
Abstract
The main objective of this study was to assess the factor structure and psychometric properties of the Czech translation of the Beliefs about Medicines Questionnaire (BMQ-CZ). It was hypothesized that the 4-factor structure of the BMQ-CZ would be confirmed and that psychometric properties would be verified by using positive or negative correlations with self-reported adherence, illness perceptions, and medication statements. A total of 627 people were approached, and 467 agreed to participate. The sample included chronically ill patients as well as patients seeking allopathic and homeopathic care. As a measure of criterion-related validity, the BMQ-CZ was administered along with the translated Czech versions of the Medication Adherence Report Scale (MARS-CZ) and the Brief Illness Perception Questionnaire (Brief IPQ–CZ) and additional assertions. The factor structure, reliability, and validity of the BMQ-CZ were evaluated. The internal consistency of the BMQ-CZ was satisfactory (Cronbach α = .69-.85). A factor analysis supported the BMQ-CZ’s 4-factor structure, and the concurrrent validity of the BMQ-CZ was supported by positive correlations with self-reported measures of adherence and beliefs about medicines and disease. The BMQ-CZ demonstrated sufficient psychometric performance as a self-reported measure of medication beliefs among patients with hypertension, diabetes, and rheumatic disease.
Keywords
Introduction
Medication treatment is an important component in the management of chronic illnesses. Although a patient’s adherence to medication is important in achieving better therapeutic outcomes, 1 published data indicate that many patients remain nonadherent to long-term therapies. According to a report by the World Health Organization, 2 nonadherence in developed countries approaches 50%. The meta-analysis of DiMateo et al 3 showed nonadherence to medical treatment prescribed by physicians (excluding psychiatrists) to be lower at 24.2%. Medication adherence can be classified as intentional and unintentional, with both of the categories being influenced by practical and perceptual barriers, among which patients’ beliefs and concerns play an important role. 4 The Necessity-Concerns Framework was developed by Horne et al 5,6 to operationalize patients’ beliefs in explaining adherence to treatment. To assess patients’ beliefs regarding their medicines, Horne et al 7 developed the Beliefs about Medicines Questionnaire (BMQ). The questionnaire has been validated and used for many diseases in various settings and countries. 8 –11 It has also been used to assess the medication beliefs of health care professionals. 12,13 As a prerequisite for using this tool for research in the Czech Republic, it is necessary to verify the conceptual equivalence of the Czech translation. The aim of our study was thus to translate the BMQ into the Czech language (BMQ-CZ) and to assess the psychometric properties of the resulting BMQ-CZ.
Methods
Patients
Main Sample
The research was approved by the ethics committees of the University Teaching Hospital and Charles University in Prague (March 2011). A sample of patients suffering from a chronic illness (main sample: n = 348) was asked to participate in the research. This group consisted of patients with diabetes (n = 129), hypertension (n = 103), and rheumatic disease (n = 116). Patients were included if they had been prescribed 1 or more medicines for regular use in the treatment of their illness at least 3 months before study inclusion. The participants were recruited at the 2nd Internal Gastroenterology Clinic (University Teaching Hospital) (patients with hypertension and rheumatic disease) and the Railway Health Centre (patients with diabetes), both in Hradec Kralove, during a 4-week period (patients with rheumatic disease and diabetes) and 6-week period (patients with hypertension) between June and August 2011. Questionnaires, together with a stamped addressed envelope, were distributed by the nurse to patients waiting for a doctor. Patients filled out questionnaires anonymously. Patients with hypertension were given consecutively numbered envelopes for the purpose of retesting. The doctor was not aware of patients’ answers as the filled questionnaires were sent to the researchers who did not know the identity of the patients. The data from the main sample were used for all statistical tests performed except for the evaluation of the discriminant validity of the BMQ-General scales in which a sample of homeopathic and allopathic care seekers was used for the assessment of discriminant validity.
Allopathic Care Sample
The patients from the allopathic care sample (n = 234) were recruited from a hospital pharmacy from June to August 2011. Because of the supposed large disparity in group size between the allopathic and homeopathic samples, if all patients had been contacted during the reporting period, it would have led to large differences in the sample size. Therefore, patients were contacted during various 2-hour periods on randomly selected days within a 2-week period. The general section of the BMQ-CZ along with background questions regarding age, gender, and education was used for the verification of discriminant validity. Consecutive patients presenting a prescription to the hospital pharmacy were approached by the researcher (P.M.) while they were waiting for their prescription to be filled.
Homeopathic Care Sample
The patients in the homeopathic care sample were recruited from a single homeopath’s office, in Pardubice, during the same period as the patients in the allopathic care sample. Consecutive patients (n = 45) were asked by the homeopath’s nurse to participate; all the participants completed the questionnaire (the response rate for the homeopathic care sample was 100%). All participants who were approached received information both verbally and in writing on the purpose of the study.
Test-retest reliability was performed to identify the stability of the scales. We used a hypertension sample and sent the repeat questionnaires to the first 40 patients. Questionnaires were sent together with a prepaid envelope 2 weeks after their visit to the clinic.
Measures
The BMQ-CZ was administered along with translated Czech versions of the Medication Adherence Report Scale (MARS-CZ) and the Brief Illness Perception Questionnaire (Brief IPQ–CZ). Additional data were surveyed (age, education, comorbidities, and total number of medicines used daily; all variables were self-reported) as well as statements (see below). Preliminary versions of all questionnaires and statements were administered to a group of 15 adult women and men who were either healthy or had a chronic disease to test their comprehension of the items. Following a discussion, definitive Czech versions of all tools were developed.
Questionnaires Used
The BMQ is a 19-item questionnaire that has 2 parts: general (measuring overall beliefs about medicines) and specific (identifying detailed beliefs about the patients’ own medicines). The back-translations (performed by a translation agency) of both the BMQ and MARS were approved by the original author of both questionnaires (R. Horne). The BMQ contains response categories on a 5-point Likert-type scale in which 1 = strongly disagree, 2 = disagree, 3 = uncertain, 4 = agree, and 5 = strongly agree.
The MARS-5 was developed to measure self-reported adherence. It is considered to be a more valuable tool for assessing self-reported adherence as compared to the Morisky questionnaire. 14 Items on the MARS-5 regarding the frequency of nonadherent behavior are scored on a 5-point Likert-type scale, while a cumulative score of 25 indicates full adherence. 15
The Brief IPQ (approval for usage was given by Elisabeth Broadbent) is a 9-item scale assessing cognitive representations of illness. 16 These are the following: consequences (“How much does your illness affect your life?”), timeline (“How long do you think your illness will continue?”), personal control (“How much control do you feel you have over your illness?”), treatment control (“How much do you think your treatment can help your illness?”), identity (“How much do you experience symptoms of your illness?”), concern (“How concerned are you about your illness?”), coherence (“How well do you feel you understand your illness?”), emotional representation (“How does your illness affect you emotionally?” [eg, “Does it make you angry, scared, upset, or depressed?”]), and cause (“Please list in rank order the 3 most important factors that you believe caused your illness.”). Each component is evaluated by 1 question, to which participants respond on a scale of 0 to 10.
To make the questionnaires specific to our population, we replaced the word “illness” with “high blood pressure” for patients with hypertension, “cukrovka” (a common Czech term used by lay people for diabetes mellitus) for patients with diabetes, and the general term “rheumatic disease” for patients with rheumatic disease.
Additional statements taken from the pool of medication statements subjected to principal component analysis (PCA) by Horne et al 7 were used for the evaluation of criterion-related validity. These were the following: “stronger medicines are more dangerous than weaker medicines,” “without medicines, doctors would be less able to cure people,” and “most medicines are safe.” The statement “it is better to do without medicines” was modified to “in my situation, it is better to do without medicines.” We added 2 new assertions: “people unnecessarily use lots of medicines” and “my medicines improve the general state of my health.” Responses were scored on a 5-point Likert-type scale (from strongly disagree to strongly agree).
Statistical Analysis
The software NCSS 2007 (NCSS LLC, Kaysville, Utah) and R 2.14.0 (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analysis. For the purpose of statistical analysis, patients from all 3 diagnostic groups of the main sample were amalgamated with the exception of test-retest reliability, the measurement of which was assessed only on patients suffering from hypertension (Horne et al 7 used only an asthma sample for this analysis).
Principal Component Analysis
A PCA using direct oblimin rotation was conducted to reveal the underlying factor structure. The criterion for factor extraction was an eigenvalue >1.0. As in the original study, 7 cases with more than 5 missing items as well as multidimensional outliers (Hotelling T 2 test with P < .001) were removed before PCA was performed. Specific and general medication beliefs were analyzed separately. The validity of separating specific and general medication beliefs was examined using an additional PCA on the combined specific and general factor items.
Reliability
The internal consistency of the BMQ subscales was assessed using Cronbach α. Test-retest reliability was evaluated using Spearman ρ.
Validity
Assessment of criterion-related validity was based on investigating the correlations of the BMQ-CZ subscales with the MARS-CZ, Brief IPQ–CZ, and 6 supplementary statements.
Testing the criterion-related validity of the BMQ scales:
Specific-Necessity: We hypothesized that people who had stronger beliefs in the necessity of their medicines would self-report higher medication adherence on the MARS-CZ. We expected a positive correlation with the consequence, timeline, treatment control, and identity components of the Brief IPQ. From the pool of additional questions, a positive correlation with “my medicines improve my general state of health” was anticipated. Conversely, we anticipated that patients with a greater belief in the necessity of their medicines would be less likely to agree with the statement “in my situation, it is better to do without medicines.”
Specific-Concerns: Patients with a more negative attitude towards their own medicines were expected to have lower self-reported adherence (MARS-CZ score) and a negative response to the treatment control component of the Brief IPQ and to the statement “my medicines improve my general state of health.” On the other hand, it was anticipated that these people would agree with the assertion “in my situation, it is better to do without medicines” (a positive correlation was expected).
General-Overuse: People who believe that the use of medicines is excessive (reflecting a negative perception of medicines in general) might be less adherent to their medication (a negative correlation with the MARS-CZ) and concur with the statement “people unnecessarily use lots of medicines” (with which agreement was anticipated).
General-Harm: People convinced that medicines are harmful would be expected to be less adherent to their own medications (a negative correlation with the MARS-CZ). Disagreement with the statements “my medicines improve my general state of health,” “without medicines, doctors would be less able to cure people,” and “most medicines are safe” was anticipated as well. To confirm the validity of separating specific and general medication beliefs, items loading on the specific and general factors were combined and subjected to further PCA.
Discriminant Validity
The discriminant validity of the BMQ-Specific subscales was tested to check the scales’ ability to distinguish between different illnesses. This was assessed using a Kruskal-Wallis 1-way ANOVA (with post hoc Kruskal-Wallis multiple comparison Z value test). The discriminant validity of the BMQ-General scales was evaluated to find out whether these scales were able to differentiate attitudes of the patients treated with allopathic and homeopathic care to medicines. This was assessed using a Mann-Whitney test. A 1-tailed test was used, as the direction of association had been specified within the relevant hypothesis. Before testing, an optimal matching based on the Mahalanobis distance (with gender as a forced match variable along with age and education as covariate variables) was conducted.
Results
Main Sample
In total, 290 of the 348 administered questionnaires were returned (83.3%). After excluding questionnaires with missing BMQ data and multidimensional outliers (see the Methods section), 279 questionnaires (80.2%) were analyzed; 105 (37.6%) of these questionnaires were obtained from patients with rheumatic disease and 88 (31.5%) from patients with diabetes, and the remaining 86 (30.8%) questionnaires were from patients with hypertension. The mean age of the study population in the main sample was 61 years (median, 63 years; range, 24-89 years), with slightly more than half being women (53.2%). Patients self-reported, on average, 6 medicines used daily (median, 6; range, 1-20).
Homeopathic/Allopathic Care Samples
In the homeopathic care sample, 45 questionnaires were given out, with 42 (93.3%) of them being returned with complete data filled in. The mean age was 44 years (median, 45.5 years; range, 18-69 years). The sample consisted mostly of women (88.1%). In the allopathic care sample, 234 people were approached, and 102 of them refused to participate (52 women); 132 people (56.4%) agreed to take part in the study, and 119 of them (50.9% of total) completed the questionnaire. The mean age of the participants was 48 years (median, 49 years; range, 18-79 years). Women comprised 53.8% of the participants. The samples were matched for gender, age, and education. Matching was carried out due to the large difference in the sample sizes and the possible confounding effect of these variables. This resulted in a total of 84 (42 + 42) questionnaires for further analysis. An overview of all the samples is presented in Table 1.
Overview of the patients who were solicited, who particip-ated, and who were included in the statistical analysis.
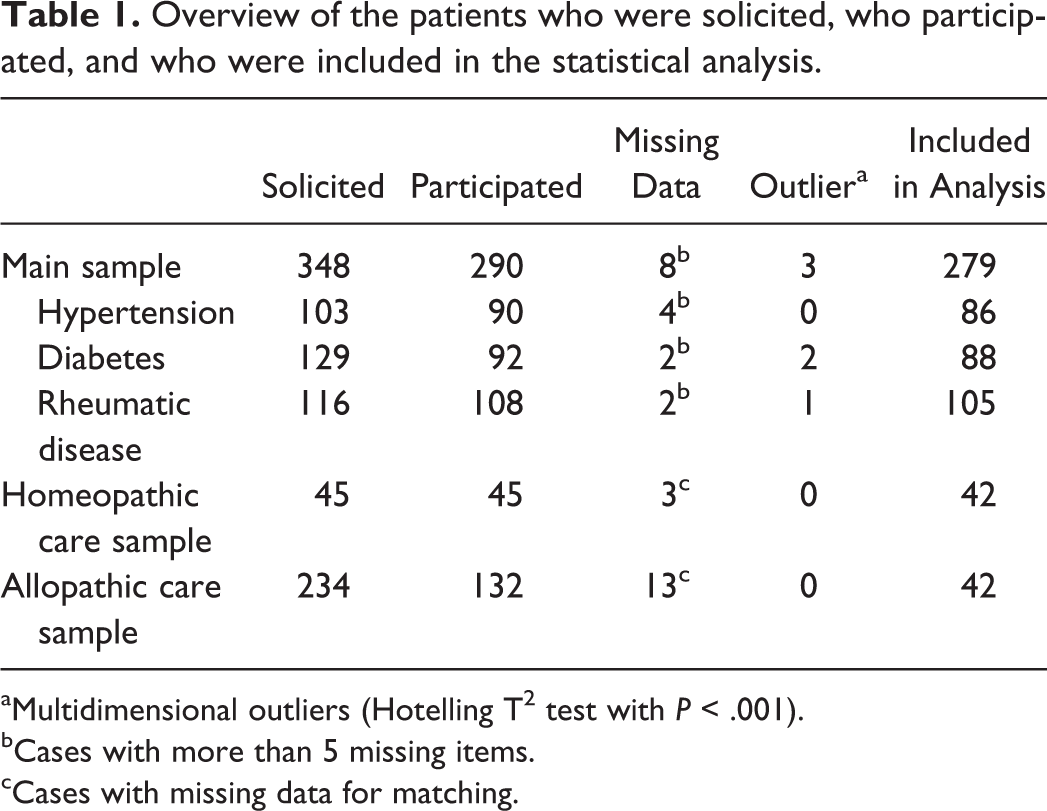
aMultidimensional outliers (Hotelling T2 test with P < .001).
bCases with more than 5 missing items.
cCases with missing data for matching.
Principal Component Analysis
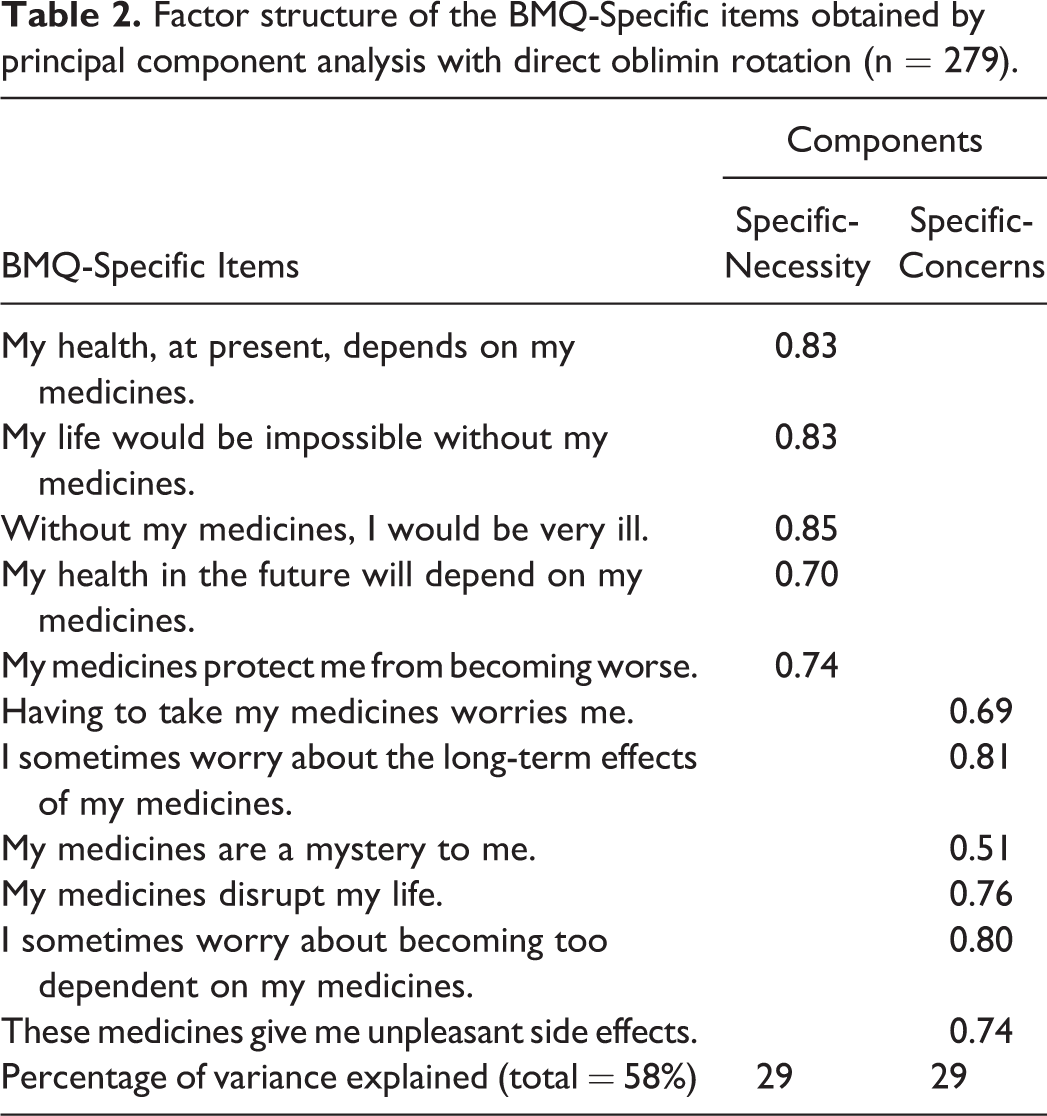
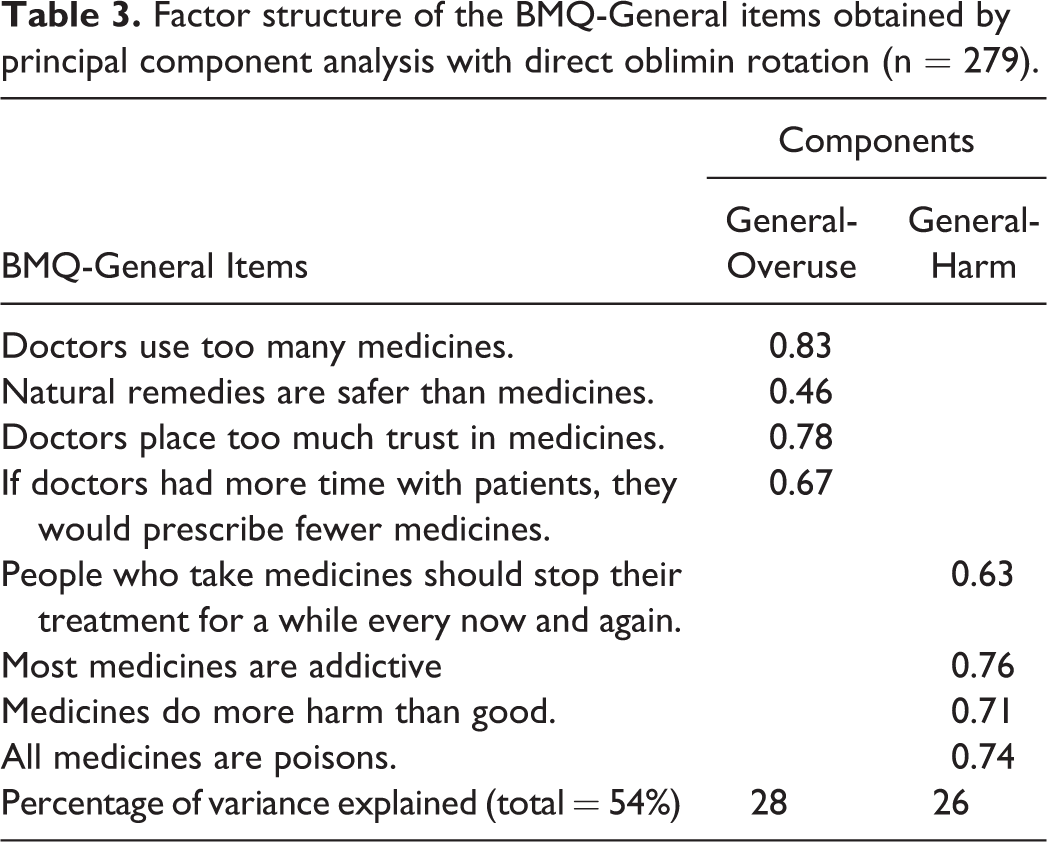
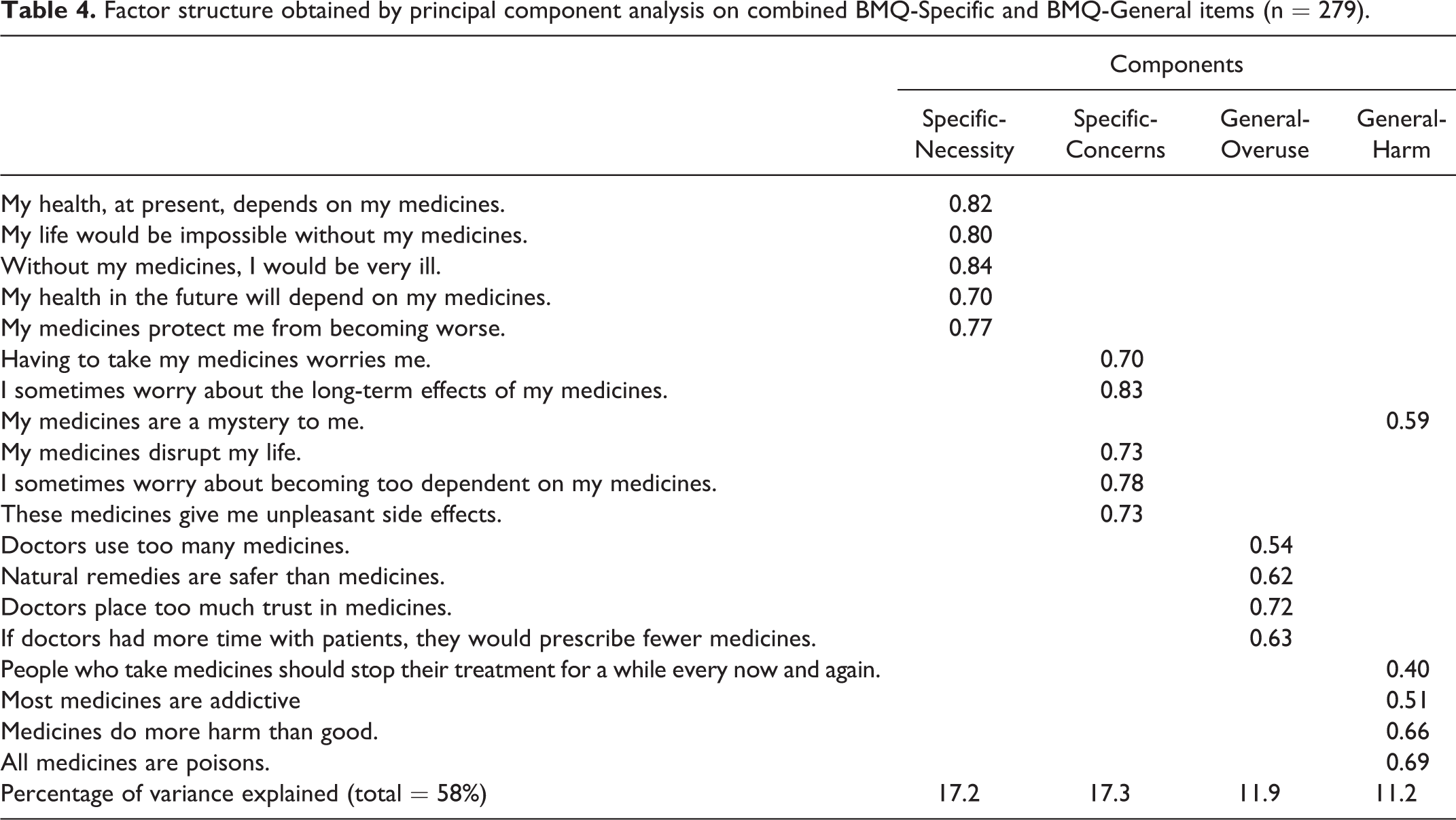
For both specific and general statements, PCA confirmed a 2-factor structure (Tables 2 and 3), explaining 58% and 54% of the total variance, respectively. The PCA on the combined specific and general items resulted in a 4-factor structure (Table 4), explaining 58% of the variance. The mean scores for the BMQ-General and the BMQ-Specific were 11.1 and 18.2, respectively.
Factor structure of the BMQ-Specific items obtained by principal component analysis with direct oblimin rotation (n = 279).
Factor structure of the BMQ-General items obtained by principal component analysis with direct oblimin rotation (n = 279).
Factor structure obtained by principal component analysis on combined BMQ-Specific and BMQ-General items (n = 279).
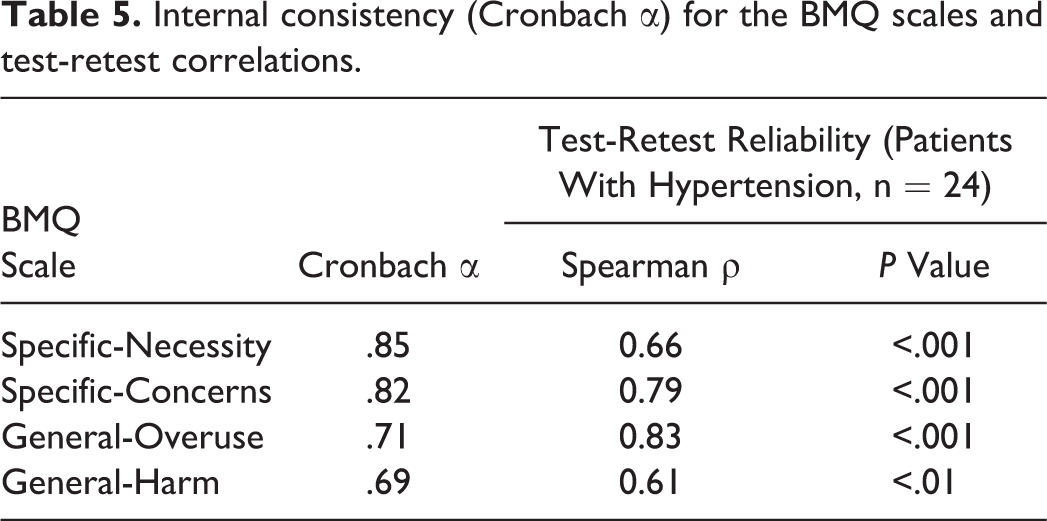
Internal consistency (Cronbach α) for the BMQ scales and test-retest correlations.
Discriminant validity of the BMQ scales.
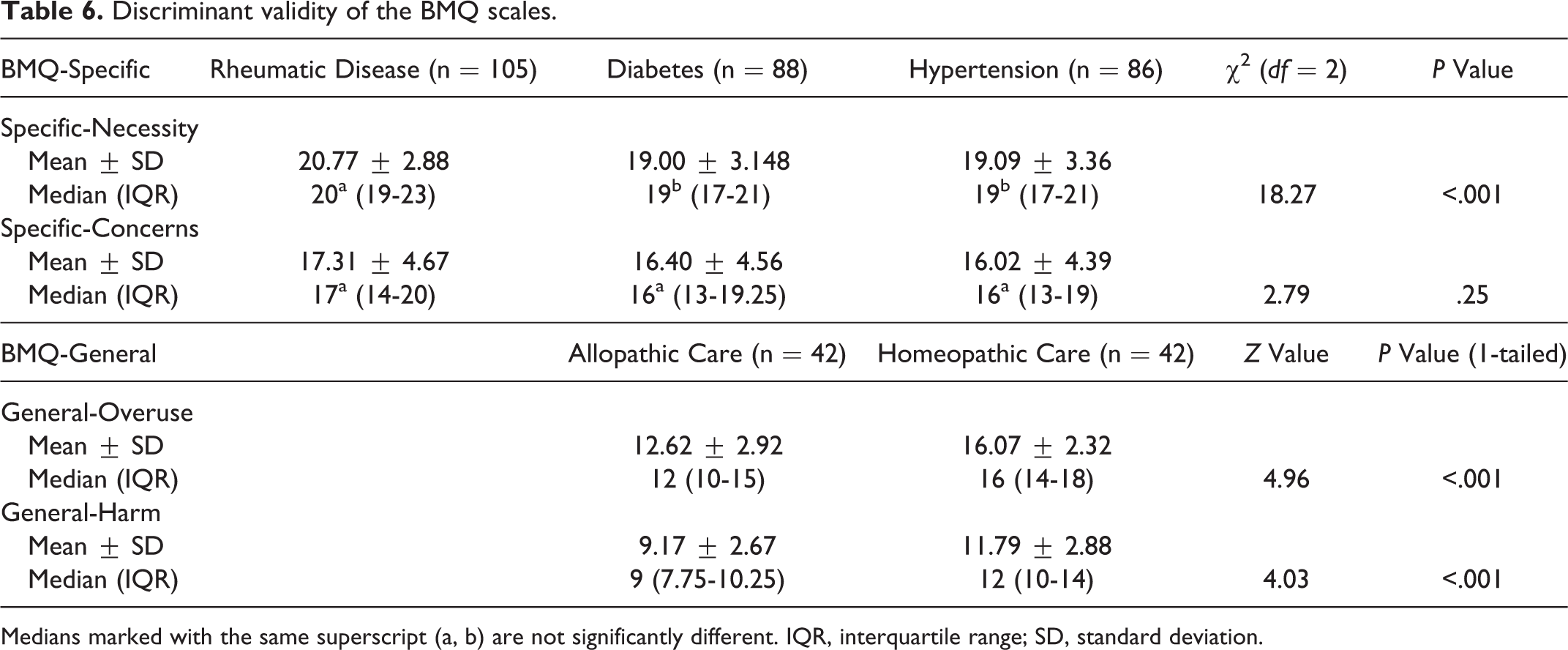
Medians marked with the same superscript (a, b) are not significantly different. IQR, interquartile range; SD, standard deviation.
Reliability
The Cronbach α for the BMQ subscales ranged from .69 to .85 (Table 5), which indicates satisfactory internal consistency. Test-retest reliability was evaluated using the hypertension sample. The first 40 patients were given the repeat questionnaire, of whom 24 (60%) returned the form filled in. The test-retest reliabilities between the initial and repeated test scores for each subscale were as follows: Specific-Necessity (ρ = 0.66; P < .001), Specific-Concerns (ρ = 0.79; P < .001), General-Overuse (ρ = 0.83; P < .001), and General-Harm (ρ = 0.61; P < .01).
Validity
Criterion-Related Validity
Correlations with the Brief IPQ
As expected, the Specific-Necessity scores positively correlated with the scores of the following components: consequences (ρ = 0.32; P < .001), timeline (ρ = 0.33; P < .001), treatment control (ρ = 0.30; P < .001), and identity (ρ = 0.30; P < .001). The Specific-Concerns scores negatively correlated with the scores on the treatment control component (ρ = –0.25; P < .001).
Adherence to treatment
The correlations between the BMQ scales and the MARS were as expected: The Specific-Necessity subscale scores correlated, although only moderately, with a higher reported adherence (ρ = 0.14; P < .05). The correlations of the MARS with the Specific-Concerns (ρ = –0.22; P < .001), General-Overuse (ρ = –0.16; P < .01), and General-Harm (ρ = –0.12; P = .06) scores were as predicted, although the correlation between the General-Harm subscale and the MARS failed to reach statistical significance.
Correlations with complementary statements
In accordance with our a priori hypotheses, Specific-Necessity scores positively correlated with scores on the statement “my drugs improve my general state of health” (ρ = 0.44; P < .001) and negatively correlated with scores on the statement “in my situation, it is better to do without medicines” (ρ = –0.42; P < .001). Scores on Specific-Concerns positively correlated with scores on “in my situation, it is better to do without medicines” (ρ = 0.24; P < .001) and negatively correlated with scores on “my medicines improve my general state of health” (ρ = –0.29; P < .001). Scores on General-Overuse positively correlated with “people unnecessarily use lots of medicines” (ρ = 0.42; P < .001). Scores on General-Harm positively correlated with scores on “stronger medicines are more dangerous than weaker medicines” (ρ = 0.26; P < .001) and negatively correlated with scores on “my medicines improve my general state of health” (ρ = –0.30; P < .001), “without medicines, doctors would be less able to cure people” (ρ = –0.27; P < .001), and “most medicines are safe” (ρ = –0.18; P < .01). The last mentioned correlation was low but as expected.
Discriminant Validity
The Kruskal-Wallis test for Specific-Necessity showed that patients with rheumatic disease had significantly higher scores than the other 2 groups (Table 6). The same test for Specific-Concerns did not show any significant difference in the diagnostic groups involved. The assessment of discriminant validity for the general scales was based on a comparison of scores reached by homeopathic and allopathic care seekers. As expected, patients seeking care from a homeopath had significantly higher scores on both the General-Overuse and General-Harm scales than the patients from the allopathic care sample (in both cases, P < .001) (Table 6).
Discussion
To be able to evaluate patients’ opinions and beliefs about medicines, it is necessary to have a tool capable of assessing them. The BMQ is a short and easy-to-use questionnaire that can be used in a large variety of adherence research.
The illness groups from which patients were sampled were chosen to reflect common chronic diseases. In 2010 (the data for 2011 are not available yet), a total of 1.707 million patients in the Czech Republic were being treated for hypertension, and there were over 806,000 patients with diabetes being treated, mostly (91.8%) for type II diabetes. A total of 10,532,770 persons were living in the Czech Republic as of December 31, 2010. 17 The mean number of medicines self-reported by patients was 6. Mahler et al 8 reported that most patients (81.7%) were treated with more than 4 medicines on a regular basis, which could be possibly comparable with our sample.
We recorded an acceptable return rate of the BMQ-CZ and accompanying questionnaires. The factor structure and test-retest reliability of the BMQ-CZ were found to be satisfactory. There was one exception for the item “my medicines are a mystery to me,” which in a factor analysis loaded on the General-Harm instead of the Specific-Concerns subscale. This observation was similar to Horne et al’s 7 validation in which this item loaded higher on the General-Harm than on the Specific-Concerns scale. This might be caused by the fact that patients generally may not feel confident in their knowledge on medicines in general. We do not have any evidence for this suggestion, however.
Sufficient internal consistency was demonstrated for 3 of the BMQ-CZ subscales (Specific-Necessity, Specific-Concerns, and General-Overuse). The boundary of internal consistency of the BMQ-CZ General-Harm subscale (α = .69) is in concordance with that shown by Perpiñá Tordera et al 10 (α = .68). Horne et al 7 reported an α for General-Harm in the range of .47 to .83. We found significant correlations between the results of the MARS-CZ and specific medication beliefs similar to those revealed in previous studies. 5,8,15,18
Patients with rheumatic disease showed significantly different Specific-Necessity scale scores than patients with hypertension and diabetes. We did not find significantly different Specific-Necessity scores in the group with diabetes, contrary to Horne et al. 7 At the same time, illness groups did not report different Specific-Concerns scores. The one possible explanation is that patients with asthma and psychiatric diseases were not included in our study, whereas they were in Horne et al’s. 7 An examination in Germany of the psychometric properties of the BMQ-D did not test discriminant validity, so we are not able to compare our results with them. 8 The other published validations used only groups with a particular disease, excluding the verification of discriminant validity. 9,10
The Czech version of the BMQ-General had sufficient discriminant validity and discriminated between patients treated with allopathic and homeopathic care. This was in concordance with the original validation during the development of the BMQ. 7
Testing of the criterion-related validity is limited by the fact that to our knowledge, there has been no other previously validated tool assessing patients’ beliefs in our country. Similar concerns were expressed as well by Horne et al 7 in the original publication. Therefore, we employed a method of using the other translated questionnaires and single-item constructs of attitudes, with the expectation that they measured the same concept that was utilized both in the original article and similarly in the Spanish validation of the BMQ in patients with bronchial asthma. 7,10 Suggested correlations between the BMQ scales and other statements were as expected.
Conclusion
We believe that the BMQ-CZ has a reasonable factor structure and psychometric properties suitable for use in the research into beliefs regarding medicines in the Czech Republic.
Footnotes
Acknowledgments
The authors appreciate the help of Helena Maresova, PharmD; Jana Vaskova, MD, homeopath; as well as Jiri Kotlar, MSc, head of the hospital pharmacy. They also thank Martina Klimkova, MSc, and Jitka Pokladnikova, PhD, for their help with the translations of the BMQ, MARS, and Brief IPQ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.