
Abstract
Background:
The incidence of vertebral fracture is commonly used as a primary endpoint in randomized clinical trials of pharmaceutical agents for osteoporosis. In order to investigate the impact of ethnic/regional difference in osteoporosis clinical trials on the incidence of vertebral fracture, we examined the correlation between the incidence of vertebral fracture in the placebo group and baseline bone mineral density (BMD), ethnic and regional differences, or other factors by meta-regression analysis.
Methods:
We studied a total of 21 trials involving 28,425 patients treated with placebo, which were identified through MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials.
Results:
A univariate meta-regression showed a significant correlation between the proportion of subjects experiencing new vertebral fracture and the proportion of Caucasian subjects (coefficient = 0.223, P = .045), and the proportion of subjects with prevalent vertebral fracture (0.161, P < .001). Baseline lumbar spine BMD did not show significant correlations. As a result of multivariate meta-regression analysis with the factors with P < .2 by the univariate meta-regression, the proportion of subjects with prevalent vertebral fracture was identified as an influencing factor (0.139, P = .001).
Conclusions:
The multivariate meta-regression showed that prevalent vertebral fracture was the most important factor to predict subsequent vertebral fracture. In addition, considering the results of the univariate meta-regression analysis, we suggest that the ethnic/regional difference should be considered as one of the important factors that influence the incidence of new vertebral fracture, a primary endpoint of osteoporosis study, when the Caucasian reference range is used in clinical trials.
Introduction
The incidence of vertebral fracture is commonly used as a primary endpoint in randomized clinical trials (RCTs) of pharmaceutical agents for osteoporosis worldwide. The prevalence of osteoporotic fracture, however, varies among regions or ethnic groups. A systematic review on the incidence of hip fracture reported that the prevalence of osteoporotic fracture was higher in Europe and Western Pacific regions than in Africa and Eastern Mediterranean regions. 1 In terms of ethnic differences, while the prevalence of vertebral fracture was reported to be similar between Asian and Caucasian women aged 80 years or younger, the prevalence of hip fracture was lower in Asians than Caucasians. 2 Furthermore, a cohort study in the United States reported that the prevalence of vertebral fracture was lower in black women compared with white women, even though both groups had the same bone mineral density (BMD) value. 3
BMD T-score, which is used as diagnostic criterion of osteoporosis and inclusion criterion in clinical trials for osteoporosis, is a score calculated in relation to the reference distribution of BMD in a young healthy population. However, normal distribution of BMD in the young healthy population varies among ethnic groups. 4 The importance of using an appropriate reference range for BMD T-score calculation in different ethnic groups or regions has been discussed for many years from the beginning of the activity for setting the bone densitometry criteria for the diagnosis of osteoporosis to the current position development conference by the International Society of Clinical Densitometry. 4,5 When the International Osteoporosis Foundation guideline and the World Health Organization technical report defined the international reference range, ethnic and regional differences were recognized as important factors for the accurate diagnosis of osteoporosis; however, there was no appropriate data with the required sample size for each ethnic group or region to set a reference range for each of the populations, and also the ethnic difference in BMD could not completely explain the ethnic difference in the fracture rate. Therefore, for the sake of simplicity of the criteria for diagnosis, the guidelines used the femoral neck BMD data on Caucasian women from the NHANES III study, a large population-based study of representative samples of the US population, to set the international reference range and standard deviation for BMD T-score calculation in the diagnosis of osteoporosis. 4,6
To align with the guidelines, the above-mentioned Caucasian reference for BMD T-score has been used as inclusion criteria in most clinical trials. In some populations for which epidemiologic data with sufficient sample size was available, on the other hand, an independent average of BMD and standard deviation different from that in the Caucasian population was shown, and a normative reference range was established based on such data in the local guidelines for diagnosis of osteoporosis, as described in the 2013 International Society for Clinical Densitometry position development conference on bone densitometry. 5 For instance, the Japanese population showed a lower average BMD in a large population survey, and a lower reference BMD compared to the Caucasian reference range was defined as the Japanese reference BMD in the Japanese diagnostic criteria. 7
Previous clinical trials also showed the importance of choosing an appropriate reference range for the BMD T-score. For example, in the FIT 2 study, which assessed the effect of alendronate on the incidence of vertebral fracture for 3 years, the reference range that was used as the inclusion criterion was updated during the study based on the NHANES III data published during the study. 8 The updated reference range corrected the overdiagnosis of subjects who had been diagnosed as having osteoporosis under the initial reference range. In addition, in the recent FRAME study, in which the incidence of vertebral fracture for 1 year was assessed to evaluate the effect of romosozumab for the prevention of vertebral fracture, the Latin American population using the Caucasian reference range for diagnosis showed a low incidence of nonvertebral fracture. This result raised a question about the use of a Caucasian reference range in a Latin American population. 9
In order to investigate the impact of ethnic/regional difference in osteoporosis clinical trials on the primary endpoint of the incidence of vertebral fracture, we examined, by a meta-regression analysis, the correlation between the incidence of vertebral fracture in the placebo group, which was not influenced by osteoporotic drug interventions, and baseline BMD, ethnic and regional differences, or other risk factors.
Methods
Search Strategy
A systematic literature search was conducted by referencing the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement. 10 We conducted a systematic search on June 20, 2018, to identify articles on RCTs of pharmacologic agents for postmenopausal osteoporosis compared to placebo, which were published up to December 31, 2017, through MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials.
Eligibility Criteria and Study Selection
The systematic literature review included all RCTs assessing efficacy and safety of pharmacologic agents for postmenopausal osteoporosis that met the following criteria: (1) comparison with placebo, (2) availability of data on the number of vertebral fractures at 3 years, (3) inclusion of Caucasian subjects, and (4) publication in English. First, potentially relevant trials were identified via the search algorithm including the terms of [vertebral] AND [fracture] AND [placebo]. Second, trials that met the criteria were retrieved after reviewing the abstract. Third, full texts of the retrieved articles were reviewed, and the trials that met the above criteria were selected.
The following trials were excluded from our review: trials performed in patients with male or glucocorticoid-induced osteoporosis, trials with less than 3 years’ study duration, extension trials from the original trials, ad hoc and subgroup analyses from the original trials, and review articles. Trials selected for review were rechecked to ensure that different trials related to the same study had not been included. The identification of relevant abstracts, the selection of trials based on the criteria described above, and the subsequent data abstraction from the full-text articles were confirmed at each step in duplicate (T.K. and M.K.). Any discrepancies were resolved by consensus. A third reviewer (M.N.) resolved any discrepancies, if the other two reviewers (T.K. and M.K.) disagreed.
Data Extraction
Data on the number of subjects experiencing new vertebral fracture in 3 years in the placebo group were extracted from each study as a response variable. Potential factors affecting the new vertebral fracture such as proportion of Caucasian subjects, participation of subjects in Asian countries, proportion of subjects with prevalent vertebral fracture, baseline lumbar spine BMD T-score, age, years since menopause, body mass index (BMI), and vitamin D supplementation, were also extracted as explanatory variables. We originally tried to collect information on the proportion of Asian, Black, and Hispanic subjects. However, the proportion of subjects other than Caucasian was not available in most of the studies, and we used the information whether subjects in Asian countries participated or not as an alternate factor. If only baseline lumbar spine BMD actual value was available in the article, we used Hologic data to convert the value to T-score with Caucasian reference data provided by the manufacturer. Vitamin D supplementation data were referred to the protocol based on the description whether concomitant use of vitamin D supplement was stipulated. Data not available in the original papers were supplementally extracted from review reports by the United States Food and Drug Administration or the European Medicines Agency.
To ensure study quality, the extracted trials were assessed by all the authors using the 5-point Jadad score, which can range from 0 to 5, with higher scores indicating higher quality. 11
Statistical Analysis
The proportion and 95% confidence interval (CI) for the number of subjects experiencing new vertebral fracture in 3 years in the placebo group were calculated. A random effects model, which accounts for heterogeneity among studies, was used to conduct a meta-regression analysis to investigate potential factors affecting the incidence of new vertebral fracture. The prespecified factors used in the meta-regression were as follows: proportion of Caucasian subjects, participation of subjects in Asian countries, proportion of subjects with prevalent vertebral fracture, baseline lumbar spine BMD T-score, age, years since menopause, BMI, and vitamin D supplementation.
A univariate meta-regression was first performed to identify potential factors affecting the incidence of new vertebral fractures. Factors with P <.2 in the univariate analysis were further analyzed by multivariate meta-regression. A statistically significant difference was defined as P < .05 in the multivariate meta-regression. All the analyses were performed using R software version 3.4.3. 12
This article does not contain any studies with human or animal subjects performed by any of the authors.
Results
Search Results and Study Characteristics
One thousand six hundred fifty-two articles were identified during the literature search in EMBASE and MEDLINE and 587 articles were identified from the search in Cochrane Central Register of Controlled trials. Five hundred fifty-eight duplicates were identified and eliminated. Of the remaining 1681 potentially relevant articles, 1626 were excluded after reviewing the titles and abstracts (Figure 1).
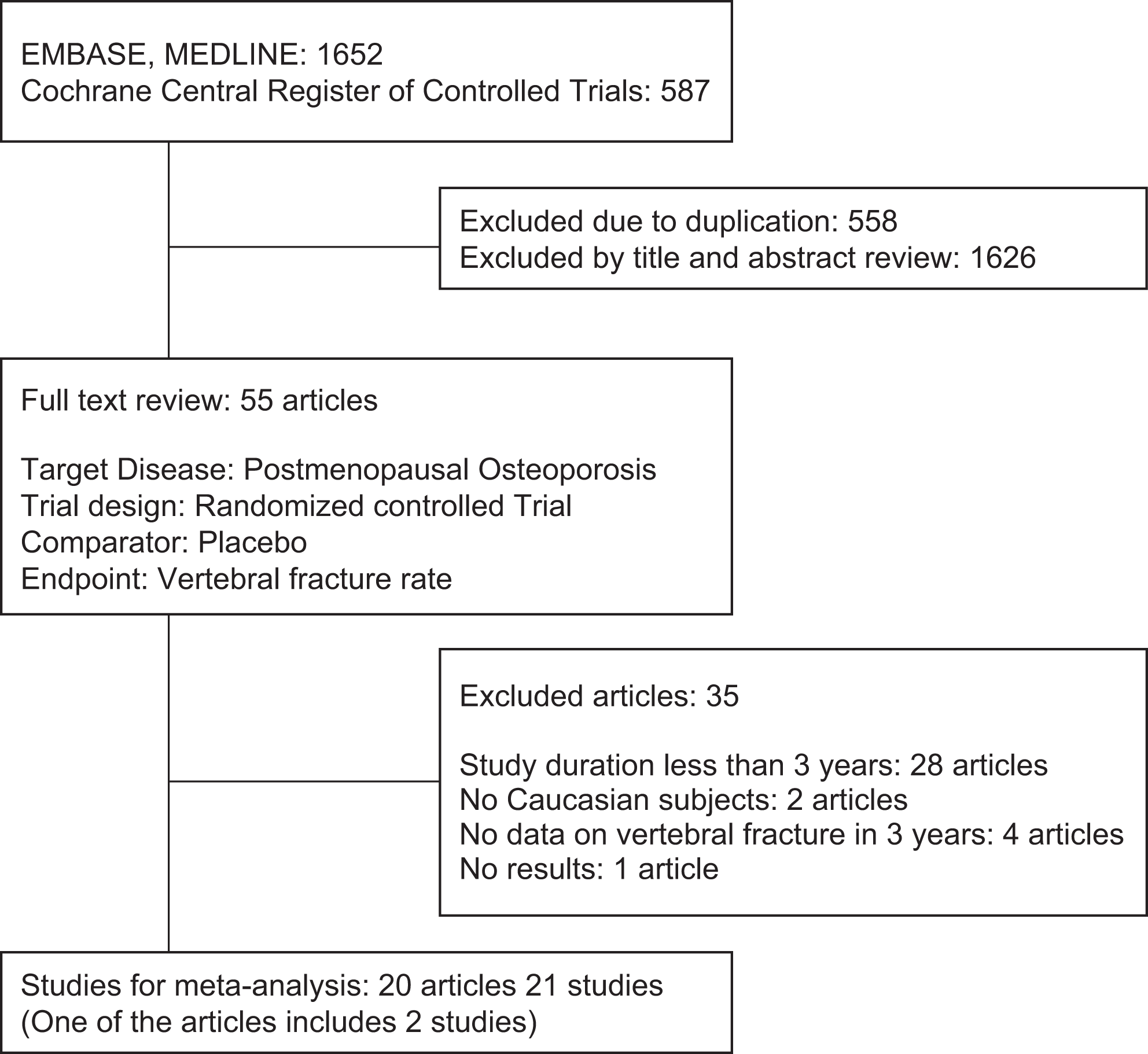
Flow diagram of study selection.
The full texts of the remaining 55 articles were reviewed, and 21 studies in 20 articles were ultimately included in the analysis. We used a total of 21 studies involving 28,425 patients in the placebo group that met the selection criteria for the analyses. The main characteristics of the 21 studies are described in Table 1. Three of 21 studies restricted enrollment of ethnic populations other than Caucasian, and 5 studies restricted enrollment of subjects without prevalent vertebral fracture by the inclusion criteria. All the extracted trials had a score of 5 in the Jadad Score.
Studies Included in the Analysis.
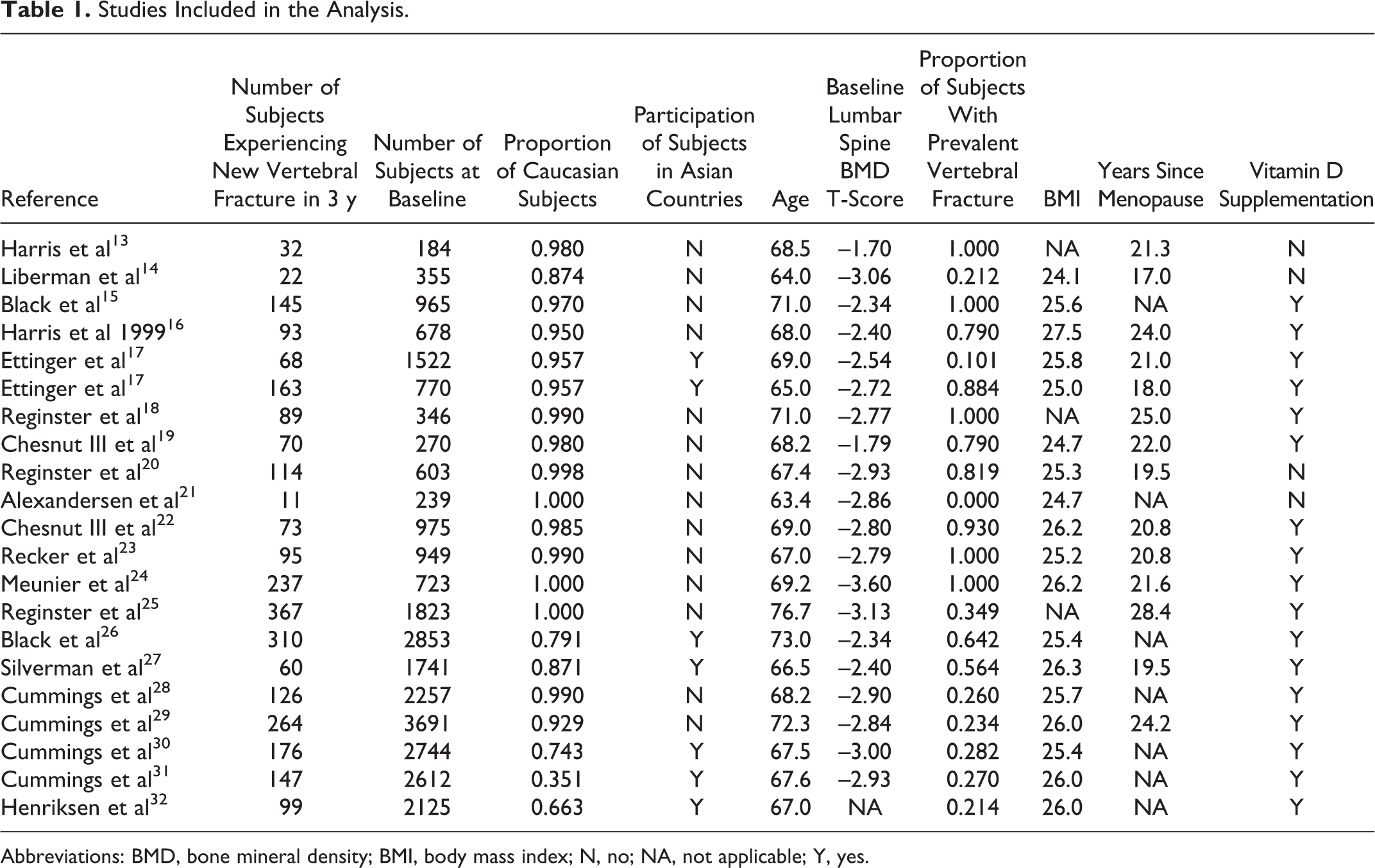
Abbreviations: BMD, bone mineral density; BMI, body mass index; N, no; NA, not applicable; Y, yes.
Univariate Metaregression
Univariate meta-regression showed significant correlations between the proportion of subjects experiencing new vertebral fracture in 3 years and the proportion of Caucasian subjects (coefficient = 0.223, P = .045) and the proportion of subjects with prevalent vertebral fracture (0.161, P < .001) (Table 2). Other explanatory variables including baseline lumbar spine BMD T-score did not show a significant correlation with the proportion of subjects experiencing new vertebral fracture in 3 years. Even though a statistically significant correlation was not observed, the coefficient estimates for each variable were consistent with the general perception of the relation of each variable with vertebral fracture, meaning that risk factors such as age showed a positive correlation and preventive factors such as BMI showed a negative correlation.
Univariate Metaregression Analysis.
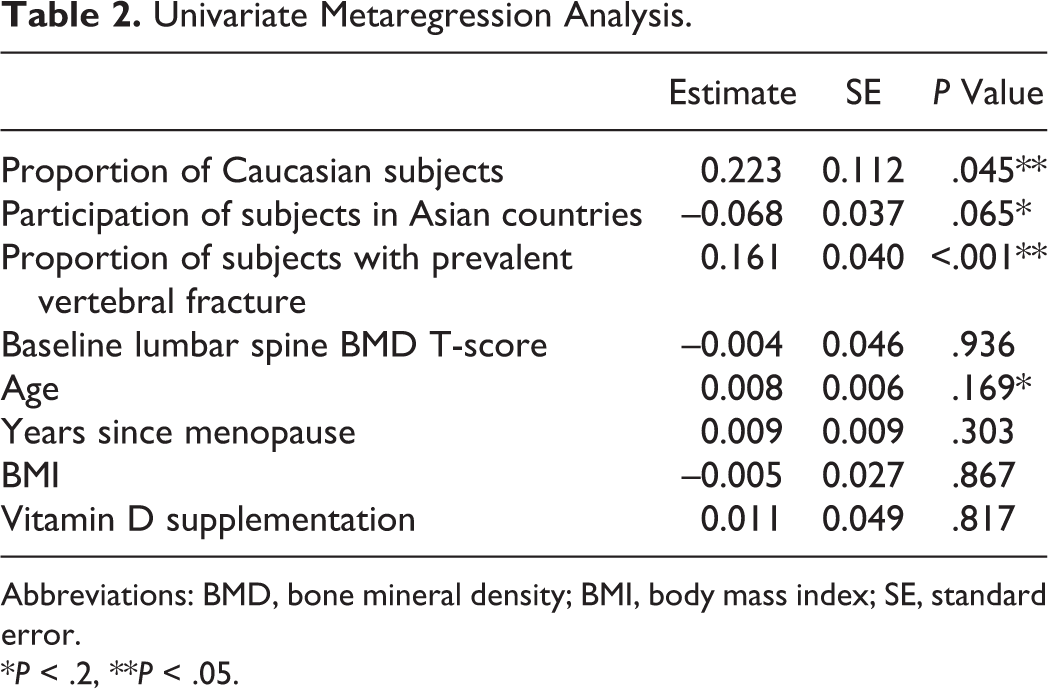
Abbreviations: BMD, bone mineral density; BMI, body mass index; SE, standard error.
*P < .2, **P < .05.
Multivariate Metaregression
Factors that showed a correlation with the proportion of subjects experiencing new vertebral fracture in 3 years with P <.2 in the univariate meta-regression were further analyzed by multivariate meta-regression (Table 3). Because the participation of subjects in Asian countries seemed to have a correlation with the proportion of Caucasian subjects, it was excluded from the multivariate analysis. As a result, the proportion of subjects with prevalent vertebral fracture was identified as an influencing factor (coefficient = 0.139, P = .001).
Multivariate Metaregression Analysis.
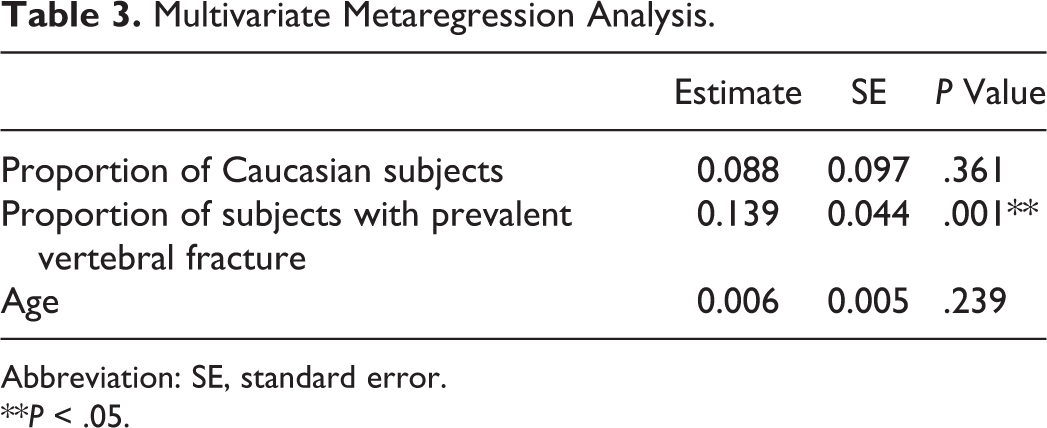
Abbreviation: SE, standard error.
**P < .05.
When we conducted the analysis using participation of subjects in Asian countries instead of proportion of Caucasian subjects, the result was not changed (data not shown). We also obtained a similar result by the analysis using additional data from 3 studies for which the fracture data were not published as an article or were available only in charts in the article (data not shown).
Discussion
The result of the present study showed that among the several factors investigated, “prevalent vertebral fracture” was the highest risk factor for the incidence of new vertebral fracture. The previous meta-analysis of cohort studies showed a correlation between previous fracture history and subsequent fracture. 33 Also, the diagnostic guidelines of osteoporosis 4,7 as well as the inclusion criteria of clinical trials of pharmaceutical agents for osteoporosis define the prevalent osteoporotic fracture including vertebral fracture as important criteria of osteoporosis. The result of the present study is consistent with the previous report, clinical guidelines, and clinical trial practice, and reconfirms the importance of the prevention of the first vertebral fracture.
In univariate meta-regression analysis, while the proportion of Caucasian subjects showed a significant positive correlation with the incidence of new vertebral fracture, participation of subjects in Asian countries showed a negative correlation, although it was not statistically significant. Prevalence of osteoporotic fracture was reported to be higher in Europe and Asia than in Africa or Eastern Mediterranean. 1 In addition, similar prevalence of vertebral fracture was reported between Asians and Caucasians. 2 Considering these previous reports, we could assume that the more Caucasian or Asian participants in clinical trials, the higher the incidence of new vertebral fracture. However, the present study showed different results. It is possible that the difference was due to the use of the Caucasian reference in the inclusion criteria of clinical trials, which resulted in overdiagnosis of osteoporosis in the Asian population. This is because, as the Japanese reference showed, the Asian average BMD is presumably lower than that in the Caucasian reference range. Taken together, we would suggest that the ethnic/regional difference should be considered as one of the important factors that influence the primary endpoint of the osteoporosis study when the Caucasian reference range is used in the clinical trial.
In the present study, “baseline lumbar spine BMD T-score” and “age” did not show a significant correlation with the incidence of vertebral fracture, despite the fact that low BMD and old age are important risk factors of osteoporotic fracture and that the BMD is used as a diagnostic criterion. We considered that one of the reasons that “baseline lumbar spine BMD T-score” did not show a significant correlation was the use of a Caucasian reference range. Previous studies showed that the use of the Caucasian reference range for a BMD T-score calculation in non-Caucasian populations led to unexpected outcomes. 8,9 Another reason would be that the BMD T-score at baseline does not fully predict the risk of fracture in the future, although it is related to the risk of fracture at the timing of measuring BMD. We considered that the reason that “age” did not show a significant correlation with the incidence of vertebral fracture was that the target subjects in postmenopausal osteoporosis studies were elderly outpatients and the mean age of subjects in each study were distributed too narrowly to show a significant correlation compared with the previous epidemiologic data.
In order to discuss the appropriateness of using the Caucasian reference range for BMD T-score calculation in non-Caucasian populations, it might be interesting to include the results of studies without Caucasian populations. We found two non-Caucasian studies that had the fracture data at 3 years, but these two studies involved Japanese samples, and the Japanese reference range was used for the BMD T-score calculation. More RCTs that evaluate the incidence of vertebral fracture in the non-Caucasian population using the Caucasian reference range for BMD T-score calculation would help to discuss the influence of ethnic differences in a broad sense in the future.
The present study has several limitations. First, this analysis was not performed at the patient level but instead used summary data; therefore, accurate assessment may be lacking as the nature of meta-analysis. However, the direction of the coefficients for each factor in both the univariate and multivariate meta-regression analysis was consistent with the previous epidemiologic report. 4 Second, the correlation between prevalent vertebral fracture and incidence of new vertebral fracture was too strong to evaluate the influence of other factors. Further investigation in populations without prevalent fracture would properly characterize the influence of ethnic or regional difference on the risk of osteoporotic fracture and its relationship with BMD. Third, the present study could not directly compare the ethnic difference based on the data of proportion of Asian, Black, and Hispanic populations. Further investigation is needed to reveal the effect of each ethnic population on the incidence of new vertebral fracture.
Conclusion
The result of this multivariate meta-regression analysis showed that prevalent vertebral fracture was the most important factor to predict subsequent vertebral fracture. In addition, considering the results of the univariate meta-regression analysis, we suggest that the ethnic/regional difference should be considered as one of the important risk factors that influence the incidence of new vertebral fracture, a primary endpoint of osteoporosis study, when the Caucasian reference range is used in clinical trials.