
Abstract
Background:
Insulin-like growth factor-1 (IGF-1) plays a role in metabolism and immune regulation. Although obesity is associated with chronic inflammation, the relationship between IGF-1 levels and systemic inflammatory markers remains unclear. This study aimed to examine the association between IGF-1 levels, systemic inflammation, and metabolic comorbidities in individuals with obesity.
Methods:
This retrospective cross-sectional study included 214 adults with a BMI ≥35 kg/m2 evaluated between June 2019 and March 2025. Participants were classified as low IGF-1 (standard deviation score [SDS] ≤ −2.0) or standard IGF-1 (−2.0 < SDS < 2.0). Clinical and laboratory data were analyzed, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, systemic immune-inflammation index (SII), systemic inflammation response index, and systemic inflammation aggregate index.
Results:
Low IGF-1 was identified in 8.88% of patients. No differences were found between groups regarding diabetes, dyslipidemia, or hypertension. NLR (2.21 vs. 1.79; p = 0.005) and SII (614.6 vs. 521.8; p = 0.041) were significantly higher in the standard IGF-1 group. SII was positively correlated with systolic blood pressure, alanine aminotransferase, and insulin. IGF-1 SDS was not correlated with inflammatory markers.
Conclusions:
Lower IGF-1 levels were not associated with higher systemic inflammation. These findings highlight the heterogeneity of inflammatory responses in obesity and suggest the need for further research.
Keywords
What Is Already Known About This Subject
Obesity is associated with chronic low-grade inflammation, which can be assessed using systemic immune-inflammatory markers. Insulin-like growth factor-1 (IGF-1) plays an important role in metabolic regulation and may be downregulated in individuals with obesity. The relationship between IGF-1 levels, subclinical systemic inflammation, and metabolic comorbidities in obesity remains unclear, with previous studies yielding conflicting results.
What This Study Adds
This is the first study to examine the association between IGF-1 levels, systemic inflammatory markers, and metabolic comorbidities in a well-characterized cohort of individuals with obesity. Low IGF-1 levels were not associated with increased subclinical inflammation; individuals with standard IGF-1 levels had higher neutrophil-to-lymphocyte ratios and systemic immune-inflammation indices. These findings challenge the assumption that low IGF-1 indicates greater inflammation in obesity and highlight the heterogeneity of the immunometabolic profiles across obesity phenotypes.
Introduction
Obesity is a major public health issue associated with several metabolic comorbidities, such as dyslipidemia, hypertension, cardiovascular disease (CVD), and type 2 diabetes mellitus.1,2 Insulin-like growth factor-1 (IGF-1) plays a key role in metabolic regulation; however, few studies have examined the relationship between IGF-1 levels and metabolic comorbidities in individuals with obesity.3,4 This relationship is complex: Lower IGF-1 levels have been associated with increased adiposity, metabolic disorders, and elevated cardiovascular risk. Individuals with obesity and low IGF-1 levels tend to have higher levels of inflammation, dyslipidemia, and hyperuricemia than those with standard IGF-1 levels. 3 Conversely, some studies report no association between IGF-1 and glucose tolerance, hypertension, or CVD.5,6 IGF-1 deficiency has been linked to impaired lipid metabolism, CVD, and altered metabolic profiles in patients with diabetes.7,8
In overweight and obese pediatric populations, findings are inconsistent. Some studies have shown that higher IGF-1 levels are associated with metabolic disorders such as dyslipidemia, hypercholesterolemia, and hypertension, potentially influenced by cortisol levels.9,10 IGF-1 metabolism is further modulated by factors such as adiponectin, hepatic growth hormone (GH) sensitivity, and IGF-binding protein 1, complicating its metabolic role.11,12
Obesity is also characterized by chronic low-grade inflammation. Proinflammatory cytokines from adipose tissue, including TNF-α and IL-6, exacerbate systemic inflammation. 13 IGF-1 may play a role in this process by enhancing the release of interferon, IL-17, and IL-22 via microbial toll-like receptor ligands and promoting neutrophil production through granulocyte colony-stimulating factor stimulation.14,15 Inflammation in obesity is heterogeneous, encompassing both hepatic acute-phase responses, typically reflected by elevated C-reactive protein (CRP), and chronic low-grade immune activation represented by hematological indices such as the neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII). Differentiating between these inflammatory phenotypes is essential for understanding IGF-1’s role in metabolic inflammation.
Emerging inflammatory markers, such as NLR, lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), mean platelet volume-to-platelet ratio, and SII, have been identified as indicators of chronic subclinical inflammation, particularly in thyroid, adrenal gland, and neuroendocrine disorders.16–20 Both NLR and PLR are elevated in obesity, reflecting chronic subclinical inflammation that may be associated with insulin resistance and metabolic disturbances.21,22 SII has been associated with obesity-related parameters, such as body mass index (BMI), waist circumference, and visceral adiposity index.23,24
To the best of our knowledge, no studies have investigated the relationship between IGF-1 levels and systemic inflammatory markers in patients with obesity. This study aimed to examine the clinical features and systemic immune-inflammatory markers associated with IGF-1 levels in individuals with obesity.
Materials and Methods
Patient population and data collection
This retrospective cross-sectional study was conducted at the Department of Endocrinology and Metabolism, Ankara Bilkent City Hospital, between June 2019 and March 2025. A total of 214 adult patients (aged ≥18 years) with a BMI ≥35 kg/m2, followed up for obesity, were included. Patients with hematological or solid malignancies, acute or chronic infections, thyroid dysfunction, pregnant or postpartum status, hepatic or renal failure, or congenital/secondary GH deficiency were excluded. Patients with known pituitary or hypothalamic disorders, including those with documented GH deficiency or structural pituitary lesions on prior imaging, were excluded. Because this was a retrospective study, GH stimulation testing was not performed; however, individuals with any clinical or biochemical evidence suggestive of secondary GH deficiency were not included. Biochemical evidence suggestive of secondary GH deficiency was defined as abnormalities in other pituitary axes, including inappropriate low/normal TSH with low free T4 (central hypothyroidism), low morning cortisol and/or ACTH suggestive of secondary adrenal insufficiency, or low gonadotropins with low sex steroids consistent with hypogonadotropic hypogonadism; patients with such findings were excluded.
Demographic and laboratory data were retrieved from medical records, including glucose, insulin, hemoglobin A1c (HbA1c), Homeostatic Model Assessment for Insulin Resistance, creatinine, aspartate aminotransferase, alanine aminotransferase (ALT), triglycerides, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total cholesterol, uric acid, TSH, CRP, IGF-1, neutrophils, lymphocytes, monocytes, and platelets. IGF-1 levels were standardized using age- and sex-specific standard deviation scores (SDSs). Patients were categorized into two groups: low IGF-1 (SDS ≤ −2.0) and standard IGF-1 (−2.0 < SDS < 2.0).
Systemic inflammatory indices were calculated as follows: NLR = neutrophils/lymphocytes; PLR = platelets/lymphocytes; LMR = lymphocytes/monocytes; SII = (platelets × neutrophils)/lymphocytes; systemic inflammation response index (SIRI) = (neutrophils × monocytes)/lymphocytes; and systemic inflammation aggregate index (SIAI) = (neutrophils × monocytes × platelets)/lymphocytes.
Definitions of diabetes, hypertension, hyperuricemia, and dyslipidemia
Diabetes mellitus was defined based on the American Diabetes Association criteria. 25 A diagnosis was established if any of the following were present: (1) fasting plasma glucose ≥126 mg/dL (7.0 mmol/L); (2) 2-h plasma glucose ≥200 mg/dL (11.1 mmol/L) during a 75 g oral glucose tolerance test; (3) random plasma glucose ≥200 mg/dL (11.1 mmol/L) with classical hyperglycemic symptoms; or (4) HbA1c ≥6.5% (National Glycohemoglobin Standardization Program standardized). For individuals without unequivocal hyperglycemia, diagnosis was confirmed on a separate day.
Patients who were already on antidiabetic medications were classified as having diabetes mellitus.
Hypertension was defined according to international guidelines. 26 A diagnosis was established if any of the following were present: (1) office blood pressure ≥140/90 mmHg; (2) home or ambulatory blood pressure ≥135/85 mmHg; or (3) current use of antihypertensive medications regardless of blood pressure measurements.
Hyperuricemia was defined as a serum uric acid >7.0 mg/dL in men and >6.0 mg/dL in women, or current use of urate-lowering therapy at the time of evaluation, regardless of uric acid levels. 27
Dyslipidemia was defined according to the 2018 American College of Cardiology/American Heart Association guidelines. A diagnosis was established if any of the following were present: (1) LDL-C ≥130 mg/dL; (2) HDL-C <40 mg/dL; (3) triglycerides ≥150 mg/dL; or (4) non-HDL-C (total cholesterol minus HDL-C) ≥160 mg/dL. All lipid parameters were directly measured without the use of the Friedewald formula. Patients receiving lipid-lowering therapy were considered dyslipidemic, regardless of current lipid measurements. 28 This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ankara Bilkent City Hospital No. 1 Clinical Research Ethics Committee (Approval No.: TABED 1-24-484, August 28, 2024). Written informed consent was obtained from all participants.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics version 30.0 (IBM Corp., Armonk, NY, USA). Normality of continuous variables was assessed using the Kolmogorov–Smirnov test and visual methods (histograms and Q-Q plots). Normally distributed variables were expressed as mean ± standard deviation, and nonnormally distributed variables as median (interquartile range). Categorical variables were expressed as frequencies and percentages. Between-group comparisons were conducted using the independent samples t-test for normally distributed variables and the Mann–Whitney U test for nonnormally variables. Categorical variables were compared using the chi-squared test or Fisher’s exact test, as appropriate. Correlations between IGF-1 SDS and systemic immune-inflammatory indices were evaluated using Pearson or Spearman correlation analyses, depending on data distribution.
Statistical significance was set at a two-tailed p < 0.05. A post hoc power analysis assuming a moderate-to-large effect size (Cohen’s d = 0.7) and a 1:10 group ratio determined that a minimum of 196 participants (18 and 178 in the low and standard IGF-1 groups, respectively) were required to achieve 80% power at an alpha level of 0.05. The study met this requirement.
Results
A total of 214 patients with obesity (BMI ≥ 35 kg/m2) were included in the study. Of these, 19 patients (8.88%) had low IGF-1 levels (IGF-1 SDS ≤ −2.0), while 195 patients (91.12%) had standard IGF-1 levels (−2.0 < SDS < 2.0). Among the study population, 175 patients (81.8%) had a BMI ≥40 kg/m2, consistent with the classification of morbid obesity. No patients had elevated IGF-1 levels (SDS ≥ 2.0). Baseline characteristics and laboratory parameters are summarized in Table 1.
Demographic, Laboratory, and Clinical Characteristics of Patients in the Low and Standard Insulin-like Growth Factor-1 Groups
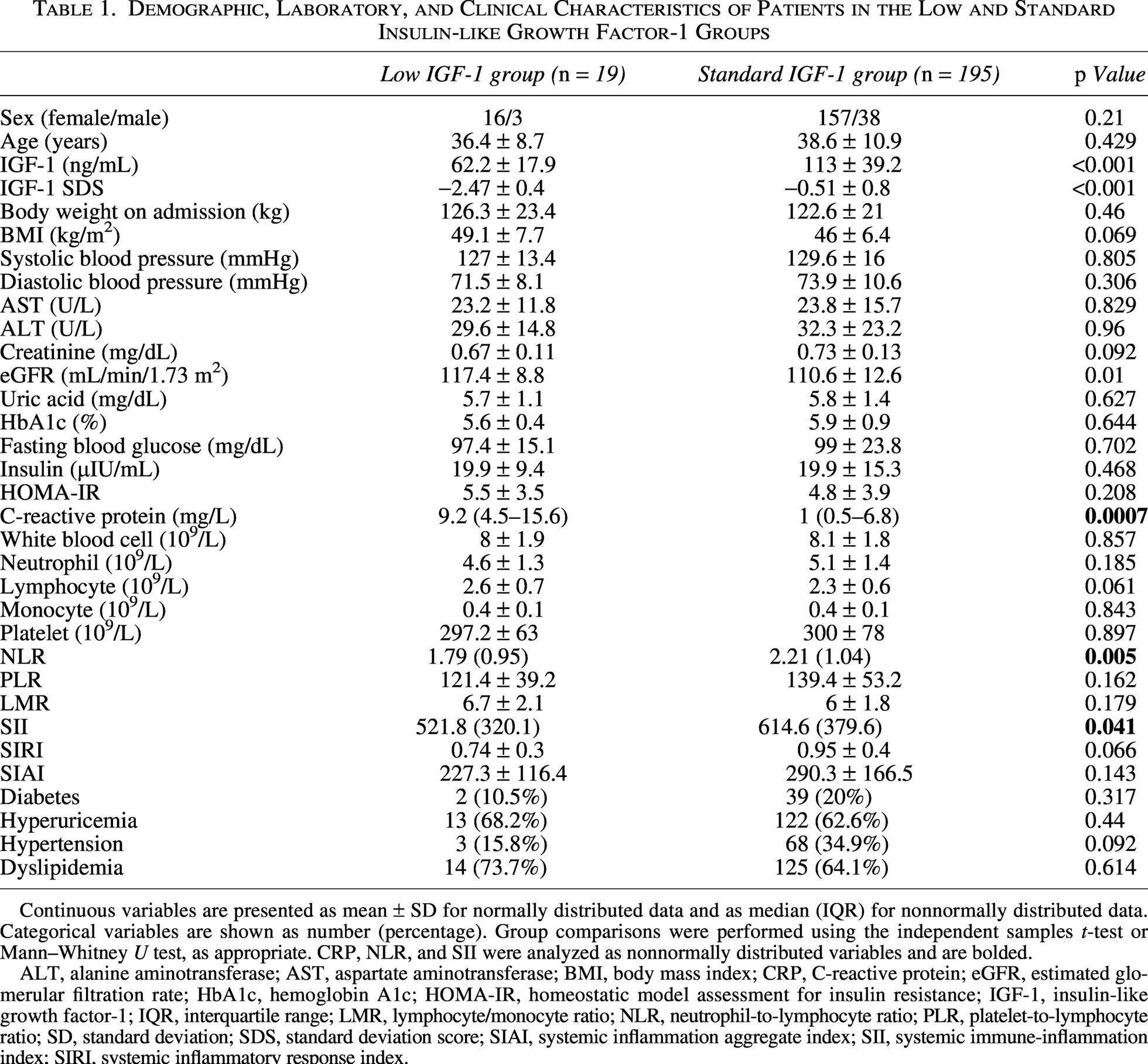
Continuous variables are presented as mean ± SD for normally distributed data and as median (IQR) for nonnormally distributed data. Categorical variables are shown as number (percentage). Group comparisons were performed using the independent samples t-test or Mann–Whitney U test, as appropriate. CRP, NLR, and SII were analyzed as nonnormally distributed variables and are bolded.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HOMA-IR, homeostatic model assessment for insulin resistance; IGF-1, insulin-like growth factor-1; IQR, interquartile range; LMR, lymphocyte/monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SD, standard deviation; SDS, standard deviation score; SIAI, systemic inflammation aggregate index; SII, systemic immune-inflammation index; SIRI, systemic inflammatory response index.
There were no significant differences in age, sex distribution, BMI, or body weight between the low and standard IGF-1 groups. Both IGF-1 (ng/mL) and IGF-1 SDS values were significantly lower in the low IGF-1 group than in the standard IGF-1 group (p < 0.001).
There were no significant differences in glycemic parameters or lipid parameters between the low and standard IGF-1 groups. Similarly, the prevalence of diabetes (10.5% vs. 20%, p = 0.317), hyperuricemia (68.2% vs. 62.6%, p = 0.44), and dyslipidemia (73.7% vs. 64.1%, p = 0.614) did not significantly differ between the groups.
Among systemic immune-inflammatory indices, the NLR and SII were significantly higher in the standard IGF-1 group than in the low IGF-1 group (NLR: 2.21 (1.04) vs. 1.79 (0.95), p = 0.005; SII: 614.6 (379.6) vs. 521.8 (321.1), p = 0.041; Figures 1 and 2). No significant differences were observed in the PLR, LMR, SIRI, and SIAI of the two groups. CRP levels were significantly higher in the low IGF-1 group compared with the standard IGF-1 group (9.2 vs. 1.0 mg/L, p = 0.0007).
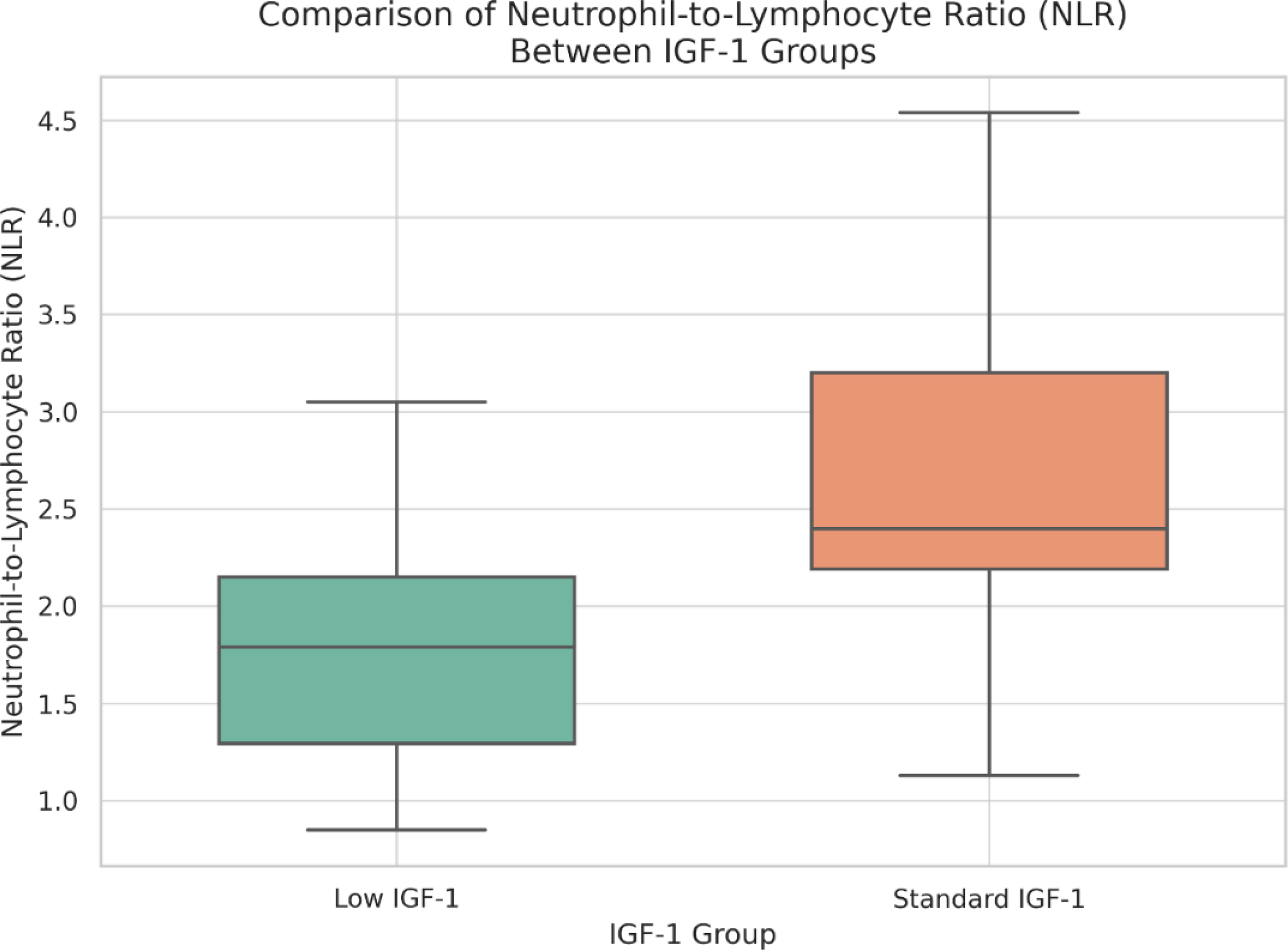
Comparison of NLR between the low and standard IGF-1 groups. NLR, neutrophil/lymphocyte ratio; IGF-1, insulin-like growth factor-1.
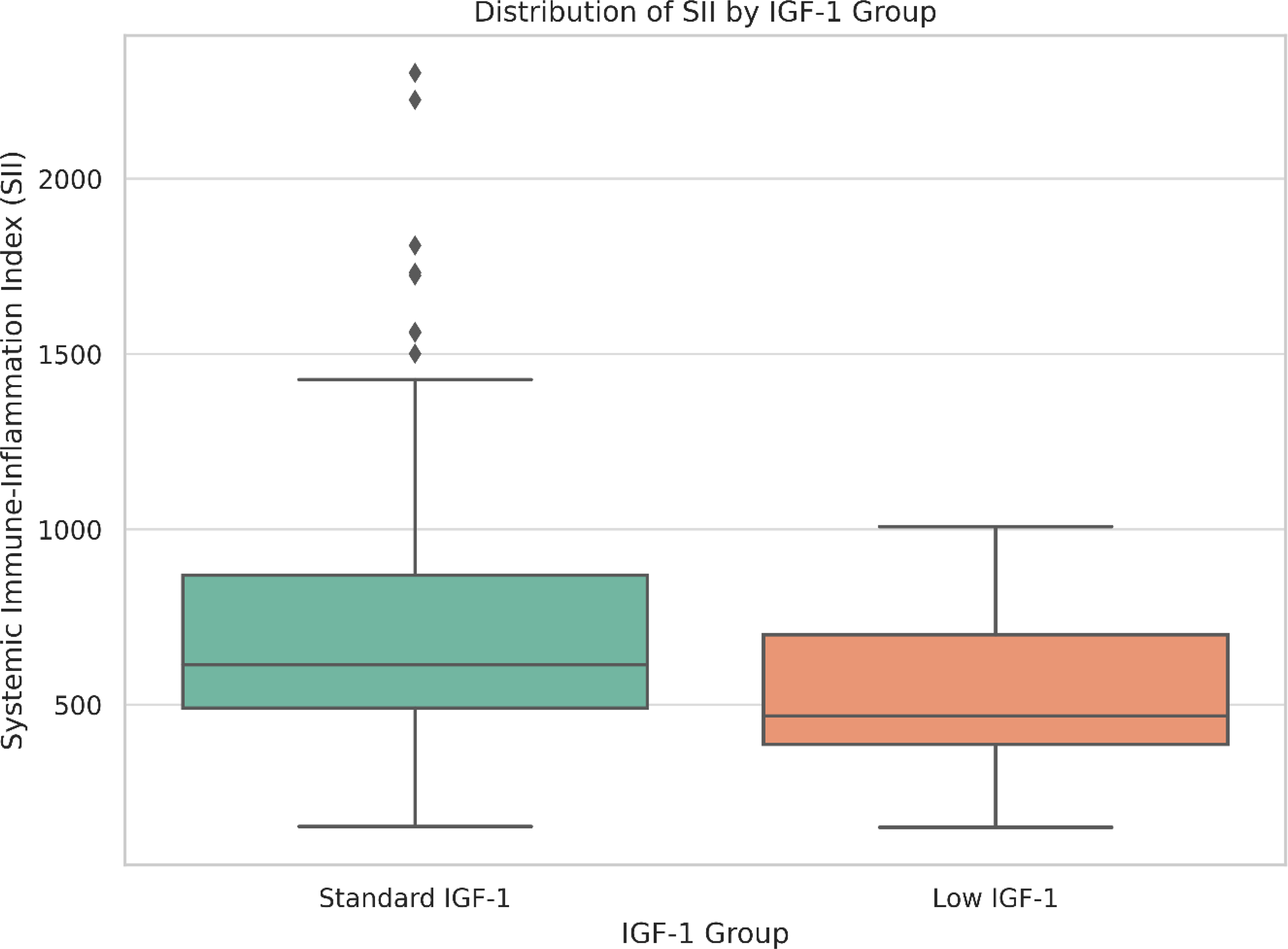
Comparison of SII between the low and standard IGF-1 groups. SII, systemic immune-inflammation index; IGF-1, insulin-like growth factor-1.
Correlation analyses revealed that the SII was positively correlated with systolic blood pressure (SBP), ALT, and insulin levels, while the SIAI was positively correlated with SBP. No significant correlation was found between IGF-1 SDS and any of the systemic inflammatory indices.
Figure 3 presents a heatmap illustrating the Spearman correlation coefficients between systemic inflammatory markers (SII, NLR, PLR, LMR, SIRI, and SIAI) and metabolic parameters (BMI, blood pressure, lipid profile, liver enzymes, insulin resistance indices). Blue and red indicate negative and positive correlations, respectively, with darker shades representing stronger correlations.
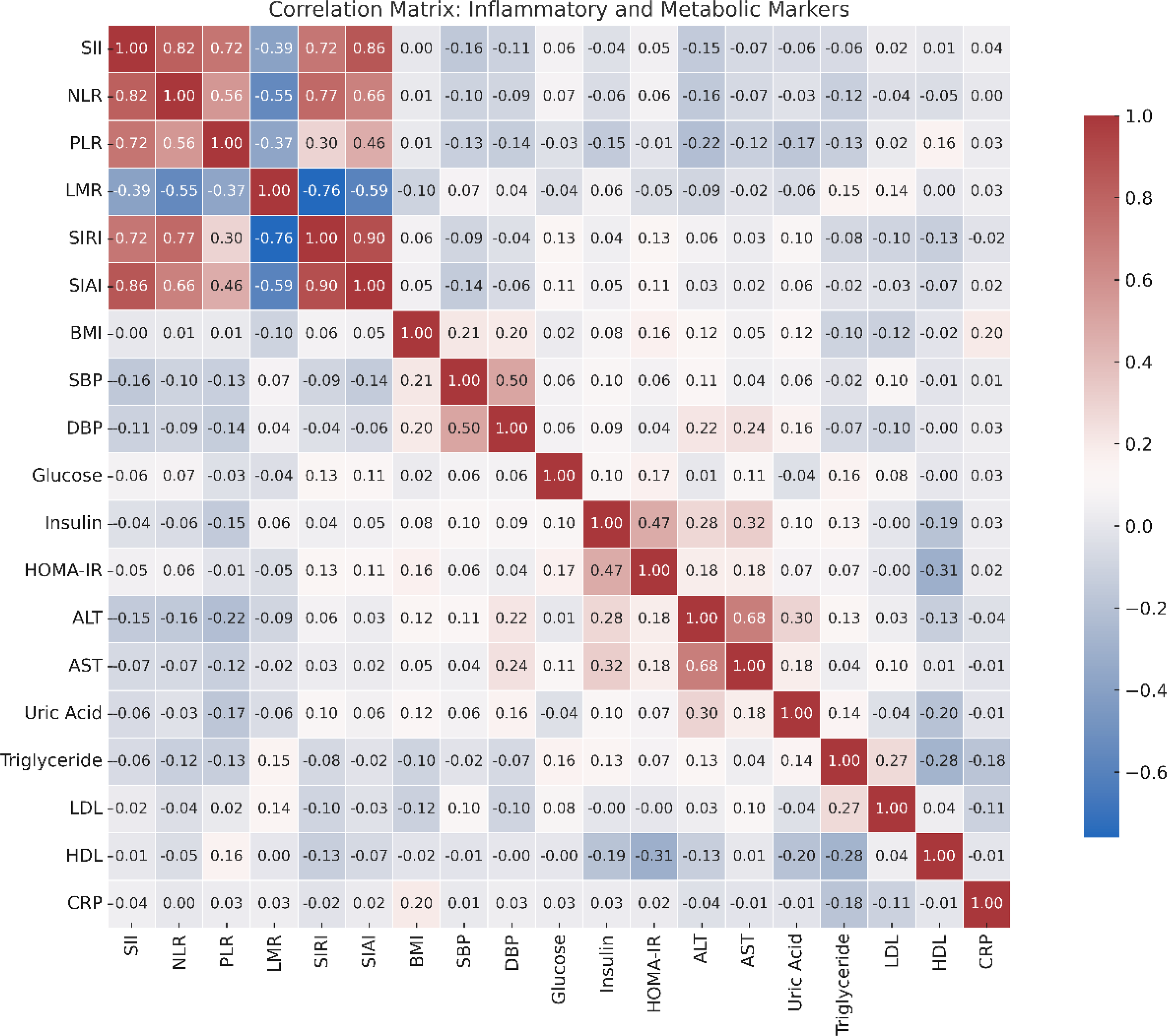
Spearman correlation heatmap showing associations between systemic immune-inflammatory markers and key metabolic parameters in the study cohort. Positive correlations are shown in red, and negative correlations are shown in red, negative in blue; darker shades represent stronger correlation coefficients. SII, systemic immune-inflammation index; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SIRI, systemic inflammation response index; SIAI, systemic inflammation aggregate index; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; AST, aspartate amnotransferase; ALT, alanine aminotransferase; LDL, low-density lipoprotein; HDL, high-density lipoprotein; CRP, C-reactive protein.
These findings suggest that lower IGF-1 levels in individuals with obesity are not associated with increased inflammation, as reflected by systemic inflammatory indices.
Discussion
This study is the first study to investigate the relationship between IGF-1 levels and systemic inflammatory markers in a well-defined cohort of patients with obesity. Our findings suggest that lower IGF-1 levels are not associated with increased levels of systemic inflammatory markers, including NLR, PLR, LMR, SII, SIRI, and SIAI. Specifically, NLR and SII were significantly higher in the standard IGF-1 group compared with the low IGF-1 group, whereas other inflammatory indices showed no significant differences between the groups.
Inflammation plays a central role in the pathogenesis of obesity. 29 Proinflammatory cytokines released by adipose tissue contribute to systemic inflammation. 13 However, not all individuals with obesity exhibit elevated cytokine levels.30–32 Some studies have reported that up to 23% of individuals with obesity demonstrate no signs of inflamed adipose tissue. 33 The mechanisms underlying this variability remain unclear. In addition to the increased secretion of proinflammatory mediators, obesity is associated with insulin and IGF-1 resistance, both of which contribute to metabolic and cardiovascular complications.34–36 Inflammatory processes may further exacerbate this resistance, amplifying the metabolic consequences of obesity.
Data on the association between IGF-1 and systemic immune-inflammatory markers are limited. In patients with acromegaly, IGF-1 was positively correlated with NLR and PLR, suggesting a link between IGF-1 and immune-inflammatory markers under GH excess. 37 In contrast, our study demonstrated that in individuals with obesity, IGF-1 levels were not significantly correlated with systemic inflammatory markers. While NLR and SII were significantly higher in the standard IGF-1 group than in the low IGF-1 group, other markers did not differ significantly between the groups. Although these differences reached statistical significance, their absolute magnitudes were relatively modest (NLR: 2.38 vs. 1.80; SII: 713 vs. 554) and remained within the expected physiological range for obesity-related low-grade inflammation. Although the absolute differences in NLR and SII were modest, their direction, being higher in the standard IGF-1 group contrary to the initial hypothesis, represents the main clinical and scientific relevance of these findings. Therefore, these variations are unlikely to be clinically meaningful in terms of immediate metabolic or cardiovascular risk stratification but may reflect subtle immunometabolic differences between individuals with varying IGF-1 levels.
The clinical importance of NLR as an inflammatory marker in obesity and metabolic syndrome is still controversial. Some studies have reported no association between NLR and obesity or metabolic syndrome severity, 38 while other studies have found elevated NLR levels in individuals with obesity and insulin resistance, as well as positive correlations with metabolic syndrome severity.21,39 In this study, NLR was significantly higher in the standard IGF-1 group compared with the low IGF-1 group, a paradoxical finding that may indicate a disconnect between IGF-1 and subclinical inflammation in obesity. This might indicate that NLR may be influenced by factors other than IGF-1 status, such as metabolic stress or hepatic injury, also supporting the heterogeneity of the inflammatory response in obesity.
The SII, which combines NLR and platelet count, has emerged as a useful marker of systemic inflammation. It has shown relevance in various clinical conditions, including sepsis, hepatic steatosis, ulcerative colitis,40–42 coronary artery disease, and cancer. 17 In obesity, SII has been positively associated with BMI, waist circumference, and visceral adiposity index, suggesting its utility as a surrogate marker of obesity-related inflammation.23,24 In line with prior findings, our analysis revealed novel associations between the SII and some metabolic parameters in obesity, specifically SBP, ALT, and insulin levels. These findings suggest that the SII not only reflects immune activation but also broader metabolic stress. This correlation with SBP is consistent with previous evidence linking low-grade inflammation to vascular dysfunction and hypertension in individuals with obesity. 43 The associations with insulin and ALT levels further implicate SII in insulin resistance and hepatic contributions to systemic inflammation, potentially through metabolic-associated fatty liver disease (MAFLD). Taken together, these findings underscore the multifaceted role of the SII as a composite marker for both immune and metabolic dysregulation in obesity. In addition, although not reaching statistical significance, a borderline trend toward a higher prevalence of hypertension was observed in the standard IGF-1 group compared with the low IGF-1 group (34.9% vs. 15.8%, p = 0.092). This finding is consistent with the observed positive association between SII and SBP and may reflect subtle immunometabolic differences that could become more evident in larger cohorts.
The observation that NLR and SII were significantly higher in the standard IGF-1 group may reflect the paradoxical nature of IGF-1 in obesity. Although low IGF-1 is generally considered a marker of metabolic dysfunction, chronic low-grade inflammation may persist even in individuals with preserved IGF-1 levels. 4 This suggests that IGF-1 does not exert an anti-inflammatory effect in individuals with obesity and elevated basal inflammation. Our data suggest that IGF-1 may not be a reliable surrogate marker of systemic inflammation in the context of obesity, despite its physiological roles in immune and metabolic regulation.
The finding of elevated CRP levels in the low IGF-1 group, despite lower NLR and SII, highlights the complex and compartmentalized nature of obesity-related inflammation. CRP is an acute-phase reactant synthesized in the liver, primarily reflecting hepatic-driven inflammation, which may occur independently of systemic leukocyte activation. In contrast, NLR and SII represent low-grade, cell-mediated inflammatory processes. Therefore, the discordant pattern of high CRP but low NLR/SII may suggest a predominance of hepatic inflammation, potentially linked to reduced IGF-1 synthesis and altered liver function, whereas higher NLR/SII in the standard IGF-1 group could reflect systemic immune activation. In this context, MAFLD may represent the most plausible upstream driver of hepatic inflammation and elevated CRP in the low IGF-1 group, given the liver-derived nature of IGF-1 and the well-established link between MAFLD and systemic acute-phase responses.
A potential explanation for the disparity between low IGF-1 levels and inflammation is hepatic dysfunction. IGF-1 is primarily synthesized in the liver, and diminished hepatic function, as indicated by elevated liver enzymes or hepatic steatosis, may lead to decreased circulating IGF-1, independent of systemic inflammation. In our cohort, patients with low IGF-1 levels demonstrated stable levels of inflammatory markers, corroborating this mechanism. In addition, the positive correlation between SII and ALT in our study suggests a hepatic contribution to systemic inflammation, consistent with the hypothesis that liver dysfunction influences both IGF-1 production and inflammatory burden through different mechanisms.
Moreover, the absence of elevated inflammatory markers in the low IGF-1 group may reflect a metabolically healthy obese phenotype. Previous studies have demonstrated that a subset of individuals with obesity do not exhibit typical inflammatory or metabolic dysfunction.44,45 This heterogeneity may explain the lack of correlation between low IGF-1 and systemic inflammation in our study. These findings are consistent with those of previous studies showing that subjects with metabolically healthy obesity have lower levels of inflammatory markers than those with metabolically unhealthy obesity. 46
Interestingly, despite lower levels of NLR and SII in the low IGF-1 group, CRP levels were significantly higher compared with the standard IGF-1 group. This apparent discrepancy may reflect differences in the biological nature and kinetics of CRP versus composite hematological inflammation markers. CRP is an acute-phase reactant primarily synthesized in the liver and can be influenced by hepatic function, subclinical infections, or comorbidities unrelated to obesity-associated immune activation. Meanwhile, markers like NLR and SII are combined values of leukocytes with platelets that can represent chronic low-grade inflammation rather than acute-phase responses. A different possibility is that obesity-related IGF-1 deficiency could be associated with low-grade hepatic steatosis or inflammation, increasing CRP without parallel increments in leukocyte-based inflammatory markers. This suggests that different aspects of the inflammatory process diverge during obesity, and no single inflammatory biomarker can reflect, in full, the immunometabolism state.
This study had several limitations. Foremost, its retrospective and cross-sectional nature did not allow causal inferences to be drawn. Second, direct measurements of proinflammatory cytokines were not assayed, and these may have augmented our understanding of systemic inflammation. Third, hepatic steatosis and insulin resistance were not determined by imaging or gold-standard methods for quantifying these parameters (hyperinsulinemic–euglycemic clamp studies). Another limitation is the relatively small sample size of the low IGF-1 group (n = 19, 7.6% of the total cohort), which may have reduced the statistical power of subgroup analyses and precluded the detection of more subtle differences or associations. Therefore, the absence of significant differences in metabolic comorbidities between groups should be interpreted with caution, as these findings may reflect limited sample size rather than true equivalence. However, the current study improves upon others by including an overall bigger trial population and using standardized IGF-1 SDS, providing more internal validity and comparability. Further work to address these limitations is crucial for replicating and validating our results.
In conclusion, our study demonstrates that low IGF-1 levels in individuals with obesity are not associated with increased systemic immune-inflammatory markers or a higher prevalence of metabolic comorbidities such as diabetes, dyslipidemia, or hypertension. While IGF-1 is often considered a metabolic health indicator, our findings suggest that low circulating IGF-1 in the context of obesity does not necessarily indicate greater inflammation or metabolic deterioration. Therefore, relying solely on IGF-1 to assess metabolic or inflammatory risk in obesity may be misleading. Adding systemic immune-inflammatory indices such as SII to IGF-1 may provide a more comprehensive assessment of metabolic risk and guide personalized management strategies. Future prospective studies including liver imaging and cytokine profiling are needed to elucidate the complex interaction between IGF-1, inflammation, and metabolic dysfunction in obesity.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Authors’ Contributions
All authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by the authors. The first draft of the article was written by G.R.B., and all authors reviewed commented on previous versions. M.K. contributed to the review and editing of the article. All authors have read and approved the final version of the article.
Footnotes
Acknowledgments
The authors thank the participants and the staff of the Department of Endocrinology and Metabolism at Ankara Bilkent City Hospital for their support during data collection.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.