
Abstract
Study Design
Systematic Review.
Objectives
Degenerative cervical myelopathy (DCM) or cervical spondylotic myelopathy (CSM) is a progressive neurological condition linked to cervical degeneration, often presenting with a wide range of symptoms that complicate diagnosis. This study aims to identify clinical, radiological, and electrophysiological measures that aid in early DCM diagnosis.
Methods
Following PRISMA guidelines a systematic review was performed. Literature from PubMed, Scopus, and the Cochrane Library up to November 2025 was analyzed. Search terms included “degenerative cervical myelopathy”, “cervical spondylotic myelopathy”, “CSM”, “Early clinical signs”, “Diffusion Tensor Imaging”, “Fractional anisotropy”, “Motor-evoked potentials”, “Sensory-evoked potentials”. The included studies primarily focused on clinical examinations, radiological imaging, and electrophysiological tests to detect early signs of DCM.
Results
A total of 36 met the inclusion criteria, involving 4596 patients. Tests for “myelopathy hand” signs showed high negative predictive values in excluding DCM. Lower limb assessments, such as the ten-second step test and Rossolimo reflex, also showed promise for early diagnosis. Among imaging techniques, DTI outperformed traditional T2-weighted Magnetic Resonance Imaging (MRI) in sensitivity, specificity, and predictive value. Kinematic CT myelography (CMCT) also demonstrated potential for early detection. Electrophysiological tests, including SEPs and MEPs, provided valuable insights into disease severity when performed both statically and dynamically.
Conclusions
DCM’s variable profile complicates diagnosis. This review highlights the importance of underused clinical evaluations for earlier detection, with DTI showing promise for early changes and preventive use. Electrophysiological measures, non-invasive and accurate, should be integrated alongside dynamic evaluations for a comprehensive, multi-modal diagnostic approach.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) or cervical spondylotic myelopathy (CSM) is a progressive neurological disorder caused by age-related cervical spine degeneration, leading to spinal cord and/or vascular compression. 1 DCM is the leading cause of non-traumatic spinal cord injury in older adults, accounting for 59% of cases in Japan, 54% in the U.S., 31% in Europe, 22% in Australia, and 4-30% in Africa. 2 Its prevalence increases with age, affecting 0.6% of individuals under 20 and rising to 9.1% in those over 70. 3 More common in men (2.7:1), DCM most frequently involves the C5/6 level, followed by C6/7, C4/5, and C3/4.4,5 As DCM progresses, the risk of severe neurological impairments increases, leading to greater physical limitations and heightened dependence on caregivers.1,6-11 Consequently, DCM imposes a major socioeconomic burden, increasing healthcare costs and disability-related losses worldwide. 12
The diagnosis of DCM is challenging due to its misleading symptoms, unclear clinical signs, and potential mismatch between clinical and radiological features, often leading to delays in diagnosis. 13
Magnetic resonance imaging (MRI) is widely considered the current standard for diagnosing DCM, with T2-weighted imaging (T2WI) often showing increased signal intensity in advanced cases, indicating swelling, inflammation, ischemia, and gliosis.14-16 However, not all patients with typical symptoms exhibit this hyperintensity, complicating diagnosis and prognosis. 17 Electrophysiological measures, including Sensory-evoked potentials (SEPs), Motor-evoked potentials (MEPs), and electromyography (EMG), are extensively used in the diagnosis and prognosis of DCM to assess spinal tract and neuron involvement, differentiate from other neuromuscular disorders, and evaluate prognosis for decompressive surgery in a non-invasive and painless manner.18,19
DCM is commonly classified into three types: preclinical, mild, and clinical. Preclinical DCM involves MRI abnormalities without clear clinical signs, while mild DCM shows neurological changes alongside MRI signs, but less severe than clinical DCM.19,20 Physical exams may reveal signs like Hoffman’s, Babinski reflex, and Lhermitte’s sign, indicating more advanced stages.21-23 Indeed, many patients fail to receive an early diagnosis of the disease, often due to misdiagnosis, with the condition typically being identified only in its late stages, where postoperative neurological recovery is limited. 24
Due to the considerable heterogeneity in clinical, radiographic, and electrophysiological presentation, the current study seeks to review the scientific literature on clinical examinations, radiological exams, and instrumental neurological tests used in diagnosing DCM, aiming to identify those that could enable an earlier diagnosis.
Materials and Methods
Study Selection and Eligibility Criteria
The formulation of the research question was done using a PIOS approach: Population (P), Intervention (I), Outcome (O), and Study Design (S). This systematic review collected and analysed data on patients with DCM (P). Clinical, radiological and electrophysiological measures (I) were adopted to evaluate its accuracy in detecting pre-clinical phases of DCM in adult patients (O). The following study designs were included (S): Randomized Control Trials (RCT), Retrospective Cohort studies (RC), Prospective Cohort studies (PC), and comparative studies.
The inclusion and exclusion criteria were established before the commencement of the study. Articles that did not focus on the cervical segment, as well as studies involving pediatric patients or patients with alternative diagnoses such as spine tumors, vertebral fractures, other spinal cord injuries, infections, or rheumatological diseases (rheumatoid arthritis and ankylosing spondylitis), were excluded. Studies focused on the general diagnosis or prognosis evaluation of advanced-stage DCM patients, as well as those examining electrophysiological measures for differential diagnosis with other neurological disorders or confirming diagnosis in patients already presenting with mild or clinical DCM, were excluded. Additionally, abstracts, commentaries or opinions, systematic or narrative reviews, case reports, cadaver studies, biomechanical studies, editorials, and studies with fewer than 10 patients were excluded.
Search Strategy
A thorough search of electronic databases, including PubMed, Scopus, and Cochrane Library was conducted from the inception of each database to November 20th 2025. Only studies concerning humans and published in the English language were selected. Terms specific to degenerative spinal cord compression, degenerative cervical myelopathy, cervical spondylosis, cervical stenosis, cervical spondylotic myelopathy, and early diagnosis were used. The following string was implemented: (“cervical spondylotic myelopathy”[Title/Abstract] OR “CSM”[Title/Abstract] OR “degenerative cervical myelopathy”[Title/Abstract] OR “DCM”[Title/Abstract]) AND (“magnetic resonance imaging”[MeSH Terms] OR (“magnetic”[All Fields] AND “resonance”[All Fields] AND “imaging”[All Fields]) OR “magnetic resonance imaging”[All Fields] OR “mri”[All Fields] OR “DTI”[All Fields] OR “Fractional anisotropy”[All Fields] OR “FA”[All Fields] OR “early clinical signs”[All Fields] OR (“electromyography”[MeSH Terms] OR “electromyography”[All Fields] OR “emg”[All Fields]) OR “SSEP”[All Fields] OR “MEP”[All Fields]).
Data Collection Process
The full text of potentially eligible studies was read and reviewed by two independently working investigators (P.B. and P.F.) to obtain the definite number of studies included in the article. In case of disagreement, the considered article was reviewed, and the conflict was solved after discussion with a third review author (F.R.). The inclusion and exclusion of the reviewed articles are reported below in the PRISMA flowchart, found in Figure 1. PRISMA 2020 flow diagram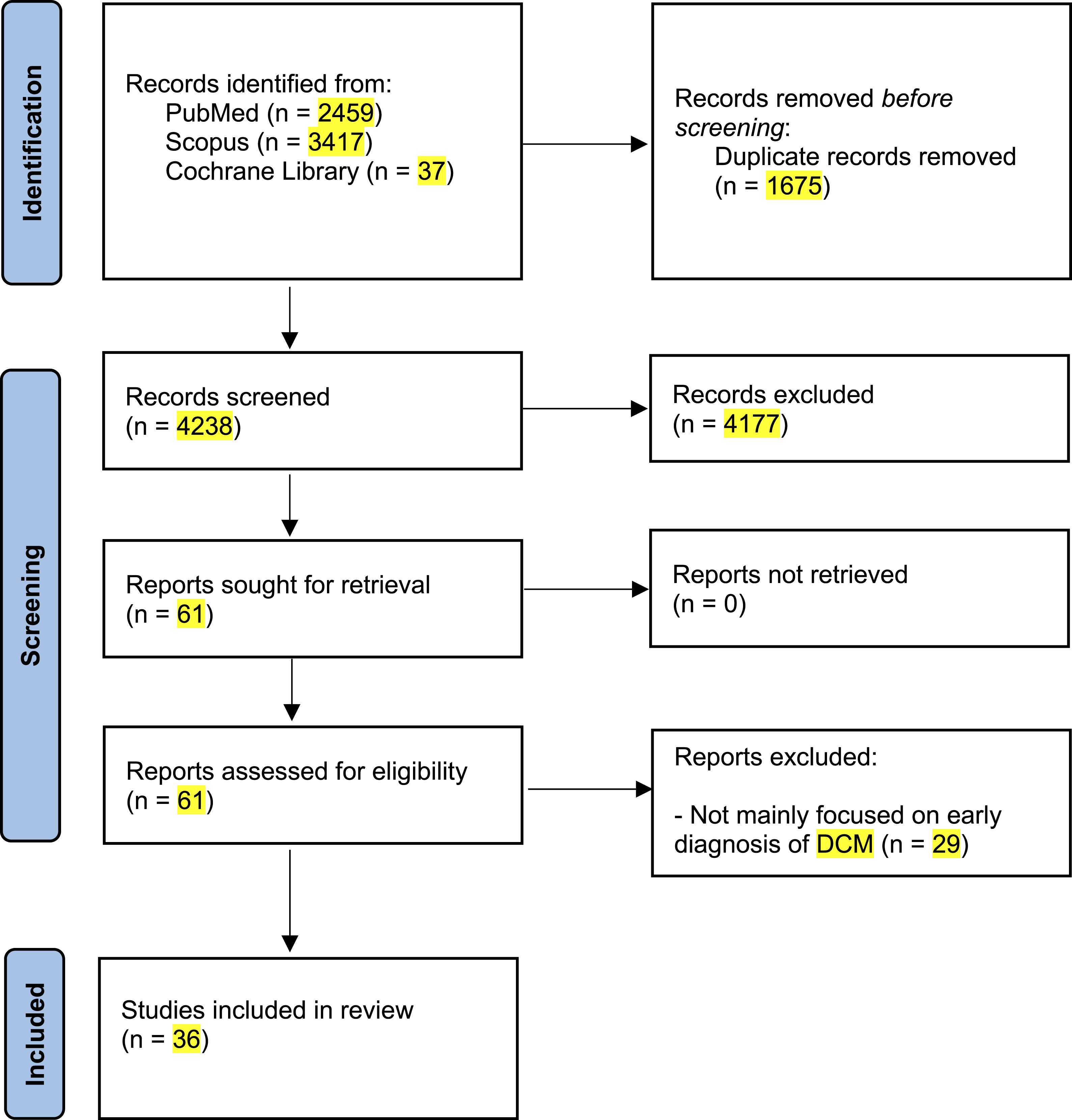
Data Items
The following data was extracted from the included articles: first author, study groups, sample size, mean age, gender and level of myelopathy. Each clinical, radiological, or electrophysiological measure evaluated in the studies was described in terms of its execution in clinical practice, how it could be considered positive, and its results regarding specificity and sensitivity in aiding the early diagnosis of DCM.
Results
Study Selection and Characteristics
The literature research identified 5913 articles. After duplicate removal, 4238 articles were screened on title and abstract. The full text of 61 articles was reviewed, and 29 were excluded for not focusing primarily on the early diagnosis of DCM. The articles included in this review were 36 (Figure 1). All the articles included in the review had as their main objective to analyse the role of clinical examinations (N = 10 [27,77%]), radiological exams (N = 15 [41,66%]), and instrumental neurological tests (N = 11 [30,55%]) used in the diagnosis of DCM and to identify which have the potential to allow for an earlier diagnosis. A total of 2703 patients were assessed through clinical evaluations, 980 through radiological exams, and 913 through electrophysiological measures.
Clinical Examinations
The majority of the included studies focusing on clinical examinations evaluated changes in strength or sensation in the upper limbs. Specifically, the Dynamic Hoffman’s sign, Wazir hand myelopathy sign, slow grip and release test, and Trömner sign were analyzed, all showing promising results for early DCM detection, with high negative predictive values for excluding cervical myelopathy compared to standard tests.25-29 Tests focused on the lower limbs, such as the ten-second step test and Rossolimo reflex evaluation, were also analyzed. Both tests demonstrated a correlation with the severity of spinal cord dysfunction in patients, making them useful for predicting postoperative outcomes.30,31 Additionally, cervicobrachial neuralgia, in addition to gait disturbance, sensory deficits, and motor deficits were evaluated in the study by Özkan at al. They concluded that cervicobrachial neuralgia was the most common initial symptom of DCM and that patients with gait disturbance as their first symptom typically received a diagnosis later (19.5 weeks) compared to those without these clinical signs (16 weeks). 32 In addition to the above, the clinical signs analyzed also included inverted supinator sign, Babinski test, 33 ankle plantar flexor maximal voluntary isometric contractions (MVIC) and knee extensor MVIC. 34
Clinical Signs and Patient Characteristics
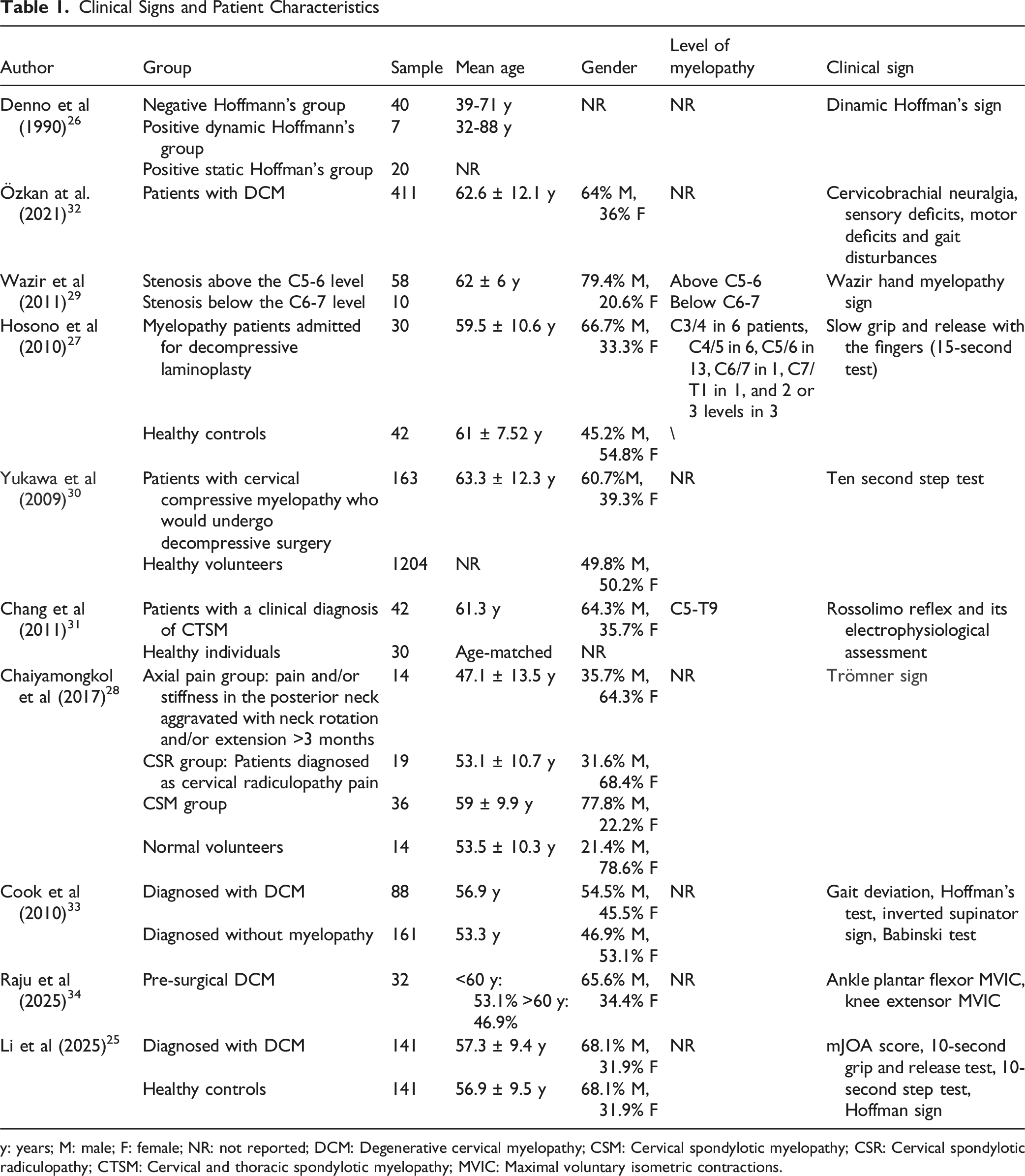
y: years; M: male; F: female; NR: not reported; DCM: Degenerative cervical myelopathy; CSM: Cervical spondylotic myelopathy; CSR: Cervical spondylotic radiculopathy; CTSM: Cervical and thoracic spondylotic myelopathy; MVIC: Maximal voluntary isometric contractions.
Clinical Signs Outcomes
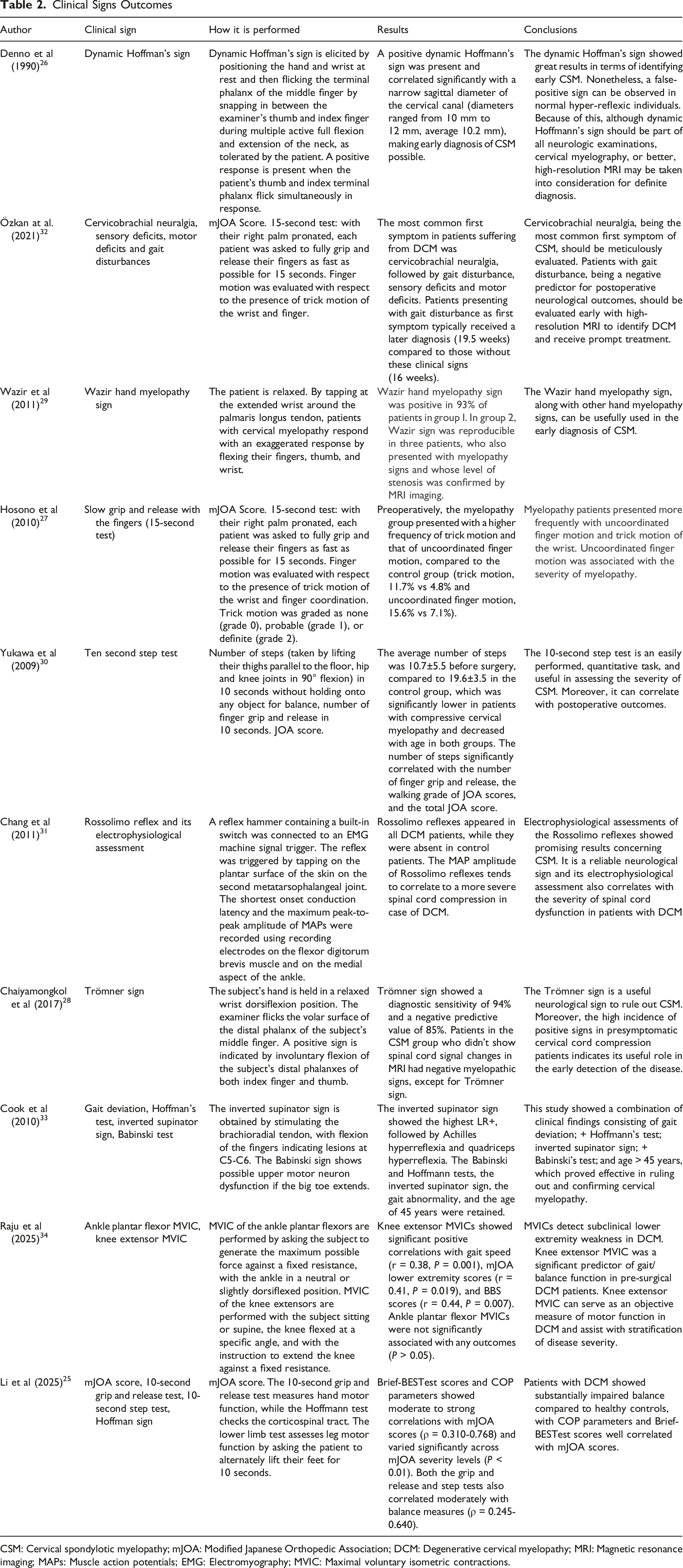
CSM: Cervical spondylotic myelopathy; mJOA: Modified Japanese Orthopedic Association; DCM: Degenerative cervical myelopathy; MRI: Magnetic resonance imaging; MAPs: Muscle action potentials; EMG: Electromyography; MVIC: Maximal voluntary isometric contractions.
Radiological Techniques
Radiological Techniques and Patient Characteristics
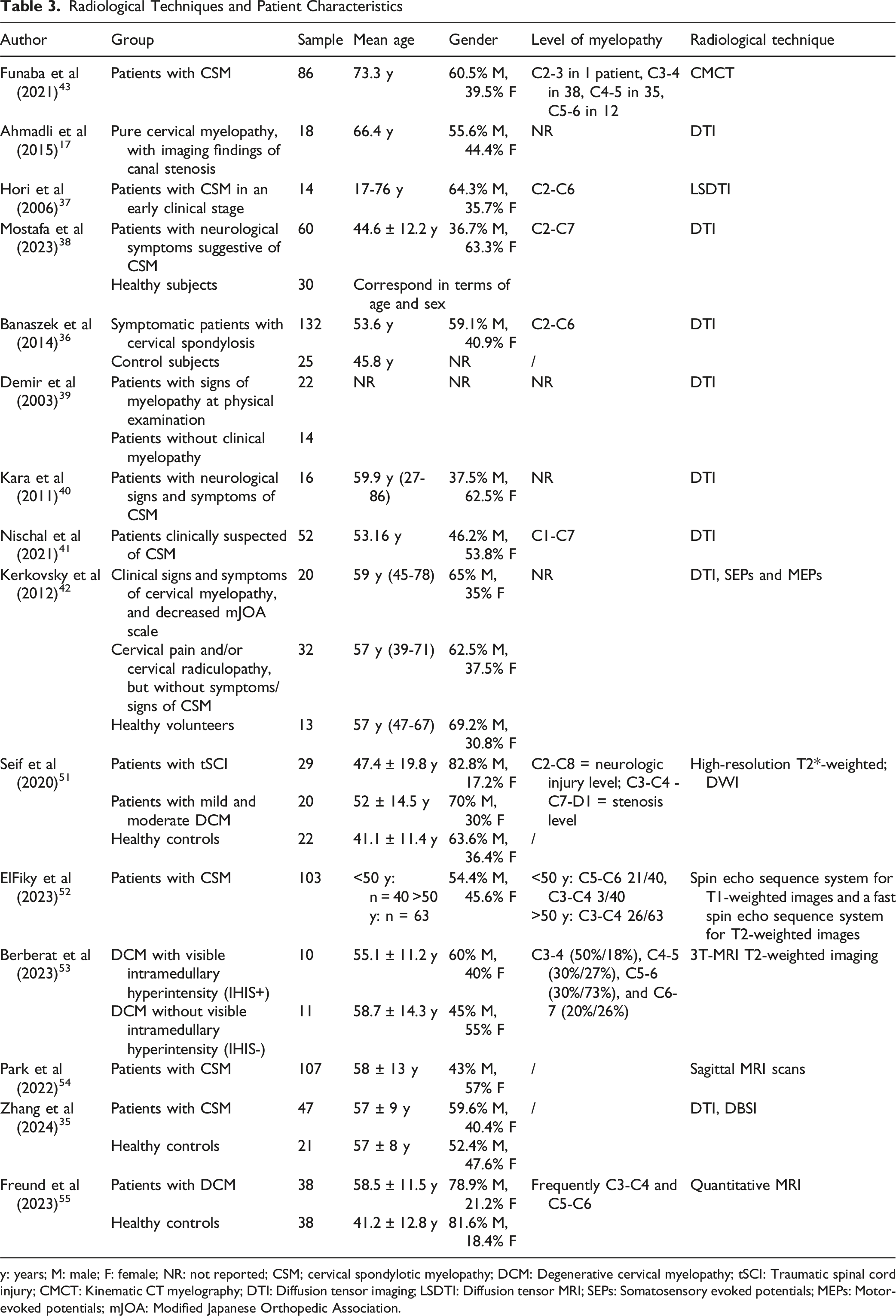
y: years; M: male; F: female; NR: not reported; CSM; cervical spondylotic myelopathy; DCM: Degenerative cervical myelopathy; tSCI: Traumatic spinal cord injury; CMCT: Kinematic CT myelography; DTI: Diffusion tensor imaging; LSDTI: Diffusion tensor MRI; SEPs: Somatosensory evoked potentials; MEPs: Motor-evoked potentials; mJOA: Modified Japanese Orthopedic Association.
Radiological Techniques Outcomes
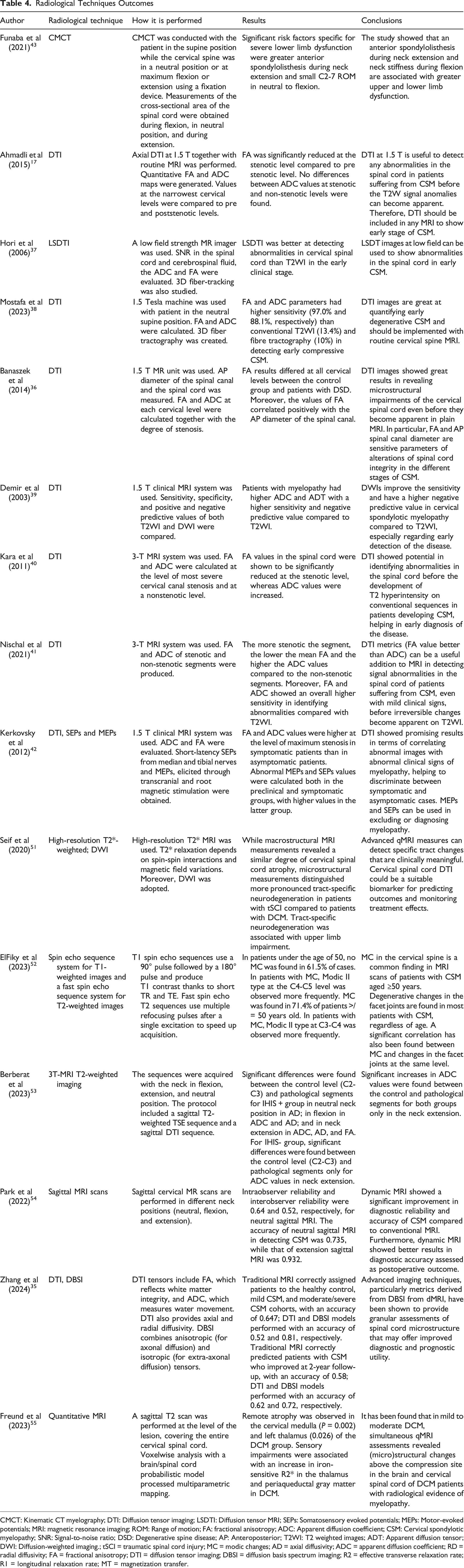
CMCT: Kinematic CT myelography; DTI: Diffusion tensor imaging; LSDTI: Diffusion tensor MRI; SEPs: Somatosensory evoked potentials; MEPs: Motor-evoked potentials; MRI: magnetic resonance imaging; ROM: Range of motion; FA: fractional anisotropy; ADC: Apparent diffusion coefficient; CSM: Cervical spondylotic myelopathy; SNR: Signal-to-noise ratio; DSD: Degenerative spine disease; AP: Anteroposterior; T2WI: T2 weighted images; ADT: Apparent diffusion tensor; DWI: Diffusion-weighted imaging.; tSCI = traumatic spinal cord injury; MC = modic changes; AD = axial diffusivity; ADC = apparent diffusion coefficient; RD = radial diffusivity; FA = fractional anisotropy; DTI = diffusion tensor imaging; DBSI = diffusion basis spectrum imaging; R2 = effective transverse relaxation rate; R1 = longitudinal relaxation rate; MT = magnetization transfer.
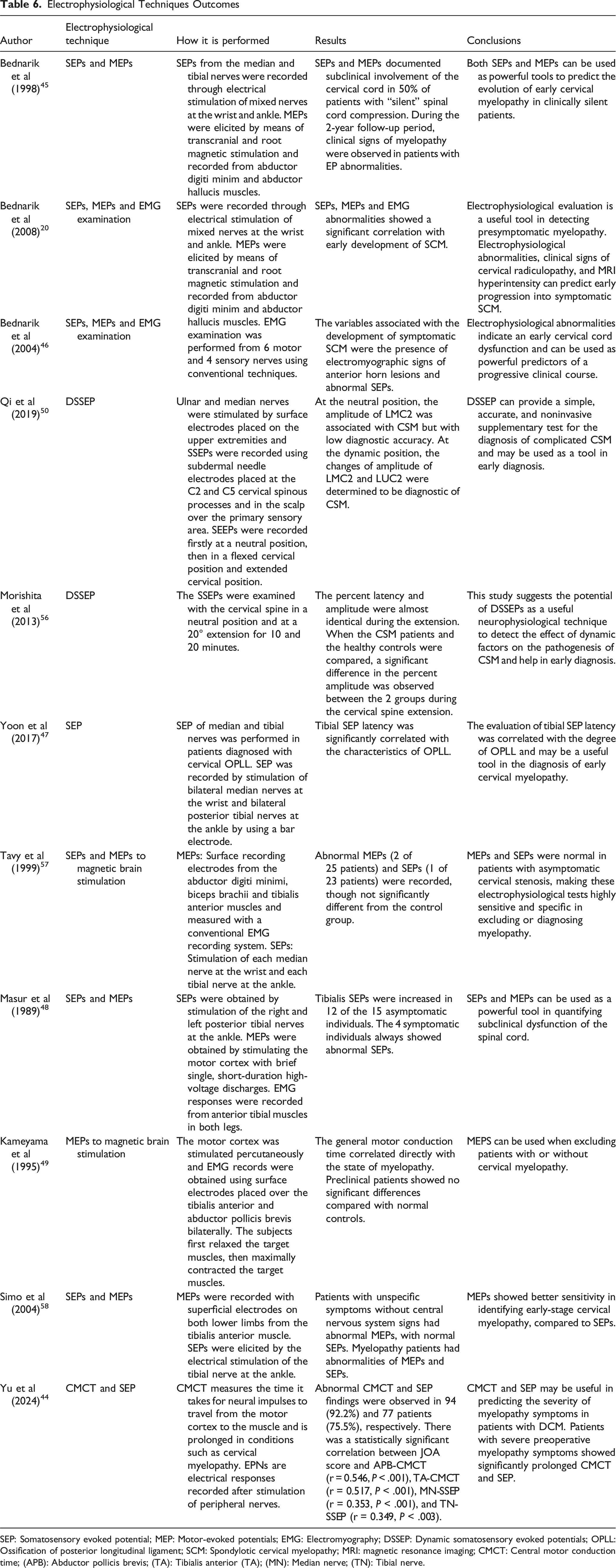
Electrophysiological Measures
Among the 11 articles included, 6 evaluated SEPs and MEPs, 2 assessed Dynamic Somatosensory Evoked Potentials (DSSEPs), and 2 examined SEPs and MEPs with magnetic brain stimulation. SEPs and MEPs consistently showed promising results for assessing cervical cord dysfunction and predicting the evolution of early DCM.20,44-48
Magnetic brain stimulation of MEPs revealed that preclinical patients did not show significant differences compared to normal controls, suggesting that while they can be useful for distinguishing between patients with and without cervical myelopathy, they may not be suitable for evaluating preclinical myelopathy. 49
Electrophysiological Techniques and Patient Characteristics
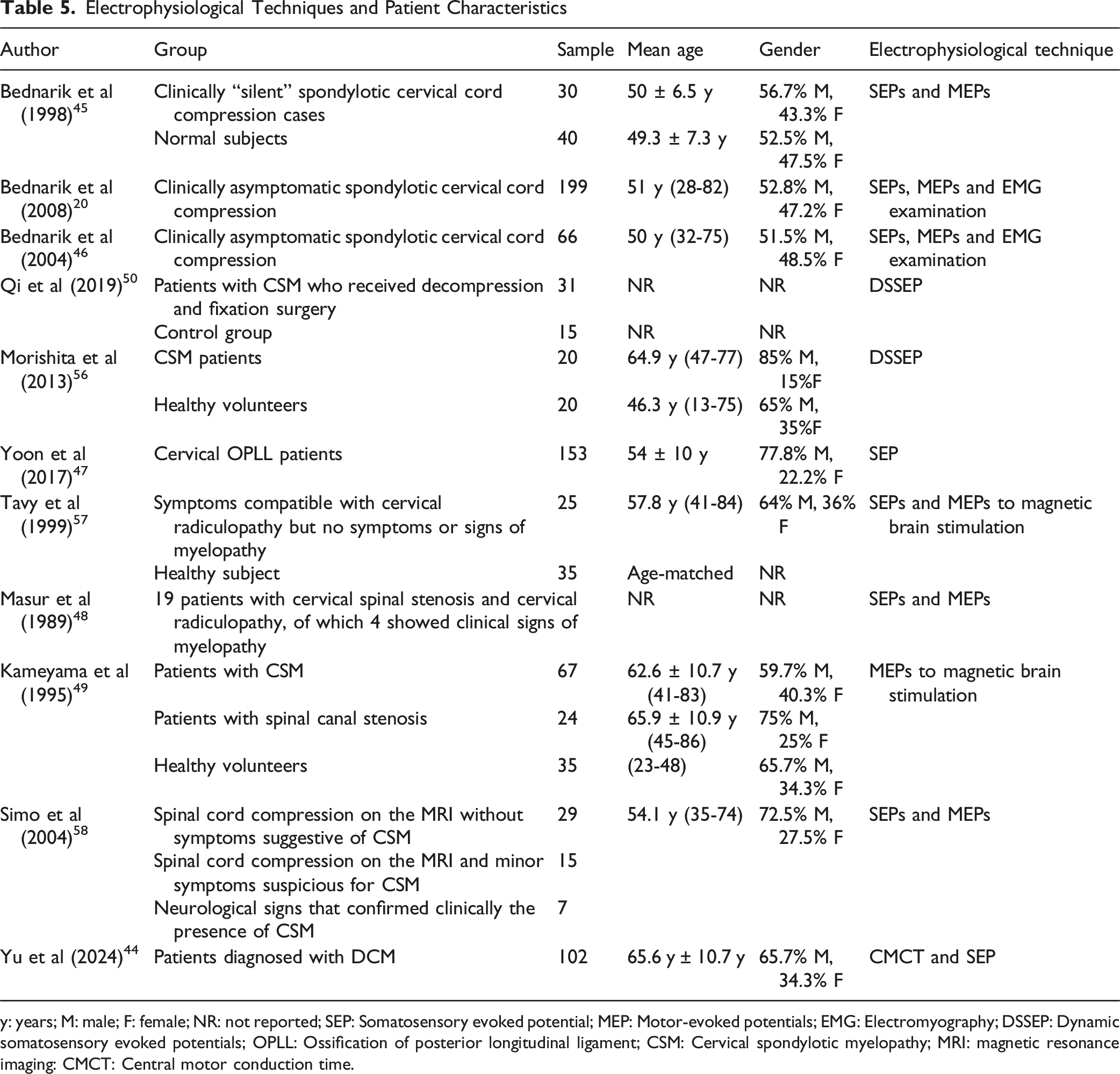
y: years; M: male; F: female; NR: not reported; SEP: Somatosensory evoked potential; MEP: Motor-evoked potentials; EMG: Electromyography; DSSEP: Dynamic somatosensory evoked potentials; OPLL: Ossification of posterior longitudinal ligament; CSM: Cervical spondylotic myelopathy; MRI: magnetic resonance imaging: CMCT: Central motor conduction time.
Electrophysiological Techniques Outcomes
SEP: Somatosensory evoked potential; MEP: Motor-evoked potentials; EMG: Electromyography; DSSEP: Dynamic somatosensory evoked potentials; OPLL: Ossification of posterior longitudinal ligament; SCM: Spondylotic cervical myelopathy; MRI: magnetic resonance imaging; CMCT: Central motor conduction time; (APB): Abductor pollicis brevis; (TA): Tibialis anterior (TA); (MN): Median nerve; (TN): Tibial nerve.
Discussion
This study aimed to review the literature on the diagnosis of DCM, emphasizing the importance of early clinical signs and innovative radiological and electrophysiological methods. An earlier and more accurate diagnosis of the disease enables timely treatment, helping clinicians identify patients at risk of myelopathy or those exhibiting mild signs of DCM, ultimately enhancing clinical outcomes.
DCM is often called one of the great mimickers in medicine because of its varied symptoms and difficult diagnosis. 59 Even though it is a well-acknowledged disease, being first described in 1956 by Clarke and Robinson as the evolution of cervical spondylosis, there have been no significant advancements in the ability to achieve an early diagnosis of the condition over the past few decades. 60 Incorrectly diagnosing DCM can have devastating outcomes for both individuals and society, with rising social costs annually.5,61,62 As DCM is age-related, its incidence and prevalence are expected to increase with the aging population, making it an increasingly significant issue. 63
Decompressive surgery is the standard treatment for clinical DCM, but most patients are diagnosed in advanced stages, leading to limited postoperative improvement and mostly halting disease progression. 64
On the other hand, as shown by a study that analyzed data from the Swedish national spine registry, it is clear that decompressive treatment in patients with DCM, both young and elderly, shows reasonable recovery rates that justify the choice of a surgical approach to the condition. 65
For this reason, in recent years, various efforts have been made to identify effective methods for early diagnosis of DCM. 66 Functional outcome measures, such as the Japanese Orthopaedic Association (JOA) and modified mJOA, are commonly used to assess neurological status, though they rely on subjective patient reports and can be influenced by other disabilities, potentially leading to bias and inaccurate conclusions.67,68 Clinical signs like Hoffmann’s, Lhermitte’s, and Babinski’s are commonly used in the diagnosis of DCM,21-23 but they often appear only in advanced stages and have variable sensitivity in diagnosing the condition. 69 DCM often manifests with characteristic hand dysfunctions, known as “myelopathy hand,” resulting from reflex and motor neuron pathway involvement. 70 In the present study, several tests assessing finger coordination and hand strength, including variants of Hoffmann’s test, have been shown to effectively identify early DCM and exclude cervical myelopathy, with high negative predictive values compared to standard tests.26-28
In particular, Cook et al showed how the presence of a positive Hoffman’s test, positive Babinski test, inverted supinator sign, and gait deviation represent valid clinical criteria for confirming the presence of cervical myelopathy. 33 With regard to clinical signs, it can be noted that, in the study by Raju et al, the maximal voluntary isometric contractions (MVIC) of the ankle plantar flexors and the MVIC of the knee extensors were significant predictors of gait and balance function in pre-surgical patients with DCM. 34 Finally, it was observed that the 10-second grip and release test was moderately correlated with balance measures. 25
These non-invasive clinical signs, including those for the lower limbs, should be incorporated into routine clinical practice, especially for patients over 50, to detect DCM in both its preclinical and mild phases.
Routine MRIs, especially T2WI, are the standard for diagnosing DCM, but they often show alterations in later stages of the disease, where recovery is usually not possible. 16 To address this issue, DTI has been developed, using water molecule diffusion to assess white matter integrity, and it proved to be valuable not only for spinal conditions but also for diagnosing various neurological and psychiatric disorders.71,72 Changes in fractional anisotropy (FA) and apparent diffusion coefficient (ADC) values indicate degenerative spinal changes, particularly at the stenotic level, reflecting conditions like disc degeneration and spinal canal narrowing that could lead to clinical DCM 73 and DCM. 53 Moreover, DTI can assess various biomolecular factors in the spinal cord during chronic damage, such as ischemic injury, excitotoxicity, and cellular apoptosis, often detecting abnormalities before they appear on conventional T2WI-MRI images. 74 Given its effectiveness in detecting early cervical spinal changes, DTI could be used during the preclinical phase of DCM in patients with positive T2WI-MRI signs but no symptoms, to confirm the diagnosis. Furthermore, the widespread adoption of DTI could lower costs and make it a potential preventive tool for certain age groups in the future.75,76
In particular, Seif et al showed how microstructural measurements, performed using DTI, distinguished more pronounced tract-specif neurodegeneration in patients with traumatic spinal cord injury (tSCI) compared to patients with DCM. 51
In any case, even when equipped with excellent diagnostic tools, the diagnostic process for the condition in question is often flawed by the time lost by patient in the long journey between the general practitioner, the performance of the required diagnostic tests, and finally the definitive diagnosis made by the spine surgeon. 77 Analysis of this process lays the foundations for possible future healthcare initiatives aimed at reducing the time lost, with the ultimate goal of making a diagnosis that is both early and rapid.
Regarding radiological techniques, dynamic MRI showed a significant improvement in the diagnostic reliability and accuracy of DCM. 54 Furthermore, MRI scans revealed a significant correlation between Modc changes (MC) and degeneration in facet joints at the same level. 52
Dynamic factors in DCM cause spinal cord compression: flexion leads to impingement by osteophytes or disc protrusions, while hyperextension compresses it between the vertebral body and posterior structures.78,79 Repetitive neck movements may accelerate degenerative changes in the cervical spine, ultimately leading to DCM. 80 To aid in early diagnosis, CMCT is being investigated as a radiological tool to assess the impact of dynamic motion and detect intersegmental instabilities contributing to DCM. 81 The included article by Funaba et al found that excessive anterior displacement of the vertebral bodies during extension, along with stiffness and contracture during flexion, may be linked to limb dysfunction. 43 However, further research is needed to confirm the clinical value of CMCT in the early detection of DCM.
Electrophysiological and neurophysiological examinations provide a non-invasive assessment of central and peripheral neural pathway integrity, aid in differentiating neuromuscular disorders, and can detect early spinal cord dysfunctions with high negative predictive value, helping predict outcomes and rule out DCM in patients.82-85 Bednarik et al found that abnormalities in MEPs and SEPs are positively correlated with the onset of symptoms and clinical signs, concluding that both tests are powerful tools for predicting the progression of early DCM in asymptomatic patients. 45 Several studies in this review highlight the value of non-invasive electrophysiological measures in the early diagnosis of DCM, particularly in the preclinical phase, serving as complementary tests to confirm myelopathy in patients with T2WI alterations but no clear clinical signs, thereby guiding appropriate treatment decisions.19,57
In particular, Yu et al highlighted how CMCT and SSEPs (or SEPs) can be useful in predicting the severity of myelopathy symptoms in patients with DCM, and that pre-operative patients with myelopathy symptoms showed significantly prolonged CMCT and SSEPs. 44
Recent electrophysiological techniques, such as contact heat-evoked potentials (CHEPs) and laser-evoked potentials (LEPs), have been explored to detect early spinothalamic tract alterations and are primarily used to assess sensory nerve conduction damage after traumatic spinal cord injury, showing superiority over SEPs.19,86 Despite their promise, research on the use of these techniques in chronic central neurological conditions like DCM remains limited, underscoring the need for further investigation.87,88
In this systematic review, we analyzed the potential of DTI in the early diagnosis of degenerative processes affecting the cervical spine. The mJOA scale, clinical signs in the lower limbs, and electropysiological measurements are useful tools for monitoring the evolution and symptomatic improvement of patients treated with decompression surgery. On the other hand, it is clear that these tools must be used together in order to improve not only diagnostic process but also the post-operative evaluation of patients with CSM.
Strengths and Limitations
A strength of this review is the similarity in the mean age of participants across all studies, leading to a more homogeneous population. However, the study has several limitations, including the potential bias from observer-reported or self-reported tools used to assess results and outcomes across the included articles. Additionally, the limited number of studies, particularly those examining dynamic factors in DCM patients, is a constraint. Furthermore, the data on early clinical signs are highly heterogeneous, as they cover a variety of distinct signs with the common objective of evaluating their effectiveness in diagnosing DCM early.
Nevertheless, to the best of available knowledge, this study is the only comprehensive systematic review in the literature that evaluates clinical signs, radiological, and electrophysiological alterations for the early diagnosis of DCM.
Conclusion
DCM exhibits a highly variable clinical, radiographic, and electrophysiological profile, which complicates its diagnosis. This systematic review has brought attention back to clinical evaluations that were previously underused, despite their potential for earlier DCM detection compared to standard clinical signs. DTI shows promise in detecting early degenerative changes in the cervical spine, and its broader use could improve outcomes, reduce long-term costs, and potentially be applied preventively in certain age groups. Additionally, electrophysiological measures, due to their simplicity, accuracy, and non-invasive nature, should be integrated as supplementary diagnostic tools from the preclinical phase of DCM and enhanced by dynamic evaluations. A comprehensive, multi-modal approach to diagnosing DCM should incorporate the tests highlighted in this review to enhance the standard of care for this prevalent and challenging condition.
Footnotes
Author Contribution
Conceptualization, F.R., P.B.; methodology, G.F.P., P.B., F.R., P.F.; validation, F.R., G.F.P. R.P., G.V., V.D.; formal analysis, G.F.P., P.B. and P.F.; investigation, P.B., P.F., G.F.P.; data curation, G.F.P, P.B., N.F., P.F.; writing—original draft preparation, P.B., G.F.P., F.R., N.F.; writing—review and editing, F.R., G.F.P.; visualization, R.P., V.D.; supervision, G.V., R.P. and V.D.; project administration, R.P. and V.D.; funding acquisition, R.P., and V.D. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.