
Abstract
For six decades, human spaceflight has largely been shaped by stringent medical and operational eligibility criteria. However, the commercialization of low Earth orbit and the broader ethos of the New Space era invite a reexamination of who space systems are designed for. This Perspective argues that disability inclusion in commercial spaceflight should be treated not only as a matter of equity but also as a driver of safer and more adaptable design. Drawing on the Social Model of Disability and the United Nations Sustainable Development Goals, we suggest that in some intravehicular microgravity contexts, certain terrestrial impairments may become less limiting, while also emphasizing that launch, landing, emergency egress, and mission duration remain major constraints. We further argue that design features developed for users at the margins—such as multisensory cues, simplified controls, and adaptable interfaces—can produce broader safety and usability benefits across commercial crews. This is not an argument that all disabilities can already be accommodated across all mission profiles. Rather, it is a case for staged, mission-specific inclusion under clearly defined safety conditions. Framed in this way, disability becomes a serious design lens through which commercial spaceflight can broaden participation, strengthen resilience, and align more credibly with the principle that space should benefit all humanity.
Keywords
INTRODUCTION: THE END OF THE “PERFECT BODY”
Since the dawn of the Space Age, astronaut selection has been shaped by stringent medical and operational eligibility standards, reflecting narrow safety margins and severe constraints in early human spaceflight. In practice, these constraints favored bodies that could meet demanding physiological and functional requirements, while many nontraditional profiles were treated as higher risk or operationally incompatible.
However, early signals of this shift are already visible. The AstroAccess initiative has used parabolic flight to test accessibility concepts in microgravity with a crew of disability ambassadors, including participants with mobility, vision, and hearing disabilities. 1 The successful orbital mission of the all-civilian Inspiration4 crew—alongside subsequent multiomics and physiological analyses reported by Mason et al. and Jones et al.—has begun to establish empirical baselines for how civilian bodies respond and adapt to spaceflight.2,3 In parallel, the European Space Agency’s Fly! initiative has begun to examine, in a staged and operationally specific way, what technical, medical, and procedural changes may be required to support disabled spaceflight. 4 Rather than asking simply, “Can they fly?” the more useful question is what kinds of disabled participation may be feasible under which mission conditions. As humanity expands into the cosmos, the question arises whether future architectures will replicate terrestrial exclusions or embody the “Leave No One Behind” principle of the United Nations Sustainable Development Goals (SDGs).
This Perspective argues for the latter, reframing disability not as a liability but as a catalyst for better engineering and a more sustainable human presence in space. This Perspective does not argue that all disabilities can presently be accommodated across all commercial spaceflight profiles at the current state of the art. Rather, it argues for a staged, mission-specific approach to inclusion, one that distinguishes among suborbital tourism, short-duration orbital missions, and longer-duration station or research roles. In that framing, accessibility must be evaluated in relation to mission duration, vehicle architecture, operational task demands, and emergency procedures, rather than treated as a single abstract question of whether spaceflight is “inclusive” or “noninclusive.” 4
These distinctions matter in practice. A suborbital passenger flight lasting only minutes does not raise the same accessibility questions as a multiday orbital mission, and neither is equivalent to a longer-duration station or research role. For that reason, any serious discussion of disability inclusion in commercial spaceflight must remain mission-, vehicle-, and task-specific. 5
THEORETICAL FRAMEWORK: THE SOCIAL MODEL IN ORBIT
To understand the potential of parastronauts, a pivot from the Medical Model to the Social Model of disability is required. As Shakespeare articulates, the Medical Model locates the “problem” in the individual’s body, seeking to fix or exclude the person. 6 This has been the basis of aerospace medical certification to date. In contrast, the Social Model locates the “problem” in the environment—such as stairs without ramps—and seeks to redesign the environment to accommodate the user.
In the context of spaceflight, the Social Model helps shift attention from bodies alone to bodies-in-environments. In some intravehicular microgravity contexts, the inability to walk may become less limiting than it is on Earth, and upper-body propulsion, hand-based translation, and spatial awareness are already central to how astronauts move through spacecraft. Recent studies on upper extremity health in spaceflight underscore how upper-body dominant activity is routine in orbit. 7 This raises the possibility that some wheelchair users on Earth may bring strengths that are operationally relevant for intravehicular activity. Edgerton et al. also highlighted how spaceflight research has informed the understanding of the plasticity of spinal cord injury. 8 At the same time, disability does not disappear in space. Functional barriers may persist—or reappear in different forms—during launch, landing, suited operations, emergency response, and postflight recovery. The more accurate claim is not that microgravity eliminates disability, but that it can reconfigure which abilities matter, for whom, and in which mission phase. In that sense, the space environment makes visible a broader point long emphasized in disability studies: Limitation is not only a property of the body but also of the system within which the body is expected to function. Anthropometric studies confirm that body dimensions shift in space even for healthy astronauts due to spinal elongation and fluid shifts. 9 This evidence supports the argument that flexible, adjustable design is a requirement for everyone, regardless of disability status.
THE “CURB-CUT EFFECT”: INNOVATION FOR ALL
A common critique of inclusive design is cost. Why engineer a spacecraft for a minority? Part of the answer lies in the “Curb-Cut Effect”—the phenomenon whereby features designed for people with disabilities often end up benefiting a much wider population, such as parents with strollers, travelers with luggage, or delivery workers. 10 In space, this logic becomes especially relevant because the environment itself can degrade strength, orientation, dexterity, and sensory processing. As illustrated in Figure 1, design interventions targeted at parastronauts can create systemic redundancies that improve safety and usability for the wider crew. This does not mean that accessibility is cost-free. Incorporating accessibility into spacecraft, suits, onboard systems, hygiene systems, and emergency procedures may increase upfront human factors and human–systems integration demands. However, when accessibility is considered early, rather than retrofitted late, it may also reduce redesign burden, improve usability, lower training demands, and strengthen safety margins for a broader range of users. In that sense, inclusive design is not only a matter of accommodation but also of sound systems engineering. 11
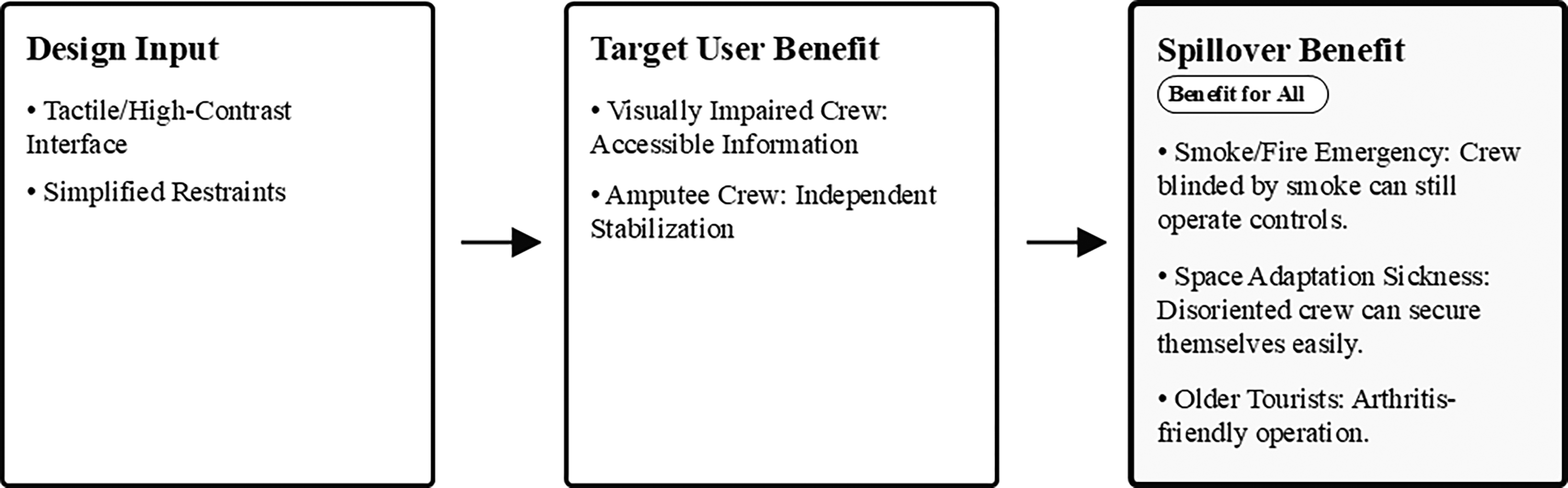
The “Curb-Cut Effect” in commercial spaceflight. Design interventions targeted at parastronauts (e.g., simplified restraints, multisensory interfaces) create systemic redundancies that enhance safety and usability for all crew members, including older space tourists and professional astronauts during off-nominal scenarios (e.g., smoke in the cabin or spatial disorientation). Inclusive design acts as a force multiplier for mission resilience.
Visual and Tactile Cues
Consider a spacecraft interface designed for a visually impaired crew member. It would likely rely on high-contrast displays, audio readouts, and haptic feedback suits. While critical for the disabled user, these features become lifesavers for all crew members during a high-stress emergency, such as smoke in the cabin. When visual obscuration blinds a “healthy” astronaut, or when sensory overload degrades cognitive processing, the multisensory redundancy ensures that critical information is still received.
Simplified Ergonomics
A toilet or sleeping restraint designed to be operable by a person with limited dexterity (e.g., severe arthritis or upper-limb amputation) is inherently easier to use for everyone. This includes an older space tourist with reduced grip strength or a healthy astronaut suffering from debilitating space adaptation sickness (SAS) who cannot orient themselves. Flexible, adjustable design—a core tenet of Universal Design 12 —is therefore a requirement for everyone, not just parastronauts. Blue et al. (2023) demonstrated that laypersons with varied physiological baselines can tolerate simulated spaceflight forces with appropriate training. 13 However, their ability to perform tasks under G-load or in microgravity is significantly enhanced if the interface does not require “perfect” physiology. Gleaton et al. emphasize that involving people with disabilities in emergency planning improves response protocols for the entire population. 14 Thus, by designing for the margins, New Space companies create systems that are more robust, intuitive, and safe for the entire user base. Inclusion becomes a quality assurance strategy.
ALIGNMENT WITH SDGS: A MORAL AND BUSINESS IMPERATIVE
The commercial space industry does not exist in a vacuum; it is part of the global economy and society. Aligning with the SDGs is crucial for the sector’s long-term legitimacy and social license to operate.
SDG 10 (Reduced Inequalities)
As argued by Aganaba et al., space exploration must not be left to a few powerful nations or elites. 15 Opening the frontier to people with disabilities directly targets the reduction of inequality. It dismantles the ableist narrative that space is only for the “physically elite.”
SDG 8 (Decent Work and Economic Growth)
People with disabilities constitute a substantial share of the global population and represent an often-overlooked pool of potential customers, employees, and collaborators. By excluding this demographic, the space tourism industry narrows both its market and its talent base. Integrating this demographic can support economic growth while also widening the range of expertise brought into the sector.
SDG 9 (Industry, Innovation, and Infrastructure)
Technologies developed in support of more accessible spaceflight could also generate terrestrial benefits. More adaptable prosthetic interfaces, accessible control systems, and stronger telemedicine protocols may have downstream relevance for rehabilitation, assistive technology, and remote care on Earth. Charting a “moral future” for space exploration requires moving beyond technical feasibility to ethical desirability, 16 and prioritizing the SDGs is the clearest path to that future. 17
NURSING AND MEDICAL CONSIDERATIONS: THE ROLE OF THE ENABLER
As the demographics of space travelers shift, the role of the flight nurse or medical officer must also evolve from a guardian of physiology to an “Environmental Enabler.” Recent data support the safety of this evolution. King and Blue demonstrated that individuals with diabetes mellitus can tolerate centrifuge-simulated spaceflight, 18 and Fernandez et al. showed similar tolerance in patients with prior cardiac surgery. 19 These findings suggest that well-managed chronic conditions are not barriers to flight.
However, specific operational challenges remain that require nursing innovation.
Skin Integrity and Prosthetics
For amputees, fluid shifts in microgravity present a dynamic challenge. As fluid migrates cephalad, the volume of the residual limb (stump) can fluctuate significantly, causing prosthetics to fit poorly or creating friction points. Dunn et al. reviewed dermatologic manifestations in spaceflight, noting the fragility of skin in microgravity. 20 Consequently, nursing protocols must focus on rigorous skin monitoring and the development of adjustable, breathable socket interfaces (e.g., air-bladder systems). Furthermore, the necessity of the prosthesis itself must be evaluated; in zero-G, a leg prosthesis may be dead weight for mobility but critical for restraint during launch and landing. Protocols for “donning and doffing” in a confined space must be established.
Neuro-Vestibular Adaptation
Crew members with sensory impairments may require novel orientation strategies. Panic et al. highlight the otolaryngological considerations for commercial spaceflight, noting that neuro-vestibular adaptation is a universal challenge. 21 For a visually impaired parastronaut, or one with compromised vestibular function, “Sensory Substitution” technologies become vital. Tactile vests that vibrate to indicate “down” or auditory spatial cues can replace lost sensory input. Nurses must be trained to support crew members through the disorientation of SAS using these alternative sensory modalities, rather than relying solely on pharmacological management.
Continence and Catheterization
For crew members with spinal cord injuries or neurogenic bladders, self-catheterization in zero-G presents unique fluid dynamics challenges. In the absence of gravity, urine does not flow downwards into a bag; it requires active suction or a closed-system catheter to prevent droplet release. This is not merely a hygiene issue but a safety-critical one; floating fluids are a biohazard and an electrical risk. Nurses must codesign procedures and privacy spaces that allow for dignified, autonomous self-care. The habitat’s waste management system must be compatible with catheter disposal, integrating these needs into the Environmental Control and Life Support System (ECLSS) design phase.
Emergency Egress
The most critical operational and medical consideration is emergency response. Launch-pad abort, tower descent, transfer into escape baskets or rescue vehicles, post-landing extraction, and evacuation under smoke, fire, or water conditions may each impose different functional requirements. For that reason, accessibility cannot be assessed in the abstract; it must be evaluated against a specific vehicle, mission phase, crew role, and rescue concept. 14 Standardized buddy systems, simplified latch mechanisms, multisensory cues, and assisted egress procedures may improve safety for disabled and nondisabled crew alike, but some mission profiles will remain limited unless safe assisted or independent egress can be demonstrated through testing, procedures, and training. 22
CHALLENGES AND LIMITATIONS
While the moral and business cases for inclusion are strong, several major constraints remain.
First, mission profile matters. A suborbital passenger flight lasting only minutes does not raise the same accessibility questions as a multiday orbital mission, and neither is equivalent to a longer-duration station or research role. Duration changes the operational threshold for medical support, hygiene, sleep, emergency response, and crew task performance. For that reason, disabled participation in commercial spaceflight should be discussed in mission-specific rather than universal terms. 5
Second, the launch, reentry, and emergency environment remain a bottleneck. While intravehicular microgravity may reduce some terrestrial barriers, the hypergravity of launch and reentry, together with time-critical evacuation requirements, may pose substantial risk for individuals with spinal instrumentation, osteopenia, specific cardiovascular conditions, or severe mobility limitations. The data from Blue et al. are promising, 13 but further research is needed to define operational limits for specific clinical and functional profiles. 22
Third, legacy architecture poses a financial and design barrier. Retrofitting existing capsules (e.g., Soyuz, Dragon) that were designed for a narrow anthropometric and functional range is expensive and engineering-intensive. Meaningful progress will be easier when accessibility is considered earlier in vehicle, habitat, and procedure design, rather than added after core systems have already been fixed in place. 11
Fourth, the long-term physiology remains incompletely understood. Data on how specific disabilities interact with spaceflight-associated hazards remain scarce. Does altered circulation after spinal cord injury affect neuro-ocular risk? Does an amputee’s residual limb experience different patterns of skin breakdown or bone loss over time? These questions argue for a staged “crawl, walk, run” approach to evidence generation, beginning with analog environments, parabolic flights, and carefully selected short-duration missions before contemplating longer-duration or higher-risk exploration profiles.
Fifth, scope must be defined carefully. This article does not assume that all disability profiles are currently compatible with all vehicles, mission durations, or operational roles. A more realistic path forward is staged and evidence-based: selected suborbital participation in carefully defined cases, short-duration orbital inclusion where safety requirements can be met, and only then broader consideration of longer-duration or operational crewed roles. The goal is not universal accommodation in the abstract, but credible expansion of access under clearly defined safety conditions.
Ethically, this also matters. Inclusion in commercial spaceflight should mean more than symbolic representation; it requires proportionality between risk and benefit, meaningful informed consent, and avoidance of invitations unsupported by engineering, medical planning, or operational validation. In that sense, the most defensible path is neither blanket exclusion nor performative inclusion but evidence-based expansion of access. 23
CONCLUSION: THE RIGHT TO FLOAT
Commercial spaceflight offers a genuine opportunity to rethink who space systems are designed for. But that opportunity should not be framed as a claim that every disability can already be accommodated across every mission profile. The more useful question is which forms of inclusion can be pursued safely, under which vehicle and mission conditions, and through which design, training, and operational adjustments. Framed in that way, the “Right to Float” is not a slogan about ignoring constraints. It is an argument for taking disability seriously as a design lens. Doing so can widen participation, improve usability and resilience, and align the commercial sector more credibly with the principle that space should benefit the full spectrum of humanity.
AUTHORS’ CONTRIBUTIONS
K.K.: Conceptualization, methodology, writing—original draft, writing—review and editing, and project administration. Y.I.: Conceptualization, validation, writing—review and editing, and formal analysis (disability studies and universal design frameworks). All authors have read and agreed to the published version of the article.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.