
Abstract
Study Design
Retrospective cohort study.
Objective
To evaluate the therapeutic effects of postoperative repetitive transcranial magnetic stimulation (rTMS) on neuropathic pain (NP) and neurological recovery in patients with degenerative cervical myelopathy (DCM).
Methods
Fifty-nine DCM patients who underwent cervical decompression between 2017 and 2024. Twenty-seven received postoperative rTMS (20 Hz, 20 trains of 40 pulses at 90% resting motor threshold over the biceps brachii for 5 consecutive days) in addition to routine care, while 32 received routine care only. Pain intensity at the neck, upper limbs, and below-neck regions was assessed using the 10-cm Visual Analog Scale (VAS). NP was identified by a Douleur Neuropathique 4 (DN-4) score ≥4. Hand dexterity, myelopathy severity, and conduction function were evaluated by the 10-second grip-and-release test, modified Japanese Orthopedic Association (mJOA) scale, and somatosensory/motor evoked potentials (SSEP/MEP) respectively.
Results
Among patients with NP (n = 25), rTMS significantly reduced VAS pain scores in the upper limbs and below-neck regions (P < 0.05), but not in the neck. No effect was observed in non-NP patients (n = 34). rTMS also improved hand dexterity, mJOA scores, and recovery rates compared with controls, particularly in patients with preoperative mJOA ≤14 (P < 0.05). These benefits persisted for 6 months. However, SSEP and MEP results were comparable between groups, suggesting that rTMS did not alter cervical conduction.
Conclusion
Five-day postoperative rTMS was associated with NP and functional recovery in DCM, especially in severe cases, possibly by modulating higher central pathways.
Keywords
Introduction
Cervical spine degeneration is frequently observed and may evolve into spinal cord injury, leading to the degenerative cervical myelopathy (DCM). 1 DCM can present with various symptoms such as poor coordination, pain, weakness, gait disturbance, dysfunction of the bladder or bowels, and even quadriplegia in severe cases. 1 DCM is closely associated with the aging population, and causes considerable disability, social economic burden and an impact on quality of life. 2
Surgical decompression remains the only evidence-based intervention to halt disease progression in moderate to severe DCM. 3 However, by removing the compression elements from the spinal cord and prevent additional harm, surgery does not resolve the existing damage, and many patients continue to experience long-term neurological impairment. The neurological recovery after decompression surgery has been attributed to neuroplasticity. 4 Postoperative rehabilitation in DCM is rarely studied, and interventional trials are scarce—prompting its identification as a top priority in the RECODE-DCM research initiative.5,6
Transcranial magnetic stimulation (TMS) is a non-invasive technique that uses brief, high-current pulses in a coil to generate a magnetic field, inducing an electric current in the brain and activating neurons locally and remotely. 7 Repetitive TMS (rTMS) can lead to changes in neural activity lasting, and modulates neuroplasticity. 7 Beyond DCM, rTMS has been applied in a broad spectrum of neurological conditions, including stroke, Parkinson’s disease, and neuropathic pain(NP), where it has demonstrated efficacy in improving motor function and alleviating chronic pain symptoms. 8 Importantly, several studies have investigated rTMS in patients with spinal cord injury (SCI), reporting improvements in neuropathic pain, spasticity, and motor recovery.9,10 Given the overlapping pathophysiological mechanisms between SCI and DCM, such as demyelination, axonal injury, and maladaptive plasticity, these findings provide translational relevance and support the rationale for testing rTMS in DCM. 11 Mechanistically, rTMS is believed to exert its therapeutic effects by enhancing neuroplastic reorganization, restoring excitatory–inhibitory balance in cortical circuits, facilitating corticospinal connectivity, and engaging descending pain modulatory pathways. 10 Collectively, these mechanisms may complement surgical decompression by promoting functional recovery and alleviating neuropathic pain in patients with DCM.
In this two-centre retrospective cohort study, we evaluated the efficacy of postoperative rTMS as a rehabilitation tool in alleviating pain, improving sensorimotor function, and enhancing neurophysiological conduction in patients with DCM. The study aims to elucidate the therapeutic potential of rTMS in mitigating pain and promoting neurological recovery following surgery in DCM.
Materials and methods
Participants
This retrospective study was approved by the institutional review boards (IRB) of the First Affiliated Hospital of Sun Yat-sen University and Guangdong Provincial People's Hospital (Trial registration number: [2024]265) on November 10th, 2024. We utilized only de-identified, retrospective medical data. Ethical approval was obtained from the IRBs of both participating institutions, which waived the requirement for informed consent in accordance with the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. In this cohort, all patients had a confirmed diagnosis of DCM and underwent cervical decompression surgery performed by 6 senior spine surgeons (H.G., X.Z., and Z.Y.), with comprehensive clinical and neurophysiological assessments documented in their medical records. The diagnostic criteria for DCM required at least 1 clinical sign of myelopathy (see below) and imaging-confirmed cervical spinal cord compression, with no evidence of thoracic or lumbar stenosis. The clinical signs of DCM included: (a) segmental signs – upper limb muscle atrophy/weakness or selective reflexes loss in a segmental pattern (biceps, triceps, or finger flexors); (b) long-tract signs – leg spasticity, hyperreflexia, positive Babinski sign, or unexplained sensory symptoms on segments below the thoracic spine; (c) unambiguous sensory abnormalities of the upper limb. Exclusion criteria were: (a) prior spinal surgery; (b) concomitant spinal cord trauma (c) other conditions that may lead to neurological dysfunction.
Participants underwent rehablitative rTMS or routine postoperative rehabilitation including early mobilization, respiratory training, and basic physical therapy (eg, gait and balance exercises). No additional structured neurorehabilitation was involved. All participants had standard postoperative analgesia with Celecoxib (100 mg, twice daily for 2 weeks). For those with a history of chronic neuropathic pain on long-term analgesics, preoperative medications were maintained when clinically indicated and later adjusted according to standard postoperative regimens.
rTMS Protocol
Rehablitative rTMS therapy was performed for 5 consecutive days starting from 1 day after cervical decompression surgery. rTMS stimulation was applied using a Magstim Super Rapid stimulator (Magstim Co., UK) with a 100 mm circular coil over the C3 or C4 site, contralateral to the more painful side, based on the 10-20 EEG system
12
(Figure 1B). To ensure precise repositioning, after the first stimulation the hotspot was marked directly on the scalp with a skin-safe line marker, and subsequent sessions were delivered consistently at the same marked site. The resting motor threshold (RMT) was defined as the lowest stimulation intensity that elicited MEPs of at least 50 μV peak-to-peak amplitude in the relaxed biceps brachii muscle in ≥50% of 10 consecutive trials.
13
Each session included 20 trains of 40 pulses stimulations at 20 Hz frequency, with the intensity of 90% of the RMT for the biceps brachii. Stimulation was performed either by a technician (J.C.) or by a clinician (Z.Y.); both have been long-term colleagues with more than 10 years of clinical experience in electrophysiology. Flowchart of the retrospective cohort study design and illustration of rTMS and neurophysiological assessments. (A) Flowchart of the retrospective patient collection and the study design. (B) International Federation of Clinical Neurophysiology (IFCN) 10-20 System—Map of the head stimulation point illustration. rTMS was performed over the predominant side of the primary motor (M1) cortex, which is the C3 point. (C) The somatosensory evoked potential (SSEP) and Motor evoked potential (MEP) components in the present study (a 43-year-old DCM male with preoperative testing). Conduction time between the N9-to-N13 onset and N13-to-N20 onset, and onset-to-peak amplitudes of the N13 and N20 waves were recorded from the SSEP. MEP components are received from the abductor digiti minimi (ADM) muscle of the hand. Central motor conduction time (CMCT) is measured from the onset of cervical stimulation wave to the onset of brain cortical stimulation wave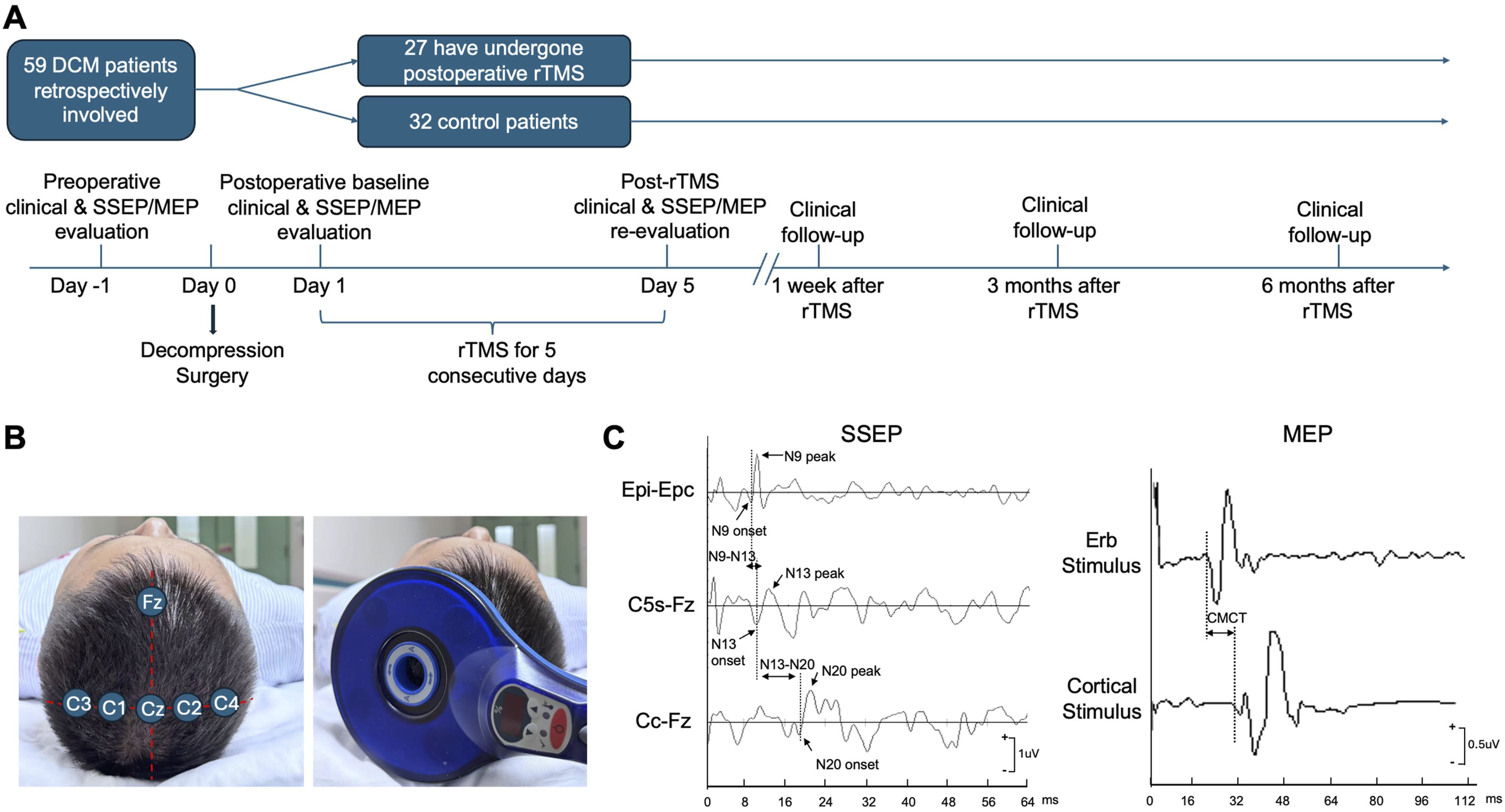
Clinical Data Collection
Data on the clinical characteristics of the patients, including age, gender, symptom duration, follow-up period, body mass index, smoking history and medical history were retrospectively collected. For pain evaluation, the intensity was evaluated based on the 10-centimeter Visual Analog Scale (VAS, 0 = no pain and 10 = maximal pain imaginable). Moreover, we applied the Douleur Neuropathique 4 (DN-4) to interpret the presence of neuropathic pain (NP) quality, 14 and Michigan Body Map (MBM) to determine its location. 15 Patients with DN-4 ≥ 4 are diagnosed with neuropathic pain. 14 We collected the VAS pain intensity data in the neck (VAS_neck), either side of upper extremity (VAS_upper), and trunk or lower extremity (VAS_trunk&lower) according to the MBM anatomical classification. Stenotic levels were identified based on the sagittal and axial images of the cervical magnetic resonance imaging (MRI). Surgical decompression levels and decompression procedures were also collected.
For motor function evaluation, we assessed the hand dexterity with the 10-second grip and release (10s-G&R) test. 16 DCM patients are reported to suffer from mild (17 to 20 cycles), moderate (14 to 16 cycles), and severe (13 cycles or less) hand dexterity impairment according to the 10s-G&R test. 16 Overall neurological function in all DCM patients were also assessed by the modified Japanese Orthopedic Association (mJOA) scores (18-points scale). 17 The mJOA recovery rate (RR) calculated through Hirabayashi method 18 was used to assess the outcomes: RR = [postoperative mJOA score - preoperative mJOA score] / [18 - preoperative mJOA score] × 100%. All clinical assessment data were collected by trained assessors (X. Cheng, S. Zeng and S. Zhan) who were blinded to group allocation.
Electrophysiological Assessments
An electrophysiological monitoring system (Nicolet Endeavor CR) was used to record the evoked SSEPs by stimulating the peripheral nerves. Recording electrodes were placed over the spinous process of the fifth cervical vertebra (C5S), the contralateral parietal cortex (Cc) and forehead reference site (Fz) regions of the scalp, and Erb’s points ipsilateral (EPi) and contralateral (EPc) to the stimulation. 19 The SSEP waves detected in the EPi-EPc, C5s-Fz, and CC-Fz montage are referred to as N9, N13, and N20, respectively. The somatosensory conduction time including the N9-N13 and N13-N20 inter-onset latencies, as well as the amplitudes of N13 and N20 were recorded. 20 After measuring the SSEPs, a Magstim 200 stimulator (Magstim, Whitland, UK) was used to deliver transcranial and transforaminal stimuli through a circular coil on C5 spinous process and contralateral parietal cortex. The MEP signals were recorded from the abductor digiti minimi (ADM) muscle of the hand in respond to the MEP elicited. Central motor conduction time (CMCT) was calculated by subtracting the peripheral conduction time from cervical nerve root to the muscle from the latency of responses evoked by cortical stimulation. 21 (Figure 1C).
Outcome Measures
The primary endpoints of this study were the changes in neuropathic pain intensity (VAS) and neurological function (mJOA) following surgery. The secondary endpoints included pain quality (DN-4); pain distribution (MBM); hand dexterity (10s-G&R); the mJOA recovery rate; and neurophysiological parameters (SSEPs and MEPs). Clinical assessments were performed at preoperative baseline, 1day after decompression surgery (2 hours before the first rTMS stimulation), 6 days after surgery (immediately after the last rTMS session), and during postoperative follow-up at 1 week, 3 months, and 6 months after.
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation (SD). Baseline demographic and clinical characteristics were compared between the rTMS and control groups using the independent-samples t test for continuous variables and the χ2 (chi-square) test for categorical variables. Within-group comparisons across different time points were performed using the Wilcoxon signed-rank test. Between-group comparisons at corresponding time points were conducted using the independent-samples t test. Subgroup analyses of mJOA scores were prespecified according to DCM severity, categorized as mild (mJOA ≥15), moderate (mJOA 12-14), and severe (mJOA <12), to evaluate the differential effects of rTMS across disease severities. All statistical tests were two-tailed, and a P value <0.05 was considered statistically significant.
Results
Demographic and Preoperative Disease Severity of Patients Enrolled in rTMS-Treated and Control Groups
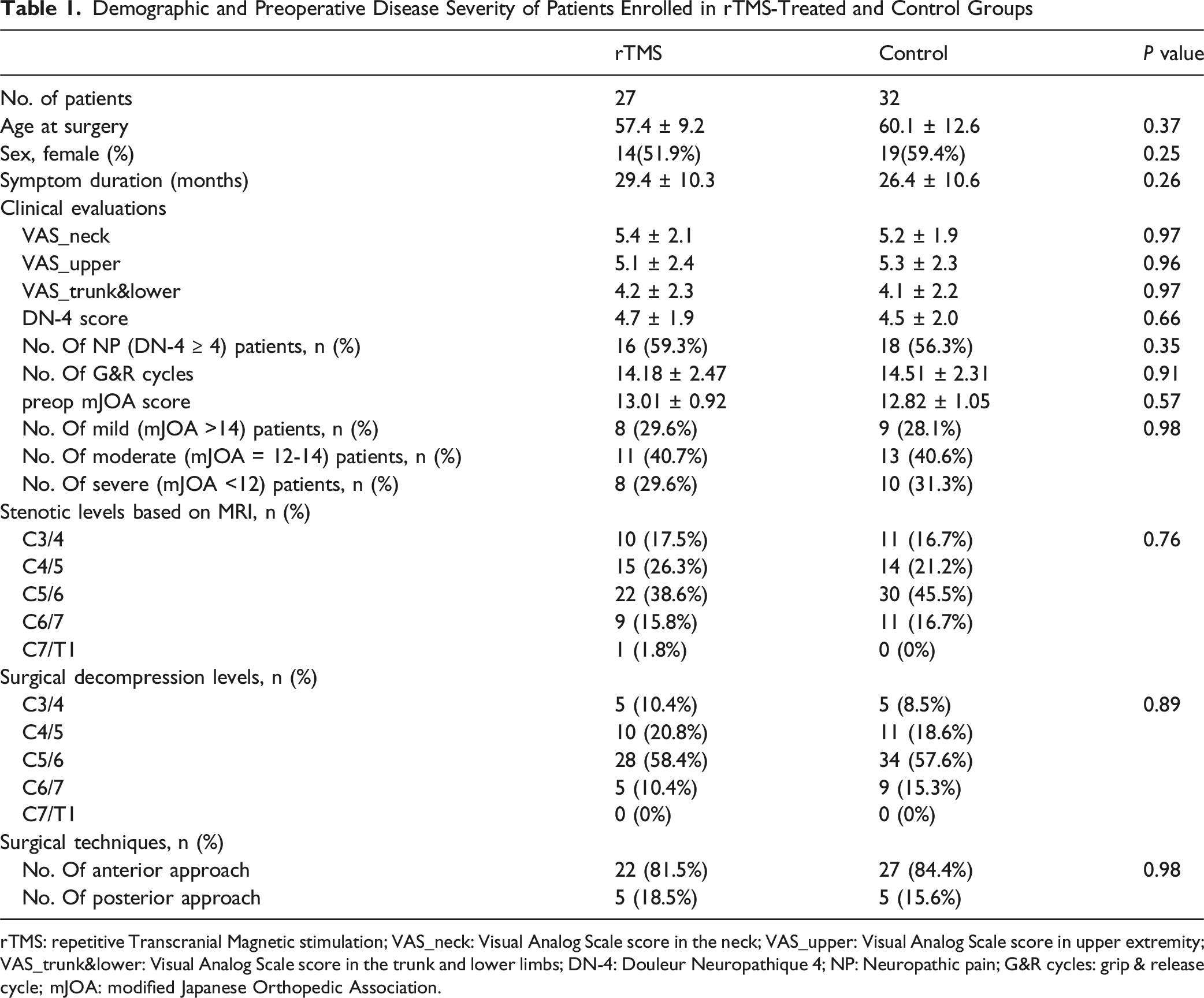
rTMS: repetitive Transcranial Magnetic stimulation; VAS_neck: Visual Analog Scale score in the neck; VAS_upper: Visual Analog Scale score in upper extremity; VAS_trunk&lower: Visual Analog Scale score in the trunk and lower limbs; DN-4: Douleur Neuropathique 4; NP: Neuropathic pain; G&R cycles: grip & release cycle; mJOA: modified Japanese Orthopedic Association.
Clinical Evaluation of Pain
Changes in Pain Intensity Among DCM Patients With and Without NP Following Control or Active rTMS
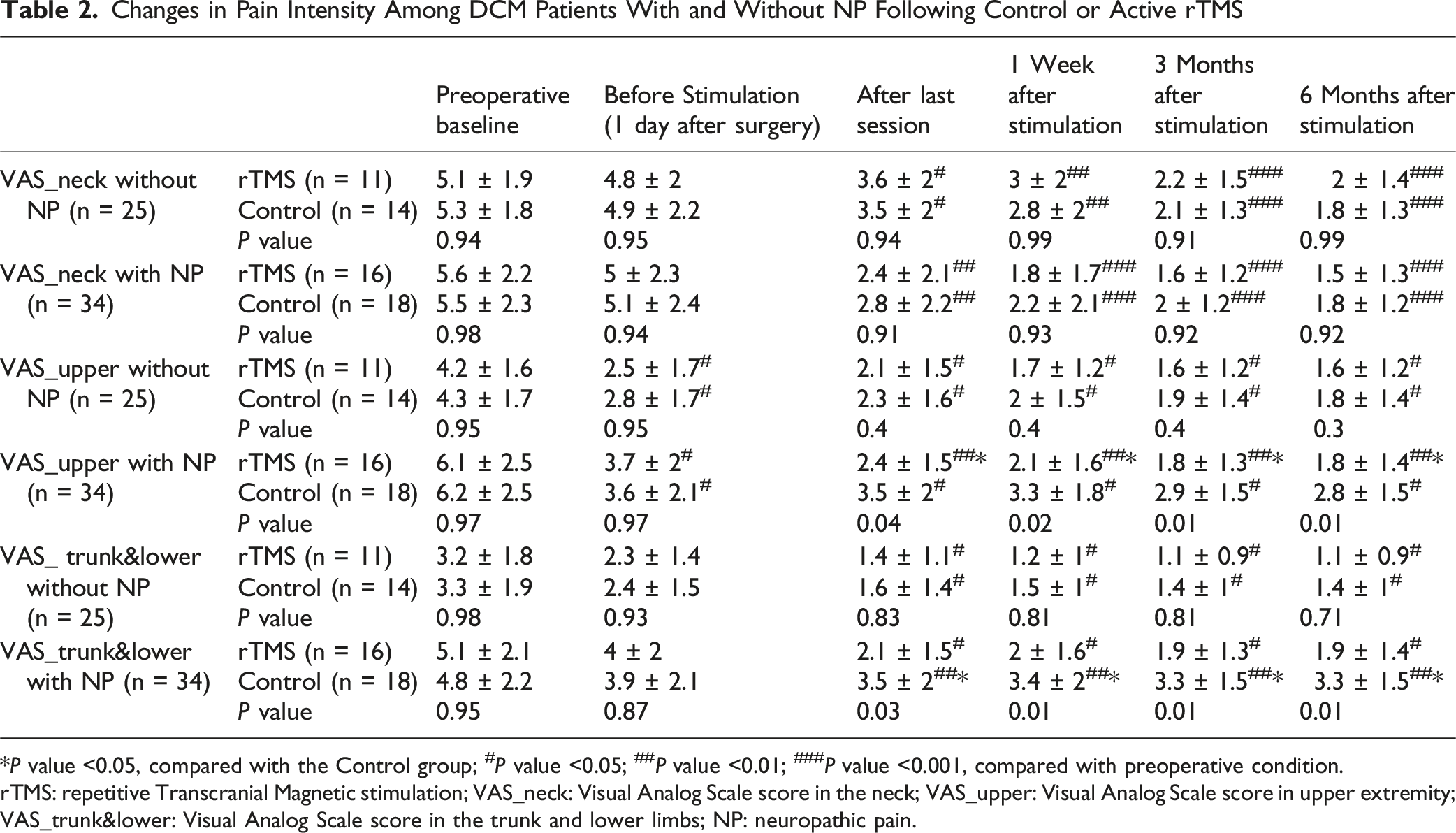
*P value <0.05, compared with the Control group; #P value <0.05; ##P value <0.01; ###P value <0.001, compared with preoperative condition.
rTMS: repetitive Transcranial Magnetic stimulation; VAS_neck: Visual Analog Scale score in the neck; VAS_upper: Visual Analog Scale score in upper extremity; VAS_trunk&lower: Visual Analog Scale score in the trunk and lower limbs; NP: neuropathic pain.
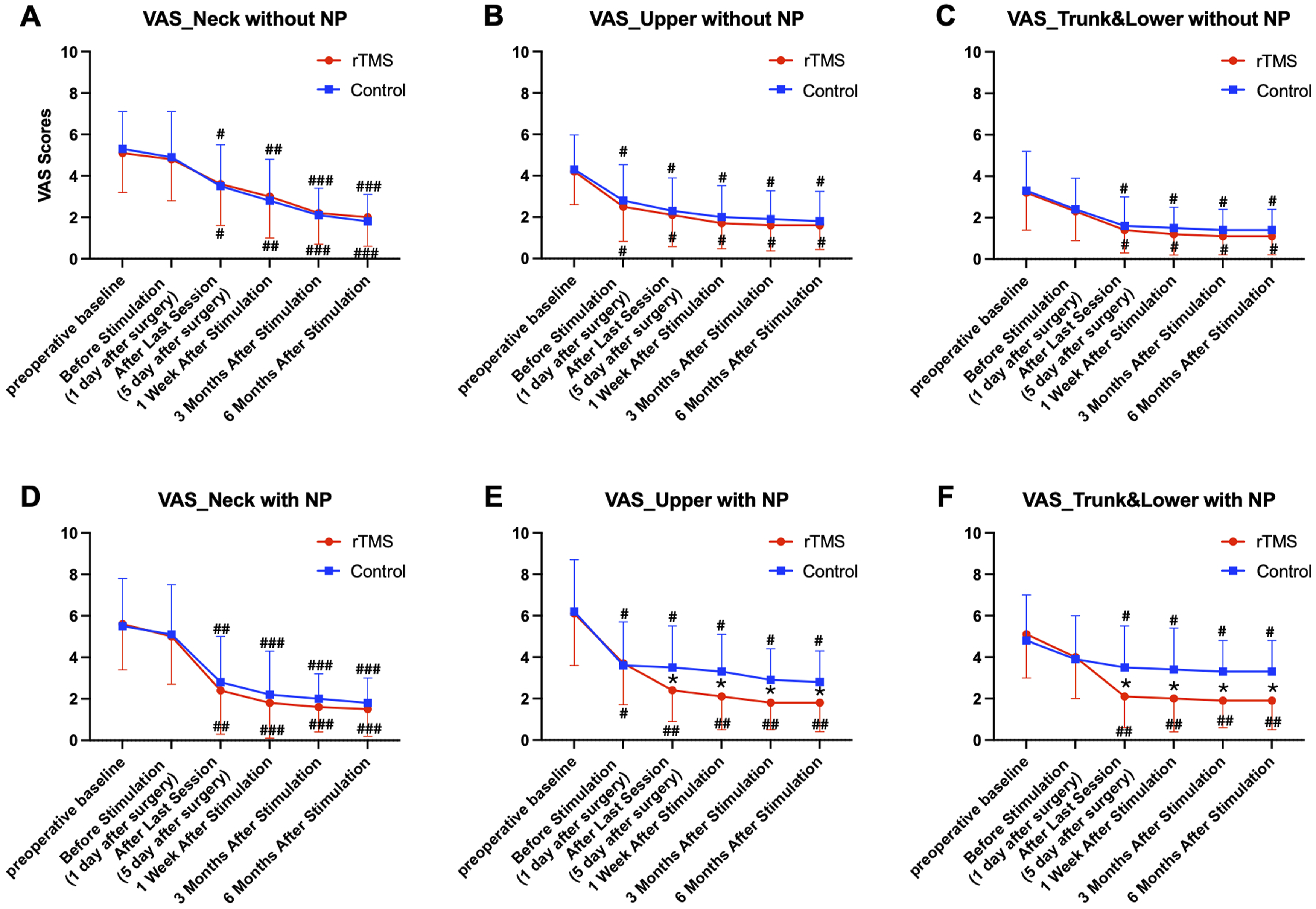
Changes in pain intensity among DCM patients with and without neuropathic pain (NP) in the control and rTMS groups. (A–C) Visual analogue scale (VAS) pain scores for the neck, upper extremities, and below-cervical regions in 25 DCM patients without NP. (D–F) VAS pain scores for corresponding body regions in 34 DCM patients with NP 1
Clinical Evaluation of Hand Dexterity
Changes in Hand Dexterity (Number of G&R Cycles) in Patients With Control or Active Stimulation
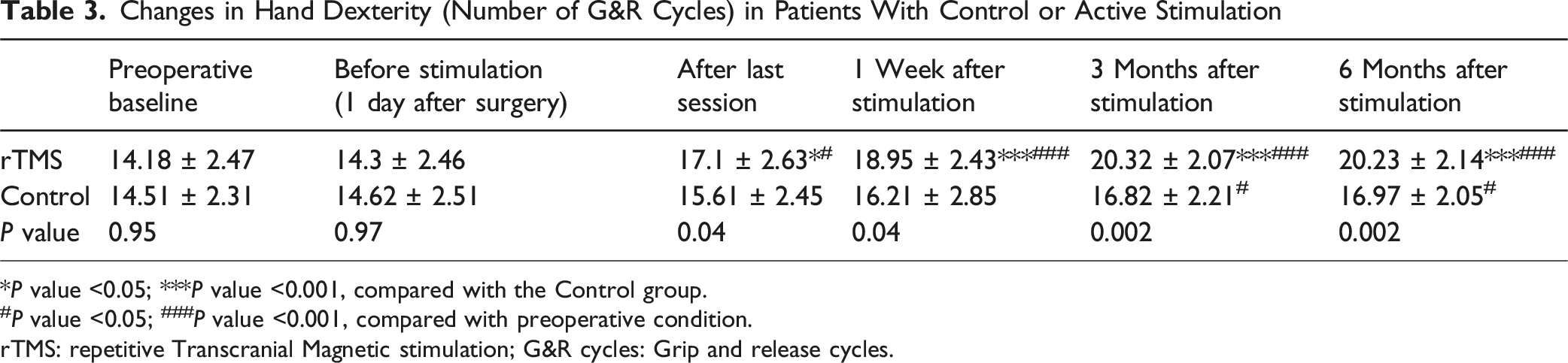
*P value <0.05; ***P value <0.001, compared with the Control group.
#P value <0.05; ###P value <0.001, compared with preoperative condition.
rTMS: repetitive Transcranial Magnetic stimulation; G&R cycles: Grip and release cycles.
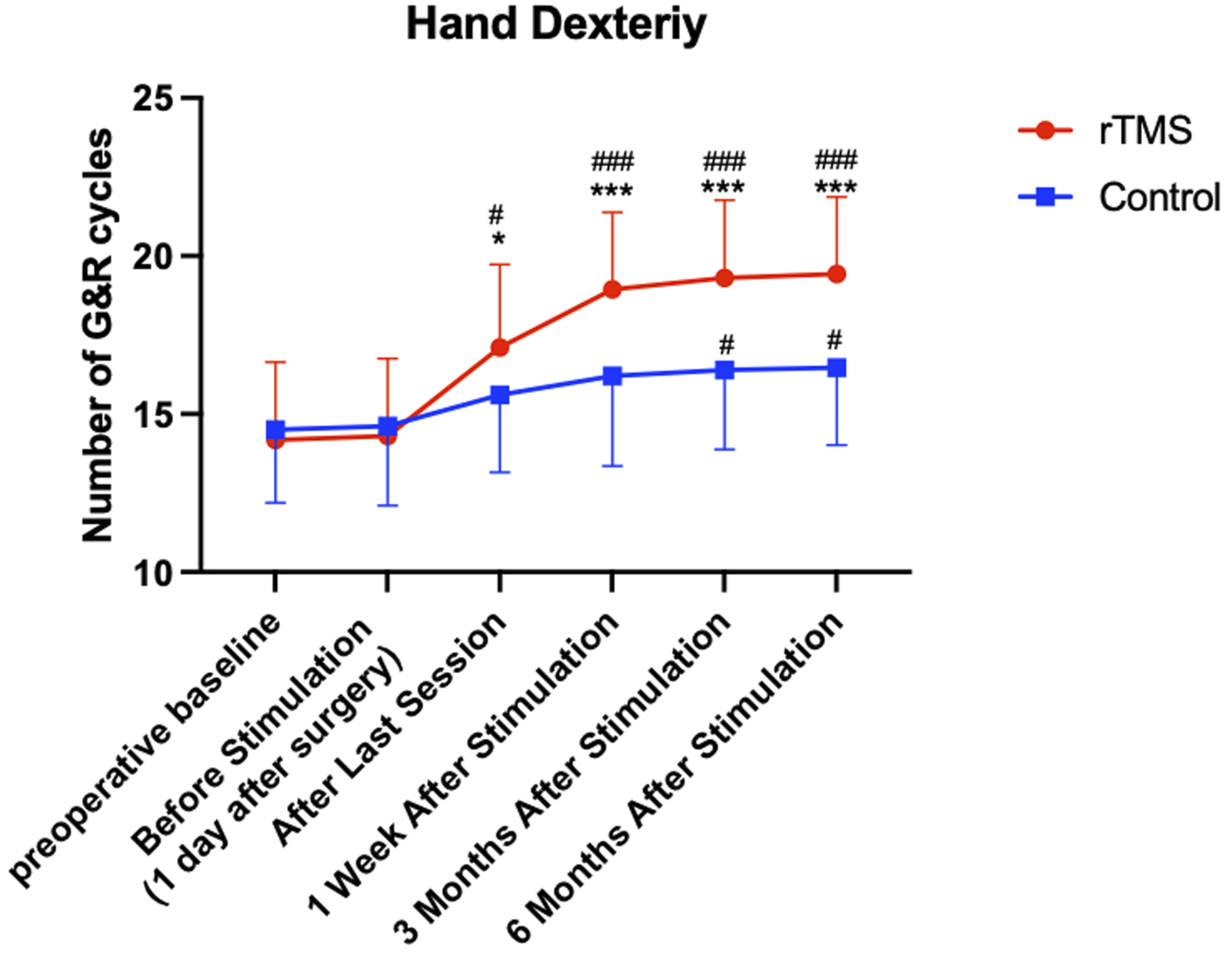
Changes in hand dexterity, expressed as the number of grip-and-release (G&R) cycles, in DCM patients from rTMS and control groups 2
mJOA Functional Recovery
mJOA Recovery in Patients With Control or Active Stimulation
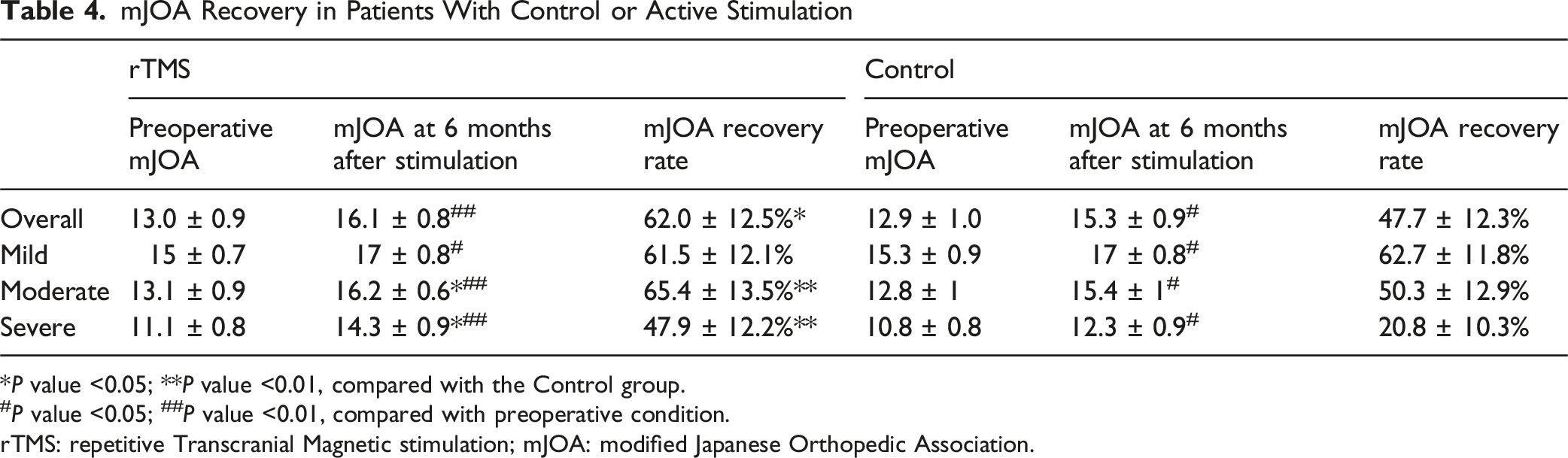
*P value <0.05; **P value <0.01, compared with the Control group.
#P value <0.05; ##P value <0.01, compared with preoperative condition.
rTMS: repetitive Transcranial Magnetic stimulation; mJOA: modified Japanese Orthopedic Association.
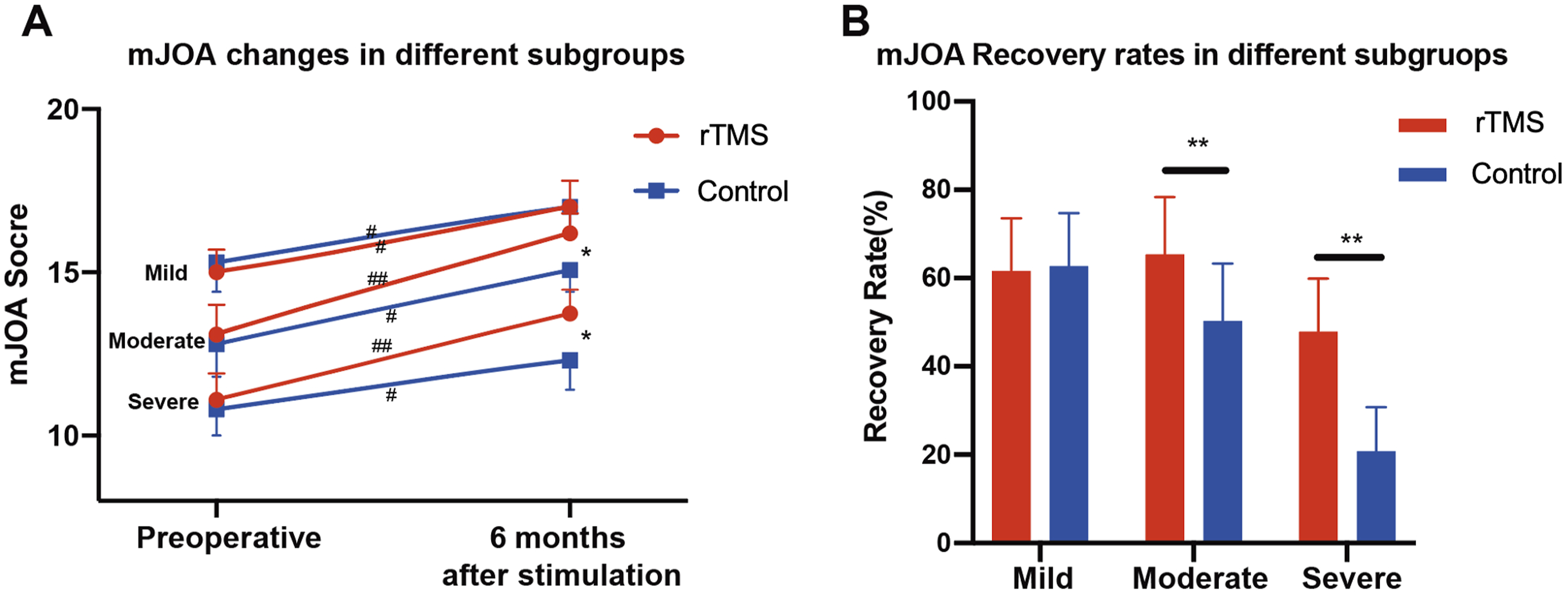
mJOA recovery in DCM patients with different baseline severity. (A) mJOA scores at preoperative and 6 months after stimulation timepoints in different severity subgroups. (B) mJOA recovery rates at 6 months follow-up in different severity subgroups 3
Neurophysiological Recordings
Mean and Standard Deviation of the Neurophysiological Data
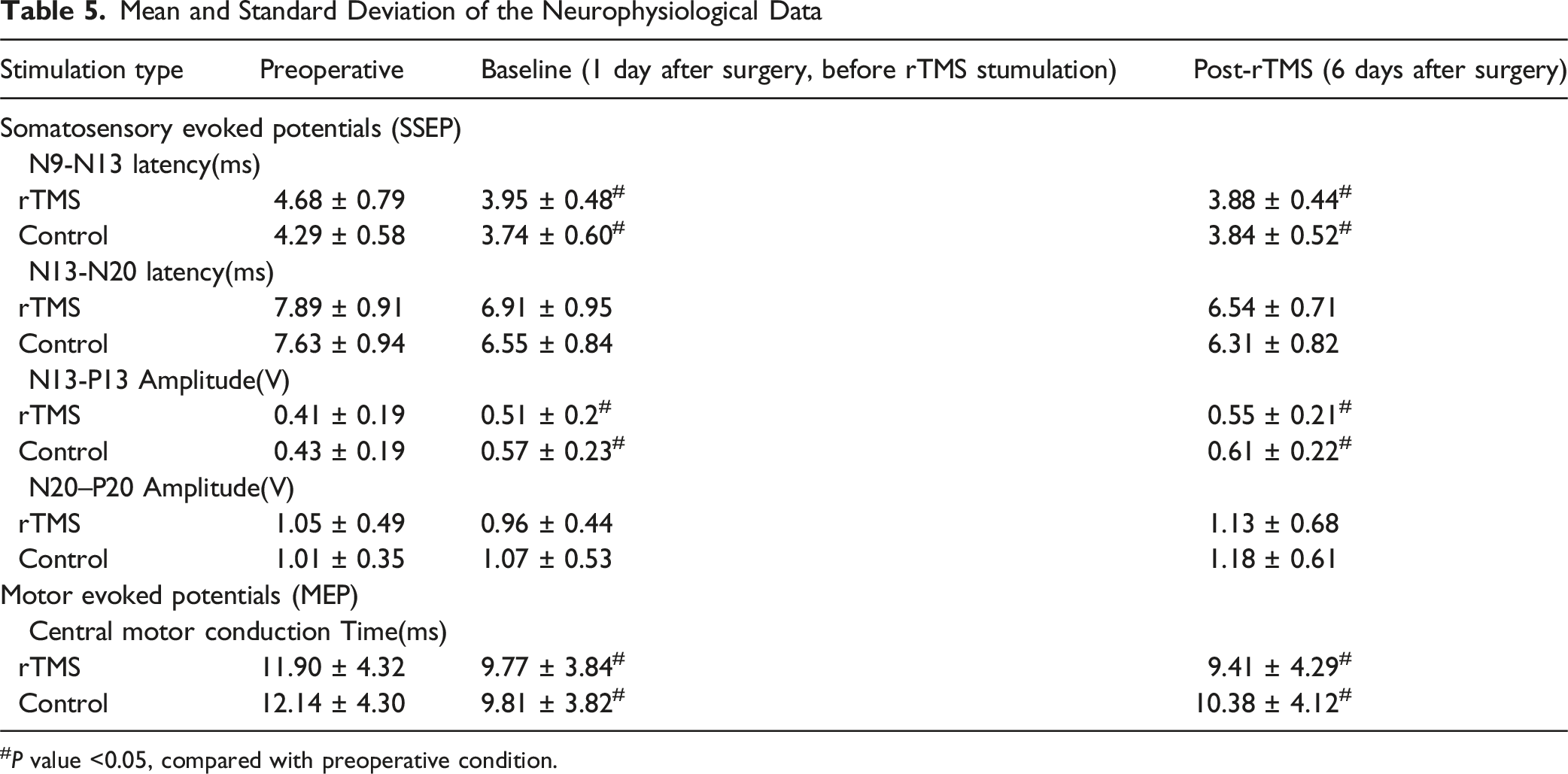
#P value <0.05, compared with preoperative condition.
Discussions
While repetitive transcranial magnetic stimulation (rTMS) has been extensively studied in the screening, diagnosis, and prognosis of DCM, this study is the first to evaluate its therapeutic potential. Our results demonstrate that post-operative rTMS was associated with reduced neuropathic pain, better hand dexterity, and favorable neurological recovery compared to control stimulation, particularly in patients with moderate-to-severe DCM (preoperative mJOA ≤14). These findings highlight rTMS as a promising adjunctive therapy for NP and sensorimotor functional rehabilitation in DCM patients.
Current treatment for DCM focuses primarily on surgical decompression, which physically alleviates spinal cord compression. However, surgeries do not always lead to full functional recovery, especially in cases with chronic and severe compression. 1 At present, evidence for physiotherapy in DCM is limited and supports its use only in mild cases as part of non-surgical management. 22 There have been no previous reviews of postoperative rehabilitation in DCM. However, promising data reported that either a long-standing spinal cord injury or a decompression surgery could affect the cortical metabolism and functional connectivity of the brain, which in turn influences postoperative outcomes.23,24 This raises the possibility that interventions such as rTMS which modulate the brain, may facilitate DCM recovery. Several mechanisms of rTMS have been reported. At the synaptic level, it can modulate synaptic structure and function, influencing long-term potentiation/depression (LTP/LTD)-like processes and altering neurotransmitter release by increasing BDNF expression. 25 At the neuronal level, high-frequency rTMS and intermittent theta burst stimulation can enhance cellular excitability and reduce inhibition, 26 which can also induce structural changes, such as increased white matter integrity and gray matter volume. 27
Our study showed rTMS was associated with significant improvement of pain recovery in post-operative DCM patients, especially in patients with NP(ND-4≥4). Pain was ranked as the highest priority for recovery, independent of baseline functional status by a previous survey of 659 DCM patients, pressing its research priority in DCM. 28 In patients with DCM, pain can be broadly categorized into 3 types. The first is neck pain, typically attributed to musculoskeletal degeneration, intervertebral disc pathology, and soft tissue strain. The second type is segmental pain in the shoulder and upper limbs, primarily resulting from cervical radiculopathy caused by direct compression of nerve roots. The third is widespread pain extending beyond the aforementioned regions, which is believed to reflect a neuropathic component related to spinal cord injury. 28 The latter 3 types of pain involve lesions in the peripheral or central nervous system, may induce central sensitization and thus meet the criteria for NP. 29 In this study, rTMS was effective in alleviating radiculopathy-related upper extremity pain as well as pain in the trunk and lower limbs among patients with NP. These results align with earlier reports on the analgesic effects of rTMS in lumbar radiculopathy or SCI.30,31 We applied a 20 Hz rTMS protocol over the M1 area contralateral to the most painful side, which has previously shown robust analgesic effects in chronic NP related to spinal cord injury 30 and other conditions resistant to conventional pharmacological treatments. 32 Our study demonstrates that, beyond its established role as a standalone therapy for NP in SCI and radiculopathy, rTMS is also effective as an adjuvant intervention following decompression surgery in DCM patients.
The analgesia induced by motor cortex rTMS may involve multiple mechanisms of action, including the activation of descending pain modulatory systems spanning from the brainstem to the spinal cord, 33 and the involvement of endogenous opioids. 34 Notably, functional MRI study have demonstrated post-operative pain relief in DCM was strongly associated with brain modulation and reorganization. 35 It is possible that the rTMS therapy modulates pathological central sensitization and alleviates neuropathic pain in post-operative DCM patients by activating the brain plasticity. Nevertheless, the rTMS treatment in our study did not have a significant effect on neck pain and segmental pain in non-NP patients. We believe this pain is primarily caused by peripheral soft tissue inflammation and nerve compression due to spondylosis, rather than central sensitization. 28 Alleviation of this pain mainly depends on the reduction of soft tissue inflammation, such as discogenic inflammation and radicular compression, achieved through surgery rather than brain modulation therapy.
For the 10s-G&R test and mJOA evaluation, our study demonstrated that the beneficial effects of rTMS on hand dexterity and mJOA persisted for up to 6 months after surgery, even though stimulation was delivered for only 5 days. Comparable long-lasting effects have also been reported in patients with stroke, traumatic brain injury36,37 and SCI. 38 Previous studies further confirmed that in DCM patients, hand dexterity, 39 gait disturbance 40 and overall neurological function measured by mJOA 41 are associated with cerebral reorganization. Therefore, we hypothesize that the long-lasting hand dexterity improvement and neurological recovery attributed to rTMS therapy could be arise from its effect on promoting cortical reorganization and neuroplasticity.
Another explanation for improved motor sensory functional performance in DCM patients is that it can alleviate muscle spasticity. 9 Muscle spasticity is a common symptom resulting from damage to the spinal cord in severe DCM patients, leading to increased muscle tone and stiffness. 1 This condition can cause involuntary muscle contractions, impairing movement, coordination, and daily functioning. 1 Current management of spasticity in DCM may involve physiotherapy, or medications like muscle relaxants. 5 In this study, we found that DCM patients also reported improved tightness sensation of the body, decrease in muscle tone in passive limb movement after the rTMS treatment. Since the rTMS directly stimulates the brain by electromagnetic impulses, it is possible that the rTMS improved the hand clumsiness symptom by stimulating the brain and facilitating its plasticity.
Moreover, our results suggest that patients with moderate-to-severe DCM may derive greater benefit from rTMS, which could be attributed to their lower baseline mJOA scores and consequently greater potential for improvement after rTMS treatment. Previous studies also reported severe DCM and SCI patients rely more heavily on cerebral neuroplastic reorganization.38,41 In contrast, patients with mild DCM often recover well following decompression alone, resulting in a ceiling effect that may limit the observable impact of rTMS.
The measurement of MEPs following TMS and SSEPs following peripheral nerve electrical stimulations are noninvasive methods to evaluate the electrophysiological functions of the corticospinal tract and dorsal column respectively.19,42 Central motor conduction time (CMCT) and somatosensory conduction time, which included N9-N13, N13-N20 in this study, are core parameters to reflect the motor and sensory transduction functions of the spinal cord, and prolonged CMCT and somatosensory conduction time have been reported to correlate with the severity of DCM.43,44 In this study, our MEP and SSEP results indicate that the central motor and sensory conduction time were not affected by the rTMS therapy, suggesting that the rTMS does not necessarily exert its therapeutic effects by acting on the lesion area of the spinal cord. These findings further suggest that postoperative rTMS may exert its rehabilitative effects by modulating the activity of the higher central nervous system.
This study has several limitations, including its retrospective design, relatively small sample size, and a 6-month follow-up period that may not fully capture long-term outcomes. Future research should adopt a prospective design with larger cohorts, longer follow-up, and outpatient-based rTMS therapy to validate and extend our findings. Another limitation is that spasticity was not quantitatively assessed, which limits our findings; future studies will incorporate standardized measures (eg, Modified Ashworth Scale) to address it.
Conclusions
In summary, our study investigated the therapeutic role of rTMS in postoperative DCM patients. Our findings suggest that the 5-day postoperative rTMS was associated with reduced neuropathic pain, better hand dexterity, and favorable neurological recovery. Our results indicate that the rTMS can be effective for DCM postoperative rehabilitation, likely by modulating the activity of higher central nervous system.
Footnotes
Ethical Considerations
This retrospective study was approved by the institutional review boards (IRB) of the First Affiliated Hospital of Sun Yat-sen University and Guangdong Provincial People’s Hospital (Trial registration number: [2024]265) on November 10th, 2024. This study utilized only de-identified, retrospective medical data. Ethical approval was obtained from the IRBs of both participating institutions, which waived the requirement for informed consent in accordance with the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations.
Author Contributions
Z. Yu and J. Chen analyzed the data, drafted and revised the manuscript. K. Lin revised the manuscript critically for important intellectual content. HG and XZ made substantial contributions to the conception and design of the study, and provided final approval of the version to be published. X. Cheng, S. Zeng and S. Zhan were involved in the acquisition of data. All authors read and approved the final manuscript.
Funding
Guangzhou Municipal Science and Technology Project (No. 2024A04J3697), and Guangdong Basic and Applied Basic Research Foundation (No. 2023A1515110141) for ZY; National Natural Science Foundation of China (No. 82201360), and Guangdong Provincial People’s Hospital Full-time High-level Talent Introduction Foundation (No. KY0120231008) for XC; National Natural Science Foundation of China (No. 82402757) and Guangdong Basic and Applied Basic Research Foundation (No. 2025A1515012393) for YY.
Declaration of conflicting interests
The authors declare that they have no competing interests.