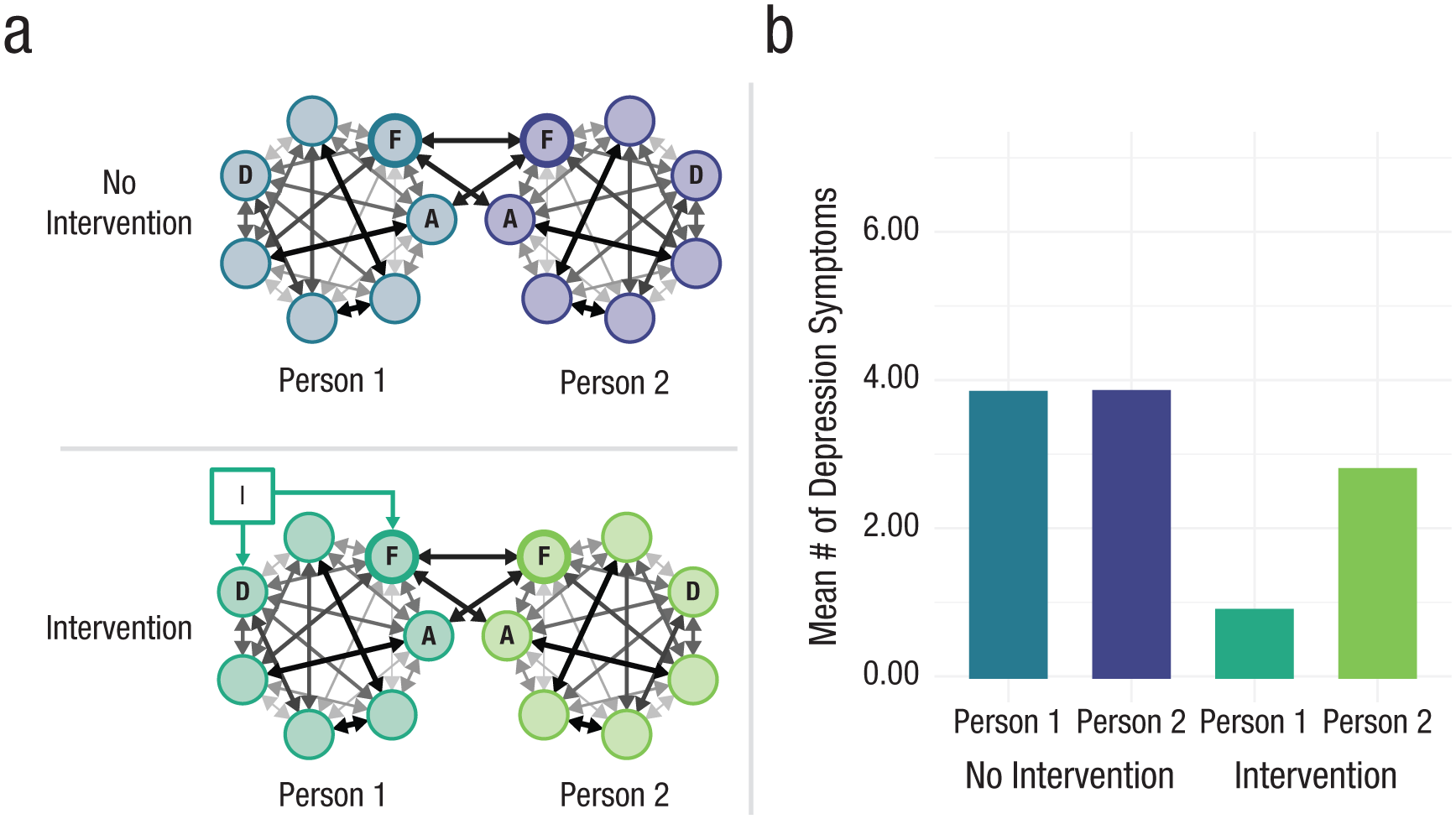
An illustration of the dynamics that can follow from an “interacting minds” framework (Wheatley et al., 2024) in which symptoms, represented by nodes in Figure 5a, interact not only within an individual but also across individuals in a social network (cf. Veenman et al., 2024). Building from the “moderate connectivity” Ising model in Figure 3, we extend the network to include interactions among fatigue (F) and anhedonia (A) for two individuals in a dyad (Person 1 and Person 2; for further detail, see the Supplemental Material available online). We then simulate under a control condition with no intervention and an intervention condition in which we lowered the propensity for fatigue (F) and depressed mood (D) to occur in Person 1. As depicted in Figure 5b, the intervention leads to significant symptom reduction for Person 1. Moreover, despite not being the target of intervention, symptom reduction is also observed for Person 2. Code used to produce this figure is available at https://osf.io/yp7zc/files/dn3ej.
Note that the relationship between fatigue and one’s social network may be mutually reinforcing (Fig. 5). As we showed in the allostatic models of fatigue reviewed in the previous subsection, the subjective feeling of tiredness is a signal: an alert that one’s resources are insufficient to meet the current demands of one’s environment (Stephan et al., 2016). Individuals are likely to respond to this signal by taking action to conserve energy, such as by withdrawing from social activities. Although an appropriate response to the signal of fatigue, this social withdrawal would create a pernicious cycle: As social connections fade, isolation intensifies, which, in turn, exacerbates stress and impairs recovery mechanisms, such as immune functioning (Matthews et al., 2024) and sleep (Grey et al., 2020). In other words, the amplifying feedback loops necessary to create the harmful stable states characteristic of depression can exist not only within the psychological system but also across social, psychological, and biological systems. Moreover, this example illustrates how efforts to regulate one’s internal systems in the short-term (e.g., staying home to conserve energy) could potentially erode the processes that promote long-term health (e.g., supportive relationships), a loss of resilience that places an individual at significant risk of shifting into a harmful stable state of depression.
Environmental systems
Although the label “biopsychosocial” implies a model with three levels of analysis, Engel envisioned a more expansive framework that included large-scale structural factors, such as one’s cultural and physical environment. In the years since Engel’s proposal, other theorists have gone further, explicating integrated frameworks that lay out how cultural and environmental factors may affect mental health (e.g., Bronfenbrenner, 1977, 1994; Kirkbride et al., 2024; Thimm-Kaiser et al., 2023), including modern frameworks that are well rooted in systems science (e.g., Rutter et al., 2017; van der Wal et al., 2021). The popularity of these theoretical frameworks, especially in the field of developmental psychopathology, attests to the field’s recognition of the important role that environmental factors play in mental health, especially those factors experienced early in life. Perhaps nowhere has this recognition been more explicit than in the rapidly developing field of population mental health. Population mental health rests on the view that mental-health researchers must move past the effort to identify single proximate causes for mental-health challenges and instead must understand health within a broader socio-ecological framework (Purtle et al., 2020). This means incorporating a focus on the pervasive macrosocial factors that influence a person throughout the course of life, spanning everything from social-cultural factors, such as discrimination, to the political structures in which one is embedded and the features of the built environments in which one lives (Kirkbride et al., 2024; Sampson & Galea, 2018, Uskul & Oishi, 2020).
As with the systems discussed at other levels of analysis, socio-ecological systems are composed of interrelated factors affecting mental health. However, rather than directly producing mental-health phenomena, as seen in the systems at other levels of analysis, socio-ecological systems principally affect mental health by constraining or enabling more proximal processes and circumstances related to mental health (Ross, 2024). To understand this role of socio-ecological systems in shaping the course of mental health, it is important to note that these systems are pervasive and typically operate at much slower timescales (years or decades) than the psychological processes most proximal to mental-health challenges. Note that this is a general feature of systems: At higher levels of organization (e.g., cultures or societies), systems tend to evolve more slowly than the systems embedded within them (e.g., an individual; Mobus & Kalton, 2014). From a person-level perspective, the years- or decades-long time horizon of socio-ecological systems often renders them “invisible”: They are simply the water one swims in, so to speak. From the perspective of mental-health research, these long time horizons make socio-ecological systems and their impact on mental health very difficult to study. Nonetheless, in the broader domain of systems science, researchers have carefully demonstrated how slow-changing environmental factors shape the behavior of systems operating at shorter timescales (Ludwig et al., 1978), and within the specific domain of mental health, there is ample evidence that socio-ecological systems shape and constrain mental health by differentially exposing individuals to social and material conditions that relate to mental-health outcomes. Adverse environmental factors associated with vulnerability to mental-health challenges, such as major depressive disorder, include current and persistent housing problems (Pengcheng et al., 2021; Pevalin et al., 2017), limited access to ambient green spaces (Geary et al., 2023), air pollution (Bhui et al., 2023), and rates of local crime (Baranyi et al., 2020). Exposure to these environmental stressors disproportionately falls on marginalized communities because of systems that produce and sustain intergenerational inequalities (e.g., systemic racism; Kirkbride et al., 2024) and are strongly related to poverty and deprivation (Evans & Cassells, 2014; Ridley et al., 2020).
The effects of environments characterized by poverty and deprivation are worth considering in the context of fatigue and depression. Environments characterized by deprivation are not only associated with increased exposure to harms in one’s physical environment (e.g., pollution and crime), they are also associated with potent social harms, such as household dysfunction, maltreatment, and lower levels of social trust (McElroy et al., 2019; Walsh et al., 2019). Together, the exposure to physical and social harms in these environments is likely to heighten the external demands one is experiencing while simultaneously undermining the ability to rely on others to help meet those demands, thereby plausibly giving rise to the discrepancy between resources and demands that elicits a subjective feeling of fatigue. Moreover, such environments foster a sense that the world is a harsh and unreliable place and that one is not in control over one’s own life (Orton et al., 2019; Weinberg et al., 2024), perceptions that, in turn, may further heighten risk for depressed mood (Culpin et al., 2015). Through these influences, environments characterized by deprivation may alter the symptom networks of individuals living in those environments, increasing the propensity for symptoms such as fatigue and depressed mood to arise and thereby creating vulnerability to the broader depression syndrome (see Fig. 6).
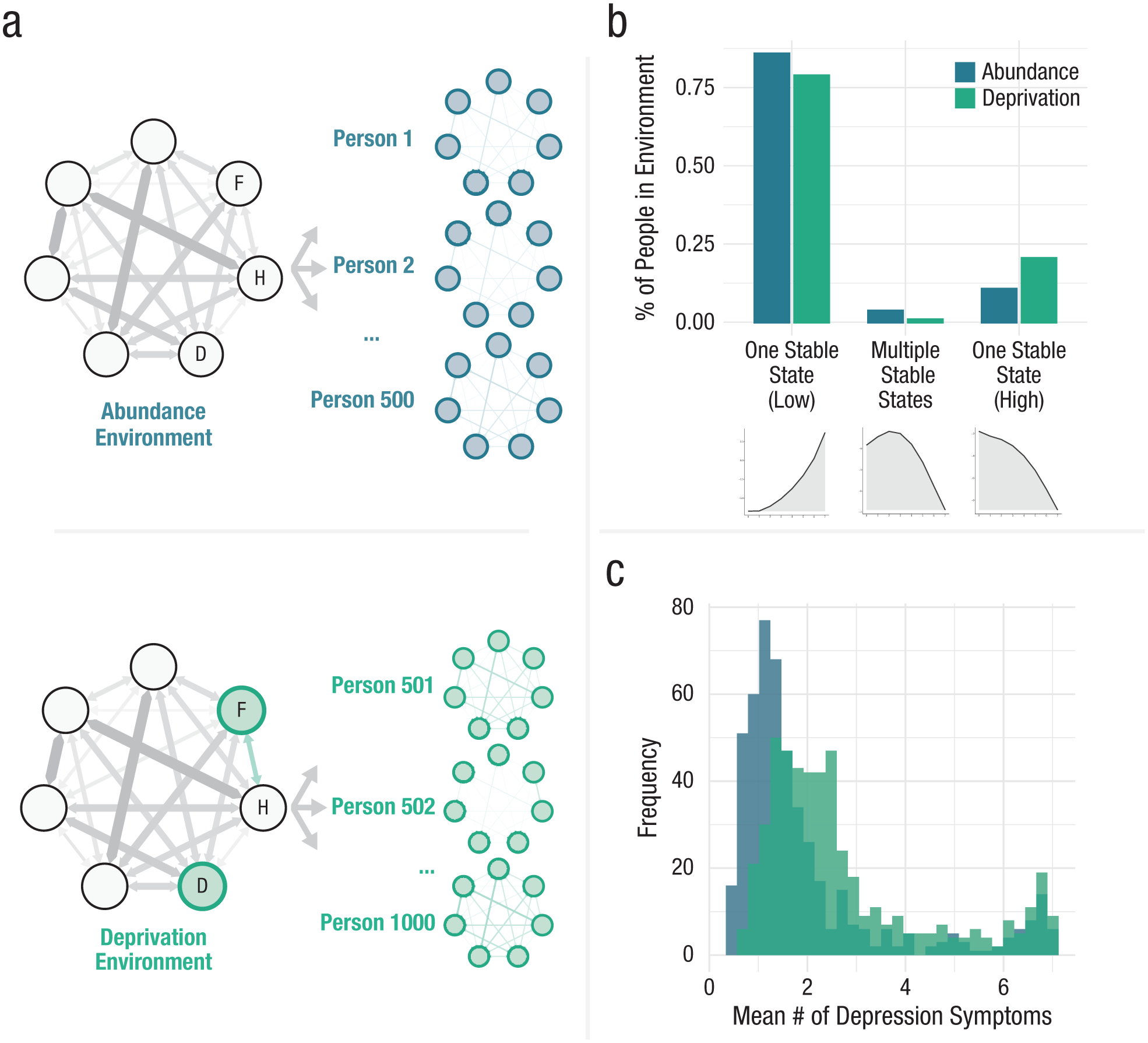
An illustration of the dynamics that could follow from environmental influences on the psychological-symptom network. (a) Building on the Ising model depicted in Figure 3, we generated symptom networks for 1,000 individuals with varying symptom connectivity. For half of these simulated individuals, the network was left unaltered, representing an “abundance” environment in which environmental resources were sufficient to meet one’s needs. The remaining simulated individuals were placed in a “deprivation” environment in which resources were insufficient to meet one’s needs. Here, there was, on average, a greater propensity to experience fatigue (F) and depressed mood (D) and a strengthened association between fatigue and feelings of hopelessness (H). (b) Those in the deprivation environment were more likely to have stability landscapes characterized by a single stable state of elevated depression symptoms. As a consequence, (c) individuals in the deprivation environment were more likely to exhibit persistently elevated depression symptoms. Code used to produce this figure is available at https://osf.io/yp7zc/files/mhgf4.
Note that these shifts in one’s perceptions of the world may also create fertile ground for behaviors that are effective in the short-term when resources are scarce and unpredictable but hinder the attainment of longer-term goals, thereby perpetuating deprivation within the socio-ecological system (Sheehy-Skeffington, 2020). Environments characterized by deprivation therefore can remain stubbornly persistent, in part, because they give rise to socio-cognitive and behavioral responses that, in turn, exacerbate or maintain the socio-ecological system. In other words, these environments can become self-perpetuating because of amplifying feedback between individual and environmental factors. As a result, interventions that would have been capable of preventing an environment from falling into a harmful stable state may have minimal effect if applied after the environment has already fallen into that harmful state (e.g., for a demonstration of this hysteresis effect arising from interactions between individual and environmental factors, see De Courson et al., 2023). This exchange between individual and environmental factors may be especially important in the context of severe psychopathology that substantially impairs functioning, heightening risk for exposure to harmful environments and, in turn, exacerbating psychopathology (van der Wal., 2021).
Given the time course on which socio-ecological systems operate, it is perhaps not surprising that population mental research often incorporates a developmental perspective, giving consideration to the cumulative and chronic influence of deprivation and stressful environments over the course of one’s life (Evans & Cassells, 2014; Weinberg et al., 2024). Likewise, developmental psychopathologists have long been mindful of the role of environmental systems in mental health (e.g., van Geert, 2009). In both disciplines, researchers have paid particular attention to the impact of early life events on the course of mental health. The mutually reinforcing nature of the interactions within sociocultural systems (e.g., financial challenges undermining the stability of the home environment which, in turn, exacerbates financial challenges) and between sociocultural systems and the individual (e.g., deprivation of social support fostering distrust and, in turn, a further deprivation) suggests that adverse experiences in childhood can ripple throughout the life span. Indeed, these amplifying effects provide important context for the many physical- and mental-health factors found to be associated with childhood abuse, including the experience of persistent fatigue and depression (Borsini et al., 2014; Maniglio, 2010).
As noted, a fundamental insight from systems science is that the effort to shift an individual from a harmful and resilient stable state of distress is likely to be substantially more costly than preventing the formation of such a stable state in the first place. From a socio-ecological systems perspective, this lesson underscores the importance of early intervention and calls for systems-based and complexity-science approaches to understanding how environmental factors relate to mental health. For applied clinical and counseling psychologists, this work also stresses the importance of transdisciplinary collaboration with researchers investigating the structural, legal, political, and ideological systems that perpetuate exposure—and inequality in exposure—to environmental and social stressors (Fink et al., 2016; Haynes et al., 2024; Langellier et al., 2019; Rydin et al., 2012).
Conclusion
Engel’s biopsychosocial model posited that mental disorders arise from a hierarchy of systems embedded within other systems. As even our cursory review illustrates, there is now substantial evidence gathered across scientific fields to support the view that systems operating across levels of analysis contribute to mental-health challenges. Recent work conceptualizing mental disorders as systems of interacting symptoms affords some insight into how researchers might begin to integrate findings from across domains of science into a more comprehensive understanding of mental health. Working from this framework, researchers can consider how the various ways in which systems at one level of analysis may constitute, interact with, amplify, or constrain the processes operating on another, thereby integrating these mechanisms into a more comprehensive understanding of psychopathology. Although a promising path forward, this integrative work will require extensive transdisciplinary collaboration, work that is likely to be challenging and may run counter to the incentive structures that guide mental-health research. In the final section of this article, we consider how to address these obstacles and lay a foundation for transdisciplinary work.
Toward a Transdisciplinary Systems Science of Mental Health
To this point, we have argued that transdisciplinary collaboration rooted in systems science is needed if the field is to realize Engel’s vision for a biopsychosocial approach and make meaningful advances in the understanding of mental health. We suspect it will be especially helpful to collaborate with systems scientists (e.g., network scientists, control theorists, and systems engineers), researchers working in substantive domains with a strong focus on systems (e.g., ecologists, systems biologists, and systems neuroscientists), and researchers working in substantive domains of clear importance to biological, psychological, social, or environmental domains affecting mental health (e.g., physiologists, cognitive scientists, sociologists, and experts in population mental health). Such collaborations are necessary both to learn from the advances other fields have made in understanding the principles that guide system behavior and because mental disorders are inherently transdisciplinary phenomena that will require integration of expertise from a wide range of domains to fully explain.
Unfortunately, transdisciplinary collaboration is exceedingly challenging. Discipline-specific conceptual frameworks, jargon, methods, incentives, and professional networks all hinder efforts to bring together researchers across disciplines to advance understanding of mental health. Recently, the psychologist Dylan Gee and her colleagues (2022) argued that clinical psychologists have a unique opportunity to help overcome these challenges by serving as hubs that connect researchers across disciplines and facilitate efforts to work together toward a more complete understanding of mental health. We agree and, in this section, identify three steps that the field can take to equip clinical, counseling, and other applied psychologists with the skills and resources needed to serve in this role as facilitators of transdisciplinary mental-health research.
Step 1: adopt integrative pluralism as a framework for transdisciplinary collaboration
The biopsychosocial model neither excludes nor prioritizes any single system in mental-health treatment or research. We consider this a significant strength, but it is not without challenge: If an array of intertwined systems can contribute to mental-health problems, each of which may be an entire field of study unto itself, how can one hope to make meaningful advances toward a cumulative understanding of mental disorders? Whereas a traditional hypothetico-deductive approach may suffice when working from a reductionist framework, it is unlikely to be sufficient for advancing the understanding of complex systems. A biopsychosocial framework requires a scientific method that embraces the complexity of the systems under investigation and the need for cumulative and integrative advances in the understanding of mental health.
In our view, the most promising path by which the field might proceed is through piecemeal integrative pluralism: an approach in which the field works, bit by bit, to integrate systems operating across levels of analysis into causal models that explain specific mental-health-related phenomena and from which the field might iteratively move toward a more complete understanding of psychopathology (Kendler, 2005; Mitchell, 2002). Drawing from this framework and the abductive theory of scientific method (Haig, 2008), we see two central tasks for researchers aiming to develop and advance biopsychosocial theories of specific mental-health conditions.
First, explaining mental-health-related phenomena requires that the field first identify and rigorously describe them (Eronen & Bringmann, 2021; Jack et al., 2018). In many fields, the early stages of the discipline focused extensively on establishing and describing phenomena (e.g., people spent centuries mapping the motion of planets across the sky before Kepler and Newton sought to explain their motion). However, in its rush to be taken seriously as a science, psychology quickly moved toward a focus on hypothesis testing and largely skipped this stage of carefully describing the phenomena under investigation (Tinbergen, 1963). For clinical and counseling psychologists to serve effectively as domain experts with deep substantive expertise on a given mental-health phenomenon, it will be critical to step back and devote efforts toward establishing and rigorously describing robust mental-health phenomena.
In the study of complex systems, it is especially important to collect rich data on phenomena as they evolve over time. Intensive longitudinal data are therefore likely to be especially valuable for describing the dynamics of the phenomena under investigation. Given the breadth of timescales at play across biological, psychological, social, and environmental systems, it will be especially valuable to investigate the behavior of phenomena over time across multiple timescales within the same sample of participants (e.g., rigorously examining the dynamics and correlates of individual components of fatigue over minutes in experimental paradigms, hours in ecological momentary assessments, days in daily diary studies, and months or years in panel studies over critical periods of development), ideally in samples large enough to study interindividual differences of intraindividual processes.
The second task is the generation and integration of theories that explain well-established mental-health phenomena. The history of systems science (Mobus & Kalton, 2014) and the scientific study of complex phenomena (Mitchell, 2002) suggest that models, especially mathematical or computational models that lay out how a posited system might operate, will be critical to advancing the understanding of the interlocking systems giving rise to psychopathology. Models provide support for deducing precisely what a given theory predicts, something that is critical in the domain of systems science because it is typically all but impossible to anticipate how a complex system will behave using mental reasoning alone (Smaldino, 2017). Model-derived predictions equip the field to evaluate what the theory can and cannot explain (Van Dongen et al., 2024) and to develop more rigorous tests of biopsychosocial theories than are possible when relying only on Engel’s broad conceptual framework (Haslbeck et al., 2022). In the context of integrative pluralism, mathematical and computational models have the additional benefit of expressing theories transparently and in a language used across scientific disciplines, thereby facilitating the integration of theories across scientific domains. For example, a differential equation model positing specific psychological processes at play in the onset of psychosis may specify how parameters of that model vary as a function of environmental context and, in turn, how the psychological system’s behavior may alter one’s environment. In this article, we have used toy models to illustrate how systems might plausibly be integrated across levels of analysis. However, efforts to do so in more theoretically rigorous and empirically grounded ways will face significant obstacles. At this stage, the statistical models that can readily and reliably be estimated from data (e.g., an Ising model) are unlikely to faithfully represent the processes at play in mental-health systems, and the models that represent these processes in all their complexity (e.g., differential equation models) are extremely difficult to estimate from the kinds of noisy data available in psychological research. Accordingly, efforts to model biopsychosocial theories of mental health are likely to be challenging. Nonetheless, mathematical and computational models provide theorists with a means by which they might slowly begin to tackle this challenge of working to better integrate and accumulatively develop biopsychosocial theories of mental-health phenomena (Robinaugh et al., 2021).
Step 2: train psychologists in the foundational skills needed for transdisciplinary systems science
In their proposal for clinical psychologists to serve as transdisciplinary scientists, Gee et al. (2022) placed an emphasis on the role of graduate and undergraduate training, arguing that clinical psychologists must be trained to communicate with experts across disciplines. The question becomes what languages should educators be teaching students to facilitate this communication. What training do psychologists need to guide the integration and ongoing development of biopsychosocial theories of mental health?
If science has a common language, it is the language of mathematics. From the earliest stages of general system theory, mathematics, especially differential equations, have played a critical role in shaping the understanding of how systems behave by equipping them to generate mathematical models of the phenomena under investigation. The formalization of systems theories as mathematical equations is one means by which researchers across disparate disciplines, such as biology, ecology, and physics, were able to identify consistency in the structure and dynamics of the systems they study. Researchers in mental-health sciences are increasingly making use of these mathematical tools (e.g., Wang et al., 2023); however, most training programs have not yet evolved to support students in developing these skills (Gee et al., 2022). Without this foundation, students are not well positioned to use the mathematical or computational tools needed to rigorously describe the dynamics of mental-health phenomena or to develop formal biopsychosocial theories to explain those phenomena.
There are at least two potential means by which this training might be provided to students. In the first, advanced methods would be taught in dedicated courses to graduate students in psychology (e.g., mathematical modeling for clinical psychologists), particularly those students focused on careers in research. Although preferable to the status quo, there are limits to taking this approach in isolation. In many cases, graduate students lack the relevant foundational skills to set them up for success in such courses, and introducing additional advanced coursework at the graduate level alongside the many other demands on their time is likely to create a challenging environment in which to develop this skill set. Accordingly, if such coursework were adopted, it would, at a minimum, be necessary to ensure that there is time and space afforded for acquiring these skills in ways that do not simply entail adding another requirement atop all others. A second (potentially complementary) option is to provide trainees with foundational skills in their undergraduate training that will allow them to better engage with advanced topics in their later graduate studies. For example, undergraduate students in STEM fields routinely take math and computer-science courses (e.g., linear algebra, differential equations, basic programming) that provide a foundation for later training. By incorporating such coursework into the required training of undergraduate students in psychology, particularly individuals who are aiming for a career in psychological research, educators would equip students to succeed in developing the common language of mathematics and computational programming that will allow them to communicate with researchers across disciplines. Moreover, with this foundation, students will be better positioned to learn the advanced statistical tools needed for rigorously analyzing time-series data and the theory-construction and theory-modeling skills that will allow them to contribute to the generation, integration, and ongoing development of biopsychosocial theories of mental health formalized as mathematical or computational models.
Alongside this foundation, psychologists will also benefit from training in systems science, a position advocated by Engel (1977) in his original proposal of the biopsychosocial model (see the quote that introduces this article). As noted throughout this article, systems are ubiquitous, and dynamical systems are studied across domains of science. If psychologists are to support transdisciplinary teams in their effort to work together to unravel the complexity of the systems underlying mental disorders, then they will need a firm understanding of how systems operate (e.g., understanding amplifying feedback loops, regulatory feedback loops, alternative stable states, hysteresis, and other concepts we have reviewed here). In other words, the systems-based nature of the biopsychosocial model not only makes clear that the field needs transdisciplinary collaboration, but it also provides a conceptual framework through which such collaborations can occur, and it will be important for psychologists to be well versed in this framework. In addition, systems science can provide a clear scaffolding from which to incorporate training in the role of structural and culture systems in mental health, going beyond merely noting that social determinants are important factors of which to be aware by generating a deeper appreciation for their role in mental health and the ways in which environmental-systems-level intervention may promote well-being (Sharma et al., 2018).
The reimagining of psychology training that we have proposed here would provide a foundational step to equipping applied psychologists to thrive as transdisciplinary collaborators. However, this is a long-term step that will take considerable time to bear fruit and fails to support individuals who have already completed their undergraduate or graduate studies. Moreover, the barriers to revising training at this level are likely to be significant and risk being inequitable in their accessibility because only well-resourced institutions may be positioned to implement and support such changes. Accordingly, it will also be critical to develop resources beyond formal university-based coursework alone, including conference workshops, summer schools, massive open online courses, and both physical and virtual spaces by which transdisciplinary researchers might come together to support one another’s efforts. In the domain of systems science, the Complexity Explorer produced by the Sante Fe Institute provides a model to which the field can aspire—a collection of freely available online courses, tutorials, and other resources for studying complex systems (Santa Fe Institute, 2024). In its own right, the Complexity Explorer is a highly valuable and accessible resource for mental-health researchers aiming to learn the language and methods of systems science. More importantly, the website also provides a model for how the field might create a structured set of resources that can meet the needs of researchers regardless of the backgrounds from which they are approaching this work.
As we imagine opportunities to bolster the training of applied psychologists as hubs of transdisciplinary collaboration, it is important to note that systemic inequities have long limited access to training opportunities in mathematical and computational sciences, especially for women and people of color, often leaving these groups underrepresented in the kinds of disciplines that will be needed to facilitate transdisciplinary collaboration. Moreover, alongside psychology, many such fields have long-standing and troubling histories of racism and sexism that have led to the exclusion of individuals from marginalized backgrounds (Charlesworth & Banaji, 2019; Copur-Gencturk et al., 2020). As the field seeks to bring new training opportunities into applied psychology, it must ensure that this training is available, accessible, and supportive to individuals from all backgrounds, especially groups that have been historically excluded from such training (Birhane & Guest, 2020; Copur-Gencturk et al., 2020; Wang, 2021). This need is clear from a systems-based biopsychosocial lens, with its emphasis on large-scale social and environmental systems that not only harm mental health but also shape the research priorities in the field and restrict opportunities for care. Accordingly, any effort to move toward greater systems-focused transdisciplinary training and research must be aligned with broader efforts to dismantle systemic inequities in psychology (Auguste et al., 2023; Buchanan et al., 2021; Rodriguez-Seijas et al., 2024; Tseng & Lee, 2021).
Step 3: incentivize transdisciplinary research
The steps described here would focus research on the description and explanation of robust mental-health phenomena and foster the development of skills for transdisciplinary research in applied psychology. However, no amount of training in mathematics, modeling, time-series analysis, or systems science will encourage robust transdisciplinary research if the incentive structures through which careers advance do not reward such research. It will be important to consider incentives for at least three levels of organization: the transdisciplinary team, the fields of clinical and counseling psychology, and the broader field of mental-health research.
Participation in transdisciplinary teams affords unique and highly rewarding opportunities. Indeed, for us, transdisciplinary collaborations have provided many of our most valued experiences as researchers. However, these teams also present many unique challenges. In part, these challenges lie in difficulty communicating across disciplines, but there are also challenges presented by the distinct norms, interests, and incentive structures for researchers coming from different disciplines. For example, whereas the academic “currency” in psychology is focused on journal publications, computer scientists prioritize publishing in conference proceedings. Given this, it is important for researchers to define clear, shared goals in their collaborative projects and clear roles and responsibilities to ensure that progress is made toward shared outcomes that are of interest to all parties involved.
Even when teams are well organized and aligned, transdisciplinary research requires significant time investment and comes with many additional challenges compared with traditional within-field research. In mental-health science, it is thus important that formal programs and institutional incentive structures are developed that help motivate transdisciplinary collaboration. Such efforts could include group-based awards and recognition for transdisciplinary collaborations, recognition and encouragement of transdisciplinary collaborations in departmental merit- or tenure-review processes, and prioritization of transdisciplinary collaborations in conference symposia and workshops to both encourage greater transdisciplinary research and foster opportunity to inject new ideas from other fields into professional societies and identify shared interests and goals with researchers from different disciplines.
Finally, it will be critical to advocate for greater funding for research across the full spectrum of systems at play in mental health. A recent commentary on the biopsychosocial model highlighted that a reinvigoration of this model may serve as a valuable unifying force, bringing researchers together toward a more coherent investigation of mental health, but only if such research is valued and funded (Tabb, 2021). Tabb (2021) made a compelling case that despite the broad notional acceptance of the biopsychosocial model, major funding agencies have increasingly prioritized biological research and that funding priorities have become increasingly divorced from investigating mental health as a societal problem (see also, Scull, 2021). By focusing research disproportionately on biological factors, the mental-health field risks an impoverished understanding of mental health and an inadequate repertoire of interventions for addressing mental-health challenges. It is therefore critical for mental-health researchers to advocate for greater funding for psychological, social, and environmental research that will support the kinds of transdisciplinary collaborations needed to make progress in reducing the burden of mental disorder.
Conclusion
If the mental-health field takes the biopsychosocial model seriously, a transdisciplinary approach will be needed to advance the understanding of mental health. Clinical and counseling psychologists can play a critical role in this work, serving as skilled facilitators of communication across disciplines and experts in the mental-health phenomena they seek to explain. As a systems-based framework, the biopsychosocial model not only calls for transdisciplinary research but also provides a foundation for that work to take place, aligning researchers in the effort to understand the systems that give rise to mental health and the interventions that can most effectively reduce the burden of mental illness. Accordingly, the future of the biopsychosocial model will be strengthened if the field invests in building toward a transdisciplinary systems science of mental health.
Footnotes
Acknowledgements
Ethical approval was not required. Analyses were conducted using fully de-identified data made available for public use. Because the data are not individually identifiable, our use of these publicly available data did not require institutional-review-board approval. No studies were preregistered. Supplementary materials, including all code used for this article, are available at https://osf.io/yp7zc/. Data used for this article are available at ![]() . In this article, we do not present an empirical or simulation-based study. Analyses and simulations were used only to produce illustrations of systems and system behavior and should not be interpreted as empirical or substantive contributions to the literature.
. In this article, we do not present an empirical or simulation-based study. Analyses and simulations were used only to produce illustrations of systems and system behavior and should not be interpreted as empirical or substantive contributions to the literature.
Transparency
Action Editor: Alexander Shackman
Editor: Jennifer L. Tackett
Author Contributions