
Abstract
Study Design
Prospective Cohort Study.
Objectives
This study aimed to (1) compare anticipated and encountered post-operative barriers following lumbar decompression surgery, (2) assess the relationship between encountering barriers and achieving meaningful improvement (MCID) in Oswestry Disability Index (ODI) scores, and (3) evaluate the association between socioeconomic status and encountered barriers via Social Vulnerability Index (SVI).
Methods
Patients completed pre-operative surveys assessing anticipated recovery barriers and ODI. Post-operative surveys collected 6 weeks post-operation captured encountered barriers and ODI. Barriers were quantified with a 1-5 Likert scale. Wilcoxon Rank Sign tests assessed differences between anticipated and encountered barriers. Logistic regression evaluated associations between barriers and achievement of ODI MCID. Spearman correlation tested associations between SVI and barrier frequency.
Results
Patients were generally able to predict post-operative barriers accurately. Exercise adherence, financial stress, and care understanding were frequently reported concerns. Five post-operative barriers decreased the likelihood of achieving MCID: difficulty meeting exercise goals (OR = 0.43, P = 0.00036), difficulty obtaining medications (OR = 0.32, P = 0.030), transportation challenges (OR = 0.42, P = 0.036), communication issues with the care team (OR = 0.52, P = 0.015), and limited understanding of care plan (OR = 0.58, P = 0.044). Higher SVI scores correlated with difficulty obtaining medications (P = 0.035) and increased financial stress (P = 0.033).
Conclusions
Post-operative recovery challenges—particularly in exercise adherence, medication access, transportation, and care plan comprehension—are associated with reduced odds of functional improvement. Higher social vulnerability exacerbates specific barriers. These findings underscore the importance of individualized peri-operative planning to optimize outcomes in lumbar decompression surgery.
Keywords
Introduction
Surgical intervention for degenerative lumbar spine pathology has increased by 300% over the past 20 years in the United States. 1 As the volume of these procedures has grown, so has the emphasis on the quality of care, with reimbursement being increasingly tied to patient-reported outcome measures (PROMs). 2 A cornerstone to the foundation of high quality spine surgery is perioperative counseling, which plays a vital role in successful patient outcomes.
Despite this importance, there is a paucity of literature on personalized health priorities in the peri-operative period.3,4 Of the limited studies on this topic, Accardi-Ravid et al 5 explored patients’ qualitative experiences in the lead up to spine surgery. The authors identified a common feeling of ill-preparedness for the post-operative period. Similarly, prior literature has identified common barriers to post-operative recovery that include challenges with rehabilitation exercises, adherence to work and driving restrictions, access to medications, wound care, family obligations, financial stress, and transportation limitations.6-16 The post-operative period for lumbar decompression surgery is routinely completed in the outpatient setting. Thus, success in this period is reliant on patient understanding, buy-in, and adherence to post-operative instructions. Variation in these domains has the potential to confound PROMs and impact perceived surgical outcomes. Additionally, the barriers anticipated by the surgeon may not be the barriers that patients actually encounter. Compounding this discrepancy is a lack of clarity on the impact of socioeconomic status on specific barriers. 17 By examining these barriers in detail, clinicians may gain insights into potential gaps in treatment protocols that contribute to variability in spine surgery outcomes.
This study aims to investigate the specific barriers that patients face after lumbar decompression surgery. There are 3 objectives to this study: (1) to compare anticipated and encountered post-operative barriers to recovery, (2) to assess how encountered barriers affect patients’ ability to achieve minimum clinically important difference (MCID) as measured by the Oswestry Disability Index (ODI), and (3) to identify associations between socioeconomic status and perceived and realized barriers. While previous studies have qualitatively explored barriers to surgical recovery, to our knowledge, this is the first paper to quantify both anticipated and experienced barriers within a prospective cohort and examine their direct impact on MCID.
Methods
This study was approved by our Internal Review Board (IRB) with a waiver of signed consent. The waiver was granted because data collection involved minimal risk to participants, consisted solely of routine survey responses and de-identified information, and did not alter the standard of clinical care. All procedures were conducted in accordance with institutional ethical standards and regulatory requirements for human subject research.
Patient Population
We performed a prospective cohort study of patients at a single tertiary care center between July 2022 and August 2023. Inclusion criteria included patients 18 years and older who underwent elective 1 or 2-level lumbar discectomy or laminectomy for degenerative pathology, with a minimum of 6 weeks of follow-up. These procedures were performed by seven fellowship-trained spine surgeons with a mix of orthopedic and neurosurgery backgrounds. Exclusion criteria included pregnant individuals, non-English speaking individuals, and patients undergoing surgery for trauma, infection, cancer, spinal cord injury, or those presenting in an emergent fashion. Non-English speaking individuals were excluded to ensure comprehension and consistency in survey responses, as validated translations were not available for the study instruments. Other exclusions were applied to maintain a homogeneous elective degenerative cohort and reduce confounding from urgent or non-degenerative pathologies. Patients who were missing pre-operative patient-reported outcome measures (PROMs) or failed to complete any post-operative surveys were excluded from the study. A total of 104 patients were included in the study sample; 16 failed to complete all the required follow-ups (15%), leaving 88 patients in the final analysis.
Survey Design
Patients completed a novel pre-operative survey by assessing anticipated barriers on a 1-5 Likert scale, where one represents minimal concern and five represents the most significant concern (Appendix 1). The use of Likert scales for the measurement of barriers, while novel in this study, is well established in orthopedic literature, and is the predominant metric assessing patients’ perceptions. 18 This methodology allowed for the comparison of pre-operative and post-operative scores to evaluate for anticipated vs encountered barriers, and provided a means for patients to convey the severity of the variable. Patients also completed pre-operative ODI scores. Follow-up surveys were collected 6 weeks post-operation, assessing encountered barriers on the same 1-5 Likert scale and post-operative ODI scores. To minimize recall bias, surveys were administered prospectively at standardized time points, with post-operative questionnaires distributed within six weeks of surgery to capture experiences while still recent. Survey questions were phrased similarly and in the same order between pre- and post-operative forms to promote consistency and reduce interpretation bias. The 6-week interval was selected for a focused assessment of early recovery patterns related to a specific operative episode of care. Surveys were collected via GetWell (SAIGroup, Palo Alto, CA) and Research Electronic Data Capture (RedCap, Vanderbilt, Nashville, TN).
Socioeconomic status was assessed using the Social Vulnerability Index (SVI), which was originally piloted by the CDC in 2011. 19 The SVI consists of four scores: socioeconomic status, household composition, minority status, and housing/transportation. 20 Within these categories, SVI is based on 15 variables, each of which is given a score ranging from 0 to 1, with the higher score indicating greater socioeconomic vulnerability. 21 Scores range from 0 (lowest vulnerability) to 1 (highest vulnerability). Practically, higher SVI scores correspond to patients residing in communities with greater average socioeconomic deprivation, including limited healthcare access, lower educational attainment, transportation challenges, and housing instability—all of which were hypothesized to potentially impact patient outcomes. SVI data was extracted using online mapping tools and individual patient addresses. Patients’ demographics, including age, sex, race/ethnicity, insurance payer, and zip code, were also collected.
Statistical Analysis
Categorical variables are expressed as percentages. Continuous variables are expressed as mean ± standard deviation. Non-parametric Wilcoxon Ranked Sign tests were performed to evaluate the difference in pre- and post-operative barrier scores. Logistic regression analysis was used to examine the association between post-operative barriers and achieving MCID. Consistent with previous published work, a 30% reduction in baseline ODI was used as the MCID benchmark, as this is the most recent definition of MCID in lumbar spine surgery. 22 Achieving MCID reflects a level of improvement in pain and function that is perceptible and meaningful to patients. Using this outcome enhances the clinical relevance of findings by excluding results that may be statistically significant but do not impact patients’ experiences.
A binomial logistic regression model was fitted for each barrier using the maximum likelihood estimation method. For this analysis, each barrier’s Likert score (1-5) was treated as a continuous independent variable, and achievement of MCID was modeled as a binary dependent variable. To mitigate the risk of model overfitting given the sample size, barriers were modeled individually rather than simultaneously in multivariate regression. To estimate effect sizes for each postoperative barrier’s association with MCID, Cohen’s d was calculated by converting the natural logarithm of the odds ratio (ln[OR]) using the formula:
For the postoperative model, “NA” responses (ie, retired individuals when asked about work restrictions) were addressed using Multiple Imputation via Chained Equations (MICE) with predictive mean matching (5 imputations, 5 iterations per imputation). This approach allowed us to retain statistical power while limiting potential bias from case-wise deletion due to missingness. Spearman Correlation tests were performed comparing the correlation between SVI and each barrier for pre- and post-operative, as well as with ODI. Patients reporting a “Not-applicable” response to barriers were excluded from that specific barrier analysis. Statistical analysis was performed using R version 4.3.2 (2023-10-31 ucrt). P-values of <0.05 were interpreted as statistically significant.
Results
Descriptive Statistics
Patient Demographics
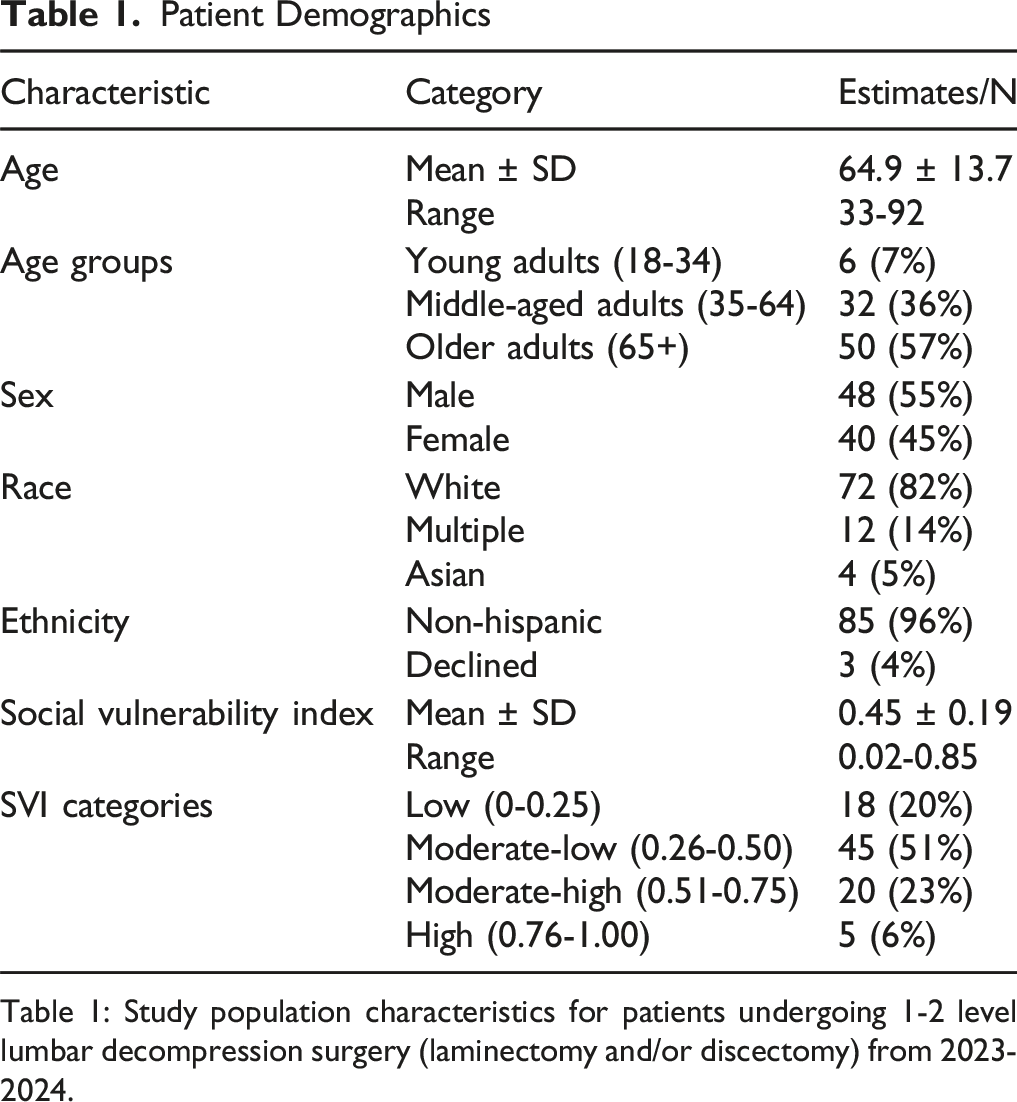
Table 1: Study population characteristics for patients undergoing 1-2 level lumbar decompression surgery (laminectomy and/or discectomy) from 2023-2024.
Pre-operative Anticipated Barriers and Frequency of Encountered Barriers
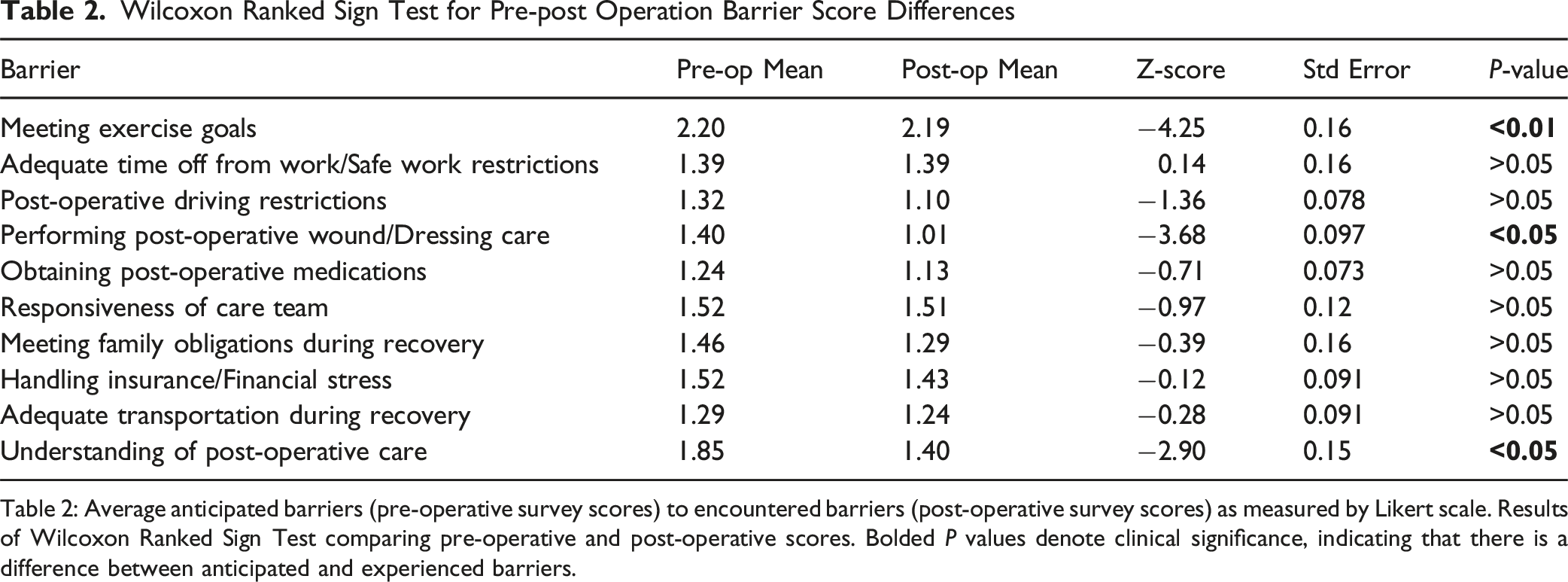
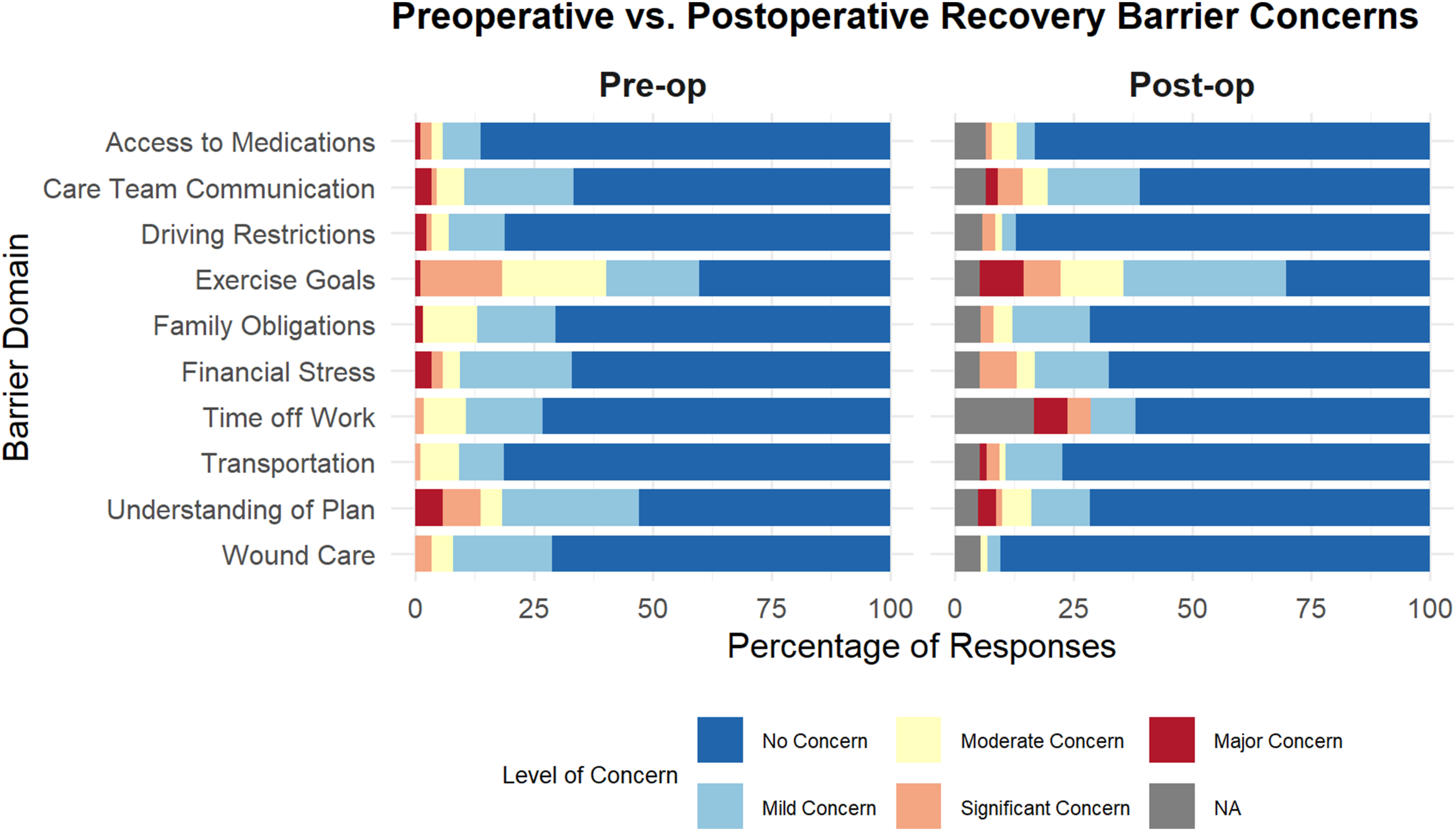
Mean responses to anticipated and experienced barriers are presented below in Figure 1 and in Table 2. Additionally, raw Likert responses from the pre-operative and post-operative surveys are seen in Figure 2. The most cited anticipated barriers were concerns about meeting exercise recovery goals, potential financial stress, and a lack of understanding of post-operative care. The most frequently encountered barriers in the post-operative arm included not meeting exercise goals, concerns with care team responsiveness, financial stress, and a lack of understanding of the post-operative plan. Table 2 presents the results of the Wilcoxon Rank Sign tests between pre- and post-operative surveys for each barrier. There was statistically significant variation in patients’ pre- and post-operative scores for meeting exercise goals (Z = −4.25, P < 0.01), performing post-operative wound care (Z = −3.68, P < 0.05), and an understanding of the post-operative care plan (Z = −2.90, P < 0.05), indicating that these barriers were encountered less frequently than anticipated. Mean Pre-operative (Anticipated) Barriers, and Experienced (Post-operative) Barriers Measured at 6 Weeks. Significant Wilcoxan Ranked Sign Testing Between Pre-operative and Post-operative Scores are Noted With an Astricts (P < 0.05) Wilcoxon Ranked Sign Test for Pre-post Operation Barrier Score Differences Table 2: Average anticipated barriers (pre-operative survey scores) to encountered barriers (post-operative survey scores) as measured by Likert scale. Results of Wilcoxon Ranked Sign Test comparing pre-operative and post-operative scores. Bolded P values denote clinical significance, indicating that there is a difference between anticipated and experienced barriers. Likert Distribution Plot Showing Raw Anticipated and Encountered Barrier Responses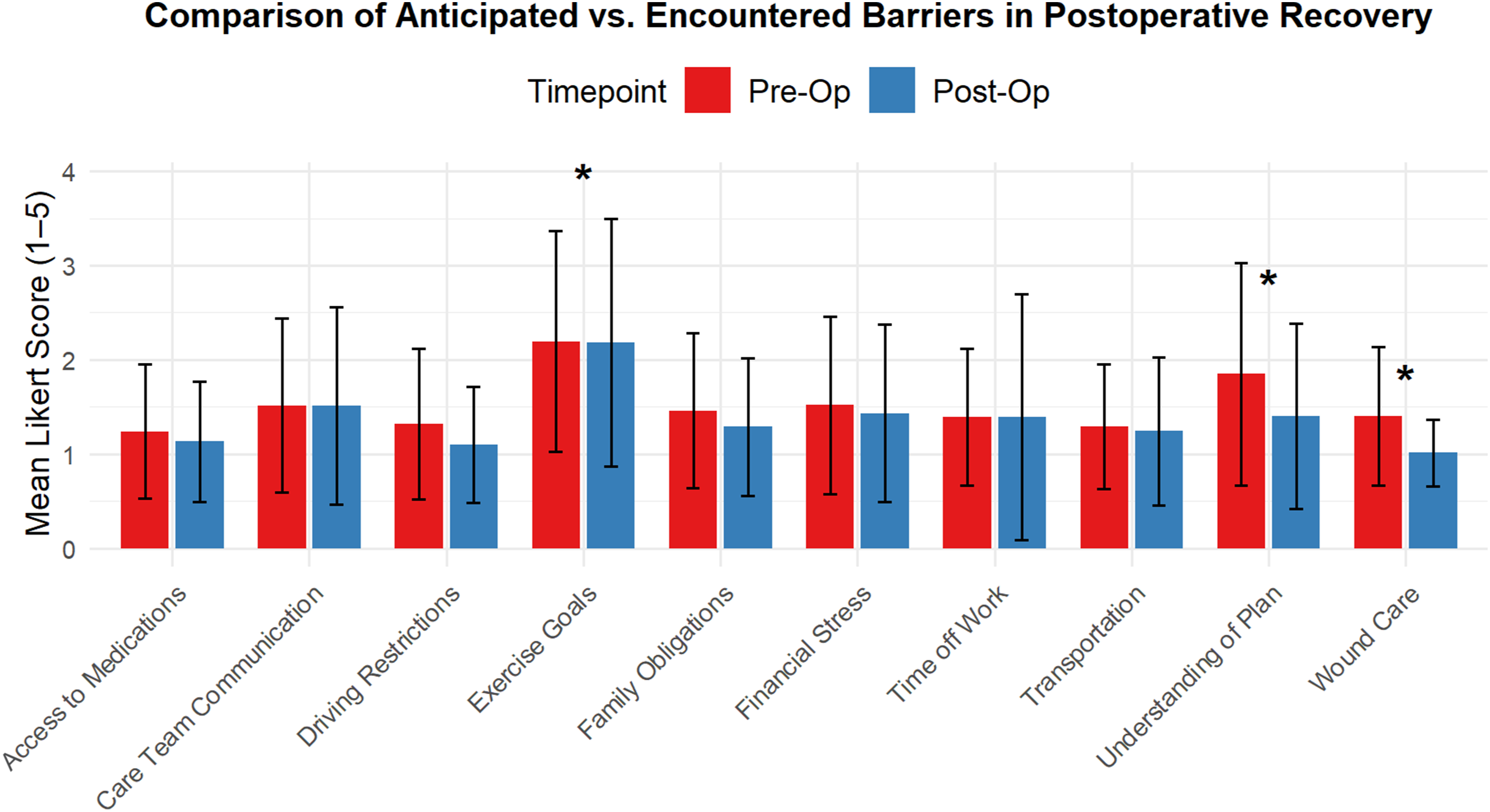
Relation of Barriers to Patient-Reported Outcomes
Logistic Regression of MCID for ODI Compared to Encountered Barriers
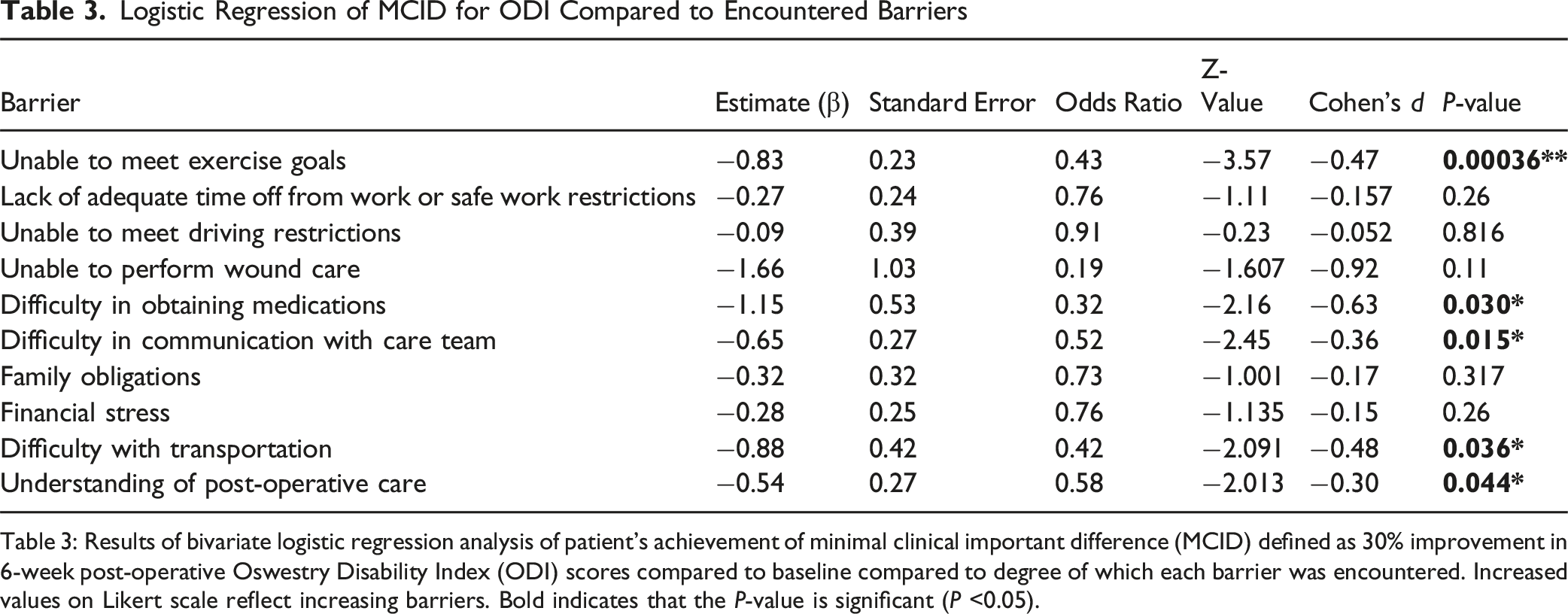
Table 3: Results of bivariate logistic regression analysis of patient’s achievement of minimal clinical important difference (MCID) defined as 30% improvement in 6-week post-operative Oswestry Disability Index (ODI) scores compared to baseline compared to degree of which each barrier was encountered. Increased values on Likert scale reflect increasing barriers. Bold indicates that the P-value is significant (P <0.05).
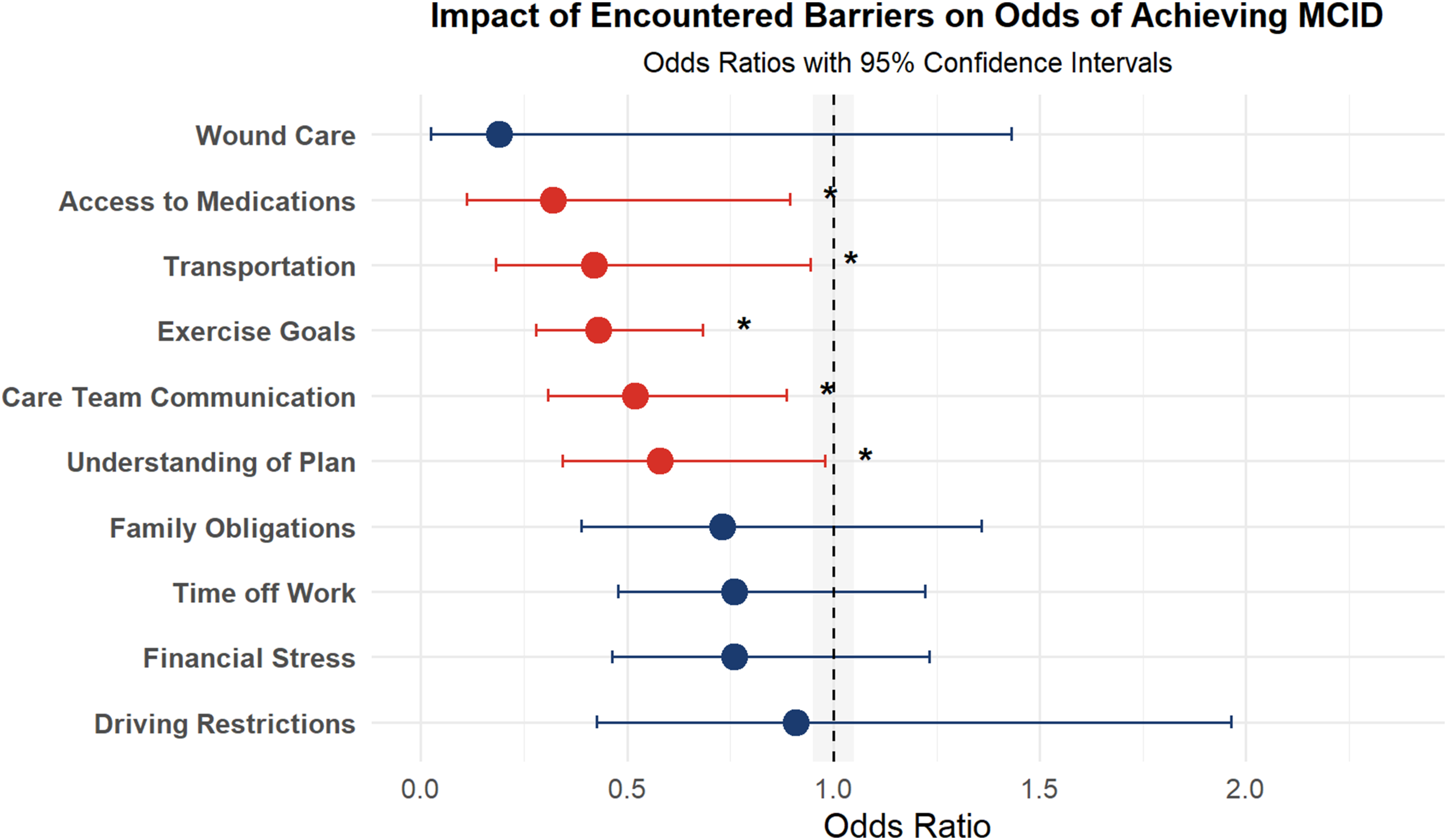
Forest Plot Depicting the Odds of Failing to Achieve MCID in ODI Scores Based on Encountered Post-operative Barriers. Odds Ratios (OR) and 95% Confidence Intervals (CI) Were Derived From Logistic Regression Analysis. ORs Below 1 Suggest a Decreased Likelihood of Failing to Achieve MCID. Statistically Significant Barriers (P < 0.05) are Marked With an Asterisk
By contrast, other encountered barriers were not significantly correlated with achieving MCID. These included difficulty with work restrictions, driving restrictions, wound care, family obligations, and financial stress.
Correlation of Barriers and Social Vulnerability Index
Social Vulnerability Index Spearman Correlations
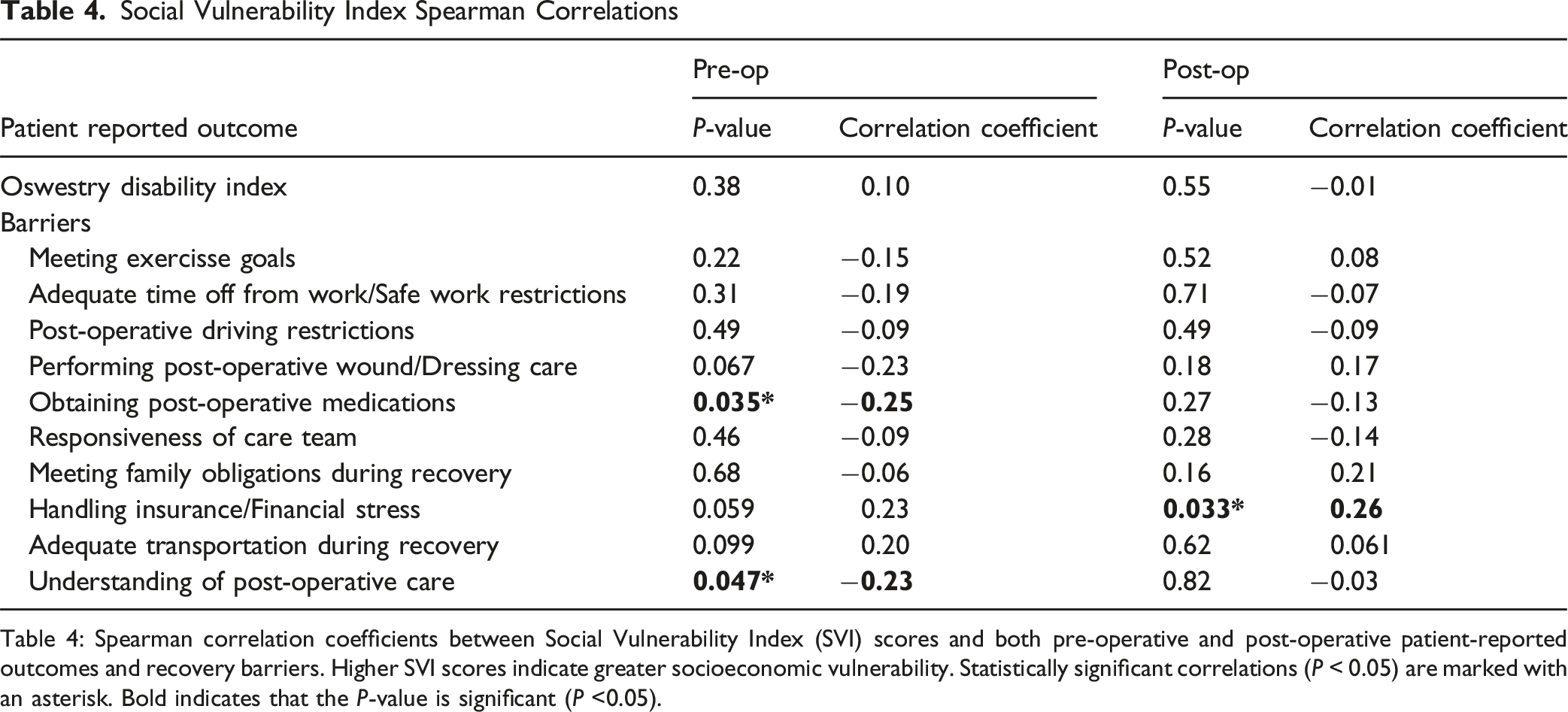
Table 4: Spearman correlation coefficients between Social Vulnerability Index (SVI) scores and both pre-operative and post-operative patient-reported outcomes and recovery barriers. Higher SVI scores indicate greater socioeconomic vulnerability. Statistically significant correlations (P < 0.05) are marked with an asterisk. Bold indicates that the P-value is significant (P <0.05).
Discussion
As the global population continues to age, it is expected that the volume of degenerative lumbar spine surgeries will continue to climb, potentially doubling by 2050. 24 It is therefore critical to gain a detailed understanding on what factors drive patient outcome. The current study aimed to examine patients’ anticipated and experienced barriers after 1-2 level decompression surgery, the correlations between these barriers and PROMs, and the impact of socioeconomic status on outcomes.
Comparison of Anticipated and Encountered Post-operative Barriers to Recovery
In the current study, patients expressed apprehension and uncertainty during the pre-operative period. These concerns were centered on the ability to meet exercise goals, understand their recovery plan, and concerns over finances related to their surgical episode of care. These concerns provide clinicians with insight into how best to target patient education, as they may not be openly stated during formal clinical encounters with the care team. In the post-operative period, the barriers patients encountered were similar to those they were most concerned about in the pre-operative period.
This study demonstrated that generally there was no significant difference between pre-op anticipated and post-operative encountered barriers. The exceptions were the barriers of wound care, meeting exercise goals, and understanding of recovery. For these exceptions, all Z-scores were negative, indicating that patients anticipated more significant barriers than they encountered. These results indicate that patients have good insight into the parts of the surgical recovery that will be challenging for them, providing an opportunity for preventive interventions.
Our novel exploration of patients’ anticipated barriers compared to those they experience is helpful for both patients and clinicians. For patients, these findings help guide discussions and provide reassurance for areas of increased concern. From the clinician’s standpoint, these findings support that patients have the most significant insight into their unique social situation. The time to tailor interventions to specific patients can begin in the pre-operative phase of care. Trusting patients to self-identify barriers may provide a method to target interventions most cost-effectively and strategically.
Encountered Barriers Affect Patient-Reported Outcomes
The second objective was to measure the impact of encountered barriers on achieving MCID for ODI scores. Among the ten barriers assessed in this study, five showed a statistically significant correlation with lower odds of achieving MCID: difficulty in exercise, access to medications, transportation, difficulties contacting the care team, and understanding of the post-operative plan.
The strongest correlation was between patients who experienced issues meeting exercise goals and those who did not encounter such issues following their surgery. Specifically, for each unit increase in barriers to exercise, the odds of obtaining MCID decreased by approximately 57%. This stepwise risk progression underscores one of the main purposes of seeking qualitative measures of barriers, as opposed to previous narrative-based explorations of patients’ post-operative spine recovery. This finding also had a moderate effect size (Cohen’s d = −0.47), underscoring its clinical relevance. By using statistics to guide how each severity level of a patient’s score for a particular barrier is associated with further decreasing outcomes, we hope to spark further studies and open discussion between patients and providers regarding the post-operative period.
The influence of post operative exercise and activity level following spinal surgery has, in part, been limited by the ambiguity on the definition of “exercise.” A lack of standardization across many exercise recommendations and patient-specific limitations compounds this ambiguity. Review of the literature describes patients with a higher number of post operative steps following their surgery were more likely to achieve optimal surgical outcomes. 25 Additionally, several recent meta-analyses have found small clinical benefits for supervised physiotherapy in the post-operative period.26,27 Further randomized control studies are needed to evaluate the role post-operative exercise, with specific attention to identifying patients that would benefit from early intervention. The current study demonstrates that difficulty in post-operative exercise decreases the likelihood of achieving MCID. Thus, the treating surgeon may want to consider targeting pre-operative education and enrollment in potential interventions for patients with self-identified risk barriers to exercise to improve outcomes.
The association between difficulties in obtaining medications and a decrease in achieving MCID highlights the role of pain management and post-operative pharmacological support in the early stages of recovery. This result echoes previous studies, which described that financial constraints, insurance coverage issues, pharmacy availability, and prescription delays result in worse pain levels, reduced mobility, and delayed functional improvement.28,29 Furthermore, the current study adds an important socioeconomic dimension, as difficulty in medication access was significantly associated with higher SVI.
Similarly, transportation barriers have previously been identified as a social risk factor associated with healthcare disparities across the United States. 30 The current study results that transportation barriers are associated with a lower likelihood of achieving MCID, adding to this body of literature, and providing specific evidence for addressing this need in the spine surgery population. As described in prior studies, potential interventions include expanding telemedicine follow-up options and considering hospital-supported patient transport services for at-risk patients.31,32
The final two barriers found to have a significant correlation with a lower likelihood of achieving MCID were difficulties in communication with the care team and limited understanding of the post-operative care plan. Both barriers highlight the essential nature of effective communication and education in the pre- and post-operative care phases, while showing that there is room for improvement in our current approach. In an era focused on precision medicine and personalized care, understanding these specific stressors provides opportunities to improve post-operative outcomes and satisfaction with surgical care.
This approach provides a more objective and specific understanding of the recovery period, and guides which barriers have the most significant clinical impact. Highlighting these specific barriers provides evidence for health systems, policymakers, and institutions to implement practical improvements in patient care. Clinicians can apply these findings by incorporating structured pre-operative education that anticipates patient-specific barriers, such as clarifying exercise expectations, confirming medication access before discharge, and arranging transportation or telehealth options for follow-up. The most promising aspect of this study is the barrier to meeting post-operative exercise goals, which is represented by the strongest statistical correlation and is the most promising candidate for targeted interventions into potential enhanced recovery protocols. Future studies should evaluate the effectiveness of these targeted interventions and assess whether addressing these barriers improves long-term functional outcomes.
Patient Socioeconomic Status and Post-operative Barriers
The final objective of the current study was to assess the effect of socioeconomic status as measured by SVI on the frequency of encountered barriers. The results of the current study demonstrate that more at-risk patients (higher SVI scores) were correlated with increased pre-operative concern for obtaining medications, as well as a lack of understanding of the recovery plan. Regarding the increased concern for obtaining medications, one contributing factor may be the distribution of pharmacies. A 2023 geospatial analysis performed by Adepoju et al 33 found that patients living in medically underserved areas face twice the travel distances to pharmacies, compounded by a disproportionate rate of pharmacy closures. Identification of this barrier provides an opportunity for pre-discharge interventions such as “Meds-to-Beds,” which has previously been shown to increase post-operative compliance in select populations. 34 The other barrier correlated with increased SVI was post-operative financial stress. This has previously been reported in patients undergoing hand surgery. Our findings contribute to the evidence that this stress is disproportionately experienced by individuals living in high social vulnerability areas. 35 Embedding social vulnerability screening (eg, SVI mapping or brief intake questions) can help identify at-risk patients early and prompt targeted support through social work or care coordination.
Limitations
This study had several notable limitations. First, the sample size was limited, drawn from a single urban center, with demographics that may not reflect the United States population at large. This may limit the generalizability of the findings and not be representative of some ethnic/racial groups, and the small cohort may limit the ability to detect smaller effect sizes. The study also relied on self-reported data, which may be subject to recall bias, patient attention, and selection bias. Although surveys were administered prospectively to reduce recall bias, patient perception and response variability remain possible sources of error.
Additionally, the study did not account for potential confounding factors such as comorbidities, variations in surgical techniques, and variations in the post-operative plan method. The use of a Likert scale for assessing barriers may not capture the full extent of patient experiences. The original questions assessing the barriers are not from a validated questionnaire, which could call into question their effectiveness in measuring the intended variables. Our study collected patients from seven orthopedic and neurologic surgeons, and variation in personal practice style may have impacted patients’ pre-operative and post-operative experience. Another important limitation is that outcomes were assessed only at 6-week postoperatively, which may not reflect long-term recovery patterns or the sustained impact of postoperative barriers on patient outcomes. The reason for selecting the 6-week follow-up data was to control for variation in patient recovery in the long term. With procedures such as 1-2 decompression surgeries, a relatively quick recovery is expected. May patients undergoing spine surgery have chronic low-back pain and comorbidities that may impact more longer-term outcome follow up and confound functional outcome scores, concern that extending follow-up into longer periods of time would not be focused on isolated recovery from a single surgical procedure, but would be moving towards a generalized picture of a patients health and function, which is beyond the scope of this paper. Future studies should include larger, multi-center cohorts, validated survey instruments, and longer-term follow-up to confirm these findings and determine the persistence of observed associations.
Conclusion
The current study provides observations on patient perspectives of anticipated and experienced barriers associated with lumbar decompression surgery. Our study found that patients were typically able to predict what barriers they were likely to experience in the post-operative period. The barriers associated with a lower likelihood of a successful surgical outcome included issues with post-operative exercise, difficulty obtaining medications, transportation problems, communication difficulties with the care team, and a lack of understanding of the post-operative plan. All these barriers demonstrated a moderate effect size. This study provides novel insight into how preoperative patient expectations align with postoperative realities and how this alignment (or misalignment) affects functional recovery. The ability to identify barriers most predictive of poor outcomes—such as difficulties with post-op exercise, medication access, and understanding care instructions—offers a foundation for targeted interventions.
Supplemental Material
Supplemental Material - Barriers to Adhering to Post-operative Recovery in Spinal Decompression Surgery and Impact on Patient-Reported Outcomes
Supplemental Material for Barriers to Adhering to Post-operative Recovery in Spinal Decompression Surgery and Impact on Patient-Reported Outcomes by Paul Wilson, Kiumars Edalati, Michael Jeffko, Aiyush Bansal, Trisha Lipson, Kenneth Nguyen, Jerry Du, Eric Varley, Philip K. Louie in Global Spine Journal.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All raw data for this study is available upon request to the authors.
IRB Approval
This study received approval from the institutional review board (IRB23-013).
Previous Presentations
The preliminary findings of this study were presented at the 2024 Society for Minimally Invasive Spine Surgery Annual Meeting in Las Vegas, Nevada as an E-poster.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.