
Abstract
Study Design
Retrospective cohort study of a national database.
Objectives
This study investigates the association between preoperative antidepressant use and postoperative opioid utilization as well as overall outcomes following primary anterior cervical fusion (ACF) and posterior cervical fusion (PCF).
Methods
We conducted parallel retrospective cohort analyses utilizing TriNetX for patients aged ≥18 years old with ≥2-year follow-up undergoing primary ACF and PCF between December 31, 2006, and December 31, 2022. Cohorts were thoroughly matched resulting in 4575 ACF and 3497 PCF pairs. Medical outcomes, opioid abuse, healthcare utilization, mechanical and surgical outcomes were assessed through risk ratios (RR), risk differences, P-values, and Kaplan-Meier analysis.
Results
Antidepressant use was associated with increased new opioid prescriptions from 2 weeks to 2 years (ACF RR 1.090-1.130, P < 0.001; PCF RR 1.060-1.078, P < 0.001), higher hospital readmissions (RR 1.484, P < 0.001), prolonged inpatient stays (RR 1.329, P < 0.001), and ED visits from 6 weeks to 2 years (ACF RR 1.150-1.184, P < 0.001; PCF RR 1.092-1.144, P ≤ 0.034). Postoperative infections were elevated at 2 years (ACF RR 1.679-2.060, P ≤ 0.008; PCF RR 1.375-1.677, P ≤ 0.020). Opioid abuse was higher at 2 years (ACF RR 2.8000, P = 0.003; PCF RR 2.667, P = 0.001), and pulmonary embolism increased in ACF at 2 years (RR 1.633, P = 0.032). Reoperations were elevated at 1 and 2 years (RR 1.238-1.371, P ≤ 0.045), with reduced 2-year reoperation-free survival in ACF (P = 0.001) and PCF (P = 0.045).
Conclusion
Preoperative antidepressant use is associated with significantly increased risks of postoperative opioid utilization and both medical and surgical complications, including sepsis, infections, adjacent segment disease, and reoperations, up to 2 years after primary anterior or posterior cervical fusion.
Keywords
Introduction
Cervical spine fusion is an increasingly utilized surgical approach for the management of degenerative, traumatic, and compressive pathologies through both anterior and posterior procedures. In recent years, the utilization of both anterior and posterior cervical fusion procedures has increased substantially, with current estimates exceeding 160,000 procedures annually in the United States, a trend largely driven by an aging population and the broadening of surgical indications.1,2 Despite improvements in surgical technique and perioperative optimization, the risk of complications such as infection, adjacent segment disease, pseudoarthrosis, and revision surgery remains a significant concern.3-5 In the effort to optimize surgical outcomes, attention has turned toward identifying perioperative factors that may influence both medical and mechanical postoperative complications.
One such factor is the preoperative use of antidepressant medications. This class of medications, which include selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and atypical agents, are frequently prescribed for depression, anxiety, and chronic pain—conditions often seen in spine surgery patients.5,6 Recent national data estimate that over 15% of U.S. adults use antidepressants, making these medications particularly relevant in the perioperative setting. 7 Beyond their neurochemical effects, antidepressants have been implicated in physiologic alterations that may impact surgical risk profiles. For example, serotonergic agents may impair platelet aggregation and increase bleeding risk, while others may interfere with bone metabolism and healing, potentially affecting arthrodesis rates.8-12
These concerns are supported by studies in general and orthopedic surgery, which have found associations between antidepressant use and increased intraoperative blood loss, postoperative transfusions, infection, and delayed wound healing.13-15 In spine surgery, antidepressant use has been associated with an increased risk of complications such as pseudarthrosis and revision procedures.16,17 However, many of these studies are limited by single-center designs, modest sample sizes, single-level fusions, or short-term outcome windows.
To address this gap, the present study examines the relationship between preoperative antidepressant use and postoperative outcomes following primary 1-2 level anterior and posterior cervical spine fusion. Using a large, multicenter national database, we analyzed both short-term medical complications and long-term mechanical outcomes, along with postoperative opioid use and healthcare utilization. We hypothesize that antidepressant use is associated with higher rates of opioid use and increased risk of both short-term and long-term postoperative complications following anterior or posterior cervical fusion. Understanding these associations may support a more informed, multidisciplinary approach to perioperative care in this high-risk population.
Methods
Study Design and Data Source
This retrospective cohort study utilized de-identified patient data from TriNetX, a U.S.-based federated health research network comprising over 130 million patients across more than 100 healthcare organizations. TriNetX standardizes data using controlled clinical terminologies (e.g., ICD, CPT, LOINC, RxNorm), allowing for large-scale, multisite clinical queries. Data quality, completeness, and granularity depend on the documentation practices of the contributing institutions, and site-specific data validation protocols are not publicly disclosed. However, TriNetX employs internal data curation and standardization procedures to promote consistency across the network. Data queries for this study were executed on April 3, 2025. As this study relied solely on aggregated, de-identified patient records without individually identifiable information, it was approved for exemption from Institutional Review Board approval by our academic institution. Medication exposure reflects recorded prescriptions and does not confirm adherence.
Patient Selection
Adult patients (≥18 years) undergoing either primary anterior cervical fusion (ACF) or primary posterior cervical fusion (PCF) between December 31, 2006, and December 31, 2022, were identified using CPT codes (22551, 22552) and (22600, 22614), respectively. The index event was defined as the date of the surgical procedure. Patients were stratified into 2 main analytical groups based on their surgical approach: anterior cervical fusion (ACF) or posterior cervical fusion (PCF). Within each surgical group, patients were further divided into 2 cohorts: (1) an antidepressant cohort, defined by active prescriptions for antidepressant medications (identified by NLM:VA:CN600) within the 90 days leading up to and including the day of the index surgery, and (2) a control cohort, comprising patients with no record of antidepressant prescriptions within the same 90-day preoperative window. Patients were required to have at least 2 years of follow up data to be included. Patients were excluded from both cohorts if they had pre-existing records of cervical fracture (ICD-10-CM: S12), malignant or unspecified neoplasms of the vertebral column or spinal cord (ICD-10-CM: C41.2, C79.5, D33.4, D43.4).
Propensity Score Matching (PSM)
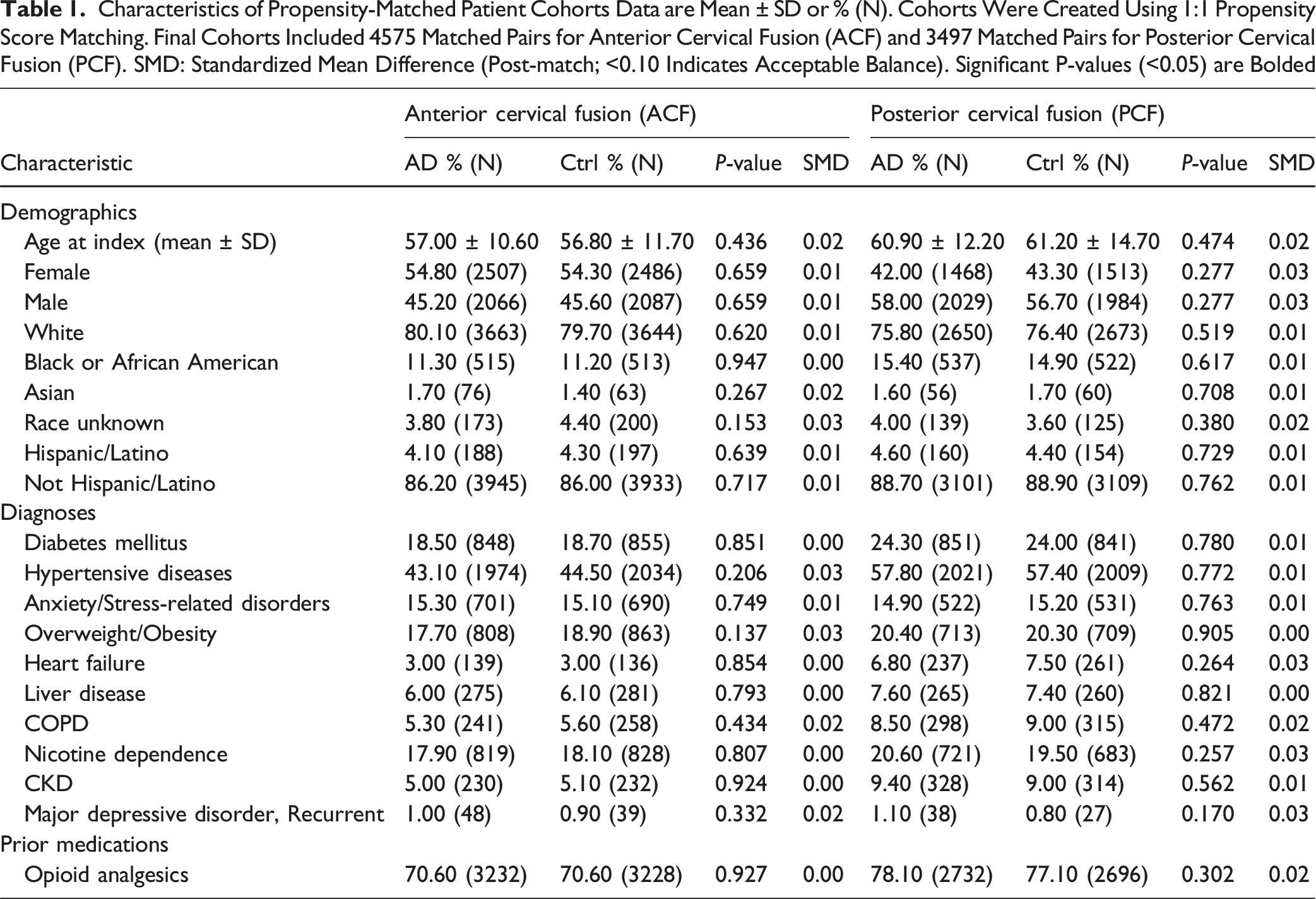
Characteristics of Propensity-Matched Patient Cohorts Data are Mean ± SD or % (N). Cohorts Were Created Using 1:1 Propensity Score Matching. Final Cohorts Included 4575 Matched Pairs for Anterior Cervical Fusion (ACF) and 3497 Matched Pairs for Posterior Cervical Fusion (PCF). SMD: Standardized Mean Difference (Post-match; <0.10 Indicates Acceptable Balance). Significant P-values (<0.05) are Bolded
Variables
Baseline patient characteristics included demographics (age, sex, race, ethnicity), relevant comorbidities (diabetes mellitus, hypertensive diseases, anxiety disorders, overweight and obesity, heart failure, diseases of liver, chronic obstructive pulmonary disease, nicotine dependence, chronic kidney disease, major depressive disorder), and prior medication use (prior opioid analgesics). These characteristics before and after matching for both ACF and PCF analyses are detailed in (Table 1).
Outcomes
The evaluated outcomes were categorized as: (1) Resource Utilization, Substance Abuse, and Medical Complications, and (2) Surgical and Mechanical Complications. Specific ICD-10-CM, CPT, NLM, and RxNorm codes used to define these outcomes are listed in (Supplemental Table S1). Resource utilization, substance abuse, and medical complications included: new opioid prescriptions, hospital readmission, inpatient hospitalization, overall postoperative infection, sepsis, emergency department (ED) visit, new diagnosis of opioid abuse, pulmonary embolism (PE), pneumonia, deep vein thrombosis (DVT), and mortality. These outcomes were assessed at 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and 2 years postoperatively. Surgical and mechanical complications included: adjacent segment disease (ASD), spine infection (discitis, osteomyelitis, intraspinal abscess), reoperation, pseudarthrosis, surgical wound disruption, and hardware failure. These outcomes were assessed at 6 months, 1 year, and 2 years postoperatively.
Statistical Analysis
Descriptive statistics were used to summarize baseline patient characteristics, presented as means with standard deviations (SD) for continuous variables and as percentages for categorical variables. Differences between cohorts before and after PSM were assessed using t-tests for continuous variables, and chi-squared or Fisher’s exact tests for categorical variables, as appropriate.
For postoperative outcomes, relative risks (RRs) with 95% confidence intervals (CIs) and risk differences (RDs) were calculated to compare the antidepressant and control cohorts within each matched surgical group (ACF and PCF). P-values were derived from these comparisons. Kaplan-Meier survival analysis was performed to assess time to reoperation, with differences between curves evaluated using the log-rank test. Hazard ratios (HRs) from Cox proportional hazards models were also calculated for reoperation. All statistical analyses were performed using TriNetX analytics tools. A P-value <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 16,152 patients undergoing ACF and 13,336 patients undergoing PCF met the initial inclusion criteria. For the ACF analysis, 8183 patients were in the antidepressant cohort and 7969 in the control cohort before matching. After PSM, 4575 patients remained in each ACF cohort. For the PCF analysis, 6843 patients were in the antidepressant cohort and 6493 in the control cohort before matching. After PSM, 3497 patients remained in each PCF cohort.
As detailed in (Table 1), before matching, patients in the antidepressant cohorts for both ACF and PCF generally exhibited a significantly higher prevalence of several baseline comorbidities and differences in demographic factors. For instance, in the ACF cohorts, the antidepressant group had a significantly higher proportion of females (63.30% vs 40.50%, P < 0.001) and a markedly higher prevalence of anxiety, dissociative, and stress-related disorders (46.80% vs 8.70%, P < 0.001) compared to controls. Similarly, for the PCF cohorts before matching, the antidepressant group had a higher percentage of females (55.30% vs 32.10%, P < 0.001) and a greater prevalence of anxiety disorders (46.70% vs 8.70%, P < 0.001). Following propensity score matching, these and other baseline characteristics were well-balanced between the antidepressant and control cohorts for both ACF and PCF analyses, with SMDs generally <0.1.
Outcomes after Anterior Cervical Fusion (ACF)
Healthcare Utilization, Substance Abuse, and Medical Complications (ACF)
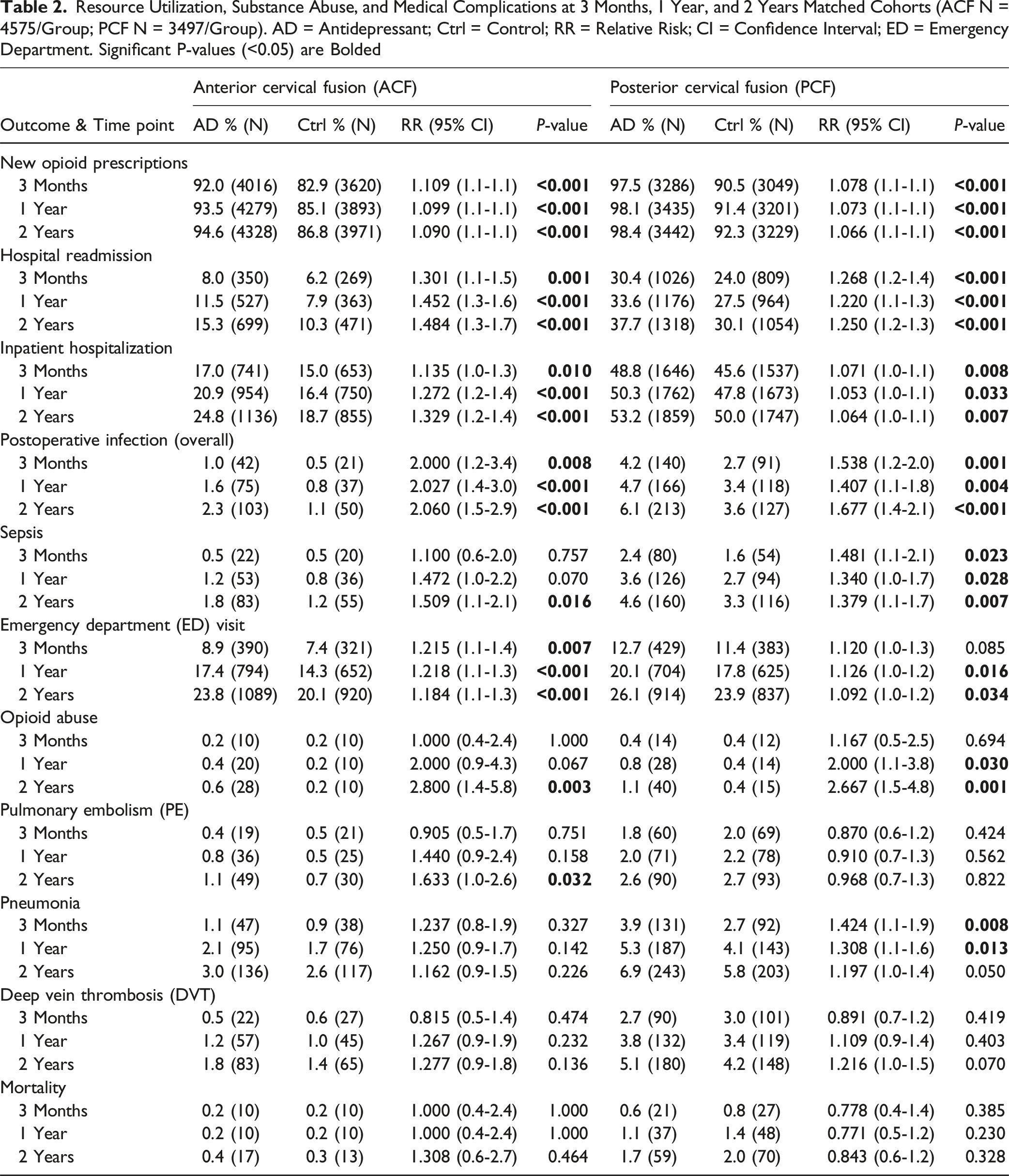
New opioid prescriptions were significantly higher in the ACF antidepressant cohort compared to controls across all evaluated time points. This difference was evident as early as 2 weeks (87.8% vs 78.0%, RR 1.130, P < 0.001) and persisted through 3 months (92.0% vs 82.9%, RR 1.109, P < 0.001), 1 year (93.5% vs 85.1%, RR 1.099, P < 0.001), and 2 years (94.6% vs 86.8%, RR 1.090, P < 0.001). Hospital readmission rates were consistently higher in the antidepressant group. At 3 months, the rate was 8.0% in the antidepressant group vs 6.2% in controls (RR 1.301, P = 0.001). This increased risk was maintained at 1 year (11.5% vs 7.9%, RR 1.452, P < 0.001) and 2 years, where readmission rates reached 15.3% in the antidepressant cohort compared to 10.3% in controls (RR 1.484, P < 0.001).
Resource Utilization, Substance Abuse, and Medical Complications at 3 Months, 1 Year, and 2 Years Matched Cohorts (ACF N = 4575/Group; PCF N = 3497/Group). AD = Antidepressant; Ctrl = Control; RR = Relative Risk; CI = Confidence Interval; ED = Emergency Department. Significant P-values (<0.05) are Bolded
Surgical and Mechanical Complications (ACF)
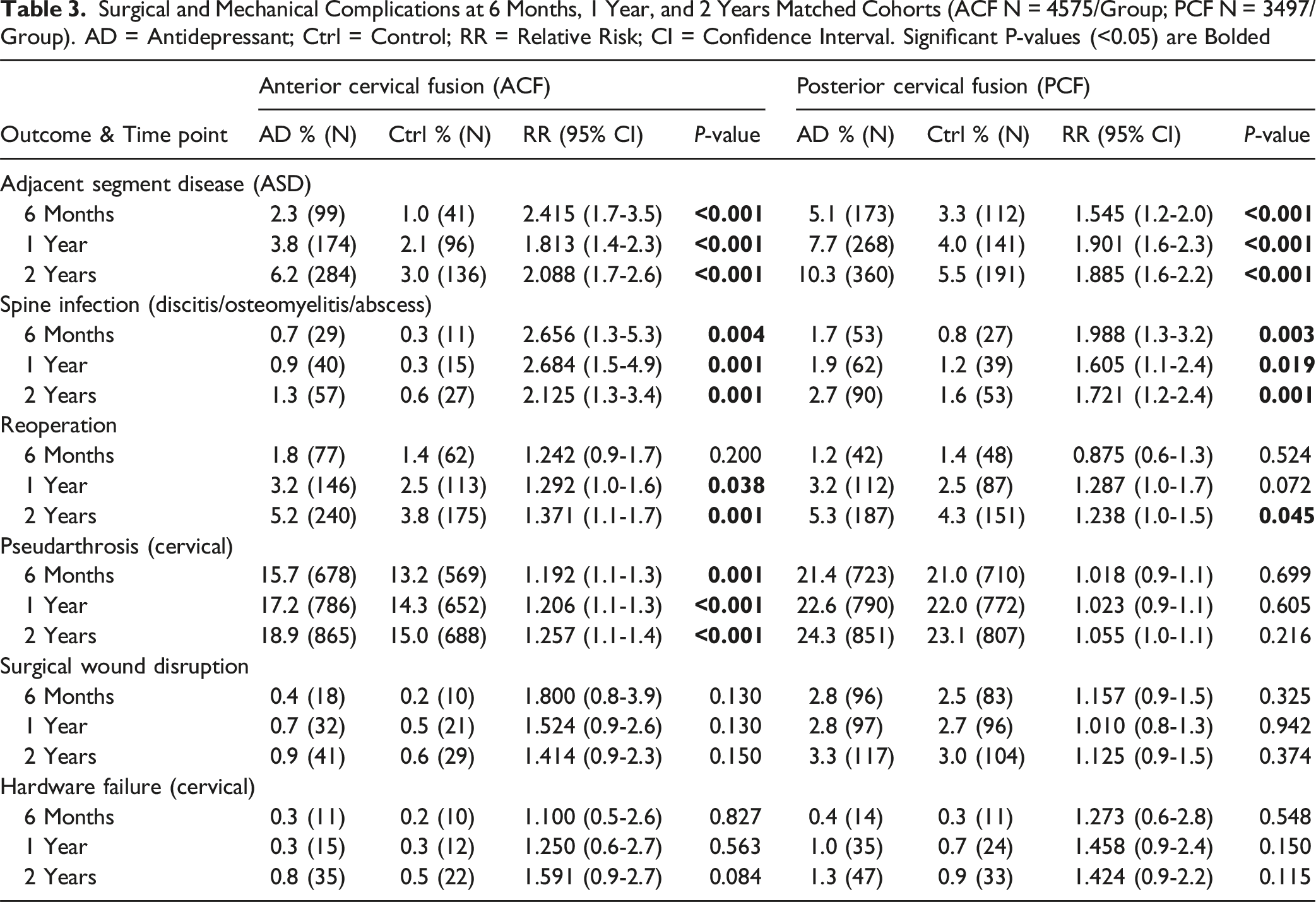
Surgical and Mechanical Complications at 6 Months, 1 Year, and 2 Years Matched Cohorts (ACF N = 4575/Group; PCF N = 3497/Group). AD = Antidepressant; Ctrl = Control; RR = Relative Risk; CI = Confidence Interval. Significant P-values (<0.05) are Bolded
Kaplan-Meier Analysis for Reoperation (ACF)
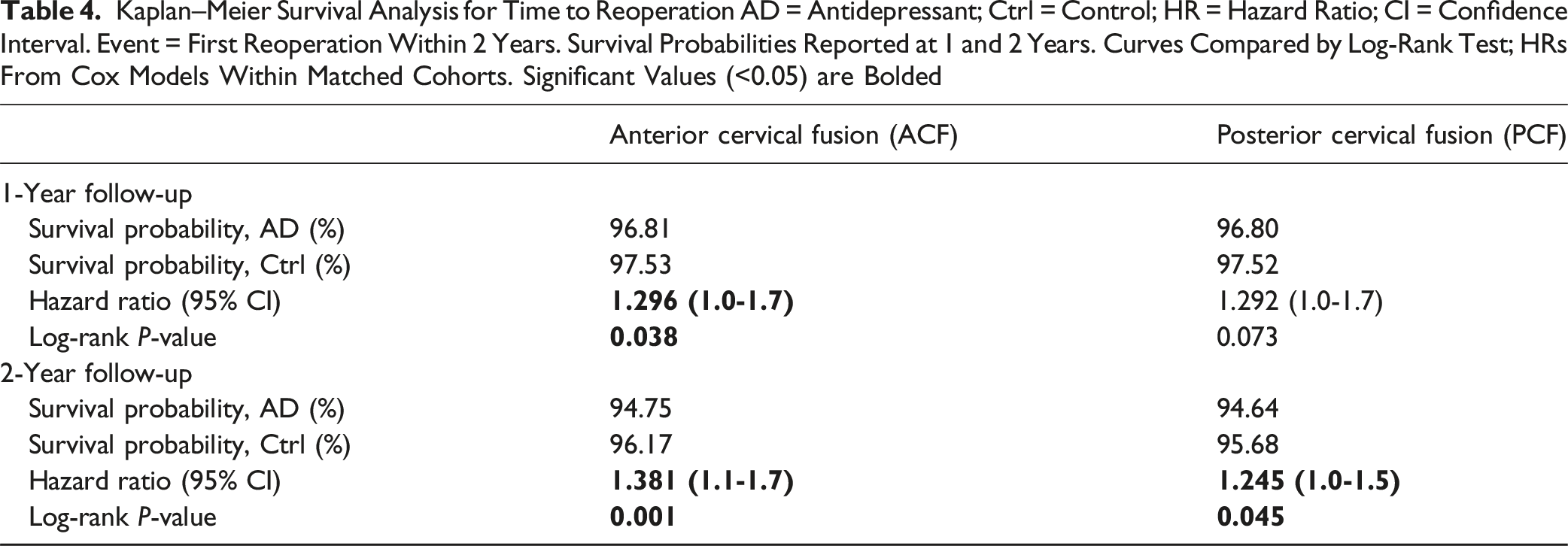
Kaplan–Meier Survival Analysis for Time to Reoperation AD = Antidepressant; Ctrl = Control; HR = Hazard Ratio; CI = Confidence Interval. Event = First Reoperation Within 2 Years. Survival Probabilities Reported at 1 and 2 Years. Curves Compared by Log-Rank Test; HRs From Cox Models Within Matched Cohorts. Significant Values (<0.05) are Bolded
Outcomes After Posterior Cervical Fusion (PCF)
Resource Utilization, Substance Abuse, and Medical Complications (PCF)
New opioid prescriptions were significantly higher in the PCF antidepressant cohort compared to controls across all evaluated time points. This difference was evident as early as 2 weeks (95.7% vs 90.2%, RR 1.060, P < 0.001) and persisted through 3 months (97.5% vs 90.5%, RR 1.078, P < 0.001), 1 year (98.1% vs 91.4%, RR 1.073, P < 0.001), and 2 years (98.4% vs 92.3%, RR 1.066, P < 0.001). Hospital readmission rates were consistently higher in the antidepressant group. This was evident as early as 2 weeks (26.3% vs 20.7%, RR 1.271, P < 0.001. At 3 months, the rate was 30.4% vs 24.0% (RR 1.268, P < 0.001). This increased risk was maintained at 1 year (33.6% vs 27.5%, RR 1.220, P < 0.001) and 2 years, where readmission rates reached 37.7% vs 30.1% (RR 1.250, P < 0.001) (Table 2).
Similarly, inpatient hospitalization was more frequent in the antidepressant cohort. Significance was observed from 3 months (48.8% vs 45.6%, RR 1.071, P = 0.008) and continued through 1 year (50.3% vs 47.8%, RR 1.053, P = 0.033) and 2 years, with rates being 53.2% vs 50.0% (RR 1.064, P = 0.007). Emergency department (ED) visits were significantly higher for the antidepressant group starting at 6 months (16.2% vs 14.2%, RR 1.144, P = 0.019), and this persisted through 1 year (20.1% vs 17.8%, RR 1.126, P = 0.016) and 2 years (26.1% vs 23.9%, RR 1.092, P = 0.034). Overall postoperative infections were significantly more common in the antidepressant cohort starting from 6 weeks (3.3% vs 2.1%, RR 1.559, P = 0.003). This difference persisted through 3 months (4.2% vs 2.7%, RR 1.538, P = 0.001), 1 year (4.7% vs 3.4%, RR 1.407, P = 0.004), and 2 years (6.1% vs 3.6%, RR 1.677, P < 0.001). Sepsis rates were significantly higher in the antidepressant group starting at 3 months (2.4% vs 1.6%, RR 1.481, P = 0.023). This increased risk was maintained at 6 months (3.1% vs 2.0%, RR 1.515, P = 0.007), 1 year (3.6% vs 2.7%, RR 1.340, P = 0.028), and 2 years (4.6% vs 3.3%, RR 1.379, P = 0.007).
New diagnoses of opioid abuse were significantly higher in the antidepressant group at 1 year (0.8% vs 0.4%, RR 2.000, P = 0.030) and this persisted at 2 years (1.1% vs 0.4%, RR 2.667, P = 0.001), though rates were low overall. Pneumonia rates were significantly higher for the antidepressant group at 3 months (3.9% vs 2.7%, RR 1.424, P = 0.008) and 1 year (5.3% vs 4.1%, RR 1.308, P = 0.013). Significance was not observed at 2 years or earlier time points. Rates of PE, DVT, and mortality were generally similar between cohorts (Table 2).
Surgical and Mechanical Complications (PCF)
Adjacent segment disease (ASD) was significantly more frequent in the antidepressant cohort from 6 months onwards. At 6 months, ASD rates were 5.1% vs 3.3% (RR 1.545, P < 0.001). This increased risk was maintained at 1 year (7.7% vs 4.0%, RR 1.901, P < 0.001) and 2 years (10.3% vs 5.5%, RR 1.885, P < 0.001). Spine infections also occurred more often in the antidepressant group. Significance was observed from 6 months (1.7% vs 0.8%, RR 1.988, P = 0.003). This increased risk was maintained at 1 year (1.9% vs 1.2%, RR 1.605, P = 0.019) and 2 years (2.7% vs 1.6%, RR 1.721, P = 0.001). Rates of reoperation were significantly higher in the antidepressant cohort at 2 years (5.3% vs 4.3%, RR 1.238, P = 0.045), with a trend towards higher rates at 1 year (3.2% vs 2.5%, RR 1.287, P = 0.072). Significance was not observed at 6 months. Surgical wound disruption, pseudarthrosis, and hardware failure did not show statistically significant differences at the evaluated time points (Table 3).
Kaplan-Meier Analysis for Reoperation (PCF)
Kaplan-Meier analysis showed significantly lower reoperation-free survival in the antidepressant cohort compared to the control cohort at 2 years (Log-Rank P = 0.045). A trend towards lower survival was observed at 1 year (Log-Rank P = 0.073) (Table 4).
Discussion
Our findings report that patients with a history of antidepressant use undergoing both anterior (ACF) and posterior cervical fusion (PCF) experienced significantly worse postoperative outcomes across a range of clinical outcomes and intervals. These patients consistently exhibited higher rates of opioid prescriptions, hospital readmissions, emergency department visits, and postoperative infections. Notably, antidepressant use was also associated with an elevated risk of serious complications such as sepsis, spine infections, adjacent segment disease, and reoperations. Kaplan-Meier survival analyses further revealed significantly reduced reoperation-free survival in the antidepressant prescribed patients.
Overall, these findings supplement existing literature indicating that preoperative depression and antidepressant use are associated with adverse postoperative outcomes. A systematic review and meta-analysis reported that depression significantly increases the risk of complications such as delirium, deep vein thrombosis, pulmonary embolism, surgical site infections, and reoperations following spine surgery. 18 Moreover, preoperative mental health diagnoses have been linked to increased postoperative opioid dependence. 19 However, our study substantially extends this literature by providing a more granular and comprehensive assessment. By using a robust, propensity-matched nationwide cohort, we offer a higher level of evidence and, for the first time, quantify these risks across a broad spectrum of medical and surgical complications for both anterior and posterior cervical fusion approaches specifically.
Our study revealed that patients on preoperative antidepressants had significantly higher rates of postoperative opioid prescriptions through 2 years for both ACF and PCF cohorts. This finding aligns closely with recent literature which found that preoperative antidepressant prescriptions were associated with higher odds of opioid use after cervical spine procedures. 20 Moreover data has underscored the strong link between depression, anxiety and persistent postoperative opioid dependence in spine surgery. 21 Given that chronic postoperative opioid use is a public health concern, our findings reinforce the importance of preoperative mental health optimization and robust multimodal pain management strategies in this population.
The increasing prevalence of depression and anxiety among surgical patients underscores the importance of understanding the implications of antidepressant use in the perioperative period. Research indicates that a significant proportion of surgical patients experience psychological distress; for instance, research utilizing the Hospital Anxiety and Depression Scale (HADS) found that 64% of hospitalized surgical patients were severely anxious, and 74% were severely depressed. 22 Specifically, in spine surgery, the prevalence of preoperative depression can be as high as 46%. 23
With such high prevalence of mental health problems amongst surgical patients, the use of antidepressants in the perioperative period presents a clinical dilemma; namely, the balance between managing a patient’s mental health and reducing the risk of post-surgical complications. Many studies have found that perioperative SSRI use is associated with increased risks including bleeding, transfusion requirements, and hospital readmission.24-26 In accordance with this data, we observed a nearly twofold increase in general postoperative infections and spine-specific infections among patients prescribed antidepressants. While these findings are concerning, discontinuing antidepressants abruptly can lead to withdrawal symptoms and exacerbate depression, potentially complicating postoperative recovery in other ways. 27 This underscores the need for antidepressant regimens to be holistically evaluated in the preoperative period, weighing the risk and benefit of discontinuing them based on individual patient circumstances.
The mechanism by which antidepressants negatively impact surgical outcomes has still not been entirely uncovered, but 1 potential mechanism is the effect of SSRIs on the bone at the cellular level. Antidepressants, particularly selective SSRIs, have been shown to adversely affect bone metabolism by negatively impacting the function of osteoblasts and osteoclasts. 28 Clinically, this is reflected in the association between antidepressants and bone loss, as well as the increased fall and fracture risk in patients on SSRIs.29-31 Another potential mechanism is that patients on antidepressants may be less likely to follow postoperative protocols after surgery, depending on the degree to which their depression is managed, and thus indirectly raise their risk of complications. This could also explain the increased likelihood of increased opioid use and overall infection rates in this cohort of patients.
While our findings highlight significant associations between preoperative antidepressant use and adverse postoperative outcomes, several limitations must be acknowledged. This study utilized a retrospective query from the TriNetX platform, which, although robust and multi-institutional, inherently limits control over data completeness and variable consistency. Furthermore, our reliance on administrative billing codes to define outcomes, such as opioid abuse, may underestimate the true prevalence of these conditions by capturing only formally diagnosed events. Moreover, our analysis focused exclusively on patients prescribed antidepressants preoperatively; those initiated on antidepressants postoperatively were not included, potentially underestimating the true impact of antidepressant use on long-term outcomes. Another limitation is the unmeasured confounding variables that may have influenced the outcomes Critically, this includes the inability to fully disentangle the effects of the antidepressant medication itself from the underlying clinical condition for which it was prescribed. Although our propensity matching controlled for diagnosed depression, the clinical nuance of disease severity, chronicity, or treatment resistance, which are themselves risk factors for adverse surgical outcomes, is not captured. Therefore, our findings should be interpreted as identifying an association with a high-risk patient profile characterized by antidepressant use, rather than demonstrating a direct causal effect of the pharmacologic agent alone. This distinction is crucial and represents a key area for future prospective research.
To strengthen the clinical applicability of our findings, future research should also incorporate prospective data collection with standardized variables and longer-term follow-up periods. We only obtained data on patients up to 2 years postoperatively and noticed a significant difference between the 1-and 2-year marks; this suggests that there could be even more significant differences years after the index surgery. Furthermore, subgroup analyses stratifying patients by antidepressant class—particularly selective serotonin reuptake inhibitors (SSRIs)—are warranted to identify whether specific pharmacologic profiles are more strongly associated with postoperative complications. Additionally, expanding this analysis to include other orthopedic surgeries, such as lumbar spinal fusions or total joint arthroplasties, would help determine whether these associations are procedure-specific or reflect a broader trend in surgical recovery among patients on antidepressants.
Conclusions
Our study found that patients prescribed antidepressants prior to anterior cervical or posterior cervical fusion experienced significantly higher rates of opioid use, hospital readmissions and surgical complications including adjacent segment disease, spine infections, and reoperations compared to matched controls. These findings highlight the need for multidisciplinary perioperative management strategies for patients prescribed antidepressants prior to cervical fusion surgery. Further prospective, multicenter studies are warranted to better elucidate this intricate relationship between preoperative antidepressant use and postoperative outcomes following cervical spine fusion.
Supplemental Material
Supplemental Material - Preoperative Antidepressants are Associated With Increased Risk of Opioid Use and Overall Complications Following Anterior and Posterior Cervical Fusion: A Nationwide Propensity-Matched Cohort Study
Supplemental Material for Preoperative Antidepressants are Associated With Increased Risk of Opioid Use and Overall Complications Following Anterior and Posterior Cervical Fusion: A Nationwide Propensity-Matched Cohort Study by Muhammad Waheed, Mohammed Fawaz, Zina Smadi, Abdelrahman Diab, Omar Diab, Hamza Dyab, Ahmad Nassr, Ilyas S. Aleem, Rahul Vaidya in Global Spine Journal.
Footnotes
Ethical Considerations
This study was reviewed by the Wayne State University IRB committee and was determined to be exempt from institutional review board approval (IRB number # 2025-061).
Consent for Publication
All authors consent to the publication of this manuscript and all associated material.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study have been acquired from the TriNetX database. The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.