
Abstract
Study Design
Prospective observational pilot study.
Objectives
Introducing endoscopic spine surgery in low- and middle-income countries (LMICs) poses logistical and clinical challenges, yet offers potential patient benefits. This study describes the implementation of a pilot endoscopic spine surgery program in Tanzania and reports early outcomes from the first patient cohort.
Methods
Weill Cornell Medicine and the University of California, Irvine facilitated the introduction of endoscopic spine surgery techniques in Tanzania through theoretical and hands-on training, equipment donations, and live surgical mentorship. Fourteen patients with lumbar pathology refractory to conservative treatment underwent endoscopic microdiscectomy and/or decompression. Outcomes were assessed using the Oswestry Disability Index (ODI) and the Visual Analog Scale (VAS) for back and leg pain, measured preoperatively and postoperatively up to 3 months. All fourteen patients (100%) completed the 3-month assessment.
Results
A structured 5-day program integrating didactic instruction, simulation-based training, and supervised live surgeries successfully introduced spine endoscopy in Tanzania. Fourteen patients underwent endoscopic lumbar decompression (FESS n = 8; UBE n = 6). At short-term follow-up, marked early reductions were observed in back-pain VAS (P < 0.001, Kendall’s W = 0.53), leg-pain VAS (P < 0.001, W = 0.59), and ODI (P < 0.001, W = 0.79). All preoperative-versus-postoperative pairwise comparisons survived Benjamini-Hochberg false-discovery-rate adjustment (q = 0.05). These results reflect feasibility and early safety only and should not be interpreted as evidence of sustained benefit or comparative effectiveness.
Conclusion
This pilot study demonstrates the successful implementation of endoscopic spine surgery in an LMIC setting through structured international collaboration. The clinical outcomes reported are short-term and observed under selected pilot conditions; larger studies with longer follow-up are needed to evaluate durability, comparative effectiveness, and external validity.
Keywords
Introduction
Degenerative lumbar spine diseases are a major cause of disability and economic burden worldwide, and low- and middle-income countries (LMICs) are estimated to have four times the burden compared to high-income countries (HICs).1,2 Despite the high incidence, access to specialized surgical care remains limited in many LMICs.3,4 For instance, the lowest densities of neurosurgeons are observed in Sub-Saharan Africa (0.51 neurosurgeons per million people), compared to HICs (2.44 neurosurgeons per million people). 5
Minimally invasive spine surgery (MISS) offers advantages such as reduced perioperative blood loss, postoperative pain, shorter hospital stays, lower infection rates, and quicker return to work.6,7 These benefits are particularly pertinent in LMICs, where healthcare follow-up is often constrained. 7
The implementation of MISS techniques can be expensive and requires a high level of continued maintenance not always available in these settings.8,9 Spine endoscopy has been shown in HIC settings to achieve comparable clinical outcomes to other open and MIS techniques.10-12 Studies in HIC populations have suggested that spine endoscopic surgery is cost-effective compared to microsurgical techniques.13,14 Only a small number of studies have described the use of spine endoscopy and other MISS techniques in LMICs, and most are surveys or limited case series.15-18 This lack of data underscores the need for evidence on feasibility, implementation, and outcomes in resource-constrained environments. This study is the first step towards addressing that gap.
The goal of this paper is twofold: (1) to describe the first hands-on endoscopic spine surgery course conducted in Tanzania, detailing our methodology for introducing this technique in an LMIC setting; and (2) to report the early outcomes of the first 14 patients who underwent endoscopic lumbar surgery at the Muhimbili Orthopaedic Institute (MOI).
Methods
Study Objectives and Endpoints
This study was designed as a prospective observational pilot study primarily focused on implementation feasibility and early safety. The primary endpoint was feasibility, defined as successful program execution and completion of procedures without major perioperative complications. Secondary endpoints included changes in patient-reported outcomes (ODI and VAS for back and leg pain), which were considered exploratory.
Program Implementation
Weill Cornell Medicine has been engaged with the Muhimbili Orthopaedic Institute (MOI) for nearly 15 years, with a strong commitment to advancing neurosurgical care, particularly in spine surgery. In 2023, spine endoscopy was briefly introduced during the Global Neurosurgery Course, and due to its success, the decision was made to launch the first Tanzanian Spine Endoscopy Course in February 2025.
The 2 senior authors supported this initiative and traveled to Tanzania to lead the course. The course was made possible by the donation of a uniportal endoscopic tower and generators for full-endoscopic spine surgery (FESS) (Joimax®, Karlsruhe, Germany) and consumables, as well as the radiofrequency generator, which was lent (Stryker®, Kalamazoo, USA) and probes for unilateral biportal endoscopy (UBE), which where donated.
The course consisted of 2 days of blended lectures and hands-on simulated spine models (Realists, Leipzig, Germany) followed by 3 days of live surgeries (Figure 1). Course structure and training components. The first 2 days of the program consisted of lectures and hands-on sessions, followed by 3 days of live surgeries. The figure includes 2 photographs of the skills lab with a Realist RealSpine Basic Endo model and one photograph illustrating a live FESS case. The figure provides a reproducible structure for short-format technique-transfer courses in LMIC settings
Local Healthcare System and Structure
MOI is the main referral center for neurosurgery in Tanzania and, thanks to its long-standing collaboration with Weill Cornell, major advances in neurosurgical and spine care have been achieved. A dedicated scoliosis program has been in place since 2020, 19 allowing complex spine surgeries to be performed regularly. The department has been equipped with spinal navigation since 2023 and cranial navigation since 2025, distinguishing it from most other hospitals in the country.
Regarding the broader Tanzanian healthcare system, there is no universal public health insurance. Most insured patients are government employees, while the remainder of the population either purchases private insurance independently or must pay out of pocket for medical care, which significantly limits access. There are only approximately 30 certified neurosurgeons in a country of nearly 70 million inhabitants. 20 As a result, specialized care is often located far from where patients live, requiring days of travel for treatment, and returning for postoperative follow-up is frequently not feasible.
For the endoscopic spine procedures performed during this pilot study, we ensured that the cost to patients remained equivalent to that of the corresponding open procedures. Once the technique becomes fully integrated and sustainable, pricing will be adjusted to appropriately reflect the consumables and expertise required for these cases. No formal cost analysis was performed during this pilot study, and economic outcomes were not pre-specified as endpoints.
Local Surgeons
The trainee team included local neurosurgeons experienced in open spine surgery for trauma and degenerative conditions, and in using microscopic tubular retractor systems. Some had extensive experience with cranial endoscopic procedures such as endoscopic third ventriculostomy (ETV); thanks to this background, they were able to learn endoscopic spine techniques in a short time.
Lectures and Simulations
Lectures covered basic anatomical principles, the basics of FESS and UBE, the interlaminar approach, the transforaminal approach, and complication prevention and management. A dedicated clinical session discussed each selected patient, the rationale for surgery, and the specific operative target.
For the hands-on session, a skills lab was created in one of the operating theaters with spine models. One station was dedicated to UBE and one to FESS. The first session lasted 4 h and focused on the interlaminar approach with both techniques. The second hands-on session lasted 6 h and covered the transforaminal approach and gave time for the surgeons to practice both interlaminar and transforaminal approaches.
For the FESS station, the Joimax tower was used together with the supplied sets; for the UBE station, the already-available cranial-endoscopy tower was used with the locally available instrument sets used for open or tubular spine surgery.
Figure 1 depicts the course structure and includes 2 images of the skills lab and 1 image illustrating a live FESS case.
Live Surgeries
For the following 3 days, live surgeries were performed by the faculty and the local surgeons. UBE operative setup for a left-sided procedure. (A): Positioning setup with a cushion system designed to allow a free-hanging abdomen, thereby reducing intra-abdominal pressure, and padded leg supports to minimize pressure points. The endoscopy tower is placed directly in front of the surgeon. (B-C): A black trash bag is positioned between the cushions and the operating table to collect irrigation fluid. A white plastic sheet is taped to the patient’s lateral flank and directed into the trash bag to facilitate controlled fluid drainage. (D): Reusable cotton surgical drapes are applied and partially tucked into the trash bag at the base to limit contamination and direct fluid runoff. The figure demonstrates that water management — frequently cited as a barrier to UBE adoption in LMICs — can be achieved without dedicated endoscopic drapes, using only consumables available in any operating theater
Main Technical Considerations and Implemented Solutions for UBE Surgery
1. 2. 3. 4. 5. 6.
Main Technical Considerations and Implemented Solutions for FESS
The adoption of FESS required fewer adaptations, as a fully equipped endoscopic tower (camera system, light source, irrigation pump, shaver/drill, bipolar coagulation unit) was donated. 1. 2. 3. 4. 5. 6.
Patient Selection
Inclusion criteria included adults with symptomatic lumbar disc herniation or spinal stenosis, failure to improve with conservative treatment (analgesics and/or corticosteroids), imaging (MRI ± CT) confirming pathology correlating with clinical symptoms, involvement of 1 or 2 spinal levels, and no significant spinal instability requiring fusion. Patients with more than 2 levels of spinal involvement or significant spinal instability necessitating fusion surgery were excluded.
The choice between FESS and UBE was based on surgeon preference, pathology (eg, foraminal vs central), and training objectives during the course. Two-level decompressions and cases of central stenosis were more commonly selected for the UBE approach, whereas disc herniations were more frequently treated with the FESS transforaminal technique. Patients operated after the course period were treated using FESS only, as the radiofrequency generator required for UBE was not available. These pathology-by-approach patterns reflect training-course logistics and surgeon preference during the pilot rather than a clinical recommendation; the cohort is too small to support inferences about which approach is preferable for which pathology.
Patients were initially screened in the neurosurgery clinic by residents and subsequently evaluated by the first author. Final selection for endoscopic surgery was determined after multidisciplinary review. Common reasons for exclusion at this gate included pathology requiring fusion or extending beyond 2 spinal levels, decompensated medical comorbidity, prior lumbar surgery at the index level, and inability to attend the planned 3-month follow-up window; categorical counts were not maintained in this pilot phase. The selection decisions favored single-level, anatomically straightforward pathology suitable for the early-implementation phase of the program. The full screening flow is shown in Figure 3. Flow diagram summarizing patient screening, selection, and follow-up. Of 78 patients initially screened, 36 were evaluated by the first author, and 14 were selected for endoscopic spine surgery after multidisciplinary review. All 14 treated patients (100%) completed the 3-month assessment. The figure documents the highly selective inclusion characteristic of an early-implementation pilot phase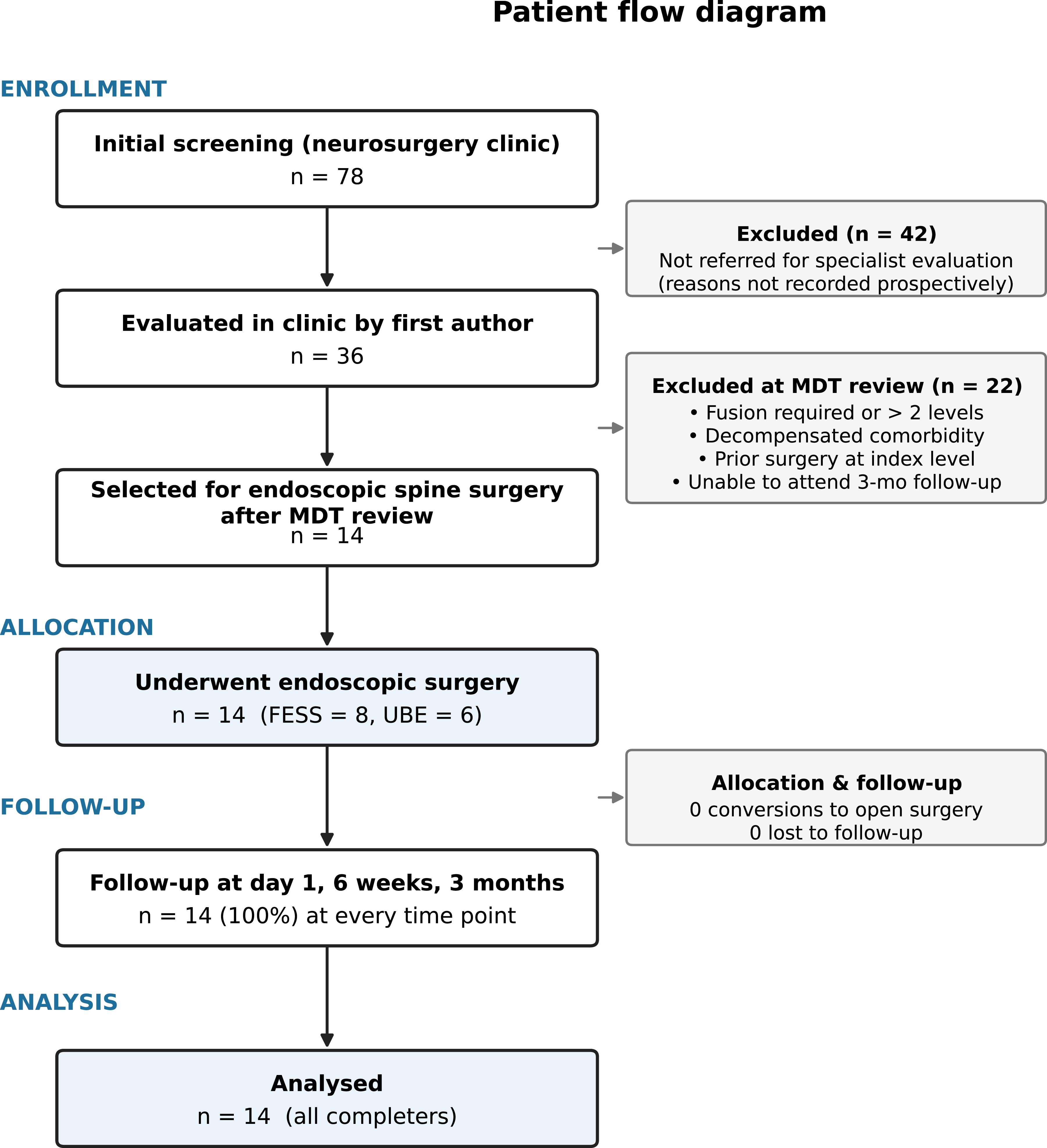
Data Collection
Preoperative and postoperative assessments were conducted using 2 validated instruments: • The Oswestry Disability Index (ODI),
21
a widely used questionnaire designed to measure functional disability related to lower back pain. It includes 10 sections, each scored 0-5, covering pain intensity, personal care, lifting, walking, sitting, standing, sleeping, social life, travel, and employment/homemaking. Scores are summed and converted to a percentage; higher scores indicate greater disability. • The Visual Analog Scale (VAS), used to evaluate the intensity of leg and back pain separately. Patients marked their pain level on a 10-centimeter horizontal line ranging from “no pain” (0) to “worst imaginable pain” (10).
Although the survey questions were in English, they were administered verbally in Swahili by a trained research coordinator fluent in both English and Swahili, to ensure comprehension and accurate responses from native Swahili speakers.
Data were collected at four scheduled time points: preoperatively (baseline), at hospital discharge (assessed daily through postoperative day 3), at 6 weeks postoperatively, and at 3 months postoperatively (Figure 3). Follow-up assessments were primarily conducted in person; for patients living in remote areas or those unable to attend the hospital due to travel constraints, assessments were performed via secure teleconsultation. All fourteen patients (100%) completed the 3-month assessment.
Postoperative Management
Postoperative analgesia followed the institution’s standardized lumbar spine protocol, consisting of acetaminophen, NSAIDs, and opioids as needed. Complications were prospectively recorded and systematically assessed, including cerebrospinal fluid (CSF) leak, transient dysesthesia, infection, hematoma, postoperative urinary retention, and hospital readmission within 3 months. Routine postoperative imaging was not performed in the absence of new or worsening symptoms.
Ethical Approval
The study protocol was reviewed and approved by the Muhimbili University of Health and Allied Sciences (MUHAS) Institutional Review Board (Approval No. DA.282/I298/01L/838).
Consent to Participate
All patients participated in comprehensive preoperative discussions addressing the risks and benefits of the procedure and provided informed consent prior to surgery and enrollment in the study. Patients were informed during the consent process that the procedure would be performed during a structured international training course with senior-faculty supervision. The senior author and visiting faculty performed or directly supervised every critical step of every case. The IRB approval (DA.282/I298/01L/838) explicitly covered the training context, including the live-surgery teaching component. The cost charged to participating patients was kept equivalent to standard open surgery and any patient declining participation in the training course would have been offered the standard surgical pathway without delay or penalty.
Data Analysis
All omnibus tests, effect sizes, and pairwise tests were computed in IBM SPSS Statistics, Version 27 (IBM Corp., Armonk, NY); Benjamini-Hochberg false discovery rate adjustment and bootstrap confidence intervals were computed in Python 3.11 (NumPy 1.26, SciPy 1.12). Continuous variables are reported as medians with interquartile ranges (IQR; computed by linear interpolation, R-7/NumPy default); categorical variables are reported as frequencies and percentages.
Changes in back-pain VAS, leg-pain VAS, and ODI scores across postoperative time points were evaluated with the Friedman test for repeated measures, with Kendall’s coefficient of concordance W reported as the corresponding effect size and interpreted using conventional thresholds (small ≥ 0.1, medium ≥ 0.3, large ≥ 0.5). Where the Friedman test rejected the null, post-hoc all-pairs comparisons were performed with the Wilcoxon signed-rank test, with multiplicity addressed by the Benjamini-Hochberg FDR procedure controlling the expected proportion of false rejections at q = 0.05 across k(k − 1)/2 pairs (15 pairs for back-pain VAS, 15 for leg-pain VAS, and 3 for ODI). The Benjamini-Hochberg procedure was preferred over the more conservative Bonferroni adjustment because, with the small sample size, BH-FDR preserves greater power to detect genuine within-subject changes while still bounding the expected false-rejection rate. Two-sided 95% confidence intervals around the median at each time point were estimated by percentile bootstrap with 10 000 resamples. Statistical significance was defined a priori as P ≤ 0.05 for the omnibus Friedman tests and as BH-adjusted P < 0.05 for the post-hoc pairwise comparisons. Achievement of the minimal clinically important difference (MCID) at 3 months was defined a priori as a ≥10-point reduction in Oswestry Disability Index 22 and a ≥2-point reduction in each Visual Analog Scale. 23 MCID achievement was computed only for patients with clinically relevant baseline scores (VAS ≥ 3 or ODI ≥ 20); patients with sub-threshold baseline scores were excluded from the denominator for that outcome.
No formal sample size or power calculation was performed, as this study was designed as a pilot feasibility study. Economic outcomes were not pre-specified as endpoints in this pilot study and were not measured. All inferential statistics on patient-reported outcomes are exploratory and are reported alongside effect sizes and confidence intervals to support transparent interpretation.
Results
Implementation Strategy
The course was completed as scheduled, with all lectures delivered by senior faculty and hands-on simulation sessions conducted as planned to facilitate technical familiarization. All selected patients proceeded to surgery according to the operative plan, with no cancellations or conversions to open procedures.
Patient Demographics, Operative Details and Outcomes
Patient Demographics, Surgical Details, and Short-Term Outcomes (N = 14)
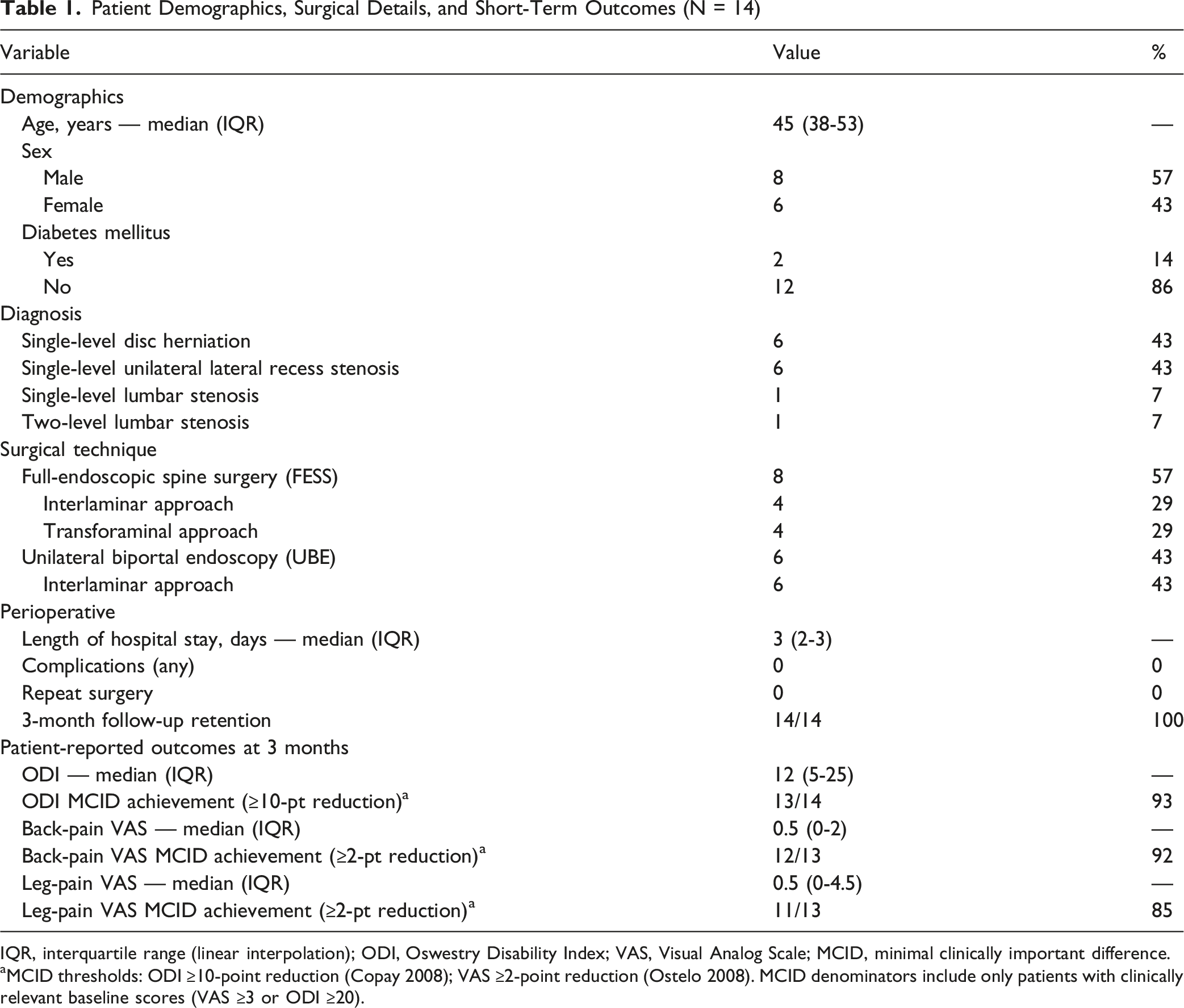
IQR, interquartile range (linear interpolation); ODI, Oswestry Disability Index; VAS, Visual Analog Scale; MCID, minimal clinically important difference.
aMCID thresholds: ODI ≥10-point reduction (Copay 2008); VAS ≥2-point reduction (Ostelo 2008). MCID denominators include only patients with clinically relevant baseline scores (VAS ≥3 or ODI ≥20).
Pain Outcomes (VAS Scores)
Back Pain (VAS)
The preoperative median back-pain VAS was 8.0 (95% bootstrap CI 7.0-8.0; IQR 7.0-8.0). A marked reduction was observed by postoperative day 1 (median 0.0, 95% CI 0.0-3.0) and persisted through the 3-month follow-up (median 0.5, 95% CI 0.0-2.0) (Figure 4). The Friedman test indicated a significant change across time points (χ2[5] = 37.33, P < 0.001) with a large effect size (Kendall’s W = 0.53). All preoperative-versus-postoperative pairwise comparisons were significant after Benjamini-Hochberg FDR correction (q = 0.05; adjusted P ≤ 0.006 for every preoperative-postoperative pair); no inter-postoperative pairwise comparison reached significance after correction (day 1-versus-day 2 and day 1-versus-day 3 adjusted P = 0.055 each, the closest to threshold). Visual Analog Scale (VAS) scores for back pain (left) and leg pain (right) measured preoperatively and at postoperative day 1, day 2, day 3, 6 weeks, and 3 months following endoscopic lumbar surgery, with 95% percentile-bootstrap confidence intervals. Both back and leg pain demonstrate a marked early postoperative reduction; values observed at the 3-month follow-up are consistent with maintained early-window improvement within the short-term observation period of this pilot study. Individual patient values are shown as light-gray points to display heterogeneity in response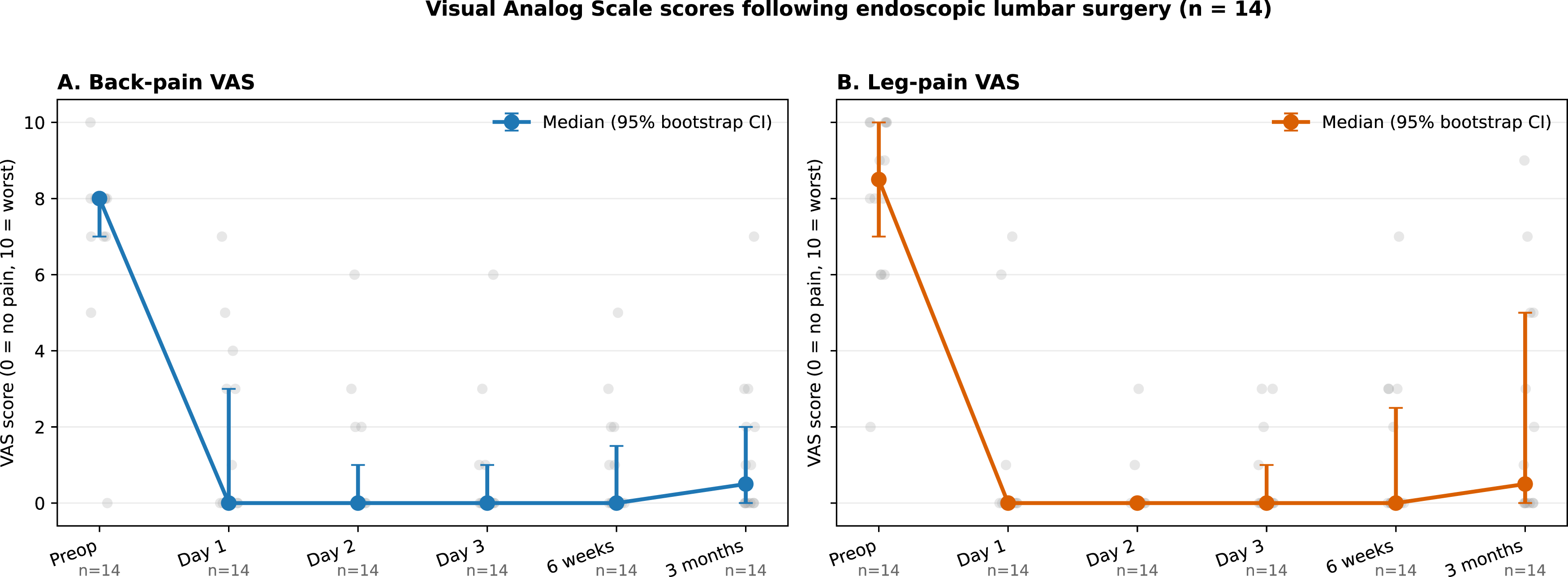
Leg Pain (VAS)
The preoperative median leg-pain VAS was 8.5 (95% CI 7.0-10.0; IQR 6.5-10.0). Median scores dropped to 0.0 by day 1 (95% CI 0.0-0.0) and were 0.5 at the 3-month follow-up (95% CI 0.0-5.0) (Figure 4, right panel). Friedman χ2[5] = 41.35, P < 0.001; Kendall’s W = 0.59 (large effect). Benjamini-Hochberg-adjusted Wilcoxon comparisons confirmed significant reductions between preoperative and every postoperative time point (adjusted P = 0.004 for every preoperative-postoperative pair); inter-postoperative pairs did not reach significance after correction.
Three individual patient trajectories deserve mention. Box plot illustrating Oswestry Disability Index (ODI) scores preoperatively, at 6 weeks, and at 3 months following endoscopic lumbar surgery. Boxes represent interquartile ranges (linear interpolation), horizontal lines indicate medians, whiskers denote range, and dots indicate individual patient values. Friedman χ2(2) = 22.15, P < 0.001; Kendall’s W = 0.79 (large effect size). Median ODI scores decreased substantially at early postoperative follow-up, indicating improvement in functional status during the short-term observation period of this pilot study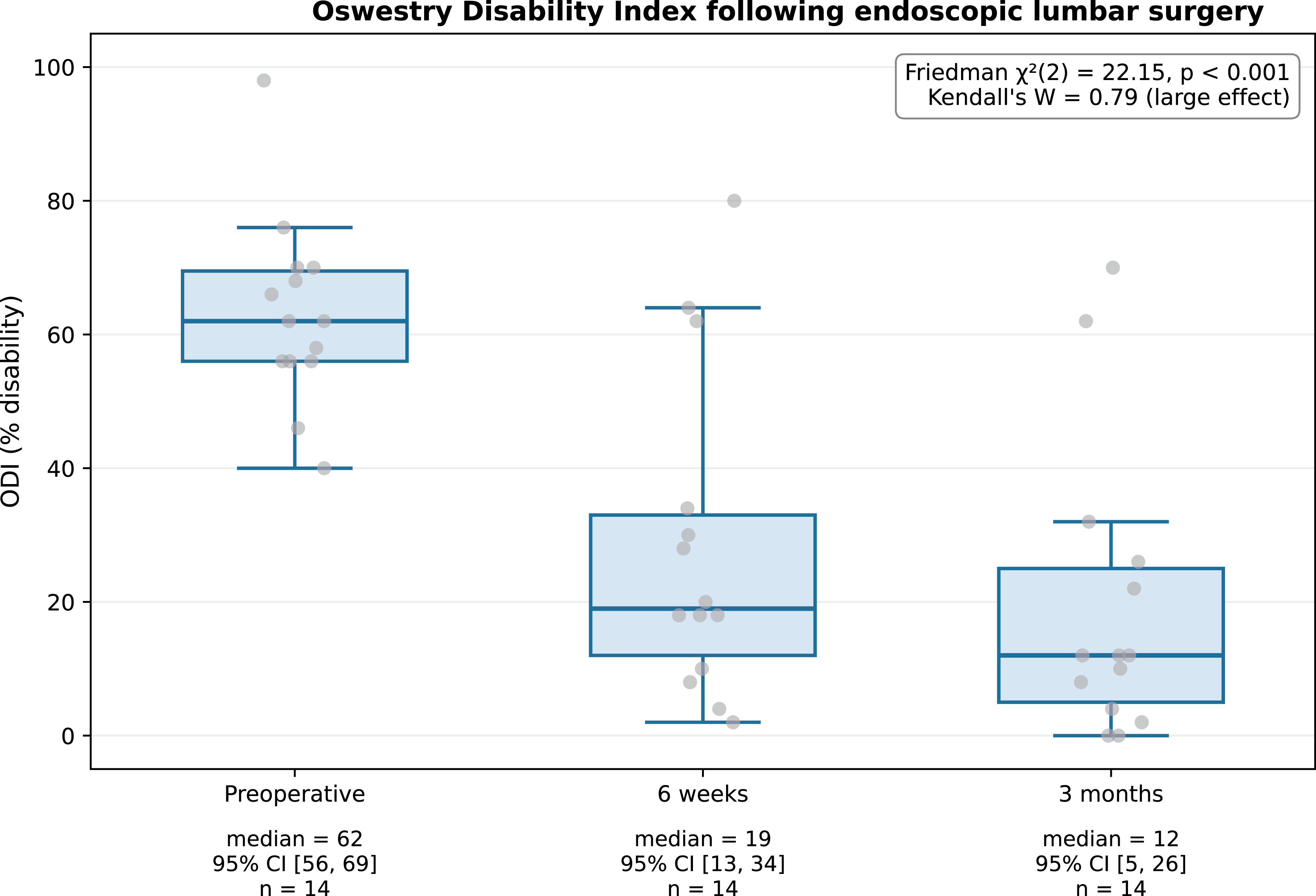
Overall, both back-pain and leg-pain VAS demonstrated marked early postoperative reduction, with values observed at the 3-month follow-up consistent with maintained early-window improvement; the pilot design and follow-up duration do not permit inferences about durability beyond 3 months.
Functional Outcomes (ODI)
The preoperative median ODI was 62.0 (95% bootstrap CI 56.0-69.0; IQR 56.0-69.5), indicating moderate-to-severe disability. At 6 weeks the median ODI decreased to 19.0 (95% CI 13.0-34.0; IQR 12.0-33.0) and at 3 months to 12.0 (95% CI 5.0-26.0; IQR 5.0-25.0) (Figure 5). The Friedman test confirmed a significant change (χ2[2] = 22.15, P < 0.001) with a large effect size (Kendall’s W = 0.79). Benjamini-Hochberg-adjusted Wilcoxon comparisons identified significant reductions for every pair: preoperative-versus-6-week (adjusted P = 0.003), preoperative-versus-3-month (adjusted P = 0.003), and 6-week-versus-3-month (adjusted P = 0.019), the last consistent with continued functional improvement between the 6-week and 3-month time points beyond what is captured by the early-window response alone. In terms of clinically meaningful improvement at 3 months: 13 of 14 patients (93%) achieved the ODI MCID of ≥10-point reduction; 12 of 13 patients with clinically relevant baseline back pain (92%) achieved the ≥2-point back-pain VAS MCID; and 11 of 13 patients with clinically relevant baseline leg pain (85%) achieved the ≥2-point leg-pain VAS MCID. Three patients failed the MCID on at least one outcome (Patient 1: leg-pain VAS; Patient 4: ODI and back-pain VAS; Patient 10: leg-pain VAS); no patient failed all 3.
Discussion
The primary contribution of this study is the successful implementation of an endoscopic spine surgery program in a low-resource LMIC setting through structured training and international collaboration. The clinical outcomes reported here represent short-term postoperative results intended to assess feasibility and early safety only; they do not, and were not designed to, support inferences about durability, comparative effectiveness, or generalizability to unselected real-world adoption.
MISS techniques may play an increasingly important role in the future of spinal care in LMICs. Their benefits, equal or improved pain outcomes, reduced tissue damage, infection risk, and hospital stay, and quicker return to work6,24-26 are particularly crucial in healthcare systems that lack robust rehabilitation and follow-up infrastructure such as the one in Tanzania.
Tubular spine surgery is an excellent MISS option, but in LMIC settings several challenges limit its adoption. One major constraint is the requirement for an operative microscope, which is not always readily available; in many neurosurgical departments, microscopes are prioritized for other procedures, such as complex skull-base surgeries. Another significant limitation is the limited availability of hemostatic agents essential in tubular surgery: in Tanzania, products such as FloSeal, TachoSil, or surgical glues are not routinely available, making effective hemostasis particularly challenging in a narrow operative corridor. 27 In contrast, endoscopic spine surgery offers a major advantage: the continuous irrigation flow facilitates hemostasis, significantly reducing reliance on hemostatic agents. In our experience, hemostatic agents were rarely required in FESS techniques, and in UBE procedures hemostasis was successfully achieved using Surgicel, with no postoperative hematomas reported.
Our current data support the feasibility of spine endoscopy with acceptable early safety in an LMIC setting, with early reductions in ODI and VAS scores observed in this pilot cohort. In our series of 14 cases, no instances of cerebrospinal fluid leak, infection, or nerve root injury were observed, which is lower than complication rates reported in larger HIC series.28,29 Two individual patients merit explicit acknowledgement (Patient 4 and Patient 10, see Results), illustrating that group-level statistics smooth over real heterogeneity in response: at the individual level, 1 patient was a functional non-responder despite early pain relief, and one experienced gradual return of leg pain after immediate postoperative relief. These cases are visible in Figures 4 and 5 and warrant closer attention in larger cohorts.
Three categories of data that would normally accompany a surgical-implementation report were not recorded prospectively in this pilot phase: (i) operative time, (ii) per-case complication time-series, and (iii) structured assessments of technical proficiency were not administered. Their absence reflects the operational realities of an early-implementation course in a resource-constrained setting rather than a methodological choice, and we have chosen not to retrofit these data from incomplete records to preserve the integrity of the dataset. Without operative-time data we cannot describe the learning curve quantitatively, and without per-case complication time-series the absence of complications in this series cannot be parsed into early-versus-late case windows. Readers should weight this report as evidence of program feasibility and early safety, not as evidence of competence acquisition or operational efficiency. To address this gap going forward, we have established a prospective program at MOI that captures operative time, intra-operative event logs, structured proficiency scores, and per-case complication categorization for every minimally invasive and open spine case from the next case forward, with follow-up extended to a minimum of 12 months to enable assessment of durability, recurrence, and reoperation rates.
Organizing hybrid didactic, hands-on, and surgery courses is essential to support the effective development and safe implementation of new surgical techniques. Structured didactic sessions ensure that all participants share a common foundational knowledge; case-based discussions are equally important, as teaching a surgical technique without addressing appropriate indications and patient selection is incomplete and potentially unsafe in early adoption. Hands-on training is the other essential component. In Eastern Africa, access to such practical training remains limited30,31; data about training options is sparse. In South America, a survey 8 showed that the vast majority of spine surgeons lacked access to proper training and material to perform MISS, a finding echoed in other reviews. 9 A narrative review estimated that less than 25% of LMIC facilities are equipped with the appropriate tools to perform endoscopic surgery. 16 In Tanzania, cadaver-based training and teaching are not used for hands-on courses; spine models were utilized as an alternative, replicating spinal anatomy and enabling acquisition of fundamental technical skills.32,33
The improvised water-management setup illustrated in Figure 2 is reproducible with materials available in any operating theater (trash bags, plastic sheets, cotton drapes, tape) and may serve as a template for other LMIC teams adopting UBE without dedicated endoscopic drapes. Concerns around the difficult learning curve for endoscopic surgery are legitimate, especially for traditionally trained surgeons. However, evidence 34 and our own qualitative experience suggest these challenges can be mitigated through targeted hands-on training, structured mentorship, and early supervised practice.
Ensuring sustained training for local surgeons is essential for the long-term success of the program. In addition to the initial 5-day course, 2 Tanzanian neurosurgeons were sponsored by Joimax to complete a mini-fellowship in Germany, where they observed clinical cases and participated in cadaver-based training. An annual endoscopic spine course will be held in Tanzania to reinforce learning and facilitate the expansion of these techniques to other regional hospitals.
No formal cost-effectiveness analysis was performed in this study, and economic outcomes were not pre-specified endpoints. Studies in HIC populations have suggested that the advantages of shorter hospital stay, low postoperative infection rate, less use of postoperative medication, and quicker return to work compensate for potentially higher surgical costs over the long term.13,14,35-38. Whether these economic benefits transfer to LMIC settings, where consumable supply chains, maintenance arrangements, and indirect-cost structures differ substantially, remains an open question and an explicit hypothesis for future LMIC cost-effectiveness analyses. During this pilot phase, patient costs were maintained equivalent to those of open surgery; long-term sustainability will depend on consumables, maintenance, and local training capacity.
The UBE approach adds an additional layer of feasibility in LMICs because it reduces reliance on single-use instruments and can often be performed using equipment that is already available, such as the arthroscopic towers routinely used by orthopedic surgeons. In Ethiopia, 5 UBE procedures were successfully performed without major economic investment and with excellent patient outcomes. 18 . This flexibility makes UBE an appealing technique for hospitals seeking to adopt advanced spinal procedures despite financial constraints.
FESS currently remains more challenging to sustain without external support, given its higher equipment demands. We anticipate that UBE will be more widely adopted across LMICs, potentially paving the way for increased local manufacturing capacity and more sustainable solutions that facilitate the broader implementation of FESS techniques.
The sustainability of this program remains a key concern. Donated equipment is expected to remain functional for several years, with maintenance ensured by Joimax, and procurement pathways for essential consumables have already been initiated. Long-term sustainability will require ongoing local training and reliable supply chains.
Several important limitations should be acknowledged. First, the cohort was small (n = 14) and selected conservatively for low anatomical and surgical complexity; this highly conservative inclusion (14 of 78 screened, 18%) is a feature of an early-implementation pilot rather than a representative sample, and the complication rate and operative challenges reported here likely under-represent those that would be encountered in unselected real-world adoption. The results should be interpreted as reflecting optimal early implementation conditions rather than routine clinical practice. Second, no control group undergoing traditional open surgery was included; conclusions regarding equivalence or superiority cannot be drawn. Third, the 3-month follow-up window is sufficient to assess perioperative safety and immediate functional response but does not permit inference regarding durability, late recurrence, or reoperation; the prospective program described above captures these outcomes for future reporting. Fourth, operational metrics that would normally support evaluation of an early-implementation surgical program, operative time, per-case complication time-series, and structured technical-proficiency scores, were not captured prospectively in this pilot phase and are addressed separately in the §Methodological transparency subsection above. Fifth, reproducing these results in other LMIC hospitals that lack similar international support may be difficult; implementing these techniques without external support for structured training, mentorship, and material resources can be particularly challenging. We have initiated a prospective data-collection program for all patients undergoing surgery for degenerative spine conditions at MOI, including both minimally invasive and open techniques, which will help assess the true benefits of these approaches and identify areas for improvement. The new program prospectively records operative time (skin-to-skin and key-step durations), intra-operative event logs, per-case complication categorization, and structured technical-proficiency scores for both faculty and trainee operators, addressing the data gaps identified during this pilot phase.
Conclusion
Endoscopic spine surgery can be implemented in low-resource settings through structured international collaboration, with acceptable perioperative safety in this carefully selected pilot cohort. The early clinical outcomes reported here support program feasibility and early safety only; they do not provide evidence of durable benefit, comparative effectiveness, or generalizability to unselected practice. Larger, multicenter studies with longer follow-up are needed to validate these preliminary observations and to inform the responsible expansion of endoscopic spine surgery in LMIC environments.
Footnotes
Acknowledgments
Thank you to Joimax and Stryker for their equipment donations allowing the trainning and surgeries to take place.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare no financial relationships with Joimax or Stryker. Equipment and consumables were provided as donations without influence on study design, data analysis, or manuscript preparation.