
Abstract
Study Design
Single-center, retrospective cohort review.
Objective
This study aims to compare the impact of robotic and imaging-only navigation modalities on radiographic parameters following minimally invasive transforaminal lumbar interbody fusion (MI-TLIF).
Methods
Patients with degenerative spondylolisthesis who underwent one-level MI-TLIF using navigation or robotic modalities were included and divided into two groups: robotic-assisted (Robo) or imaging-only navigation (Nav). Radiographic parameters were assessed preoperatively and 6 months postoperatively. Outcome measures were screw and cage characteristics, postoperative disc height (DH) improvements, lumbar lordosis (LL), and slip reduction rates. Statistical analyses included paired and independent samples t-tests and multivariable linear regression analysis.
Results
The Robo group often used larger screw diameters, deeper cages, and more expandable cages, while the Nav group used wider cages. The Robo group demonstrated significantly greater DH improvement compared to the Nav group (average improvement: 71.6% vs 22.5%, P = 0.002). However, the Nav group showed significantly greater LL restoration than the Robo group (P = 0.006), and preoperative LL was independently associated with postoperative LL (β = 0.64, P < 0.001). No clear differences in slip reduction or cage subsidence were observed.
Conclusions
In MI-TLIF, robotic guidance was associated with greater DH restoration and the use of larger screws, whereas LL restoration appeared to depend mainly on preoperative sagittal alignment and was greater with image-guided navigation. These findings suggest that each modality can be leveraged to optimize different radiographic goals and underscore the need for studies integrating implant strategies with clinical outcomes.
Keywords
Introduction
Technological advancements in spine surgery have transformed the field of minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) in recent years. Among these advancements, robotic assistance and advanced navigation are two such technologies that enable high levels of precision in spine surgery, even under conditions of limited direct visualization such as in the minimally invasive technique. These robotic navigation systems enhance the surgeon’s ability of accurate hardware placement. This accuracy helps to maximize the size of the screw based on a patient’s anatomy, leading to an improved biomechanical stability of the construct. Biomechanical stability plays a crucial role in the reduction maneuver particularly when patients require restoration in disc height (DH) and segmental lordosis due to degenerative lumbar spine disease such as spondylolisthesis.1-5 In contrast, navigation-only techniques remain widely used because of their intraoperative flexibility, allowing real-time adjustment of instrumentation. This flexibility can be advantageous during key steps such as cage positioning, rod contouring, and sequential compression or distraction.
Postoperative restoration of DH is of great interest for surgeons to achieve better alignment and indirect neuroforaminal decompression of nerves. Furthermore, an increased DH is associated with the reduced risk of adjacent segment disease by minimizing stress on adjacent levels.6-9 Achieving optimal sagittal alignment should also enhance long-term outcomes.10,11 The precise and larger screw placement achievable with robotic assistance may provide a stronger construct for DH restoration, whereas alignment correction may depend more on the surgeon’s intraoperative strategy and three-dimensional handling, which can be facilitated by navigation-only approaches. However, despite these insights, limited data exist directly comparing the impact of robotic vs navigation-only modalities on postoperative radiographic parameters, including DH restoration, spinal alignment, and spondylolisthesis slip reduction.1,4,12,13
This study aims to investigate the impact of robot-assisted vs navigation-only modalities on implant details and postoperative radiographic parameters following MI-TLIF for degenerative spondylolisthesis. We hypothesized that the use of robot-assisted modalities would allow surgeons the precision and confidence to use larger screws and interbody cages, thus stabilizing the fusion and leading to the restoration of DH, segmental lordosis, and other spinal alignment parameters. Clarifying these associations will guide surgeons in selecting navigation modalities when conducting MI-TLIFs based on operative goals, preoperative alignment parameters, and patient anatomy.
Methods
Study Design and Patient Population
This study was a single-center, retrospective cohort review, including patients from a multi-surgeon database. Patients who underwent a 1-level MI-TLIF between June 2017 and September 2023 using either robotics or navigation modalities were included. Inclusion criteria were: (1) patients with a primary diagnosis of degenerative spondylolisthesis, (2) patients with a 6-month clinical follow-up, (3) patients over 18 years of age, and (4) patients who underwent MI-TLIFs. We excluded patients with (1) longitudinal midline incision, (2) additional concurrent adjacent level procedures, (3) absence of an interbody cage, and (4) a fusion construct using more or less than four screws. This study included cases from 6 surgeons, with 4 of the 6 performing MI-TLIF using either robotics or navigation modalities, and 2 only using robotic modalities. Of the surgeons who used both modalities, they preferentially selected robotic methods (used in 56.6-91.4% of their cases). Data collection were managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center for Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.14,15
Surgical Technique
MI-TLIF were performed as previously described in the literature.16-18 Patients underwent either 3D intraoperative navigational imaging alone or combined 3D imaging with robotic assistance. Pedicle screws were placed through minimal parasagittal incisions, either manually or with robotic guidance. Facetectomy was performed under microscopic visualization using a high-speed burr and Kerrison rongeurs. After complete discectomy, the disc space was prepared with autograft or allograft bone fragments placed anteriorly, followed by insertion and expansion of an interbody cage under direct visualization.
Data Collection
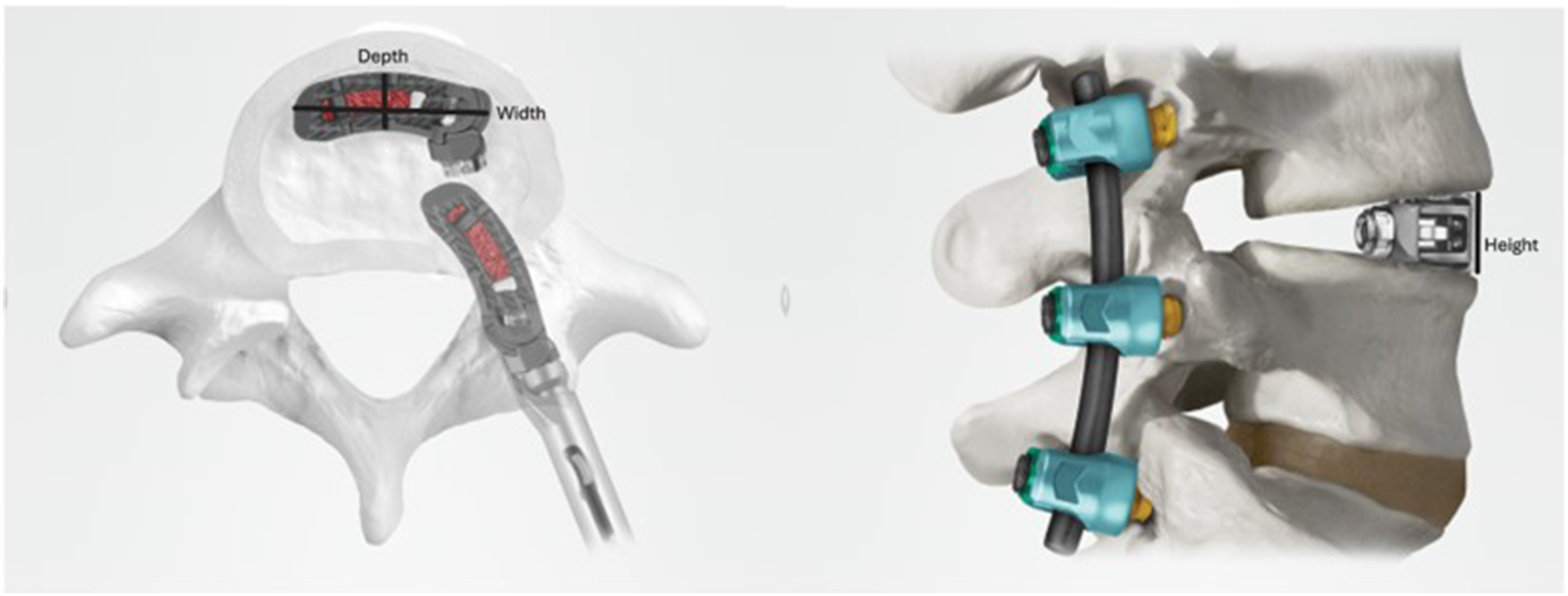
Patient demographic data was obtained from electronic medical records and included age, height, weight, body mass index (BMI), Charlson Comorbidity Index (CCI), gender, race, American Society of Anesthesiologists Physical Status Classification (ASA), navigation modality, operative time, and estimated blood loss. We additionally collected implant details used such as screw length and diameter and cage details (height, width, depth) (Figure 1). These data were collected from specific implant logs for each case, provided by the vendor. For expandable cages, the mean value between the nominal and maximum expanded heights provided by the vendor was used, whereas for non-expandable cages, the nominal height was recorded. This graphic of interbody cages used in MI-TLIFs show the dimensions analyzed (depth, width, and height). For expandable cages, the cage height median value was used for data analysis. Globus Medical provided explicit permission for use of images from their website
44
Radiographic parameters were measured by a board-certified surgeon or clinical fellows specializing in spine surgery based on standing lateral radiographs. Postoperative measurements were taken from the 6-month follow-up, including DH at the surgical segment and global spinopelvic alignment parameters. DH was calculated as the mean of anterior and posterior values (Figure 2). Global spinopelvic alignment parameters included pelvic tilt (PT), sacral slope (SS), pelvic incidence (PI), global lumbar lordosis (LL), proximal LL (pLL, L1-L4) and distal LL (dLL, L4-S1). PT is defined as the angle between the vertical axis and a line through the midpoint of the sacral end plate, SS as the angle between the sacral plate and the horizontal, PI as the angle between a line perpendicular to the sacral plate and a line extending from the femur, and LL as the angle between the superior endplates of L1 and S1. Vertebral slip was quantified as the distance between the posterior walls of the upper and lower vertebral bodies at the index level (Figure 2). Slip reduction rate was quantified as the percent reduction achieved after MI-TLIF. Lateral radiographs demonstrating anterior and posterior disc height measurement, as well as slip measurement. (A) shows the direction of the vectors used, and (B) shows the measurements of these vectors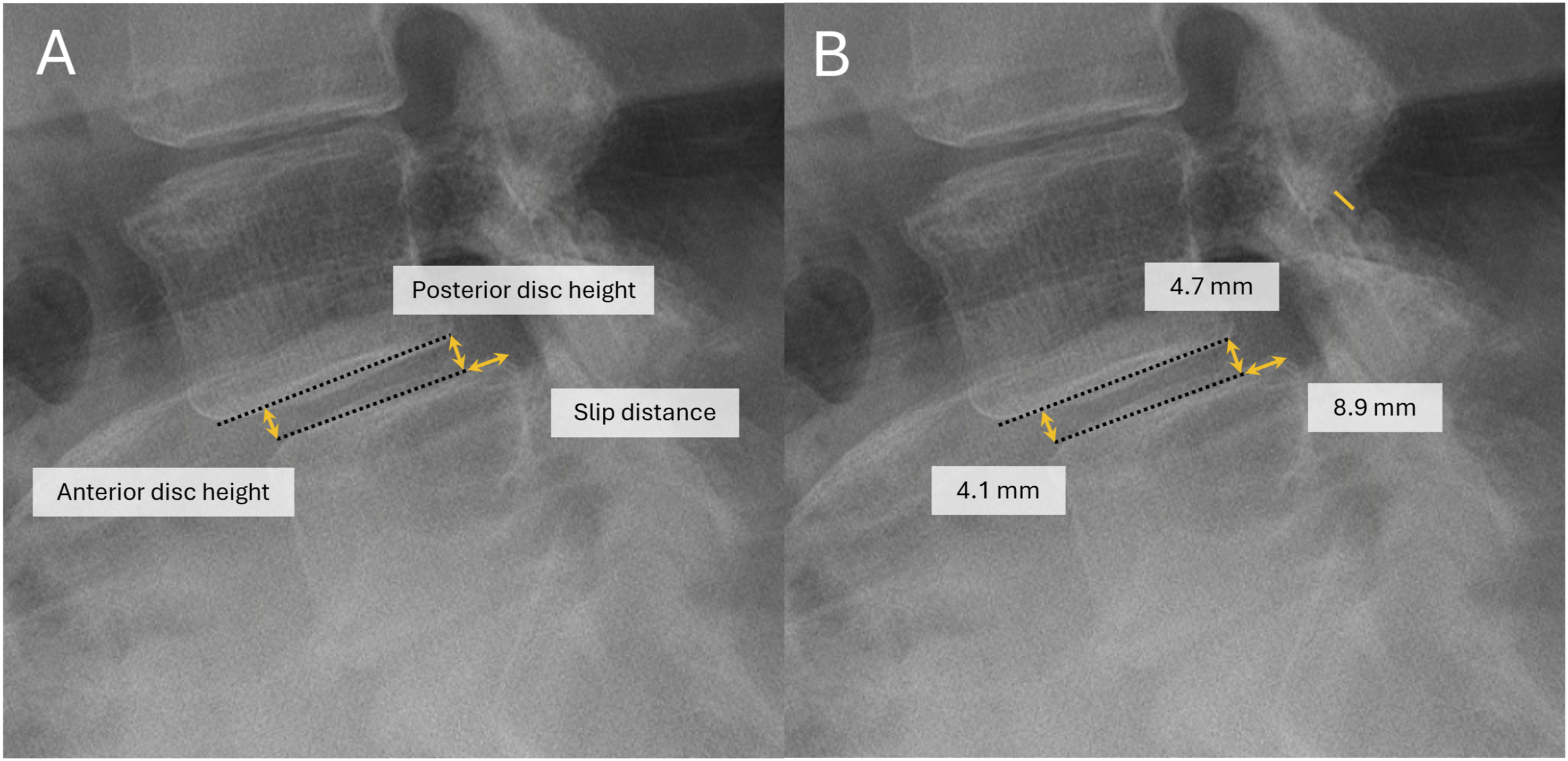
Cage subsidence was additionally measured for patients with 2-year post-operative radiographs available (n = 29). Subsidence was defined as >25% decrease of the average of the anterior and posterior disc heights of this long-term radiograph compared to the average disc height measurement immediately post-operatively (Figure 3).19,20 Due to the small sample size, statistical analysis was not performed to prevent misleading results. Lateral radiographs (A) immediately postoperative and (B) 2 years postoperative demonstrating cage subsidence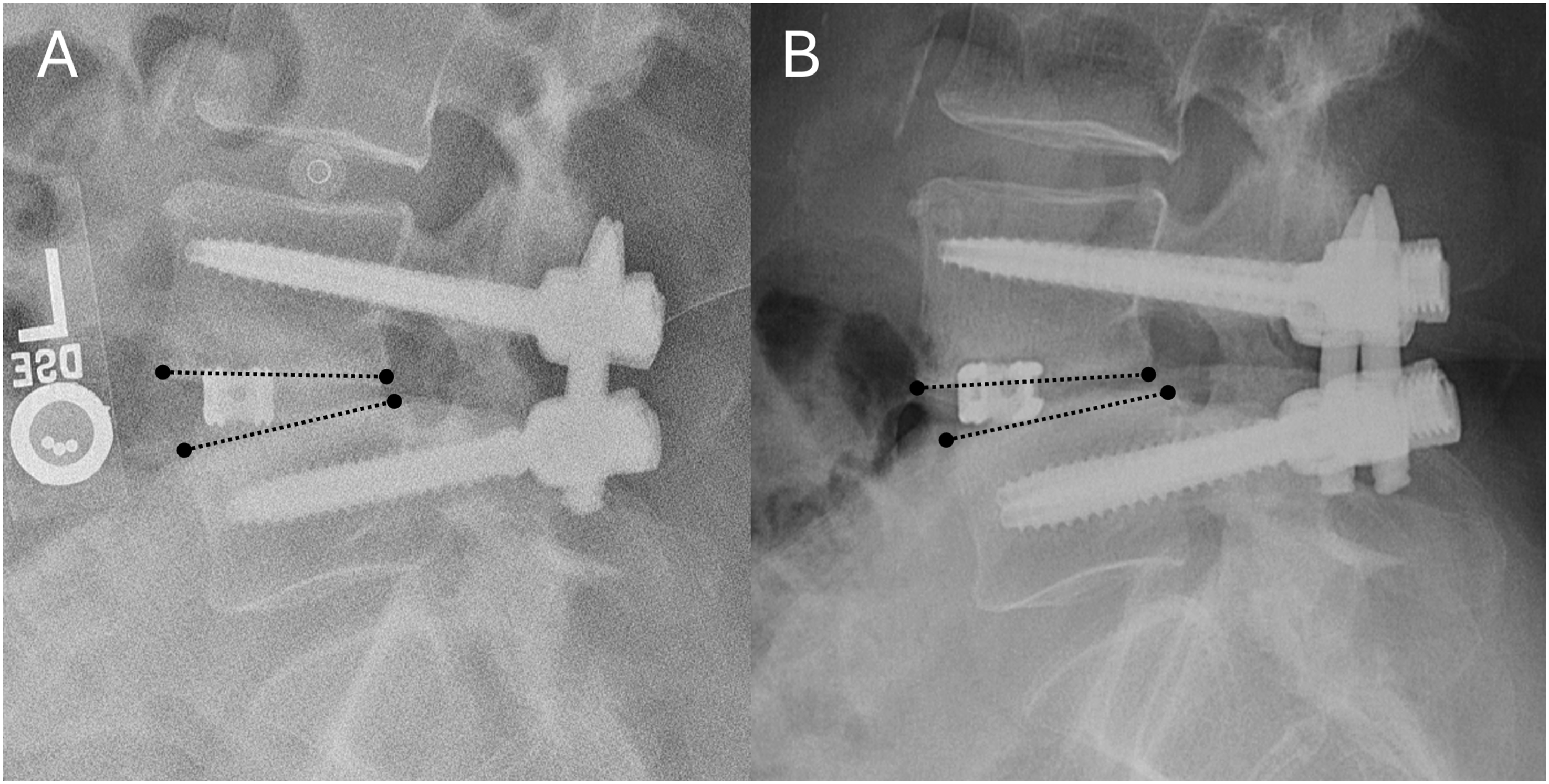
Statistical Analysis
Descriptive statistics for demographic characteristics, surgical factors, radiographic parameters, and sagittal alignment factors were reported either as mean ± standard deviation for continuous variables or as a frequency (percentage) for categorical variables.
For normally distributed variables, paired or unpaired t-tests were used. For non-normally distributed variables, Wilcoxon signed-rank test or Mann-Whitney U test was applied. A paired samples t-test was used to compare pre- and postoperative radiographic parameters, including spinopelvic alignment, DH, and vertebral slip. An independent samples t-test was used to compare screw and implant details for Nav vs Robo groups. Multivariable linear regression analysis was conducted to examine the effects of navigation modality (Nav vs Robo) on radiographic outcomes and slip reduction by adjusting spinal alignment and implant parameters. All statistical analyses were conducted on a complete case basis, performed using SPSS (version 29.0, IBM Corp., Armonk, NY, USA). Statistical significance was set at P < 0.05.
Results
Patient Demographic
Patient Demographics and Operative Characteristics
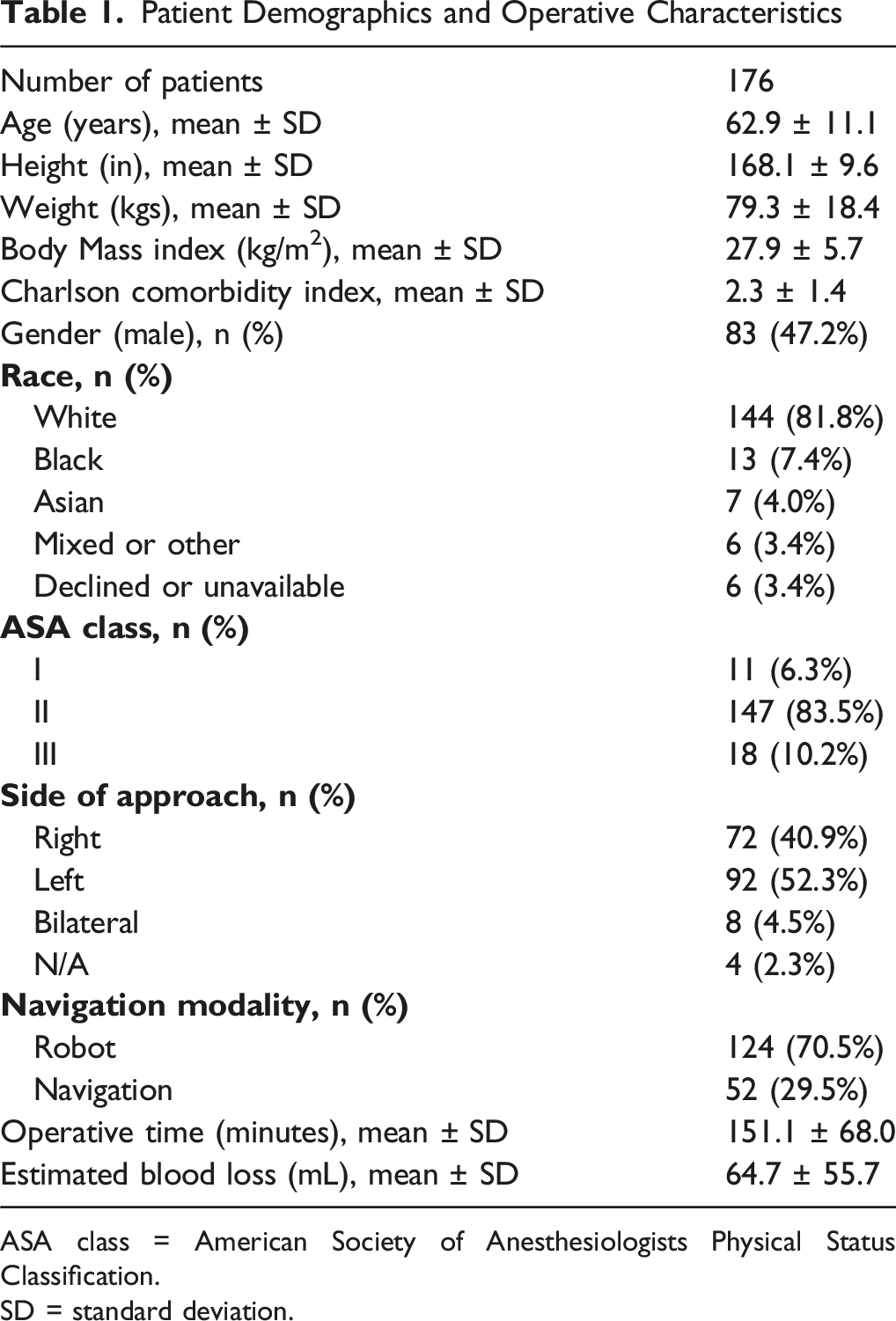
ASA class = American Society of Anesthesiologists Physical Status Classification.
SD = standard deviation.
Implant Details
Implant Details
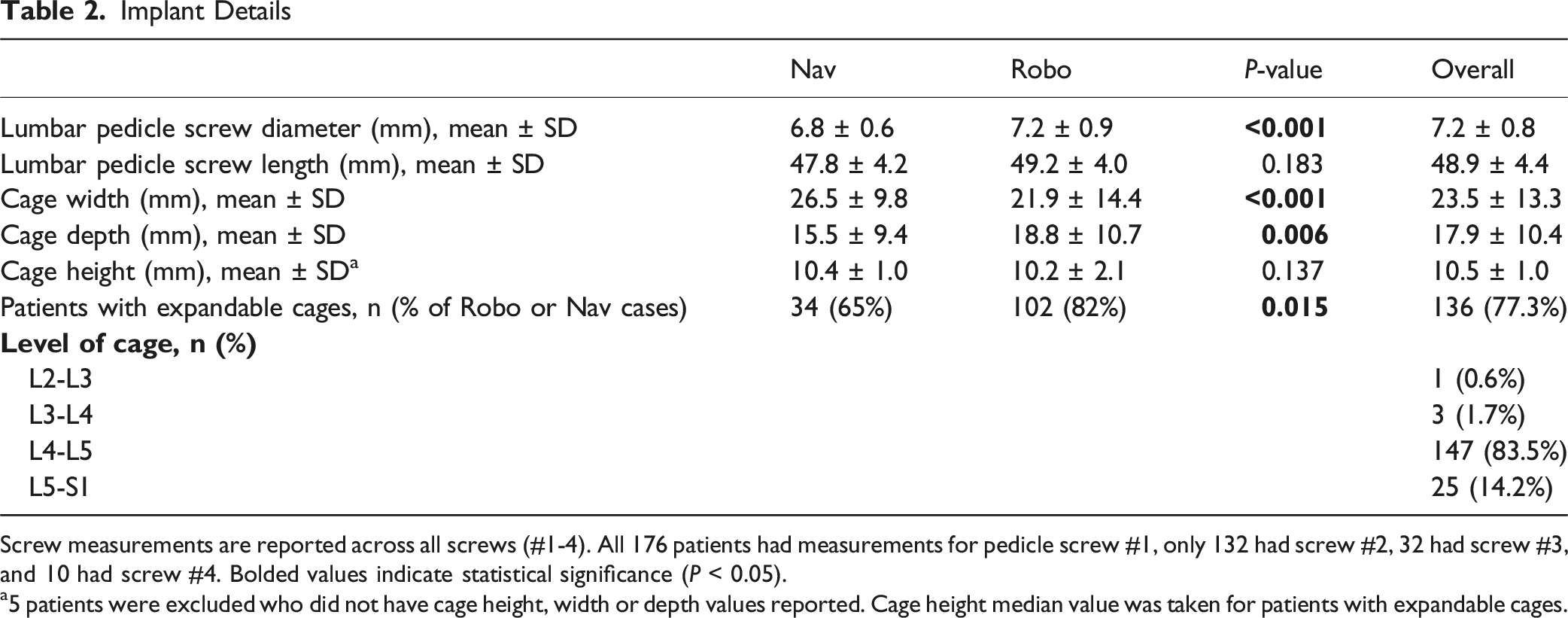
Screw measurements are reported across all screws (#1-4). All 176 patients had measurements for pedicle screw #1, only 132 had screw #2, 32 had screw #3, and 10 had screw #4. Bolded values indicate statistical significance (P < 0.05).
a5 patients were excluded who did not have cage height, width or depth values reported. Cage height median value was taken for patients with expandable cages.
Expandable cages were reported in 136 patients (77.3%), with 34 being Nav patients (65%) and 102 Robo patients (82%; P = 0.015). Five patients did not have recorded cage parameters and were excluded from these measurements. The most common level for MI-TLIF was L4/L5 (147 patients, 83.5%), followed by L5/S1 (25 patients, 14.2%; Table 2).
Radiographic Outcomes Comparison Between Pre- and Post-Operative Parameters
Disc Height Changes and Sagittal Spinal Alignment Changes Following Minimally Invasive Transforaminal Lumbar Interbody Fusion
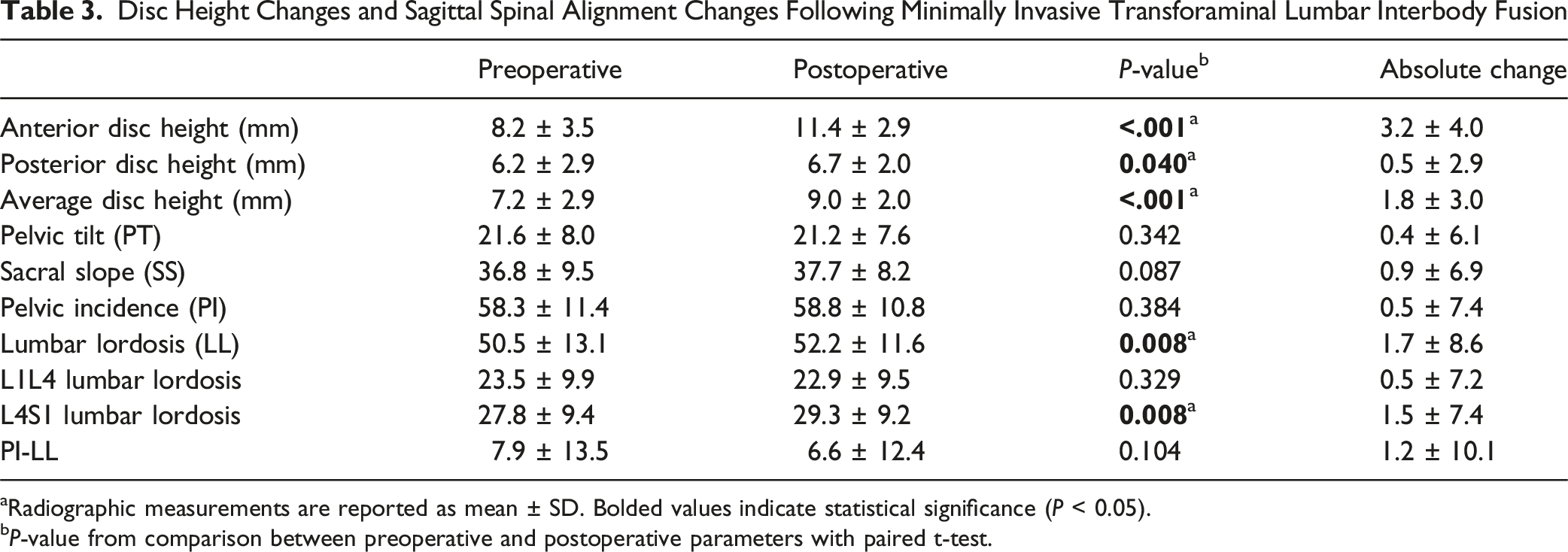
aRadiographic measurements are reported as mean ± SD. Bolded values indicate statistical significance (P < 0.05).
bP-value from comparison between preoperative and postoperative parameters with paired t-test.
Multivariable Regression Analyses
Multivariable Regression Model for Disc Height Improvement
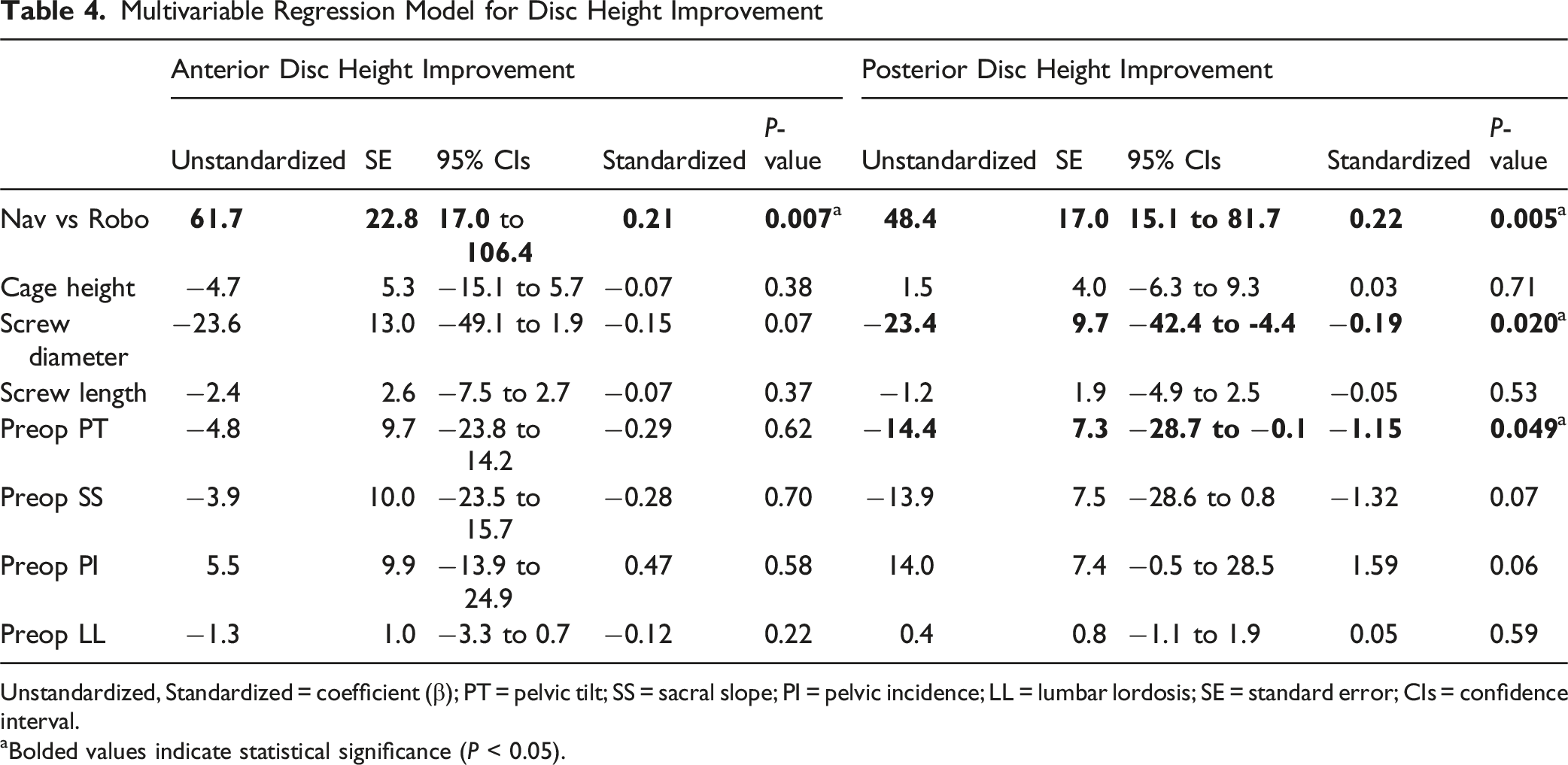
Unstandardized, Standardized = coefficient (β); PT = pelvic tilt; SS = sacral slope; PI = pelvic incidence; LL = lumbar lordosis; SE = standard error; CIs = confidence interval.
aBolded values indicate statistical significance (P < 0.05).
Multivariable Regression Model for Postoperative Lumbar Lordosis
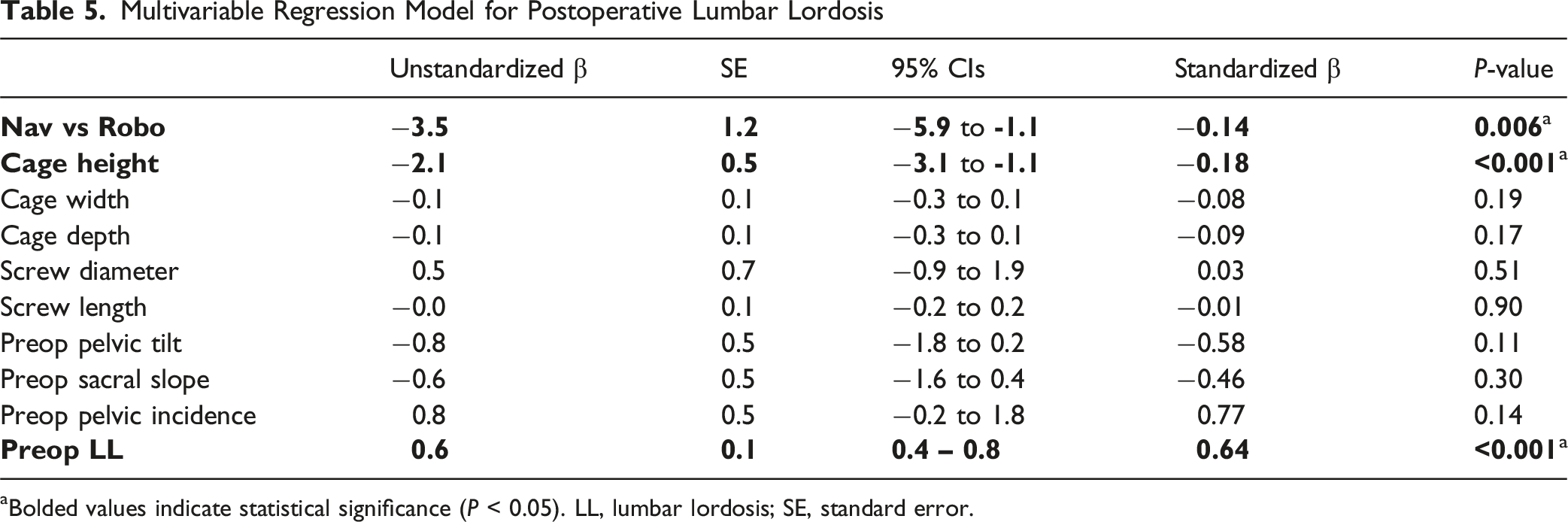
aBolded values indicate statistical significance (P < 0.05). LL, lumbar lordosis; SE, standard error.
Multivariable Regression Model for Slip Reduction Rate
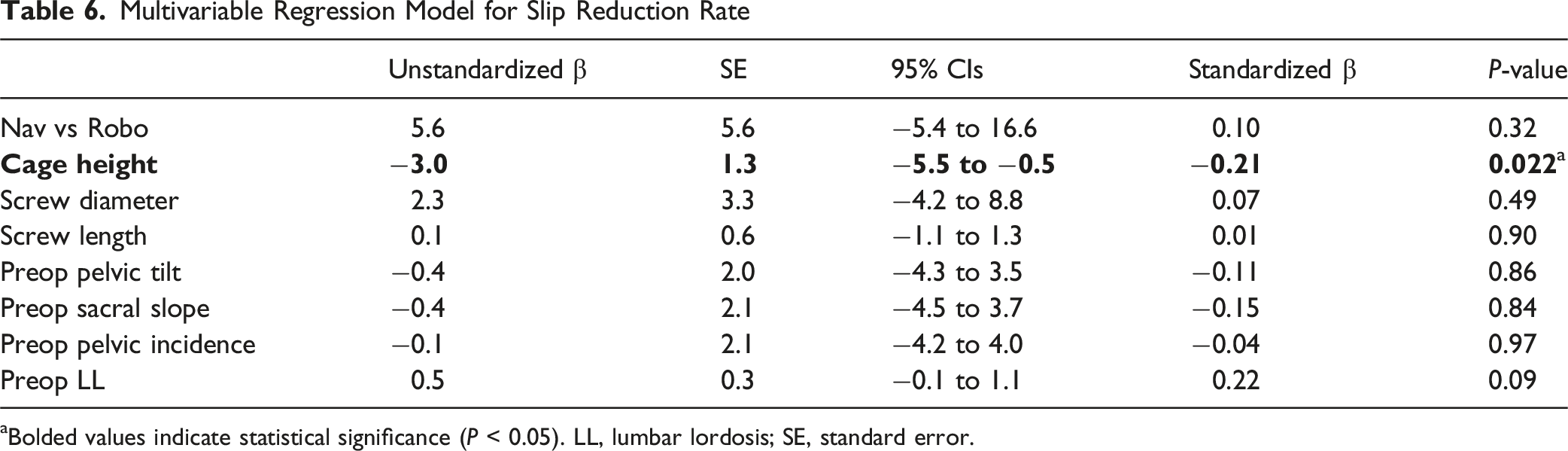
Bolded values indicate statistical significance (P < 0.05). LL, lumbar lordosis; SE, standard error.
Cage Subsidence
Cage subsidence assessment was conducted on patients who had follow-up radiographs of 24 months or greater (n = 29). Of these 29 patients, 16 used intraoperative navigation and 13 used robotic modalities. Four patients experienced subsidence (18.2%), with two (12.5%) from the Nav group and two from the Robo group (15.4%).
Discussion
This study evaluated the influence of robotic arm on postoperative radiographic outcomes, including DH, spinal alignment, slip reduction, and cage subsidence, in patients undergoing 1-level MI-TLIF. Robo group was more likely to use expandable and deeper cages and used screws with larger diameters, while the navigation group used slightly longer screws and wider cages on average, although screw length differences were not statistically significant. In terms of radiographic outcomes, Robo group achieved superior disc height restoration compared to the Nav group. In contrast, greater LL restoration was achieved through imaging-only navigation modalities. Preoperative PT and LL were also significantly associated with posterior DH improvement and LL restoration, respectively. Slip reduction and subsidence were similar between Robo and Nav groups. Overall, preoperative alignment factors and implant characteristics seem to have a larger effect size than navigation modality. These results highlight the potential benefits of robotic navigation in enhancing disc height restoration and imaging-only navigation in LL restoration while underscoring the nuanced role of implant-related factors in surgical outcomes.
Numerous studies regarding spondylolisthesis have examined the influence of fusion techniques on disc height improvement.12,21 However, no studies to date have directly compared different navigation modalities. Traditionally, robotic navigation systems are designed to improve the accuracy of implant placement.22,23 Robotic navigation has been shown to facilitate the placement of larger screws, which may enhance construct strength. 24 Among patients with similar spinal rigidity and cage sizes, achievable radiographic reduction goals may vary depending on construct strength.25-27 Furthermore, surgeons may hesitate to perform radical reductions in cases with insufficient screw parameters due to the risk of posterior instrumentation failure. While the reduced mental workload associated with robotic navigation could theoretically allow surgeons to focus more on achieving optimal radiographic outcomes,28,29 it is also possible that the observed differences reflect the preferences and surgical philosophies of those who preferentially use robotic systems rather than the technology itself. Therefore, the apparent radiographic advantages of robotic-assisted surgery should be interpreted with caution, acknowledging the potential influence of surgeon selection and practice patterns.
Restoring LL plays a crucial role in the long-term stability of the construct, potentially reducing the risk of subsequent complications such as adjacent segment disease. 30 The effectiveness of TLIF in LL restoration has been extensively studied, and Aoki et al. demonstrated that LL restoration is closely associated with preoperative LL values and can lead to improved mid-term clinical outcomes. 31 Consistent with these findings, another study reported that both MI and open TLIF approaches achieve comparable improvements in LL. 32 In our multivariable regression model, lower cage height, greater preoperative LL, and the use of navigation rather than robotic guidance were independently associated with postoperative LL. After adjusting for cage height and other implant-related variables, the residual association between navigation and greater postoperative LL likely reflects differences in preoperative sagittal alignment patterns and intraoperative positioning rather than screw size or cage width alone. Recent evidence suggests that, although overall LL correction may be similar between approaches, an open approach may provide an advantage in selected patients with high PI, indicating that postoperative regional alignment is influenced by the interaction between patient-specific spinopelvic anatomy and surgical technique rather than by the approach alone. 33 Moreover, because a single-level TLIF has an inherently limited capacity to substantially increase global LL due to compensatory mechanisms in other lumbar spine levels, 34 surgeons should consider both preoperative sagittal profiles and construct selection when planning realistic segmental alignment correction. 31 Future research should clarify which specific aspects of surgical modality, including navigation platforms, robotic systems, and exposure techniques, meaningfully influence alignment-related outcomes beyond patient-specific anatomical factors.
Cage size plays a critical role in restoring spinal morphology appropriately. 35 Most of the cages used in this patient series were expandable cages with a 15-degree lordotic angle. This system effectively improved disc height in minimally invasive approaches, optimizing fit while maintaining alignment. However, the surface design of these cages tends to grip the endplate, limiting segment mobility during rod and screw stabilization. 36 This may explain why higher cages could lock the segment in place, reducing its ability to slide or move and preventing an effective reduction maneuver. Additionally, greater cage height in non-expandable cage can also fix the segment, diminishing the reduction effect of the posterior construct, as reflected by the regression analysis. Finally, there was a statistically significant difference in use of expandable cages among patients in the Robo and Nav groups; the Robo group had a greater use of expandable cages, which may account for the greater disc height achieved with robotic modalities.
The necessity of slip reduction in spondylolisthesis remains debated. A systematic review suggested comparable intraoperative blood loss, operative time, and clinical outcomes between reduction and in-situ fusion in patients with low-grade spondylolisthesis. 37 On the other hand, a randomized controlled trial showed better radiological outcomes including fusion rates in the intentional reduction cohort although clinical outcome scores were aligned with other studies.38,39 In our cohort, the degree of slip correction did not differ between robotic and navigation modalities, suggesting that the extent of reduction may depend more on the surgeon’s intraoperative decision-making than on the surgical technology itself. Considering the inherent precision and stability that both systems provide for screw trajectory, the absence of a difference in postoperative slip reduction is reasonable. However, this study did not capture the surgeon’s intended amount of reduction or intraoperative strategy. Future research should prospectively evaluate how each modality influences the surgeon’s comfort, confidence, and ability to achieve the desired reduction under real operative conditions, including the relationship between planned and achieved slip correction.
Finally, greater interbody height restoration may increase the risk of subsidence due to the additional forces experienced by the endplates, so it was necessary to analyze long-term radiographic outcomes to determine if this was a durable finding. 40 Marchi et al. demonstrated that larger cage-endplate interfaces offer superior construct stability and decreases the chance of subsidence. 19 Depending on patient anatomy, surgeons may use different technologies to optimize this interface; for example, intraoperative navigation can facilitate the use of wider interbody cages, whereas robotic guidance may help position cages more anteriorly along the anteroposterior axis. In the subgroup of patients with at least 24 months of follow-up radiographs, no clear difference in the rate of cage subsidence was observed between MI-TLIFs performed with robotic vs navigation modalities. However, this analysis was limited by a small sample size (n = 29) and the low number of subsidence events (n = 4), and was likely underpowered to detect modest between-group differences. Therefore, the absence of an observed difference should not be interpreted as evidence of equivalence between modalities. The overall subsidence rate in this cohort was 18.2%, which is comparable to previous reports showing rates between approximately 10% and 35% after MI-TLIF, including studies using expandable cages.20,41-43 Therefore, our findings suggest that the subsidence rate observed in our series falls within the expected range and does not indicate an increased risk attributable to either navigation or robotic guidance.
There are several limitations to this study. First, this is a retrospective analysis conducted at a single academic institution, which may introduce selection bias and limit the generalizability of our findings. Surgeons’ preferences for navigation modality and instrument selection may also have influenced which patients underwent each technique and thus represent an important source of residual confounding. Second, neither intraoperative navigation nor the robotic arm was directly employed to guide sagittal alignment correction, so the observed radiographic differences are indirect and may be confounded by unmeasured factors such as mental workload, construct strategy, and case complexity. We attempted to account for these factors using multivariable regression analysis, but unmeasured confounding cannot be excluded. Third, the actual cage height post-expansion was unclear. While a consistent strategy aimed to match the adjacent or healthy disc height, adjustments were made intraoperatively based on bone quality and endplate conditions, potentially introducing bias. Fourth, the relatively small overall sample size, particularly in the subsidence subgroup, represents a major limitation and reduces the statistical power to detect modest differences between modalities. Fifth, due to the limited number of patients, we did not perform propensity score matching, as matching would have further reduced the analyzable cohort and potentially produced unstable estimates. Instead, we used multivariable regression analysis to adjust for baseline imbalances between groups. Therefore, causal inferences should be interpreted with caution. Finally, this study did not include clinical outcome measures, limiting the ability to determine whether the observed radiographic improvements translate into patient benefits. Therefore, the clinical utility of the robotic arm should be interpreted in the context of other factors such as cost-effectiveness, learning curve, and accessibility. Nevertheless, our findings contribute to the growing discussion on the role of robotic arms not only in enhancing screw placement accuracy but also in improving surgical efficiency to achieve experienced surgeons’ goals.
Conclusions
In conclusion, among patients undergoing MI-TLIF, the use of a robotic arm was associated with greater disc height restoration compared with intraoperative navigation, whereas LL restoration appeared to be influenced primarily by patients’ preoperative sagittal alignment rather than with the choice of navigation modality itself. Surgeons should select the operative modality based on patient anatomy, baseline alignment, and specific surgical goals, rather than expecting any single technology to overcome unfavorable preoperative conditions. Future studies should integrate clinical outcomes with radiographic parameters to more comprehensively evaluate the impact of robotic and navigation guidance in minimally invasive spine surgery.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: no direct funding was received for this study. However, this study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center for Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Globus Medical and Stryker (Paid presenter or speaker); Vertebral Columns/International Society for the Advancement of Spine Surgery (ISASS) (Editorial or Governing Board).
Previous Presentations
No portion of this paper has been previously presented.