
Abstract
Study Design
Retrospective
Objective
To evaluate preoperative cervical range-of-motion via cervical flexion-extension radiographs and its relation to the development of PJK/PJF following ASD correction in patients with a UIV in the upper thoracic spine.
Methods
Patients with an UIV between T1-T4, preoperative cervical flexion/extension radiographs and instrumented to the pelvis, and minimum 1yr follow-up were included. Cervical measurements included range-of-motion (ROM), flexion, extension and cervical SVA (cSVA). Patients were stratified into 3 groups: No-PJK, asymptomatic PJK (A-PJK) and symptomatic PJK including PJF (S-PJK/PJF).
Results
151 patients were included: Mean age 59.6 ± 8.0 yrs, BMI of 25.1 ± 4.5, 88.7% (n = 134) were female. PJK status: No PJK = 111 (73.5%) patients, A-PJK = 21 (13.9%), S-PJK/PJF = 19 (12.6%). S-PJK/PJF patients, however, were more likely to be diagnosed with osteopenia/osteoporosis(S-PJK/PJF: 68.4% vs A-PJK: 23.8% vs No PJK: 52.3%, P = 0.0138). S-PJK/PJF patients had significantly less cervical flexion (No PJK: 19.5 ± 14.2 vs A-PJK: 19.9 ± 10.9 vs S-PJK/PJF: 7.7 ± 11.9, P = 0.0029) and ROM than the other groups (No PJK: 52.8 ± 17.7 vs A-PJK: 53.1 ± 14.5 vs S-PJK/PJF: 39.2 ± 17.9, P = 0.0085). On multivariable models for the development of S-PJK/PJF, reduced baseline cervical flexion and ROM were independent risk factors yielding threshold values of 22.8° and 48.2°, respectively.
Conclusion
Multivariable models for the development of S-PJK/PJF demonstrated that reduced baseline cervical ROM and flexion were independent risk factors yielding threshold values of 48.2° and 22.8°, respectively. All of S-PJK/PJF patients had preop flexion <22.8°. Flexion-extension radiographs provide a quick and easy option at a relatively low cost to offer additional information that may aid in surgical planning and shared decision making with the patient regarding potential outcomes.
Keywords
Introduction
Surgical correction of adult spinal deformity (ASD) is technically challenging with an inherent high risk profile for both intraoperative and postoperative complications, some of which result in the need for reoperations.1-6 One of the more challenging complications to prevent, as well as treat, continues to be proximal junctional kyphosis (PJK).7-12 The incidence of PJK ranges between 20-40%11,13-15 and can be either an asymptomatic radiological finding or have a large negative impact the patients’ quality of life with anything in between.16-20 The more extreme end of the PJK spectrum can result in a combination of bony or instrumentation failure with possible neurological deficits leading to the need for revision surgery; termed proximal junctional failure (PJF).10,21 Therefore, identifying patients prior to the operation that will have a successful outcome with minimal or no complications is crucial but also incredibly difficult. Several studies to date have identified risk factors for PJK/PJF yet there is always a need to better understand this phenomenon in order to reduce its incidence.
Risk factors for the development of PJK following ASD correction are numerous and some of which include an age greater than 55 years,8,18,21,22 larger magnitude of deformity correction,8,14,22,23 posterior and anterior-posterior approaches,8,13,18,24 non-anatomic restoration of thoracic kyphosis,13,25 low bone mineral density (BMD), 24 presence of a comorbidity, 8 and high body mass index (BMI).8,21 In general, the literature supports that an upper-most instrumented vertebra (UIV) in the UT spine has a lower chance of developing PJK/PJF when compared to a UIV in the lower thoracic spine,26-29 however, there are also mixed results showing equivalent rates of PJK. 14 Moreover, the mode of failure has been shown to differ based on the UIV with thoracolumbar failures more likely due to bony fracture and upper thoracic UIV failures are more likely a result of soft-tissue failure. 30 This begs the question if there is something inherent to the cervical spine that may place patients at higher risk for PJK/PJF with a UIV in the upper thoracic spine, such as baseline cervical range-of-motion (C-ROM).
C-ROM is typically measured via flexion-extension radiographs31,32 and these are used in a wide range of clinical applications such as evaluating trauma,33,34 degenerative conditions,32,35 and pseudarthosis. 36 The cervical spine will undergo reciprocal changes in sagittal alignment following thoracolumbar deformity correction37,38 and the sagittal malalignment of the cervical spine can affect the thoracolumbar alignment and clinical outcomes as well.39,40 However, it remains unknown if the dynamics of the cervical spine are related to the behavior of the UT proximal junction with regards to the development of PJK/PJF. Therefore, the goal of the present study was to evaluate preoperative C-ROM via cervical flexion-extension radiographs and its relation to the development of PJK/PJF following ASD correction in patients with a UIV in the UT spine.
Methods
Study Population
This is a single-center, single-surgeon retrospective analysis focused on adult patients who underwent surgical treatment for adult degenerative or idiopathic spinal deformity from 2015-2021 with a minimum of 1 year follow up. Inclusion criteria included an UIV between T1-T4, inclusive, having had a cervical flexion/extension radiographs done prior to the preoperative visit, and instrumented to the pelvis. The choice of surgical approach, techniques, such as posterior column osteotomies (PCO), three-column osteotomies (3CO), and the use of interbody fusions were made at the discretion of the operating surgeon. Both primary and revision cases were included in this analysis. Patients lost to follow-up, without postoperative full-length radiographs, and/or without cervical flexion/extension radiographs were excluded from the study.
Radiographic Analysis and Data Collection
Patient characteristics included age, BMI, gender, history of smoking, diagnosis of osteopenia/osteoporosis, and history of prior cervical spine surgery. Operative data included the total instrumented level (TIL) and UIV designation.
Full-length standing radiographs captured on the EOS 2D/3D imaging system were collected at the preoperative and follow-up visits. Sagittal radiographic parameters including T2-T12 thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), spinopelvic mismatch (PI-LL), the C7 sagittal vertical axis (SVA), and the proximal junctional angle (PJA) were collected at baseline and follow-up. The PJA was defined as the Cobb measurement between the cranial endplate of the UIV to the cranial endplate 2 vertebrae above as denoted in prior studies9,16
Cervical flexion/extension radiographs, which captures the skull, cervical spine, and upper thoracic spine in a neutral, flexion, and extension position to clinically assess the stability of the cervical spine 41 was collected at the preoperative visit. Cervical radiographic parameters including cervical lordosis (CL), cervical flexion (CF), cervical extension (CE), C2-C7 SVA (c-SVA), and the T1 slope was collected at and evaluated at baseline. Cervical flexion and extension were measured as the angular difference from the neutral position using standard Cobb angle techniques between C2-C7 on flexion-extension radiographs. In terms of quantifying the lordotic and/or kyphotic behaviors of the cervical spine, a negative value designation was given to indicate CL and extension while a positive value designation was given to indicate cervical kyphosis and flexion. Both cervical flexion and extension were defined as the motion measured from the neutral position. The total C-ROM was calculated through the difference between the flexion and extension measurements.
Outcome Measures
The primary outcome of interest in this study was to determine whether greater C-ROM was protective against PJK among patients instrumented to the pelvis with an upper thoracic UIV (T1-T4). The secondary outcome of interest was to identify whether a threshold for C-ROM can be identified. We defined radiographic PJK as a PJA ≥10° and a ΔPJA ≥10° from the preoperative visit.9,16 However, radiographic PJK can present among patients asymptomatically. Thus, patients were divided into 3 cohorts on whether they did not develop PJK, developed asymptomatic PJK (A-PJK), or symptomatic PJK/PJF (S-PJK/PJF). We defined S-PJK/PJF as patients who presented with radiographic PJK, complained of extensive pain near the UIV, and/or were revised due to PJK/PJF.
Statistical Analyses
Continuous variables were compared using a one-way analysis of variance (ANOVA). When comparing the cervical parameters between the 3 cohorts, ANOVA was followed by a post-hoc Tukey test to discern significant pairwise comparisons. Categorical variables were compared using chi-squared/fisher’s exact test (wherever applicable). Pearson’s correlation coefficients, adjusting for multiple comparisons, were utilized to conduct a sensitivity analysis to assess for patient, surgical, and/or radiographic variables associated with the development of S-PJK/PJF. A multivariable logistic regression analysis was then preformed to assess the effect of C-ROM on the development of S-PJK/PJF, adjusting for the significant variables denoted in the sensitivity analysis. The variance inflation factor (VIF) was utilized to measure the amount of multicollinearity that existed among the independent variables included in the regression analysis. Variables with a VIF >10 were excluded to improve model diagnostics and reliability. Following the regression analysis, the youden index was used to calculate the optimal cutoff/threshold that can be utilized. Statistical significance was defined by the two-sided test with a P-value <0.05. All statistical analyses were conducted using SAS (SAS 9.4, SAS Institute Inc, Cary, NC, USA).
Results
Patient Sample and Comparison of Sample Characteristics
Comparison of Patient and Operative Characteristics Between No PJK, Asymptomatic PJK, and Symptomatic PJK/PJF
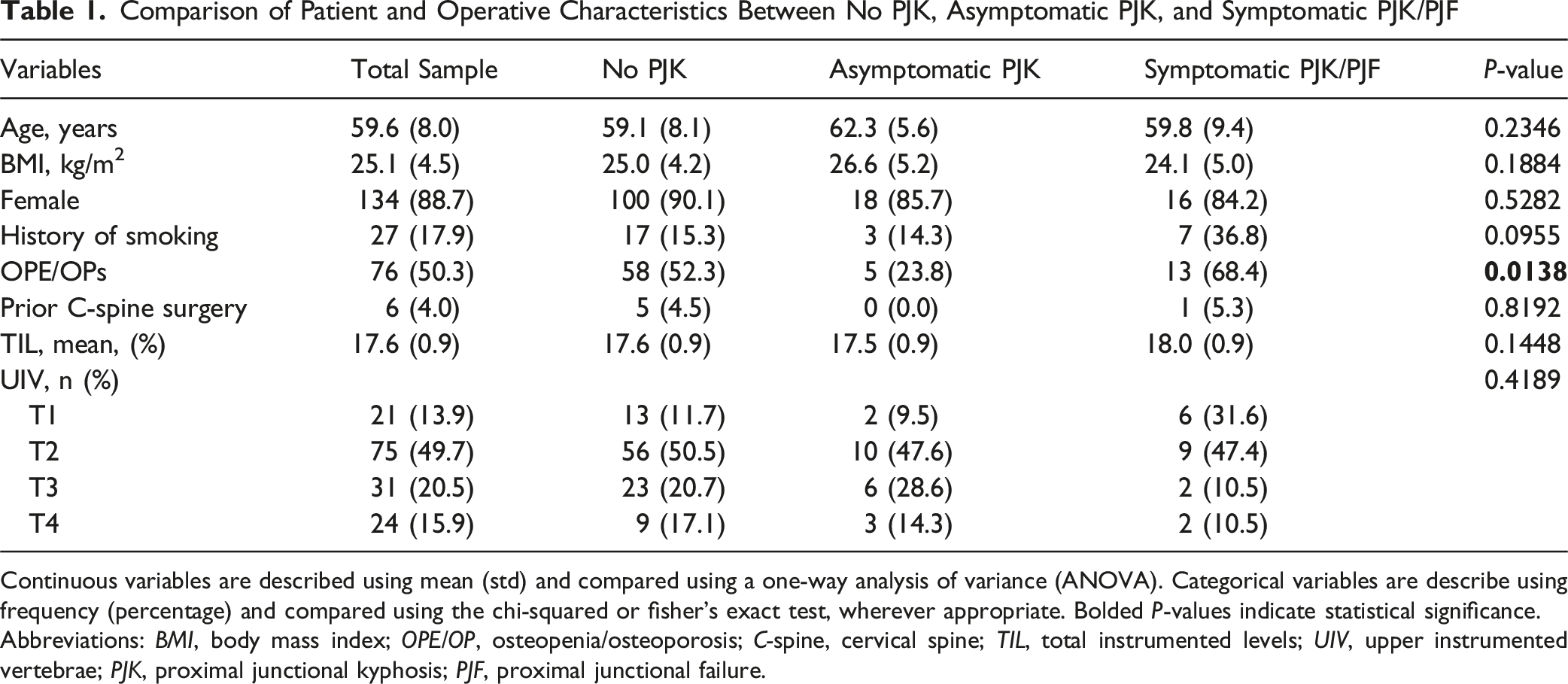
Continuous variables are described using mean (std) and compared using a one-way analysis of variance (ANOVA). Categorical variables are describe using frequency (percentage) and compared using the chi-squared or fisher’s exact test, wherever appropriate. Bolded P-values indicate statistical significance.
Abbreviations: BMI, body mass index; OPE/OP, osteopenia/osteoporosis; C-spine, cervical spine; TIL, total instrumented levels; UIV, upper instrumented vertebrae; PJK, proximal junctional kyphosis; PJF, proximal junctional failure.
Patients were stratified depending on their PJK status: No PJK = 111 (73.5%) patients, A-PJK = 21 (13.9%) patients, and S-PJK/PJF = 19 (12.6%) patients. There were no significant differences between the 2 groups in terms of age, BMI, gender composition, and history of cervical spine surgery (P > 0.05). S-PJK/PJF patients, however, were more likely to be diagnosed with osteopenia/osteoporosis (S-PJK/PJF = 68.4% vs A-PJK = 23.8% vs No PJK = 52.3%, P = 0.0138). Although S-PJK/PJF cohort consisted of more patients with a history of smoking, this observation was not statistically significant (P = 0.0955). Operatively, there were no differences in total instrumented levels and UIV designation (P > 0.05) (Table 1).
Comparison of Cervical and Sagittal Radiographic Parameters
Comparison of Preoperative Cervical Radiographic Parameters Between No PJK, Asymptomatic PJK, and Symptomatic PJK/PJF
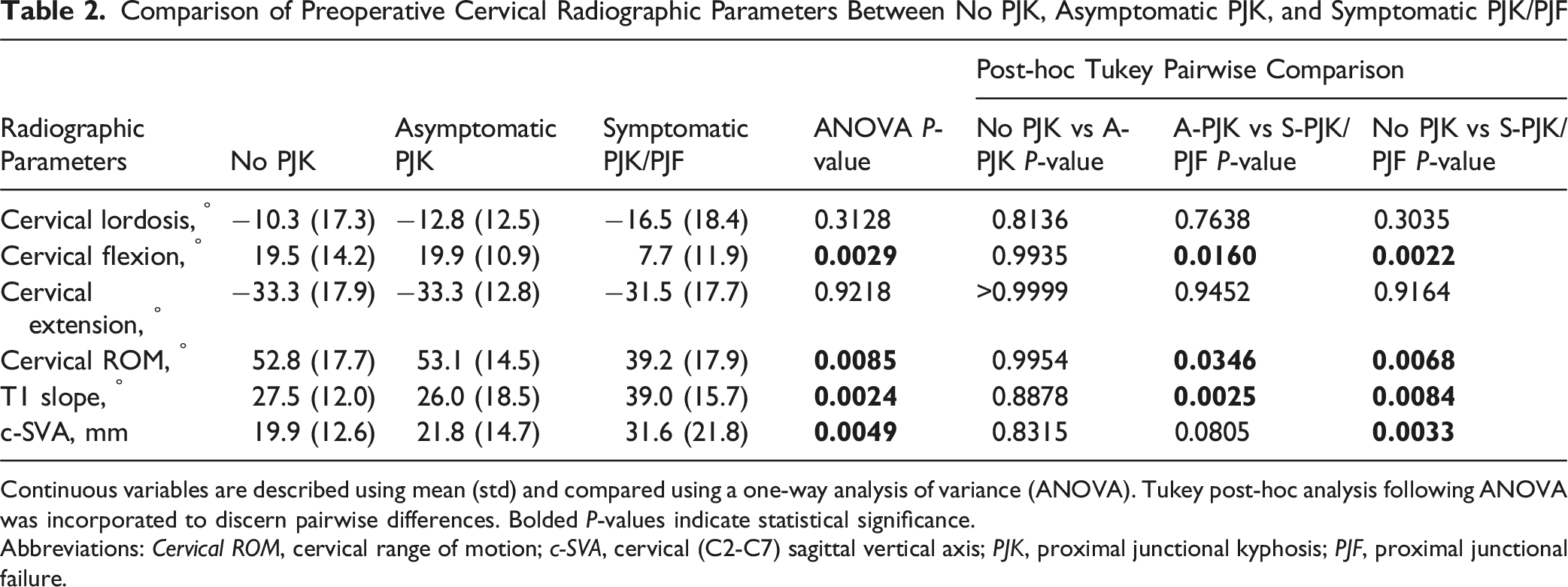
Continuous variables are described using mean (std) and compared using a one-way analysis of variance (ANOVA). Tukey post-hoc analysis following ANOVA was incorporated to discern pairwise differences. Bolded P-values indicate statistical significance.
Abbreviations: Cervical ROM, cervical range of motion; c-SVA, cervical (C2-C7) sagittal vertical axis; PJK, proximal junctional kyphosis; PJF, proximal junctional failure.
Comparison of Preoperative, Immediate Postoperative, and Final Follow up Radiographic Parameters Between No PJK, Asymptomatic PJK, and Symptomatic PJK/PJF
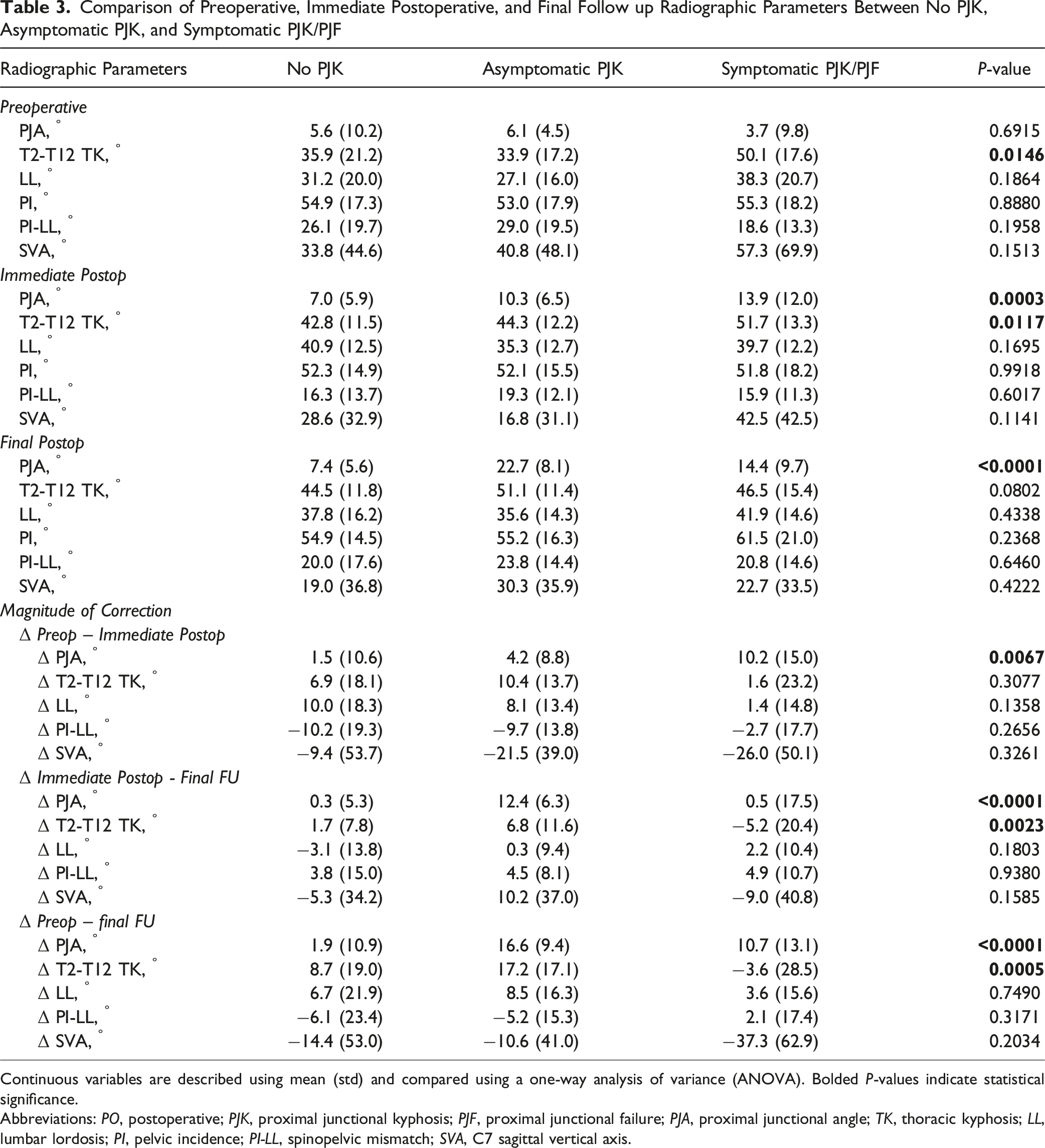
Continuous variables are described using mean (std) and compared using a one-way analysis of variance (ANOVA). Bolded P-values indicate statistical significance.
Abbreviations: PO, postoperative; PJK, proximal junctional kyphosis; PJF, proximal junctional failure; PJA, proximal junctional angle; TK, thoracic kyphosis; LL, lumbar lordosis; PI, pelvic incidence; PI-LL, spinopelvic mismatch; SVA, C7 sagittal vertical axis.
Cervical Risk Factors Associated With Symptomatic PJK
Unadjusted and Adjusted Logistic Regression Analyses for Radiographic Parameters Associated With the Development of Symptomatic PJK
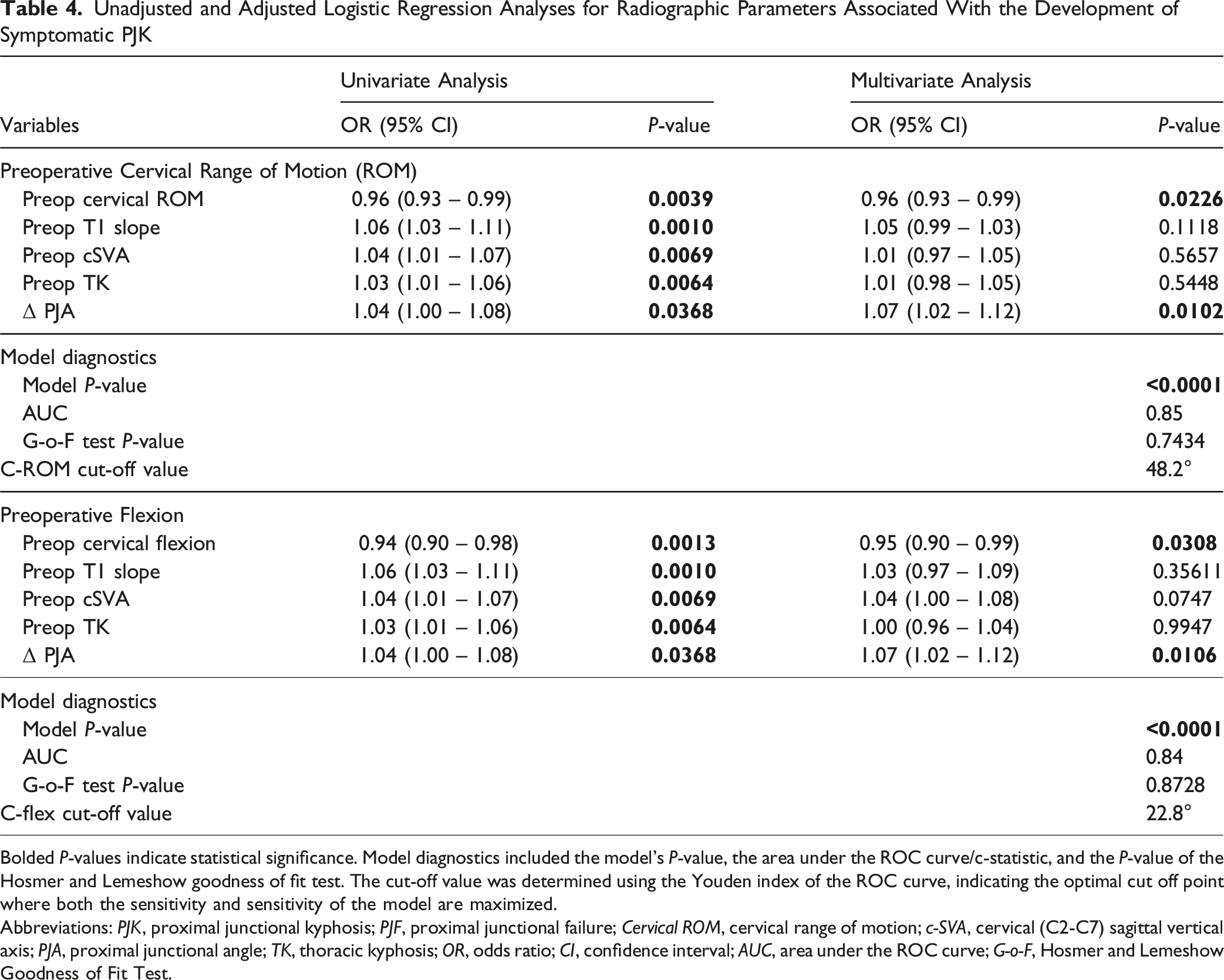
Bolded P-values indicate statistical significance. Model diagnostics included the model’s P-value, the area under the ROC curve/c-statistic, and the P-value of the Hosmer and Lemeshow goodness of fit test. The cut-off value was determined using the Youden index of the ROC curve, indicating the optimal cut off point where both the sensitivity and sensitivity of the model are maximized.
Abbreviations: PJK, proximal junctional kyphosis; PJF, proximal junctional failure; Cervical ROM, cervical range of motion; c-SVA, cervical (C2-C7) sagittal vertical axis; PJA, proximal junctional angle; TK, thoracic kyphosis; OR, odds ratio; CI, confidence interval; AUC, area under the ROC curve; G-o-F, Hosmer and Lemeshow Goodness of Fit Test.
Given that CF was the component of the C-ROM that differed significantly between the groups, a second model was devised to assess the association of CF on the development of S-PJK/PJF. After controlling for the aforementioned variables, each degree increase in preoperative CF was associated with a 1.05x odds of not developing S-PJK/PJF (OR = 0.95, P = 0.0308, model P < 0.0001, AUC = 0.84). The calculated youden index of the ROC curve discerned the optimal CF to be 22.8° (Table 4).
Comparison of the Frequency of Patients Who Were Above and Below the Calculated Cutoffs for Preoperative Cervical Range of Motion and Flexion
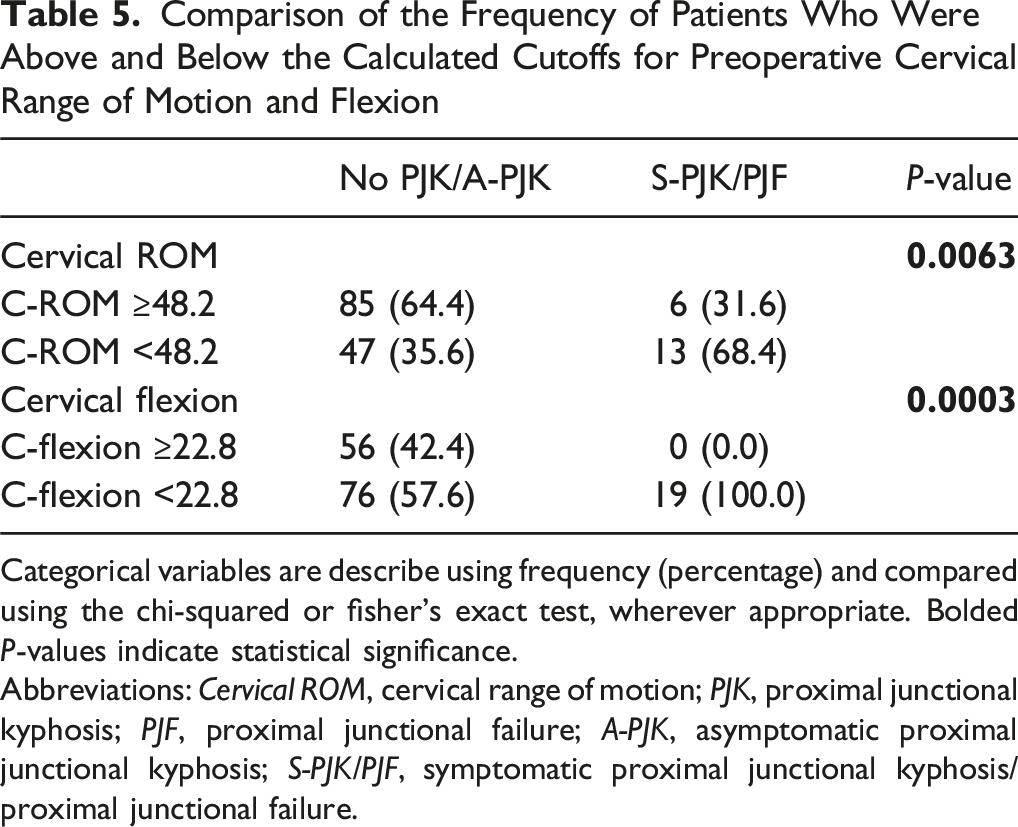
Categorical variables are describe using frequency (percentage) and compared using the chi-squared or fisher’s exact test, wherever appropriate. Bolded P-values indicate statistical significance.
Abbreviations: Cervical ROM, cervical range of motion; PJK, proximal junctional kyphosis; PJF, proximal junctional failure; A-PJK, asymptomatic proximal junctional kyphosis; S-PJK/PJF, symptomatic proximal junctional kyphosis/proximal junctional failure.

Case 1: No PJK. Preoperative flexion (up) and extension lateral cervical radiographs demonstrating 30.5 degrees of flexion and 58.7 degrees of extension for a total range of motion of 89.2 degrees. Preoperative anteroposterior (center) and lateral (right) standing radiographs demonstrating 46°, 84°, and 38° thoracic, lumbar, and fractional lumbar sacral curves, respectively, in the coronal plane, and 75° of thoracic hyperkyphosis and 56° of lumbar lordosis with 40° of pelvic incidence in the sagittal plane
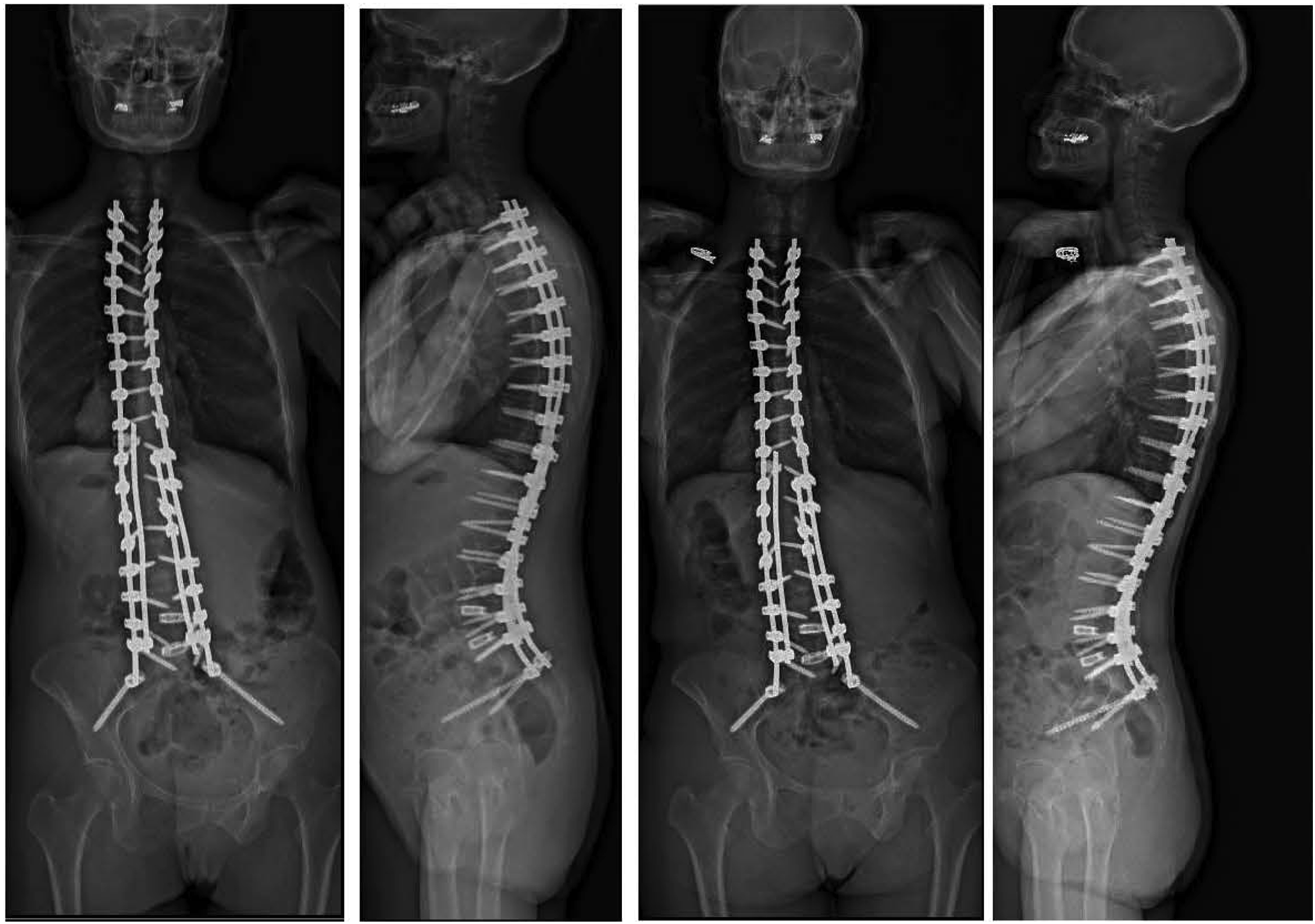
Case 1: No PJK. Postoperative anteroposterior and lateral standing radiographs prior to discharge (left) and at 2 years follow up (right) demonstrating normal alignment without PJK

Case 2: PJK. Preoperative flexion and extension lateral cervical radiographs demonstrating 14.8 degrees of flexion and 12.5 degrees of extension for a total range of motion of 27.3 degrees, which is below the calculated thresholds of 22.8 for flexion and 48.2 for overall range of motion. Preoperative anteroposterior (center) and lateral (right) standing radiographs demonstrating 25°, 50°, and 31° thoracic, lumbar, and fractional lumbar sacral curves, respectively, in the coronal plane, and 56° of thoracic hyperkyphosis and 63° of lumbar lordosis with a pelvic incidence of 75° in the sagittal plane
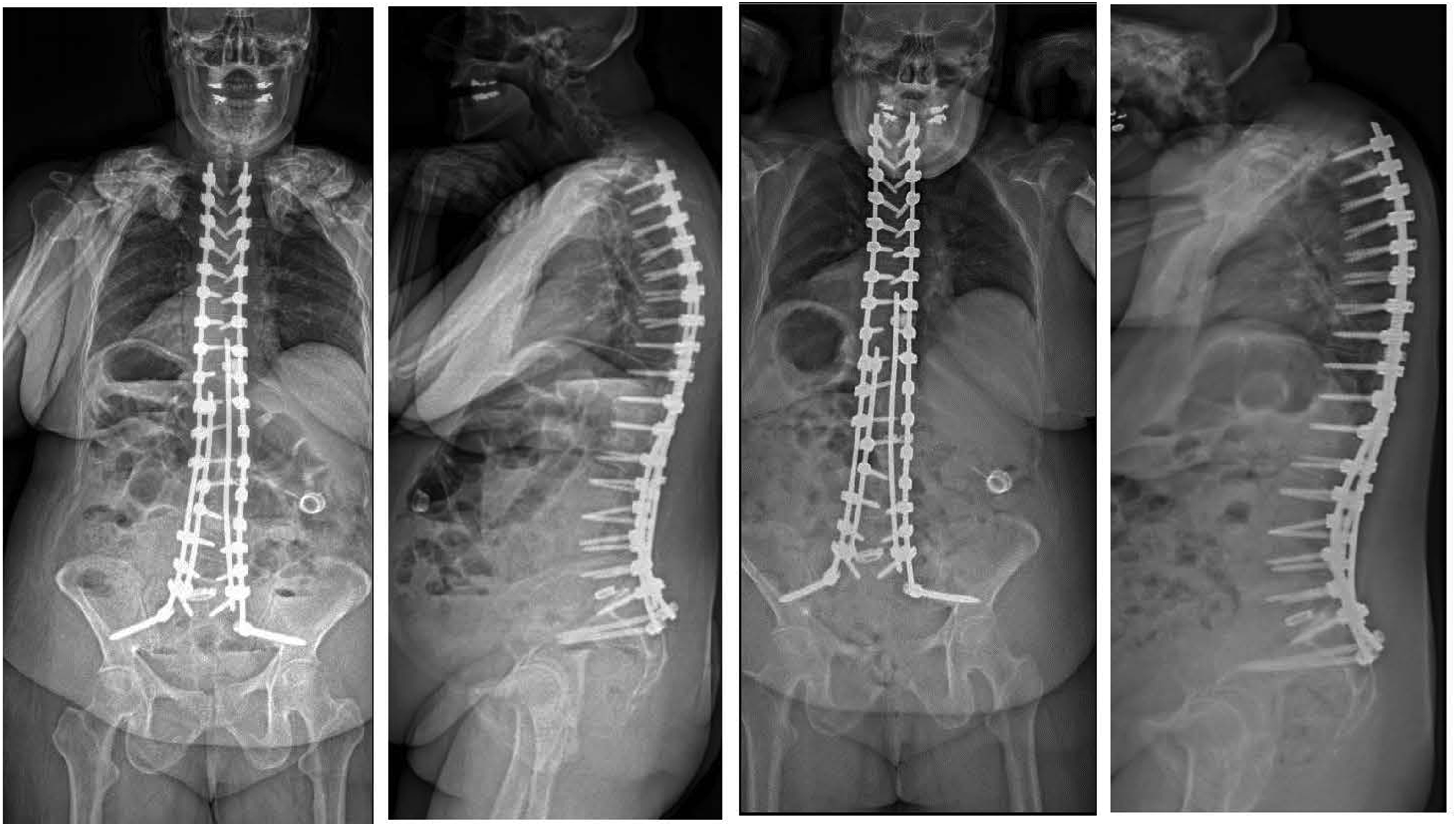
Case 2: PJK. Postoperative lateral standing radiographs prior to discharge (Left) and at 2 years follow up (right) demonstrating PJK
Discussion
Despite the large number of risk factors that have been identified, PJK/PJF is still a significant concern. Every effort should be made to not only better understand the potential causes of this phenomenon but also to find ways in which it can be predicted and then ultimately avoided. Hence, this is the first study of its kind investigating the relationship of cervical ROM and the development of PJK/PF following spinal deformity correction with long constructs to the UT spine. The present study demonstrated that preoperative CF and C-ROM was significantly less for the patients that developed S-PJK/PJF from both those that did not develop PJK and those with A-PJK. In addition, the T1 slope and c-SVA were also higher for the S-PJK/PJF group. On multivariable models for the development of S-PJK/PJF, reduced baseline C-ROM and flexion were independent risk factors yielding threshold values of 48.2° and 22.8°, respectively. Our results suggest that reduced cervical mobility may limit the ability of the unfused spine to dissipate mechanical loads, thereby concentrating stress at the proximal junction and predisposing this region to mechanical failure.
C-ROM evaluation is typically conducted via flexion-extension radiographs and these have been used in a wide variety of clinical applications including trauma,33,34 degenerative conditions,32,35 and pseudarthosis. 36 The present study shows for the first time that reduced ROM, specifically flexion, was significantly related to developing PJK following surgical correction of ASD with a UIV in the UT region. The decreased ROM could be due to a number of reasons, one of which could be significant cervical spine degeneration. It has been shown that for degenerative disc disease of the cervical spine, the flexion-extension range of motion initially increases with lower grade disc degeneration and then decreases with higher grades. 42 The reduced C-ROM in the deformity patients could be a marker for degeneration at or near the UIV junction resulting in a rigid transition zone between the UIV and non-instrumented spine and also potentially compromised tissue integrity from the degeneration itself. All of which could lead towards a high risk of developing PJK. Global spinal rigidity in ASD patients is a known risk factor for developing PJK in the thoracolumbar spine. Eaton et al studied the global flexibility of the spine, defined as the difference in C7SVA from standing and supine spinal imaging, and its relation to PJK development in thoracolumbar deformity patients. 43 The authors found that spinal rigidity was an independent risk factor for the development of PJK following deformity correction. 43 The hypothesis is that patients with a rigid spine, and thus a rigid UIV junction, create a potential stress riser at the junction from the large lever arm of the instrumented/fused spine against the non-instrumented spine. This stress riser eventually fails from the cyclic loading of the spine at the junction. In contrast, patients with flexible spines may be able to compensate for the cyclic loading by dissipating the forces more evenly throughout the non-instrumented spine reducing the likelihood of PJK/PJF development. It is unclear as to why extension was not significantly reduced but it may be related to the patients already being near their limit in cervical extension due to compensation from their deformity. The S-PJK/PJF patients had a larger mean baseline cervical lordosis and a significantly larger baseline TK. The increased TK could cause them to have less CE at baseline as they try to maintain horizontal gaze.
In addition to the reduced CF, there were other factors that may have contributed to the development of the PJK/PJF. First, the S-PJK/PJF group had a significantly higher proportion of patients with osteopenia/osteoporosis, which is a risk factor for PJK/PJF. 24 Patients with low BMD may not be able to compensate for the change in forces from the abrupt transition in stiffness at the UIV. Moreover, low BMD could be a marker for poor soft tissue integrity, specifically sarcopenia, and overall frailty of the patient as all 3 of those are related to oneanother. 44 The reduced CF could also be a result of sarcopenia and frailty, however it is difficult to isolate the individual components contributing to developing PJK as osteoporosis, sarcopenia, frailty, cervical spine degeneration are all related to various degrees. Second, the S-PJK/PJF patients had a significantly larger TK at baseline and then had a reduction in TK postoperatively. Both of these factors could have played a role in the development of PJK/PJF. Maruo and colleagues studied 90 ASD patients and found that a preoperative TK of greater than 30° was a risk factor for PJK. 14 All 3 groups in the present study had a mean TK greater than 30 however, the S-PJK/PJF group had a mean that was 20° larger than the other 2 groups. S-PJK/PJF was the only group that had a mean reduction in TK postoperatively. Wang et al investigated 123 AIS patients and found that a reduction of TK >10° was a risk factor for developing PJK. 15 Although the current study population are not adolescents, the idea of TK reduction contributing to PJK in adults could be possible in the setting of larger baseline TK, osteoporosis suggesting possible sarcopenia/frailty, and a rigid spine as evidenced by reduced cervical ROM.
The strengths of the present study include the relatively large sample size of deformity patients being treated at a high-volume center from a single senior highly experienced surgeon as well as its novelty. Cervical flexion-extension radiographs are not typically obtained in the routine preoperative planning for complex ASD surgery. However, the senior author felt this was an important aspect of the patient to capture as many of these surgeries have a UIV in the UT region. However, it is important to note that reduced cervical ROM should not be interpreted as a direct causal factor, but rather as a potential surrogate marker of global spinal stiffness or cervicothoracic junction rigidity. This distinction is critical, as the development of PJK/PJF is multifactorial and likely reflects the interaction between alignment, bone quality, soft tissue integrity, and biomechanical stress at the junction. The underlying cause of reduced preoperative C-ROM warrants dedicated investigation.
The present study is not without limitations with the most important being the retrospective nature of it which lends itself to inherent biases and reduced follow up. While a prospective study to evaluate the efficacy and utility of cervical flexion-extension radiographs as a preoperative tool to predict PJK/PJF is warranted, the present study shows promise and begins the discussion of cervical dynamics and its role in postoperative mechanical complications following long construct spinal deformity correction. Secondly, while the radiographs as demonstrate the ROM well, they do not convey much information regarding etiologies to differences in ROM. An MRI analysis would be beneficial and can provide an in depth look into multiple potentially related factors such as the number of levels and severity of disc degeneration, types and severity of stenosis, the muscle quality, lipid content, and the integrity of the ligamentous complex at the CT junction. In addition, the identified cervical ROM and flexion thresholds were derived from statistical modeling within our institutional cohort and have not been validated in an independent population. This may limit their generalizability, and external validation in multi-center cohorts will be essential to confirm their applicability. Thirdly, the development of PJK/PJF is multifactorial and the present study conducted a relatively limited analysis focusing on basic demographics and a radiological variables. There are likely other factors involved not captured with the present study’s design. Lastly, while we believe the overall sample size was reasonable, the subgroup analyses (A-PJK vs S-PJK/PJF) involved relatively small numbers within each group, which may limit statistical power and should be interpreted with caution. It is also important to note that the study design does not allow determination of whether reduced cervical ROM is causative or simply a marker of underlying pathology.
Conclusion
This is the first study investigating the relationship of C-ROM and the development of PJK/PF following spinal deformity correction with long constructs to the UT spine. Preoperative CF and C-ROM was significantly less for the patients that developed S-PJK/PJF from both those that did not develop PJK and those with A-PJK. Multivariable models for the development of S-PJK/PJF demonstrated that reduced baseline C-ROM and flexion were independent risk factors. Given these results, flexion-extension radiographs provide a quick and easy option at a relatively low cost to offer additional information that may aid in surgical planning and shared decision making with the patient regarding potential outcomes. Further work is needed to better elucidate the etiology of reduced ROM, such as the types and severity of different degeneration and stenosis in the cervical spine and their relation to PJK/PJF development.
Footnotes
Ethical Considerations
AAAQ9598. This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of Columbia University Irving Medical Center approved this study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Justin Scheer, Fthimnir Hassan, Chun Wai Hung, Ted Shi, Nathan Lee, Steven Roth and Alexander Tuchman have no relevant financial or non-financial interests to disclose. Lawrence G. Lenke has received grant support from AO Spine, International Spine Summit Group, Scoliosis Research Society, EOS Technology and Setting Scoliosis Straight Foundation as a study investigator. Ronald A. Lehman has received grant support from the Department of Defense as a study investigator. Zeeshan M. Sardar, Joseph M. Lombardi, Ronald A. Lehman, and Lawrence G. Lenke have received consulting fees from Medtronic. Lawrence G. Lenke has received consulting fees from Acuity Surgical, Momentum Health, and Abryx. Lawrence G. Lenke has received reimbursements from Broadwater, AO Spine, and Scoliosis Research Society for attending meetings/travel. Ronald A. Lehman and Lawrence G. Lenke have received royalties and are patent holders from Medtronic. Cory Walker has received consulting fees from AlphaTec. Joseph M. Lombardi has received consulting fees from Stryker.