
Abstract
Study Design
Retrospective cohort study.
Objective
To comprehensively evaluate the clinical and radiological characteristics across intramedullary increased signal intensity (ISI) grades (Grade 0, 1, and 2) on T2-weighted magnetic resonance imaging (MRI) and identify preoperative predictors of ISI severity as well as risk factors for poor postoperative recovery in patients with thoracic ossification of the ligamentum flavum (T-OLF).
Methods
A total of 148 patients who underwent posterior laminectomy surgery for T-OLF between January 2017 and August 2023 was retrospectively analyzed. Demographic, imaging, surgical, and clinical outcome data were collected. ISI grades were independently assessed by three blinded spinal surgeons. Univariate and multivariate logistic regression analyses were performed to identify independent predictors and risk factors.
Results
Higher ISI grades were associated with worse preoperative neurological status, greater spinal canal compression, more complex OLF morphology, and increased intraoperative blood loss. Multivariate analysis identified a high canal occupying ratio (COR) (Odds ratio [OR] = 3.20, P = .012) and beak-type configuration on sagittal MRI (OR = 4.24, P = .003) as independent predictors of higher ISI grades. Moreover, multi-segment OLF (OR = 2.23, P = .028) and ISI Grade 2 (OR = 3.67, P = .044) independently predicted poor postoperative recovery.
Conclusion
Preoperative ISI grade serves as a critical prognostic indicator in T-OLF. High COR and beak-type configuration on sagittal MRI predict severe ISI grades, whereas multi-segment OLF and ISI Grade 2 independently predict poor postoperative outcomes. Incorporating these parameters into preoperative assessment may improve risk stratification, patient counseling, and surgical planning.
Keywords
Introduction
Thoracic ossification of the ligamentum flavum (T-OLF) is a slowly progressive degenerative disorder that leads to spinal cord compression and subsequent motor weakness, sensory deficits, and sphincter dysfunction, substantially compromising patients’ quality of life. 1 Surgical decompression remains the only effective treatment to relieve compression and restore neurological function.2,3 However, postoperative outcomes vary considerably, and a substantial proportion of patients fail to achieve satisfactory recovery.2,4-6
Magnetic resonance imaging (MRI) provides valuable insights into intramedullary pathological changes associated with T-OLF. 7 Increased signal intensity (ISI) on T2-weighted MRI has long been recognized as a radiological marker of spinal cord injury and has been correlated with postoperative neurological recovery. 8 Nevertheless, most previous studies have simply regarded ISI as a binary variable (present or absent),2,9-11 resulting in inconsistent conclusions, with some studies reporting ISI as a predictor of poor outcomes while others found no significant association.1,5,9,12
To date, only one study by Zhang et al 13 has specifically investigated the relationship between ISI grade (Grade 0, 1, and 2) and surgical outcomes in patients with T-OLF. Although their findings supported the prognostic significance of ISI grading, interpretation was limited by the small number of Grade 2 cases, short follow-up duration, and heterogeneity in MRI acquisition across 4 centers. Furthermore, the preoperative determinants of ISI severity remain unclear, and no large-scale study has systematically evaluated how ISI grades relate to postoperative outcomes.
To address these gaps, we conducted a large single-center retrospective cohort study with long-term follow-up. This study aimed to: (1) compare demographic, radiological, surgical, and clinical characteristics across different ISI grades; (2) identify independent preoperative predictors of ISI severity; and (3) determine independent risk factors for poor postoperative recovery. We hypothesized that higher ISI grades would correlate with more severe preoperative neurological deficits and predict worse postoperative outcomes.
Methods
Study Design and Population
This retrospective cohort study reviewed the medical records of 160 consecutive patients with T-OLF who underwent posterior laminectomy at our institution between January 2017 and August 2023. Ethical approval was obtained from our institutional review board, and the study adhered to the Declaration of Helsinki. 14 Informed consent was waived due to the retrospective design. Inclusion criteria were as follows: (1) thoracic myelopathy caused solely by T-OLF confirmed by both computed tomography (CT) and MRI; (2) age ≥18 years; and (3) complete clinical data with a minimum follow-up of 2 years. Exclusion criteria included: (1) concurrent ventral compressive lesions such as thoracic disc herniation, kyphotic deformity, or ossification of the posterior longitudinal ligament; (2) incomplete data or loss to follow-up; (3) previous thoracic surgery; and (4) non-compressive intramedullary pathologies such as syringomyelia, inflammatory, or demyelinating myelopathies. All procedures were performed by the same senior spine surgery team, and posterior decompression was conducted using a standardized en-bloc laminectomy technique with instrumentation.
Postoperative Management
Postoperative care was standardized across all patients according to our institutional protocol. Early mobilization was routinely encouraged, with ambulation initiated on the first postoperative day with thoracolumbar bracing under supervision of a rehabilitation therapist. Bedside physiotherapy focusing on gait training and lower-limb strengthening, which was progressively advanced. Wound drains were removed when the daily output fell below 50 mL, after which discharge planning was arranged.
For patients with cerebrospinal fluid (CSF) leakage, ambulation was temporarily restricted and conservative management including adequate hydration and hypertonic saline infusion was provided. Bedside functional rehabilitation was continued during bed rest. Drainage tubes were removed once CSF drainage became clear, followed by pressure dressing of the wound. All patients received structured rehabilitation instructions at discharge and were regularly followed postoperatively.
Data Collection
Demographic data included age, sex, body mass index (BMI), comorbidities (hypertension and diabetes mellitus), American society of Anesthesiologists (ASA) grade, preoperative modified Japanese Orthopaedic Association (mJOA) score, disease duration, nonambulatory status, sphincter dysfunction, and follow-up duration. Imaging data included the presence of multi-segment OLF, location of maximal stenosis, canal occupying ratio (COR), axial CT configuration, sagittal MRI configuration, and presence of diffuse idiopathic skeletal hyperostosis (DISH). Surgical variables included the number of decompressed segments, dural ossification, incidental durotomy, operative time per segment, and estimated blood loss (EBL) per segment. Postoperative complications included CSF leakage, transient neurological deterioration, epidural hematoma, wound infection, instrumented vertebrae fracture, and systemic complications. Clinical outcomes included neurological recovery and length of hospital stay.
Imaging Evaluation
Multi-segment OLF was defined as ossification extending across three or more vertebral levels. Axial CT configuration was classified as unilateral, bilateral, or bridged types
15
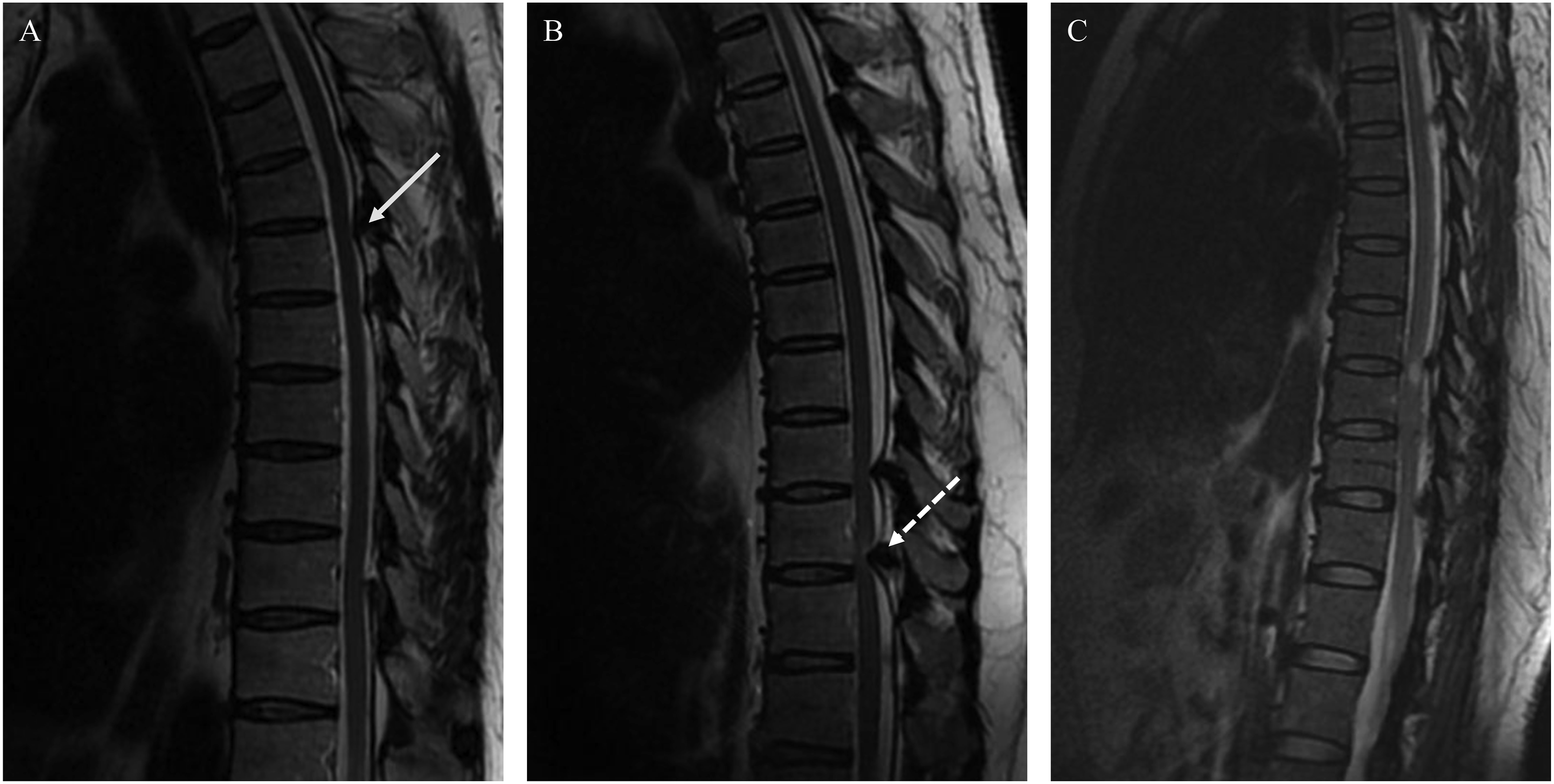
(Figure 1), and sagittal MRI configuration as round or beak types9,15 (Figure 2). DISH was diagnosed according to Resnick’s criteria.
16
The cross-sectional area (CSA) of the spinal canal at the pedicle level of the most stenotic segment was measured on axial CT images and defined as the reference CSA
17
(Figure 1). COR was calculated as: COR = (area of ossified mass at the narrowest level/reference CSA) × 100%. A COR >50% was defined as high. ISI grades were assessed on sagittal T2-weighted MRI according to Yukawa et al
18
: Grade 0 (none), Grade 1 (light or obscure), and Grade 2 (intense or bright) (Figure 2). Three experienced spine surgeons independently assessed all MRI scans in a blinded manner, and final grades were determined by consensus. OLF configuration type on axial CT and COR measurement. ISI Grades and OLF configuration type on sagittal T2-weighted MRI.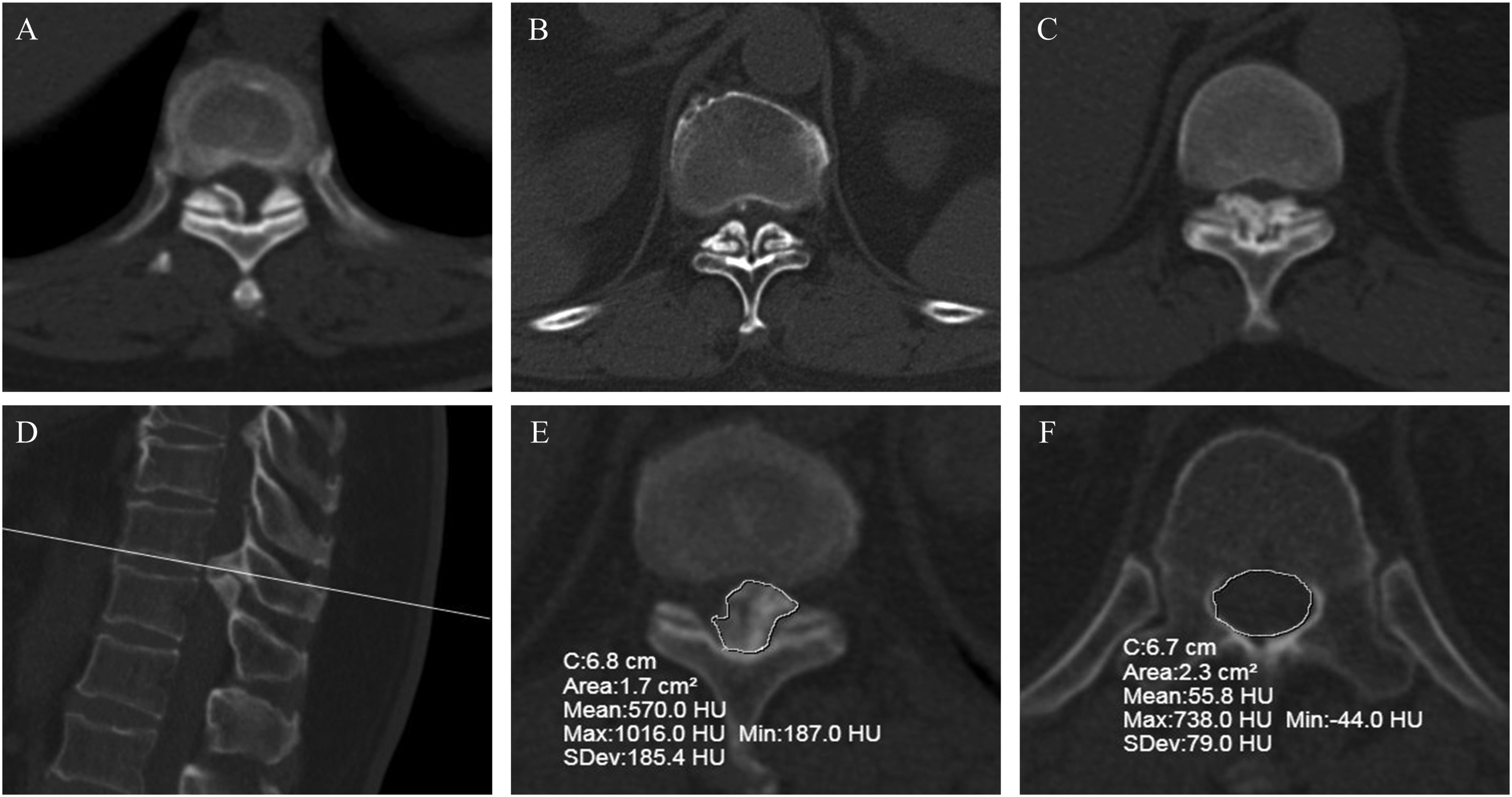
Neurological Assessment
Neurological function was assessed using the mJOA scores system both preoperatively and at final follow-up. The mJOA scores system excluded upper extremity function, with a maximum of 11 points. 19 Recovery rate (RR) was calculated as: RR = (postoperative mJOA score - preoperative mJOA score)/(11 - preoperative mJOA score) × 100%. 19 RR ≥50% was defined as good recovery, and RR <50% as poor recovery, consistent with previously thoracic myelopathy studies.11,19,20
Statistical Analysis
All statistical analyses were conducted using R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria). Normality of continuous variables was tested using the Shapiro–Wilk test. Continuous data were expressed as mean ± standard deviation (SD) and compared using one-way analysis of variance, Kruskal–Wallis test, unpaired t test, or Wilcoxon rank-sum test as appropriate. Categorical variables were presented as counts (percentages) and compared using the Chi-square or Fisher’s exact test. Interobserver reliability for ISI grades was evaluated using the intraclass correlation coefficient (ICC) and 95% confidence intervals (CIs), with ICC >0.8 indicating excellent agreement. Variables with P < .05 in univariate analysis were included in multivariate logistic or ordinal regression analyses to identify independent predictors. Odds ratios (ORs) with 95% CIs were calculated. Multicollinearity was assessed using the generalized variance inflation factor (GVIF), with GVIF <5 considered acceptable. Sample size adequacy was evaluated according to the 10 events-per-variable principle, ensuring no overfitting in multivariable models. A two-tailed P < .05 was considered statistically significant.
Results
Patient Demographics
Demographic Characteristics of Patients Among Different ISI Grades
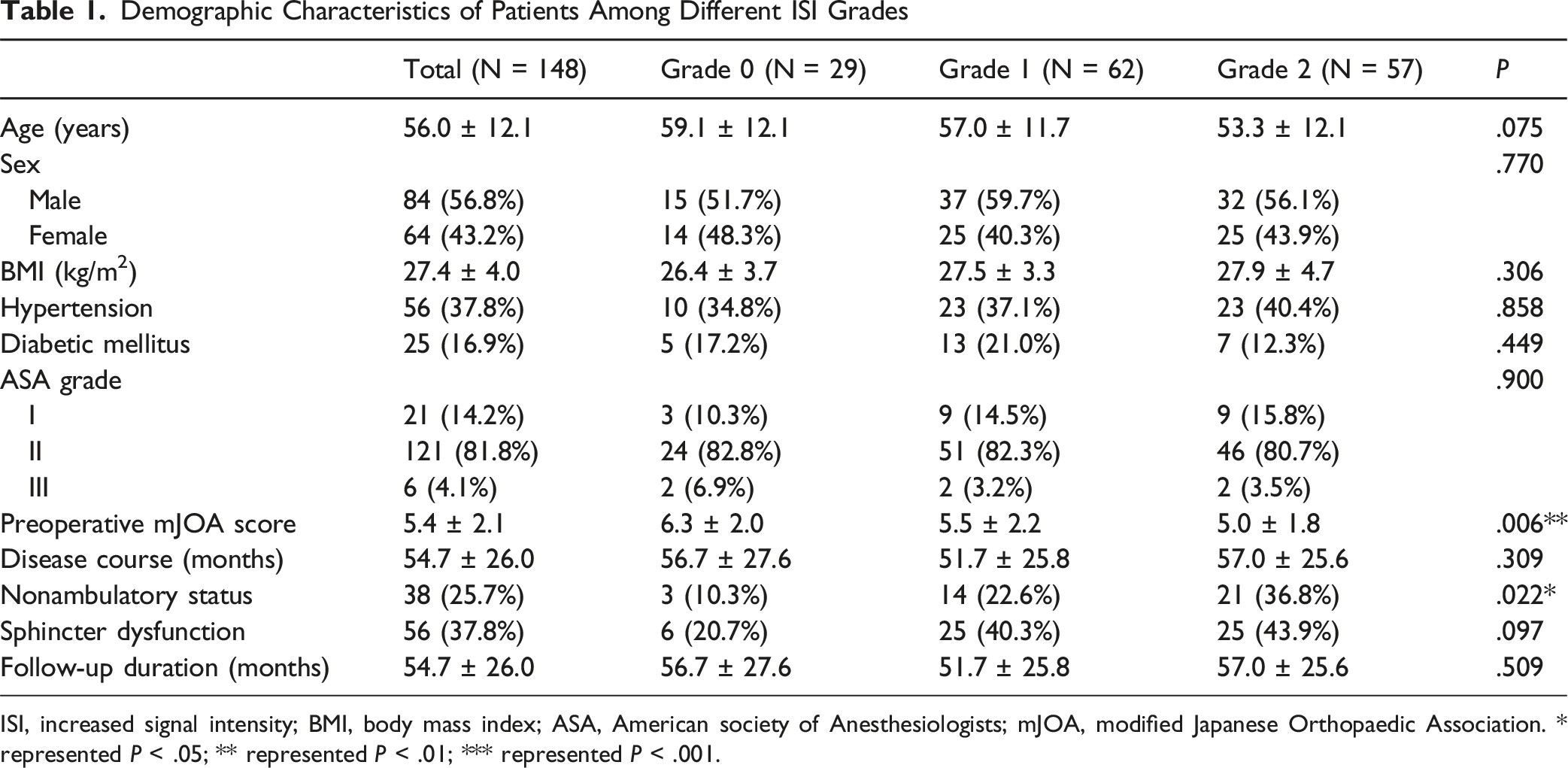
ISI, increased signal intensity; BMI, body mass index; ASA, American society of Anesthesiologists; mJOA, modified Japanese Orthopaedic Association. * represented P < .05; ** represented P < .01; *** represented P < .001.
Imaging Characteristics
Comparisons of Imaging Features Among Different ISI Grades
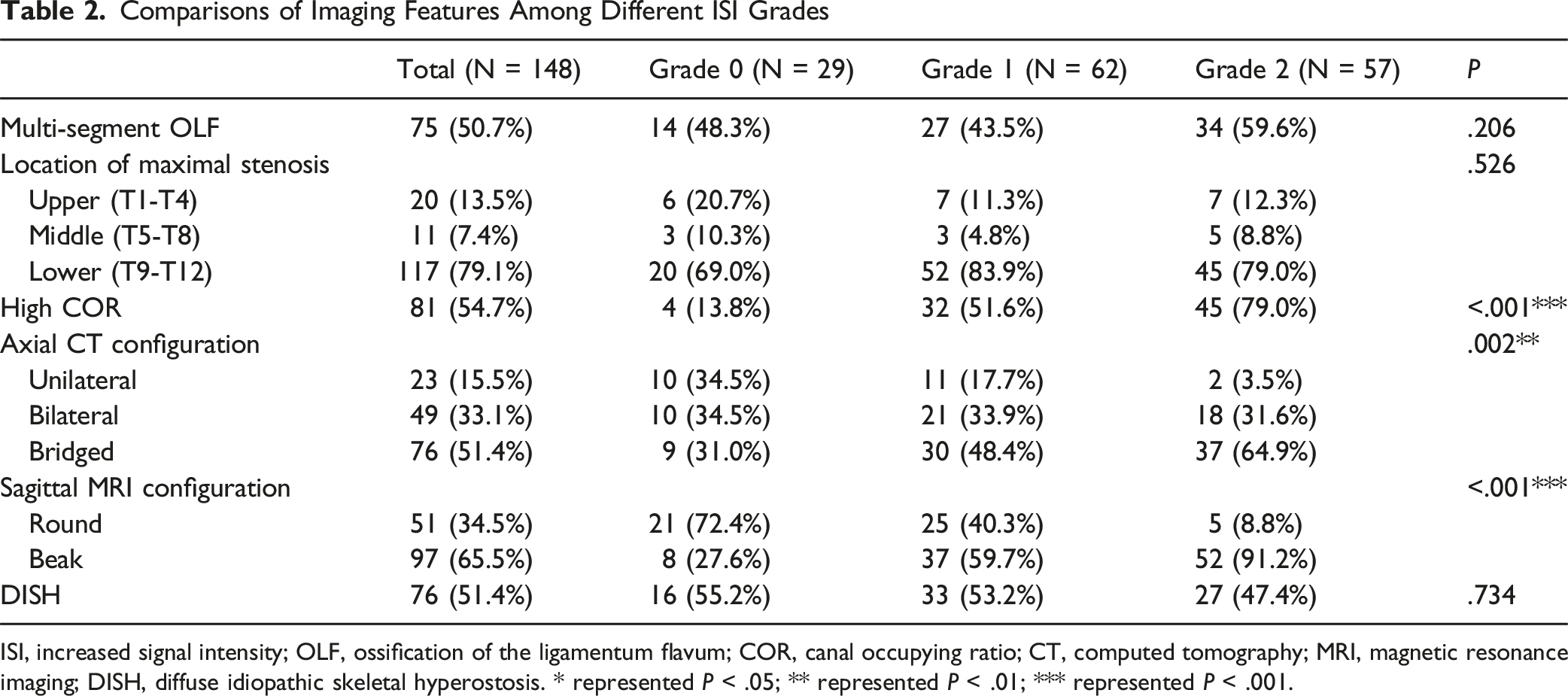
ISI, increased signal intensity; OLF, ossification of the ligamentum flavum; COR, canal occupying ratio; CT, computed tomography; MRI, magnetic resonance imaging; DISH, diffuse idiopathic skeletal hyperostosis. * represented P < .05; ** represented P < .01; *** represented P < .001.
Surgical Findings and Postoperative Outcomes
Comparisons of Surgical Details, Complications and Clinical Outcomes Among Different ISI Grades
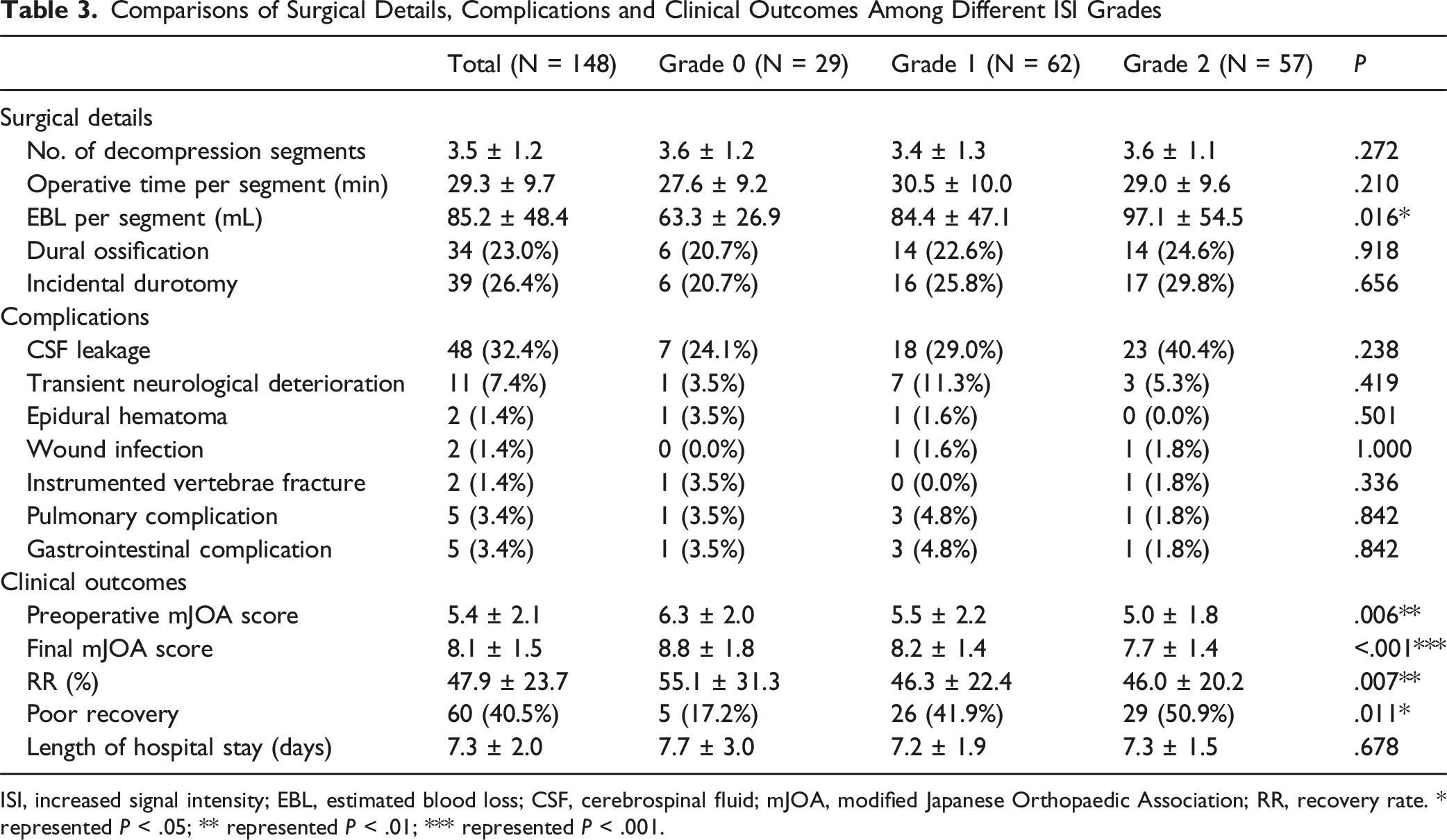
ISI, increased signal intensity; EBL, estimated blood loss; CSF, cerebrospinal fluid; mJOA, modified Japanese Orthopaedic Association; RR, recovery rate. * represented P < .05; ** represented P < .01; *** represented P < .001.
Neurologically, the mJOA scores improved significantly from 5.4 ± 2.1 preoperatively to 8.1 ± 1.5 at final follow-up (P < .001) and improved significantly within each ISI subgroup (all P < .001). However, both the final mJOA score (P < .001) and RR (P = .011) differed significantly among the three groups, with Grade 2 ISI showing the poorest recovery. Overall, 40.5% of patients experienced poor recovery, which was most frequent in Grade 2 ISI (50.9%). Length of hospital stay was comparable across groups (P = .678) (Table 3).
Predictors of ISI Severity
Multivariate Ordinal Logistic Regression Analysis for ISI Grade
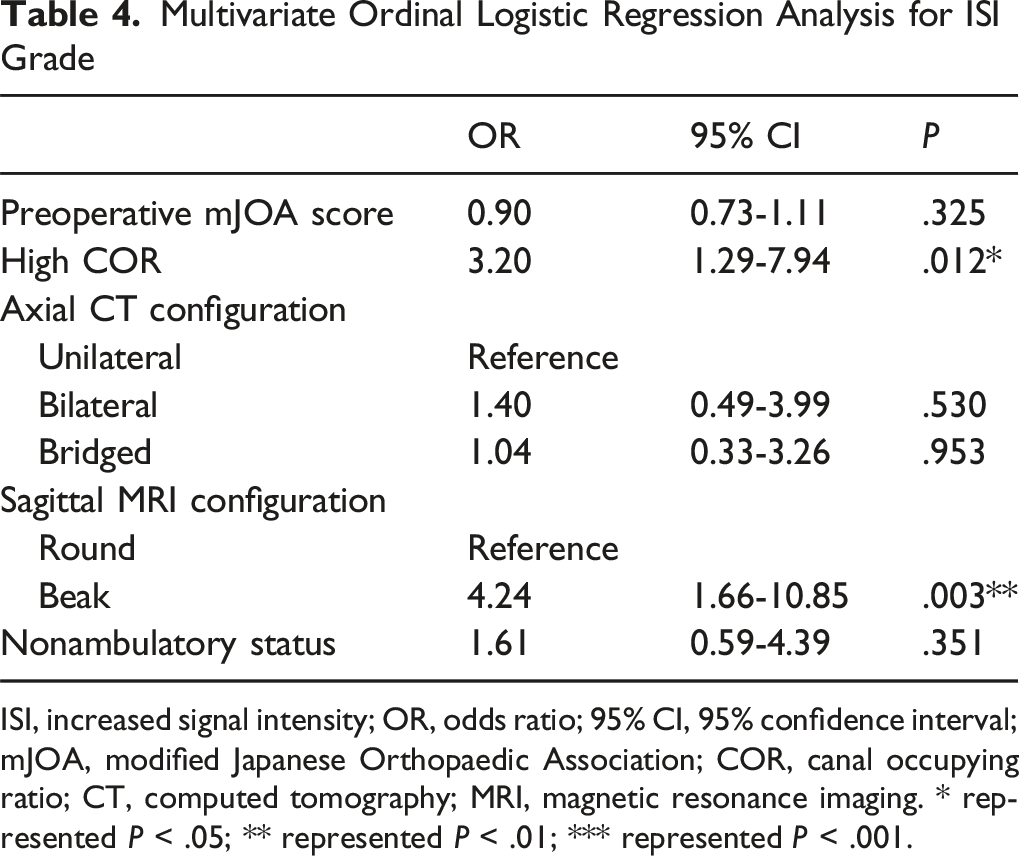
ISI, increased signal intensity; OR, odds ratio; 95% CI, 95% confidence interval; mJOA, modified Japanese Orthopaedic Association; COR, canal occupying ratio; CT, computed tomography; MRI, magnetic resonance imaging. * represented P < .05; ** represented P < .01; *** represented P < .001.
Risk Factors for Poor Recovery
Univariate Analysis Between Good and Poor Recovery Groups
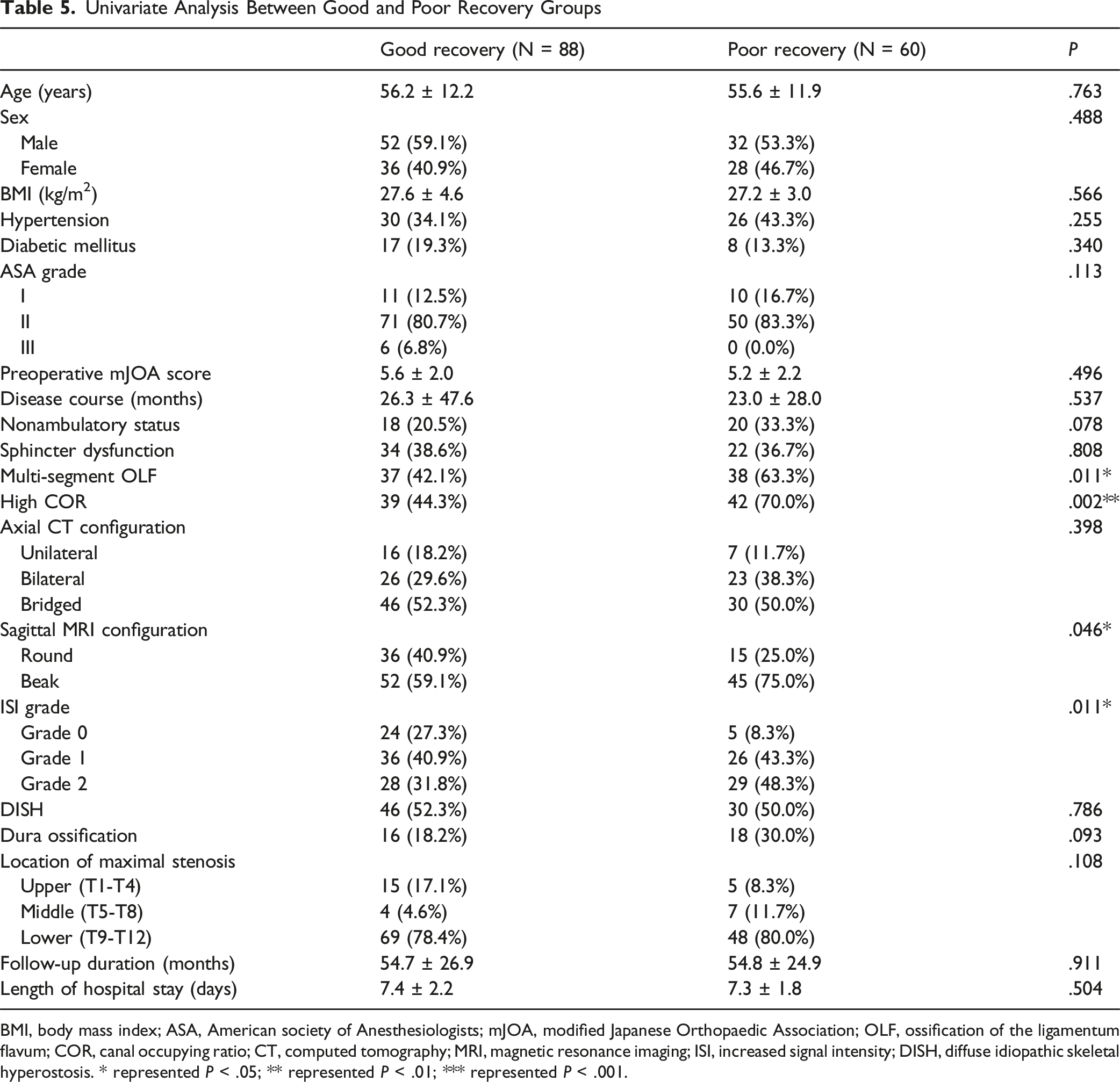
BMI, body mass index; ASA, American society of Anesthesiologists; mJOA, modified Japanese Orthopaedic Association; OLF, ossification of the ligamentum flavum; COR, canal occupying ratio; CT, computed tomography; MRI, magnetic resonance imaging; ISI, increased signal intensity; DISH, diffuse idiopathic skeletal hyperostosis. * represented P < .05; ** represented P < .01; *** represented P < .001.
Multivariate Logistic Regression Analysis of Risk Factors for Poor Recovery
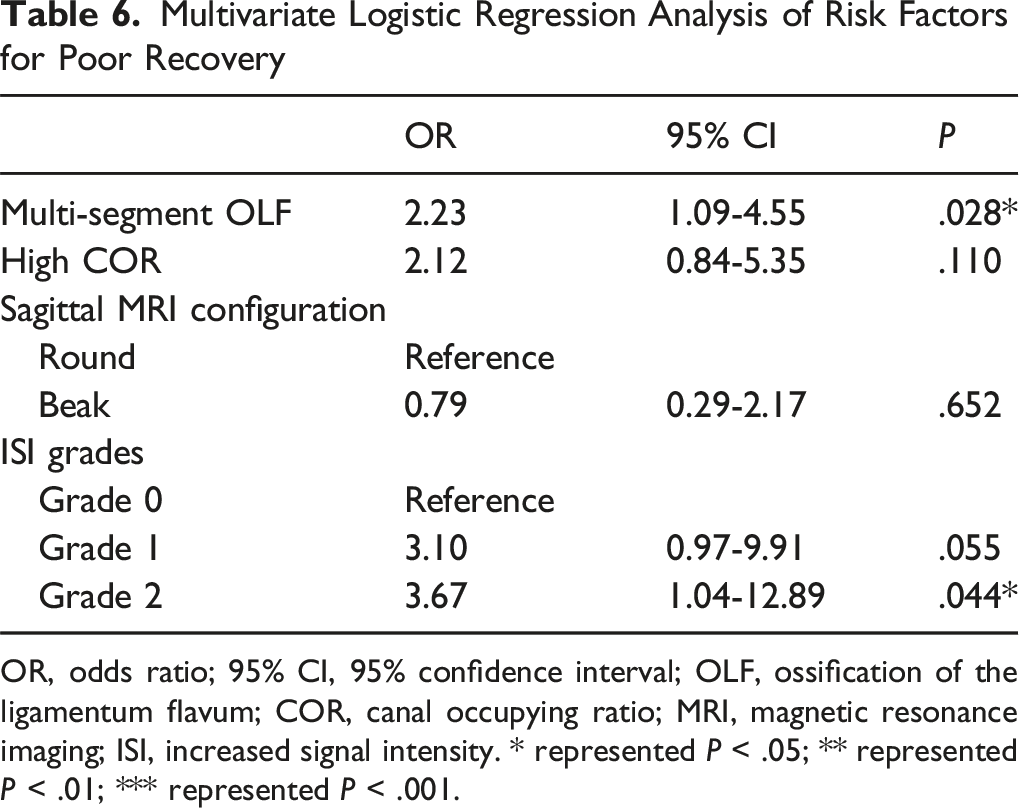
OR, odds ratio; 95% CI, 95% confidence interval; OLF, ossification of the ligamentum flavum; COR, canal occupying ratio; MRI, magnetic resonance imaging; ISI, increased signal intensity. * represented P < .05; ** represented P < .01; *** represented P < .001.
Discussion
To our knowledge, this retrospective cohort represents the largest study and longest follow-up study to comprehensively evaluate the clinical and radiological implications of preoperative ISI grades in patients with T-OLF undergoing posterior laminectomy. Our findings demonstrated that preoperative ISI grades served as a significant prognostic indicator, correlating with disease severity, radiological morphology, intraoperative complexity, and postoperative neurological recovery. In particular, a high COR and beak-type configuration on sagittal MRI independently predicted higher ISI grades, whereas multi-segment OLF and ISI Grade 2 were identified as independent risk factors for poor neurological recovery.
Consistent with previous evidence in cervical myelopathy, intramedullary hyperintensity on T2-weighted MRI is generally regarded as a surrogate of underlying spinal cord pathology, such as edema, ischemia, myelomalacia, demyelination, or necrosis.21,22 In this cohort, 80.4% of patients exhibited intramedullary T2 hyperintensity on T2-weighted MRI, consistent with prior studies reporting incidence of 41% - 79%. 23 The strong association between higher ISI grades and high COR aligns with the hypothesis that mechanical compression plays a major role in the development of intramedullary signal alterations. 23 Moreover, progressive worsening of preoperative neurological status and higher rates of nonambulatory status were observed with increasing ISI grades. Patients with Grade 2 ISI also experienced significantly greater intraoperative blood loss, which may be mechanistically linked to the higher prevalence of complex OLF configurations in this subgroup, potentially contributing to venous plexus congestion. These findings are in line with Zhang et al 13 who also demonstrated that preoperative ISI classification was associated with clinical severity, disease duration, degree of spinal cord compression, and surgical outcomes.
Multivariate ordinal logistic regression analysis further confirmed that a high COR and beak-type configuration on sagittal MRI were independent predictors of higher ISI grades. Previous literature by Kuh et al 15 has likewise suggested that beak-type OLF is associated with greater surgical difficulty and worse prognosis compared with round-type morphology. We speculate that the focal, sharp compression produced by beak-type OLF, combined with severe stenosis, may result in microvascular compromise and irreversible neural injury, ultimately manifesting as intense intramedullary hyperintensity (Grade 2) on MRI.
With regard to surgical outcomes, 40.5% of patients experienced poor recovery at a mean follow-up of 54.7 months. Multivariate analysis identified multi-segment OLF and preoperative ISI Grade 2 as independent predictors of unfavorable postoperative neurological recovery. The adverse impact of extensive OLF involvement on recovery is consistent with the findings of Nagesh et al 19 Moreover, the independent predictive value of ISI Grade 2 is supported by neuropathological evidence indicating that Grade 1 ISI generally reflects reversible intramedullary edema, 4 whereas Grade 2 ISI reflect corresponds to more advanced and irreversible histopathological changes, including necrosis and cavitation.24,25 Collectively, these findings highlight the clinical importance of ISI grades as a noninvasive marker of irreversible spinal cord injury in T-OLF.
Our findings provide clinically meaningful guidance for patient management. Preoperatively, identifying a high COR, beak-type morphology, multi-segment OLF, and particularly ISI Grade 2 enables more accurate risk stratification and prognostic counseling. Intraoperatively, recognizing these high-risk features allows surgeons to better anticipate technical challenges, optimize surgical planning, and prepare adequate blood management strategies, including autologous blood salvage systems and appropriate blood product availability. Moreover, the strong association between ISI Grade 2 and irreversible cord damage underscores the potential importance of timely surgical intervention before progression to advanced intramedullary pathology.
Several limitations should be acknowledged. First, the retrospective design and single-center nature of this study may have introduced selection and information bias. Second, the study included only patients with T-OLF, so the conclusions may not be generalizable to other etiologies of thoracic myelopathy. Third, although dichotomizing RR at a 50% threshold is clinically intuitive and widely adopted in previous literature, this approach may reduce outcome granularity and potentially attenuate statistical power. Finally, although the ISI grading system demonstrates excellent interobserver reliability, it remains a qualitative assessment and is unable to directly quantify the severity of intramedullary pathology. The absence of quantitative MRI metrics, such as signal intensity ratios or radiomics-based texture parameters, limits the biological interpretation of ISI alterations. Future studies integrating advanced quantitative MRI techniques, together with prospective multicenter investigations, are warranted to validate these findings and further clarify their clinical implications.
Conclusions
In conclusion, preoperative ISI grade on T2-weighted MRI represents a critical prognostic biomarker in patients with T-OLF. Higher ISI grades are associated with greater canal compression, more complex radiological morphology, and poorer postoperative neurological recovery. High COR and beak-type sagittal MRI configuration independently predict severe ISI changes, whereas multi-segment OLF and ISI Grade 2 independently are independent risk factors for unfavorable postoperative outcomes. Early surgical intervention before progression to high-grade ISI may help prevent irreversible spinal cord injury and optimize neurological recovery.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee of Peking University Third Hospital (No. M20241067) and conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
All identifiable individual data presented in this article were obtained with informed consent from the participants.
Consent for Publication
Informed consent was waived due to the retrospective nature of the study.
Authors Contribution
Juncai Lei contributed to the study design, data analysis, and manuscript drafting. Panpan Hu contributed to data analysis and materials support. Yanchao Tang and Xiao Liu assisted in data collection and material supports. Zhongjun Liu contributed to study design and material supports. Hua Zhou, Feng Wei, and Xiaoguang Liu conceived the study, supervised the manuscript. All authors read and approved the final manuscript. Juncai Lei and Panpan Hu contributed equally. Hua Zhou, Feng Wei, and Xiaoguang Liu shared corresponding authorship.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 82372451) and Beijing Natural Science Foundation (No. 4252025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from Peking University Third Hospital. However, restrictions apply to the availability of these data, which were used under institutional license and are not publicly accessible.