
Abstract
Objectives
Instrumentation failure remains a significant complication in spinal surgery. Preoperative bone health assessment is critical prior to spinal fusion surgery. Currently, bone mineral density (BMD) and Hounsfield Unit (HU) are common preoperative assessments, although it remains unclear which is more predictive of screw fixation strength. We aimed to identify the most reliable preoperative evaluation method for predicting screw insertional torque in patients undergoing lumbar fusion surgery.
Methods
Patients who underwent lumbar fusion surgery utilizing pedicle screws between 2021 and 2023, were prospectively registered in our database. All participants underwent preoperative lumbar CT and Dual-Energy X-ray Absorptiometry (DEXA) scans. We analyzed data from 109 patients who underwent lumbar fusion surgery with 6.5 mm pedicle screws. Preoperative BMD was measured via DEXA (lumbar spine and femur), and HU values were obtained from preoperative lumbar CT scans. Insertional torque of the screws was measured intraoperatively using a calibrated torque wrench. Correlations between insertional torque and BMD/HU as well as patients’ demographic/lab data were analyzed.
Results
A total of 335 pedicle screws were analyzed. Femoral BMD exhibited the strongest correlation with insertional torque (r = 0.557, P < 0.001), compared with lumbar BMD and HU. Age, ASA grade, BMI, serum calcium, and albumin showed weak correlations.
Conclusions
Femoral BMD demonstrated the strongest, although still moderate, association with intraoperative insertional torque among all preoperative bone quality measures evaluated, suggesting that it may offer a more informative estimate of underlying bone strength in patients undergoing lumbar fusion.
Introduction
With the aging population, instrumented lumbar fusion has become increasingly common. Despite recent technological advancements, instrumentation failure remains a significant concern in spinal surgery. Osteoporosis frequently coexists in this population and is associated with screw loosening and construct failure, including pedicle screw failure secondary to poor pull-out strength.1,2 As such, preoperative evaluation of bone health is essential to mitigate the risk of instrumentation failure.
Several cadaveric studies have investigated screw pull-out strength in osteoporotic bone.3,4 However, assessing pull-out strength in actual patients is not feasible, since testing a screw to failure would cause significant complications. Surgeons commonly use the insertional torque of pedicle screws to judge the strength of fixation, and prior research has demonstrated a strong correlation between pull-out strength and pedicle screw insertional torque.5,6 Thus, quantifying screw insertional torque and exploring its relationship with bone health would yield valuable insights.
Common preoperative assessments of bone health include bone mineral density (BMD) and the T-score from Dual-Energy X-ray Absorptiometry (DEXA) and Hounsfield Unit (HU) values obtained through computed tomography (CT). DEXA is the gold standard for assessing bone mineral density (BMD). There are several biomechanical studies indicating that the pull-out strength of a pedicle screw is influenced by BMD.4,7 Over the past decade, HU has gained popularity, as the majority of patients undergo CT scans for surgical planning prior to surgery. BMD and HU exhibit a moderate to strong correlation.8-10 However, it remains controversial which preoperative assessment -BMD of the femur, BMD of the lumbar spine, or HU- is the most reliable predictor of screw insertion torque. If HU demonstrates comparable accuracy to DEXA, it could emerge as a gold standard for testing. Therefore, we hypothesized that HU would demonstrate a comparable correlation with pedicle screw insertional torque when comparing with DEXA. Our objective was to identify the most effective preoperative evaluation method that accurately reflects screw insertional torque. In this study, we examined the correlation between screw insertion torque and BMD/HU in patients undergoing lumbar fusion surgery.
Materials and Methods
Subjects
This is a retrospective review of prospectively collected data from a single institution. Patients who underwent lumbar fusion surgery utilizing pedicle screws between August 2021 and July 2023, were systematically registered in our database. All included patients underwent lumbar fusion for degenerative spinal disorders, such as lumbar spinal stenosis, degenerative spondylolisthesis, or foraminal stenosis. Patients with adult spinal deformity, trauma, tumor, infection, or inflammatory disease were excluded. All participants underwent preoperative lumbar CT and DEXA scans. Given that 6.5 mm diameter screws were the most frequently utilized, we extracted data for patients who had at least one 6.5 diameter screw from the database for analysis. S1 screws were excluded from the analysis due to the distinct morphology of S1 pedicles compared to other lumbar vertebrae. Cases involving revision, tumors, and infections and patients under 18 years old were also excluded. Informed consent was obtained from all participants.
Procedure and Measurement of Insertional Torque
The same pedicle screw system (New TREND Spinal System, SHOWA IKA, Aichi, Japan) was used for all patients. The screw size was determined based on preoperative CT imaging. All pedicle screws were inserted using a standard freehand technique. In brief, pilot holes were prepared with a 2 mm burr. After probing with Gearshift, 1 mm smaller tapping was applied only through the pedicle. The vertebral body portion of the trajectory was intentionally left untapped to preserve cancellous bone engagement and optimize screw purchase. Insertional torque was measured prospectively during each surgery. For every screw placed, the maximum insertional torque was recorded in real time using a calibrated torque wrench (TRUE SHEED Co., Ltd., Kyoto, Japan; Figure 1) before completion of the construct. All torque values were documented immediately by the assisting staff. Screw torque wrench. The insertional torque was measured using a calibrated torque wrench with a specially designed connector for spine screw systems
Postoperative CT was used to exclude screws with medial, lateral, superior, or inferior breaches or clear endplate engagement or violation. This screening process ensured that all screws included in the analysis represented accurate freehand placement, thereby minimizing the effect of technical factors on insertional torque measurements.
Evaluation of Bone Mineral Density
All DEXA scans were performed with use of Hologic QDR series (Hologic, Waltham, MA) within 3 months prior to surgery. BMD of the lumbar spine (L1-4) and femoral neck was measured preoperatively and analyzed by a radiologist at a central facility.
Evaluation of HU
CT scans were obtained using either SOMATOM definition AS ICT (Siemens, Munich, Germany) or Discovery HD 750 VEO (GE Healthcare, MA, USA) within 3 months prior to surgery. HU values were measured using the AW server 3.2 (GE healthcare, Munich, Germany). Standardized HUs were measured in the L1 vertebra using the standard method. 8 In this cohort, one patient had a previous L1 fracture, and HU was therefore measured at L2 for the patient. Measurements were performed at 3 locations: immediately below the superior endplate, at the center of the vertebral body, and above the inferior endplate. The largest possible elliptical region of interest, excluding cortical margins, was manually drawn within the cancellous portion of the vertebral body at these 3 locations, and the average of the 3 was taken as the HU value. Areas with Schmorl’s nodes or calcifications were excluded from the average. All measurements were performed manually using the PACS workstation tools. In 2 cases where a fracture was observed in the first lumbar vertebral body, measurements were performed on L2 vertebral body. Local HU was measured at the vertebral bodies where spinal instrumentation was planned in the same manner as the standardized HU. To assess measurement reproducibility, 2 independent spine surgeons performed HU measurements in a randomly selected subset of 20 patients. Inter-rater reliability was excellent, with an intraclass correlation coefficient (ICC = 0.92).
Blood Samples/Bone Turnover Markers
We evaluated serum levels of albumin, calcium, and bone turn over markers, including total N-terminal propeptide of type 1 procollagen (total P1NP; reference range in postmenopausal women, 26.4-98.2 μg/L; estimated using a total P1NP assay on an Elecsys automated analyzer; Roche Diagnostics, Switzerland) and tartrate-resistant acid phosphate type 5b (TRACP-5b; reference range, 170-590 mU/dL in men and 120-420 mU/dL in women; estimated using Osteolink® TRACP-5b® test kit; DS Pharma Biomedical Co, Ltd., Osaka, Japan). 11
Statistical Analysis
Categorical and continuous variables were analyzed using the Fisher exact probability test and Student’s T-test, respectively. Pearson’s correlation coefficients (r) were calculated to assess the relationships between screw insertional torque and variables. Because screw length influences insertional torque, screws were analyzed according to their implant length. Specifically, correlation analyses were performed separately for 40-mm and 45-mm screws to minimize confounding by screw length. This separation allowed evaluation of the association between bone quality parameters and insertional torque within each standardized length category.
To statistically compare the strength of these correlations within the same sample, Steiger’s Z test for comparing dependent correlations sharing one variable was applied.
This test accounts for the intercorrelation among the predictor variables (ie, femur BMD, lumbar BMD, and HU) when evaluating whether the correlation coefficients with insertional torque differ significantly. All pairwise comparisons (femur BMD vs lumbar BMD, femur BMD vs HU, and lumbar BMD vs HU) were performed, and Bonferroni correction was applied to adjust for multiple testing.
All statistical analyses were conducted using SPSS Statistics 26 (IBM Corp., Armonk, NY), with statistical significance set at P < 0.05 (two-tailed).
Results
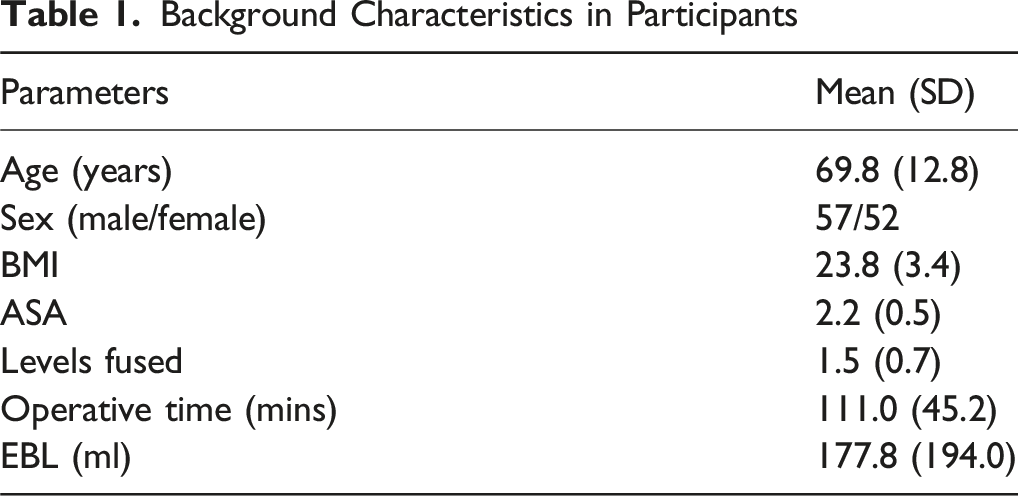
A total of 123 patients were identified in the database. Seven patients were excluded due to incomplete data, and an additional 7 were excluded for not having a 6.5 mm diameter screw. A total of 109 patients (57 males, mean age 69.8 years) were included in our analysis.
Background Characteristics in Participants
Summary of Bone Health Data in Participants
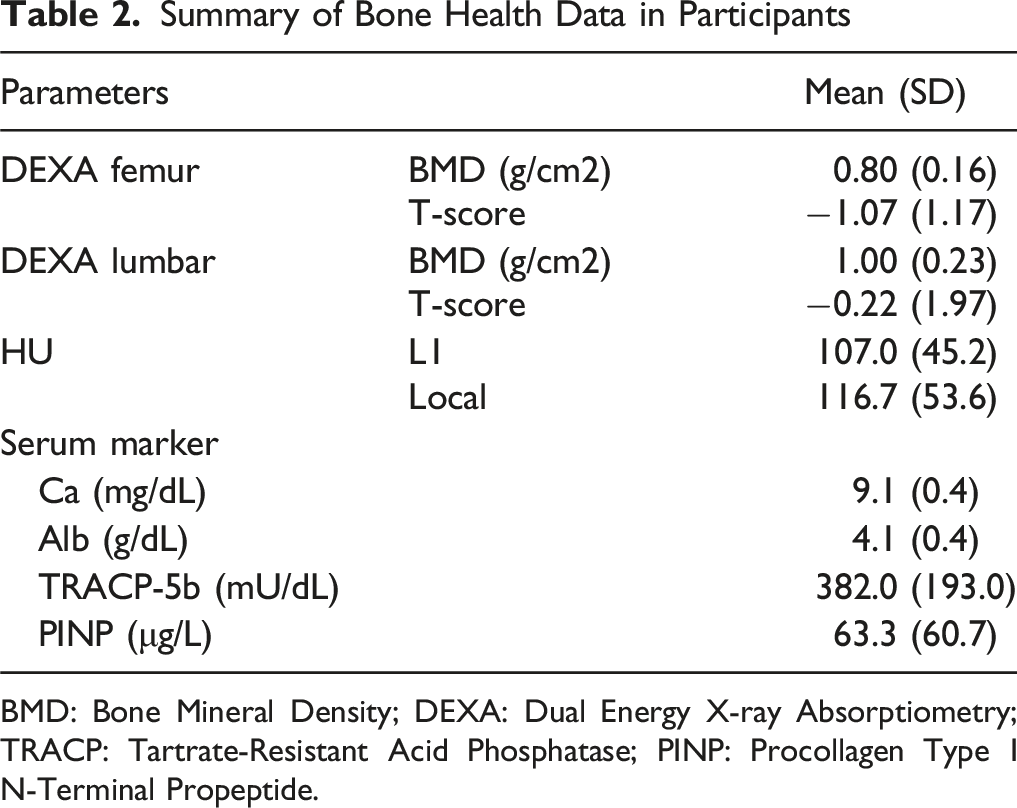
BMD: Bone Mineral Density; DEXA: Dual Energy X-ray Absorptiometry; TRACP: Tartrate-Resistant Acid Phosphatase; PINP: Procollagen Type I N-Terminal Propeptide.
A total of 586 pedicle screws were identified in the cohort. Of these, 240 screws (41%) were excluded because they did not meet the standardization criteria (ie, screws with diameters of 5.5 mm or 7.5 mm, or lengths of 35 mm or 50 mm). An additional 11 screws (1.9%) were excluded due to malposition, including medial or lateral cortical breach or engagement of the superior endplate. The final analysis therefore included 335 correctly positioned 6.5-mm screws with standardized lengths (190 screws with 6.5 × 40 mm and 145 screws with 6.5 × 45 mm), in order to minimize biomechanical variability across measurements. The mean insertional torque was 1.89 ± 0.88 and 2.07 ± 0.87 Nm, respectively). Longer screws exhibited a significantly higher insertional torque ((Figure 2; P = 0.035). Insertional torque by pedicle screw size Bar graph showing mean insertional torque (Nm) for 6.5 × 40 mm screws (n = 190) and 6.5 × 45 mm screws (n = 145). Error bars indicate standard deviation (SD) in the positive direction. The insertional torque was significantly higher in the 6.5 × 45 mm group compared to the 6.5 × 40 mm group (P = 0.035)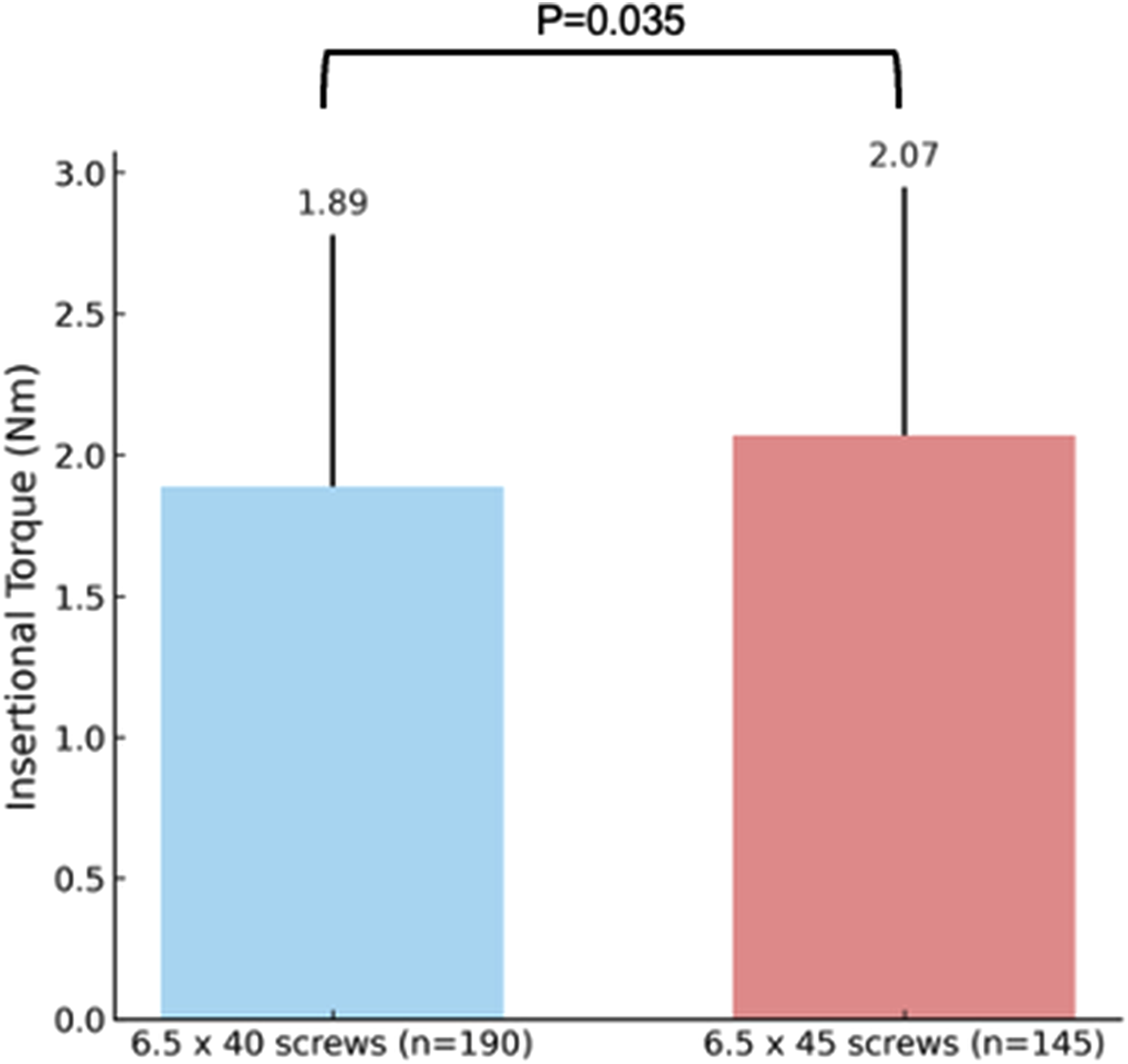
Correlation Between Insertional Torque With 6.5 × 40 mm Screws and Variables
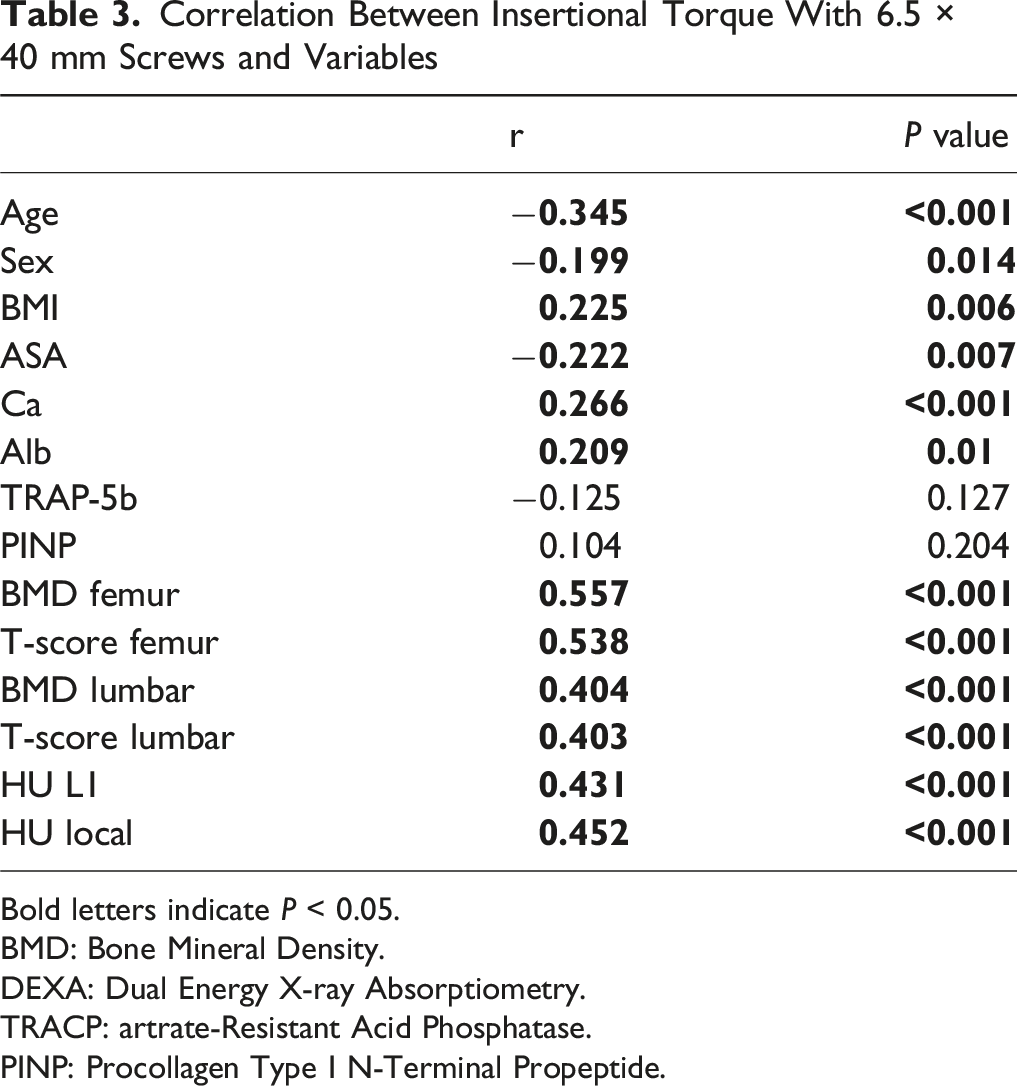
Bold letters indicate P < 0.05.
BMD: Bone Mineral Density.
DEXA: Dual Energy X-ray Absorptiometry.
TRACP: artrate-Resistant Acid Phosphatase.
PINP: Procollagen Type I N-Terminal Propeptide.
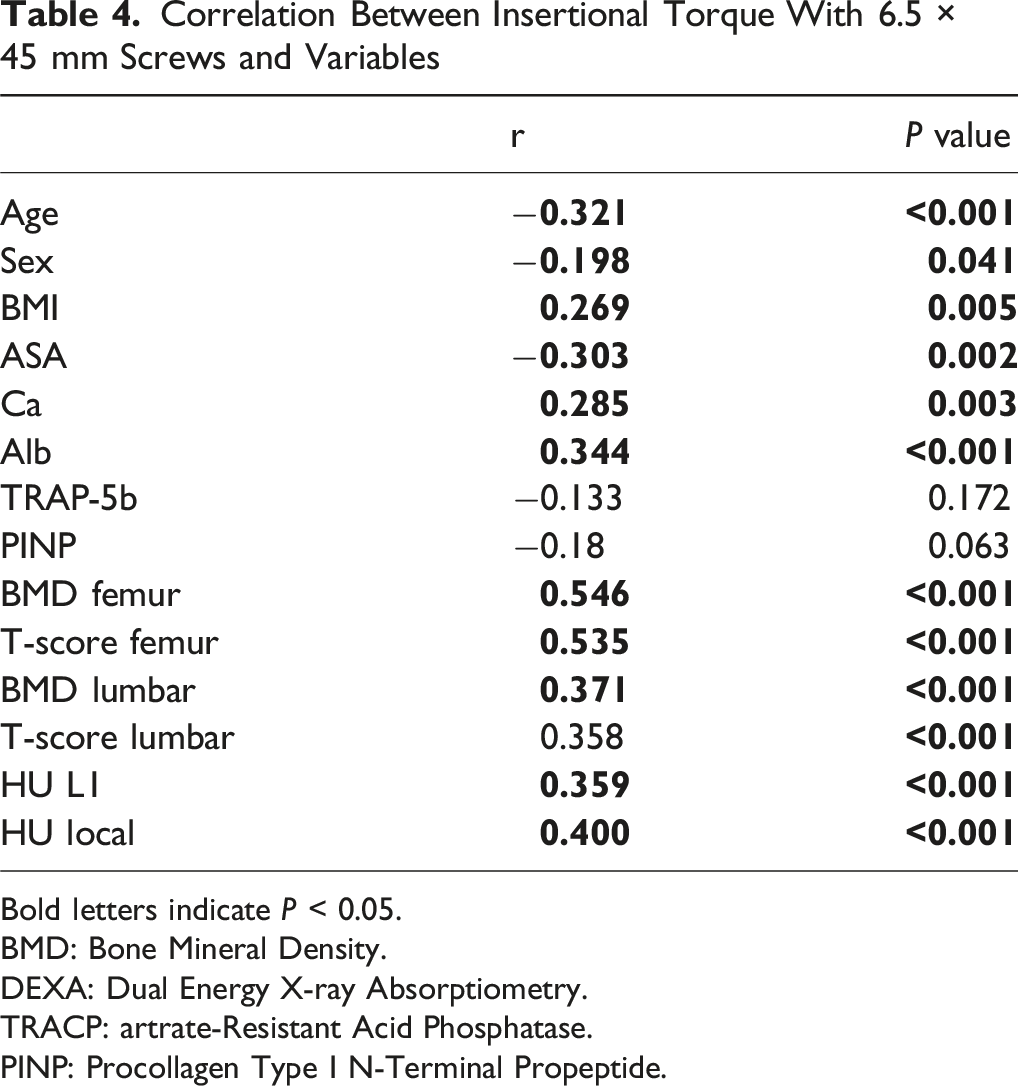
Correlation Between Insertional Torque With 6.5 × 45 mm Screws and Variables
Bold letters indicate P < 0.05.
BMD: Bone Mineral Density.
DEXA: Dual Energy X-ray Absorptiometry.
TRACP: artrate-Resistant Acid Phosphatase.
PINP: Procollagen Type I N-Terminal Propeptide.
In the cohort of 6.5 × 40 screws (n = 190), the correlation coefficients between insertional torque and the preoperative tests were as follows: femur BMD (r = 0.557), lumbar BMD (r = 0.404), standardized HU (r = 0.431), and local HU (r = 0.452). Steiger’s test demonstrated that the correlation of femur BMD with insertional torque was significantly higher than that of lumbar BMD (Bonferroni-adjusted P = 7.95 × 10-7), standardized HU (Bonferroni-adjusted P = 1.57 × 10-3) and local HU (Bonferroni-adjusted P = 8.38 × 10-3).
No significant difference was found between lumbar BMD and HUs (Bonferroni-adjusted P = 0.890).
In the cohort of 6.5 × 45 (n = 145), the correlation coefficients were femur BMD (r = 0.546), lumbar BMD (r = 0.371), standardized HU (r = 0.359), and local HU (r = 0.400). Femur BMD showed a significantly stronger correlation with insertional torque than lumbar BMD (Bonferroni-adjusted P = 7.7 × 10-5), HU (Bonferroni-adjusted P = 4.5 × 10-5) and local HU (Bonferroni-adjusted P = 6.8 × 10-4).
The difference between lumbar BMD and HUs was not statistically significant (Bonferroni-adjusted P = 0.948). In both screw types, femur BMD had a stronger correlation with insertional torque than lumbar BMD and HU (Figure 3). Correlation of preoperative measures with pedicle screw insertional torque Pearson’s correlation coefficient (r) between preoperative measures and pedicle screw insertional torque. Femur BMD demonstrated the strongest correlation with insertional torque in both screw groups: 6.5 × 40 mm screws (n = 190) and 6.5 × 45 mm screws (n = 145), compared with lumbar BMD and Hounsfield unit (HU) values. Femur BMD was significantly more strongly correlated with insertional torque than both lumbar BMD and HU, while no difference was found between lumbar BMD and HU in each group (P = 1.000). An asterisk mark indicates P < 0.01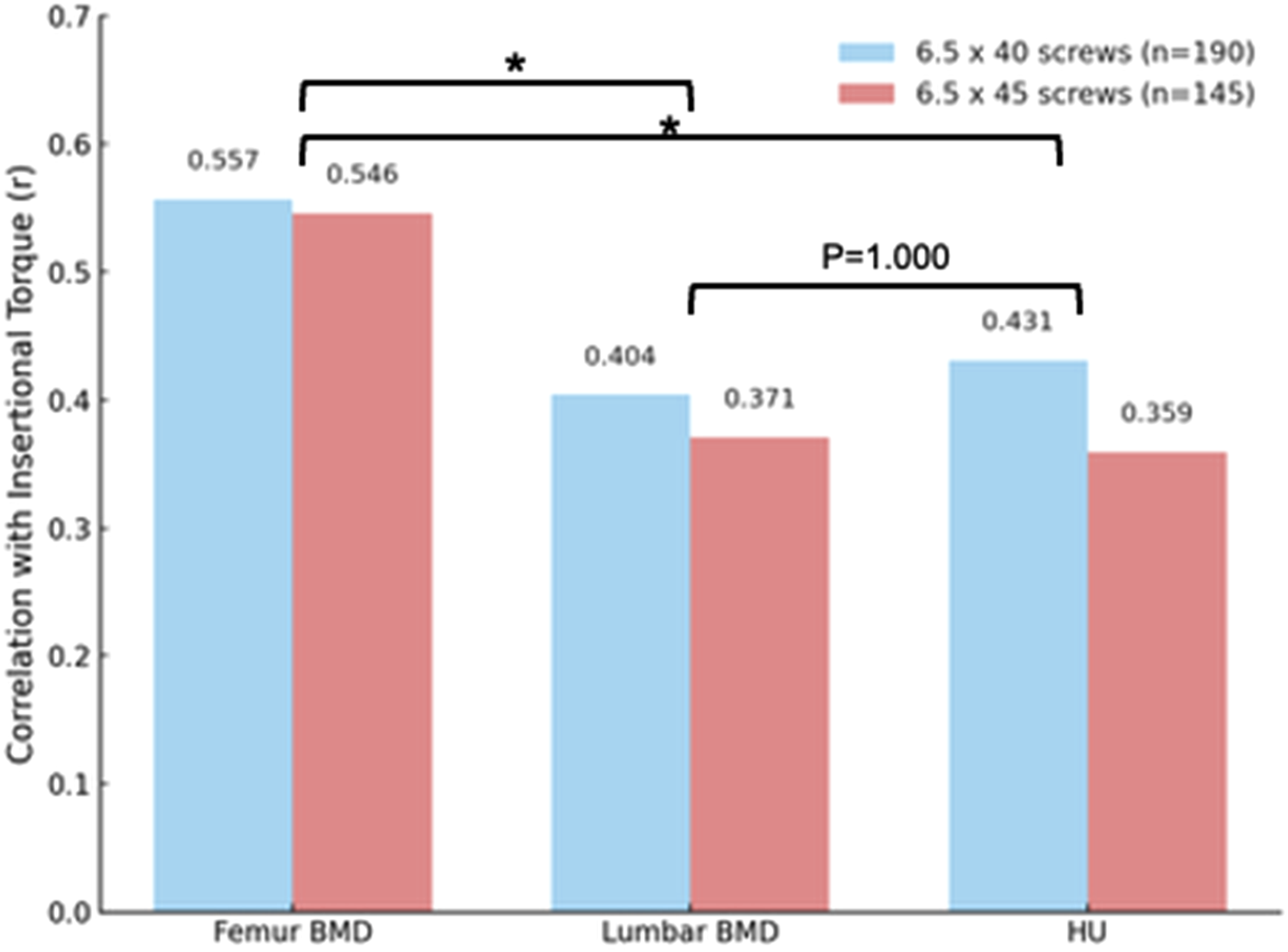
Discussion
With the increase of the aging population, the prevalence of osteoporosis has risen, and is anticipated to continue increasing in the future. Osteoporosis is associated with instrumentation failure and other complications,12,13 thus bone health assessment is crucial for patients undergoing instrumented spinal surgeries. An accurate measure for predicting screw fixation is vital for preoperative planning and optimization in spinal surgery. This study demonstrates that femoral BMD shows a stronger correlation with pedicle screw insertional torque than either lumbar BMD or HU, despite our use of both standardized (L1) and level-specific HU measurements in the analysis.
The superior predictive ability of femur BMD has several important clinical implications. First, femoral BMD reflects systemic bone quality and is less affected by degenerative changes such as osteophytes, facet hypertrophy, or endplate sclerosis, which frequently confound lumbar BMD measurements in patients with degenerative spine disease. 14 In our cohort, the mean lumbar T-score appeared to fall within the normal range despite many patients exhibiting reduced bone quality on CT-based or intraoperative assessment. This discrepancy likely reflects the well-recognized limitations of lumbar DEXA in elderly or degenerative populations, where structural changes can artifactually elevate BMD values. In contrast, femoral neck T-scores were lower and demonstrated greater variability, which may account for their stronger association with insertional torque. These findings suggest that femoral BMD may provide a more reliable preoperative indicator of systemic bone strength than lumbar BMD in patients undergoing spinal fusion.
Second, identifying patients with low femur BMD preoperatively could guide surgical decision-making. Surgeons may consider preoperative PTH use and intraoperative fixation strategies, such as larger-diameter screws, cement augmentation, or supplemental fixation techniques, in patients at higher risk of instrumentation failure. Moreover, postoperative management, including weight-bearing restrictions and tailored rehabilitation, could be optimized to minimize the risk of early implant loosening. Finally, improving preoperative prediction of screw fixation strength has the potential to reduce implant-related complications and the need for revision surgery, ultimately enhancing long-term outcomes and reducing healthcare costs. Future studies evaluating the relationship between femur BMD, screw loosening rates, and clinical outcomes will be essential to confirm these findings and further support the routine use of femur BMD in surgical planning for spinal fusion.
Several studies have investigated the correlation between HU and/or BMD with insertional torque. Oh et al conducted preoperative CT and DEXA on 53 patients undergoing thoracolumbar fusion surgery, revealing that screw insertional torque exhibited a stronger positive correlation with lumbar BMD than with HU values. 15 Several factors likely explain these differences. First, lumbar DEXA values are strongly affected by degenerative changes, including osteophytes, facet hypertrophy, and aortic calcification, which tend to artifactually elevate lumbar T-scores. In our cohort, composed entirely of degenerative lumbar disease, lumbar T-scores were near normal, making them less reflective of true trabecular bone strength. In contrast, femoral BMD provided a more reliable measure of systemic bone quality. Second, HU measurement protocols differed substantially between studies; Oh et al used midsagittal cancellous ROIs at each vertebra, whereas our study used axial cancellous ROIs at L1 only. Such methodological variation can influence the relative performance of HU. Third, the patient populations also differed. Oh et al included patients undergoing thoracolumbar surgery, and detailed information regarding underlying pathology or screw size was not fully specified. These factors may further contribute to differences in the observed relationships between bone density measures and insertional torque. Taken together, these considerations suggest that the results of the 2 studies are not truly contradictory but rather reflect differences in patient characteristics, measurement methodology, and the anatomic region used to assess bone density. Similarly, Choi et al assessed lumbar and femur BMD preoperatively for 181 patients and compared the correlations with insertional torque, demonstrating that lumbar BMD had a stronger correlation with insertional torque than femur BMD. They further indicated that the correlation between femur and lumbar BMD was only moderate (r = 0.566). The reliability of lumbar BMD may be compromised because of superimposition effects such as osteophyte formation, aortic calcification, and sclerotic changes. 14 These 2 studies included various screw diameters and lengths, as well as S1 for analysis, despite the fact that insertional torque is influenced by screw diameter and length. In the present study, to mitigate these biases, we exclusively analyzed 6.5 mm diameter screws and excluded S1 screws, given S1’s distinct morphology and the tendency of S1 screws to achieve tri-cortical purchase, leading to overestimated insertional torque. We examined the 6.5 × 40 mm and 6.5 × 45 mm screws separately, and both exhibited similar results.
We found that age and ASA had a weak negative correlation with insertional torque while BMI, serum calcium, and serum albumin level had a weak positive correlation with insertional torque. It is expected that age and ASA have a negative effect on insertional torque as the prevalence of osteoporosis increases as aging, 16 and ASA represents comorbidity.
BMI had a weak positive correlation with insertional torque. Many studies have shown underweight is an independent risk factor for developing osteoporosis.17,18 Optimal BMI range is 23.0 to 24.9 kg/m2 to minimize the risk of osteoporosis. Beyond this range, the risk of osteoporosis decreases whereas a BMI below this range may increase the risk of osteoporosis. 17 Low serum albumin was shown to be associated with low bone mineral density and increased risk of fragility fracture.19,20 Low serum albumin concentration is a historical marker of malnutrition, 21 has been consistently linked with adverse health outcomes such as cardiovascular disease, venous thromboembolism, cancer, as well as increased mortality.
Interestingly, TRACP-5b and P1NP did not correlate with insertional torque. This likely reflects the fundamental difference between dynamic bone turnover and structural bone strength. Bone turnover markers represent short-term metabolic activity—rates of resorption (TRACP-5b) or formation (P1NP)—and do not directly quantify mineralized tissue content or trabecular architecture. In contrast, insertional torque depends largely on local cancellous bone density and structural stiffness, which are more closely reflected by static imaging-based measures such as HU or BMD. Thus, although turnover markers provide systemic information on skeletal metabolism, they may not serve as reliable indicators of immediate mechanical fixation strength in the vertebrae.
Our study has several limitations. This study is limited by its retrospective single-center design and modest sample size, which may not fully capture the variability in clinical practice. Second, HU was measured only at L1 rather than at instrumented levels. Third, this is an intraoperative in vivo study evaluating an insertional torque, not pull-out strength. Pull-out strength may serve as a more indicative variable for evaluation, as it directly correlates instrumentation failure. However, numerous studies have indicated a strong correlation between insertional torque and pull-out strength.6,22,23 Since studies examining pull-out strength are feasible only in cadaveric bone, insertional torque represents a reasonable variable for in vivo evaluation. Fourth, bone quality may vary depending on the underlying pathology. Because all patients in this study had degenerative lumbar conditions, variability in bone quality attributable to differing diagnoses was minimized. However, bone metabolism and structural bone loss may differ in other clinical settings, such as adult spinal deformity, traumatic injuries, or osteoporosis-related fractures. Therefore, the generalizability of our findings to non-degenerative pathologies should be interpreted with caution. Fifth, Quantitative computed tomography (QCT) data is not available in our cohort. QCT has recently emerged as an alternative method for assessing bone quality. Unlike standard CT–based Hounsfield unit measurements, QCT provides true volumetric bone mineral density using calibration phantoms and dedicated post-processing software. QCT is less affected by degenerative changes, osteophytes, 24 and aortic calcification, which may artifactually elevate both DEXA-based T-scores and HU values. However, QCT is not routinely performed in our institution and requires specialized equipment, making it less feasible in most real-world surgical settings. Because this study relied on clinically obtained imaging, QCT measurements were not available. It is possible that QCT-derived density values could demonstrate stronger correlations with insertional torque, and future studies incorporating QCT may clarify whether volumetric bone density better reflects intraoperative mechanical fixation strength. Lastly, we evaluated only intraoperative insertional torque. Although torque is not a clinical endpoint, low intraoperative torque has direct implications for surgical decision-making, including the need for screw augmentation, modification of screw trajectory, or adjustment of perioperative bone health management. Thus, the mechanical relationships demonstrated in this study remain clinically meaningful. Nevertheless, we acknowledge that follow-up assessments, such as nonunion rates, instrumentation failure, or cage subsidence, would be valuable to determine which preoperative bone quality measure most reliably predicts postoperative mechanical complications.
In conclusion, femur BMD exhibited the most robust correlation with pedicle screw insertional torque when compared to HU and lumbar BMD. While HU has gained popularity in clinical practice, our findings indicate DEXA, in particular femur BMD, remains the most reliable assessment for evaluating bone health prior to instrumented lumbar surgery. Additionally, other variables such as age, ASA grade, BMI, as well as serum calcium and albumin levels, were also found to correlate with insertional torque and should be evaluated preoperatively.
Footnotes
Consent to Participate
All research participants provided written consent to be a part of study.
Authors’ Contribution
Yoji Ogura, MD, PhD-Conceptualization (lead); Methodology (lead); Formal Analysis (equal); Investigation (equal); Writing – Original Draft (lead); Writing – Review & Editing (lead); Supervision (equal); Project Administration (equal).
Taisei Kato, MD-Data Curation (lead); Investigation (lead); Formal Analysis (equal); Writing – Review & Editing (equal).
Yuichiro Nishiyama, MD, PhD-Methodology (equal); Investigation (equal); Resources (equal); Writing – Review & Editing (supporting).
Arya Varthi, MD-Investigation (supporting); Validation (equal); Writing – Review & Editing (supporting).
Yoshihisa Suzuki, MD, PhD-Supervision (lead); Project Administration (lead); Resources (lead); Writing – Review & Editing (equal).Investigation (lead); Data Curation (lead); Formal Analysis (lead); Writing – Review & Editing (equal). Study Design: Single-center, retrospective analysis of prospectively collected data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
Approval from the Institutional Review Board of Tachikawa Hospital 2018-020.