
Abstract
The role of the medical science liaison (MSL) within the industry is evolving yet well established. Reports of MSL activities have uniformly been from the view of the pharmaceutical company. This report describes the desired activities from the perspective of the health care professional (HCP) using a blinded, 2-phase survey method. The first phase was an online quantitative survey conducted among key opinion leaders (KOLs) in the academic and practicing fields for diabetes research and treatment who have met with an Amylin MSL in the past 6 months. The second phase consisted of 1-on-1 telephone interviews with a subset of participants from phase 1 to better understand what KOLs want and need from MSLs, to explore how MSLs can add value to their interaction with KOLs, and to understand how Amylin MSLs are performing. The research evaluated a number of questions, including how KOLs view the MSLs and the value they bring to the KOLs. There were 116 KOLs who completed the online survey and who were considered qualified completers. Diabetes MSLs are a valuable resource to KOLs. They must first and foremost present themselves as ethical and unbiased. They help KOLs stay up to date on industry information and happenings, saving time for the busy KOL. The KOL’s key information needs are around pipeline and research. They would like to get to know their MSLs better, to understand their background and experience, and to see them more often.
Introduction
Within the pharmaceutical industry, medical science liaison (MSL) groups have evolved since their origination in 1967, 1 and there has been a steady increase in the number of these groups within the past decade. 2 Medical science liaisons are therapeutic specialists with advanced training and degrees in life sciences and are traditionally employed to educate health care professionals (HCPs) on a company’s therapeutic capability in a given geography at a given stage of a product’s life cycle. However, the actual activities of the MSL when interacting with an HCP are varied, evolving, and highly dependent on the individual company. Surveys of MSL managers and field-based MSLs have assessed trends across the pharmaceutical industry in defining and managing MSLs, identifying tools they employ, and understanding new or nontraditional roles they have assumed in recent years. 3–6 These surveys provide great insight into the role of the contemporary MSL from the perspective of the MSL or MSL manager. However, we are not aware of published data on the expectations that HCPs have for these growing ranks of MSLs from the HCP perspective. This would imply that the selection of individuals to fill the role of MSLs, their day-to-day field activities, and the tools they employ when interacting with HCPs are initiated without really knowing what the customer wants. This lack of published information on customer needs as well as a desire to objectively assess the performance of our own field-based medical liaison team led us to examine the HCP-MSL relationship from the HCP perspective using a blinded survey method. In this report, we looked specifically at a subset of HCPs referred to as key opinion leaders (KOLs), who are viewed by many as the therapeutic trendsetters within diabetes. The comments we received from KOL surveys and interviews included many that ultimately helped us to enhance our field medical team and showcase its impact on customers to corporate management.
The objective of this survey was to assess the expectations of HCPs for their MSLs in the diabetes therapeutic area. An additional objective was to determine the effectiveness of the Amylin Pharmaceuticals (San Diego, California) MSL field medical team in meeting these expectations; however, these results are not reported here.
In 2008, we conducted a similar blinded survey that has not been published. For reference and trending purposes, we have provided responses to those questions in the present survey in which corresponding responses are available from 2008.
Methods
We explored the current relationship between Amylin MSLs and KOLs involved in diabetes research and treatment and assessed areas for improvement by conducting a blinded survey using a third-party vendor. Harris Interactive (Rochester, New York) was commissioned to conduct a 2-phased study to investigate these relationships. The first phase was an online quantitative survey conducted among academic and practicing KOLs in diabetes research and treatment who have met with an Amylin MSL in the past 6 months. The second phase consisted of 1-on-1 telephone interviews with a subset of participants from phase 1 to better understand what KOLs want and need from MSLs, to explore how MSLs can add value to their interaction with KOLs, and to understand how Amylin MSLs are performing. The phase 1 survey was blinded to the KOL participant. Questions were asked in such a way as to mask the identity of the sponsor company (Amylin). For questions that included a list of companies from which the KOL was to select, the order of the companies was random for each question so as to minimize selection bias.
The research evaluated a number of questions including how KOLs view the MSL and the value that the MSL brings to the KOL. The survey was also designed to assess how well Amylin MSLs performed against other company MSLs in the same therapeutic space. While the Amylin MSL was viewed as a most valuable asset in terms of information sharing, the specific results of these questions will not be addressed in this report.
The phase 1 online survey was administered by Harris Interactive from June 24, 2011, to August 9, 2011. The KOLs were recruited from a target list provided by Amylin. The list included 737 academic and practicing KOLs who are targeted by Amylin MSLs. The KOLs were emailed an invitation if an email address was available. The Harris Interactive Physician Panel was used to supplement either those KOLs with no email or email bounce backs from the target list. Qualified respondents who were academic or practicing KOLs were provided with a modest honorarium. An additional bonus was offered to any academic KOLs who participated in the survey between August 2, 2011, and August 9, 2011, due to an initial low response rate.
Academic KOLs were defined as physicians who (1) have a primary practice setting in an academic teaching institution, (2) have met with an Amylin MSL in the past 6 months, and (3) are recruited from a targeted list provided by Amylin. Practicing KOLs were defined as physicians who (1) spend 50% or more of their time in clinical practice, (2) dedicate time in a primary practice setting that is not an academic teaching institution, (3) have met with an Amylin MSL in the past 6 months, and (4) are recruited from a targeted list provided by Amylin.
There was no weighting applied to the final data. While statistical significance was tested at the 95% confidence interval for most responses, these data are omitted from this report.
The phase 2 survey was a live, 1-on-1 telephone interview of randomly selected phase 1 participants who were qualified completers and also agreed to take part in phase 2. Interviews were conducted between July 18, 2011, and July 25, 2011. Each interview lasted approximately 45 minutes. A total of 10 telephone interviews among 5 academic KOLs and 5 practicing KOLs were conducted.
Results
There were 116 KOLs (29 academic KOLs and 87 practicing KOLs) who completed the online survey and were considered qualified completers. Results from key questions obtained in the phase 1 quantitative survey are provided in Figures 1 through 4. Where available, results from our unpublished 2008 survey of diabetes KOLs (27 academic KOLs and 82 practicing KOLs) are shown as reference for trending purposes. Because the scale and attributes for the question shown in Figure 4 were changed in 2011, we have omitted reference data for 2008.
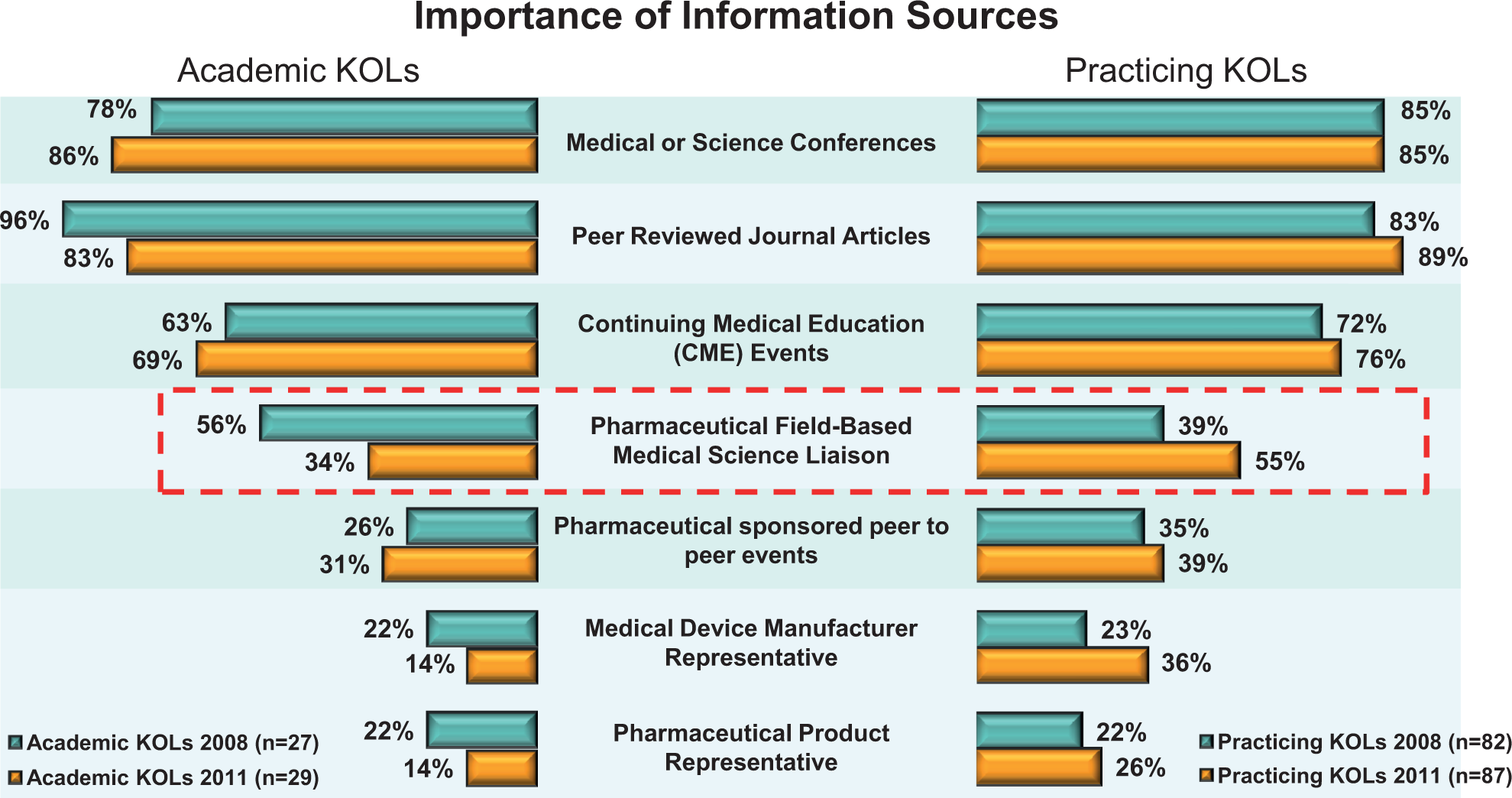
Responses to the question “Thinking about how you acquire knowledge that is useful in your practice, please rate the importance of the following information sources.”
Key results from both the phase 1 and phase 2 surveys are as follows:
The MSLs are viewed as important to KOLs because they provide current education to the KOL on a wide range of information, provide networking opportunities, and can engage in intellectual conversations.
The KOL’s perception of the MSL as being ethical is highly important in the KOL’s mind.
The “best” MSLs are aware of emerging products, are responsive, are reliable, and have a long-term relationship with the KOL.
For academic KOLs, additional important attributes for an MSL were the ability to answer unsolicited questions by the following: – providing unbiased product comparisons, – addressing safety issues, and – providing value at every meeting.
For practicing KOLs, top attributes were the ability to answer unsolicited questions by the following: – knowledge of the disease state, – addressing efficacy issues, and – being up to date on diabetes research trends.
Discussion
One issue we wanted to resolve at the outset was the value of the MSL relative to other information sources that the KOL uses or has access to. Figure 1 shows the results of the question “Thinking about how you acquire knowledge that is useful in your practice, please rate the importance of the following information sources.” As expected, sources that are considered peer driven such as journals and conferences were seen as the most important sources of information. The MSL was rated as a first or second option of importance by over half of practicing KOLs and about a third of academic KOLs. As shown as boxed text in Figure 1, this was almost a complete reversal in response from our 2008 assessment in which academic KOLs had viewed MSLs as more useful in acquiring knowledge than did practicing KOLs. The gratifying aspect was that the KOL in general viewed the MSL as a credible resource of information. The MSL was rated higher than industry-sponsored promotional programs that are given by a physician peer as the speaker.
The responses to the question “Which of the following services do you typically receive from diabetes MSLs/MLs?” are shown in Figure 2. This speaks directly to the issue of the information that the MSL provides that the MSL believes is of value. As one might expect, the most common response was “product-specific education.”
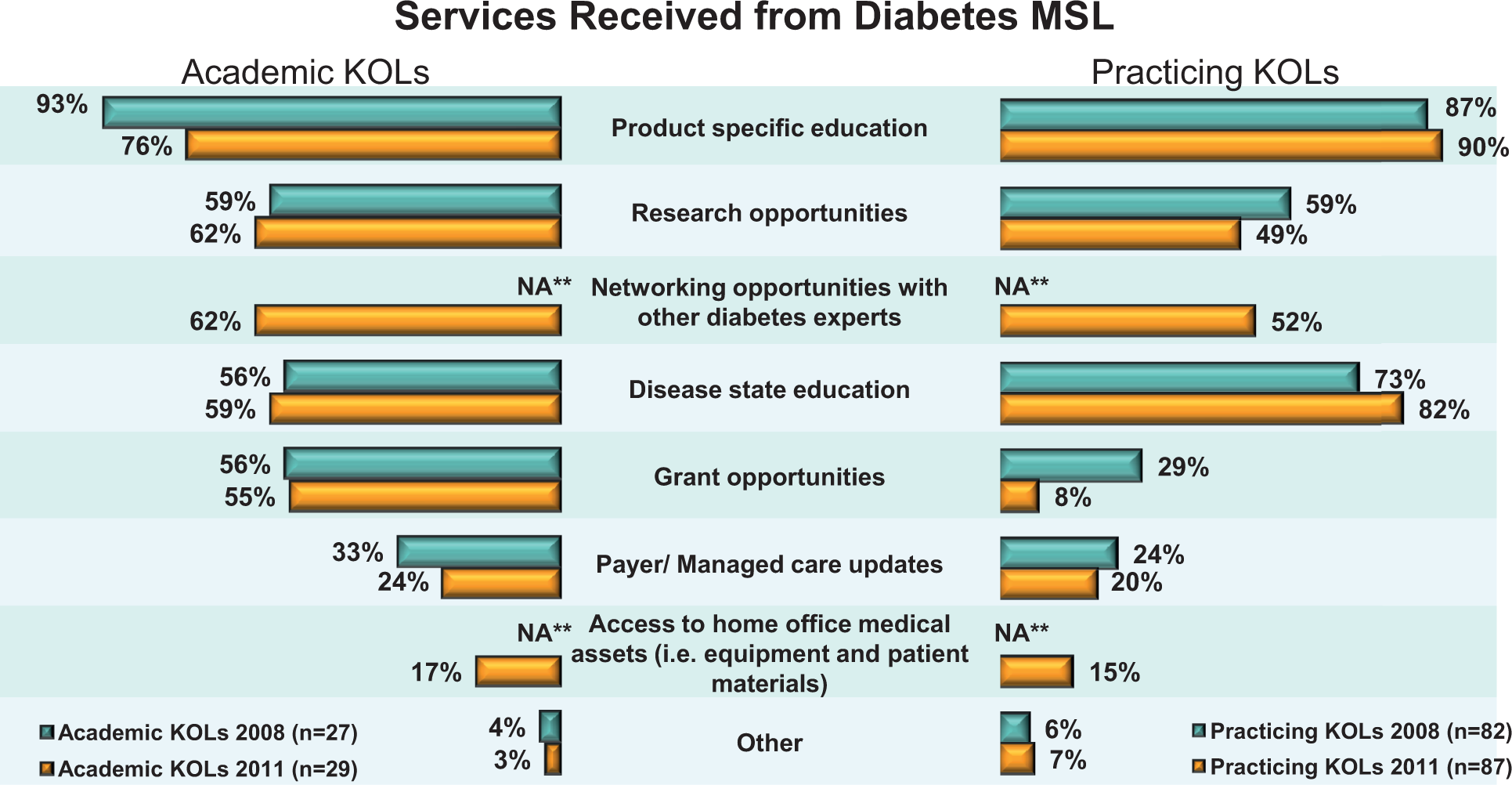
Responses to the question “Which of the following services do you typically receive from diabetes MSLs/MLs? Please select all that apply.” **NA, new attribute in 2011.
In contrast, Figure 3 shows the responses to the question “What type of information or services do you expect to receive from an MSL/ML for diabetes?” The responses show that current studies, latest research information, and new/pipeline product discussions are all top of mind for the KOL. The phase 2 interviews added further color to this response in that KOLs are not necessarily looking for the MSL to provide an update only on their company’s research and pipeline. Rather, the KOL is really looking for an intellectual discussion about the pipeline in general that would include information about all products in the area of interest. This expectation creates both an opportunity and also a degree of danger to the MSL. First, it creates the opportunity of adding tremendous value to the KOL to be able to provide a wide assortment of information to meet the KOL’s need: the added opportunity to allow the MSLs to not only be well versed in their own company’s development but to allow the MSL to be the expert to some extent for all compounds in the area of interest. The danger is that it puts the MSL potentially at risk for discussing issues for which data may be incomplete. Likewise, one of the key findings from the survey was the KOL’s desire to have the MSL act in an unbiased and ethical manner. Again, the phase 2 data put a fine point on this in which the KOLs surveyed were clear that they did not like to hear an MSL “bash” another company’s products. The line between offering fair and balanced information and offering a perspective on how therapeutics relate to each other in terms of efficacy and safety can be difficult.
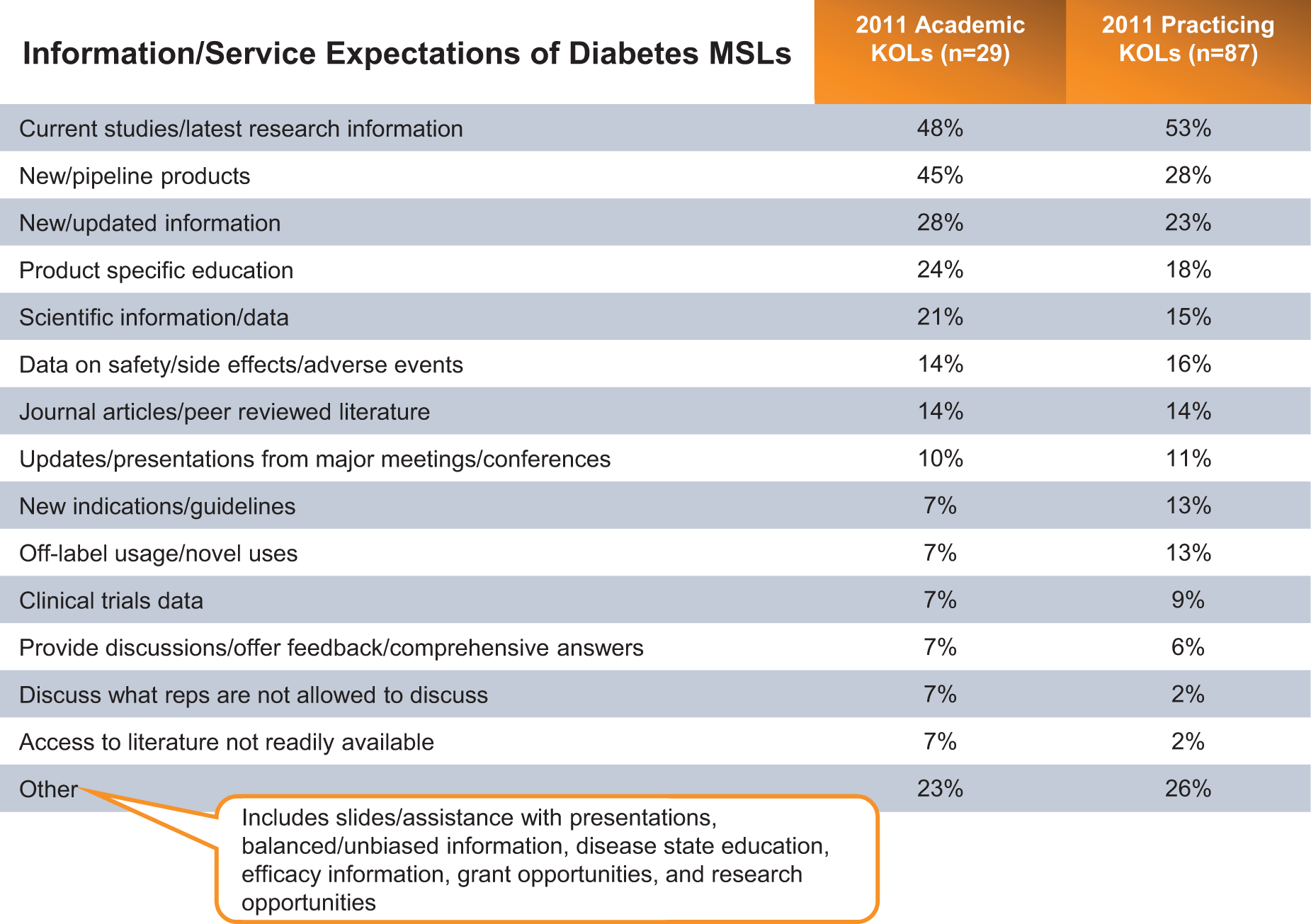
Responses to the question “What type of information or services do you expect to receive from an MSL/ML for diabetes?”
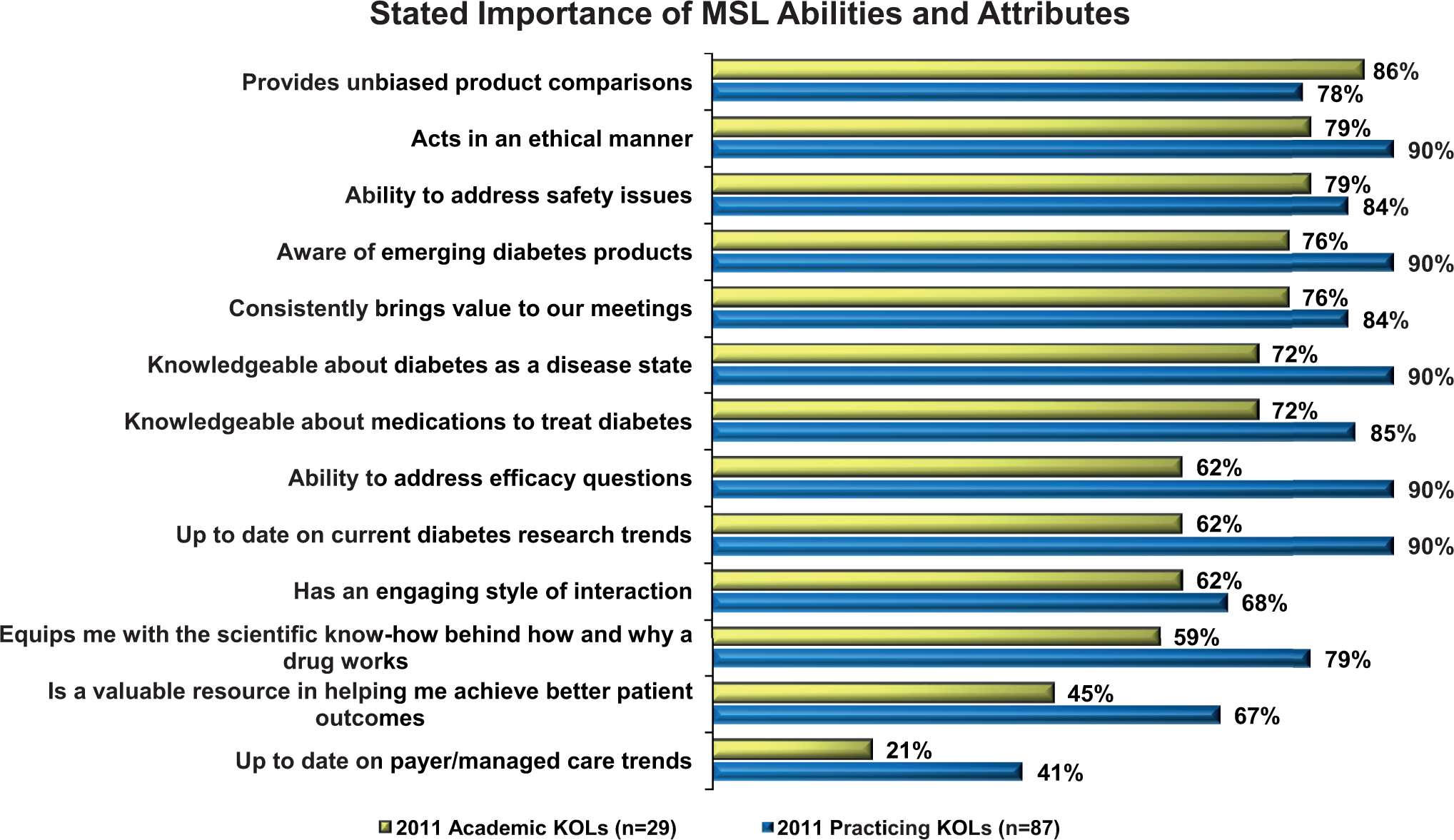
Responses to the question “Indicate how important the following MSL abilities and attributes are to you and your practice.”
The KOL responses to the question “Indicate how important the following MSL abilities and attributes are to you and your practice” are shown in Figure 4. The KOLs ranked receiving unbiased product comparisons and acting in an ethical manner as highly important attributes for their MSLs in Figure 4.
As a result of their specialized role, KOLs state that the MSL is a very important resource for their practice. When asked, the MSL can inform KOLs with up-to-date information in the diabetes field overall, not simply the MSL’s products and company. In response to unsolicited questions, the MSLs can provide a wealth of information and resources such as presentations, slides, abstracts, and other information from major conferences or congresses, such as the American Diabetes Association.
The MSLs can discuss conceptually the latest research being conducted by their company. This information exchange may be limited due to the lack of public disclosure, but even then, the level of interaction or discussion is most often at a higher informational or educational level than a marketing or sales approach typically will be.
The MSL is seen as a “time saver” by many KOLs, as the MSL can ease the KOL burden of needing to constantly “stay on top” of all the events and happenings in their field. The MSLs attend conferences, conduct literature searches, and then provide KOLs with a summary of information most relevant to their practice upon request. More rural KOLs (not attached to a major academic medical center), in particular, report more difficulty in staying up to date on information and in attending conferences. They especially note the importance of the MSL as a resource for information and updates from conferences.
The MSLs act as a bridge with other physicians and with their company. The KOLs value the networking opportunities with other physicians created by the MSL. The MSLs are able to have an intellectual conversation about the overall disease state and current research and science with KOLs that separates them from other contacts. The KOLs value MSLs who are able to speak to and understand the more scientific-level details (ie, statistics in the research) about a product, research, and events in the therapeutic area.
This survey approached KOLs with a series of questions about the services and information provided by MSLs and the relative value they place on such activities. However, it is important to recognize that the activities of an MSL are mostly triggered by unsolicited questions and requests from KOLs, and therefore, not all KOLs will be exposed to all potential MSL activities.
There are limitations to these research findings. Our work only surveyed KOLs known to our company and seen recently by our MSLs. In addition, these observations were obtained exclusively from KOLs in the diabetes therapeutic area. Nevertheless, these survey results provide a unique view of the MSL-KOL relationship from the perspective of the target customer: the KOL. Moreover, we believe that many of the findings are relevant and applicable to field medical teams operating in other therapeutic areas.
Conclusion
Diabetes MSLs are a valuable resource to KOLs. They must first and foremost present themselves as ethical and unbiased. They help KOLs stay up to date on industry information and happenings, saving time for the busy KOL. The KOL’s key information needs are around pipeline and research. They would like to get to know their MSLs better, to understand their background and experience, and to see them more often.
Previous surveys of MSLs and MSL managers across a diverse group of pharmaceutical, biopharmaceutical, and medical device companies provide a broad understanding of the practice trends and activities of contemporary MSL groups. These surveys, taken together, offer a solid reference point for building or developing an MSL team. Understanding the customer’s perspective via periodic survey assessments allows an MSL team to determine its effectiveness in meeting customer needs and identify areas for improvement.
The present survey provides a valuable view of the expectations that academic and clinical HCPs practicing in the diabetes therapeutic area have for the MSLs who visit them. These data may be used as an objective assessment of the perceived value of the field medical team to key customers and, when collected serially, can document the achievement of team objectives over time.
Footnotes
Portions of these data were presented at the DIA Medical Communications Workshop, Orlando, Florida, March 2012.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employees of Amylin Pharmaceuticals LLC.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.