
Abstract
In drug development, a safety index—the ratio of the highest exposure that does not induce toxicity to the exposure that exerts efficacy—is used to quantify the balance between the safety and efficacy of a test drug. Here, the phase 1 index (maximum area under the curve [AUC] in phase 1/therapeutic AUC) and no-observed-adverse-effect level (NOAEL) index (AUC at NOAEL/therapeutic AUC) of recently approved drugs in Japan were calculated and characterized by therapeutic areas and indications. A large variation within both indices was observed, with a median of 3.2 for the phase 1 index and 3.5 for the NOAEL index. Furthermore, the safety indices were affected by the therapeutic area, which might be attributed to the difference in unmet medical needs for certain diseases. This study provides a qualitative measure for interpreting the phase 1 index versus the NOAEL index and might help inform the decision-making process following phase 1 trials.
Introduction
In clinical development, phase 1 is the first stage where the safety, tolerability, pharmacokinetics (PK), and possibly pharmacodynamics (PD) of a test drug are investigated in humans, following required preclinical studies on toxicology, pharmacology, and drug metabolism/PK. 1 Phase 1 studies are generally conducted in healthy subjects, with dose levels increasing in single and multiple administrations. Following phase 1 trials, a decision has to be made whether or not safety and tolerability are ensured sufficiently to further advance development, typically to move on to a proof-of-concept study. This decision-making process requires multidisciplinary knowledge and sometimes raises tough argument from standpoints of research, clinical development, and marketing.
To quantify the balance between the safety and efficacy of a test drug, a safety index, the ratio of the highest exposure that does not induce toxicity to the exposure that exerts efficacy, is used as a safety margin in drug development. The decision to advance development of a test drug is often undertaken with reference to the safety index throughout the research and clinical development stage, and phase 1 is the first key milestone in clinical development to decide whether a test drug is worth further developing.
The results of phase 1 and toxicology studies often raise a question on whether or not the obtained safety index is sufficient to advance development or, in other words, whether or not the safety and tolerability when administering a dosage exceeding the therapeutic exposure are sufficiently ensured to proceed with further clinical development. Related to a safety index, the International Conference on Harmonisation E14 guideline addresses the use of a supratherapeutic dose in the context of the design of a thorough QT/QTc study. 2 Such a study is intended to determine whether or not a test drug has a threshold pharmacologic effect on cardiac repolarization, as detected by QT/QTc prolongation. As a supratherapeutic dose, the guideline recommends a dose that produces concentrations similar to those observed under conditions that produce maximum exposure. Generally, it is needed that the highest phase 1 dose covers the supratherapeutic dose range. With respect to drug developability, however, no regulatory guidance or systematic research has been drafted to specifically address a standard or appropriate safety index. Muller and Milton 3 investigated therapeutic index determination and interpretation with some examples, along with the progression through drug research and development. They emphasized the need to understand the preliminary therapeutic index from the lead identification stage onward and the fact that therapeutic indices should be continuously refined as a test drug progresses from in vitro to animal to human studies. Furthermore, they indicated that decisions based on the therapeutic index depend on multiple factors that characterize an acceptable risk-benefit profile for the targeted indication of a test drug.
Here, to systematically explore factors affecting the safety index, we calculated and characterized the safety indices of recently approved drugs in Japan by attributes such as therapeutic area and indications.
Methods
Data Source
We analyzed drugs classified as new molecular entities that were recently approved in Japan. Summary New Drug Application dossiers, review reports, and package inserts of new molecular entities approved between 2008 and 2012 in Japan were obtained from the website of Pharmaceutical and Medical Device Agency (http://www.pmda.go.jp). Of the 174 new molecular entities approved during the period, we excluded the following categories of drugs: Anticancer drugs Endogenous substances, such as hormones and peptides, and their analogues, for which there is previous clinical experience with similar products Enantiomer, prodrugs, or active metabolites of approved drugs Drugs not intended for systemic administration Drugs with little or no absorption Vaccines Drugs approved in other countries before 2000 Drugs with a scarcity of research data
We excluded anticancer drugs, as cancer patients are normally subjects for phase 1 studies and evaluation on safety versus potential benefit is generally different with anticancer drugs that drugs in other therapeutic areas. 4
We then collected the following information: Highest tolerable area under the curve (AUC) extrapolated to infinity (AUCinf) from single-ascending-dose studies conducted. Highest tolerable AUC per day over a dose interval at a steady state (AUCss) for multiple-ascending-dose studies conducted. Approved maximum dose in Japan and AUCss at that dose. We collected the AUCss from section 2.6.6 of the CTD (Common Technical Document for New Drug Application) for each drug if exposure comparison between humans and animals was performed in that section. When that was not the case, we collected the AUCss from PK studies with patients or healthy volunteers. The no-observed-adverse-effect level (NOAEL) and AUCss at the NOAEL (rodent and nonrodent) were determined in 13 weeks of repeated toxicology studies. If these data were not available, data were then collected from 4 weeks or more than 13 weeks of studies.
The AUC of an unchanged drug was basically used in this study. We also used the highest AUC tested if no information on tolerability was obtained. A phase 1 study was adopted regardless of the countries in which the study was carried out.
Data Analysis
Figure 1 shows the general relationship of the dose range of a phase 1 first-in-human study, target therapeutic dose, and NOAEL in animal toxicology studies. From a safety viewpoint, NOAEL and toxicologic findings with toxicokinetics obtained from repeated toxicology studies are the major determinants for setting the dose range in first-in-human studies. From an efficacy viewpoint, the target therapeutic dose is generally obtained before first-in-human studies via translation of information on the preclinical PK-PD relationship into humans. The target therapeutic dose is then modified on the basis of clinical PK and PD data.
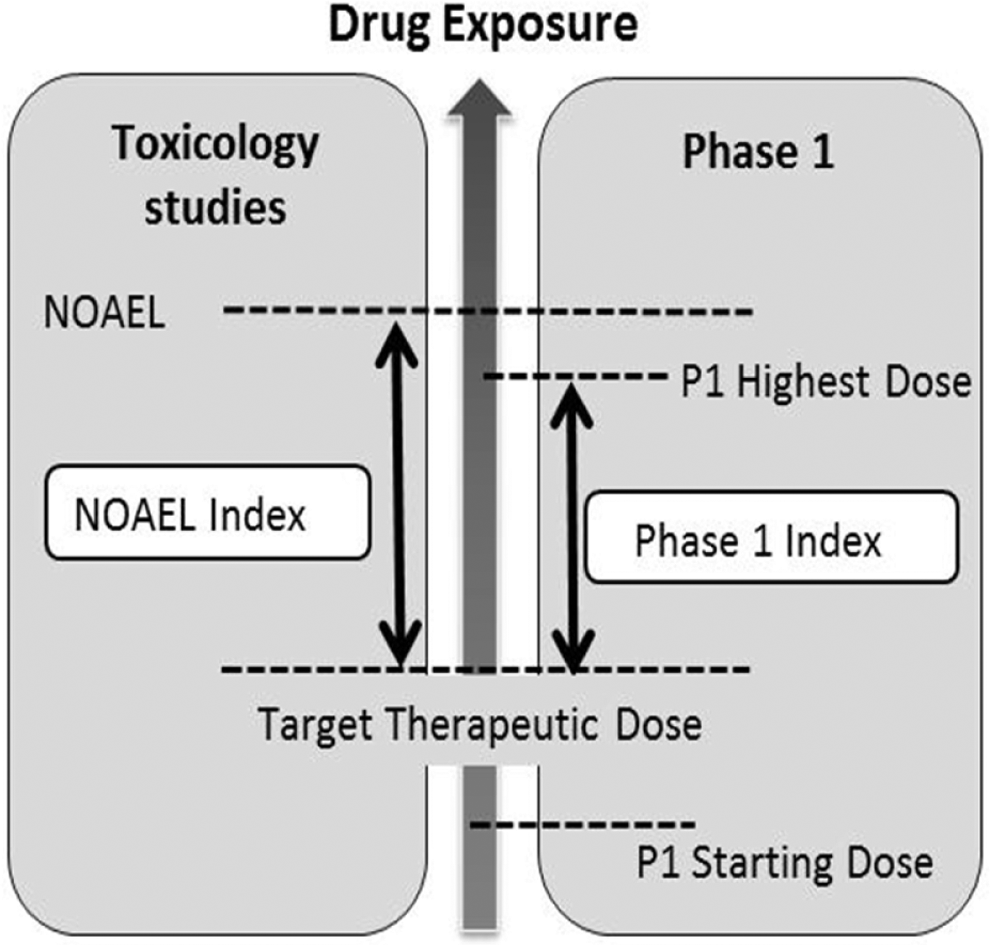
Relationship of phase 1 dose range, target therapeutic dose, and no-observed-adverse-effect level (NOAEL).
We utilized the NOAEL index and phase 1 index as safety indices, and each index was calculated as follows:


where maximum AUC in phase 1 is the highest AUC of the AUCinf for single ascending dose or the AUCss for multiple ascending dose and where AUCss at NOAEL is the AUC of the most sensitive animal species (the mean of male and female subjects).
Analysis of the Phase 1 Index and NOAEL Index
Summary statistics of the phase 1 index and NOAEL index were calculated, and the relationship between the 2 indices was investigated. The obtained phase 1 and NOAEL indices were stratified on the basis of drug attributes from the Anatomical Therapeutic Chemical (ATC) classification code, therapeutic indication, administration route, molecular features (biopharmaceuticals vs chemicals), and “orphan drug” designation. Classification by the ATC code was applied when at least 5 drugs had the same ATC code. Drugs for which no ATC code had been assigned were categorized to the appropriate ATC main group for research purpose. Analysis was performed via StatsDirect statistical software (v 2.7.9; StatsDirect Ltd, Cheshire, UK).
Results
Of the 174 new molecular entities approved in Japan between 2008 and 2012, 60 were analyzed in the present study (Table 1). The breakdown of the excluded drugs was as follows: anticancer drugs, n = 24; endogenous substances, n = 8; enantiomer, prodrugs, or active metabolites of approved drugs, n = 11; drugs not intended for systemic administration, n = 14; drugs with no or little absorption, n = 3; vaccines, n = 14; drugs for no main therapeutic purpose, n = 9; drugs approved in other countries before 2000, n = 25; and drugs lacking sufficient research data, n = 6.
New molecular entities analyzed in this study.
Summary statistics of the phase 1 and NOAEL indices are shown in Table 2. Both indices exhibited large variation; the geometric mean and median, respectively, were 3.7 and 3.2 for the phase 1 index and 3.8 and 3.5 for the NOAEL index. The interquartile range of the phase 1 index was 1.9 to 5.4, and that of the NOAEL index was 0.8 to 13.8. The relationship between the NOAEL and the phase 1 indices is shown in Figure 2. Linear regression analysis for the indices showed no statistically significant correlation (Spearman rank correlation coefficient = 0.238; P = .0888).
Overall phase 1 index and NOAEL index for drugs studied.
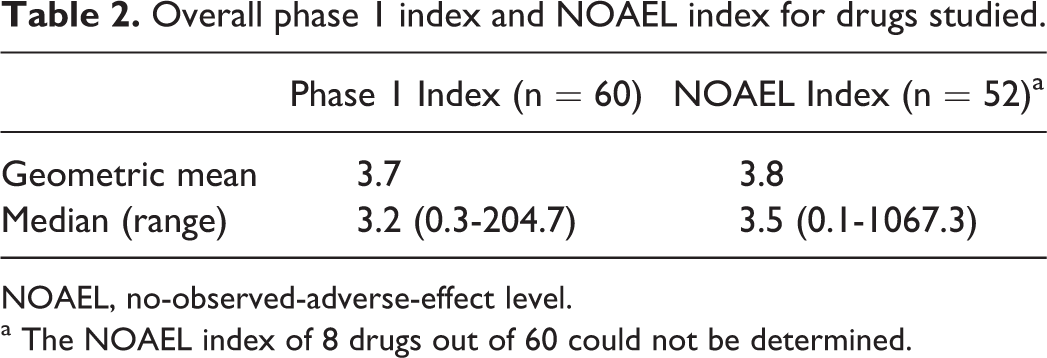
NOAEL, no-observed-adverse-effect level.
a The NOAEL index of 8 drugs out of 60 could not be determined.
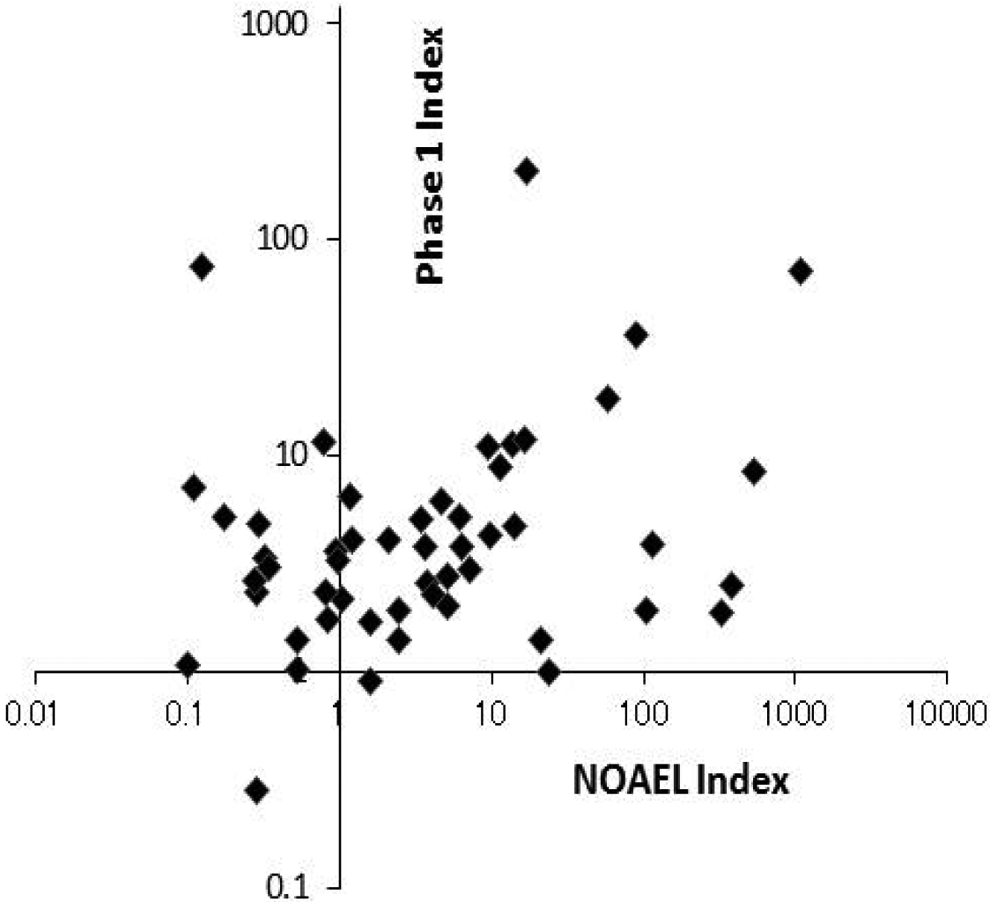
Plot of phase 1 index versus NOAEL index of the 52 drugs.
The indices were classified by ATC code as shown in Figure 3. The median phase 1 index for each was as follows: A, alimentary tract and metabolism (5.2); B, blood and blood-forming organs (3.6); J, anti-infectives for systemic use (2.3); L, antineoplastic and immunomodulating agents (4.2); and N, nervous system (2.0). In contrast, the median NOAEL index was as follows: A, alimentary tract and metabolism (13.7); B, blood and blood-forming organs (3.6); J, anti-infectives for systemic use (0.8); L, antineoplastic and immunomodulating agents (9.8); and N, nervous system (1.6). Although a high degree of variation was observed in both phase 1 and NOAEL indices, the median phase 1 index and NOAEL index were smaller in drugs used to treat infectious diseases and disorders of the nervous system.
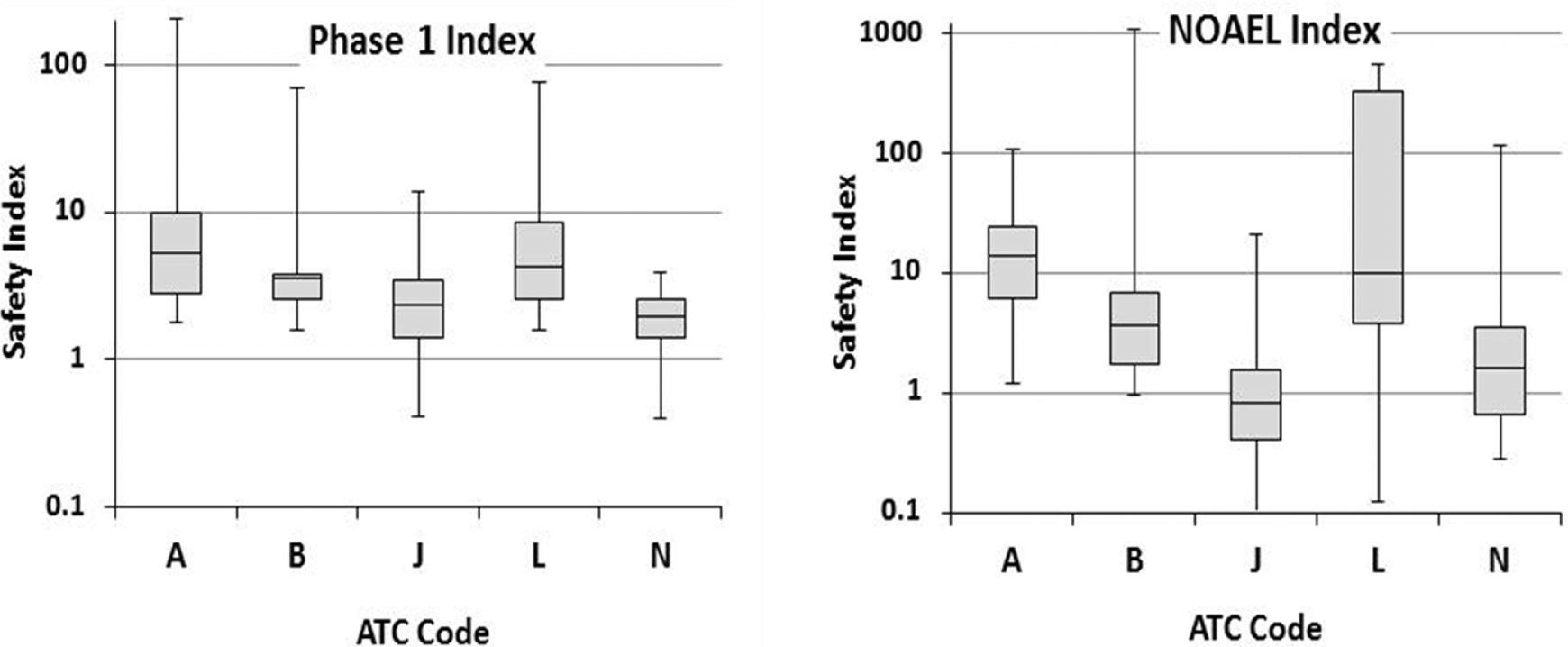
Phase 1 index and NOAEL index classified by ATC codes. The ATC codes and the number of the phase 1 index and NOAEL index, respectively, were as follows: A, alimentary tract and metabolism, n = 11 and n = 9; B, blood and blood-forming organs, n = 7 and n = 7; J, anti-infectives for systemic use, n = 12 and n = 11; L, antineoplastic and immunomodulating agents, n = 9 and n = 9; and N, nervous system, n = 8 and n = 6.
A comparison of the phase 1 index and NOAEL index between chemicals and biopharmaceuticals is shown in Figure 4. Results showed that the median NOAEL index of biopharmaceuticals was larger than that of chemicals, with no notable differences in the phase 1 index. The median phase 1 index and NOAEL index, respectively, were 3.3 and 1.9 for chemicals and 2.5 and 41.3 for biopharmaceuticals. The phase 1 and NOAEL indices were calculated for monoclonal antibodies, which accounted for half the biopharmaceuticals examined (6 of 12 drugs). The median phase 1 index for monoclonal antibodies was 2.5, while that of the NOAEL index was 194.4. Regarding the route of administration, the NOAEL index on subcutaneous administration was larger than that on oral or intravenous administration. The median values of the phase 1 index for each route of administration were as follows: oral (3.8), subcutaneous (2.3), and intravenous administration (2.8). In contrast, median values of the NOAEL index were as follows: oral (1.6), subcutaneous (104.5), and intravenous administration (1.0).
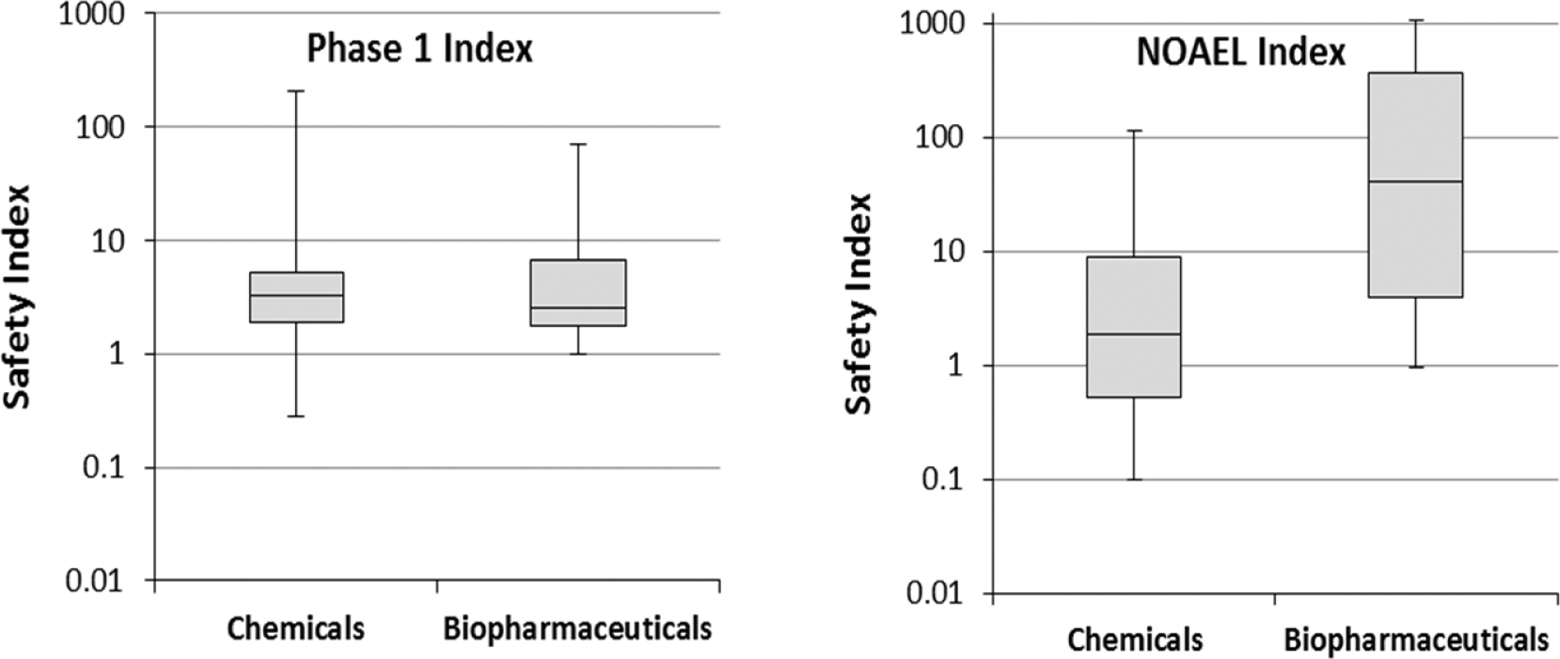
Comparison of safety indices between chemicals (phase 1 index, n = 48; NOAEL index, n = 42) and biopharmaceuticals (phase 1 index, n = 12; NOAEL index, n = 10).
Table 3 shows a list of drugs with both a phase 1 index and NOAEL index of <3. Generally, lower safety indices indicate a greater likelihood of adverse events, as the drugs are sensitive to increases in exposure. According to the list, drugs used to treat infectious diseases or disorders of the nervous system and orphan drugs have been observed to be the majority of “the smaller index group.”
List of drugs with a phase 1 index and NOAEL index <3.
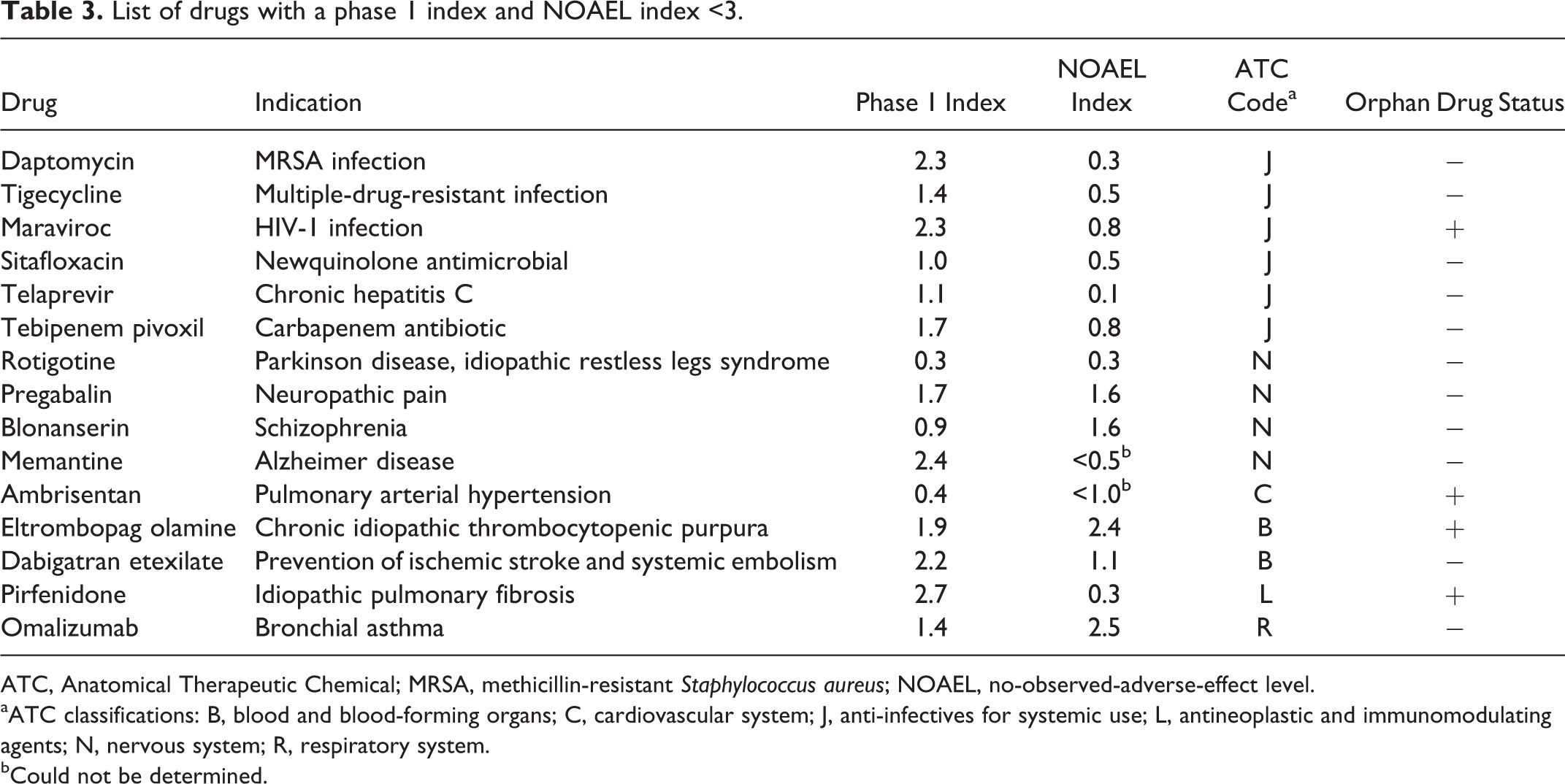
ATC, Anatomical Therapeutic Chemical; MRSA, methicillin-resistant Staphylococcus aureus; NOAEL, no-observed-adverse-effect level.
aATC classifications: B, blood and blood-forming organs; C, cardiovascular system; J, anti-infectives for systemic use; L, antineoplastic and immunomodulating agents; N, nervous system; R, respiratory system.
bCould not be determined.
Discussion
The phase 1 and NOAEL indices both exhibit a large degree of variation. Classification by ATC code showed that these indices were affected by the therapeutic area and that the medians of the safety indices were smaller in drugs used to treat infectious diseases and disorders of the nervous system. The median NOAEL index of the biopharmaceuticals was larger than that of chemicals, with no notable differences in the phase 1 index.
Investigation of the relationship between the NOAEL and phase 1 indices revealed that there was no significant positive correlation (Figure 2). This may be relevant to the fact that no maximum tolerable doses were defined in most of the drugs studied. The NOAEL index may be an index for scientific facts obtained from toxicology studies, while the phase 1 index has a strategic aspect on the foundation of integrated assessment of clinical and preclinical safety information.
The interquartile range of the phase 1 index was 1.9 to 5.4, which indicates that safety and tolerability are confirmed exceeding the therapeutic exposure. This finding may be relevant to the recommended use of supratherapeutic dose in the context of the thorough QT/QTc study design. Generally, a supratherapeutic dose is one that produces maximum exposure in a so-called worst-case scenario, which includes but is not limited to plasma concentration increase by the concomitant use of drugs with metabolic inhibition potential and administration to poor metabolizers and special population (eg, elderly patients, patients with renal/hepatic impairment). For example, when in vitr metabolism data of a test drug suggest the predominant contribution of CYP3A4 to total body clearance of humans, the possible impact of drug-drug interaction in clinical development is often determined by clinical drug-drug interaction studies with strong inhibitors, such as itraconazole, followed by studies with moderate or weak inhibitors when required. 5,6 Consideration is therefore required when deciding if the phase 1 index is sufficient in terms of “coverage of supratherapeutic dose.”
In contrast, the interquartile range of the NOAEL index was 0.8 to 13.8, and the NOAEL indices of 20 drugs were <1. This finding suggests that the safety and tolerability of the drugs were clinically investigated by exceeding the drug exposure of the NOAEL index based on the assessment of clinical findings observed in phase 1 and the nature of preclinical toxicity. Although the NOAEL index calculated from most sensitive animal species may have a conservative aspect, it does not mean that a NOAEL index <1 is generally acceptable to proceed with clinical development. Here, no qualitative analysis of toxicity was taken into consideration. As such, appropriate interpretation of the NOAEL index requires consideration of the following qualitative aspects: severity, seriousness, reversibility, monitorability and translatability of observed toxicities.
For example, the median phase 1 index of aprepitant is 3.6, while that of the NOAEL index could not be determined. A 14-week repeated toxicology study in rats indicated that NOAEL was <5 mg/kg/day, where the toxicologic finding at 5 mg/kg/day was vacuolar degeneration of the thyroid follicular cell. Since this finding was thought to be a change secondary to the hepatic enzyme induction in rats, the applicant explained in the NDA dossier that translatability of the histopathological change into humans was low.
Due to serious toxicologic findings, such as convulsion, an exposure cap in phase 1 studies is sometimes set below NOAEL to ensure safety, with the maximum possible clinical exposure not being limited by NOAEL. The interpretation of the NOAEL index from the standpoint of translation into humans is therefore important for appropriately exploring safety and tolerability in phase 1 studies and discussing the transition to the next clinical phase.
The comparison of the safety indices between chemicals and biopharmaceuticals is shown in Figure 4. The NOAEL index of biopharmaceuticals is larger than that of chemicals, while there appears to be no notable difference in the phase 1 index. This difference was more notable for monoclonal antibodies. This property might be due to the poorer quantitative translatability of biopharmaceuticals. In toxicology studies for biopharmaceuticals, relevant animal species that express the desired epitope and demonstrate a tissue cross-reactivity profile similar to that of human tissues have been used in accordance with the International Conference on Harmonisation S6 (R1) guideline, 7 optimizing the ability to evaluate toxicity arising from the binding to the epitope and any unintentional tissue cross-reactivity. In addition, when a phase 1 study is planned, especially a first-in-human study, the relevance and limitations on the quantitative translatability of toxicologic data into humans need to be taken into consideration. 8 –10 To ensure an ascending dose level in a phase 1 study, PD markers such as target binding and occupancy are often monitored, in addition to evaluation based on safety index. This approach is important not only to understanding whether or not drug exposure is sufficient to exert pharmacologic effects but also for avoiding on-target toxicity, by integrating preclinical pharmacologic and toxicologic findings. The NOAEL index in subcutaneous administration was larger than that of oral and intravenous administration, possibly due to the subcutaneous dosing routes of biopharmaceuticals with a higher NOAEL index.
Drugs with a phase 1 index and NOAEL index of <3 are listed in Table 3. The majority of this list consists of drugs used to treat infectious disease and defects of the nervous system as well as orphan drugs and is consistent with the outcome of stratified analysis by ATC code. In Japan, orphan drugs are indicated for the treatment of serious diseases, including difficult-to-treat diseases, for which there are a limited number of patients (<50,000). Benefit-risk balance in this category may result in relatively low phase 1 and NOAEL indices.
Nervous system disorders have been acknowledged to have a high degree of unmet medical needs, 11 –16 and central nervous system drug development is believed to be more challenging and have a higher risk than other indications. Reasons for this include a lack of knowledge of fundamental biology and pathophysiologic underpinnings of many central nervous system disorders, as well as the high use of subjective diagnosis and primary endpoints. Furthermore, low tolerability is sometimes observed, which leads to a lower phase 1 index due to the nature of the target molecule.
Here, the drugs for infectious diseases categorized in “the smaller index group,” including HIV-1 infection (orphan designation), multidrug resistant infection, and chronic hepatitis C, are considered to have a high degree of unmet medical needs. Of note, the NOAEL index was smaller than that of the phase 1 index. Dabigatran etexilate has been used as an oral anticoagulant to satisfy unmet medical needs. While warfarin has been widely used as an anticoagulant, it has a narrow safety margin and is difficult to handle due to its interaction with food and drugs and frequent laboratory monitoring. As mentioned above, a common feature of “the smaller safety index category” is for diseases with a low standard of care and a high degree of unmet medical needs.
The phase 1 index and NOAEL index of 6 drugs (DPP4 inhibitors) indicated for type 2 diabetes were calculated, and the medians of the indices were 7.6 and 8.8, respectively, which indicates that the medians of these safety indices were larger than that for all drugs examined (Table 2). This finding may be due to a higher standard of patient care, more manageable conditions, and a more competitive market.
When safety indices are calculated, it is also important to predict a target therapeutic dose as accurately as possible. The application of PK/PD modeling and simulation would support it, 17,18 although the present study did not address this point. Recently, PK/PD modeling and simulation have been applied not only to late phase development but also to preclinical and early phase clinical drug development. Integrating preclinical and clinical data, its application in early development helps us to predict a target therapeutic dose range.
In a decision-making process regarding further drug development based on phase 1 results, safety indices play a key scientific element. First, we need to appropriately interpret the safety indices by considering qualitative aspects of toxicologic findings (eg, severity, seriousness, reversibility, and translatability of the observed toxicities). Second, it is important to evaluate the potential benefit-risk balance in light of the target product profile of a test drug, where its clinical positioning is clarified and the acceptable benefit and risk balance is elucidated for the decision making. For example, when a sufficient phase 1 index (safety/tolerability at supratherapeutic exposure) is not obtained due to the lack of tolerability/safety and/or low NOAEL index, it may be considered difficult to advance the development. In that case, however, we need to evaluate the benefit-risk balance in light of the target product profile. If unmet medical needs, such as seriousness of the targeted disease condition and availability of alternative effective therapeutic options, overweigh the possible safety concerns, a test drug could move on to phase 2. From a scientific perspective, PD data in phase 1—for instance, biomarker measurements and positron emission tomography target occupancy studies to show the proof of pharmacology in humans—would support the decision making. Encouraging clinical PD findings would affect the decision in a positive way, and PK/PD modeling and simulation would support the quantitative decision making, integrating preclinical PK/PD data.
Besides scientific evaluation, it needs to be noted that the likelihood of return on investment of a test drug generally affects the decision making. Factors affecting the return on investment include, but are not limited to, drug development cost, marketability of a test drug, and the success probability of clinical development. If there are some safety issues, the clinical development strategy may be more complicated, and the risk of failure as well as the development cost would be higher. From a financial perspective, marketability enough to recover the possible investment may be one of the important factors for the decision making. As we mentioned earlier, orphan drugs are a component in “the smaller index category” (see Table 3). When a test drug qualifies as an orphan drug, the government provides various development incentives for the sponsor (eg, subsidies, guidance and consultation, longer market exclusivity period). It is an important option in clinical development strategy to utilize the orphan drug/medical device designation system to satisfy the unmet medical needs by providing therapeutic options for the treatment of serious diseases.
As mentioned above, there are multiple factors affecting the decision making following phase 1 trials. The safety indices are a key determinant from a safety standpoint, and in terms of efficacy, positive PD data encourage a transition of a test drug to phase 2. Financially, the return on investment is another important factor. Multidisciplinary discussion should be a critical success factor for the appropriate decision making.
Conclusion
In the present study, the phase 1 and NOAEL indices of drugs recently approved in Japan were calculated and characterized on the basis of drug attributes such as therapeutic area (ATC code), molecular features (chemicals vs biopharmaceuticals), route of administration, and indication. Our results indicated that the safety and tolerability of the drugs examined here were ensured in phase 1 at an exposure exceeding the therapeutic exposure by 3.2-fold (the median phase 1 index). The phase 1 and NOAEL indices were both affected by the therapeutic area, which might be due to the difference in unmet medical needs for certain diseases. In conclusion, this study provides a qualitative measure for interpreting the phase 1 index versus the NOAEL index and might help inform the decision-making process following the phase 1 trials.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.