
Abstract
Motor symptoms have emerged as a promising target for understanding mechanisms, prognosis, and treatment in psychology. Although motor abnormalities are observed across mental-health conditions, transdiagnostic research has been limited. It is not well understood whether motor symptoms are a broad endophenotypic marker or a predictor of specific symptoms. We leverage a hierarchical dimensional symptom structure to examine transdiagnostic relationships between psychological and self-reported motor symptoms in 3,460 participants in the Multi-Site Assessment of Psychosis-Risk study. Overall motor problems (βs = 0.07–0.25), dyskinesia (βs = 0.07–0.31), and coordination (βs = 0.05–0.23) were related positively at different strengths to all symptom domains. Amount of physical activity was positively related to mania and substance use (βs = 0.08–0.09) and negatively related to detachment, fear, and distress (βs = 0.05–0.27). These results suggest that motor domains may provide utility as both a general endophenotypic marker and more specific predictor of serious mental illness; we discuss implications for research and clinical settings.
Keywords
Motor abnormalities, such as deficits in coordination, sensorimotor integration, and motor activity, are present in the diagnostic conceptualization of particular mental disorders, such as autism spectrum disorder, attention-deficit/hyperactivity disorder (ADHD), schizophrenia, and mood disorders (Poletti & Raballo, 2022). However, they are not widely recognized in either psychological research or clinical practice. A growing body of research has highlighted an essential role of motor symptoms in psychology, suggesting that an understanding of motor symptoms can provide critical insight into the mechanisms, intervention points, and prognostic predictions in serious mental illness (e.g., Peralta & Cuesta, 2017). However, there is some lack of clarity in the role that motor systems serve in psychopathology. Motor abnormalities have been conceptually proposed as serving as both a broad transdiagnostic marker of general risk for serious mental illness and a specific predictor in clinical conditions, such as psychosis (Burton et al., 2016; Poletti & Raballo, 2022). This leaves an open question about how motor symptoms fit into and contribute to the conceptualization of psychopathology. To address this gap, we examined self-reported motor variables in the context of a symptom framework based on the principles of the Hierarchical Taxonomy of Psychopathology (HiTOP), a hierarchical dimensional framework that is ideally suited for characterizing psychopathology transdiagnostically by differentiating across broad and specific symptom dimensions.
Understanding the motor system in psychopathology is particularly useful for several reasons. Motor systems develop throughout the course of infancy and childhood, coinciding with critical developmental periods and providing information about a combination of early genetic and environmental factors (Poletti & Raballo, 2022). In addition, these systems have been well mapped and can provide insight into relevant neural circuitry that has been implicated in serious mental illness (e.g., dopaminergic circuitry; Walther & Mittal, 2022). Finally, in both categorical conceptualizations of diagnoses (e.g., slowed motor activity in the conceptualization of depression in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association, 2013) and behavioral work (e.g., motor slowing in depression; Schrijvers et al., 2008; Wüthrich et al., 2022), motor abnormalities, including deficits in coordination, impaired motor control, and altered motor activity, have been observed across a number of conditions, including depression, bipolar disorder, psychosis, and ADHD (Osborne et al., 2024; Peralta & Cuesta, 2017; Walther & Mittal, 2022; reviewed in Table 1). This prevalence of motor symptoms across diagnostic categories provides strong evidence for the interplay between psychological and motor functioning, which may be relevant for understanding both developmental and functional mechanisms in mental illness.
Summary of Literature Surrounding Motor Symptoms in Psychology
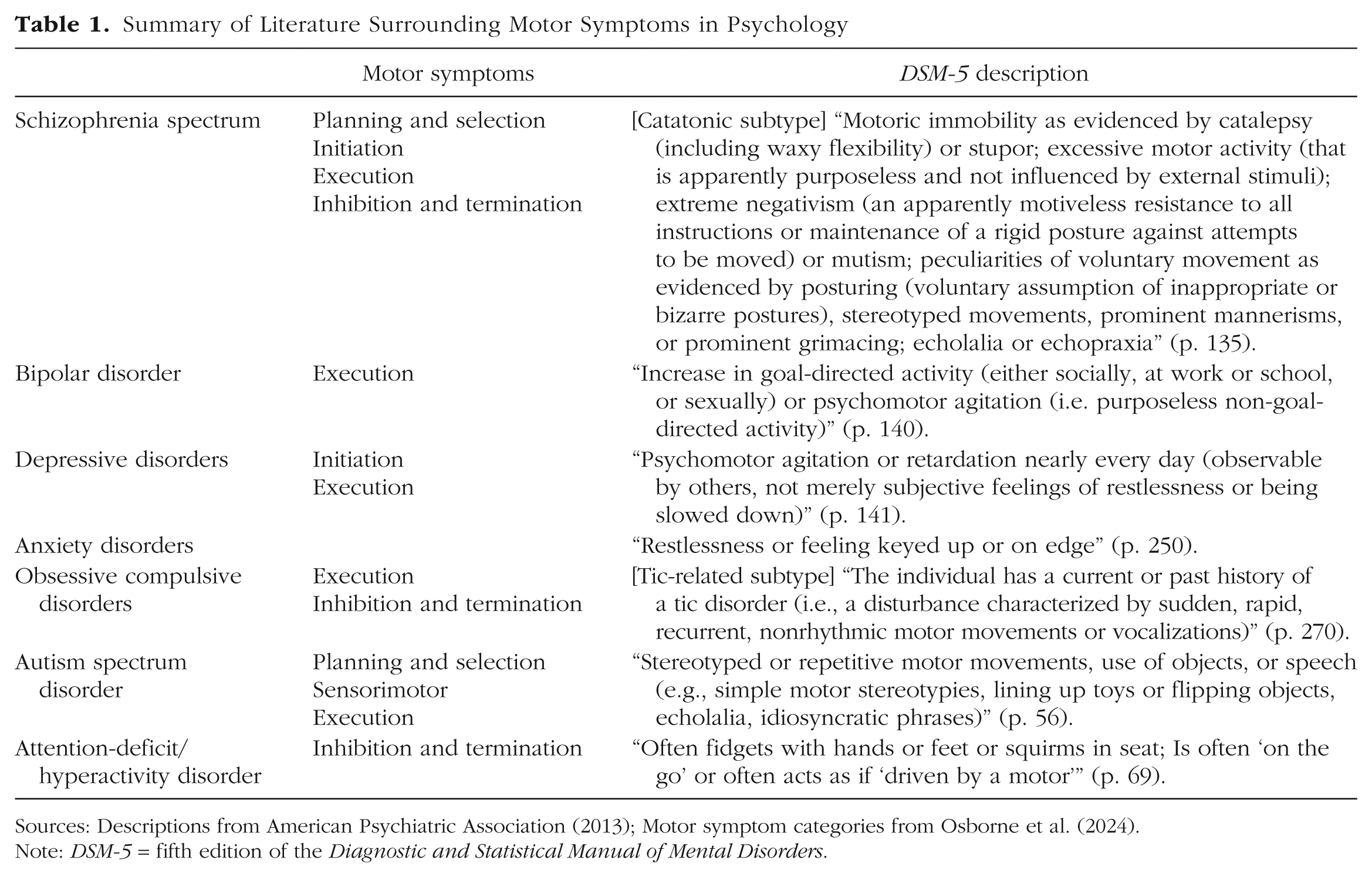
Sources: Descriptions from American Psychiatric Association (2013); Motor symptom categories from Osborne et al. (2024).
Note: DSM-5 = fifth edition of the Diagnostic and Statistical Manual of Mental Disorders.
In addition to their general transdiagnostic relevance, motor symptoms may provide prognostic value in specific psychiatric conditions, notably psychosis. Work in individuals at clinical high risk for psychosis has suggested that motor symptoms, such as dyscoordination, dyskinesia (sudden, uncontrolled movements), and motor slowing, predict later functioning, symptom severity, and risk for transition to a threshold psychotic disorder (Carrión et al., 2013; Damme et al., 2020, 2024; Schiffman, 2017). Consistent with these findings, motor symptoms have been positioned as a central feature of the psychosis spectrum and have been used to drive mechanistic theories about the development of psychotic disorders (Walther & Mittal, 2017). However, research on psychomotor symptoms in psychiatric disorders has been historically limited to the psychosis literature (Peralta & Cuesta, 2017). Therefore, the prevalence of motor findings in psychosis could, in part, be related to limited research in other clinical conditions. Indeed, although there is evidence for the importance of motor symptoms both across and within disorders, transdiagnostic research with motor symptoms is highly limited.
An ideal framework for addressing this gap is one that allows psychopathological symptoms to vary across both broad factors and more specific latent symptom dimensions. Such a framework, based on the principles of systems like HiTOP, is well situated for addressing questions about heterogeneity and overlap between clinical symptoms (Kotov et al., 2022). Note that psychomotor alterations are already present in the HiTOP hierarchy, represented by symptoms such as cleaning rituals, agitation, retardation, problematic impulsivity, and impatient urgency (Kotov et al., 2022). In the current study, we examine a heterogeneous sample of individuals with a range of psychopathological symptoms (Ellman et al., 2020) in which the principles of HiTOP have already been used to develop a hierarchical dimensional structure of clinical symptoms (Cowan et al., 2024). If motor symptoms are a purely nonspecific endophenotypic marker of risk, we would expect them to relate to broad dimensions (e.g., the “p factor,” or one-factor, model) without clearly differentiating between symptom domains. On the other hand, if motor symptoms were purely specific predictors, we would expect motor symptoms to relate to specific symptom dimensions (e.g., the 10-factor model) and would differently relate to symptom domains. By investigating psychomotor symptoms in this framework, in the current study, we are the first to integrate motor symptoms into a dimensional conceptualization of psychological symptoms, and we discuss implications for driving the understanding of the utility of motor symptoms for characterizing the shared and unique mechanisms and prognostic indicators of mental illness.
Transparency and Openness
Preregistration
This study’s analyses were not preregistered and are clearly labeled as exploratory.
Data, materials, code, and online resources
Data from the current study were periodically uploaded to a publicly accessible data repository, consistent with the data-sharing plan and approved by institutional review boards at all study sites. All participants gave informed consent to participate in the current study. Data can be accessed at https://nda.nih.gov/edit_collection.html?id=2783. The questionnaires used in the current study are easily accessible and can be found at https://osf.io/ug5yd. Study analysis code is available online and can be accessed at https://github.com/hrcowan/HiTOP-MAP and https://osf.io/ug5yd.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures relevant to the current research question. The current study involved an analysis of data within the context of a larger preexisting research study (for full details, see Ellman et al., 2020).
Ethical approval
The current project was approved by institutional review boards at each of the study sites, and all participants provided written informed consent (or assent for participants under age 18 and consent of a parent).
Method
Participants
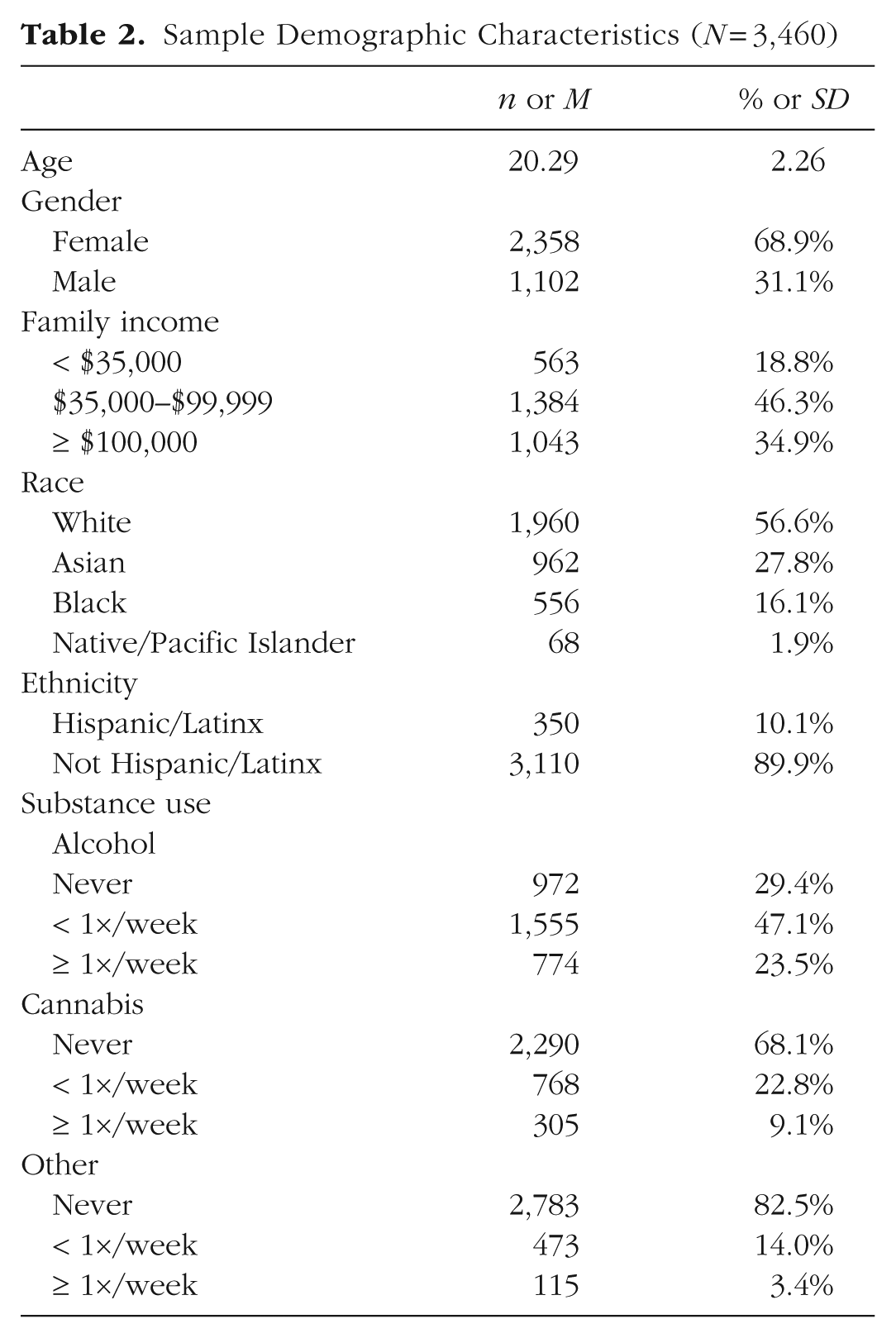
The sample consisted of 3,460 participants who took part in the Multi-Site Assessment of Psychosis-Risk Study (for details, see Ellman et al., 2020), a subset of the final sample in which a hierarchical dimensional symptom structure was derived when data collection was ongoing (Cowan et al., 2024). Participants were a socioeconomically, racially, and ethnically diverse sample of individuals recruited from the greater regions of Philadelphia, Baltimore, Chicago, and Irvine (including surrounding suburban and rural areas). Participants were eligible if they were ages 16 to 30, had sufficient proficiency in English to complete online questions, and had vision that was normal or corrected to normal. Participants were not excluded based on any demographic or clinical characteristics. All participants completed an online battery of questionnaires that included demographic variables, psychotic-like experiences, depression, anxiety, mania, dissociation, substance use, and self-reported motor issues (see Measures). For sample demographic characteristics, see Table 2.
Sample Demographic Characteristics (N = 3,460)
Measures
In previous work with this sample, a hierarchical dimensional symptom structure was derived by unfolding or “bass-ackwards” factor analysis of 204 self-report items from questionnaires assessing psychotic-like experiences, depression, anxiety, mania, dissociation, and substance use (Cowan et al., 2024; Goldberg, 2006). These questionnaires included the Prodromal Questionnaire (Loewy et al., 2005); Prevention Through Risk Identification, Management, and Education screen (Kline et al., 2012); Prodromal screen (Heinimaa et al., 2003); Center for Epidemiological Studies – Depression Scale (Kohout et al., 1993); State-Trait Anxiety Inventory – Trait form (Bieling et al., 1998); Social Phobia Scale (Mattick & Clarke, 1998); General Behavior Inventory – Patient Version (Youngstrom et al., 2008); Dissociative Experiences Scale (Bernstein & Putnam, 1986); and Drug Use Frequency Scale (O’Farrell et al., 2003). In the current study, we leveraged the previously defined factor structure as an established hierarchical dimensional structure of clinical symptoms (see Fig. 1; Cowan et al., 2024).
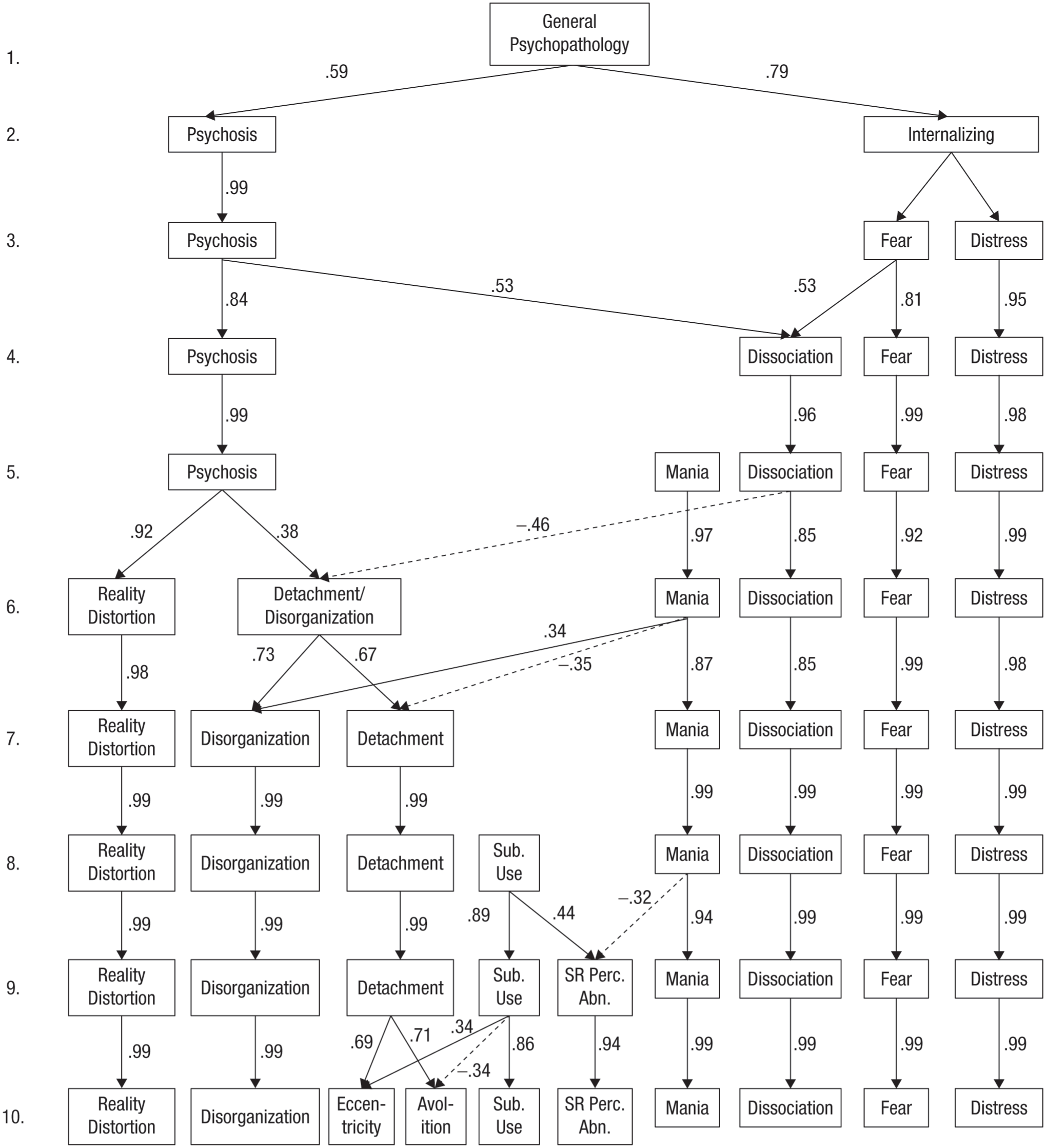
Hierarchical dimensional factor structure of clinical symptoms. Reproduced from Cowan et al. (2024).
The Sensorimotor and Activity Psychosis-Risk (SMAP-R) Scale is a 14-item self-report questionnaire containing items related to early developmental motor delays, sensorimotor functioning and abnormalities, and frequency of physical activity (Damme et al., 2021). The scale was validated in the current study sample and was shown to have good discriminant, convergent, and predictive validity for assessing motor symptoms in populations at clinical high risk for psychosis and other psychopathology (Damme et al., 2021). In the current study, we examined mean scores on the SMAP-R and scores on three subscales with good reliability in both exploratory and validation samples: sensorimotor abnormalities-dyskinesia (e.g., “Do you experience urges to twitch or move suddenly, or make noises?”; exploratory sample: α = .67, validation sample: α = .68), sensorimotor abnormalities-coordination (e.g., “Do you feel clumsy?”; exploratory sample: α = .71, validation sample: α = .75), and physical activity (e.g., “How often do you participate in physical activities [jogging, team sports] each week?”; exploratory sample: α = .68, validation sample: α = .69). The sensorimotor-abnormalities facet and coordination-abnormalities subscale showed good convergent validity such that greater scores were related to lowered rate of finger tapping (Damme et al., 2021). The SMAP-R has been shown to distinguish psychosis risk from other psychopathology (i.e., anxiety and depression) and relates to risk for psychosis (Damme et al., 2021). In replication samples, it was also shown to pick up on sensorimotor abnormalities associated with depression and anxiety (Damme et al., 2021).
Statistical analysis
To examine the factor structure that best predicted self-reported motor symptoms, regression models were run predicting SMAP-R mean score and dyskinesia, coordination, and activity subscales using factor scores at Levels 1 through 10, following Cowan et al. (2024; see Fig. 1). Next, the model of best fit was selected based on adjusted R2, Akaike information criterion (AIC), and Bayesian information criterion (BIC). The model that performed best on average across the metrics was selected for each motor-outcome variable. All final models performed either best or second best across all metrics (see Table S1 in the Supplemental Material available online). After the best-fitting regression model was selected, that model’s predictors were examined to determine which symptom clusters best predicted self-reported motor symptoms.
Results
Selection of models
Figure 2a shows model fit for models with self-reported motor symptoms entered as dependent variables and symptom dimensions (reproduced from Cowan et al., 2024) at increasing complexity of the factor hierarchy (Factor Levels 1–10) entered as independent variables. For adjusted R2, AIC, and BIC for each model, see Table S1 in the Supplemental Material. The selected models were as follows: SMAP-R mean score, Level 5 (adjusted R2 = .1089, AIC = 1,752.60, BIC = 1,791.55); dyskinesia, Level 8 (adjusted R2 = .2517, AIC = 2,244.40, BIC = 2,300.04); coordination, Level 8 (adjusted R2 = .1608, AIC = 4,093.10, BIC = 4,148.73); and activity, Level 8 (adjusted R2 = .1140, AIC = 4,468.92, BIC = 4,524.56).
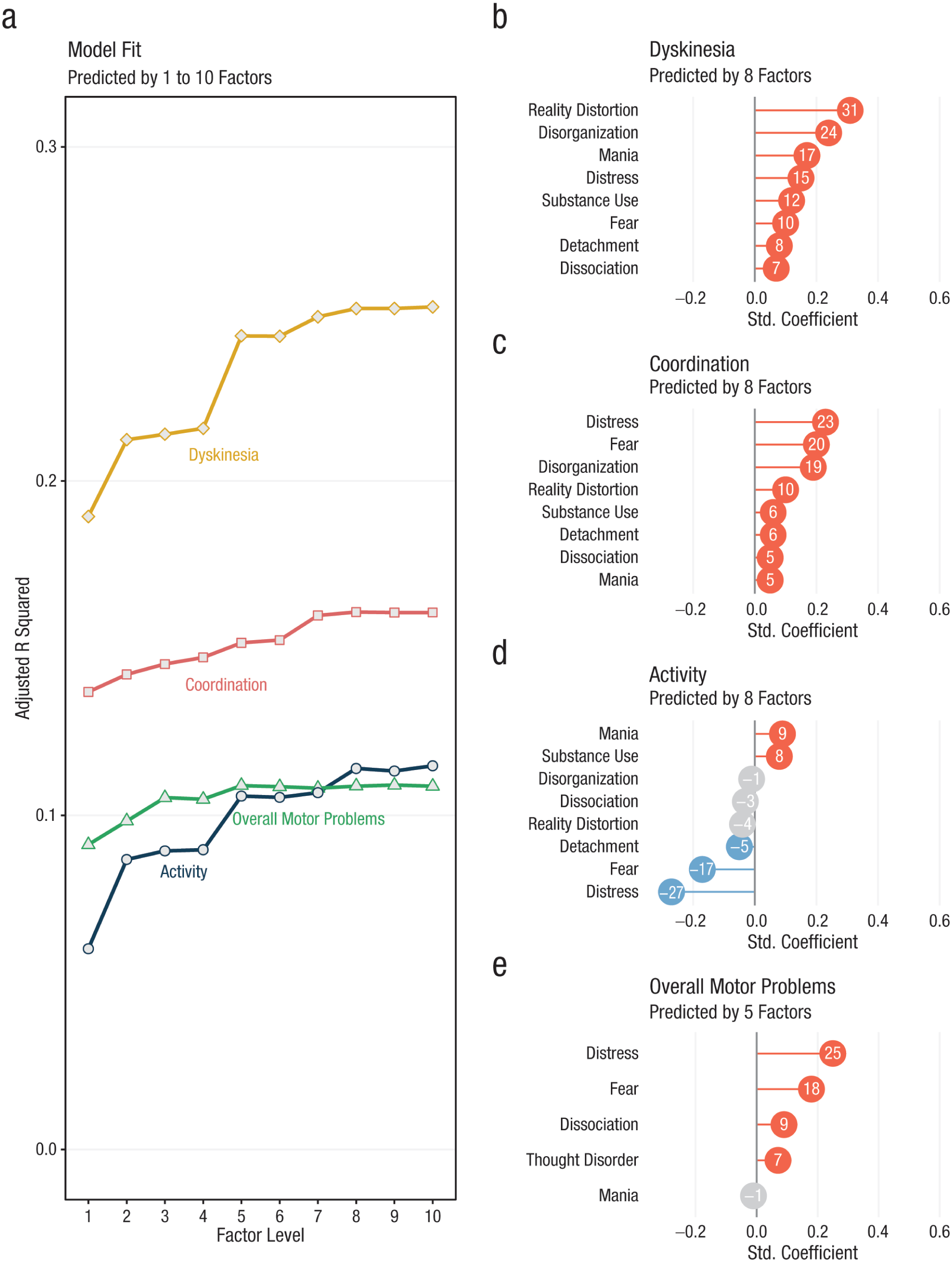
Relationships between hierarchical transdiagnostic factors (see Fig. 1) and self-reported motor symptoms. (a) Overall model fit for regressions with mean score (green triangles), dyskinesia facet (yellow diamonds), coordination facet (red squares), and activity subscale (blue circles). (b–e) Standardized regression coefficients for the selected models. Red indicates a significant positive coefficient (p < .05), blue indicates a significant negative coefficient (p < .05), and gray indicates a nonsignificant coefficient (p ≥ .05).
Associations between clinical and motor symptoms
In examining the relationships between the model with five factors and the SMAP-R mean score (Fig. 2e), we found a significant relationship between SMAP-R mean score and distress (β = 0.25, 95% confidence interval [CI] = [0.09, 0.13], p < .001), thought disorder (β = 0.07, 95% CI = [0.03, 0.11], p = .001), fear (β = 0.18, 95% CI = [0.14, 0.23], p < .001), and dissociation (β = 0.09, 95% CI = [0.05, 0.13], p < .001) such that greater self-reported motor abnormalities were related to more severe clinical symptoms. The relationship between SMAP-R mean score and mania was not significant (β = −0.01, 95% CI = [−0.05, 0.03], p = .723).
In examining the relationships between the eight-factor model and the dyskinesia subscale (Fig. 2b), we found a significant relationship between dyskinesia and distress (β = 0.15, 95% CI = [0.11, 0.19], p < .001), reality distortion (β = 0.31, 95% CI = [0.27, 0.35], p < .001), fear (β = 0.10, 95% CI = [0.07, 0.14], p < .001), detachment (β = 0.08, 95% CI = [0.04, 0.12], p < .001), mania (β = 0.17, 95% CI = [0.13, 0.21], p < .001), dissociation (β = 0.07, 95% CI = [0.03, 0.11], p < .001), disorganization (β = 0.24, 95% CI = [0.20, 0.28], p < .001), and substance use (β = 0.12, 95% CI = [0.08, 0.16], p < .001) such that greater dyskinesia was related to greater psychopathology.
In examining the relationships between the eight-factor model and the coordination subscale (Fig. 2c), we found a significant relationship between self-reported coordination abnormalities and distress (β = 0.23, 95% CI = [0.19, 0.27], p < .001), reality distortion (β = 0.10, 95% CI = [0.06, 0.15], p < .001), fear (β = 0.20, 95% CI = [0.16, 0.25], p < .001), detachment (β = 0.06, 95% CI = [0.02, 0.10], p = .003), mania (β = 0.05, 95% CI = [0.00, 0.09], p = .029), dissociation (β = 0.05, 95% CI = [0.01, 0.09], p = .018), disorganization (β = 0.19, 95% CI = [0.15, 0.23], p < 0.001), and substance use (β = 0.06, 95% CI = [0.02, 0.10], p = .003) such that greater coordination abnormalities were related to more severe psychopathology.
In examining the relationships between the eight-factor model and the activity subscale (Fig. 2d), we found a significant relationship between activity and distress (β = −0.27, 95% CI = [−0.31, −0.23], p < .001), fear (β = −0.17, 95% CI = [−0.21, −0.12], p < .001), and detachment (β = −0.05, 95% CI = [−0.08, −0.01], p = .027) such that greater activity is related to lower psychopathology. There was also a significant relationship between mania (β = 0.09, 95% CI = [0.05, 0.13], p < .001) and substance use (β = 0.08, 95% CI = [0.04, 0.12], p < .001) such that more severe symptoms were related to greater activity.
Discussion
In light of increasing evidence for the importance of motor symptoms in psychopathology, in the current study, we address an important gap in characterizing the contributions of motor symptoms to a hierarchical dimensional symptom framework based on the principles of HiTOP. These findings have implications for driving forward an understanding of the utility of motor assessments in research and laying the foundation for incorporating psychomotor symptoms into clinical practice. First, we found that more specific models at the level of symptoms outperformed the more general p-factor model, providing evidence against psychomotor symptoms being an entirely nonspecific predictor of psychopathology. Second, we found significant relationships between psychomotor symptoms and symptom domains such that all symptom domains were significantly related to psychomotor symptoms. These results support the prevalence of motor symptoms in psychopathology and highlight the need for additional cross-diagnostic research. Third, we found that the strength and patterns of relationships across psychomotor symptom domains differed across clusters of clinical symptoms, which could provide insight into relevant mechanisms. Key findings and implications are reviewed in more detail below.
Testing broad and specific conceptualizations
We found that general motor problems were best predicted by a five-factor structure in which the dyskinesia, coordination, and activity subscales were all best predicted by an eight-factor structure of clinical symptoms. Given that more specific models outperformed more general p-factor models, this provides initial evidence against motor signs being an entirely nonspecific endophenotypic marker. On the other hand, overall motor problems, dyskinetic movements, and coordination abnormalities were all significantly and positively related across symptom domains (with the exception of overall motor problems and mania, which was nonsignificant). In addition, models predicting general motor problems improved only marginally with increasing model complexity. These results may suggest that shared variance related to general psychopathology is predictive of overall motor problems and that increasingly complex factor structures may be providing only additional granularity in understanding the degree of relationships across factors. Therefore, although there is evidence that motor symptoms are not entirely nonspecific markers, study findings suggest that overall motor problems and coordination abnormalities are indeed generally related to an increased severity of psychopathology, as has been proposed in previous models (Burton et al., 2016). These results are consistent with the tension identified in the prior literature, suggesting that any psychopathological symptoms may be generally related to motor abnormalities but that specific symptom clusters differ in the direction and degree to which they relate to psychomotor domains. By examining patterns of relationships across subscales, further insight about the interplay between motor symptoms and domains of psychopathology can be gained.
Psychomotor symptoms across symptom domains
Reality distortion, disorganization, and thought disorder (dimensions related to psychosis risk) demonstrated a pattern of relationships consistent with sensorimotor abnormalities, particularly within the domain of dyskinetic movements. Dyskinesia often emerges as a particularly informative predictor of outcomes in psychosis-risk populations (Callaway et al., 2014; Mittal et al., 2010), reflecting abnormalities in striatal-dopamine activity that are thought to be central to the psychosis spectrum (DeLong & Wichmann, 2007). Given that sensorimotor abnormalities were positively related to all symptom domains but (in the case of dyskinesia) most strongly related to psychosis-risk symptoms, results of the current study support prior theory suggesting that sensorimotor abnormalities, particularly dyskinesia, may be prognostically useful in psychosis-risk populations but may not be predictive of psychosis risk in a general population sample (Burton et al., 2016, 2023).
Mania was related to increased motor abnormalities in all subscales, reflecting both sensorimotor abnormalities and an increase in reported physical activity. This profile is consistent with findings of motor hyperactivity in mania, which have been conceived as a core feature of the manic syndrome (Cheniaux et al., 2014, 2024; Perry et al., 2016). Substance use showed a similar pattern of relationships and was the only other factor to relate to increased physical activity. Given that substance use disorders are conceptualized along the disinhibited externalizing spectrum (Kotov et al., 2022), this may be consistent with increased impulsivity along that symptom dimension (Loree et al., 2015). Bipolar spectrum and substance use disorders have been observed to show neurological hard signs (e.g., involuntary movements) and soft signs (e.g., coordination abnormalities) at an increased rate, although to a lesser extent than schizophrenia (Whitty et al., 2009). The observed relationship with dyskinesia and coordination could be consistent with this shared vulnerability.
Distress was strongly related to psychomotor symptoms across all domains, including an increase in dyskinesia and coordination abnormalities, and considerably reduced physical activity. This profile of dyscoordination and reduced motor activity is consistent with reductions in motor activity in depressive disorders and states (Schrijvers et al., 2008; Wüthrich et al., 2022) and significantly elevated rates of coordination abnormalities that are predictive of long-term course of depressive symptoms (Damme et al., 2022). A similar pattern of relationships, although to a lesser degree, was observed with both detachment (i.e., negative psychotic symptoms) and fear (i.e., anxiety). Negative symptoms present with a similar pattern of anhedonia and amotivation as depressive symptoms, which is reflected in reduced motor activity, consistent with this finding (Nuoffer et al., 2022; Walther et al., 2015). On the other hand, research on motor symptoms in anxiety is limited. However, anxiety disorders fall along the internalizing spectrum with depressive disorders, and therefore, this profile could be consistent with motor changes associated with internalizing psychopathology (Kotov et al., 2022).
Strengths and limitations
The current study has several limitations and a number of strengths. First, participants were recruited from four catchment areas in the United States and therefore may not generalize to different contexts. Second, although the study benefited from leveraging a short self-report questionnaire in its accessibility, it is difficult to determine whether psychomotor symptoms reported in the study are a result of differences in self-report or true behavioral differences in motor functioning. Future studies should further validate the SMAP-R in additional samples and replicate the current findings with direct measures of motor functioning (e.g., passive-sensing data). Finally, the current analyses were cross-sectional in nature and used only the questionnaire portion of the Multi-Site Assessment of Psychosis-Risk study to ascertain symptom categories; therefore, it would be interesting for future studies to assess these association across mental-health disorders. Furthermore, the model in the current study does not represent the full range of HiTOP spectra. Therefore, future work should integrate a broader range of metrics to determine whether results differ in the full HiTOP model. A key strength of this study is its sample size and conceptual innovation. It is the first and largest study to date to examine motor functions in the context of the principles of HiTOP. By integrating data from 3,460 participants, it offers a uniquely comprehensive transdiagnostic perspective on motor symptoms across a broad spectrum of psychological domains. The large, well-characterized sample allows for robust statistical modeling and improves the generalizability of the results.
Conclusions and next steps
Together, these findings suggest that motor symptoms may provide both general and specific contributions to understanding domains of psychopathology within the principles of the HiTOP framework. In other words, assessment of general motor ability may provide utility as a transdiagnostic marker, and assessment of specific motor domains (particularly the patterns of deficits across domains) and within target populations (e.g., psychosis-risk populations) may provide more specific predictive utility. These results have important implications for future work. First, they highlight that motor symptoms could provide insight into the shared and distinct mechanisms across clusters of psychological symptoms. With future work in populations with diagnosed mental-health conditions, this may lay the groundwork for development of interventions and prognostic screening tools. Furthermore, the study advances the field by linking self-reported motor abnormalities to hierarchical symptom dimensions rather than categorical diagnoses, offering new insights into the role of motor domains as general endophenotypic markers and specific predictors of severe mental illness. This approach bridges the gap between mechanistic understanding and clinical relevance and lays the groundwork for future research on motor biomarkers and intervention targets in psychiatry.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261450607 – Supplemental material for Motor Abnormalities and the Hierarchical Taxonomy of Psychopathology: Incorporating a Psychomotor Perspective Into a Hierarchical Dimensional Symptom Framework
Supplemental material, sj-docx-1-cpx-10.1177_21677026261450607 for Motor Abnormalities and the Hierarchical Taxonomy of Psychopathology: Incorporating a Psychomotor Perspective Into a Hierarchical Dimensional Symptom Framework by Jessica Fattal, Lauren M. Ellman, Jason Schiffman, Dusan Hirjak, Sophia Parmacek, Henry R. Cowan and Vijay A. Mittal in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
Henry R. Cowan and Vijay A. Mittal are co-final authors.
H.R. Cowan and V. A. Mittal are co-senior authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.