
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare pain, disability, and quality-of-life outcomes following anterior cervical discectomy and fusion (ACDF) between elderly and younger patients with degenerative cervical myelopathy (DCM).
Methods
A prospectively maintained institutional registry was reviewed for patients undergoing primary ACDF for DCM between 2005-2014. A total of 219 patients were stratified into Young (<70 years; n = 188) and Elderly (≥70 years; n = 31) cohorts. Patients undergoing surgery for trauma, infection, malignancy, or revision were excluded. Outcomes included VAS neck and limb pain, AAOS Neurogenic Symptoms and Neck Pain & Disability, Neck Disability Index, Japanese Orthopaedic Association score, and SF-36 Physical and Mental Component Summary scores, collected preoperatively and at 6 months and 2 years. Satisfaction and expectation fulfilment were assessed using anchor questions.
Results
Elderly patients had higher rates of hypertension (P = .016), osteoarthritis (P = .034), and longer length of stay (P = .045). Baseline PROMs were comparable, except for higher preoperative limb pain in younger patients (P = .027). At 6 months, younger patients showed greater improvement in limb pain (P = .016), with no other differences. At 2 years, elderly patients had worse neck-related disability (P = .043), lower physical component scores (P = .035), and less improvement in neurogenic symptoms (P = .039). Expectation fulfilment was lower in elderly patients (64.5% vs 80.3%, P = .049), while satisfaction rates were similar.
Conclusions
Elderly patients demonstrated smaller improvements in neurological symptoms, disability, and physical quality of life after ACDF, although both groups showed substantial improvement. These findings suggest that older age is associated with differences in recovery magnitude rather than likelihood of improvement.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is the leading cause of spinal cord dysfunction in adults and can result in progressive neurological impairment and reduced health-related quality of life if untreated. Surgical decompression remains the most effective means of halting neurological decline and restoring function, with large prospective multicenter cohorts demonstrating significant improvement in functional and quality-of-life outcomes following surgery. 1 Among available surgical options, anterior cervical discectomy and fusion (ACDF) is widely utilized for DCM due to its ability to directly address ventral cord compression and achieve reliable decompression and stabilization.
As surgical indications increasingly extend to aging populations, the impact of advanced age on postoperative outcomes has become an area of active debate. Several recent studies suggest that older patients may achieve postoperative recovery and fusion rates comparable to younger individuals, although with slower functional improvement trajectories.2,3 In contrast, large DCM registries have identified age as an independent predictor of lower postoperative functional scores, even when improvements remain clinically meaningful. 4 Furthermore, elderly patients have been shown to experience higher perioperative risk and prolonged hospitalization following ACDF. 5
Despite these insights, the extent to which postoperative functional and quality-of-life outcomes differ between elderly and younger patients after ACDF for DCM remains incompletely understood. In particular, limited data exist on longer-term patient-reported outcomes and expectation fulfilment in age-stratified cohorts. Furthermore, much of the existing literature includes heterogeneous surgical approaches rather than ACDF-specific populations and focuses primarily on neurological recovery or short-term outcomes, as reflected in large multicenter DCM studies.1,4
Unlike prior studies that include heterogeneous surgical approaches, this study isolates ACDF and evaluates longitudinal PROM trajectories alongside expectation fulfilment, providing a procedure-specific assessment of age-related recovery patterns. To our knowledge, few studies have evaluated longitudinal PROM trajectories with expectation fulfilment specifically in an ACDF-only cohort, allowing a more procedure-specific understanding of recovery patterns across age groups.
The objective of this study was therefore to compare pain, functional, and quality-of-life outcomes between elderly (≥70 years) and younger (<70 years) patients undergoing primary ACDF for DCM, and to evaluate differences in satisfaction and expectation fulfilment at 2 years postoperatively.
Methods
Study Design and Patient Selection
This retrospective cohort study analyzed data from a prospectively maintained institutional spine registry at a tertiary academic medical center. All consecutive patients who underwent primary anterior cervical discectomy and fusion (ACDF) for degenerative cervical myelopathy (DCM) between January 2005 and December 2014 were identified. Inclusion criteria consisted of a clinical diagnosis of degenerative cervical myelopathy, based on myelopathic symptoms (eg, hand clumsiness, gait imbalance, upper motor neuron signs) and MRI-confirmed cervical spinal cord compression due to degenerative pathology, with failure of nonoperative management. Patients were excluded if they had undergone prior cervical spine surgery or presented with cervical trauma, infection, malignancy, or insufficient postoperative follow-up.
A total of 219 patients met inclusion criteria and were stratified into two age-based cohorts for comparative analysis: Young (<70 years; n = 188) and Elderly (≥70 years; n = 31). Patients with incomplete PROM data at baseline, 6 months, or 2 years were excluded from the final analysis. As only patients with complete longitudinal PROM data were available in the registry extract, the number of patients excluded due to incomplete follow-up could not be reliably reconstructed.
Institutional approval (CIRB:2017/2628) was obtained for this study. A cutoff of 70 years was selected, as this threshold is commonly used in spine outcomes literature to define elderly cohorts.
Surgical Technique
All procedures were performed by fellowship-trained spine surgeons using a standard Smith–Robinson anterior cervical approach. Discectomy and neural decompression were performed at one or more levels as indicated by pathology, followed by interbody fusion with structural graft and anterior cervical plating according to surgeon preference. Postoperative care and physiotherapy followed standardized institutional protocols.
Outcome Measures
Patient-reported outcome measures (PROMs) were collected preoperatively and at 6-month and 2-year follow-ups. The following validated PROMs were evaluated: • Visual Analogue Scale (VAS) for neck pain (NP) and limb pain (LP) • AAOS Cervical Spine Questionnaire: Neurogenic Symptoms (NS) and Neck Pain & Disability (NPD) • Neck Disability Index (NDI) • Japanese Orthopaedic Association (JOA) score • SF-36 Physical Component Summary (PCS) and Mental Component Summary (MCS)
The original Japanese Orthopaedic Association (JOA) score was used, as this was the standardized neurological assessment captured in the registry during the study period. Satisfaction and expectation fulfilment were assessed using standardized anchor questions. Responses were analyzed as binary variables (satisfied vs dissatisfied; expectations met vs unmet) for statistical comparison. These anchor-based measures were dichotomized to facilitate clinically interpretable comparisons between groups, consistent with prior outcomes studies. Only patients with complete PROM data at baseline, 6 months, and 2 years were included in the final analysis cohort (n = 219).
Data Collection and Variables
Demographic and perioperative variables collected included age, sex, body mass index (BMI), individual comorbidities, operative time, number of fused levels, and postoperative length of stay (LOS). Clinical outcomes were analyzed both as absolute PROM scores at baseline, 6-month, and 2-year follow-up, and as change-from-baseline (Δ) values for each outcome measure at the respective follow-up intervals. As radiculopathy was not recorded as a discrete variable in the registry, baseline limb pain (VAS LP) was used as a proxy measure.
Statistical Analysis
Continuous variables were compared between groups using independent-samples Student’s t-tests or Mann–Whitney U tests, depending on distribution normality. Categorical variables were analyzed using chi-square or Fisher’s exact tests where appropriate. Change-from-baseline (Δ) improvements were compared across groups using independent-samples t-tests. Statistical significance was set at P < .05. As no multivariable or longitudinal modeling was performed, analyses represent unadjusted between-group comparisons. Given the limited size of the elderly cohort (n = 31), adjusted models would not meet recommended events-per-variable thresholds and would risk model instability and overfitting. All analyses were performed using IBM SPSS Statistics Version 27 (IBM Corp., Armonk, NY, USA).
Results
Patient Demographics and Perioperative Characteristics
Patient Demographics and Preoperative Clinical Scores (n = 219)
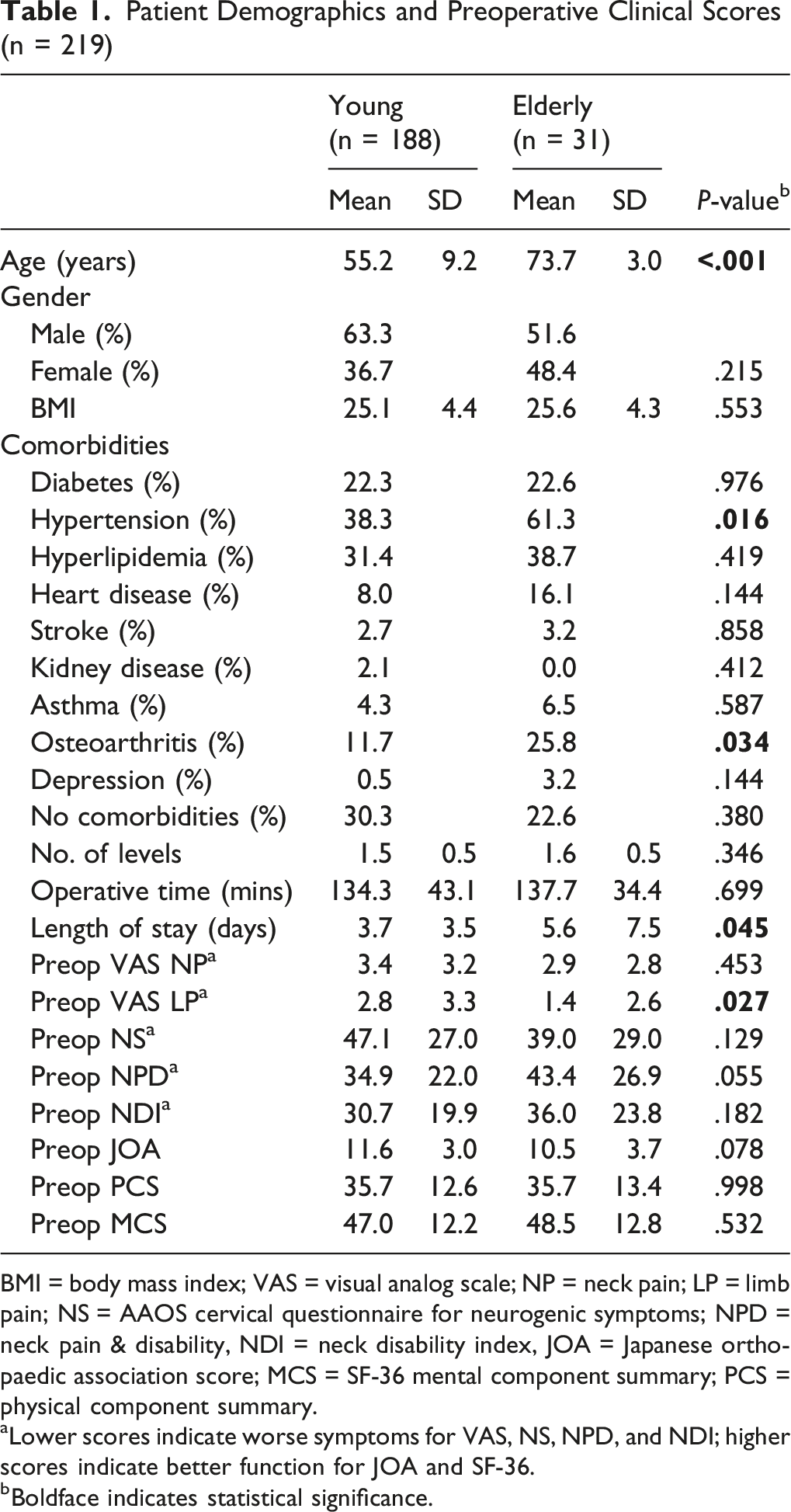
BMI = body mass index; VAS = visual analog scale; NP = neck pain; LP = limb pain; NS = AAOS cervical questionnaire for neurogenic symptoms; NPD = neck pain & disability, NDI = neck disability index, JOA = Japanese orthopaedic association score; MCS = SF-36 mental component summary; PCS = physical component summary.
aLower scores indicate worse symptoms for VAS, NS, NPD, and NDI; higher scores indicate better function for JOA and SF-36.
bBoldface indicates statistical significance.
Patient-Reported Outcomes
Preoperative PROMs
Preoperative outcome measures were comparable between groups for VAS NP, NS, NPD, NDI, JOA, PCS and MCS (all P > .05), indicating similar baseline functional status. The only significant difference was higher preoperative limb pain in younger patients (P = .027), which may reflect variation in the prevalence or severity of concomitant radiculopathy between groups (Table 1).
Six-month Outcomes
Comparison of Clinical Outcomes Between Groups at Different Time Intervals (n = 219)
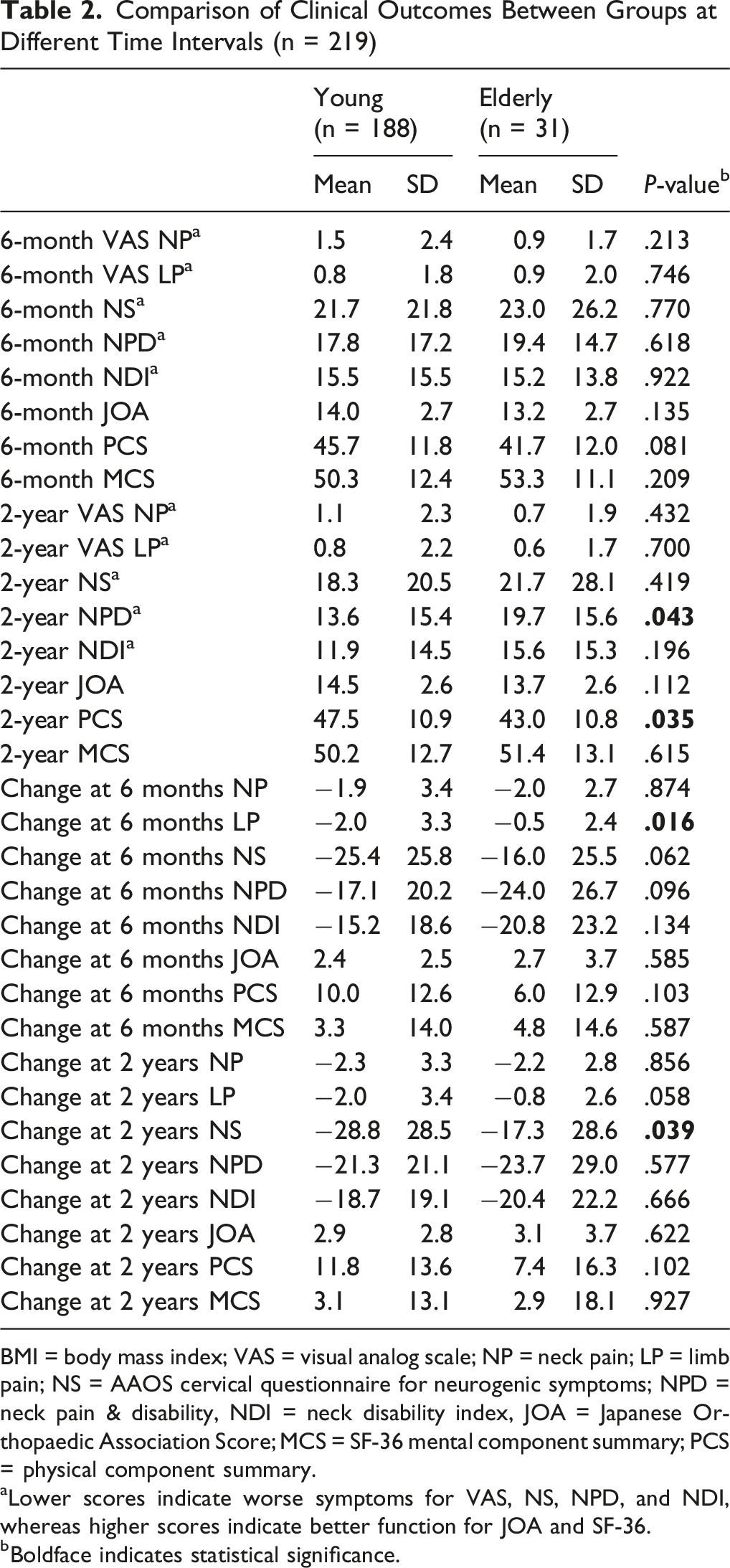
BMI = body mass index; VAS = visual analog scale; NP = neck pain; LP = limb pain; NS = AAOS cervical questionnaire for neurogenic symptoms; NPD = neck pain & disability, NDI = neck disability index, JOA = Japanese Orthopaedic Association Score; MCS = SF-36 mental component summary; PCS = physical component summary.
aLower scores indicate worse symptoms for VAS, NS, NPD, and NDI, whereas higher scores indicate better function for JOA and SF-36.
bBoldface indicates statistical significance.
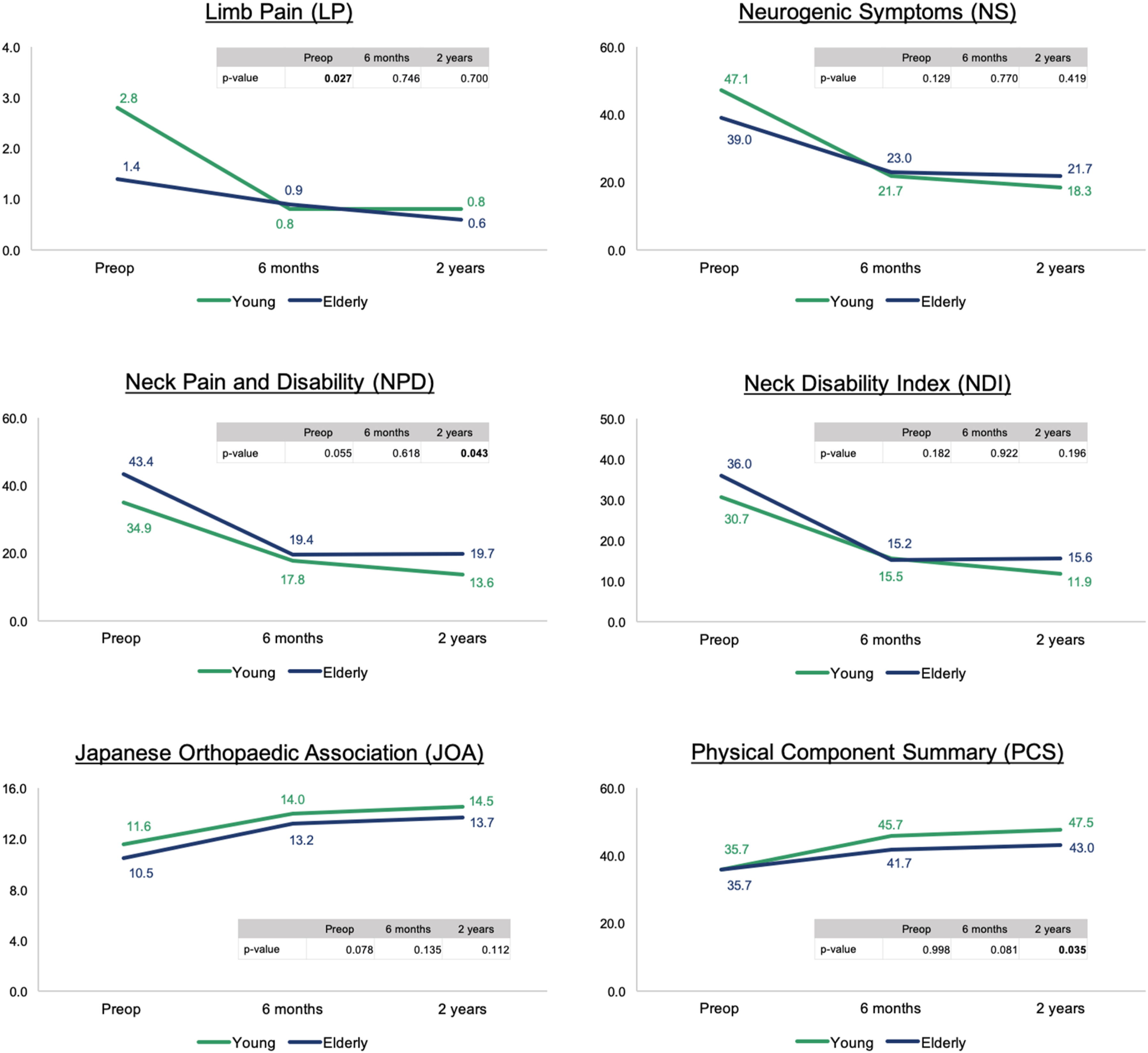
Results of patient-reported outcomes preoperatively and postoperatively (6 months and 2 years) *Boldface indicates statistical significance. Y-axis denotes value of outcome scores, while x-axis denotes different timeframes
Two-year Outcomes
Divergences in absolute PROM scores emerged at 2 years, particularly in neck-related disability and physical quality of life. At 2-year follow-up, elderly patients demonstrated significantly worse neck-related disability (NPD; P = .043) and lower physical component (PCS) scores (P = .035), whereas VAS NP, VAS LP, NDI, JOA, and MCS remained similar between groups (all P > .05) (Table 1; Figure 1). These findings suggest a modest divergence in long-term functional recovery between age groups.
Change-score Analysis
Younger patients experienced significantly greater improvement in limb pain (ΔLP; P = .016) compared with elderly individuals, indicating greater early improvement in limb pain among younger patients, although this difference did not persist at 2 years. Elderly patients also exhibited significantly less improvement in neurogenic symptoms (NS) over 2 years (P = .039), indicating a difference in neurological symptom recovery between groups. Improvements in NP, NDI, JOA, PCS and MCS did not differ significantly between groups (all P > .05). (Table 1).
Satisfaction and Expectation Fulfilment
Satisfaction and Expectation Fulfilment at Different Time Intervals (n = 219)
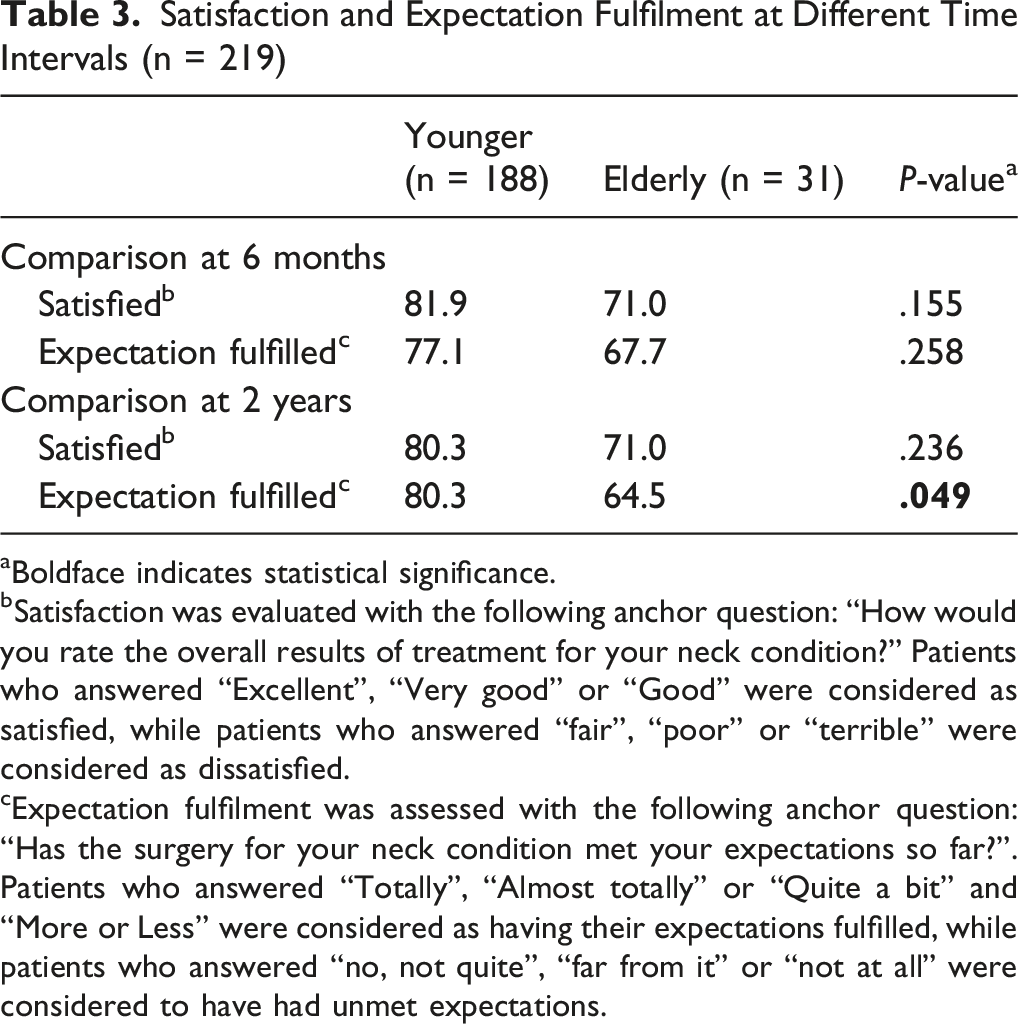
aBoldface indicates statistical significance.
bSatisfaction was evaluated with the following anchor question: “How would you rate the overall results of treatment for your neck condition?” Patients who answered “Excellent”, “Very good” or “Good” were considered as satisfied, while patients who answered “fair”, “poor” or “terrible” were considered as dissatisfied.
cExpectation fulfilment was assessed with the following anchor question: “Has the surgery for your neck condition met your expectations so far?”. Patients who answered “Totally”, “Almost totally” or “Quite a bit” and “More or Less” were considered as having their expectations fulfilled, while patients who answered “no, not quite”, “far from it” or “not at all” were considered to have had unmet expectations.
Complication and reoperation data were not consistently captured in the registry and were therefore not analyzed; no reliable subgroup comparison could be performed.
Discussion
Elderly patients demonstrated less improvement in neurogenic symptoms and neck-related disability at 2 years following ACDF, as reflected in lower PCS scores compared with younger patients. Expectation fulfilment was also lower in the elderly cohort at 2 years, despite similar satisfaction rates between groups.
These findings build on existing literature by focusing specifically on ACDF and by incorporating longitudinal PROM trajectories alongside expectation fulfilment, both of which remain underreported in age-stratified DCM cohorts. Nevertheless, both age groups demonstrated substantial postoperative improvement in pain, neurological symptoms, and health-related quality of life, supporting the effectiveness of ACDF across age ranges.
Importantly, although between-group differences reached statistical significance in selected domains such as NPD and PCS, these differences were not consistently observed across all patient-reported outcome measures, including the NDI and JOA score, and may not consistently translate into clinically important differences across domains. This pattern suggests a more nuanced recovery profile, in which elderly patients continue to derive substantial postoperative benefit but may experience somewhat attenuated improvement in selected pain and physical quality-of-life domains rather than globally inferior recovery.
Given the observational design and absence of multivariable adjustment, residual confounding cannot be excluded, and the observed differences may partly reflect baseline group differences. Accordingly, these findings should be interpreted as associative rather than reflecting independent effects of age.
The absence of early differences but divergence by 2 years may reflect differences in sustained postoperative recovery between age groups, although these findings are associative and may be influenced by unmeasured confounders rather than a direct effect of age. Frailty and sarcopenia, which are associated with slower functional recovery and delayed disability improvement, may contribute to similar early trajectories but more limited long-term gains in elderly patients.6,7
Our findings are consistent with prior literature demonstrating that ACDF remains an effective intervention in older adults, with a tendency toward slower or attenuated recovery trajectories in older individuals. Multilevel ACDF has been shown to yield comparable functional outcomes and fusion rates in elderly and younger patients, despite a tendency toward slower recovery trajectories in older individuals. 2 Similarly, comparative analyses of older age strata have reported no significant differences in clinical or radiologic outcomes between patients aged 65-74 years and those aged 75 years or older, suggesting that advanced age alone should not be considered a contraindication to surgery. 3 In contrast, larger prospective AOSpine cohort analyses have demonstrated that age independently predicts lower postoperative functional scores, while still confirming substantial neurological improvement across all age groups. 4 These findings suggest that older age is associated with differences in the magnitude of postoperative improvement, rather than the likelihood of improvement.
In addition, the observed reduction in expectation fulfilment among elderly patients in our cohort highlights the importance of structured preoperative counseling. The dissociation between comparable satisfaction and lower expectation fulfilment suggests that elderly patients may recalibrate expectations postoperatively, achieving satisfaction despite not fully meeting preoperative expectations. Prior outcomes research has demonstrated that expectation fulfilment is one of the strongest predictors of postoperative satisfaction, independent of objective functional improvement. 8 Elderly patients in our cohort demonstrated a longer length of stay, consistent with prior studies. 5 While prior studies have reported increased perioperative risk in elderly patients, this could not be assessed in the present cohort due to incomplete capture of complication data, reinforcing the need for realistic goal-setting and individualized perioperative optimization. Incorporating frailty assessment and targeted postoperative rehabilitation pathways may help align anticipated and achievable outcomes and improve long-term patient-reported value.
This study has several limitations. First, the analysis was based on unadjusted comparisons without multivariable or longitudinal modeling, and residual confounding cannot be excluded. Important baseline differences, including comorbidities (eg, hypertension, osteoarthritis), preoperative limb pain, and length of stay, were not adjusted for and may confound observed between-group differences, such that findings may partly reflect baseline differences rather than independent age-related effects. The relatively small elderly cohort (n = 31) may also limit statistical power and precision of between-group comparisons. Furthermore, no formal correction for multiple comparisons was performed, and findings should be interpreted as exploratory.
Second, detailed complication and reoperation data were not consistently captured in the registry and were therefore not included in the current analysis. As such, differences in perioperative risk between age groups could not be reliably assessed, and no conclusions regarding perioperative safety can be drawn.
Third, concomitant radiculopathy was not independently recorded, and baseline limb pain was used as a surrogate marker. This represents an indirect approximation of radicular symptom burden and should be interpreted with caution. This may bias comparisons in pain-related and functional outcomes, particularly if younger patients had a higher prevalence of radiculopathy, potentially exaggerating early improvements.
Fourth, the retrospective design and inclusion of only patients with complete PROM data may introduce selection and survivorship bias. As only patients with complete longitudinal PROM data were available in the registry extract, the number of excluded patients could not be reliably reconstructed, precluding comparison between included and excluded patients. As such, the study cohort may represent a healthier or more compliant subset, potentially leading to overestimation of postoperative outcomes and limiting external validity.
Fifth, the cohort spans 2005-2014, and changes in perioperative care and frailty assessment may limit generalizability to contemporary practice, particularly given the absence of modern frailty assessment and enhanced recovery protocols.
Finally, key variables such as frailty, symptom duration, smoking status, baseline neurological severity beyond PROMs, and radiographic alignment were not available for analysis.
Future studies should incorporate cervical sagittal alignment metrics, frailty scoring, and advanced imaging correlates of spinal cord integrity to better characterize recovery patterns in elderly patients. Prospective multicenter studies using longitudinal modeling may further refine prognostic stratification.
Conclusion
Elderly patients undergoing ACDF demonstrated less improvement in neurogenic symptoms and neck-related disability at 2 years, with lower physical quality-of-life scores and reduced expectation fulfilment compared with younger patients. Despite this, overall satisfaction remained comparable, and both age groups demonstrated substantial postoperative improvement. These findings indicate that older age is associated with differences in the magnitude of recovery rather than the likelihood of achieving clinically meaningful improvement. Focused preoperative counseling and individualized rehabilitation strategies may help optimize outcomes in elderly patients. Age should not be considered a contraindication to ACDF, but rather a factor associated with postoperative recovery trajectory and expectation management.
Footnotes
Ethical Considerations
Institutional review board approval was obtained (CIRB:2017/2628) prior to study initiation. Due to the retrospective nature of the study and use of de-identified data, informed consent was waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AO Spine Membership
Last author: John L.T. Chen – AO Spine Member ID: pp100018073. Additional author: Reuben C.C. Soh – AO Spine Member ID: pp100073910.