
Abstract
Study Design
Eco-epidemiological study.
Objectives
Vertebral fractures (VFs) are a major cause of morbidity, disability, and mortality in women, with risk increasing sharply after menopause due to accelerated bone loss. However, global patterns of VF burden by menopausal status and long-term projections remain poorly characterized.
Methods
We analyzed Global Burden of Disease (GBD) 2021 data on VF incidence, prevalence, and years lived with disability (YLDs) for 204 countries from 1990-2021. Women were categorized as premenopausal (15-49 years) or postmenopausal (≥50 years). Age-standardized rates (ASRs) were calculated per 100,000 population. Temporal trends were assessed using estimated annual percentage change and joinpoint regression. Socio-demographic disparities were examined with Slope Index of Inequality and Concentration Index. Decomposition analysis quantified contributions of population growth, aging, and epidemiologic change. Bayesian age–period–cohort models projected trends to 2050.
Results
In 2021, 1.15 million VFs occurred in premenopausal women and 1.63 million in postmenopausal women, causing 50,060 and 206,652 YLDs, respectively. Absolute VF counts rose substantially since 1990, although ASRs declined in most regions. Postmenopausal women bore the highest burden, with marked geographic heterogeneity and persistent pro-poor inequality. Population growth and aging were the main drivers of increasing burden, and projections indicate that absolute VF cases will continue to rise globally through 2050 despite modest ASR declines.
Conclusions
The global burden of vertebral fractures in women is rising in absolute terms, especially among postmenopausal women. Targeted osteoporosis screening, fall-prevention programs, and equitable treatment access are needed to mitigate the projected growth.
Keywords
Introduction
Vertebral fractures (VFs) impose a substantial global health burden. These fractures arise from both high-energy trauma (commonly affecting younger individuals) and low-energy osteoporotic events in older adults. 1 In older women, diminished bone strength after menopause makes VFs particularly common and often clinically silent until complications arise. 2 Nevertheless, even a single vertebral fracture is a predictor of future fractures and chronic disability. 3 Worldwide, VFs lead to chronic back pain, reduced mobility and quality of life, and increased mortality. 4 With increasing age, the absolute number of such fractures has risen sharply, although age-standardized rates have remained stable or have declined in some regions. 5 Addressing vertebral fracture risk in women is therefore a growing public health priority.
Hormonal changes at menopause exacerbate fracture risk. 6 During the menopausal transition, estrogen levels decrease dramatically, accelerating bone loss and osteoporosis. 7 Postmenopausal women may have an annual bone loss rate of 3-5% in the first 5-10 years after menopause, markedly increasing fracture susceptibility. 8 In contrast, premenopausal women generally have greater bone density, and VFs in younger women more often result from trauma rather than fragility. However, lifestyle shifts and factors such as early menopause or iatrogenic ovarian failure increase fracture risk in younger cohorts. 9 Importantly, vertebral fracture etiology and outcomes differ before and after menopause; however, most epidemiological studies have not disaggregated women by menopausal status.
Vertebral fracture incidence and burden also vary substantially by region and development level. High-income countries (North America, Europe, Australia) report the highest age-standardized rates, 1 reflecting their aged populations and better detection. Conversely, many low- and middle-income regions are likely to underreport fractures, 1 partly due to limited screening and lower awareness. Prior relevant studies1,4,5 have evaluated the global burden of VFs across all populations but have not focused on women’s menopausal status. Moreover, regional studies suggest that fracture burdens increase with age, but systematic global comparisons by age or sociodemographic index (SDI) have been rare.
To fill these gaps, we analyzed Global Burden of Disease (GBD) 2021 data on VFs in women from 1990 through 2021, categorizing cases by age as a proxy for menopausal status. We report the incidence, prevalence and years lived with disability (YLDs) for pre- and postmenopausal age groups across regions and SDI quintiles. We also project counts to 2050 via GBD population forecasts. By emphasizing trends and disparities by menopausal status and region, our analysis highlights the growing impact of VFs in aging female populations and the need for targeted prevention strategies.
Materials and Methods
Data Source
The GBD 2021 study, the most recent iteration produced by the Institute for Health Metrics and Evaluation (IHME), provides comprehensive epidemiological estimates spanning 1990-2021. This dataset encompasses 371 diseases and injuries, alongside 88 risk factors, across 204 countries and 21 regions.10,11 The GBD methodology synthesizes diverse data sources, including hospital records, emergency department visits, insurance claims, population surveys, and vital registration systems. 12 Detailed protocols for data processing, modeling strategies, and uncertainty estimation are documented in the supplemental materials.
Disease Definition
Within the GBD framework, VFs—encompassing cervical, thoracic, and lumbar spine injuries—were identified via the International Classification of Diseases (ICD) codes: ICD-9 (805.0-806.9) and ICD-10 (S12.0-S12.9, S22.0-S22.1, S32.0). This standardized classification enabled systematic data aggregation and comparative analysis. We extracted incidence, prevalence, and YLD estimates for VFs directly from the GBD 2021 database. These metrics quantify both individual quality-of-life impairment and population-level health burdens.
The female population was stratified into seventeen 5-year age groups: 15-19, 20-24, 25-29, 30-34, 35-39, 40-44, 45-49, 50-54, 55-59, 60-64, 65-69, 70-74, 75-79, 80-84, 85-89, 90-94, and ≥95 years. Menopausal status was defined operationally: premenopausal (ages 15-49vyears) and postmenopausal (age ≥50 years), which was consistent with previous GBD-based work and with widely used epidemiological conventions for defining postmenopausal age. 13
Data Collection and Processing
The primary outcomes included absolute counts and age-standardized rates (ASRs) with 95% uncertainty intervals (UIs) for incidence, prevalence, and YLDs. The supplemental materials detail these metric definitions. To account for demographic shifts, we utilized age-standardized incidence rates (ASIRs), age-standardized prevalence rates (ASPRs), and age-standardized YLD rates (ASYRs), which were calculated as follows
13
:
Statistical Analysis
We compared absolute numbers and ASRs (with 95% UI) for vertebral fracture incidence, incidence, and YLDs between pre- and postmenopausal women from 1990-2021. Temporal trends were quantified via estimated annual percentage changes (EAPCs). Joinpoint regression analysis (Joinpoint Regression Program, Version 5.4.0.0; National Cancer Institute, USA) identified significant inflection points in trends, reporting average annual percentage changes (AAPCs) with 95% confidence intervals (CIs). 15 In practical terms, we first summarized absolute numbers and age-standardized incidence, prevalence, and YLD rates for vertebral fractures by menopausal group, year, region, and country, and then used joinpoint regression to describe average annual percentage changes in these rates over time. We further examined the underlying causes attributed to VFs, primarily comprising Level 3 causes within the GBD hierarchy. To improve clarity, extremely rare or conceptually implausible causes (drowning; environmental heat and cold exposure; fire, heat, and hot substances; poisonings) have been grouped into an aggregated “others” category.
Spline regression models characterized the association between the SDI and ASRs across 21 GBD regions (1990-2021). SDI—a composite metric (0-1 scale) derived from lag-distributed income per capita, mean educational attainment (≥15 years), and total fertility rate (<25 years)—reflects regional development status and is strongly correlated with health outcomes. 16 Pearson correlation coefficients were used to assess the SDI-ASR relationships. Frontier analysis defined the minimum achievable burden given development levels. These spline models treated SDI as a continuous measure of development and allowed us to visualize how vertebral fracture rates change across the full development spectrum, rather than simply comparing arbitrary SDI categories.
Health inequalities were measured via the slope index of inequality (SII) and the concentration index for YLDs. 17 Absolute inequality was defined as the mean value of a health indicator in one population group subtracted from the mean value of that health indicator in another population group. 17 The SII (absolute inequality) represents the difference in the mean ASR between extremes of the SDI distribution and is obtained by regressing country-level ASRs against their relative SDI rank. The concentration index (relative inequality, range: −1-1) was computed via Lorenz curve integration, plotting the cumulative YLD proportion against the cumulative population ranked by the SDI. Values of zero indicate no inequality; larger absolute values denote greater disparity. The slope index of inequality estimates the absolute difference in vertebral fracture burden between the hypothetical lowest- and highest-SDI countries, whereas the concentration index summarizes whether YLDs are disproportionately concentrated in poorer vs richer countries.
Decomposition analysis quantified the distinct contributions of population growth, aging, and epidemiological changes to temporal trends in vertebral fracture burden among pre- and postmenopausal women, while other factors remained constant. 18 This methodology isolated the influence of each factor on the observed variations in incidence and YLD. The net effect of each factor on the overall change in incidence or YLD is represented visually via dot plots. Positive values denote an increase in burden attributable to the factor, whereas negative values indicate a mitigating effect. This decomposition separates the impact of demographic changes (population growth and aging) from changes in age-specific incidence and YLD rates, helping to clarify whether rising case numbers are primarily driven by population dynamics or by worsening epidemiology.
The projections to 2050 for ASIR and ASYR in both menopausal groups utilized a Bayesian Age-Period-Cohort (BAPC) model fitted via Integrated Nested Laplace Approximation (INLA), 19 implemented in the R packages “BAPC” (version 0.0.36) and “INLA” (version 25.06.07). In brief, the Bayesian age–period–cohort models borrow information across age groups, calendar periods, and birth cohorts to project future age-standardized incidence and YLD rates under a continuation of recent trends, providing posterior means and 95% credible intervals for projected rates.
All analyses and visualizations employed R software (v4.5.1) and joinpoint. Statistical significance was defined as two-sided P < 0.05. The methodological details are expanded in the supplemental data.
Ethics Statement
The GBD 2021 followed the Guidelines for Accurate and Transparent Health Estimates Reporting statement 20 and was performed by the Institute for Health Metrics and Evaluation (IHME) using anonymous data and public accessibility 21 ; therefore, no ethics approval and informed consent were required.
Patient and Public Involvement Statement
No patients or the general public were involved in the analysis.
Results
Spatiotemporal Patterns of Global Vertebral Fracture Burden in Pre- and Postmenopausal Women
Estimated Numbers of Incidences Prevalence and YLDs of Vertebral Fractures in Pre-and Post-menopausal Women in 1990 and 2021
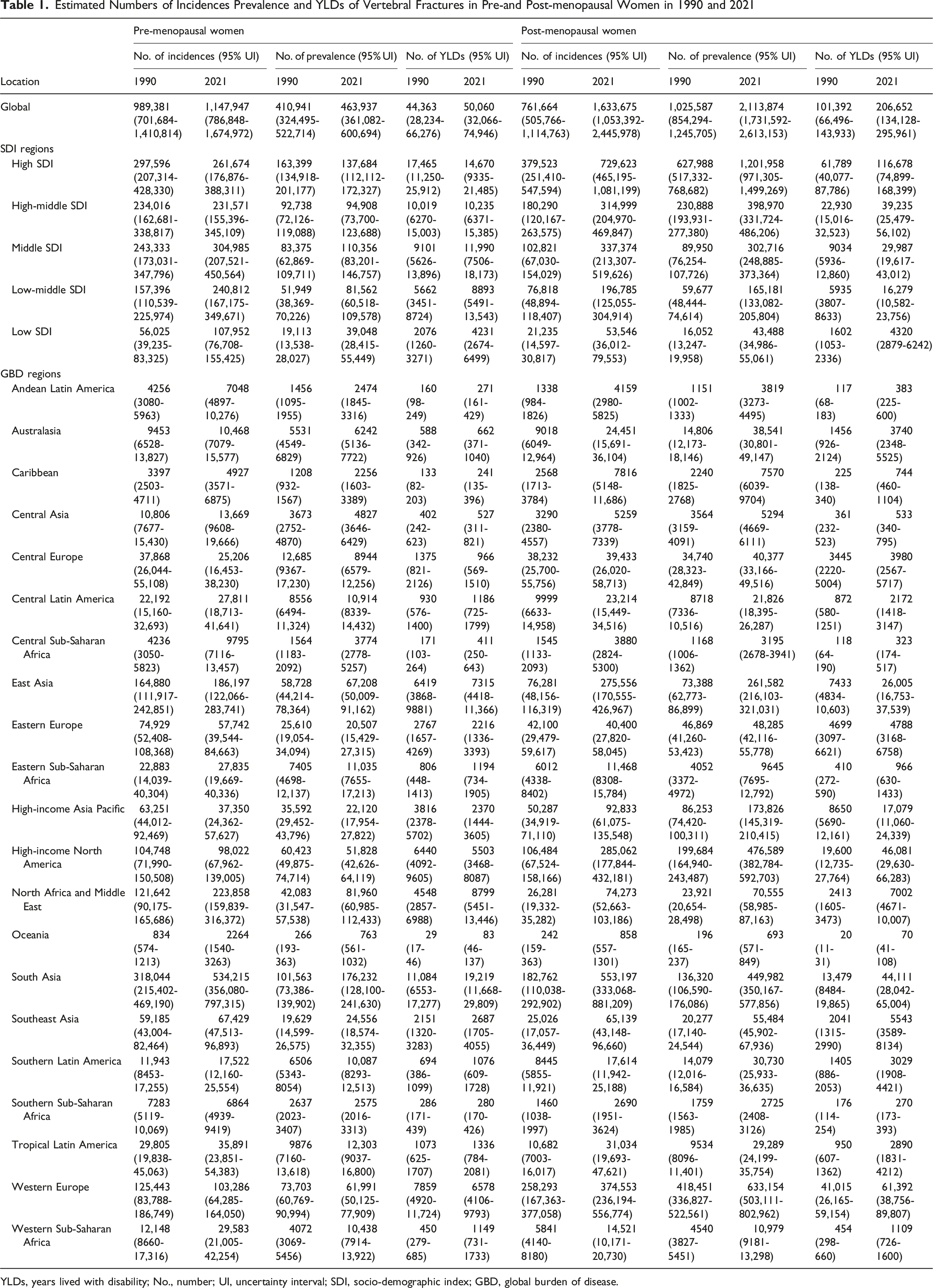
YLDs, years lived with disability; No., number; UI, uncertainty interval; SDI, socio-demographic index; GBD, global burden of disease.
ASIRs (per 100 000), ASPRs (per 100 000), ASYRs (per 100000) and AAPCs (%) of VFs in Pre- and Post-menopausal Women, 1990-2021
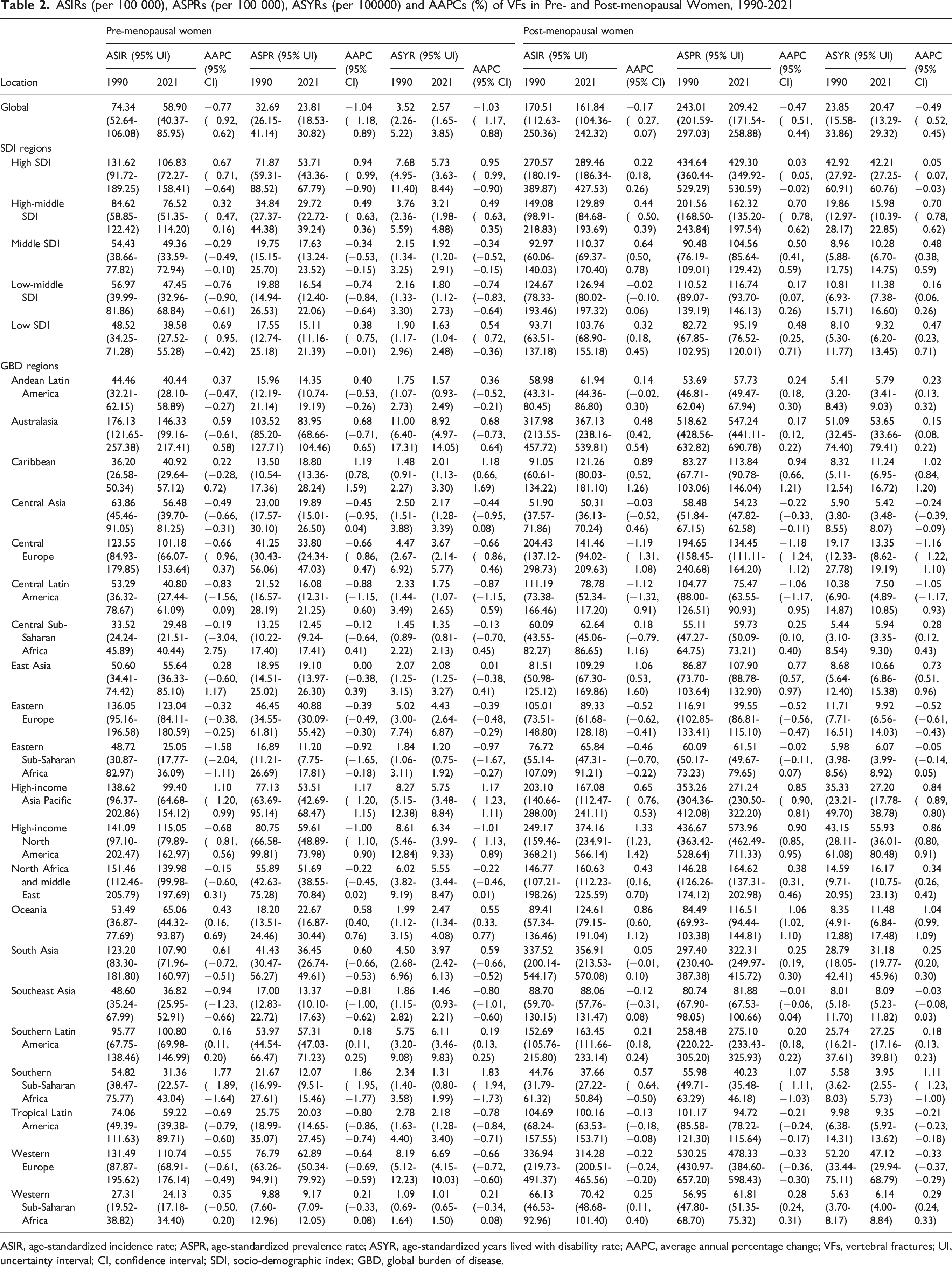
ASIR, age-standardized incidence rate; ASPR, age-standardized prevalence rate; ASYR, age-standardized years lived with disability rate; AAPC, average annual percentage change; VFs, vertebral fractures; UI, uncertainty interval; CI, confidence interval; SDI, socio-demographic index; GBD, global burden of disease.
From 1990-2021, the ASIRs, ASPRs, and ASYRs of VFs consistently decreased across all SDI regions among premenopausal women. Conversely, among postmenopausal women during the same period, these three metrics demonstrated significant decreasing trends only in high–middle-SDI regions but showed increasing trends or nonsignificant changes in other SDI regions (Table 2).
Joinpoint regression analysis revealed temporal trends in the ASIR, ASPR, and ASYR for VFs among women with different menopausal statuses globally from 1990-2021 (Figure 1, Table S2). Significant inflection points in the ASIR trend for postmenopausal women occurred in 1995, 1999, and 2005, whereas notable changes for premenopausal women were identified in 1999 and 2015 (Figure 1). Decreasing ASIR trends for postmenopausal women were observed from 1990-1995 and 2000-2021, whereas an increasing trend occurred from 1996-1999 (Figure 1). In contrast, the ASIR consistently decreased across all periods for premenopausal women. Significant shifts in the ASPR for postmenopausal women occurred in 1995, 2000, 2005, 2010, and 2017, whereas substantial changes in premenopausal women were noted in 1999, 2005, 2008, and 2016 (Figure 1). Decreasing ASPR trends for postmenopausal women were observed from 1990-1995 and 2001-2021, in contrast with an increasing trend from 1996-2000 (Figure 1). Like the ASIR, the ASPR consistently decreased across all periods for premenopausal women. Furthermore, the significant changes and temporal trends in the ASYR followed a comparable pattern in both menopausal groups (Figure 1). Joinpoint regression analysis of global ASIRs (A), ASPRs (B), and ASYRs (C) for vertebral fractures among premenopausal and postmenopausal women from 1990 to 2021. Each panel shows separate trend lines for premenopausal (blue) and postmenopausal (red) women fitted with a multiple joinpoint regression model. Circles denote observed age-standardized rates, and numbers along the trend lines indicate the APC for each segment; asterisks denote APC values that are statistically significant at P < 0.05. Vertical gray lines mark the joinpoint years. ASIR, age-standardized incidence rate; ASPR, age-standardized prevalence rate; ASYR, age-standardized years-lived-with-disability rate; APC, annual percentage change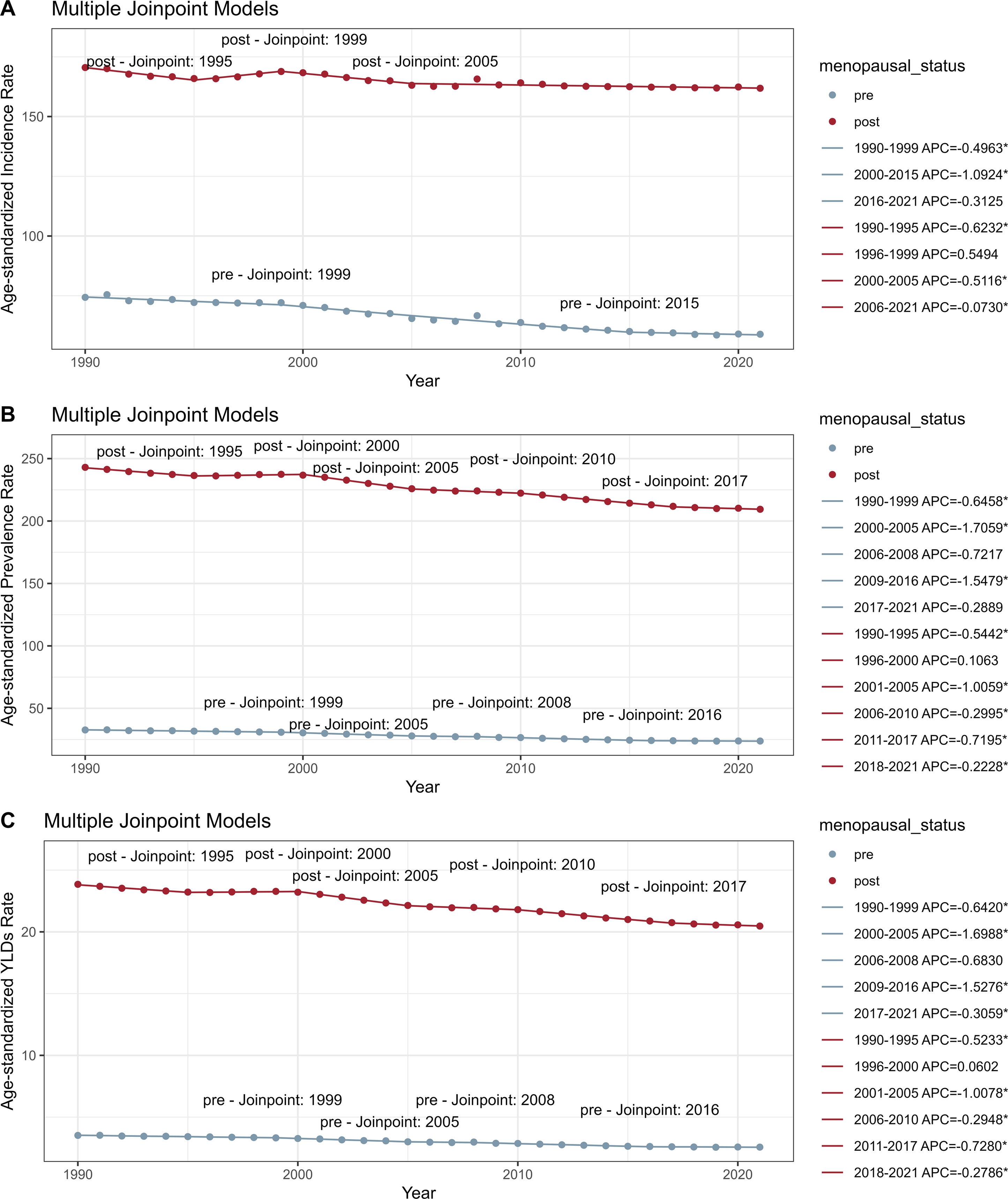
Significant geographical disparities existed in the VF burden between pre- and postmenopausal women (Figure 2). In 2021, the five countries with the highest ASIRs for VFs among premenopausal women were the Solomon Islands, Andorra, New Zealand, Belgium, and Saudi Arabia, whereas the lowest ASIRs were observed in Malawi, Gambia, Uganda, Senegal, and Zimbabwe. Among postmenopausal women, the highest ASIRs occurred in Andorra, Belgium, Greenland, the Netherlands, and Switzerland, and the lowest occurred in Bangladesh, Kiribati, Turkmenistan, Mauritius, and South Africa. For ASYR in premenopausal women, the highest rates were in New Zealand, Andorra, Australia, Finland, and Belgium, and the lowest rates were in Malawi, Gambia, Senegal, Kenya, and Zimbabwe. Among postmenopausal women, the highest ASYRs were in Andorra, Belgium, Greenland, Switzerland, and France, and the lowest were in Kiribati, Bangladesh, Mauritius, Turkmenistan, and Seychelles (Figure 2, Table S3). Geographic patterns and temporal changes in vertebral fracture burden in premenopausal and postmenopausal women. Panels A–B and D–E map ASIRs, panels G–H and J–K map ASYRs, and panels C, F, I and L map EAPCs for vertebral fractures in premenopausal (A–C, G–I) and postmenopausal (D–F, J–L) women across 204 countries and territories. For each group, the maps for 1990 (left column) and 2021 (middle column) illustrate how absolute rates have changed over time, while the EAPC maps summarize the direction and magnitude of trends. Warmer colors (red) denote higher ASIRs or ASYRs or larger positive EAPCs, whereas cooler colors (blue) denote negative EAPCs. Color bar scales indicate the exact range of values for each panel. ASIR, age-standardized incidence rate; ASYR, age-standardized years-lived-with-disability rate; EAPC, estimated annual percentage change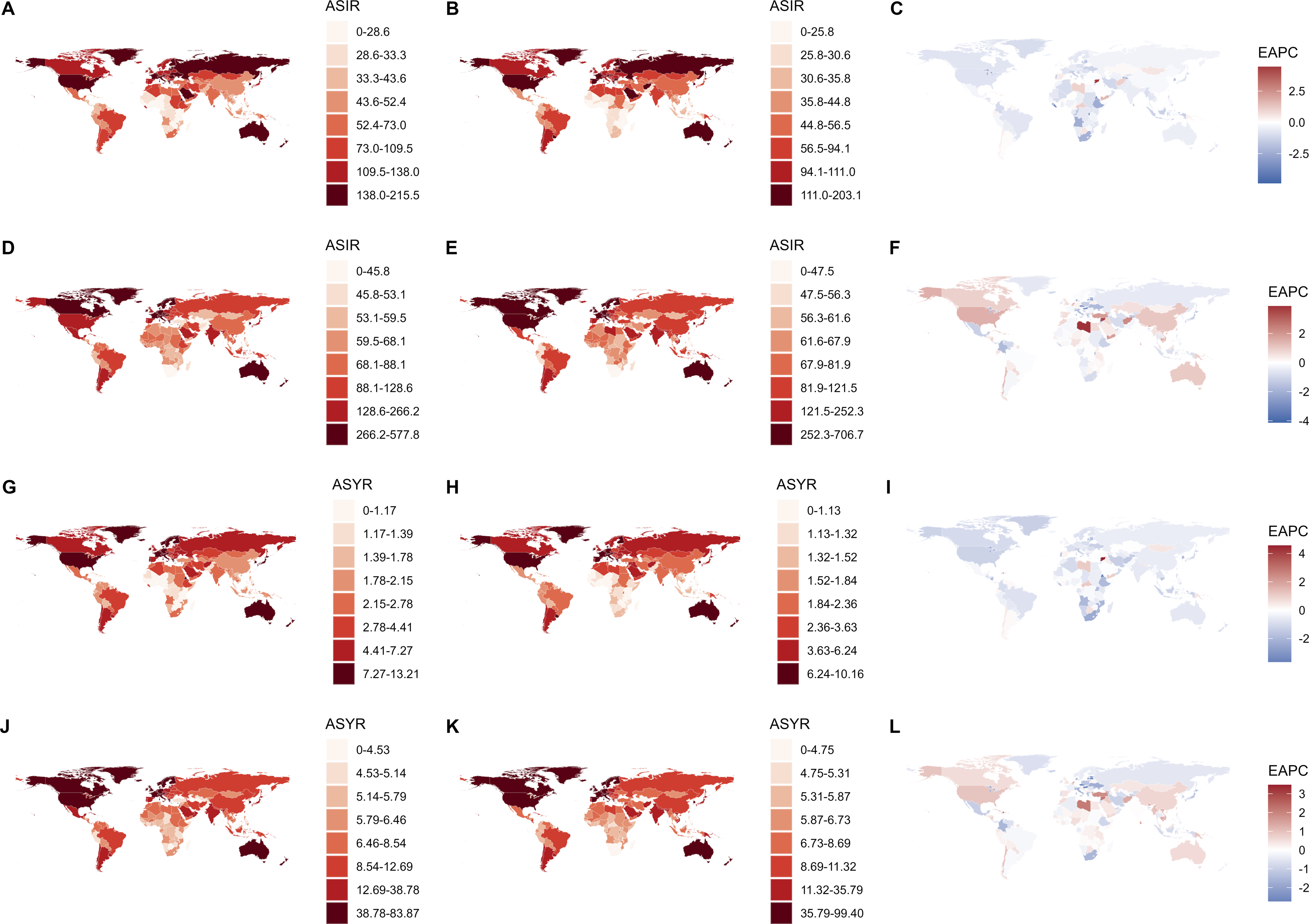
From 1990-2021, the fastest increase in the ASIR among premenopausal women occurred in the Syrian Arab Republic [EAPC: 4.44 (95% CI 2.76, 6.15)], whereas the steepest decline was observed in Burundi [EAPC: −4.87 (95% CI -7.35, −2.32)]. Among postmenopausal women, Libya presented the most rapid increase in the ASIR [EAPC 3.88 (95% CI 3.11, 4.66)], and Lebanon presented the sharpest decrease [EAPC -4.12 (95% CI -5.1, −3.13)]. For ASYR trends in premenopausal women, the Syrian Arab Republic experienced the fastest growth [EAPC: 4.56 (95% CI: 3.36, 5.77)], and Eritrea demonstrated the most rapid decline [EAPC: −3.65 (95% CI: −4.18, −3.12)]. Among postmenopausal women, Haiti had the highest ASYR increase [EAPC 3.47 (95% CI 2.27, 4.68)], whereas Latvia presented the steepest decrease [EAPC -2.73 (95% CI -2.99, −2.46)] (Figure 2, Table S4).
Causes of Vertebral Fractures in Pre- and Postmenopausal Women
The GBD data indicated that VFs in both menopausal groups stemmed from multiple causes (Figure 3). Falls constituted the primary cause globally and across all SDI regions in 2021, with their proportional contribution increasing since 1990. Road injuries, exposure to mechanical forces, and interpersonal violence are also common etiologies. Notably, in low-SDI regions, conflict and terrorism represented significant causes of VFs among premenopausal women, although their proportional contributions decreased between 1990 and 2021. Causes of vertebral fractures in premenopausal and postmenopausal women. Horizontal stacked bar charts show the proportional contribution of major external causes (eg, falls, road injuries, exposure to mechanical forces) to the total vertebral fracture burden in 1990 and 2021 at the global level and across Socio-Demographic Index (SDI) quintiles. Separate panels compare premenopausal (right) and postmenopausal (left) women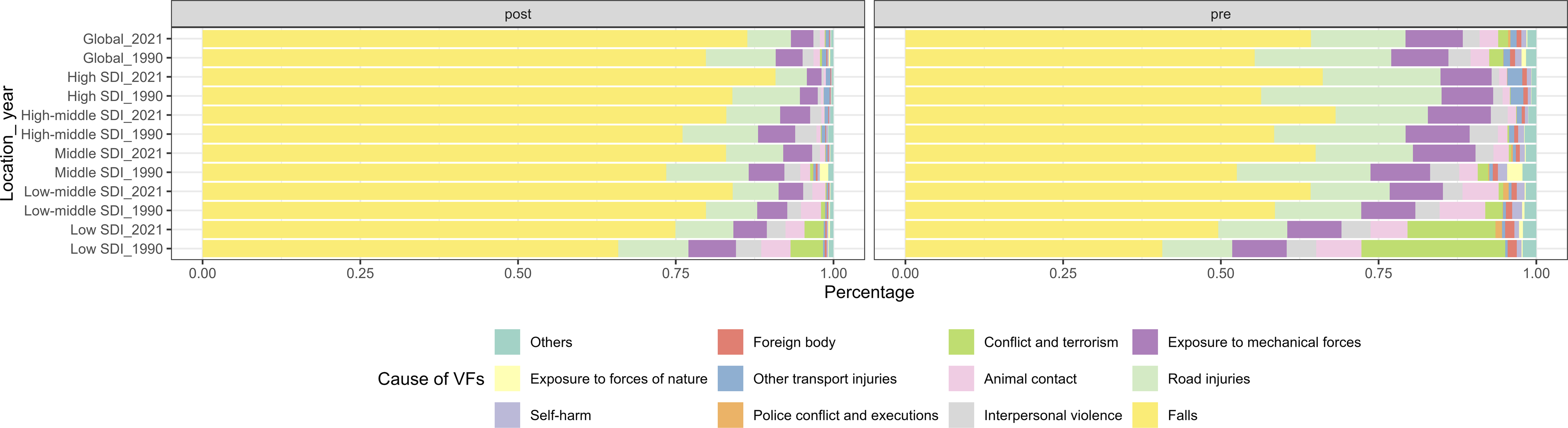
Correlation and Frontier Analysis
Across 21 GBD regions, significant positive correlations were identified between the SDI and ASIRs (premenopausal: ρ = 0.502, P < 0.001; postmenopausal: ρ = 0.393, P < 0.001), ASPRs (P premenopausal: ρ = 0.621, P < 0.001; postmenopausal: ρ = 0.507, P < 0.001), and ASYRs (P premenopausal: ρ = 0.624, P < 0.001; postmenopausal: ρ = 0.516, P < 0.001) (Figure S2). However, among premenopausal women, the ASRs tended to decrease when the SDI exceeded 0.8, whereas the ASRs continued to increase in postmenopausal women with higher SDI values.
Globally, the ASRs for VFs in both menopausal groups across 204 countries and territories in 2021 increased with increasing SDI, particularly after the SDI reached 0.7 (Figure S3). Spearman’s correlation analysis confirmed positive correlations between the SDI and ASIRs (premenopausal: ρ = 0.708, P < 0.001; postmenopausal: ρ = 0.464, P < 0.001), ASPRs (P premenopausal: ρ = 0.654, P < 0.001; postmenopausal: ρ = 0.507, P < 0.001), and ASYRs (P premenopausal: ρ = 0.662, P < 0.001; postmenopausal: ρ = 0.508, P < 0.001) (Figure S3).
Frontier analysis quantified the gap between the observed ASYRs and the theoretical minimum achievable burden across 204 countries and territories, revealing temporal trends (Figure S4). Among high-SDI countries, ASYRs exhibited a parabolic relationship with the SDI. The analysis identified the top 10 countries with the greatest potential for reducing VF burden in premenopausal (New Zealand, Andorra, Australia, Finland, Belgium, Switzerland, France, Greenland, Cyprus, Spain) and postmenopausal (Andorra, Belgium, Greenland, Switzerland, France, Netherlands, Finland, USA, Norway, Australia) women (Figure S4, Table S5). These countries presented higher ASYRs than expected given their sociodemographic conditions. Additionally, we highlighted five countries/territories in low-SDI regions with the smallest efficiency gaps (Figure S4).
Health Inequality Across Countries and Regions
Given the correlation between the SDI and ASYRs, we further assessed health inequality across 204 countries via the SII and concentration index (Figure 4). For ASYRs in premenopausal women, the SII decreased from 3.8589 (95% CI: 3.0312-4.6866) in 1990 to 3.3582 (95% CI: 2.6873-4.0292) in 2021, whereas the CI changed from −0.2623 to −0.1543. Similarly, among postmenopausal women, the SII decreased from 26.3644 (95% CI: 21.5099-31.2188) in 1990 to 15.2029 (95% CI: 11.9807—18.4250) in 2021, and the CI changed from −0.5710 to −0.4869. Consequently, while the VF burden demonstrated persistent pro-poor inequality (disproportionately affecting low-SDI regions) in both menopausal groups, the magnitude of this socioeconomic health inequality improved toward greater equity between 1990 and 2021. Socioeconomic inequalities in the YLD burden of vertebral fractures among premenopausal (A–B) and postmenopausal (C–D) women worldwide in 1990 and 2021. Panel A and panel C show the SII scatter plots: each point represents a country with marker size proportional to population in 2021, the x-axis gives the relative rank by SDI, and the y-axis shows the age-standardized YLD rate (per 100000). Solid lines represent the fitted regression, and the dashed lines mark the global average YLD rate. The SII values and their 95 % uncertainty intervals for 1990 and 2021 are annotated on the plots. Panels B and D depict concentration curves: the orange diagonal line indicates perfect equality, and the colored curves show the cumulative share of YLDs vs the cumulative share of population ranked by SDI for 1990 (blue) and 2021 (red); the CI values are reported on each plot. Negative CI values indicate that the YLD burden is disproportionately concentrated in lower-SDI countries. SII, slope index of inequality; CI, concentration index; YLD, years lived with disability; SDI, socio-demographic index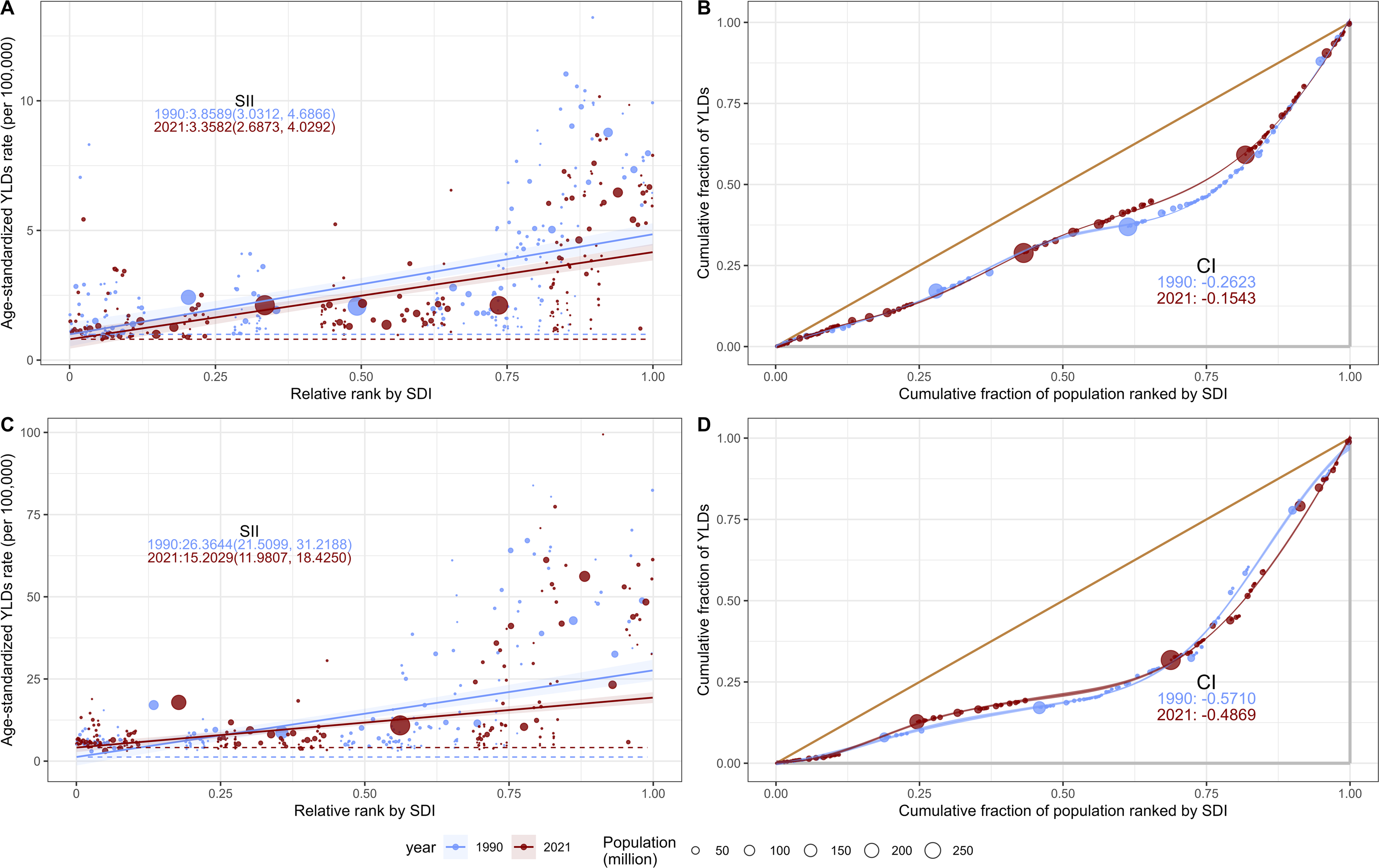
Decomposition Analysis of Vertebral Fractures
Decomposition analysis quantified the contributions of population growth, aging, and epidemiological changes to trends in VF incidence and YLDs over three decades (Table S6 and Figure 5). Population growth has emerged as the predominant driver of increasing incidence rates and YLDs in both menopausal groups across all SDI regions, despite aging being a well-established risk factor for osteoporosis-related fractures.
22
Epidemiological changes constitute the second most influential factor in most regions. Notably, epidemiological changes have mitigated VF incidence and YLDs among premenopausal women globally, whereas aging has contributed to increasing incidence rates and YLDs among postmenopausal women in all regions. Decomposition of changes in vertebral fracture incidence and YLDs from 1990 to 2021. Panels A and B decompose the absolute change in incident cases in premenopausal (A) and postmenopausal (B) women at the global level and across five SDI quintiles; panels C and D do the same for YLDs. For each location, colored bars quantify the contributions of population growth (orange), population aging (red), and epidemiological changes (blue) to the overall change, and the black dots indicate the observed net change. Positive values reflect increases and negative values reflect decreases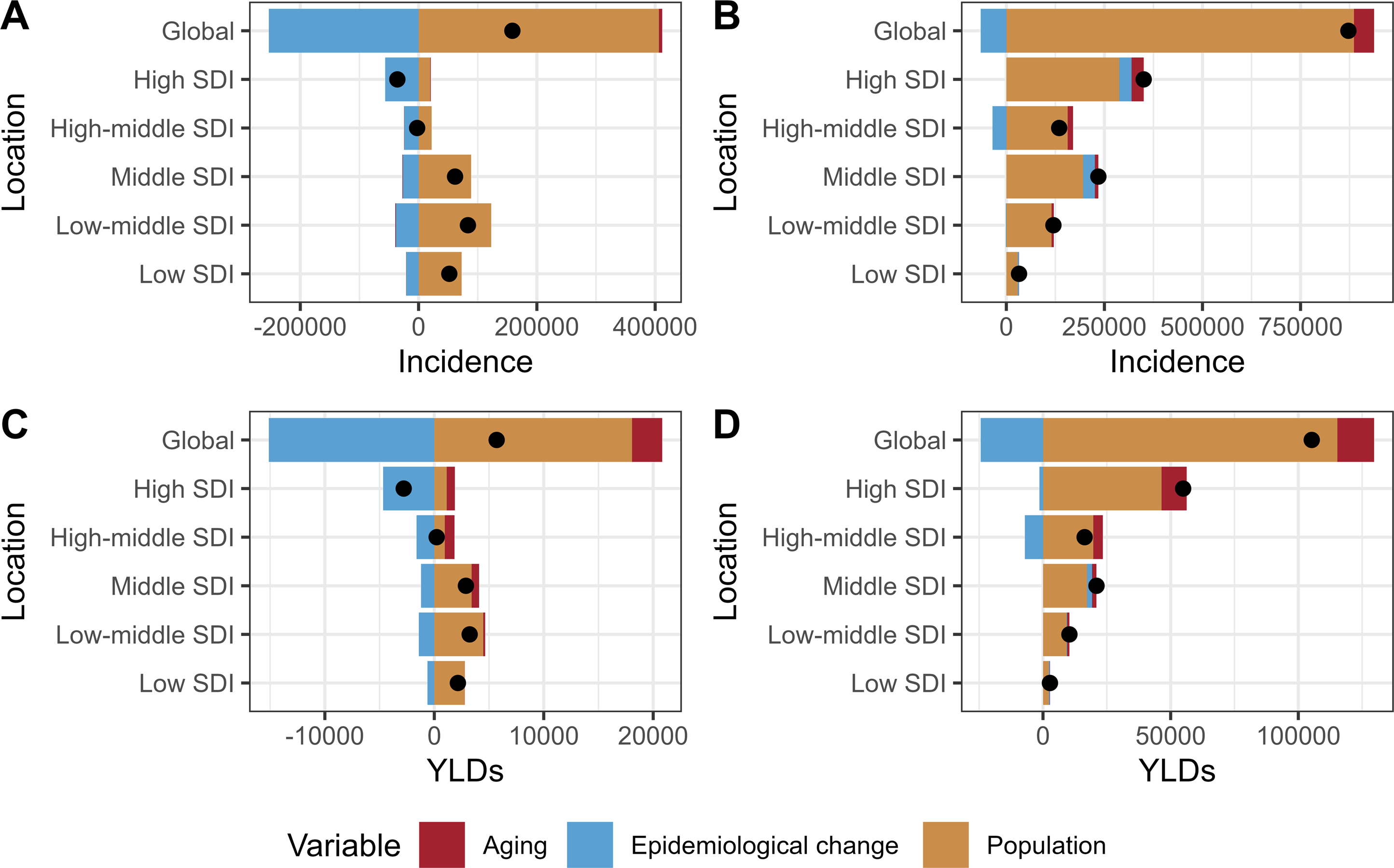
Projected Vertebral Fracture Burden in Pre- and Postmenopausal Women by 2050
BAPC modeling projected global trends in the ASIRs and ASYRs of VFs to 2050 (Figure 6, Table S7). Among postmenopausal women, ASIRs are projected to decrease from 161.83 (95% CI 159.10-164.56) in 2022 to 146.92 (95% CI 16.31-277.52) in 2050, with ASYRs showing a similar decline from 20.41 (95% CI 20.10-20.72) to 17.81 (95% CI 4.42-31.20). However, among premenopausal women, both ASIRs and ASYRs are projected to exhibit only minor fluctuations between 2022 and 2050, which may be associated with the relatively low baseline burden of VFs in this group and the limited potential for further reduction. Observed and projected ASIRs and ASYRs for vertebral fractures among premenopausal (A, B) and postmenopausal (C, D) women worldwide. Black dots represent observed age-standardized rates from 1990 to 2021; the dashed vertical line marks 2021, after which projections (2022-2050) are derived from Bayesian age–period–cohort models. Blue shaded bands around the projection lines show the 95 % credible intervals, with darker shading indicating higher posterior density. ASIR, age-standardized incidence rate; ASYR, age-standardized years-lived-with-disability rate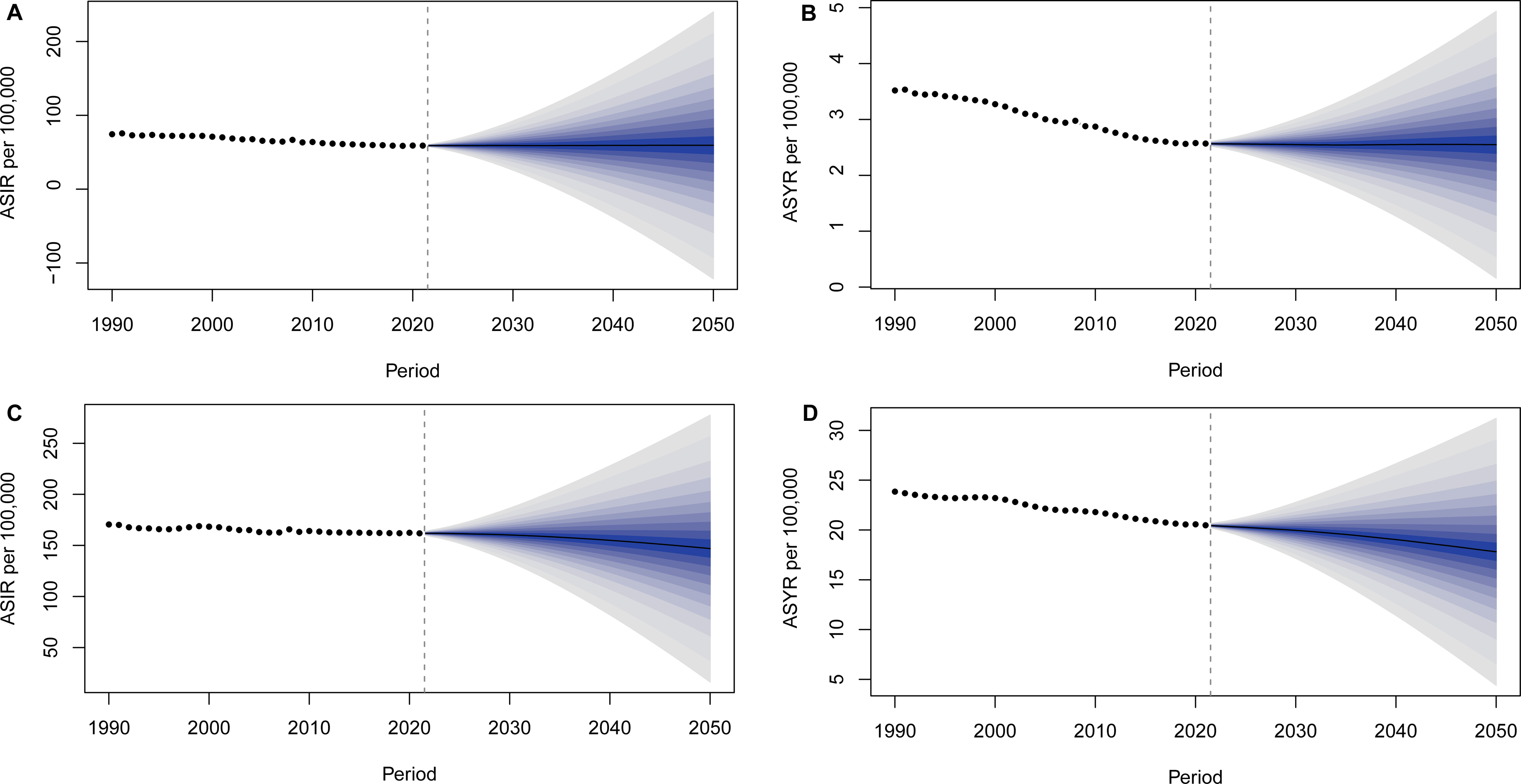
Discussion
This comprehensive analysis of GBD data highlights VFs as a major and growing source of disability in women, with an especially large burden after menopause. We found that absolute counts of incident and prevalent VFs rose globally from 1990-2021 in both younger (15-49 years) and older (≥50 years) women, driven primarily by population growth and aging. In contrast, age-standardized VF incidence, incidence, and YLD rates generally declined or plateaued over this period. These patterns align with other GBD studies showing modest declines in VF rates.1,4,5 For perspective, approximately 200 million women worldwide have osteoporosis, and epidemiological analyses estimate that approximately one-third of women aged ≥50 years will sustain osteoporotic fractures in their remaining lifetimes. 23
The stark contrast in VF burden between pre- and postmenopausal women is biologically plausible. Menopause results in a rapid loss of bone density, which markedly increases the risk of fragility fractures. 6 In contrast, premenopausal women typically maintain higher peak bone mass, and their VFs are more often due to high-energy trauma. Clinical trial evidence illustrates these effects; for example, the Women’s Health Initiative demonstrated that estrogen plus progestin therapy in older women increased bone mineral density and reduced fracture risk by approximately 24%. 24 This finding is consistent with our results showing a much higher VF incidence in postmenopausal women than in younger women. Although our primary focus was on women because of the clear mechanistic link between menopause-associated estrogen deficiency and vertebral fracture risk, vertebral fractures in older men are also common, underdiagnosed, and undertreated; future Global Burden of Disease analyses should explicitly quantify the burden among men aged 70 years and older and explore sex-specific determinants and care gaps.
The temporal trends also varied by region and development level. In high-income (high-SDI) countries, age-standardized VF incidence and prevalence rates declined significantly between 1990 and 2021, likely reflecting improved osteoporosis case finding and prevention (eg, DXA screening, calcium/vitamin D supplementation, and antiresorptive therapies).25-27 Indeed, clinical trials of bisphosphonates have shown approximately 40-50% reductions in new vertebral fractures, 28 which likely contributed to the decreasing trends observed. In contrast, many middle- and low-SDI regions showed smaller declines or even increases in VF rates, perhaps due to nascent risk factors (urbanization, lifestyle changes) coupled with limited access to prevention and treatment. Several important considerations should be noted when interpreting temporal changes in vertebral fracture incidence. Estimates derived from the GBD framework reflect modelled population-level incidence rather than directly observed clinical case counts. Given the well-recognized underdiagnosis of vertebral fractures, particularly in settings with limited access to imaging and specialized care, observed decreases in age-standardized incidence rates should not be interpreted as unequivocal evidence of a true reduction in fracture risk. Instead, such trends likely represent a composite effect of demographic change, evolving risk factor profiles, preventive efforts, and changes in diagnostic practices and reporting over time. This limitation is especially relevant for middle-income countries, where improvements in health-care access and fracture recognition may obscure underlying epidemiological patterns.
Clear geographic and socioeconomic disparities emerged. In 2021, the highest postmenopausal VF incidence rates were reported in Europe and North America (eg, Andorra, Belgium, Greenland, Switzerland), and the lowest rates were reported in many parts of Asia and Africa (eg, Bangladesh, Kiribati, South Africa). These differences largely follow the SDI: more developed countries tend to have older populations (thus more osteoporosis) and better diagnostic capacity, whereas developing countries underreport fractures. Inequality metrics quantify this: VF-related YLDs are disproportionately concentrated in lower-SDI countries (a pro-poor inequality), although our analysis revealed modest improvements from 1990-2021. Together with frontier analysis, these findings suggest that even some high-income countries (New Zealand, Andorra) could reduce burden by optimizing care, whereas low-income countries require expanded fracture prevention and treatment resources. In high-SDI settings, broad availability and reimbursement of oral bisphosphonates, denosumab, and other potent anti-osteoporotic agents, together with organized fracture liaison services and multifactorial fall-prevention programs, likely contributed to the declines observed in some countries; in contrast, in many low- and middle-income countries, limited access to dual-energy X-ray absorptiometry, high out-of-pocket costs for osteoporosis medications, and nutritional deficiencies may have constrained implementation of effective primary and secondary fracture prevention, helping to explain the persistently high or rising vertebral fracture burden in these settings.
Falls are by far the dominant cause of vertebral fractures worldwide. 29 This finding emphasizes that fall prevention is a linchpin of fracture reduction. Robust evidence shows that multifactorial fall prevention programs—especially those combining balance/strength training with home hazard reduction and medication review—significantly reduce fall rates and fall-related fractures in older adults. 28 Importantly, women who have sustained one vertebral fracture are at very high short-term risk of another fracture (“fracture cascade”), 30 underscoring the need for secondary prevention. In practice, any elderly woman with a new VF should be evaluated for osteoporosis and started on therapy to prevent debilitating recurrences. 31
Our decomposition analysis confirmed that population growth and aging are the principal drivers of increasing VF case counts. In every region, the growth of the female population contributed the most to increasing incidence rates and YLDs. Aging was the next largest factor, particularly for postmenopausal women (who bear age-related risk). In contrast, changes in age-specific VF rates played a smaller role; in fact, epidemiological improvements in younger women modestly offset the increase in absolute cases.
This study has several limitations. First, we used age 50 years as a pragmatic proxy for menopausal status; although this threshold is widely used in Global Burden of Disease–based analyses, ages at natural menopause vary across individuals and regions, leading to some misclassification between the pre- and postmenopausal groups. Second, vertebral fractures are substantially underdiagnosed, especially in low- and middle-income countries where access to spine imaging is limited and awareness of osteoporotic fractures is low, so the true burden may be higher than estimated in our study. Finally, our projections assume continuation of recent trends in risk factors, prevention programs, and treatment access; major policy changes, novel therapies, or unforeseen shocks (such as future pandemics) could alter the future trajectories we report.
In summary, vertebral fractures remain a major source of morbidity in women worldwide, and their absolute burden is projected to increase as populations age. Postmenopausal women account for the vast majority of VF cases and disability, whereas younger women experience relatively few fragility fractures. Importantly, we documented pronounced regional and socioeconomic disparities: older women in wealthy countries have the highest reported VF rates, but low- and middle-income countries suffer a disproportionate share of fracture-related disability. Addressing this challenge will require an integrated approach: global guidelines advocate routine osteoporosis screening in older women, 32 and our findings support broad implementation worldwide. Women identified with osteoporosis or prior VF should be offered effective pharmacotherapies (bisphosphonates, denosumab) proven to reduce the risk of vertebral fracture.33-36 In parallel, fall prevention programs—including exercise training and home safety interventions—should be expanded in aging communities. 28 Strengthening fracture liaison services and public awareness will also be crucial to mitigate the projected VF epidemic and reduce its inequitable impact.
Conclusions
Vertebral fractures represent a growing global health problem for women, especially after menopause. Although age-adjusted rates have declined in many regions (suggesting some success in prevention and treatment), the absolute number of fractures and associated disability is increasing due to demographic changes. The burden of VFs falls overwhelmingly on older women and is distributed inequitably toward lower-resource countries. Our findings highlight an urgent need for concerted public health action: policies should promote routine osteoporosis screening in at-risk women, ensure access to evidence-based treatments for those diagnosed with osteoporosis or fragility fractures, and implement broad fall prevention strategies. Such interventions are critical to avert future increases in the incidence of vertebral fractures and improve women’s bone health worldwide.
Supplemental Material
Supplemental Material - Global Burden of Vertebral Fractures in Women by Menopausal Status, 1990–2021, With 2050 Projections: An Analysis of Global Burden of Disease 2021
Supplemental Material for Global Burden of Vertebral Fractures in Women by Menopausal Status, 1990–2021, With 2050 Projections: An Analysis of Global Burden of Disease 2021 by Jun Fan, Weijie Liu, Genfeng Li, Kangqi Ji, Lingfei Wang, Xiaoyu Lian, Yigong Wang and Yanpeng Jian in Global Spine Journal.
Footnotes
Acknowledgments
We express our sincere gratitude to the Institute for Health Metrics and Evaluation and the Global Burden of Disease study collaborations.
Ethical Considerations
The GBD study protocol was approved by the research ethics board at the University of Washington (UW). The GBD studies must be conducted in full compliance with UW policies and procedures, as well as applicable federal, state, and local laws. Therefore, all ethical standards are justified by properly citing the respective sources (![]() ). Consequently, ethical approval and informed consent procedures are not needed for this study.
). Consequently, ethical approval and informed consent procedures are not needed for this study.
Author Contributions
J. Fan: Writing – original draft, Formal analysis, Data curation. W.J. Liu: Formal analysis, Data curation. G.F. Li: Formal analysis, Data curation. K.Q. Ji: Visualization, Validation. L.F. Wang: Visualization, Validation. X.Y. Lian: Methodology, Software. Y.G. Wang: Conceptualization, Project administration, Supervision, Writing – review & editing. Y.P. Jian: Project administration, Supervision, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed is publicly provided by the Institute for Health Metrics and Evaluation (https://www.healthdata.org/; ![]() ).
).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.