
Abstract
In a rapidly changing health care environment, it is more important than ever that pharmaceutical manufacturers improve the quality and efficiency of their research and development efforts in order to help ensure the right drug gets to the right patient at the right time. The evolving role of the Medical Affairs, Health Economics & Outcomes Research (HEOR) and other functions engaged in evidence generation within the pharmaceutical industry is leading to earlier involvement in the clinical development process so that the proof of concept for new therapies can be more strongly linked to the proof of medical value. In this article, the authors outline key components of an Early Engagement Model that connects the proof of concept to proof of medical value through a systematic approach linking molecular profile with early insights on disease, unmet needs, stakeholder requirements, and patient-centric differentiation.
Introduction
The health care landscape is rapidly changing on many fronts. Decision makers such as payers and health technology assessment (HTA) bodies continue to evolve their evidentiary requirements for coverage and payment of new medical technologies. Stakeholders such as physicians and provider organizations (ie, accountable care organizations) are now facing quality, efficiency, and cost issues. 1,2 In some situations, this has led provider groups to publicly challenge the pharmaceutical industry on the prices for new therapies. 3,4 Organizations such as the Critical Path Institute 5 and the Patient-Centered Outcomes Research Institute 6 are appropriately increasing the influence of the patient perspective in the drug development process. Regulatory requirements are evolving, with expedited programs for drug development (eg, fast track, breakthrough therapy, and accelerated approval) that in many cases are leading to compounds moving directly from Phase 1 to Phase 3. 7 -11 With the advent of precision medicine, increasingly, clinical trials are enrolling niche populations that require a depth of information related to disease biology. 12,13 From an overall research and development (R&D) perspective, this changing landscape highlights the increasing need to get the right drug to the right patient at the right time.
To meet this challenge, pharmaceutical manufacturers need to proactively improve their approach to designing and generating evidence through clinical development programs and be more efficient with their R&D spending. The inclusion of early and extensive real-world analyses, insights, and strategic planning will allow the pharmaceutical industry to select the right patient population, understand the patient journey, choose appropriate comparators, and design and implement relevant and meaningful endpoints that can address true unmet needs and link innovation to real patient benefit. Below we provide examples where manufacturers have not been as successful with their trial programs as intended: In 2012, Germany’s Joint Federal Commission (G-BA) gave an indication of “minor benefit” to Almirall’s cannabis sativa drug (Sativex), which was indicated for symptom improvement in patients with moderate to severe spasticity due to multiple sclerosis. The G-BA noted that the manufacturer did not define prior therapies nor identify (ie, factor out) the patients from the overall study population who had not responded to prior therapy. Thus, there was uncertainty about the total number of eligible patients. The consequence? The manufacturer was given 3 years to conduct an additional study against optimized therapy in patients who have failed prior therapies.
14
In 2015, the G-BA ruled
15
that ibruitinib (developed jointly by Pharmacyclics [acquired by AbbVie in May 2015] and Janssen Biotech) had an “unquantifiable added benefit” due to the lack of a comparator arm in the clinical trials. The manufacturers had not included a comparator arm in the drug’s trial as they believed the overall response rate from a single-arm design would suffice. A recent analysis of reasons for recommendation and rejection by the United Kingdom’s National Institute of Health and Clinical Excellence identified each of the following as being common reasons for drug appraisal rejections: failure to use appropriate comparators, study population not reflecting the intended population in clinical practice, and inappropriate endpoint measures used.
16
In today’s drug development and commercialization environment, innovations being promoted by pharmaceutical manufacturers are not routinely linked to stakeholder expectations, especially those of payers, providers, and patients. There are several barriers to knowledge transfer that exist between “the bench and the bedside.” 17 Sean Tunis 18 describes the delay in the transfer of knowledge in terms of a “molecular basis of uncertainty” (see Figure 1). In this model, research on new drugs is driven primarily by the scientific interests of investigators, who typically are not aware of the needs of decision makers, or may consider needs based on a proof of concept rather than proof of medical value. In this situation, there is a strong focus on regulatory approval and not enough emphasis is placed on product differentiation and relative medical value that will be meaningful to decision makers. One clear portrayal of such continuing trend is that even in an era of greater patient centricity, patient-centric (both humanistic and economic) endpoints that can help further delineate product value and demonstrate the impact of product on patient benefit are still often not employed in randomized controlled trials. 19
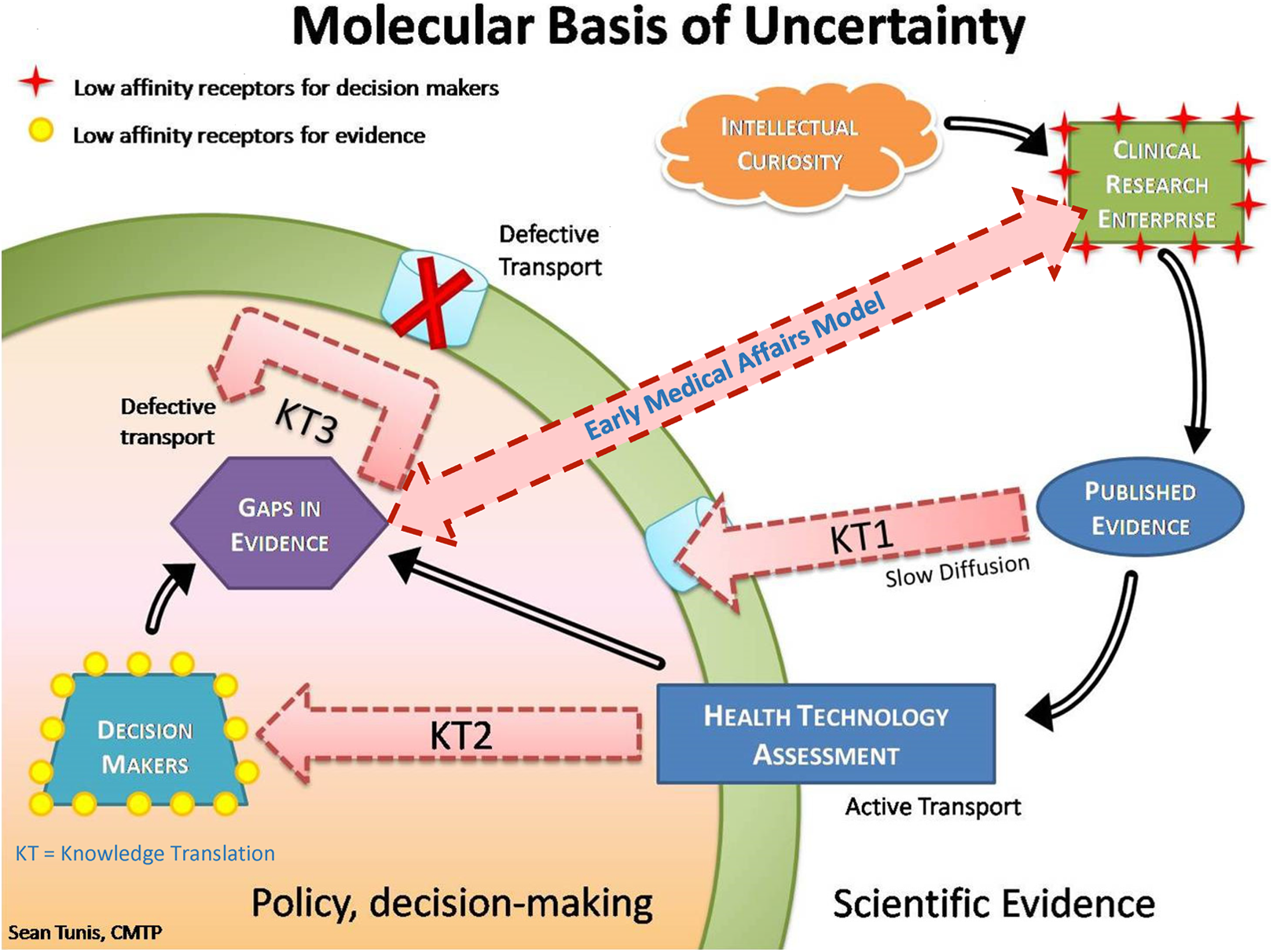
Molecular basis of uncertainty. Image adapted from Tunis. 18 Reproduced with permission.
Traditionally, insight-gathering and evidence-generation strategies are developed in silos across the Medical Affairs (MA) and Health Economic & Outcomes Research (HEOR) functions, and is primarily focused on the late stage of development and commercialization. The HEOR function is mostly centered on payer-related evidence and tools, whereas the MA function typically manages key external expert relationships, drug-related medical information, and publications, as well as supports Phase 4 evidence generation. However, the business model is changing rapidly, 20 whereby continued regulatory pressure on drug promotion and compliance has shifted many responsibilities to the science functions, and at the same time these functions are facing pressure to ensure and harness an evidence continuum, relative medical value incorporation, and real-world evidence needs in the earlier stages of drug development. In parallel, patient centricity has become an increasingly important element in the pharmaceutical industry's business model, and it requires a highly integrated, end-to-end, evidence-based approach, with core scientific functions needing to be working early on in seamless resonance to influence the patient value chain.
In light of this fast-changing landscape, the pharmaceutical industry needs to adopt a highly integrated evidence-generation strategy that is aligned and coordinated across MA, HEOR, and other evidence-generation entities and initiated early on in development to enhance the organizational effectiveness and R&D decision confidence. Early engagement should be representing a larger, broader set of stakeholders spanning providers patient and payers, and systematically bridging collective external insights from these stakeholders into the strategic planning processes and tactical execution frameworks. This is typically not the case today, where traditionally most of the MA and HEOR focus starts to build in Phase 3 of development, when opportunities to harness learning and influence evidence generation is quite limited.
The Evolving Role of MA and HEOR in Clinical Development: An Early Model
In considering the evolving role of the MA- and HEOR-related functions and the efforts required to shape R&D’s efficiency and value chain, an Early Engagement Model framework is proposed that is geared toward improving the efficiency of evidence continuum in R&D and maximizing the medical value of innovation. The guiding principles of the Early Engagement Model include the following.
First, the proof of concept is linked to proof of medical value
Value can be defined as the achievement of improved patient health outcomes (ie, clinical, patient-reported functional and/or overall health status), generally in the context of cost/resources used. 17 It is imperative that the innovation being driven by today’s early development science is relevant to the unmet needs of real-world stakeholders, which besides regulators now also include patients, providers, and payers (the 3Ps). Thus, key aspects/decision points of the clinical development program must be assessed early to ensure proper alignment of target product profile (TPP) to those unmet needs, especially those coming from the patient/payer perspective, as both of these stakeholders have an expanding role in assessing product value in today’s health care environment. The key decision points from a framework perspective in this regard include actual design of trials, the target patient population, the relevant treatment comparators, and the appropriate endpoints/outcomes. MA and HEOR functions need to work seamlessly, utilizing their broad-based capabilities to provide targeted input into trial design and R&D strategy. In parallel, these functions need to develop channels of evidence/insight sharing from an extended stakeholder platform (ie, the 3Ps) for early and effective 2-way communication between the bedside and the bench. 17
Second, the evidence base has to be assessed and incorporated early
Gaining a thorough understanding of a disease area is becoming more complex with large amounts of information/data available to review, synthesize, and distill, both from a disease biology and personalized medicine perspective. The evidence base (both stakeholder insights and evidentiary requirements, plus knowledge of disease, treatment landscape, patient journey, and unmet needs) has to be collected, assessed, and incorporated at the time of Phase 1/2 to allow for the creation of a relevant early TPP that can guide the optimization of the Phase 3/4 program. Once a drug reaches Phase 3, the opportunities to influence evidence generation, target population, or patient-centric value pathway become very limited. As an example, in many disease areas there exists a significant gap in the knowledge of the patient journey. This is due in part to new technologies (eg, genomics) that now allow for identification of certain disease pathways and niche patient populations that previously went undetected. Thus, in many cases we know little about how different diseases or particular patient populations within different diseases are identified and treated and what are key outcomes—all factors that are critical to the strategy and design of a clinical development program.
An early understanding of the foundational epidemiology, disease burden, patient journey, and stakeholder insights helps increase confidence that the clinical program and the medical/commercial strategies developed are insight driven and that the innovation will drive real value. The organization also gains from efficiencies in evidence planning and the ability to put limited resources in the right places. Finally, this approach helps to improve partnerships with key external stakeholders and bridge the gap between internal and external stakeholders.
Third, the structure is lean and efficient
Traditionally MA and HEOR teams have been composed of very specialized individuals focusing on specific roles (eg, publication planning, communications, real-world evidence, economic modeling, patient-reported outcomes, expert engagement). In the Early Engagement Model, the need is for a few individuals with strategic acumen, end-to-end evidence generation experience, and multidimensional expertise broad enough to assess a wide range of evidentiary needs (eg, target patient population, appropriate humanistic endpoints) that are all critical to ensuring a strong clinical development program.
Based on these guiding principles and today’s health care requirements, the Early Engagement Model delivers 5 focused components that can be established by any organization in the early space to influence value-based end-in-mind clinical development. These 5 components are Evidence synthesis of the disease Mapping of the patient journey to identify barriers to care and assess patient experience from diagnosis to experiencing an health outcome Linking and translating molecular profile to patient benefit/patient-centric differentiation A clear evidence-based foundation of early TPPs followed by continuous TPP risk mitigation Digital expert engagement
The Components of the Early Engagement Model
The Early Engagement Model is composed of 5 distinct components that have unique impacts on TPP development and the evidence continuum starting early in development (see Figure 2 for overview of model). Each component is described in detail below.
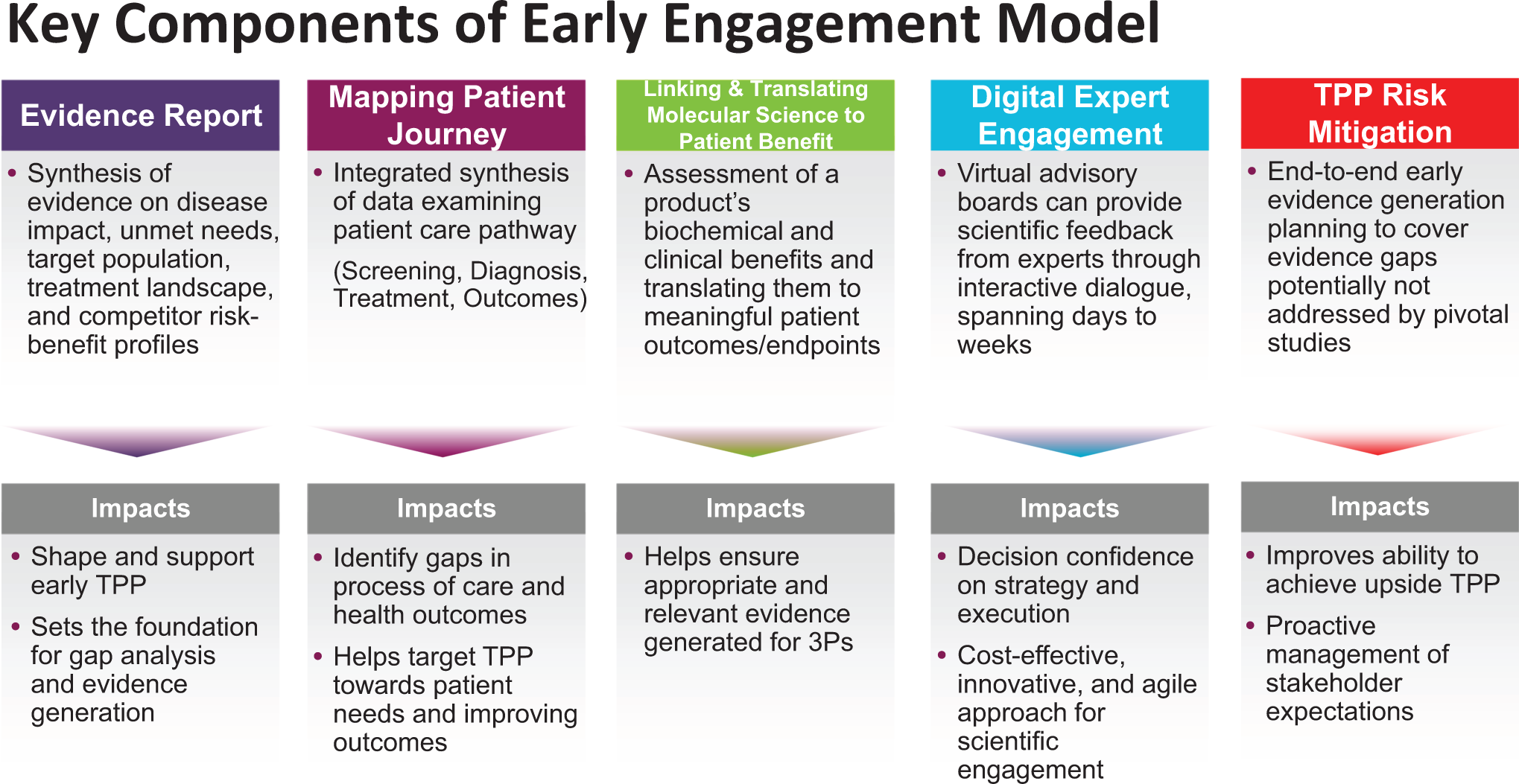
Overview of the Early Engagement Model.
The medical evidence report
A structured medical evidence report represents the first step toward development and refinement of the TPP, competitive differentiation, and value enhancement. An evidence synthesis centered on the target population, treatment landscape, comparators’ benefit/risk profiles, clinical/economic/humanistic burden of the disease, and HTA landscape provides a well-rounded strategic base to guide TPP development and preliminary gap assessment from a 3P stakeholder perspective. Preparing such a medical evidence report requires review and synthesis of emerging science, existing product and disease materials, plus a targeted literature search focused on the components of TPP including current treatment impact and health outcomes. The report output should address key questions regarding the disease area through specification of unmet needs, the clinical, humanistic, and economic impact, epidemiology, patient segmentation, treatment guidelines, and benefit/risk attributes across key comparators.
Learnings from the evidence report are shared by MA and HEOR leaders across matrix teams to (1) apprise internal stakeholders of the true positioning of unmet needs from a patient population and endpoint perspective and (2) systematically create consensus toward the development of a fully aligned early-phase TPP, especially in terms of target population, choice of comparator, selection of endpoints, and desired effect sizes. Separately, the report with its bibliography also serves as an evidence repository needed in the early stages of a clinical program for evidentiary inquiries and as a key reference document for internal stakeholders including country affiliates.
Mapping the patient journey
The foundation for a strong patient-centric development/commercial strategy is built by the comprehensive mapping of the patient journey. Given the confluence of factors affecting the patient in today’s health care environment along with the focus on personalized medicine, it is important to gain an in-depth understanding of the diversity in patient population, their experiences/barriers in navigating the health care system, health outcomes with current medications, and patient expectations attached to any new treatments on the horizon. All the relevant questions and information around the patient experience and unmet needs have to be identified early in Phase 1/2 of a clinical program so as to provide enough time for the clinical and commercial teams to harness the learnings toward the Phase 3 pivotal trial and launch plan.
Hence, mapping the patient journey is a critical component of the Early Engagement Model that begins with the identification of the stages that patients experience from disease awareness to diagnosis and treatment to empowerment (see Figure 3). Traditionally, MA and associated groups have relied on primary research (eg, patient focus groups, physician interviews) as the main data source for constructing the patient journey, but this approach is no longer adequate given the lack of depth and representativeness in the approach and related outputs. With the advancement in real-world evidence, social media, Big Data development, and analytics, it is now possible to gain in-depth understanding of the patient journey dynamics spanning key markets, and perspectives that are uniquely relevant to the patients. MA and HEOR teams need to evolve their approach and enhance their evidentiary acumen to understand different dimensions of Big Data and its related applicability to mapping the patient journey. On the application side, once the map of the patient journey sheds light on the standard of care (SOC), important treatment drivers and barriers, gaps in care, and patient preferences, the teams need to develop the strategic acumen to systematically apply the findings toward trial design as well as clinical and commercial decision support.
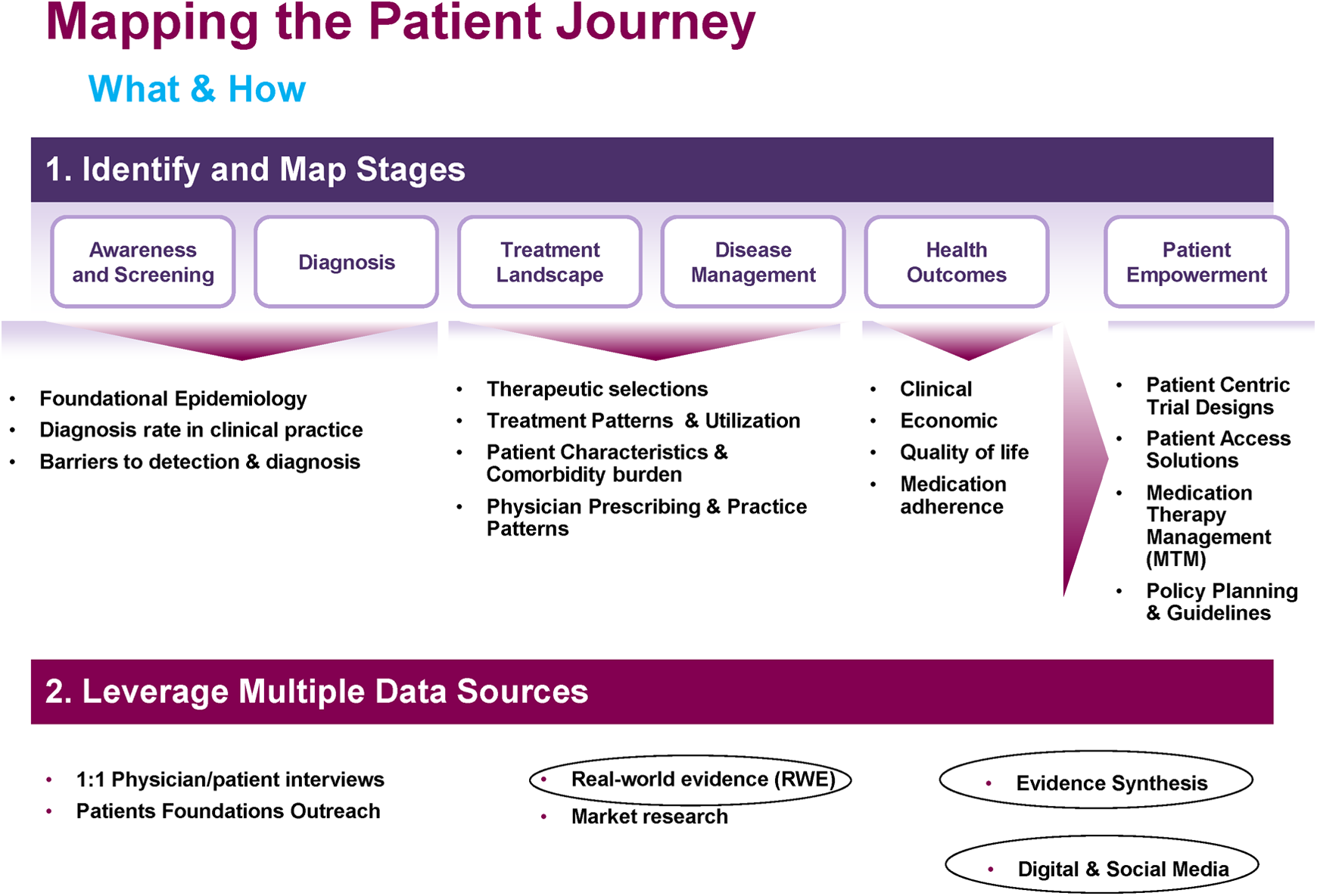
Mapping the patient journey.
As a recent example, an MA/HEOR team working on a compound in Phase 2 development to treat a neurodevelopment disorder in a pediatric patient population (6-17 years) embarked on a rigorous in-depth exercise to map the patient journey through Big Data (real-world evidence + social media) sources. Substantial underdiagnosis, comorbidities (attention-deficit hyperactivity disorder [ADHD], obsessive compulsive disorder [OCD]), polypharmacy (antidepressants, anxiolytics), a different SOC compared to treatments approved by the Food and Drug Administration (FDA), and marked decrements in quality of life (QOL) were observed as part of the patient journey output. The learnings were systematically applied toward a more naturalistic Phase 3 trial design that included a broad patient population including ADHD/OCD comorbidity subgroups, a co-primary QOL endpoint to address patient needs, addition of a third arm in the trial that added the identified SOC in addition to the FDA-approved treatment arm, and secondary endpoints to evaluate and demonstrate no adverse impact on ADHD/OCD outcomes for the patient population. Similarly, learnings from the patient journey were applied to launch planning, especially in terms of the forecast, scope of market conditioning programs, and patient access solutions. Evidence coming out of such an improved naturalistic Phase 3 trial is in a fundamentally better position to address real-world unmet needs of the patients, and to have the potential to deliver a broad-based optimized product label, preferred access, and reimbursement.
Linking and translating molecular science to patient benefit
Linking molecular science to patient benefit requires conceptualizing a health outcomes assessment strategy and endpoint development process that is centered on the benefits of therapy from the patient perspective. Early on in clinical development it is important to assess—and enhance understanding of—what will move the needle for decision makers/stakeholders with respect to patient-centric health outcomes. This assessment needs to be robust and to provide an optimal integration of insights from the 3Ps on product value. Serving as a focal point from an external stakeholder perspective, MA and HEOR functions are responsible in today’s environment to bring these collective insights by working systematically with the commercial groups, payer teams, and key affiliates in major markets.
After the 3P insights have been collected, a cross-functional exercise is conducted with the clinical development team scientists and patient-reported outcome (PRO) experts to assess, map, and link the mechanism of action to the ultimate patient benefit (see Figure 4). The initial step is to link the mechanism of action to the disease process, followed by a delineation of the actual clinical impact of the disease process in terms of signs and symptoms. The next step in the process is the systematic translation of potential patient benefits into meaningful outcomes and endpoints to be assessed in the trial program.
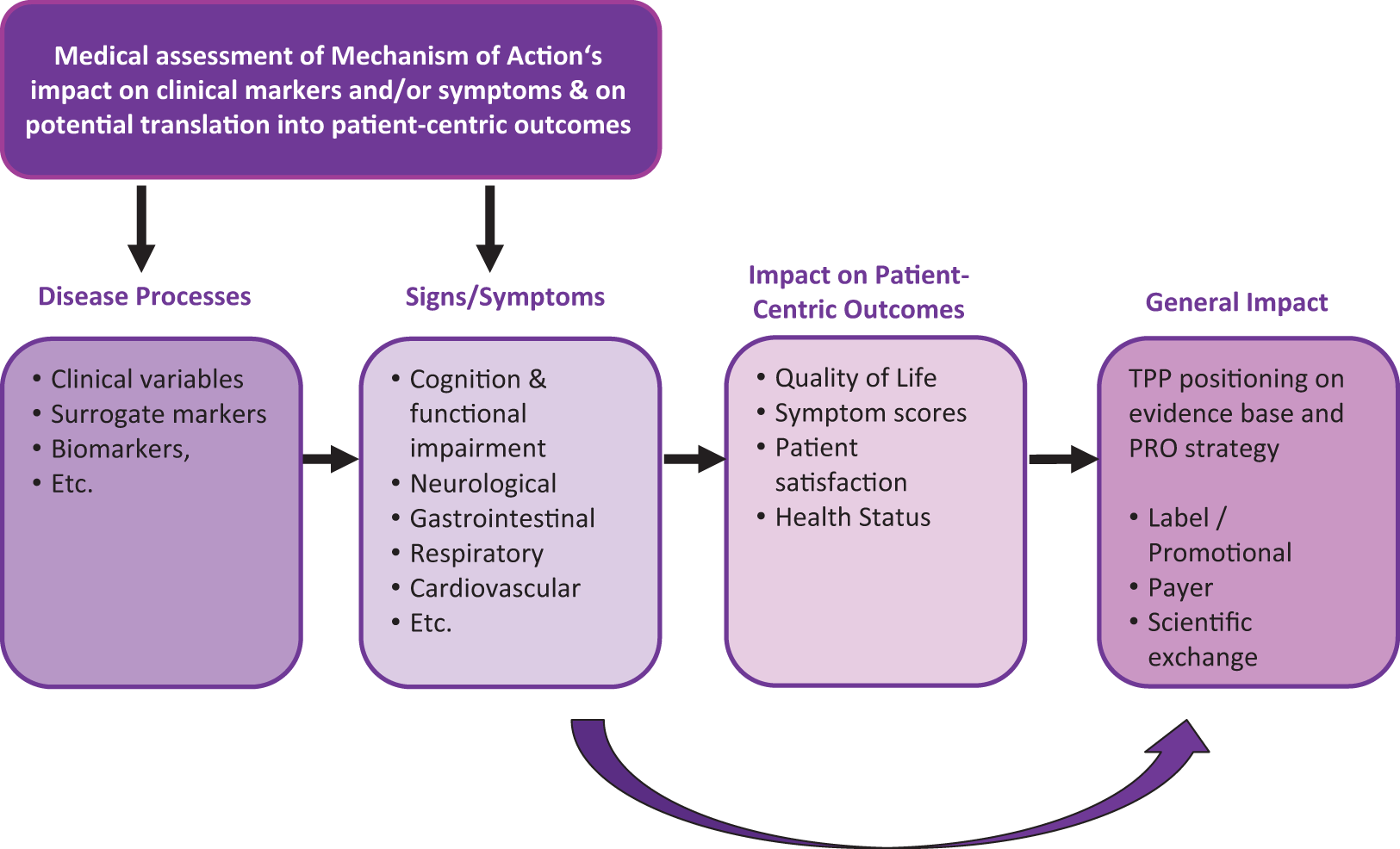
Linking and translating molecular science to patient benefit.
An important example of the linking and translating process is the development of PROs. There remains a lack of up-to-date, reliable, validated, and patient-centric PRO measures that are accepted by regulatory agencies. While existing measures are psychometrically sound, they mostly do not suffice, given the standards set forth by the FDA guidance on PROs, 21 in terms of needed validity and reliability. Successful PRO measures are those that were scientifically developed and validated in specific alignment with the disease biology/product profile; the development of such fit-for-purpose PRO measures needs to start early in Phase 1/2 to scientifically shape and finalize a claim-based endpoint strategy for Phase 3 programs (see Figure 5). The Early Engagement Model provides a platform for developing a fully integrated end-in-mind PRO strategy and strategically incorporating the patient benefit into clinical programs with label implications.
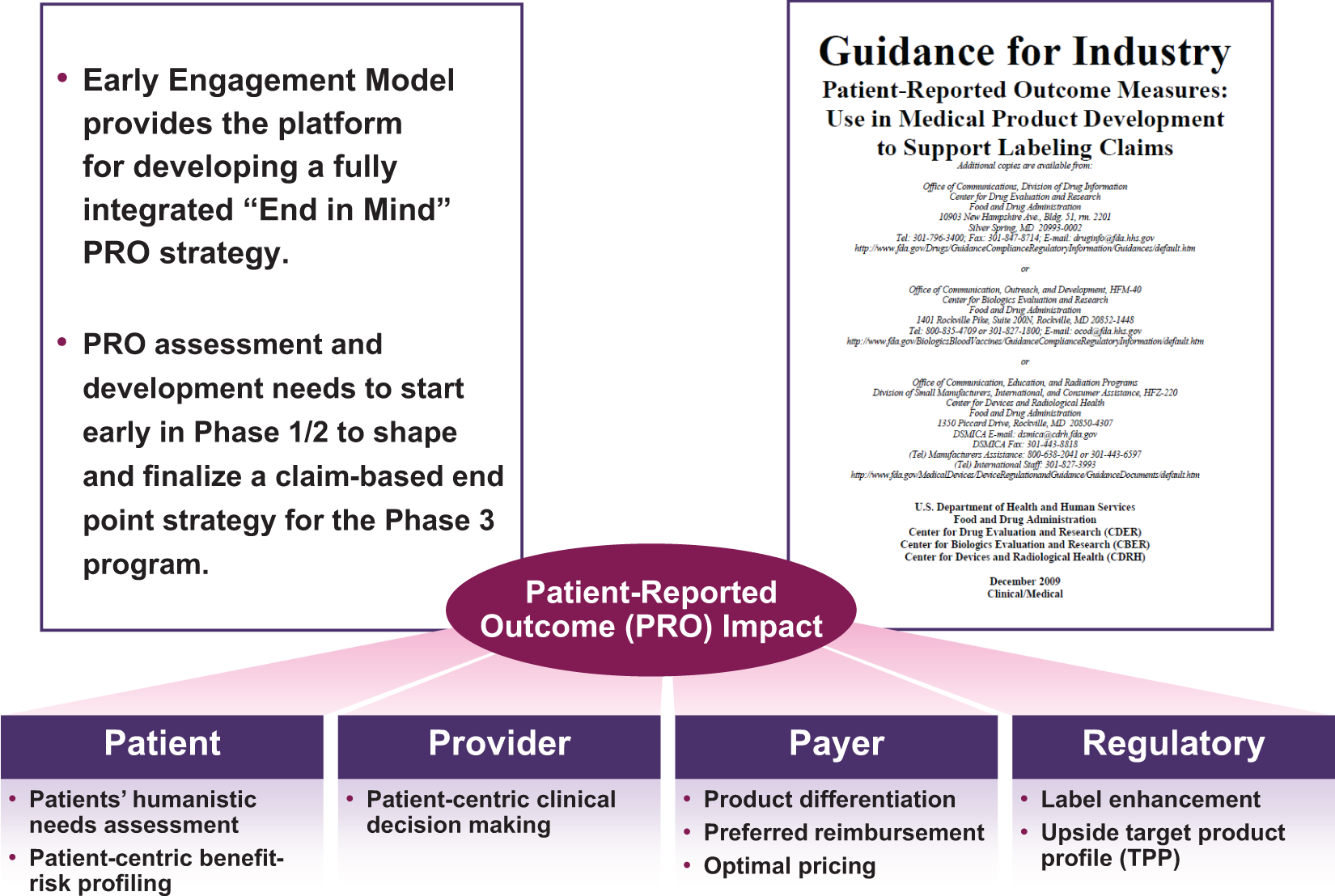
End-in-mind patient-reported outcome strategy.
Digital expert engagement
Scientific engagement with physicians and science experts is a cornerstone of every medical strategy and tactics development. In the early R&D space, given the increasing number of molecules with uncertain proof of concept and limited medical resources at hand, there is a need to rely on efficient and flexible engagement models that can provide relatively quick and cost-effective expert input and validation on an array of scientific inquires all along the early development cycle. In that regard, harnessing digital technologies for physicians’, payers’, and other stakeholders’ outreach can provide cost-effective, innovative, and agile solutions for scientific engagement and should be adopted as a mainstream method of soliciting expert input in early development. One example is virtual advisory boards, which can represent a dynamic platform for engaging a multidisciplinary spectrum of experts (including key clinical opinion leaders, policy makers, patient advocates, and lead researchers) on specific topics or questions of interest at a fraction of the cost of a traditional advisory board. With such platforms, experts can offer scientific feedback on a quick and recurring basis throughout the early development of a molecule through interactive dialogues spanning several days to weeks. This approach provides the thought leaders the flexibility of engaging at their own time and pace, with 24-hour accessibility, and outreach for expert input can be initiated any time in a quick and compliant fashion whenever there are important pending inquiries to be addressed.
TPP risk mitigation
As an annual or biannual exercise, TPP risk mitigation allows for the TPP to be updated on a regular basis, in the light of the evolving science, competitive landscape, and evidence gaps from a 3Ps perspective. Changes in competitive landscape with new data or additional evidentiary requirements in relation to feedback from the regulators or payers can render an ongoing Phase 3 program inadequate for launch success or optimal reimbursement. Led by the MA/HEOR team, this cross-functional exercise can have the mandate to evaluate TPP claims (clinical, economic, patient-centric) in relation to the current developmental strategy and clinical program, and to devise specific recommendations to address any emerging evidentiary gaps that need to be plugged in order to achieve sustained competitive advantage. This exercise can be approached from various angles including proposing Phase 3b/4 studies, real-world evidence and observational studies, health economic modeling, etc with the goal of broadening the label (eg, endpoint spectrum, comparator choices, enriching targeted subpopulations) or generating payer-centric evidence.
As an example, an MA/HEOR team supporting the medical strategy and evidence plan for a new diabetes therapy learned through targeted expert/payer engagements and patient journey exercises that nocturnal hypoglycemia may have a larger impact on patient function and QOL than previously thought. As part of a TPP risk mitigation exercise, the team assessed the likely impact on the TPP to capture the benefits of the new therapy in terms of the impact of having fewer nocturnal hypoglycemia episodes, a notion that was lacking in the ongoing Phase 3 endpoint strategy. Based on the assessment, it was agreed upon that such an outcome could make a tremendous difference in the TPP; hence, the company decided to initiate in parallel an early access program that included a fit-for-purpose PRO instrument designed to assess the impact of nocturnal hypoglycemia episodes on patients’ QOL. The evidence package at launch demonstrating add-on impact of the product on patients’ nocturnal outcomes was extremely well received by the payers and physicians, resulting in optimal pricing and reimbursement.
Discussion
A well-planned and executed Early Engagement Model in R&D can provide tangible benefits for multiple stakeholders. The manufacturer can achieve a more robust assessment of a product’s medical value to compliment the commercial-focused, net present value assessment. Senior management can feel more confident that the medical and evidence-generation strategy follows the science and is well informed, appropriate, and on track, and the organization will have increased its ability to achieve the upside TPP and maximize the value of the asset. From an external perspective, payers will receive more relevant evidence to inform their decisions, and both providers and patients will have a better understanding of how the mechanism of action translates to patient benefit.
As has been documented by McKinsey & Company 22 and others, the MA and HEOR functions within the pharmaceutical industry face growing internal and external challenges as well as new opportunities. As cost pressures continue to rise given ongoing health care reform, the decision-making power is gradually shifting from physicians to payers and patients. Traditional engagement models with key external experts and advisory boards will significantly transform in the future, given intense public scrutiny and demands for greater transparency through financial disclosures. Delegation of cost to patients (increased premiums, copays, coinsurances) along with medically focused widespread use of social media will lead to an ever-increasing greater voice of patients in medical decision making. The definition of value is now much broader and will expand further as payers and patients continue to demand a demonstration of relative value increase. This will be coupled with increased focus on evidence and higher hurdles for proving product medical value.
The introduction and strategic application of the Early Engagement Model has the ability to cater to the changing health care paradigm and translate current challenges into strategic opportunities. Moving from an opinion-based to an evidence-based way of medical thinking, engaging early on in clinical development to optimally harness learnings, and renewing the focus on the patient can deliver a cohesive value chain where evidence and medical value together become the cornerstone of stakeholder engagement, partnerships, and organizational decision support. Second, the Early Engagement Model can allow for more efficient integration of core medical functions into clinical development and launch planning, with a head start in early development on efficiency and end-in-mind strategy delineating must-have TPP components. This is coupled with the opportunity to provide sustained leadership in driving the evidence continuum from efficacy to effectiveness and reducing gaps from bench to bedside (see Figure 6). However, to properly address these, the use of the Early Engagement Model will likely have specific implications on organizational effectiveness. First, it may require acquisition and/or development of the right medical talent to cultivate and build a strong, evidence-based function that can capitalize on a new set of required competencies to navigate the future health care landscape. These competencies can include: (1) knowledge of different real-world data sources and how to leverage Big Data to gain necessary insights on the patient journey and spot growth opportunities; (2) the ability to systematically gain collective insights and conduct strategic interactions with a varied set of external experts, including policy makers, payers, and patients; and (3) the methodological skill set to identify and evaluate the relevant patient-centric endpoints to support relative medical value differentiation.
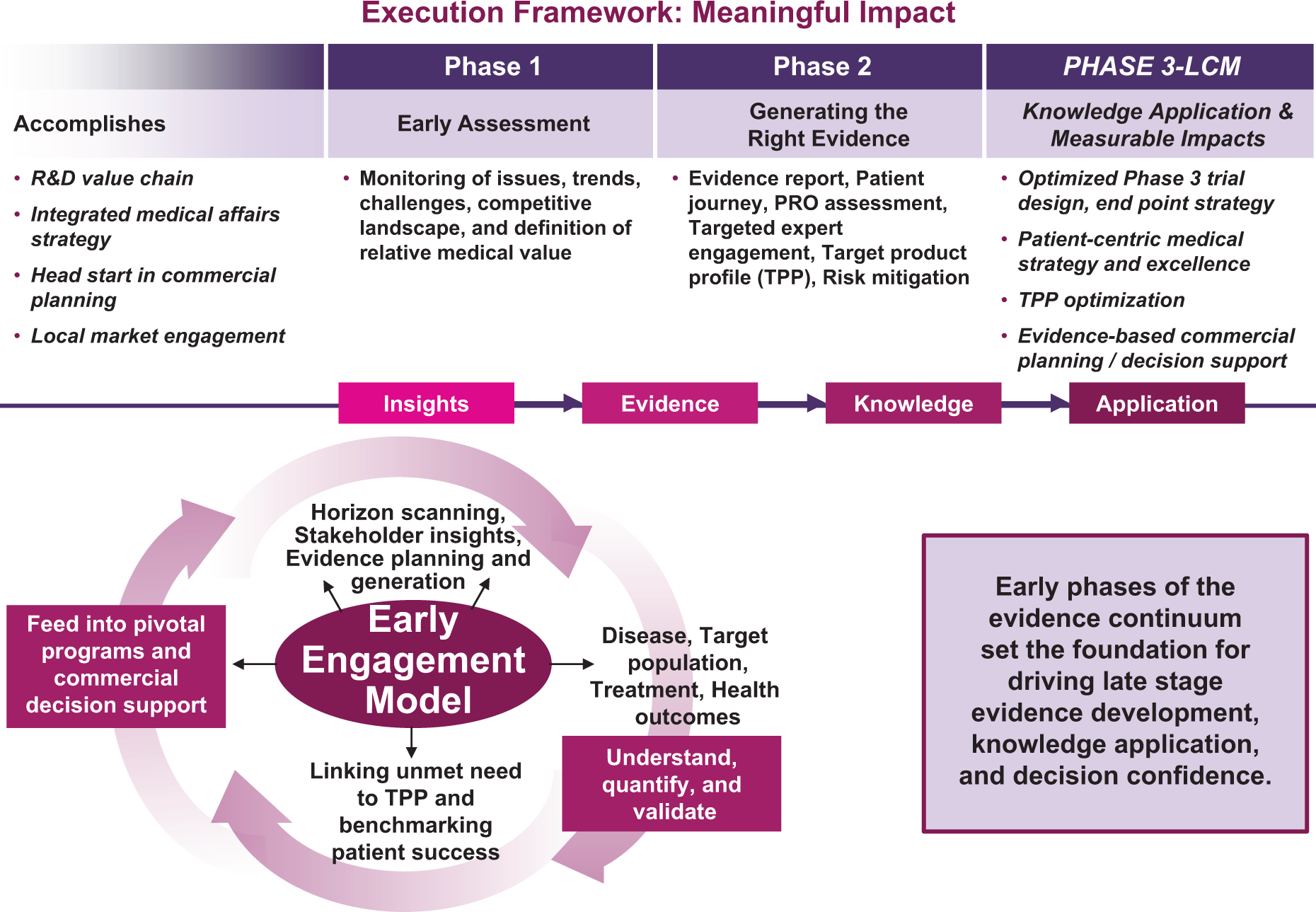
Impact of the Early Engagement Model.
Conclusion
Pharmaceutical companies need to evolve their approach for designing and executing clinical development programs in the rapidly changing health care environment. Clinical proof of concept must be complemented today with compelling demonstrations of treatment value and linkage of scientific innovation to real patient benefit. Strategic application of the Early Engagement Model has the potential to maximize pipeline value, bring benefit to patients, improve quality of care, and meet a future demand for value-based medical practices.
Footnotes
Acknowledgments
The authors acknowledge the contributions of Jon Williams and Marissa Mihos to this article.
Author Note
The views expressed in the manuscript are solely of the authors and do not necessarily represent those of AstraZeneca.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Iqbal, Salimi, and Dunlop are all employees and shareholders of AstraZeneca. Mr Paramore is an employee of Evidera, which provides consulting and other research services to pharmaceutical, device, and other organizations. In his salaried position, he works with a variety of client organizations and is precluded from receiving payment or honoraria directly from these organizations for services rendered.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The manuscript was funded by AstraZeneca. The work represents equal contribution from all authors.