
Abstract
Background:
The delay of initiation of clinical development is considered a causes of delay of approval of drugs (drug lag) in Japan.
Methods:
For oncology drugs newly approved between 2000 and 2012 in Japan, a possible impact of delay of initiation of clinical development (development start lag [DSL]) on delay of approval (approval lag [AL]) was investigated, focusing on the delay from the US timelines. The equation defining the relationship between the DSL and AL of 33 oncology drugs was calculated by using simulation models, then the Pearson coefficient of correlation between parameters was calculated.
Results:
From the analysis of all drugs investigated, a positive relationship between the DSL and AL was suggested. However, the relationship seemed to have 2 phases, including a flat phase, followed by a linearly increased phase with a breakpoint at 2340 DSL days (approximately 6.4 DSL years).
Conclusions:
Shortening the DSL is important for reducing large AL, but it is not necessary to eliminate the DSL completely for the purpose of minimizing the AL.
In the past decade, the delay in approval for new oncology drugs in Japan compared to US or EU timelines (ie, “drug lag”) has become a major concern in Japanese society. 1 It has been suggested that the drug lag consists of 3 factors, including (1) delay in initiation of development in Japan, (2) prolongation of the development period in Japan, and (3) prolongation of the review period for a new drug application (NDA). 2 It has been reported that the development period for oncology drugs in Japan has been shortened, especially for molecularly targeted drugs, with improvement of the approaches to the development of oncology drugs. 3 The NDA review time has also been shortened substantially in the last few years. The median duration of NDA review for oncology drugs in Japan in 2009 was 19.6 months for standard review and 14.4 months for priority review. In 2011, the duration was 16.9 months for standard review and 12.0 months for priority review. 4 The Pharmaceuticals and Medical Devices Agency (PMDA) stated that its target median NDA review period is 12 and 9 months for standard review and priority review, respectively. 5 This target is close to the FDA’s target review time for new drugs: 8 months for priority review (2 months’ validation and 6 months’ review) and 12 months for standard review (2 months’ validation and 10’ months review). 6 Martell et al reported that the FDA’s review time for oncology drugs is getting shorter. They investigated the relationship between several parameters and the approval time for oncology drugs in the US. 7 Kawabata-Shoda et al suggested that the initiation of clinical development in Japan is a remaining issue for the drug lag for oncology drugs. 3 Yonemori et al reported that the delay in initiation of clinical development accounts for a part of the oncology drugs’ approval lag (AL) in Japan. 1
Regarding the approved oncology drugs in Japan, most drugs’ clinical development activities started while development in the US/EU was at midstage. Hirai et al suggested that pharmaceutical companies’ strategies affected the AL. 8 Yet, there are multiple examples of oncology drugs approved in Japan with an AL <1 year, even though there had been several years of delay in the start of clinical development activities in Japan compared with the US (development start lag [DSL]). This fact may suggest that a certain proportion of the DSL can be absorbed by shortening the clinical development time or the regulatory authority’s review time of NDAs. However, there is no report of any investigation into whether an absolute elimination of the DSL is essential to resolve the AL for oncology drugs in Japan. In this study, we investigated the impact of the DSL on the AL of oncology drugs in Japan as compared to the US and discussed if absolute elimination of the DSL is necessary to seek a resolution of the AL issue without harming the productivity of clinical development of new oncology drugs in Japan.
Materials and Methods
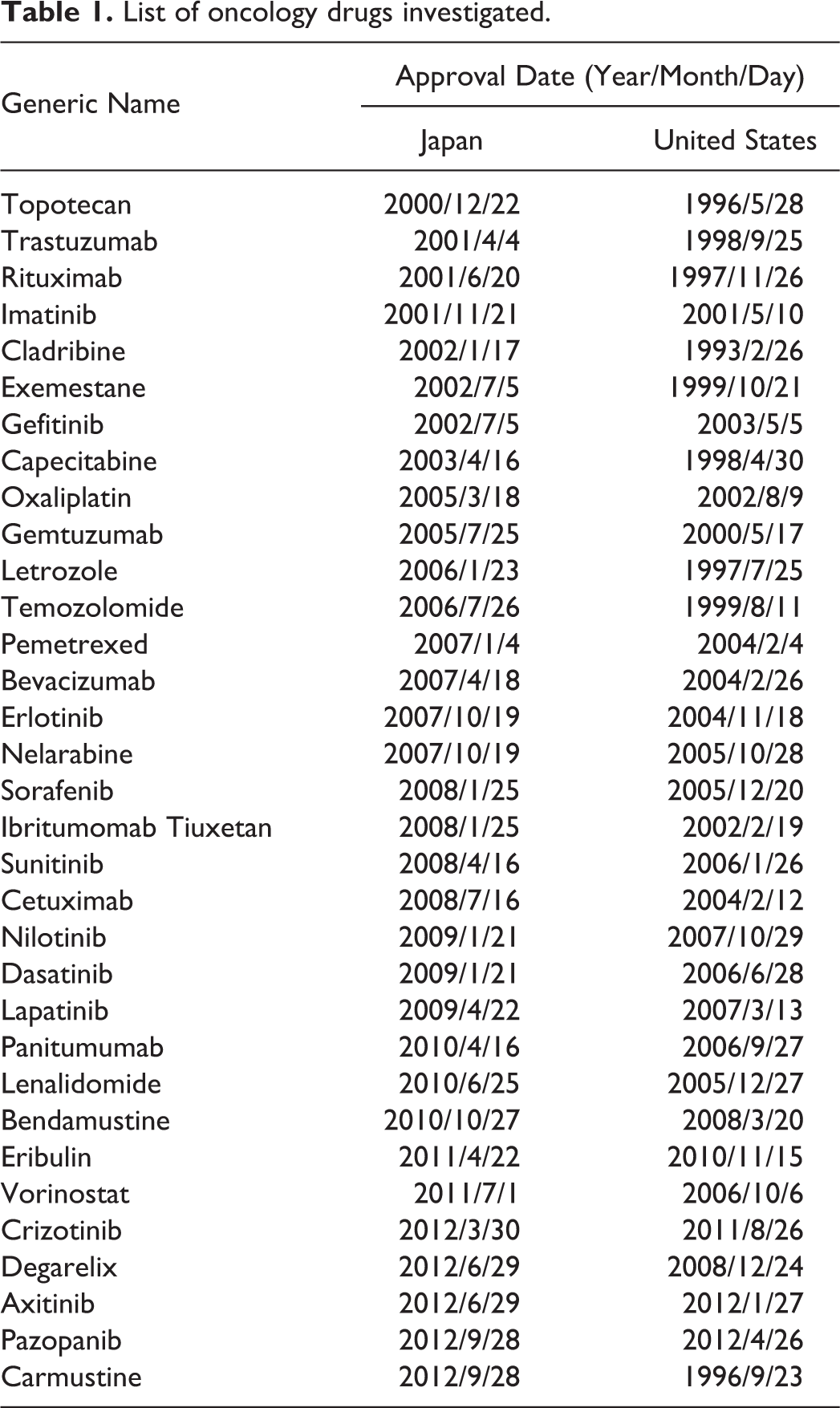
A total of 33 new chemical/biological entities for oncology indications approved between January 2000 and December 2012 in Japan were investigated. Those drugs were extracted from the listing of approved drugs of a commercial database provided by the Japan Pharmaceutical Information Center. The DSL and AL between the US and Japan were calculated. Each drug’s start time for Japan development was collected from open sources—for example, the PMDA website, 9 the media, or commercial research reports (Asuno-shinyaku, Technomics). We defined the start time of US clinical development as the investigational new drug (IND) submission date, which was collected from Drugs@FDA on the FDA website. 10 For some drugs, the IND date was not available. For those drugs, we collected the initiation date of the first phase 1 study in the US from an open source, such as the company’s website or the media. In cases where the year and month of development start could be identified but the actual date could not, we set the 15th of the month as a hypothetical development start date. Timing of submission and approval of an NDA in Japan or the US was collected from the review report at the PMDA’s website or Drugs@FDA. The development time in Japan was defined as the period between the start of clinical development and the NDA filing. Drugs that are not approved in the US or for which the development start date in Japan or US was unknown (amrubicin, azacitidine, bortezomib, miriplatin, talaporfin, tamibaloten, temsirolimus, thalidomide) were excluded from the analysis. Nelarabine was the only drug for which absolutely no clinical trial was conducted prior to submission of the Japanese NDA. Therefore, we defined the Japanese NDA date as the development start date for nelarabine.
We estimated the equations regarding the relationship between AL and DSL. When the relationship was assumed to be linear, the relationship between the AL and the DSL seemed to fit equation 1:

In addition, we formulated a hypothesis that may fit the actual data, which has a breakpoint in the slope of the correlation between the AL and the DSL. In this model, the slope was divided into 2 parts, including equation 2 (that the AL size was not affected by the size of DSL) and equation 3 (that the AL and the DSL showed a linear relationship). The breakpoint was estimated by the ordinary least squares method using the NONMEM software system (version 7.2.0, Icon Development Solutions).
Equations 2 and 3 are shown here, where T represents the breakpoint that is the upper limit of the DSL, which does not affect the AL size.


Adequacy of the model was evaluated using the objective function value (which is –2*log likelihood) provided by NONMEM.
The Pearson coefficient of correlation between the AL and each parameter—including the DSL, development time, and NDA review time—was calculated using SAS Enterprise Guide (version 4.2, SAS Institute Inc).
Results
Table 1 shows a listing of the 33 oncology drugs approved in Japan from January 2000 to December 2012 that were investigated in this study. The relationship between the DSL and the AL is plotted in Figure 1. The median DSL for all drugs investigated was 1444 days. In terms of all the plots, a tendency for a positive relationship was shown. Equation 1, assuming the linear relationship between the AL and the DSL, was estimated as follows:
List of oncology drugs investigated.
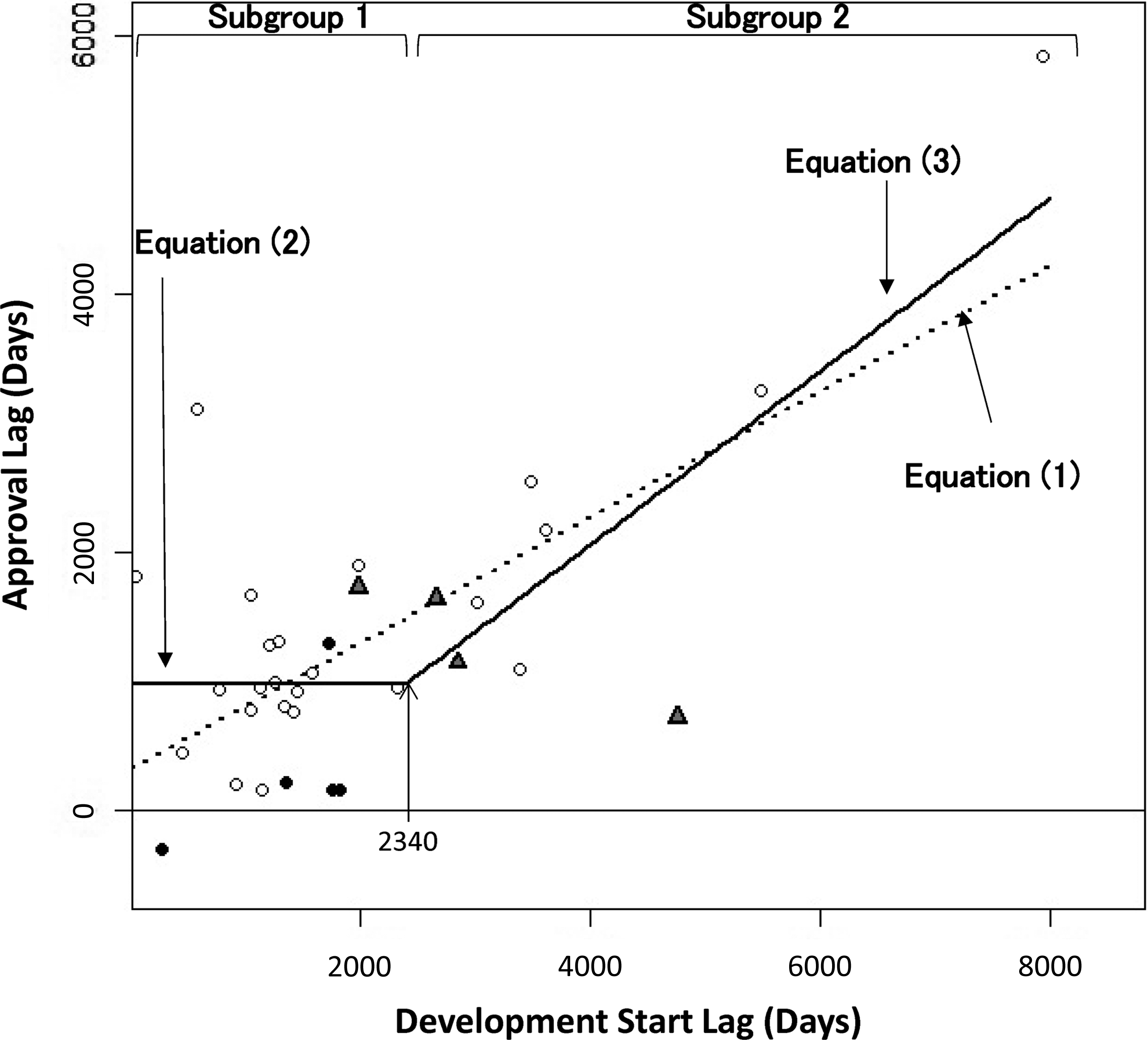
Relationship between the approval lag and the development start lag. The median approval lag and development start lag were 1065 or 1444 days, respectively. In the simple linear model, the slope was 0.488, and the intercept was 321.94 days (equation 1: dashed line). For the hypothesized breakpoint, the hypothesized breakpoint of the development start lag for the change of slope was estimated at 2340 days by NONMEM (equations 2 and 3: solid line). Closed circles show drugs that were developed under multinational clinical trials with Japan’s participation. Triangles show the drugs approved with J-P2/3 waiver. Opened circles show the other drugs.

However, we found that the plots were widely varied, especially when the DSL was relatively small. The AL seemed to increase in proportion to the DSL from about 6 years or longer of DSL. However, the relationship was less clear when the DSL was <6 years. Therefore, we considered that there were other factors affecting the AL other than the DSL, especially for drugs with a shorter DSL. Based on this observation, we estimated the breakpoint model. The breakpoint analysis in equations 2 and 3 provided T (breakpoint) as 2340 days, approximately 6.4 years. The observed 2340 days was close to the median clinical development time in the US (2163 days) for drugs investigated in this study. The slope of equation 3 was estimated to be 0.672, and the intercept was 976 days in this model.


Next, to identify the factors affecting the AL, the coefficient of correlation was investigated regarding the relationship between the AL and the factors that affect the drug lag—namely, the DSL, the development time in Japan, and the review time in Japan. All investigated drugs were divided into 2 subgroups by the hypothetical breakpoint of the DSL: subgroup 1, DSL <2340 days; subgroup 2, DSL ≥2340 days. The parameters shown for all drugs were calculated for the 2 subgroups as well.
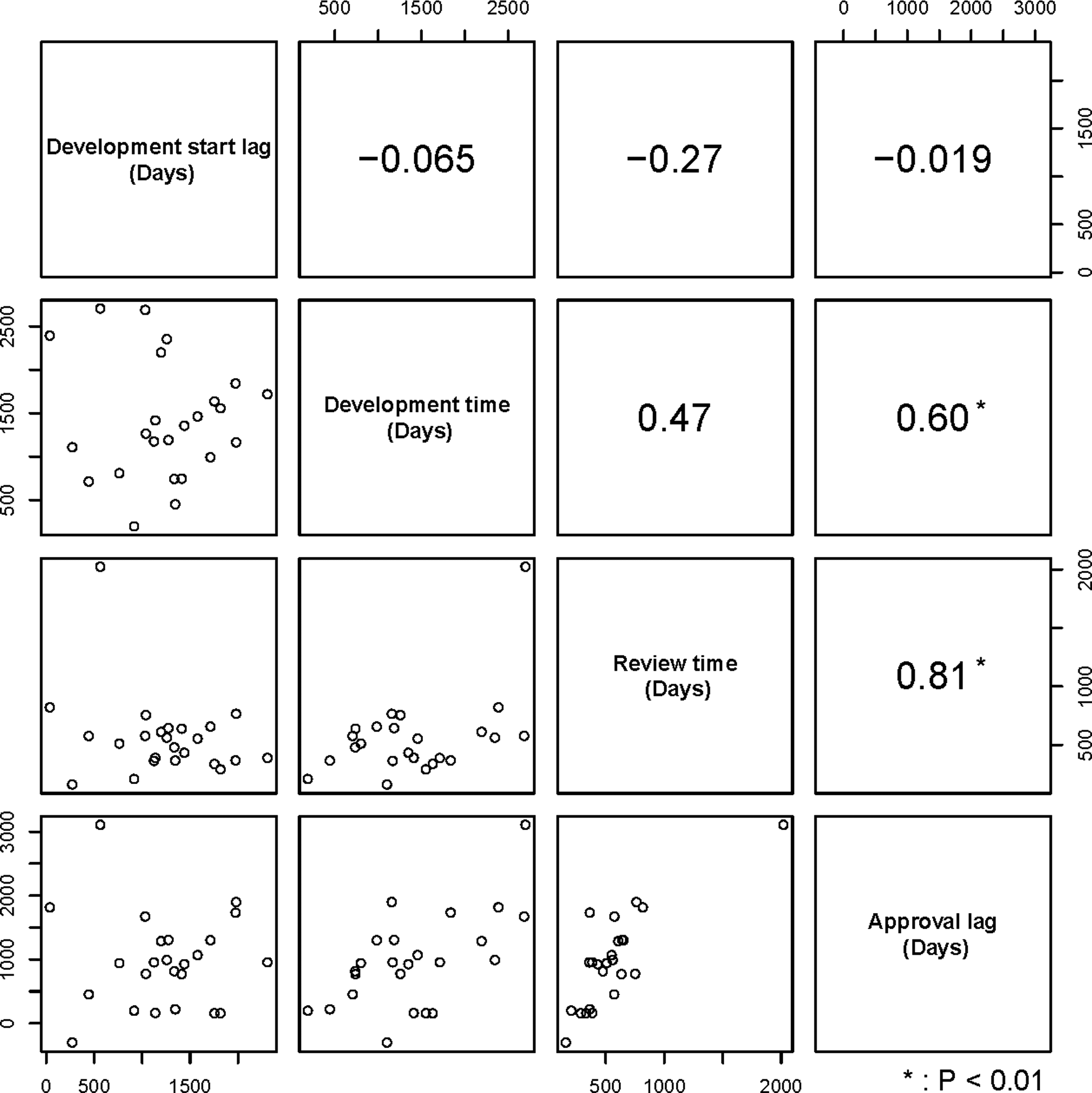
Figure 2 shows the relationship between 2 of 4 parameters investigated (AL, development time, review time, and DSL) for all drugs investigated. A positive relationship between the AL and the DSL was observed, with a coefficient of correlation of 0.69 (P < .01). Neither development time nor NDA review time showed any clear relationships with the AL. This tendency was kept in subgroup 2 (DSL > 2340 days). The coefficient of correlation between the AL and the DSL was 0.84 (P < .01; Figure 3). However, in subgroup 1, the coefficient of correlation of the DSL and AL was –0.019 (P = .9289) (Figure 4). The coefficient of correlation between the AL and Japanese development time and review time was 0.60 (P < .01) and 0.81 (P < .01), respectively, in this subgroup. This may suggest that, for drugs in subgroup 1, the impact of development time or review time in Japan on the AL was more significant compared to the impact of the DSL.
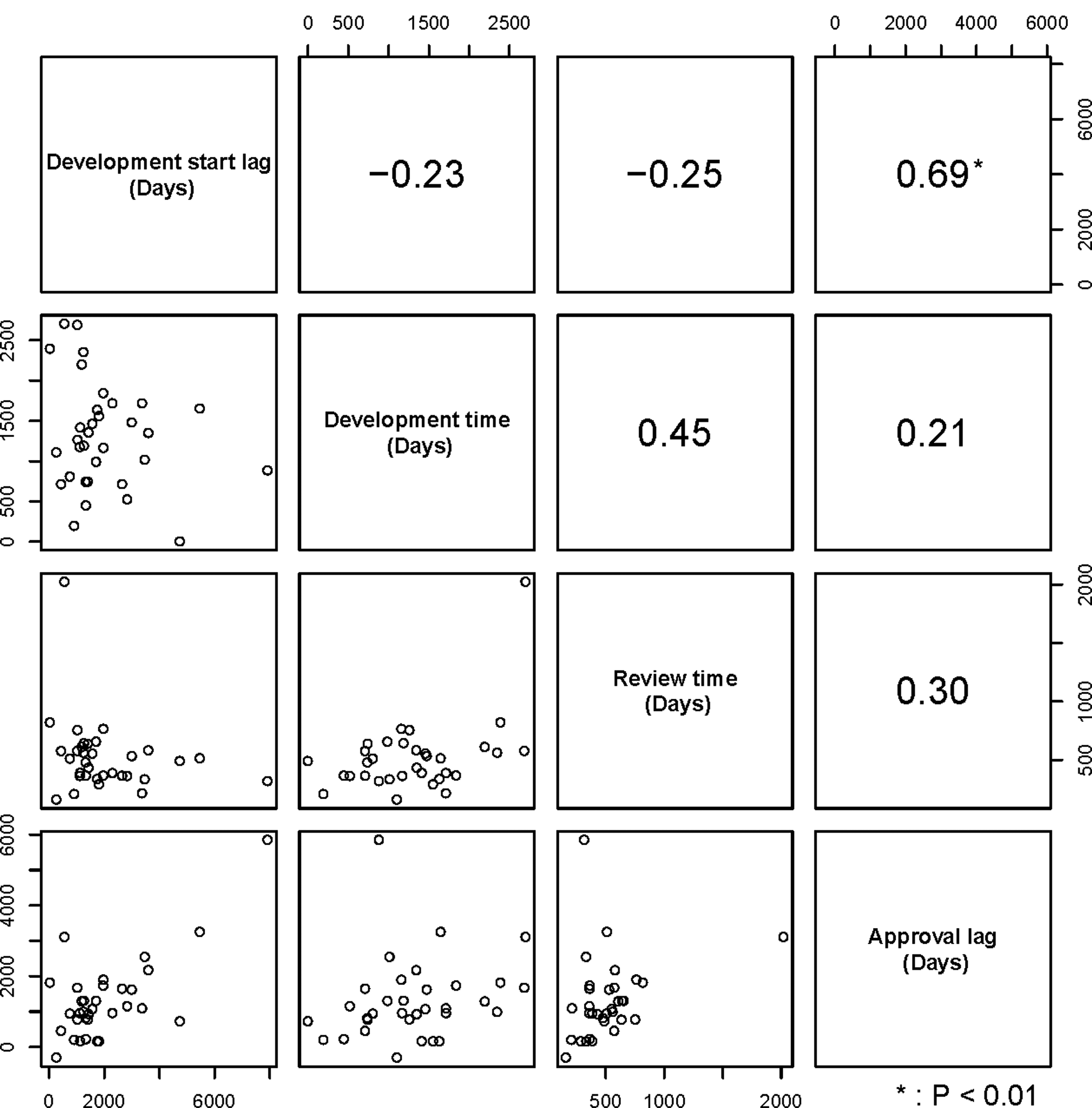
Relationship between 2 of 4 investigated parameters (approval lag, development time, new drug application review time, and development start lag) for all drugs. Coefficients of correlation between the 2 parameters and those plots are shown in the upper and lower panels, respectively.
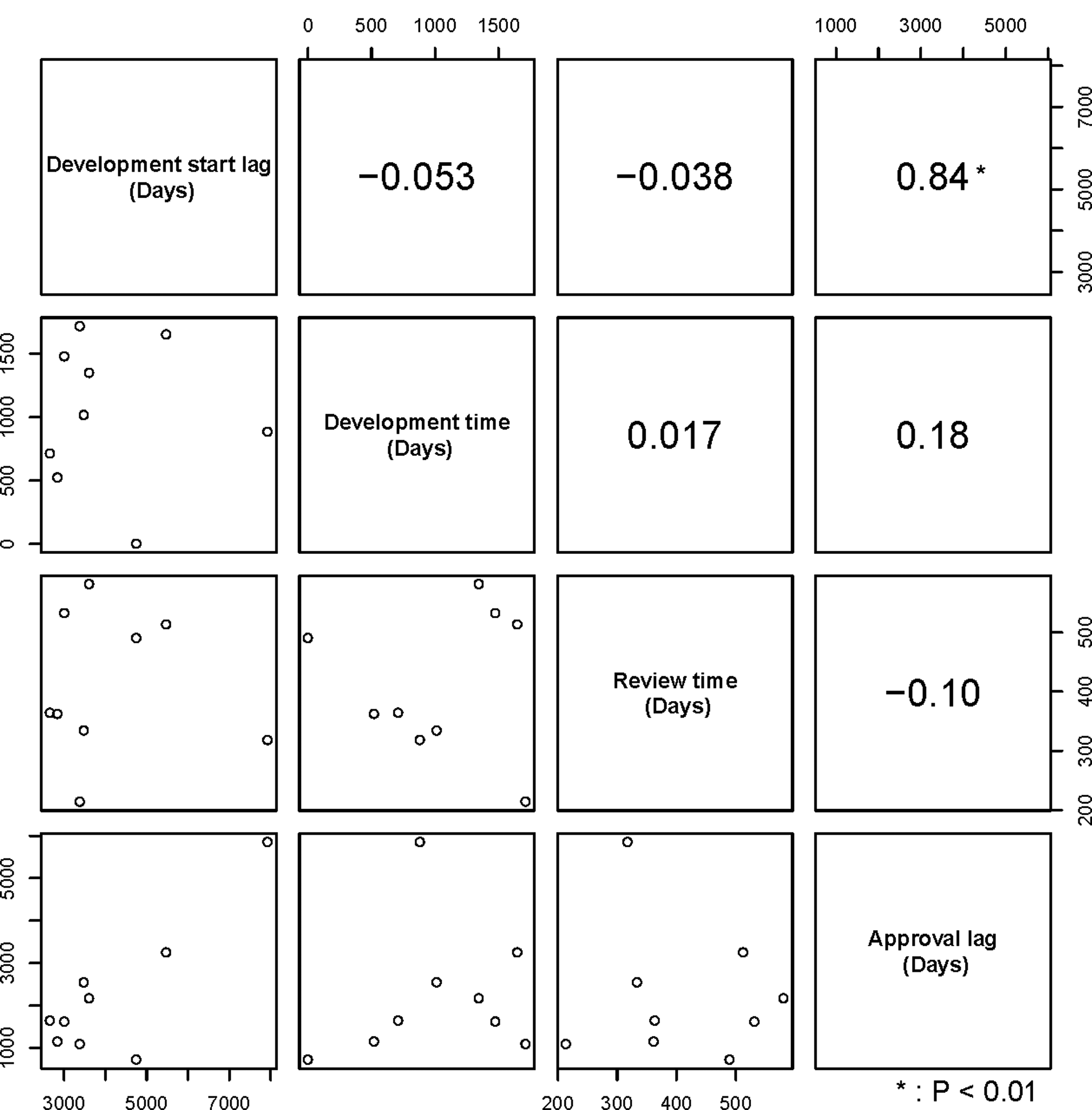
Relationship between 2 of 4 investigated parameters (approval lag, development time, new drug application review time, and development start lag) for subgroup 2. Coefficients of correlation between the 2 parameters and those plots are shown in the upper and lower panels, respectively.
Relationship between 2 of 4 investigated parameters (approval lag, development time, new drug application review time, and development start lag) for subgroup 1. Coefficients of correlation between the 2 parameters and those plots are shown in the upper and lower panels, respectively.
In subgroup 1, there were 6 drugs with an AL <365 days, including gefitinib, axitinib, eribulin, pazopanib, imatinib, and crizotinib. For 4 of those 6 drugs (gefitinib, axitinib, pazopanib, crizotinib), Japan participated in multinational phase 2 or 3 clinical trials that were included in the clinical data packages for both the US NDA and Japanese NDA (closed symbols in Figure 1). Panitumumab is another drug for which Japan participated in a multinational clinical trial, in addition to the 4 drugs described above. However, its US NDA was submitted in March 2006 before the initiation of the multinational study including Japan in May 2006, and the drug was approved in the US in September 2006 before the completion of the study. There was no other drug for which Japan participated in a multinational clinical trial as a pivotal study, among the drugs currently investigated.
The 33 drugs included 4 drugs (nelarabine, bevacizumab, lenalidmide, vorinostat) that we reported as “J-P2/3 waiver” that were approved in Japan without either Japanese phase 2 or phase 3 data in the clinical data packages (triangles in Figure 1). In the case of nelarabine, the AL was 721 days. It was markedly shorter than its DSL (4754 days). The plots of 3 other drugs (bevacizumab, lenalidmide, and vorinostat) were located relatively close to the regression line.
Discussion
Background of the DSL
The DSL has been hitherto considered as one potential reason for the AL in Japan. However, considering the high rate of failure of clinical development for new drugs, it may be difficult for pharmaceutical companies to start Japanese clinical development at the same time as the beginning of worldwide development for every candidate compound. The success rate of drug development in the clinical phase is not high. 11 Hirai et al reported that the success rate of transition of clinical development from phase 2 to phase 3 in Japan tended to be higher in cases where the initiation of clinical development in Japan was at a time of later-stage development in the US. 12
Therefore, we investigated whether it is necessary to absolutely eliminate the DSL to solve the AL challenge in Japan. Similar to the previous studies, the length of the DSL and the AL showed a positive correlation for overall drugs in this study. The median DSL for all investigated drugs was 1444 days (approximately 48.1 months) in this study. It was longer than the previous report of Yonemori et al describing the DSL compared to US/EU (38.5 months) for drugs approved between 2000 and 2009. 1 The possible reason for the different observations could be that we did not include supplemental NDAs (eg, new indications, new dosage), which were included in Yonemori’s report. The slope of the equation 1, which is the linear model, was 0.488. This means that 1 year of DSL resulted in only a half year (0.488) of AL. This is considered as the result of the efforts of industry, investigators, and health authorities to shorten the development time and/or review time in Japan. However, equation 1 suggested that the AL remains about 1 year, even if the DSL could be completely eliminated. Therefore, it is considered that factors other than the DSL might have affected the AL, at least for the drugs with a relatively short DSL.
Difference of the Impact of DSL on AL by the Length of DSL
In this study, we found that the DSL of investigated drugs ranged from 41 to 7935 days. The range was wider than development time (1-2703 days) or review time (161-2022 days). The current study suggested that the impact of DSL varied by the length of DSL itself, with a breakpoint at 2340 days (approximately 6.4 years). This value slightly exceeded the median clinical development time in the US in this study (2163 days) and the previously reported mean time of the clinical phase of small molecule antineoplastic drugs approved in the US between 1982 and 2001. 13 If the DSL exceeds the US development time, it means that there is little chance to catch up to the US NDA timeline. Therefore, it is considered reasonable to set the hypothetical breakpoint at 2340 days for the subgroup analysis. The slope of equation 3 was 0.672 in subgroup 2. If the slope could be applied to subgroup 1 as well, the value of the DSL at the point of no AL was estimated to be 887.6 days. This may suggest that if there had been no additional delay due to the development time or review time, there may be a possibility to make the AL zero, as long as the DSL was kept at ≤887.6 days—that is, approximately 2.4 years.
Possible Reasons for Discrepancy in the Relationship of the AL and DSL Between Subgroups 1 and 2
One possible reason for the discrepancy in the relationship of the AL and DSL between subgroups 1 and 2 is the presence of drugs with an extremely long DSL in subgroup 2. Those drugs may have emphasized the relationship between AL and DSL in the subgroup. However, the DSL did not show a significant correlation with AL, but development time and/or review time did, in subgroup 1. Since both median clinical development time and NDA review time tended to be longer in subgroup 1 than in subgroup 2, it might make the correlation between AL and DSL unclear in subgroup 1. For example, capecitabine’s development time and review time in Japan were 2392 and 820 days, respectively. The pivotal data for the Japanese NDA consisted of mainly Japanese clinical trials, since the dosages were different between studies in Japan and other countries. As a result, the AL of the drug was 1812 days, even though the DSL was only 41 days.
In the case of letrozole, its development time and review time in Japan were 2703 and 2022 days, respectively. Letrozole’s dosage for Japanese patients was also determined in Japan independently in the original NDA. However, the Japanese regulatory authority required the manufacturer to conduct an additional high-dose clinical trial in Japan after Japan’s NDA submission, to reevaluate its dosage in Japan in line with the overseas/global dosage. As a result, the NDA review time became very long and resulted in its AL of 3104 days.
Those cases may suggest that the development strategy (eg, Japanese dosage, clinical data package) makes a big impact on the AL rather than the DSL, especially for the drugs with relatively shorter DSL.
Various efforts have been made by investigators, industry, and health authorities to shorten the development time or NDA review time. For example, the Ministry of Health, Labour and Welfare has established a committee to evaluate and recommend accelerating the development of clinically important unapproved drugs. 3 For oncology drugs, the clinical data package requirements for the NDA may be modified depending on the clinical significance of the investigational drug. 14 Further positive discussions are expected among academia, industry, and health authorities to improve the oncology drug development environment.
For 4 of 6 drugs in which the AL was <1 year, Japan has participated in multinational phase 2 or phase 3 clinical trials. There was no drug with an AL >1 year where a multinational clinical trial was included in the Japanese NDA as pivotal data, except for panitumumab. In the case of panitumumab, Japan participated in the multinational clinical trial after the submission of its US NDA. This may suggest that Japan’s participation in multinational trials is an effective strategy to reduce the AL in Japan, rather than attempting to completely eliminate the DSL. Two drugs (imatinib, eribulin) were approved with a relatively short AL but did not used multinational trials for Japan’s NDA. Imatinib was approved before publication of new Japanese guidance encouraging participation for multinational clinical trials from Japan. The Japanese NDA review document for imatinib states that the drug could be a cutting-edge drug and that the Japanese NDA before completion of the ongoing phase 2 clinical trials was acceptable. Eribulin’s Japanese NDA was submitted on the same day as the US, by using a kind of “bridging strategy” consisting of the overseas phase 3 data and the Japanese phase 2 data. This approach is considered an effective option to catch up with the EU/US development.
In the case of eribulin, the NDAs in the US and Japan were submitted on the same day. However, its AL was 158 days. It is attributed to the difference in the review time in the US and Japan. The crizotinib case was similar. The Japanese NDA was submitted on the next day after the US NDA, and its AL was 217 days. These cases may suggest that not only DSL but also length of review time is still one of important factors affecting the AL. The reason why nelarabine’s AL was shorter than other drugs with a J-P2/3 waiver was that all Japanese clinical trials before the NDA were waived. The 4 drugs that received a J-P2/3 waiver were granted fast-track designation in the US. This means that the AL of those drugs could be longer, if those drugs had to conduct Japanese phase 2 or 3 trials.
We tried to estimate the equation in the breakpoint model, excluding 9 drugs that used multinational clinical trials or a J-P2/3 waiver, as “nontraditional” development models. As a result, the program failed to converge for the model with a breakpoint but converged successfully for the linear model (data not shown). A possible reason of this is that the revised sample size may have become too low for an appropriate estimation of the breakpoint model, due to the exclusion of the 9 drugs. Another possibility is that the drugs with a multinational clinical trial or J-P2/3 waiver acted as important factors to set the breakpoint, by making the AL short compared to the DSL.
Although there may still be a challenge for the PMDA to review the global clinical trial data, 15 Ueno et al reported that the lag of NDA timing in Japan from the US was markedly shorter for the drugs that were developed with global clinical trials involving Japan based on the analysis of the drugs of all therapeutic areas that were approved in Japan between 2007 and 2012. 16 This finding is consistent with our study results.
This study has some limitations. For some of the drugs approved in the investigated period, we could not find the timing of IND submission or the timing of the first study in Japan. Those drugs were excluded from the investigation. This study investigated oncology drugs approved in Japan between 2000 and 2012. However, the recent oncology drug development timelines have been further shortened. Therefore, the acceptable DSL may have been shortened further for the latest approved oncology drugs.
Conclusions
The results of this study suggest that shortening a large DSL is important for reducing the AL of oncology drugs in Japan, but it is not necessary to eliminate the DSL completely to minimize the AL. Participating in multinational clinical trials may be an effective approach. Companies developing oncology drugs are expected to devise a strategy to accelerate the development timeline of their drugs by using the above mentioned approach.
Footnotes
Acknowledgment
We appreciate Natsu Fujita for providing data about the date of beginning of first study in Japan. We also appreciate Masahiro Hayashida for help with data analysis. We are deeply grateful for the advice of Dr Hisashi Urushihara on the analysis of the data. We express our deep gratitude for support and advice from Dr Toshio Suwa especially regarding the discussion section.
Declaration of Conflicting Interests
Keitaro Nakajima, Ramzi Dagher, and Laurie Strawn are employees of Pfizer Inc. The other authors declared no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.