
Abstract
Study Design
Retrospective cohort study.
Objectives
As cancer survival improves, metastatic spinal cancer has become increasingly common worldwide. Given the high resource demands of spinal oncology care, tools to optimize perioperative planning are essential. The objective of the study was to assess the effectiveness of the Risk Assessment and Prediction Tool (RAPT) in predicting post-operative needs in patients undergoing surgery for spinal tumors.
Methods
Consecutive patients (n = 384) undergoing spinal oncology surgery were enrolled and prospectively assessed with RAPT. Coarsened exact matching (CEM) was used to retrospectively isolate risk factors associated with outcomes. Enrolled patients with a low RAPT score (≤9, n = 44) were exact matched against high-scoring patients (10-12, n = 44). The primary outcome of interest was post-acute care disposition; secondary outcomes were 30- and 90- day ED visits, readmissions, and reoperations. McNemar’s test was utilized for matched comparisons.
Results
A low RAPT score was significantly associated with non-home discharge (OR = 4.33 [1.23, 15.20], P = 0.02) and 30-day readmission (OR = 3.66 [1.02, 13.14], 0.03). Among low-scoring patients, 31.8% required post-acute care (while only 11.3% of high-scoring patients required post-acute care). A low RAPT score was not associated with ER visits, reoperation, or mortality. Isolation of the RAPT walk score alone significantly predicted non-home discharge (OR = 2.8 [1.01, 7.78], P = 0.04).
Conclusions
When applied prospectively before spinal cancer surgery, the RAPT tool and its subcomponents effectively predict post-acute care needs. Pre-operative prediction of non-home discharge may help guide in-hospital resource allocation and post-acute care of spinal oncology patients.
Introduction
Spinal tumors are becoming increasingly common. 1 Nearly 30% of cancer patients develop spine metastases and require surgical intervention to mitigate symptoms and morbidity. 2 While surgery can alleviate spinal cord compression, recovery can be associated with overutilization of post-acute resources.3,4 A meta-analysis of 13 spine surgery studies found that 30-day readmission rates ranged from 4.2% and 7.4%, with common reasons for readmission including wound infections and medical complications. 4 Additionally, these patients often utilize high amounts of healthcare resources during the course of their multi-modal treatment.1,2 To address these challenges, the Penn SOaR 2 program (Surgical Spinal Oncology, Medical Oncology, and Radiation Oncology/Radiology) was established to coordinate care for spinal oncology patients. However, predicting which patients can be safely discharged to home, as opposed to a higher level of care, after surgery remains difficult. Therefore, clinical prediction tools are needed to appropriately manage perioperative risk factors and patient discharge planning.
The Risk Assessment and Predictor Tool (RAPT) was initially developed in 2003 to assess the need for post-operative care within orthopedic surgery patients.3-7 It is based on six factors: age, gender, walk score, gait assist score, community support score, and home support score. Higher RAPT scores indicate likely home discharge while lower score indicate probable need for further inpatient rehabilitation. Previous studies have illustrated RAPT’s ability to predict post-operative outcomes for patients in several neurosurgical procedures, such as cervical spine surgery and lumbar fusion.8-10 However, there is a lack of well-controlled studies into the tool’s effectiveness for spinal oncology patients.
The primary objective of this study is to evaluate the effectiveness of RAPT in predicting post-acute care disposition for patients undergoing spinal tumor surgery. The secondary objective is to determine the effectiveness of RAPT in predicting ER visits, readmissions, and 30- and 90-day reoperation rates. This work has the potential to provide valuable insights into the impact of RAPT on post-operative care for spinal tumor patients and could be used to further enhance the quality of spine surgical care by informing resource allocation in a targeted manner.
Methods
Patient Selection
Data was retrospectively collected from 1841 consecutive spine tumor surgeries from 2013-2024 at a multi-hospital academic medical center. Given the retrospective design of the study, patient consent was waived. All included cases were inpatient admissions, utilized general anesthesia, had a documented RAPT score from a pre-operative visit, and surgical pathology confirming neoplasm. Primary and metastatic spine tumors were both included, as well as cases with and without instrumentation. A total of 384 cases were further analyzed (Figure 1). Patient Selection. Flowchart indicating the patients selected for matching for RAPT score and sub-score analysis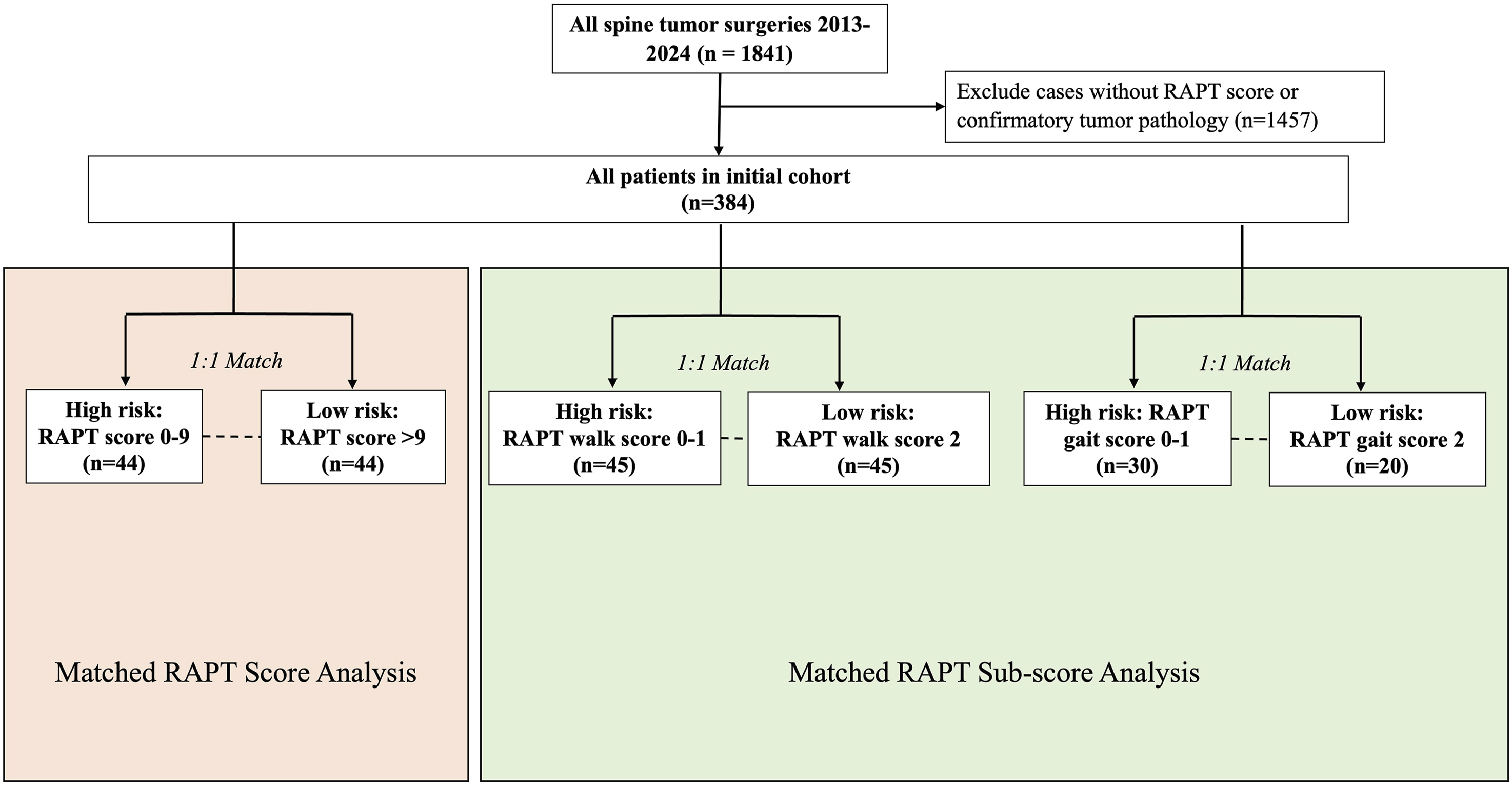
Data Extraction
RAPT scores were prospectively recorded at the pre-operative visit using a standard questionnaire that assesses the patient’s age, gender, baseline ambulation, assistive devices, and presence of support systems. EpiLog, 11 a non-proprietary software designed for electronic medical record data collection and quality improvement initiatives, was used to collected other patient medical and demographic data, such as sex, American Society of Anesthesiologists (ASA) grade, smoking status, insurance type, surgical history, body mass index (BMI), median household income (MHI), race, and all 16 comorbid conditions assessed in the Charlson Comorbidity Index (CCI).
The primary post-operative outcome was discharge disposition (home vs non-home). Secondary outcomes included 30- and 90-day post-operative Emergency Department (ED) visits, readmissions, and reoperations following the operation. At post-operative follow-up visits, patients were routinely asked about encounters at outside health systems to allow for documentation and inclusion of these events in the analysis.
This study was approved by the Institutional Review Board at the participating institution (IRB #825431).
Statistical Analysis and Matching
Patients were clustered into predicted risk cohorts based on RAPT score, as in prior orthopedic research 7 : low-risk (score >9) vs high-risk (score = 0-9). Subsequently, coarsened exact matching (CEM) was performed to generate exact-matched groups among risk cohorts. Low and high-risk patients were matched one-to-one along the following covariates: gender (male vs female), 12 ASA grade (exact), 13 smoking history (prior/never), 14 insurance type (public/private), 15 prior surgery (binary), 16 CCI score (<4, 5-6, >7), 17 BMI (<18.5, 18.5-30, or >30), 18 race (white/non-white), 19 and median household income (below/above median). 20 These criteria were intentionally selected for the matching protocol due to the known effect of these covariates on surgical morbidity and post-operative outcomes.14,17-19 We did not match on age due to its inclusion in the RAPT score. Exact matching resulted in a study cohort of 44 matched pairs of patients based on these factors. Sub-analysis of matched cohorts based on the individual RAPT components was similarly done. For the individual RAPT walk scores, patients were grouped by score 0-1 (cannot walk more than 2 blocks) vs 2 (can walk 2+ blocks) and for the RAPT gait scores, patients were grouped by score 0-1 (requires some assistive device to walk) vs 2 (does not require assistance). Matching was conducted with the same covariates as detailed above and 45 exact matches for the walk score analysis were uncovered. Thirty (30) matches for the gait score analysis were uncovered.
Differences in patient demographics and characteristics were assessed using chi-squared and non-parametric tests. Outcomes in the coarsened exact matched analysis were assessed using McNemar’s test and non-parametric testing for categorical and continuous variables, respectively.
Results
Demographics
Patient Characteristics for Pre- and Post-matching Cohorts
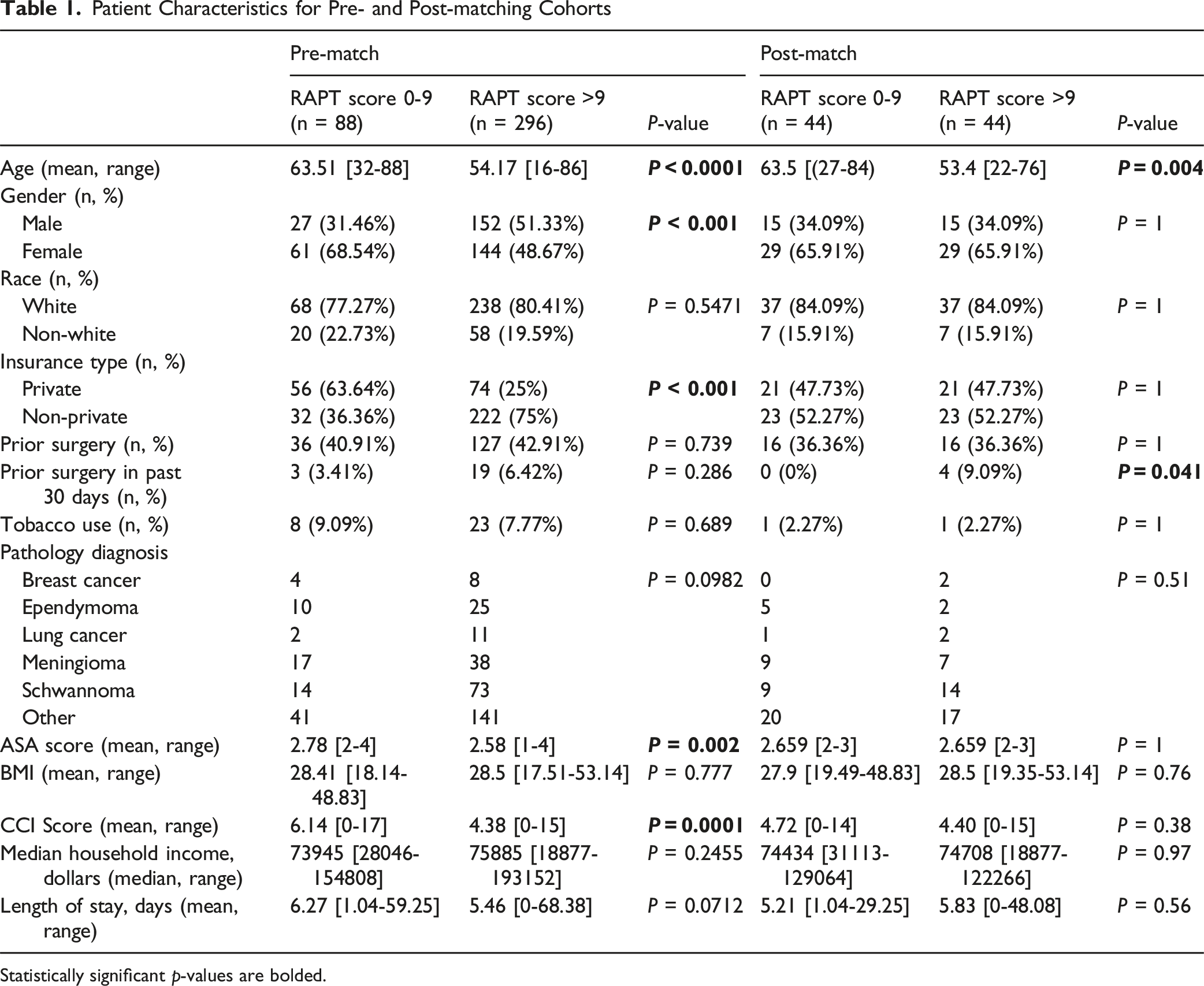
Statistically significant p-values are bolded.
Outcomes After Matching
Surgical Outcomes Based on Matched Patients With RAPT Score 0-9 vs RAPT Score >9
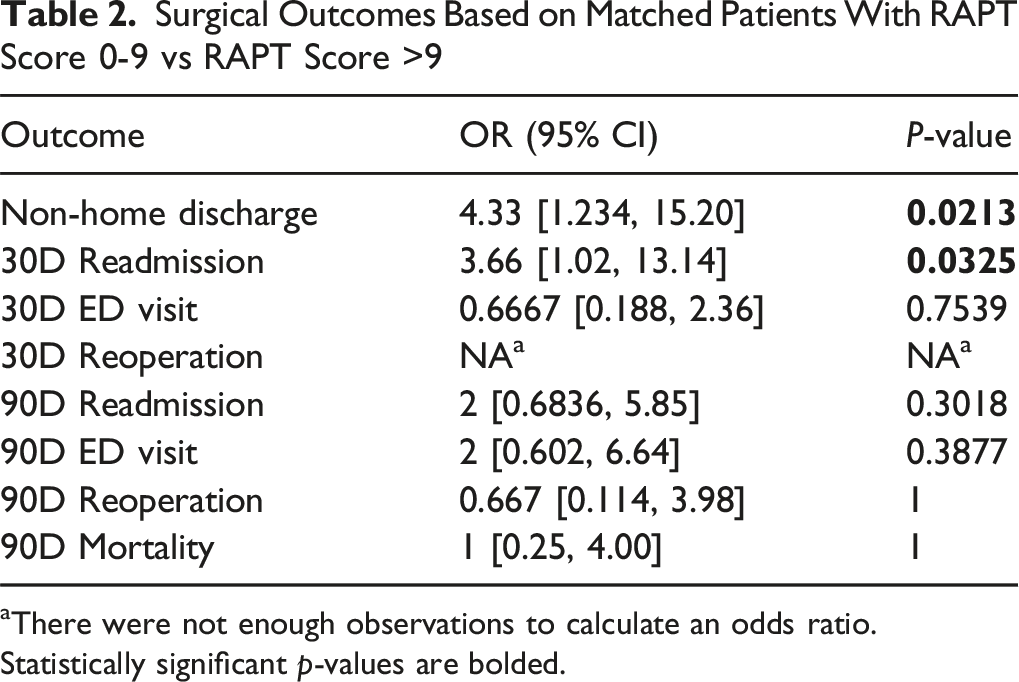
aThere were not enough observations to calculate an odds ratio.
Statistically significant p-values are bolded.
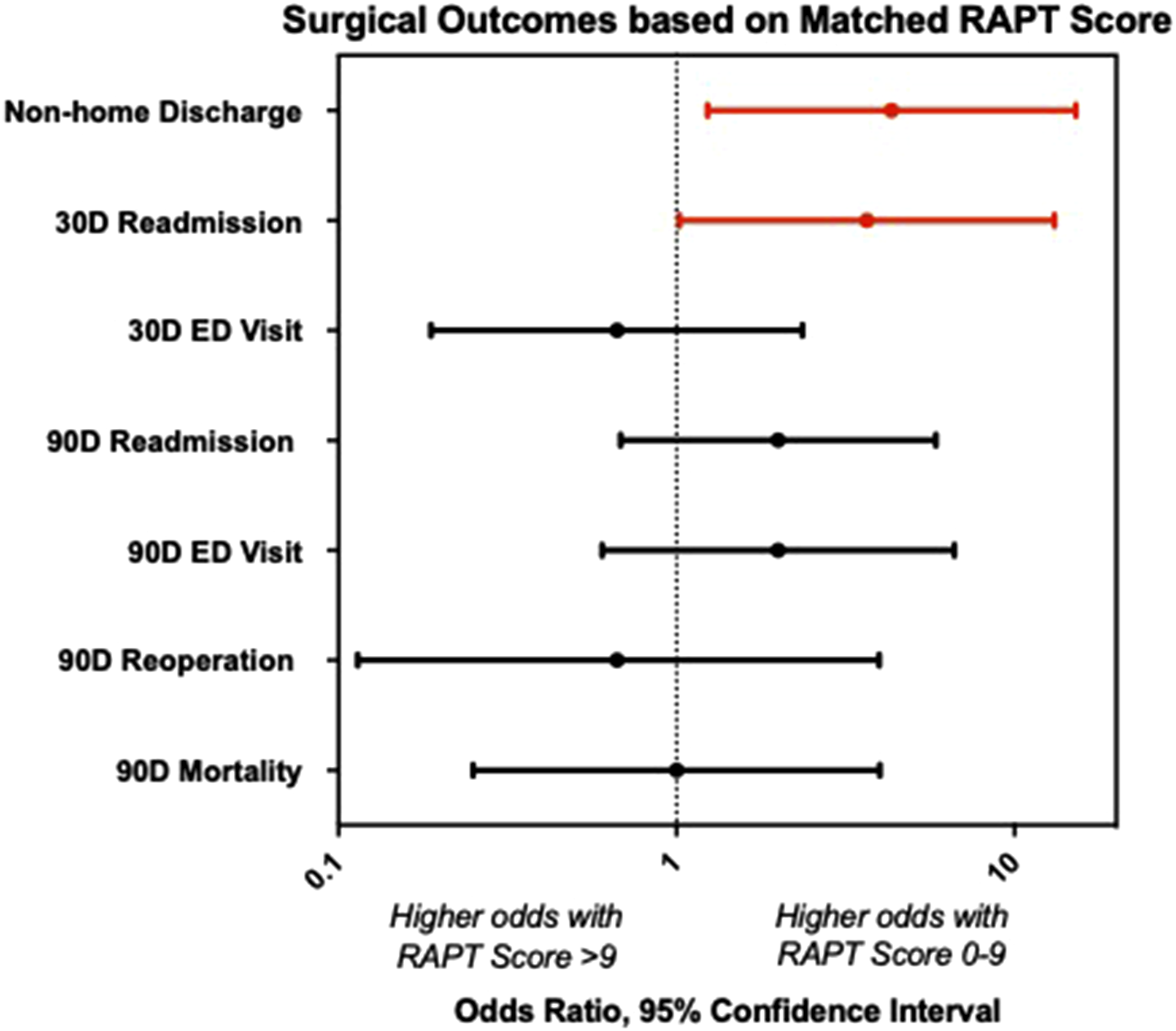
Surgical Outcomes associated with RAPT Score in Matched Patients. Forest plot demonstrating odds ratios of surgical outcomes comparing matched patients with RAPT score 0-9 (high risk group) vs RAPT score >9 (low risk group). Odds ratio >1 indicates that the outcome is more likely in the score 0-9 group, while odds ratio <1 indicates that the outcome is more likely in the score >9 group. Error bars denote 95% confidence intervals and dotted line marks odds ratio of 1. Significant results with P < 0.05 are depicted in red
Matched RAPT Sub-Score Analysis
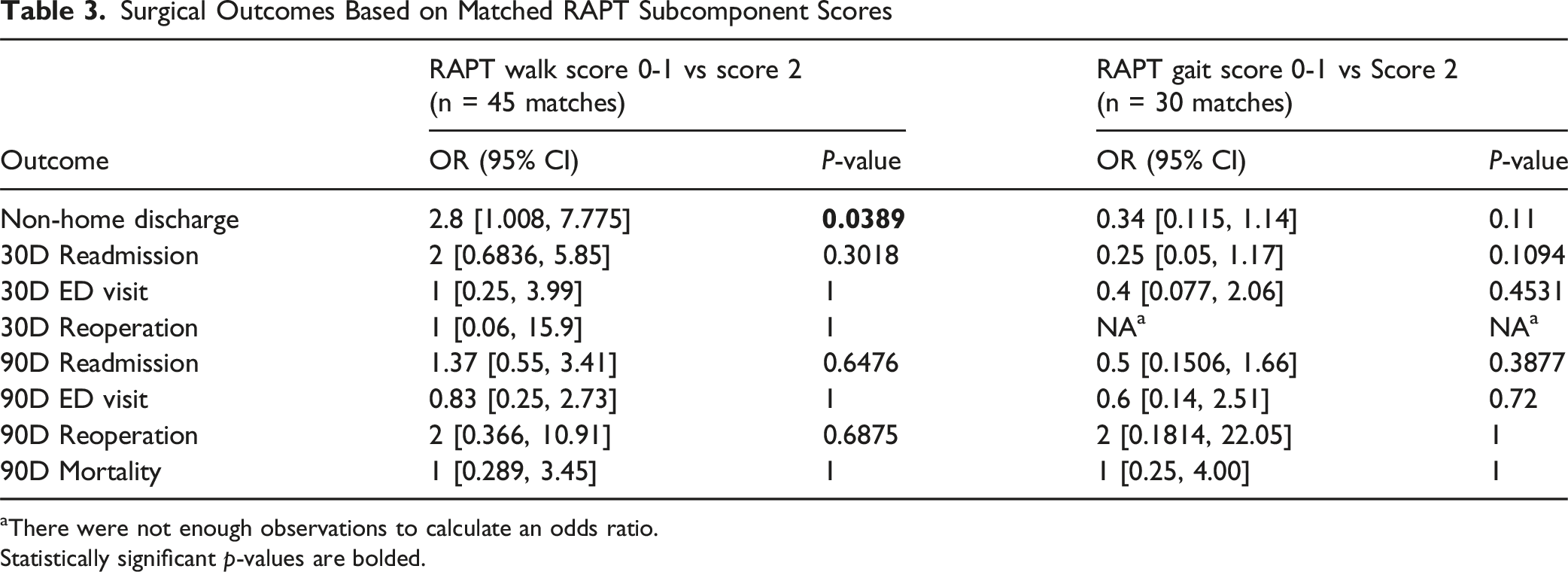
Analysis of the individual RAPT walk scores among matched patients showed that a walk score of 0-1 increased the chance of a non-home discharge (OR = 2.8 [1.008, 7.775], P = 0.0389), compared to otherwise similar patients who had a walk score of 2 (Table 3, Figure 3). There were no differences in 30- or 90- day readmissions (OR = 2 [0.6836, 5.85], P = 0.3018; OR = 1.37 [0.55, 3.41], P = 0.6476), ED visits (OR = 1 [0.25, 3.99], P = 1; OR = 0.83 [0.25, 2.73], P = 1), or reoperations (OR = 1 [0.06, 15.9], P = 1; OR = 2 [0.366, 10.91], P = 0.6875). Mortality after 90 days was also similar between both groups (OR = 1 [0.289, 3.45], P = 1). Analysis of RAPT gait scores revealed no differences in non-home discharge (OR = 0.34 [0.115, 1.14], P = 0.11), 30-day readmission (OR = 0.25 [0.05, 1.17], P = 0.1094), or 30-day ED visits (OR = 0.4 [0.077, 2.06], P = 0.4541) when comparing matched patients with gait score 0-1 vs score 2. Furthermore, 90-day outcomes, including readmission (OR = 0.5 [0.1506, 1.66], P = 0.3877), ED visits (OR = 0.6 [0.14, 2.51], P = 0.72), reoperations (OR = 2 [0.1814, 22.05], P = 1) and mortality (OR = 1 [0.25, 4.00], P = 1), were also not significantly different based on gait score. Matched sub-analysis of Individual RAPT Components. Odds of experiencing surgical outcomes in matched patients with (A) RAPT walk score 0-1 (unable to walk more than 2+ blocks) vs 2 (able to walk more than 2+ blocks) and (B) RAPT gait score 0-1 (requires some assistive device to walk) vs score 2 (does not require any device to walk). Odds ratio greater than 1 indicates higher chance of outcome with walk or gait score 0-1. Odds ratios with 95% confidence intervals are shown with significant results highlighted in red Surgical Outcomes Based on Matched RAPT Subcomponent Scores aThere were not enough observations to calculate an odds ratio. Statistically significant p-values are bolded.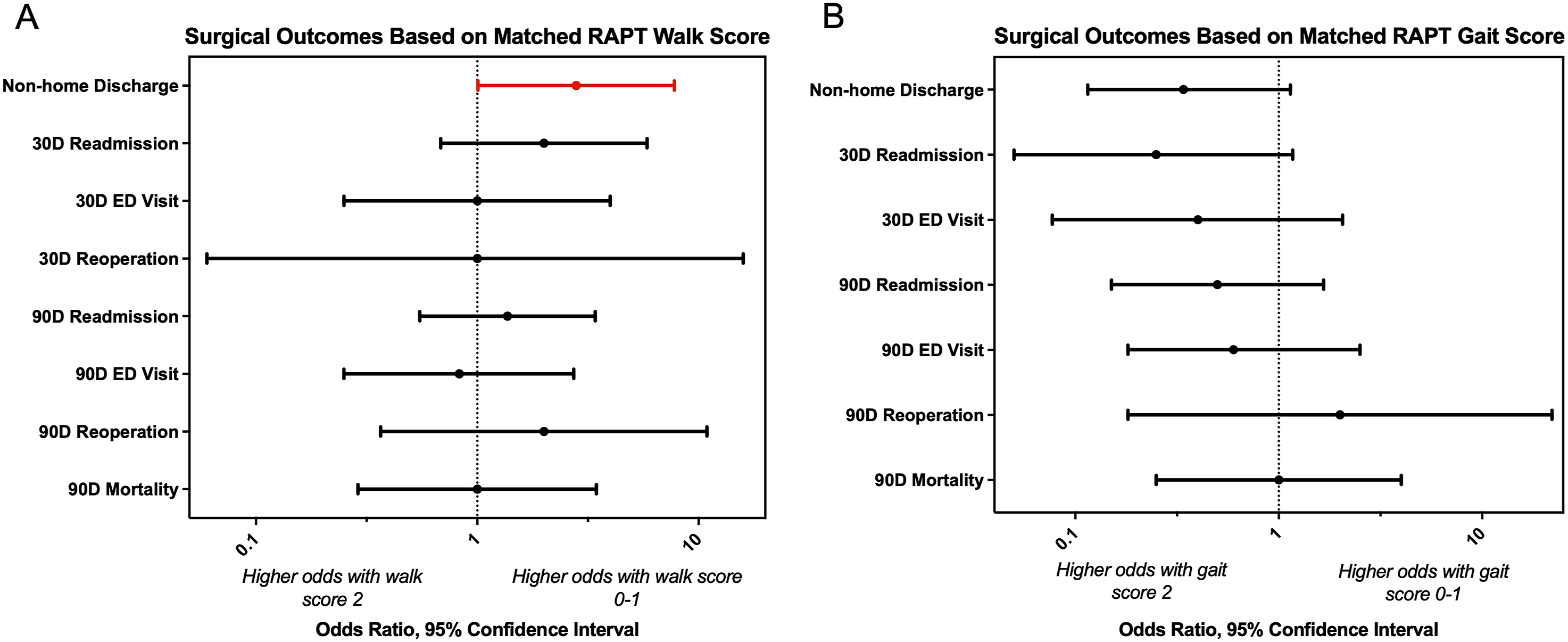
Discussion
The RAPT assessment has been a well-validated prediction tool for post-operative discharge disposition in orthopedic surgery.6-9,12,13 More recently, studies have demonstrated its application to neurosurgical procedures, 8 including lumbar fusion, 10 but whether RAPT can be applied to more complex procedures in medically complicated patients remains unknown. In this study, we assessed the ability of RAPT to predict post-operative outcomes after spinal tumor surgery. We employ a coarsened exact matching protocol to rigorously control for ten variables known to affect neurosurgical outcomes including race, BMI, and CCI score.14,17-19 Our study finds that RAPT is able to predict non-home discharge and 30-day readmission after surgery. Furthermore, the RAPT walk score alone was adequate in predicting discharge disposition.
Due to the high resource demands and the morbidity of spinal neoplasms, and their treatment, there is significant interest in developing tools to predict post-operative outcomes. A number of survival prediction tools have been developed, including Baeur, Tokuhashi, and Tomita.21-23 The Tokuhashi score takes into account general condition, number and location of metastases, site of the primary cancer and degree of spinal cord palsy. 21 It has since been revised and has demonstrated favorable accuracy in predicting patient prognosis. 24 Tomita et al later simplified Tokuhashi’s system and added weighting to each factor. 22 These two scales are often used in evaluating surgical candidacy. Other scales have focused on short-term post-operative outcomes.25-27 Pre-operative patient functional status has been consistently identified as significant predictor in non-home discharge.28,29 Ehresman et al found that non-routine discharge in patients undergoing surgery for vertebral column tumors was predicted by emergency admission, increased frailty, serum albumin level, and procedures with multiple stages. 29 Another study on intradural extramedullary spinal tumors associated older age and increased medical comorbidity burden with greater post-acute care needs. 28 Our results are largely consistent with these previous studies, as RAPT is essentially evaluating pre-operative functional status in a convenient format. Simplicity of the RAPT permits easy incorporation into the electronic medical record, as exemplified by our research group’s effort to integrate RAPT into our health system’s EMR using an automated program called EpiLog. 8 Additionally, unlike other scoring tools,25-27 RAPT does not require additional lab values, patient imaging, or comprehensive knowledge of the patient’s medical comorbidities. RAPT can be entered by any level of caregiver and even the patients themselves. Automated calculation algorithms support simple tabulation. Therefore, it can be quickly administered at a pre-operative visit with results routed to the pre-procedure note and to the social work team.
Discharge disposition is an important variable of clinical outcome and healthcare costs in the spinal oncology population, as up to 40% of patients experience a non-home discharge.30,31 Non-home discharge is associated with higher rates of post-operative mortality, wound complications, and reoperations.28,32 Pre-operative identification of high-risk patients offers the possibility to develop personalized post-operative protocols to streamline post-operative care, optimize resource allocation, and improve patient satisfaction. There is evidence that intentionally designed discharge planning pathways can reduce readmission and total post-operative healthcare resource usage after discharge,33,34 as discharge delays can account for more than 39% of the hospitalization stay cost. 35
Clinical implementation of the RAPT questionnaire can help facilitate spinal oncology care by reducing peri-operative morbidity and decreasing cost. Assessing RAPT score at a pre-operative visit can help surgeons to adequately assess surgical risk, while also providing patients with appropriate expectations for their discharge plan. Patients identified at high-risk of non-home discharge can be engaged early by case management and transfer requests can be placed promptly to reduce hospitalization time when patients are simply waiting for a bed at a different facility. Low-risk patients can engage in early mobilization after surgery to facilitate home discharge. Furthermore, our finding that the RAPT walk score alone was able to predict discharge disposition indicates that pre-operative ambulation is an important target for optimization. Walking ability is associated with many dimensions of health, including cardiovascular strength, respiratory capacity, and musculoskeletal tone. For spinal oncology patients, ambulation can also indicate the severity of disease burden and has been associated with survival and perioperative recovery. 36 Pre-operative referral of patients with low walk scores to physical therapy may increase chances of home discharge when surgical delay is deemed to be safe and further prospective studies are warranted.
Limitations
This study should be interpreted within the context of its limitations. This study was specifically designed to assess the utility of the RAPT questionnaire and its subcomponents to predict post-operative outcomes. The coarsened exact matching analysis strategy used in this study was employed to isolate and compare patients with similar medical comorbidities and demographic profiles, thereby controlling for factors known to affect post-operative outcomes. This matching protocol comes at the cost of limiting sample size, but the rigorous patient matching criteria preserves the internal validity of the results.
For this analysis, we were unable to match patients by tumor pathology due to limitations in the cohort size. Differences in tumor pathology, including primary and metastatic spinal tumors, are known to dictate long-term patient outcomes and prognosis. 37 However, patient outcomes in the intermediate post-operative period are largely influenced by pre-operative functional status rather than cancer type.25,38,39 Hence, other published discharge disposition prediction models have found no correlation with tumor pathology and omitted this variable. 29 Pre-operative outcome prediction tools that do include cancer pathology have also failed to demonstrate increased clinical utility over tools that do not include it. 40 Additionally, from a healthcare quality standpoint, primary and metastatic tumors have been shown to have similar readmission and hospitalization costs. 41 Therefore, the results of our study are still relevant to pre-operative prediction of outcomes after surgery, including in cases when the exact pathology is unknown. Follow-up study in a large multi-center cohort of spinal oncology patients is warranted to understand the relevance of RAPT in different tumor types.
Finally, RAPT was designed to predict discharge disposition, so it has limited predictive ability for other postoperative outcomes. Incorporation of other patient-specific measures, such as frailty, may increase its utility for the spinal oncology population outside the immediate postoperative period.
Conclusion
Reliable and accurate pre-operative determination of discharge disposition can help facilitate the care of spinal oncology patients, as well as reduce cost. The total RAPT score and the individual walk score can predict discharge disposition following surgery, even after matching patients on multiple covariates known to affect clinical outcomes. Our results provide the rationale for further prospective, randomized studies on the implementation of RAPT in the spinal oncology population.
Footnotes
Acknowledgements
The EpiLog Project, The Bernadette and Kevin McKenna Family Research Fund, The Leonard Davis Institute.
Ethical Considerations
This study was approved by the IRB at the Hospital of the University of Pennsylvania. The IRB number for this study is 825431. All ethical guidelines and rules were followed to protect patient privacy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NRM received support from the Bernadette and Kevin McKenna Family Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.