
Abstract
Study Design
Retrospective case series.
Objectives
To analyze the perioperative complications of oblique lateral interbody fusion (OLIF) combined with unilateral pedicle screw fixation performed in a single lateral position.
Methods
Clinical data of 258 consecutive patients with lumbar degenerative diseases undergoing OLIF-UPS fixation in a single lateral position from July 2019 to June 2025 were collected. Both single- and multi-segment fusions were included. Demographic, intraoperative and perioperative data were extracted for statistical analysis.
Results
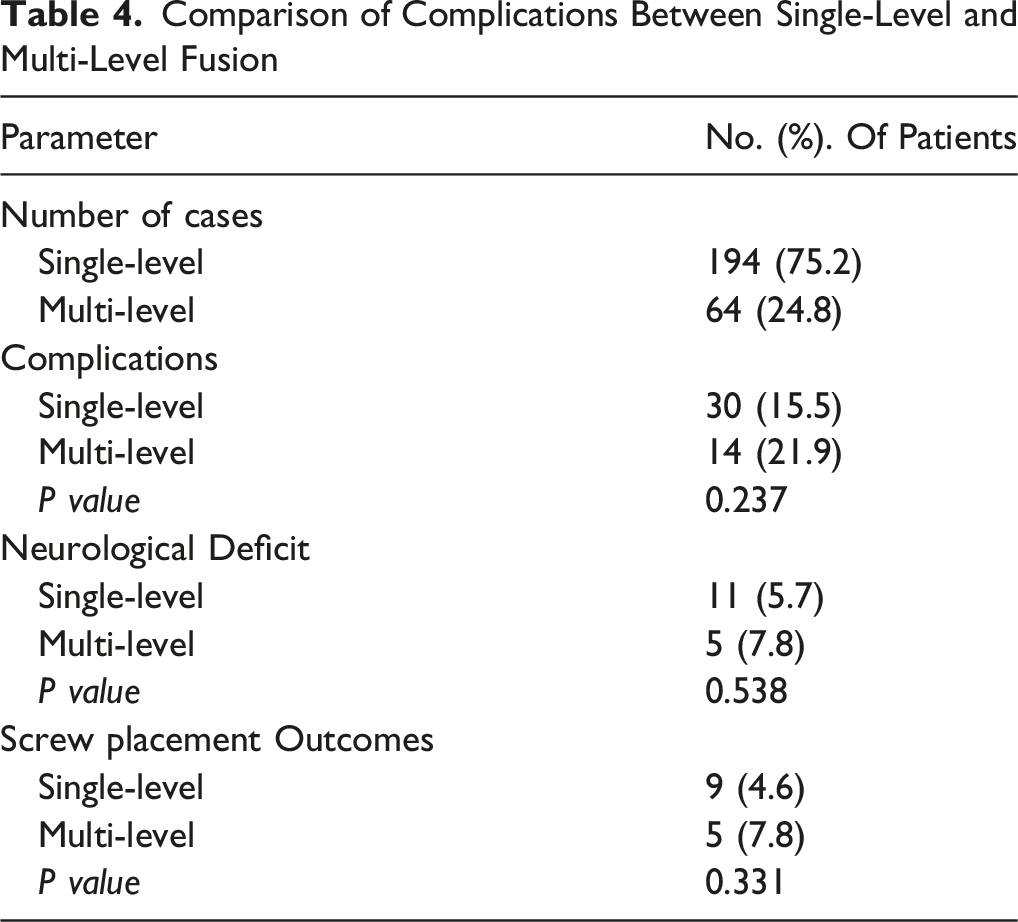
Among the 258 patients, the overall perioperative complication rate was 17.1%. Neurological deficits (6.2%) and pedicle screw insertion-related complications (5.4%) were the most common. Other complications included endplate injury (3.5%), cage malposition (2.7%), poor incision healing (1.9%), anterior longitudinal ligament injury (1.6%), vascular injury (1.6%), cage subsidence (1.2%), intestinal obstruction (1.2%), and peritoneal injury (0.4%). The complication rate was higher in the Multi-level fusion group than in the single-level group (21.9% vs. 15.5%, P=0.237). The incidences of neurological deficits (7.8% vs. 5.7%, P=0.538) and screw-related complications (7.8% vs. 4.6%, P=0.331) were also higher in the Multi-level group; however, none of these differences reached statistical significance.
Conclusions
The overall perioperative complication rate in this cohort was 17.1%, and the perioperative complications were manageable. Further controlled studies with long-term follow-up are needed to compare its efficiency and safety with alternative fixation protocols and positioning strategies.
Introduction
Oblique lateral interbody fusion (OLIF) has become a common minimally invasive procedure for lumbar degenerative diseases due to its advantages of minimal invasiveness and rapid recovery.1-4 With its widespread clinical application, complications of OLIF have gradually emerged. Literature reports indicate that the complication rate of OLIF ranges from 3.69% to 81.82%.1,5-7 Stand-alone OLIF carries a high risk of cage subsidence and migration8,9; therefore, it is often combined with pedicle screw fixation to enhance spinal stability and reduce cage subsidence.9,10 However, changing positions during OLIF with pedicle screw fixation increases operation time and additional risks.11,12
Single lateral position OLIF with pedicle screw fixation may reduce operative time and simplify workflow compared with lateral-then-prone positioning, as suggested by preliminary studies.13,14 However, in clinical practice, pedicle screw insertion was observed to be relatively difficult on the side adjacent to the operating table but highly feasible on the contralateral side in the lateral position. Previous studies have shown that although unilateral pedicle screw fixation is less stable than bilateral fixation during interbody fusion, it does not appear to compromise spinal stability or clinical outcomes.15,16 Currently, few studies have reported OLIF combined with unilateral pedicle screw fixation (OLIF-UPS) in a single lateral position, with no detailed description of perioperative complications. This retrospective study analyzed data from 258 patients with lumbar degenerative diseases (LDDs) treated with OLIF-UPS to detail perioperative complications.
Materials and Methods
Data Collection
Clinical data of 258 consecutive patients with LDDs who underwent single lateral position OLIF-UPS fixation from July 2019 to June 2025 were retrospectively analyzed. The data of this study were derived from the database of our hospital, and the study was approved by the hospital’s Ethics Committee prior to initiation.
LDDs included in this study involved 1 to 3 surgical segments, with preoperative diagnoses including lumbar spinal stenosis, lumbar disc herniation, lumbar spondylolisthesis, vertebral instability, and degenerative scoliosis. Exclusion criteria were severe spinal stenosis or disc herniation requiring nerve root exploration and decompression, lumbar spondylolisthesis > Grade II, combined with severe osteoporosis, lumbar fracture, infection or tumor, and a history of previous abdominal, retroperitoneal or lumbar surgery.
Demographic data included age, gender, BMI, BMD, comorbidities, preoperative diagnosis, and fusion levels. Intraoperative parameters included operation time, estimated blood loss, and intraoperative complications. Hospitalization data included length of stay. Screw placement outcomes, such as poor screw position requiring adjustment or wrong-level localization on intraoperative fluoroscopy, were also recorded. Postoperative radiographs were reviewed; if any of the three spine surgeons judged the screw position as unsatisfactory, CT was performed to confirm screw placement.
Surgical Technique
After general anesthesia, the patient was placed in the right lateral decubitus position with the trunk perpendicular to the table and hips and knees slightly flexed, secured with wide cloth tapes at the axilla and hip. C-arm fluoroscopy localized the target segment and marked the incision. The surgical field was disinfected and draped, reserving two operative windows for OLIF and posterior fixation.
OLIF procedure: A 3-5 cm oblique incision was made centered 4 cm ventral to the midpoint of the target disc space. The skin and subcutaneous tissue were incised layer by layer, and the abdominal muscles were bluntly dissected. The extraperitoneal fat was bluntly mobilized to expose the psoas major muscle, which was retracted dorsally to access the intervertebral space. A guidewire was inserted and verified under fluoroscopy. Sequential dilators and a lighted working channel were inserted and fixed into position. After discectomy, the intervertebral space was gradually distracted, and residual nucleus pulposus and cartilaginous endplate were thoroughly removed to prepare the fusion bed. A properly sized PEEK cage (Zhejiang Cohesion Medical Instruments Inc., China) filled with hydroxyapatite artificial bone graft (Altran Biomedical Inc., China) was implanted. Fluoroscopy was used to confirm satisfactory cage position. The surgical field was irrigated, and after ensuring hemostasis, the incision was closed layer by layer.
Posterior fixation: With the patient’s position unchanged, the operating table was raised. A 5-8 cm longitudinal incision was made 2-3 cm to the left of the spinous process. The soft tissues were dissected layer by layer, and the paraspinal muscle interval was separated bluntly to expose the screw entry point at the junction of the articular process and the midpoint of the transverse process. Using the horizontal plane as a reference, the entry point was opened with an awl, and a probe was inserted. Fluoroscopy was performed to confirm the target segment. After probing and tapping, pedicle screws were inserted. The remaining screws were placed freehand using the same technique. A connecting rod was installed and appropriately compressed. Final fluoroscopy confirmed satisfactory placement of all implants. After thorough irrigation and hemostasis, the incision was closed layer by layer and covered with sterile dressings. No drainage tubes were placed in any case.
Statistical Analysis
Statistical analysis was performed using SPSS 24.0 software (SPSS Inc., USA). Continuous data (age, operation time, estimated blood loss, length of hospital stay) were expressed as mean ± standard deviation, and comparisons between groups were made using independent samples t-test. Categorical data (gender, preoperative diagnosis, target segments, complications) were presented as n (%), and comparisons between groups were conducted using chi-square test. The two-tailed significance level α was set at 0.05.
Results
Patient Characteristics
Patient Characteristics
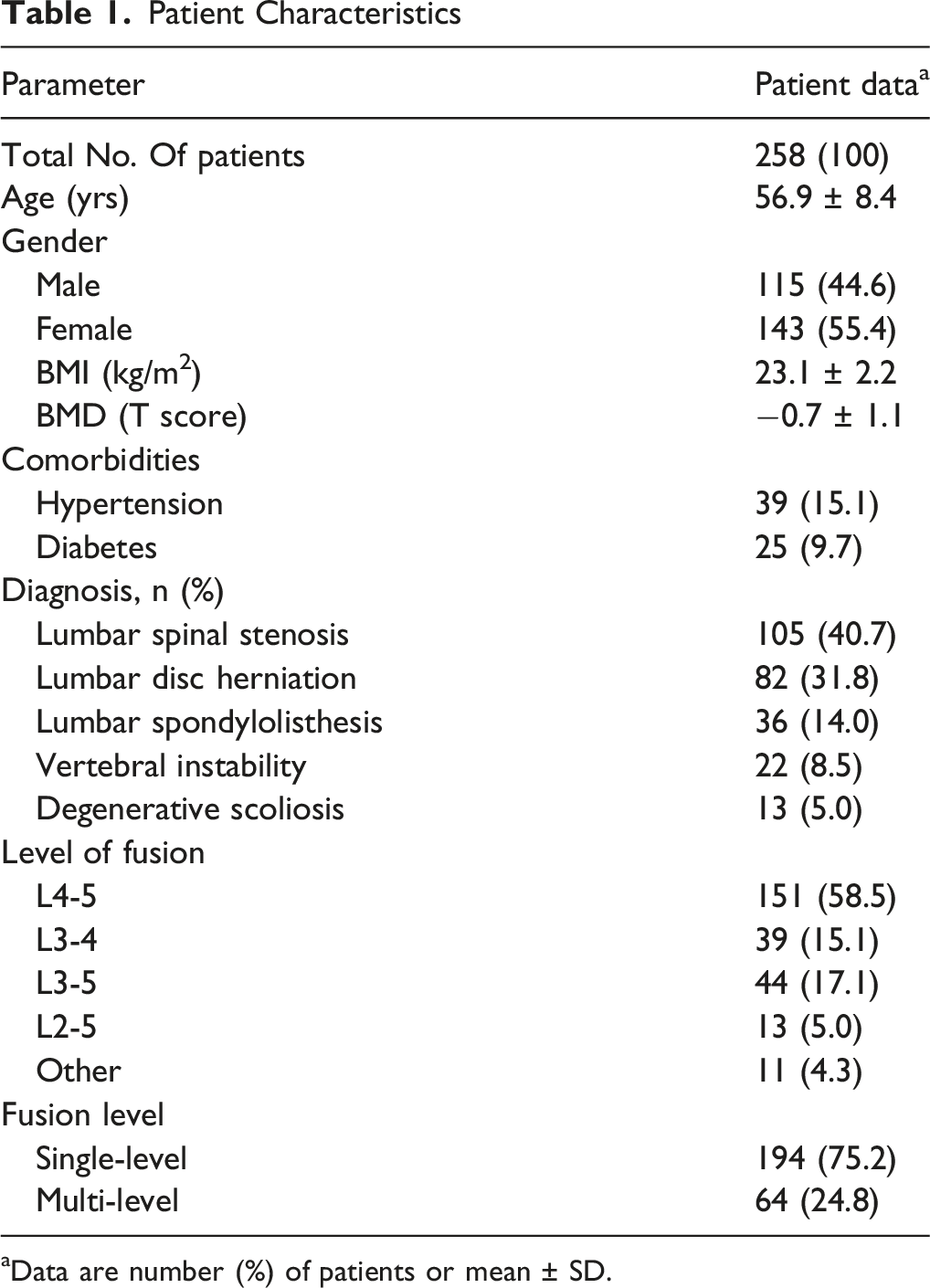
aData are number (%) of patients or mean ± SD.
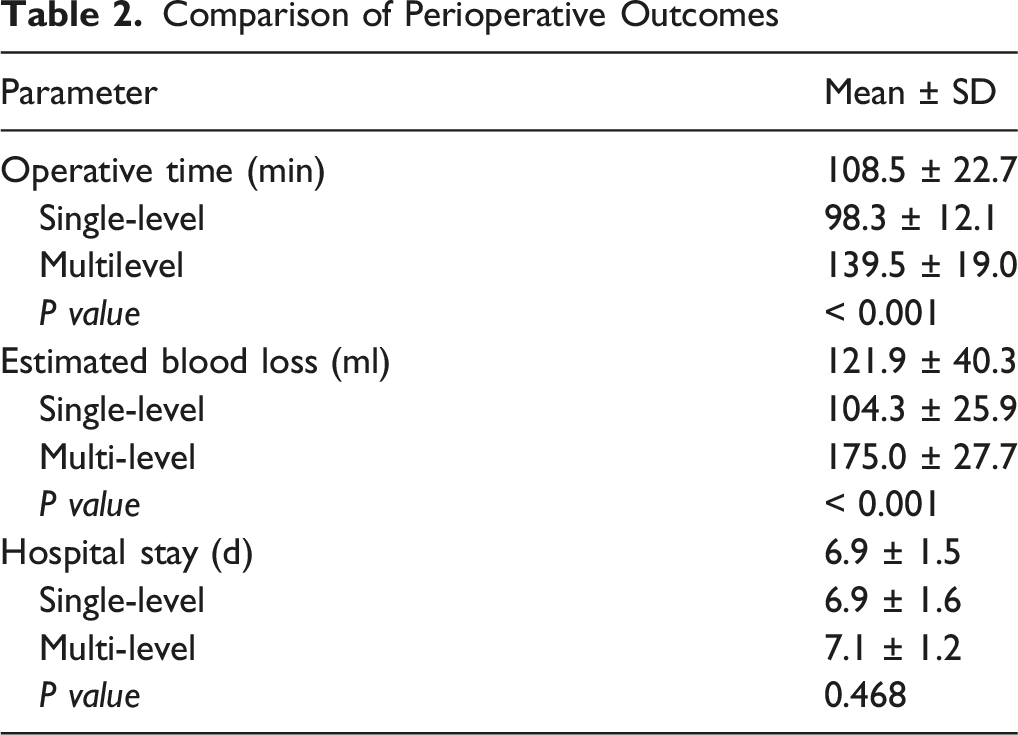
Perioperative Data and Complications
Comparison of Perioperative Outcomes
Complication Subgroups and Distribution
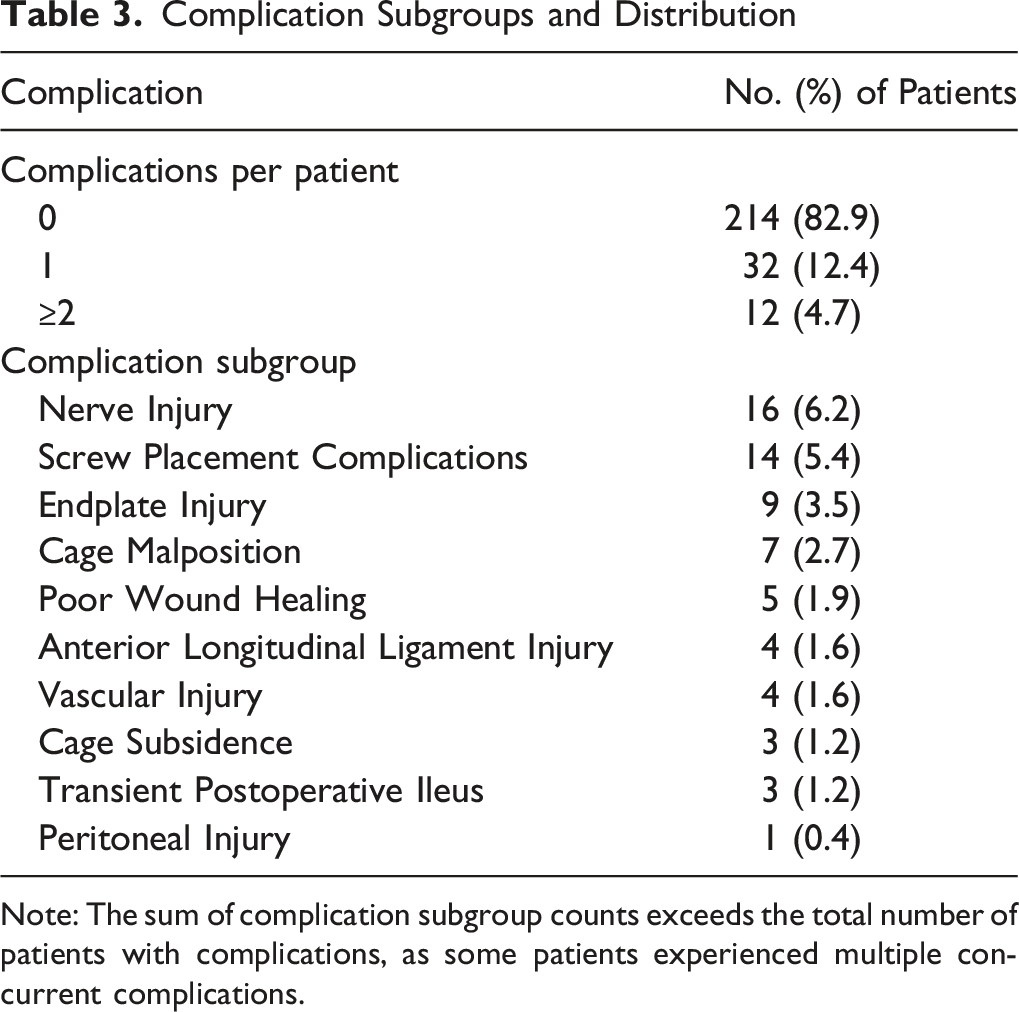
Note: The sum of complication subgroup counts exceeds the total number of patients with complications, as some patients experienced multiple concurrent complications.
Single-Level Surgery Compared With Multi-Level Surgery
Comparison of Complications Between Single-Level and Multi-Level Fusion
Neurological Deficit
Neurological deficits were identified in 16 patients (6.2%), all presenting on the first postoperative day, the majority (81.3%, 13/16) of whom achieved complete recovery to baseline neurological status during the perioperative period. These deficits were predominantly mild-to-moderate impairments in the regions innervated by the lumbar plexus, with no severe irreversible neurological injury occurring. Specifically, 11 patients (4.3%) exhibited weakness of the iliopsoas or quadriceps femoris. Following rehabilitation training and hyperbaric oxygen therapy, 8 patients (3.1%) recovered to baseline during the perioperative period, while 3 patients (1.2%) showed partial recovery with marked improvement compared with the immediate postoperative status. Additionally, 5 patients (1.9%) presented with lower extremity sensory disturbances, all of whom attained complete recovery after symptomatic treatment with neurotrophic medications.
Screw Placement Outcomes
All patients underwent pedicle screw placement via the left Wiltse approach in the lateral decubitus position. The incidence of screw-related complications was 5.4% (14/258), including 3 cases of intraoperative segmental localization error (all in single-level surgeries) and 6 cases requiring intraoperative adjustment due to suboptimal screw positioning under fluoroscopy (e.g., medial or inferior entry point deviation, inappropriate screw abduction angle). Postoperative CT identified 2 cases of medial pedicle cortical breach and 3 cases of lateral vertebral wall breach (Figure 1). Screw-related complications were observed more frequently in early operative cases. No formal learning-curve analysis was performed; therefore, a definitive proficiency cutoff cannot be determined from the present data. No vascular injury, neurological deficit, or screw loosening occurred postoperatively, and all patients were managed with regular follow-up. (A–D) Postoperative lumbar radiographs of a representative patient. The lateral view demonstrates mild cage subsidence; the anteroposterior view shows an excessive abduction angle of the L5 pedicle screw, and subsequent CT confirms screw penetration of the medial cortex (yellow arrow). (E–H) Postoperative lumbar radiographs of another patient. The anteroposterior view reveals an insufficient abduction angle of the L5 pedicle screw, and subsequent CT confirms screw penetration of the vertebral lateral wall (blue arrow)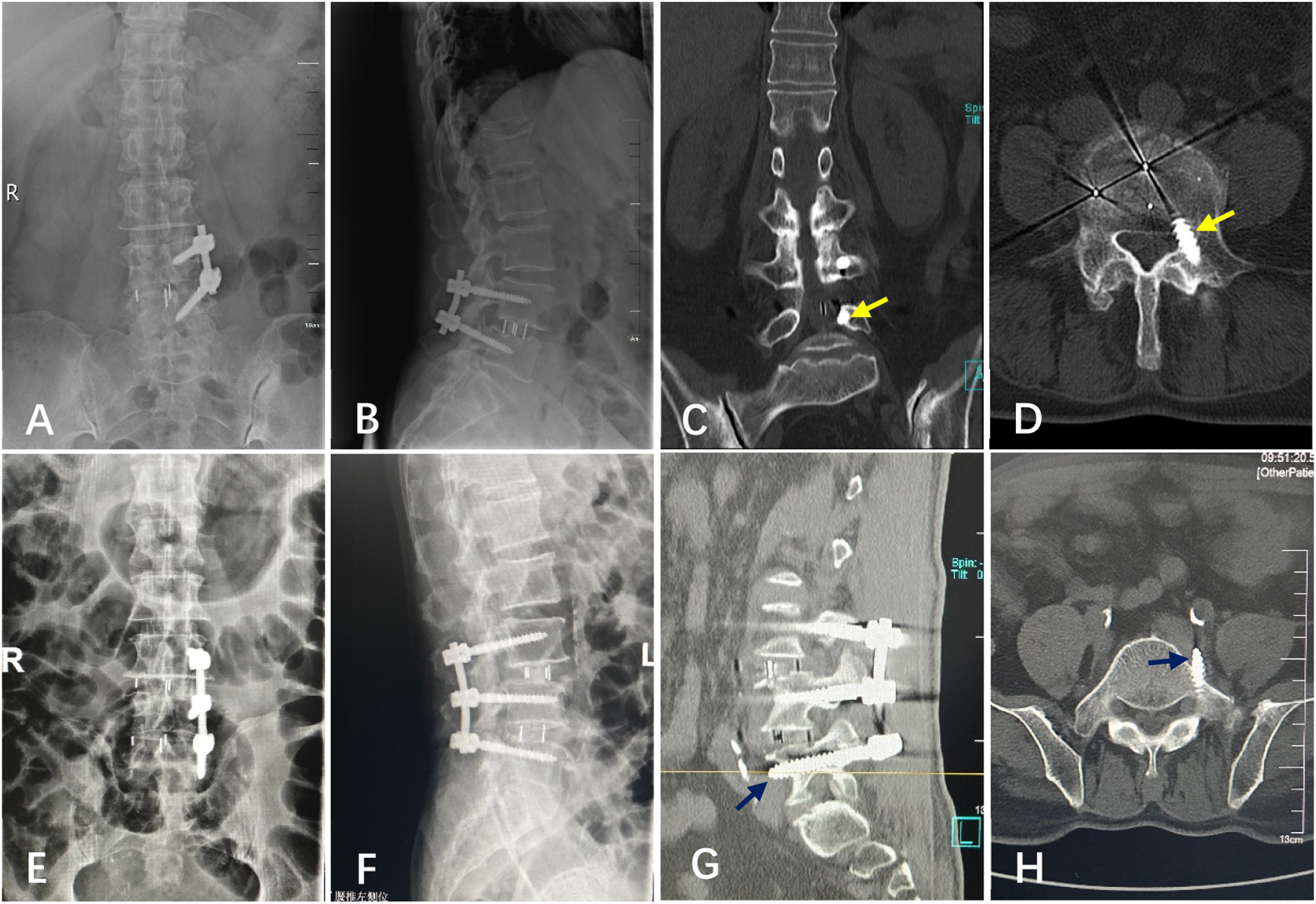
Vertebral Endplate Injury
Intraoperatively, endplate fractures occurred in 9 patients (3.5%), including 7 cases (2.7%) at the L4-5 segment and 2 cases (0.8%) at the L3-4 segment. Regarding surgical steps, 1 fracture occurred during intervertebral disc resection, 3 during endplate preparation, 1 each during trial mold placement and cage insertion, and 1 during pedicle screw insertion. Postoperative reexamination showed immediate cage subsidence in 3 patients with endplate fractures, but no relevant clinical symptoms were observed; all patients were followed up.
Unsatisfactory Cage Position
Poor cage positioning was defined as the cage being positioned adjacent to the anterior vertebral margin, approximated to the posterior vertebral margin, or non-parallel to the intervertebral space with subsequent endplate injury. Intraoperatively, cage malposition occurred in 7 patients (2.7%), consisting of 3 cases of anterior migration, 3 of posterior migration, and 1 case of angulated malposition non-parallel to the disc space accompanied by endplate injury (Figure 2). Of these, 1 case of anterior migration and 2 cases of posterior migration were corrected intraoperatively with satisfactory positioning; the remaining unadjusted cases remained asymptomatic postoperatively and were followed up routinely. (A) Endplate injury occurred at the L4-5 segment due to the cage not being aligned parallel to the intervertebral space during insertion (yellow arrow). (B) Anteriorly displaced cage with suboptimal position at the L3-4 segment (blue arrow)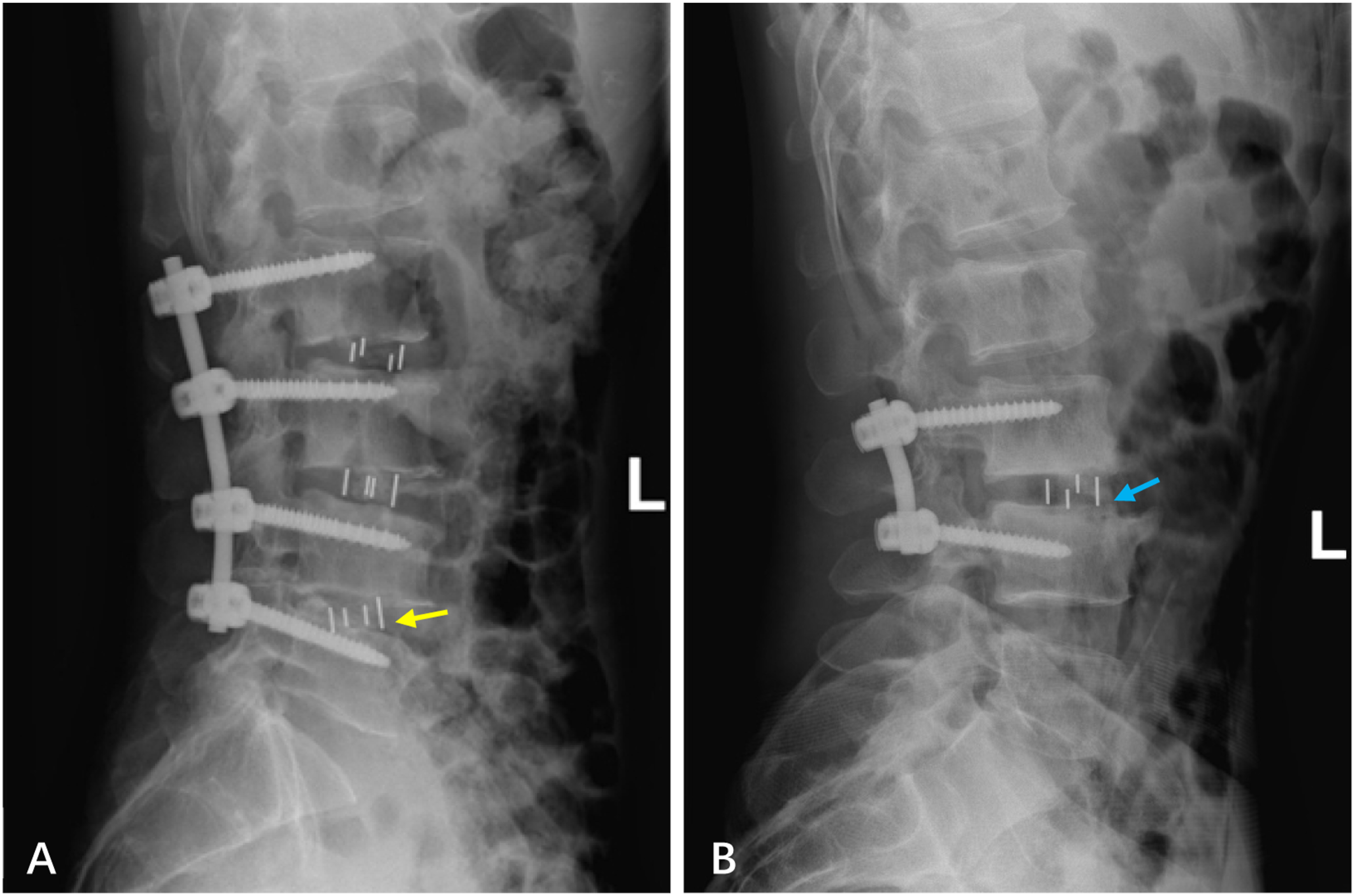
Other Complications
Intraoperative vascular injury occurred in 4 cases, including 1 case (0.4%) of iliolumbar vein injury and 3 cases of lumbar segmental artery injury. The minor laceration of the iliolumbar vein was managed with hemostasis by compression using gelatin sponge, and the operation was completed uninterruptedly without active bleeding in the surgical field. Segmental artery injuries were controlled precisely with bipolar coagulation. All 4 patients received routine drainage catheter placement; no excessive drainage was observed within 48 hours, and they were discharged smoothly after catheter removal. Intraoperative peritoneal injury occurred in 1 patient (0.4%) during disc space exposure, which was repaired immediately. The patient fasted on the operative day, and gastrointestinal function recovered on the first postoperative day without abdominal pain or distension. Anterior longitudinal ligament injury was noted in 4 cases (1.6%): 3 occurred during discectomy with nucleus pulposus forceps, and 1 resulted from excessive anterior angulation during trial insertion. All were partial injuries requiring no intraoperative intervention, and no cage migration was detected on postoperative imaging.
Postoperative wound healing disturbance occurred in 5 cases (1.9%), all of which achieved secondary healing after enhanced dressing care. Three patients (1.2%) developed transient postoperative ileus, which resolved spontaneously with early ambulation without pharmacological or surgical intervention.
Discussion
Interbody fusion is a common surgical method for lumbar degenerative diseases.17,18 With the increasing popularity of minimally invasive concepts, OLIF has emerged as a widely concerned minimally invasive technique in recent years.19,20 Different surgical approaches have specific complications: Anterior lumbar interbody fusion (ALIF) carries the risk of iliac vessel and peritoneal injury,21-23 while Lateral Lumbar Interbody Fusion (LLIF) requires psoas major muscle dissection and is prone to limited exposure of the lower lumbar spine.24,25 Thus, OLIF is considered an ideal technique to address the limitations of ALIF and LLIF, leading to its extensive clinical application. We adopted single lateral position OLIF-UPS fixation to provide spinal stability and optimize surgical workflow. However, relevant literature is scarce and lacks detailed descriptions of perioperative complications. Therefore, this study aims to conduct a detailed analysis of perioperative complications associated with single lateral position OLIF-UPS.
The overall incidence of perioperative complications in this study was 17.1% (44/258), including 32 patients with one complication and 12 with multiple complications. Complications were classified into OLIF approach-related complications, screw placement complications, and other local or systemic complications.
OLIF Approach Complications
Perioperative complications in this study were mainly OLIF approach-related, with neurological deficits (6.2%) as the most common, followed by endplate injury (3.5%). These results are generally consistent with previous literature. Abe et al.7 7 reported a 48.3% (75/155) perioperative complication rate in a multicenter OLIF study, with endplate fracture/subsidence (18.7%) being the most frequent, followed by transient psoas major weakness and thigh numbness (13.5%). Liu et al. 26 retrospectively analyzed 155 OLIF patients; besides donor site pain (24 cases, 21.2%), the main complication was neurological deficits (19 cases, 12.3%)—including 12 cases of thigh numbness/pain, 5 cases of psoas major/quadriceps weakness, and 2 cases of sympathetic neurological deficits—followed by vertebral endplate fracture (15 cases, 13.3%). In our study, the overall OLIF approach complication rate was 16.7%, with neurological deficits at 6.2% (mainly iliopsoas/quadriceps weakness and anterior thigh paresthesia) and endplate injury at 3.5%. These rates are lower than those reported above, possibly attributed to the continuous advancement of OLIF technology. Regarding segmental distribution, the incidence was relatively higher in multi-segment than single-segment surgery (7.8% vs 5.7%), which may be associated with prolonged psoas major muscle retraction during surgery. Most patients’ neurological symptoms recovered to baseline after symptomatic treatment.
During exposure, 1 case (0.4%) of peritoneal injury and 4 cases (1.6%) of vascular injury occurred. The former was managed with intraoperative repair and postoperative fasting; the latter included 1 case (0.4%) of iliolumbar vein injury (hemostased with compression due to a small laceration) and 3 cases (1.2%) of segmental artery injury (hemostased with bipolar electrocoagulation). All 4 patients had indwelling drainage tubes intraoperatively. Fortunately, no relevant symptoms occurred postoperatively, but the hospital stay was prolonged in patients with peritoneal or vascular injury. Literature reports indicate the incidence of peritoneal injury and iliolumbar vein injury is 0.6% each, 1 and that of segmental artery injury is 2.6%. 7 Notably, failure to detect these injuries intraoperatively may lead to severe consequences. Therefore, careful operation during exposure is required to avoid excessive blunt dissection, excessive retractor force, and insufficient visual field exposure, thereby reducing exposure-related complications.
During intervertebral space preparation and cage insertion, 8 cases of endplate injury, 7 cases of cage malposition, and 4 cases of anterior longitudinal ligament injury occurred. Endplate injury mainly occurred at the L4-5 segment, possibly due to iliac bone obstruction and the high proportion of pathological lesions at this segment. Endplate injury is one of the common complications,7,26 most likely to occur during cartilaginous endplate preparation. Uniform force application and avoidance of violent operation are required. One case of endplate injury occurred during trial mold placement due to incorrect anterior-posterior orientation of the mold. Intraoperative cage malposition included 3 anteriorly displaced cages, 3 posteriorly displaced cages, and 1 cage not parallel to the vertebral plate (causing endplate injury); despite intraoperative adjustments, 4 cases remained unsatisfactory. The main cause of anterior longitudinal ligament injury was excessive anterior placement during intervertebral disc resection. This reminds us to confirm the satisfactory position of the positioning guide pin via intraoperative fluoroscopy before establishing the working channel, so as to avoid cage malposition and reduce anterior longitudinal ligament injury.
Screw Placement Complications
The purpose of OLIF-assisted pedicle screw fixation is to enhance spinal stability. All screws were inserted on the left side via the Wiltse approach with the patient in the right lateral decubitus position, which is relatively convenient due to distance from the operating table. Nevertheless, positional changes can still affect screw placement outcomes.
In this study, the incidence of screw placement complications was 5.4%. Intraoperative fluoroscopy after positioning pin insertion revealed 3 cases of segmental errors, all occurring in single-segment surgeries. This may be related to less familiar exposure techniques in the lateral position and the narrower margin for error in single-segment procedures. We recommend confirming the incision location via fluoroscopy before exposure, and using hemostats or syringe needles placed at the facet joint for additional fluoroscopic verification of vertebral segments prior to screw insertion. Post-insertion fluoroscopy showed 6 cases of unsatisfactory screw positioning that required intraoperative adjustment. These cases occurred mainly in early cases and were closely associated with less familiar screw placement techniques in the lateral position. Postoperative CT reexamination identified 5 cases of pedicle screw cortical breach, but no signs of vascular/neurological injury or screw loosening were observed.
Furthermore, screw-related complications were observed more frequently in early operative cases. Collectively, screw placement in the lateral decubitus position appeared technically feasible and did not raise significant safety concerns in this series.
Other Complications
Five cases of poor postoperative wound healing were observed, all at the posterior screw placement incisions. No significant abnormalities in infection markers were detected, and microbial cultures were negative; all cases healed and were discharged after 3–5 days of intensive dressing changes. This may be related to patients’ well-developed paraspinal muscles, which necessitated substantial soft tissue retraction during surgery. Additionally, 3 cases of transient postoperative ileus occurred postoperatively, resolving spontaneously shortly after early ambulation.
Limitations and Prospects
This study has several limitations. First, as a retrospective single-center study, selection bias was inevitable and external validity is limited; therefore, the findings may not be widely generalizable. Second, patients with osteoporosis, lumbar fracture, infection, tumor, and other comorbidities were excluded, so the results cannot be generalized to the entire spectrum of lumbar diseases. Third, this was a case series without a control group (e.g., lateral decubitus OLIF combined with prone bilateral pedicle screw fixation), making it difficult to directly compare complication profiles between this technique and conventional procedures. Fourth, postoperative CT was not routinely performed to assess screw accuracy; instead, CT was only obtained when abnormalities were suspected on digital radiography, which may have underestimated the incidence of screw-related complications. Finally, this study only focused on perioperative complications and did not evaluate long-term clinical and radiological outcomes, such as interbody fusion rate, cage subsidence rate, and reoperation rate, which warrant further investigation.
Although the sample size was relatively sufficient, the single-center retrospective design and lack of long-term follow-up limited the evaluation of the long-term clinical value and functional outcomes of this technique. Therefore, the generalizability of the results should be interpreted with caution, and further prospective, multi-center controlled studies with extended follow-up periods are required to verify the long-term safety and efficacy of this technique, as well as its reproducibility in non-high-volume centers. Overall, single-position lateral decubitus OLIF combined with unilateral pedicle screw fixation was associated with acceptable intraoperative performance and a manageable perioperative complication profile in the present case series.
Conclusions
This single-center retrospective study demonstrated that single-position lateral decubitus OLIF combined with unilateral pedicle screw fixation yielded an overall perioperative complication rate of 17.1%. The perioperative complications observed in this series were manageable. Further controlled studies with long-term follow-up are needed to compare its efficiency and safety with alternative fixation protocols and positioning strategies.
Footnotes
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the institutional review board of First People’s Hospital of Yunnan Province (IRB number: KHLL2024⁃YJ021). We confirmed that all methods were carried out in accordance with relevant guidelines and regulations.
Consent to Participate
The consent statement was waived due to the retrospective nature of the study.
Author Contributions
Yonghui Zhao and Sheng Lu conceived and designed the study. Yonghui Zhao drafted the manuscript. Qiunan Lyu, Hui Zhong, Jie Liu, Qiyang Wang, and Weicheng Lin collected the data. Qiyang Wang and Weichao Li analyzed the data. Weicheng Lin, Qiunan Lyu, Hui Zhong, Jie Liu, and Jiayu Chen provided technical support. All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Yunnan Clinical Medical Center for Spine and Spinal Cord Diseases (ZX2022000101-2024JSKFKT-22), Applied Basic Research Joint Project of Kunming Medical University (202301AY070001-293), Xingdian Talent Support Program — Yunling Scholar Project (XDYC-YLXZ-2022-0015) and Medical Reserve Talent Training Program of Yunnan Provincial Health Commission for Prevention and Control Key Technologies (H-2024032).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.