
Abstract
Background:
Janssen Research & Development, LLC, part of the Janssen pharmaceutical companies of Johnson & Johnson, and NYU School of Medicine partnered to establish the Compassionate Use Advisory Committee (CompAC) to evaluate the use of an independent, external, expert committee in ensuring transparent, fair, beneficent, evidence-based, and patient-focused compassionate access to investigational medicines, a public health challenge that has been an ongoing issue for over 3 decades.
Methods:
To this end, NYU School of Medicine was responsible for the formation, member selection, and operation of CompAC, consisting of physicians, ethicists, and patient advocates, under Johnson & Johnson’s sponsorship.
Results:
A pilot was successfully run using CompAC to provide recommendations on compassionate use access to a Johnson & Johnson oncology investigational asset called daratumumab.
Conclusion:
This innovative model provides a framework that can be emulated by the industry globally.
Background
Requests for non–clinical trial access to drugs, vaccines, biologics, and devices that are investigational, and thus unapproved by regulatory authorities, pose a serious challenge for physicians, public officials, patient advocacy groups, institutional review boards (IRBs), and patients. 1 Adjudicating such requests is a growing issue for companies developing medical products, particularly given both the increase in preapproval requests and the growing use of social media to leverage public opinion in support of such requests. 2
Early in 2015, Janssen Research & Development, LLC, part of the Janssen pharmaceutical companies of Johnson & Johnson, contacted Dr Arthur Caplan, of the NYU School of Medicine’s Division of Medical Ethics, to request assistance in responding to requests for unapproved drugs. It wanted to ensure that the company’s preapproval access policies for expanded access and compassionate use (also referred to as individual patient requests) were transparent, fair, beneficent, evidence-based, and patient-focused, while not conflicting with the need to supply investigational drugs to the clinical trials used to evaluate safety and efficacy and leading to regulatory approval.
Janssen was preparing for preapproval access requests for a promising oncology biologic, daratumumab, then in late-stage clinical trials. Daratumumab had shown a compelling clinical benefit-risk profile in patients with multiple myeloma who were refractory to multiple classes of existing drugs. Daratumumab had been granted Breakthrough Therapy designation by the US Food and Drug Administration. It was anticipated that patients whose disease was unchecked by existing drugs might request preapproval access.
Methods
Janssen and the NYU School of Medicine agreed to collaborate on a novel pilot project concerning the development of ethical policies and procedures for preapproval access to daratumumab and the creation of an independent, expert committee to review individual patient requests received by Janssen. The committee was called CompAC (Compassionate Use Advisory Committee). When evaluating individual patient requests (IPRs) for compassionate use, CompAC aligned with Janssen on the company's 3 guiding principles: That all patients are treated fairly and equally That Janssen is not putting patients at risk of unnecessary harm That Janssen continues to conduct thorough scientific studies to understand the potential benefits of new medicines to provide the fundamental information needed to acquire approval from government health authorities and bring new medicines to all patients who need them
Preliminary Decisions Concerning Preapproval Access
A period of intensive discussion between Janssen and the NYU School of Medicine resulted in several determinations on which the pilot program would hinge. Access to daratumumab would be limited to those patients who were unable to receive medical benefit from available, approved drugs. Janssen would be committed to referring patients requesting daratumumab to the clinical trials being conducted on the agent whenever possible, based on eligibility criteria for the trials. The prioritization of clinical trials reflected the company’s commitment to expeditiously completing the clinical trials necessary to seek regulatory approval for the drug, thereby making it widely available if found to have a favorable benefit-risk profile.
Some requesting patients would not be eligible for enrollment in clinical trials, either because they did not meet the trial criteria or were unable to travel to a trial site. Anticipating worldwide demand for the drug after review of pivotal clinical trial data but prior to its approval in all countries where marketing registration was being sought, Janssen worked to create a broad “expanded access program” (https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM351261.pdf). Ultimately more than 1,500 patients around the world gained preapproval access to the compound through this program.
However, despite the availability of this expanded access program, a need remained, because many patients were unable to enroll in existing clinical trials or the expanded access program based on their entry criteria or due to local reasonable/geographic constraints. It was from this group of patients that IPRs were made by treating physicians. Janssen committed to provide the drug at no charge to those patients whose requests were recommended for fulfillment by CompAC.
Clinical supplies for the clinical trials only were adequate as per forecast. The CompAC pilot was brought on later. Because it was early in the development of daratumumab, demand for clinical trial supplies as well as the manufacturing constraints for this biologic medicine meant availability of daratumumab for individual patient requests was initially limited and needed to be closely monitored. Allocation priority was given first to clinical trials, then to cohort expanded access programs, followed by IPRs. Decisions on weekly requests at the start of CompAC’s operation were made while closely monitoring supply availability.
A Novel Process Including CompAC
CompAC was created and administered by the NYU School of Medicine. It was composed of internationally recognized medical experts, bioethicists, and patient representatives who were charged with providing guidance on how to fairly and transparently adjudicate individual patient requests for daratumumab. CompAC initially had 10 members from 5 nations. Two of the American members had to drop out over the course of the pilot project. Thus, there were 8 voting members, plus a nonvoting chair and a nonvoting deputy chair. While voting members were offered—and some accepted—hourly compensation at fair market value for their time, the chair and deputy chair were unpaid. All participants (NYU and non-NYU) were screened for any possible conflicts of interests with Janssen or Johnson & Johnson.
Given its international composition, CompAC met in person only once. However, the committee met virtually each week to consider requests for the drug. CompAC members discussed the requests among themselves and with subject matter experts in multiple myeloma and daratumumab. In no case were these experts permitted to vote or even hear the voting discussion. CompAC members were instructed to recuse themselves from voting if they suspected that they might know the identity of a requesting physician or patient, but this never happened. Except for Arthur Caplan, CompAC members’ names were not made public during the conduct of the pilot, to prevent patients or their supporters from being able to lobby or pressure the members.
All CompAC members and staff were invited to participate in the weekly discussion of requests, but only 3 members voted whether to recommend allocating drug to a requesting patient; decisions were made by the majority. The voting members rotated weekly, but the 3-member voting panel always included a physician, an ethicist, and a patient advocate. CompAC’s decision on each case was then conveyed to Janssen. All IPRs for daratumumab were submitted via a Janssen website. Requests were filed by the patients’ physicians, who completed a novel, customized, standardized form, designed with an intent to ensure that the same types and amounts of information would be submitted for all patients seeking access. IPRs were evaluated by Janssen physicians per prespecified criteria, including (1) whether any safety concerns precluded use of daratumumab, (2) whether patients had exhausted all alternative treatment options, and (3) whether the patients were eligible to enroll in a clinical trial or expanded-access program. The remaining requests were transmitted to CompAC for its independent review. In addition, Janssen provided CompAC with a weekly update on the drug supply status.
All requests forwarded to CompAC were anonymized, and certain information (eg, nationality, gender) was redacted from the request form to further minimize bias. CompAC’s determinations were recommendations, as Janssen was legally bound to take final responsibility for decisions to provide its unapproved product. Janssen committed to inform and explain to CompAC any variance from the committee’s recommendations (Figure 1).
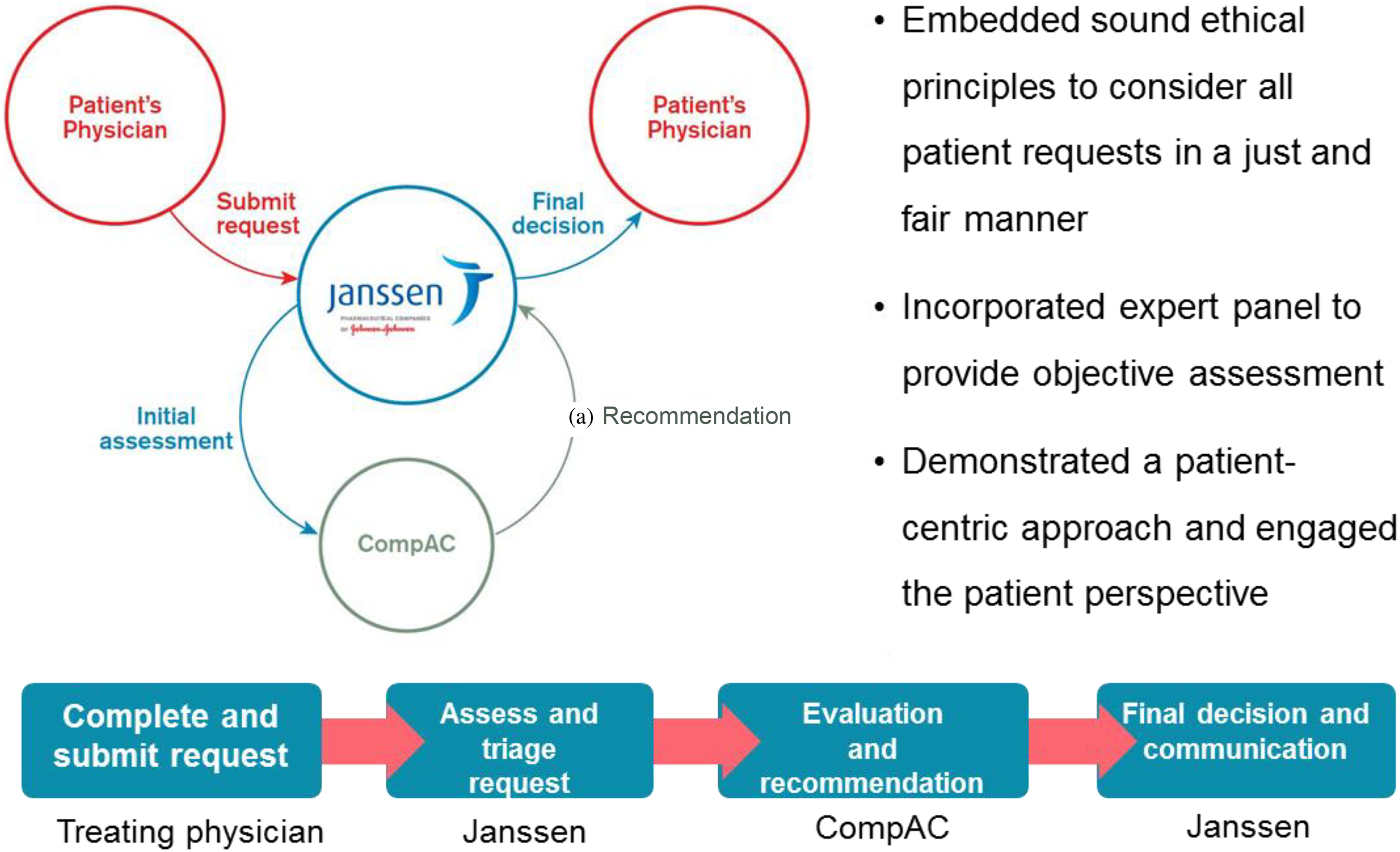
First-of-its-kind compassionate use pilot between academia and industry.
To show appropriate concern for all patients requesting access to daratumumab and ensure that patients’ requests would be dealt with expeditiously, CompAC committed to responding to all requests within 5 business days. There was also an emergency process established by which requests could be heard by CompAC within 24 hours of receiving them for patient in urgent need, based on physician guidance.
This pilot project ran from July 1, 2015, to January 31, 2017, a period encompassing the first approval of daratumumab as monotherapy by the US Food and Drug Administration (FDA) in the US in November 2015, conditional approval of monotherapy by the European Medicines Agency (EMA) in May 2016, the first approval of monotherapy in several other countries, and approval of the second indication for 2 combination therapies in an earlier setting of myeloma by the FDA in November 2016. CompAC continued to meet until January 2017 to consider preapproval access requests from patients in countries in which Janssen was seeking, but had not yet received, marketing approval.
As a result of marketing authorizations received over the span of the pilot project, increasing numbers of patients globally could access daratumumab through traditional channels, thereby reducing the number of requests for preapproval access. Supply of daratumumab also increased for individual patient requests. Also during the pilot project, Janssen further extended its expanded access programs globally, thus providing options for patients whose requests otherwise would have been reviewed by CompAC. The drug is now marketed in >54 countries as Darzalex.
The pilot was deemed a success based on criteria established at the outset of the project; that is, the process of reviewing requests was transparent, fair, beneficent, evidence-based, and patient-focused. Work is now under way to expand CompAC’s purview from preapproval access requests for one oncology drug to an ongoing research program that will advise Janssen about a diverse portfolio of medical products for which the company has received, or expects to receive, requests for preapproval, nontrial access.
Results
Overview
The results described reflect 19 months of CompAC experience in reviewing prescreened IPRs for daratumumab. During this time span, Janssen received a total of 331 IPRs; of these, 7 requests were withdrawn, leaving 324 cases for initial Janssen review.
Of the 324 cases, Janssen screened out a total of 144 requests based on preestablished criteria. Sixty-two patients presented an unfavorable or unknown benefit-risk profile for use of daratumumab (no clinical experience in a disease other than myeloma, comorbidities not evaluated to date, etc), 46 patients had approved therapies available to try, 17 requests provided incomplete clinical information, 10 patients were eligible for clinical trials or expanded access programs for daratumumab, 3 patients died, 2 had prior exposure to the investigational agent (an exclusion criteria), 3 pursued commercially available drug (Darzalex) on its approval, and 1 was internally approved by Janssen prior to the formation of CompAC.
In total, 180 of the 324 requests were forwarded to Comp-AC. After review, and with an awareness of initial low supply of daratumumab, CompAC recommended 163 for approval. Janssen approved a total of 165 requests for access to daratumumab: all of those recommended by CompAC plus an additional 2. The additional 2 patients had been initially rejected by CompAC, but were later approved by Janssen after supplementary medical information from the treating physician became available, which brought the patients’ requests in alignment with guidelines set by CompAC on its initial review.
Resubmission/Appeal Process
Janssen's preapproval access policy permits reconsideration of an IPR denial only when there is a genuine and substantial issue of fact to be added to the information that was previously reviewed, for example, new laboratory results. Based on such information, a total of 20 IPRs were submitted to CompAC for reconsideration. Of these 20, 16 were approved based on additional information. The remaining 4 were declined: 2 for incomplete clinical information and 1 for an unfavorable benefit/risk profile; 1 request was deemed eligible for an expanded access program and thus was also removed from CompAC’s purview.
Redacted Information
At the request of CompAC members, Janssen redacted information about the patients’ gender, nationality, and treating physicians’ identities from the IPR forms provided to CompAC. CompAC members felt that patients’ ages were relevant; thus, ages were preserved on the forms, as was information about the patients’ clinical condition, their medical and treatment histories, and limited social information including whether patients were financially, physically, or emotionally engaged in dependent care, be that for children, parents, siblings, or others.
To check for unconscious bias, CompAC members requested that they occasionally get summaries of the redacted information. At no point did review of this summary information raise concerns about possibly unequal disposition of requests along lines of gender, nationality, etc.
Demographics and Additional Assessment Criteria Reviewed by CompAC
Most IPRs reviewed by CompAC were from Europe (89%) (Table 1). The lower number of IPRs received from the US can be explained by several factors. First, an expanded access program in the US was initiated in June 2015. Second, as the FDA approved the drug in November 2015, there was only a limited window of time for preapproval access requests to be submitted from the US.
Origin of Requests.
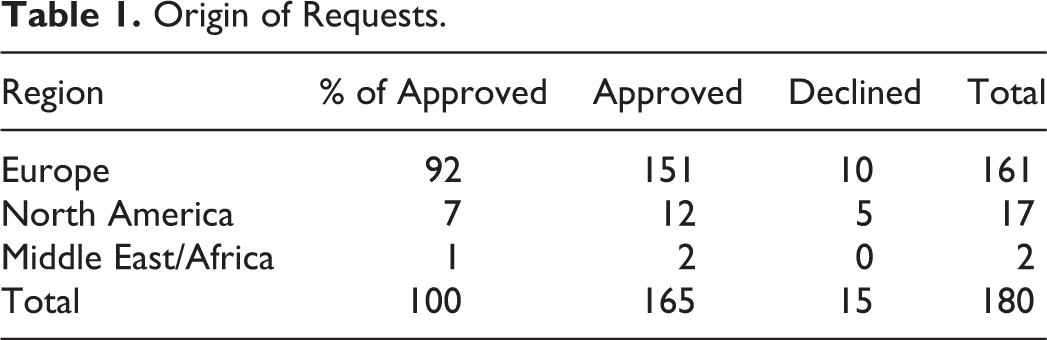
Although the European Commission granted a conditional marketing authorization for daratumumab for the treatment of adults with relapsed and refractory multiple myeloma in May 2016, Janssen continued to receive IPRs from both Europe and the Middle East, probably related to country by country regulatory decisions and to timing of post-approval reimbursement in these areas. There were no requests from Latin America or Asia Pacific, possibly related to the planned timing of regulatory submissions in these regions.
Of the requests reviewed by and approved by CompAC, 62% were for males and 38% were for females (Table 2).
Gender Distribution of Requests.
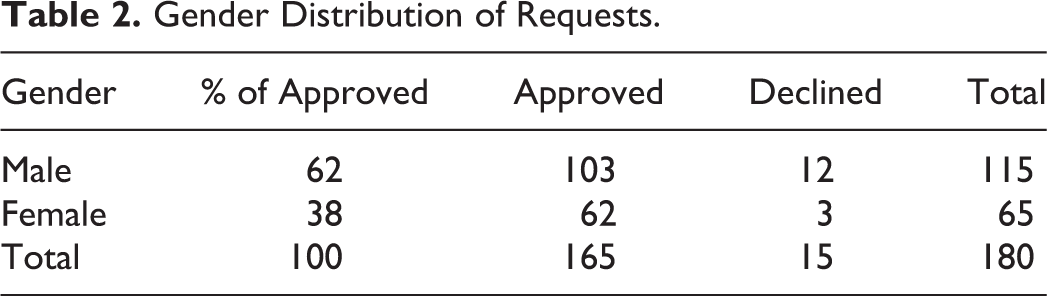
CompAC did not consider the country from which an IPR arose to be relevant to its review and recommendation, nor did it consider gender relevant. However, other factors were thought to be highly relevant. One of these was how the patient was functioning, regarding his abilities, pain, and activities of daily living. Such matters are complex determinations for which no single assessment tool was in common use in all geographic areas. The assessment that was relied upon most often was the ECOG (Eastern Cooperative Oncology Group) score. 3 The IPR form attempted to supplement the ECOG score by asking for a patient narrative and information about the patient’s ability to conduct activities of daily living; however, these portions of the form were inconsistently completed and did not prove to be helpful in many instances.
CompAC sought to identify those patients who could potentially benefit most from treatment with daratumumab while not putting patients at risk of unnecessary harm. Based on its discussions with subject matter experts, CompAC believed that patients who had not been irreversibly disabled by multiple myeloma were most likely to benefit. For example, renal functioning may be expected to improve as a result of treatment with daratumumab, while multiple fractures from brittle bones would not. As such, CompAC was very focused on each requesting patient’s clinical condition and functional status. Most the requests approved by CompAC had an ECOG value of 0 or 1 (33% and 51%, respectively, comprising over 80% of the total). ECOG values of 0 and 1 reflect full functionality to restricted in physically strenuous activity but ambulatory.
As part of robust operational planning of CompAC functioning, contingency plans were developed to address scenarios of potential scarcity, related to the company’s need to prioritize clinical study supply. Fortunately, supply constraints were overcome within a few months.
However, it was determined that if the situation arose, CompAC would look beyond patients’ medical histories and conditions to make allocation recommendations. For example, age, while not determinative in and of itself, was relevant when there was a large age difference between requesting patients who were otherwise thought equally likely to possibly benefit from daratumumab. Multiple myeloma is traditionally a disease found in older persons, so there was ongoing discussion with subject experts about whether younger patients had perhaps more severe forms of the disease or less favorable prognoses. However, based on assurances from the subject matter experts, CompAC only counted older age against requesting patients (Table 3) when supply did not meet demand in a given week—this almost never occurred. Most requests reviewed were from patients between the ages of 60 and 80, with a median age of 62.
Age Distribution of Requests.

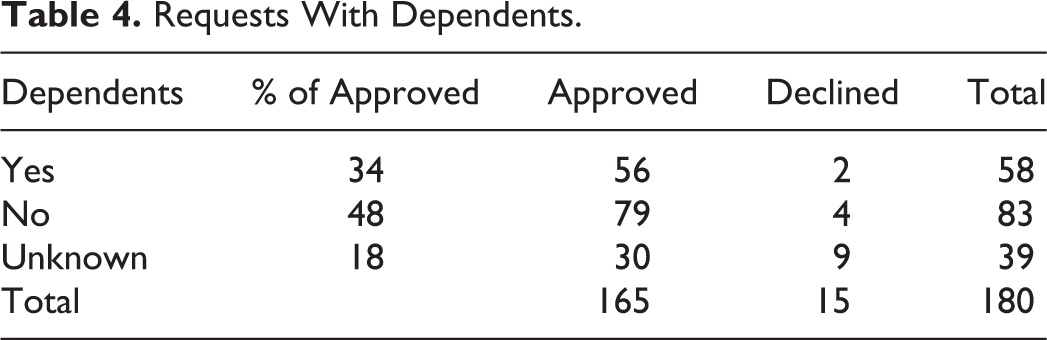
Another important consideration was dependents—whether the patient was “solely responsible for dependents (for example, spouse or partner, child(ren), siblings, other relatives, or any other individual dependent on the patient for financial and/or personal care support)” (Table 4). Age or having dependents did not by themselves determine eligibility. For age or having dependents to be taken into consideration, the patient needed to have received a positive recommendation. Age and dependency were used as tie-breakers among candidates deemed eligible to receive daratumumab. This situation arose only in a few instances.
Requests With Dependents.
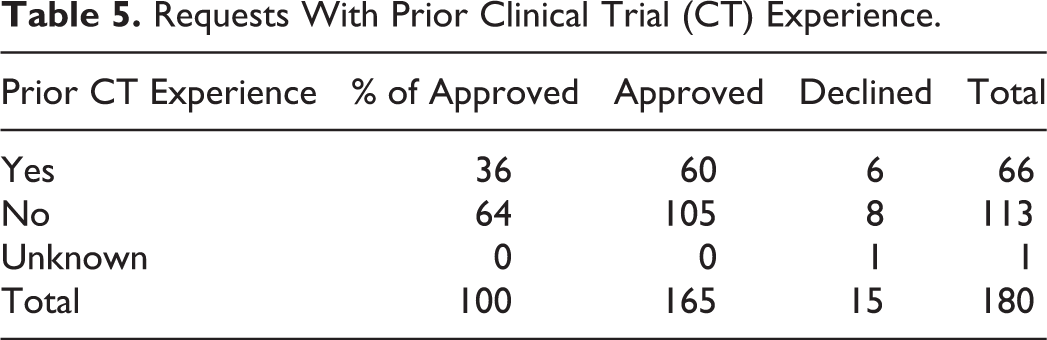
A final tie-breaking consideration was prior clinical trial experience (Table 5). This was a way to acknowledge patients for having served as research subjects and thus adding to generalizable knowledge for the good of other patients, when they met prior assessment criteria. Most requests reviewed and approved by CompAC had no mention of any prior clinical trial experience (64% and 36% for no experience vs experience, respectively) on the part of the requesting patient. But patients who had participated in a clinical trial were given a slight priority over those patients with no such experience.
Requests With Prior Clinical Trial (CT) Experience.
Resupply of Drug
While no outcome data were requested in return for receiving preapproval access, patients who, in the opinion of the treating physician, were deriving clinical benefit from daratumumab were resupplied with drug within the IPR program. Of the 165 approved patients, 145 patients started treatment on daratumumab under the IPR program, and 8 US patients went directly to commercial product (Darzalex) upon FDA approval. Treatment for 12 patients is unknown.
Emergency Requests
CompAC received 6 emergency requests, all of which were reviewed and approved within one business day of receiving the request.
Conclusion
Janssen is not the first company to receive or adjudicate preapproval access requests for a promising drug. However, few companies have documented how such requests were decided, and none has partnered specifically in the manner Janssen has with an independent entity to make such decisions. The CompAC pilot is a novel exercise in fairness and transparency and the first known instance of utilizing an international, interdisciplinary expert committee to make recommendations concerning patient requests for an unapproved medical product. Having deemed the pilot project a success, Janssen and NYU School of Medicine are now working to evolve CompAC into a company-wide endeavor. The use of an independent, heterogeneous committee incorporating medical, ethical, and patient perspectives will be maintained going forward. Other aspects—particularly what factors are deemed most vital in making allocation decisions—are expected to change as CompAC takes up other medical products, each with its own specific patient populations and treatment landscape. Other medical product developers have expressed interest in adapting CompAC for their own use, to ensure the fairest possible approach to preapproval access. Thus, this first pilot project is poised for myriad adaptations in industry, government, and NGOs (which have made informal inquiries to NYU School of Medicine about the project). These include nations with provincial, regional, or national health systems such as Canada, India, South Korea, or the UK. Other groups might include the Gates Foundation, PATH, GAVI.
Footnotes
Appendix
Acknowledgments
We thank A. Ray, CMO, and Head, GMO, and B. Harrison, Head, Patient Support, Janssen, and L. Kearns, NYU School of Medicine, and members of CompAC (T. Arawi, V. Cwik, S. Gardner, E. Mitchell, J. Różyńska, I. Singh, J. Teagarden, R. Upshur, and J. Walsh) for consultation and advice.
Declaration of Conflicting Interests
No potential conflicts were declared.
Funding
No financial support of the research, authorship, and/or publication of this article was declared.