
Abstract
Study Design
Retrospective cohort study.
Objectives
To determine whether the 5-item modified frailty index (mFI-5) is associated with in-hospital complications and 1-year adverse events among patients aged ≥70 years who underwent lumbar spine surgery.
Methods
We retrospectively reviewed data from patients aged ≥70 years who underwent lumbar spine surgery at a single tertiary referral hospital from January 2020 to December 2021, with 1-year follow-up. Participants were stratified into two groups based on an mFI-5 score of 3. The primary outcome was the odds of in-hospital complications, and the secondary outcome was the odds of 1-year adverse events. To account for confounding variables and identify independent predictors, we applied inverse probability of treatment weighting (IPTW) and multivariable logistic regression.
Results
Among 967 eligible older adults, 132 (13.6%) met the criteria for severe frailty (mFI-5 score ≥3). Following IPTW adjustment, severe frailty was significantly and independently associated with in-hospital complications (odds ratio: 1.792, 95% confidence interval: 1.243–2.585; P = 0.002). Higher American Society of Anesthesiologists Physical Status scores, functional dependence, and in-hospital complications were strong predictors of 1-year adverse events.
Conclusion
Severe frailty was independently associated with in-hospital complications in older adults undergoing lumbar spine surgery. The mFI-5 may serve as a practical tool for stratifying preoperative surgical risk and tailoring perioperative management.
Introduction
With the rapid acceleration of global aging, there is a steady rise in the number of elderly patients requiring spine surgery for degenerative conditions. 1 This trend is primarily driven by the fact that age-associated spinal deterioration, such as intervertebral disc degeneration and osteophyte development, occurs more frequently in older adults and serves as a major underlying cause for spinal disorders like spinal stenosis. 2 Accordingly, practical and clinically applicable preoperative risk assessment tools are needed to evaluate this increasingly prevalent and vulnerable patient population. 3 This is particularly critical for patients aged 70 years and older, in whom the depletion of physiological reserve and susceptibility to surgical stress become exponentially more pronounced.4,5
Frailty, defined as increased vulnerability to stressors due to diminished physiological reserves across multiple organ systems, compromises the ability to maintain homeostasis following surgical trauma. 6 Frailty increases with age and is associated with adverse health outcomes. 7 As a result, identifying eligible surgical candidates and estimating postoperative risk in older adults are clinically important. The mFI-5, a widely used measure of frailty, was derived from the 11-item modified frailty index (mFI-11) following changes in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) that reduced the number of available frailty factors from 11 to 5. 8 The mFI-11 was originally developed using frailty variables derived from the Canadian Study of Health and Aging Frailty Index (CSHA-FI). 9 Both mFI-5 and mFI-11 have prognostic utility for postoperative morbidity and mortality.10-12 In parallel, imaging-based morphometric measures are increasingly being used as adjunctive tools for preoperative risk stratification.
Sarcopenia, a progressive skeletal muscle disorder characterized by the loss of muscle mass and function, serves as a quantifiable indicator of physiological aging and provides a valuable complementary approach for assessing diminished physical reserve in surgical candidates.13,14 Frailty reflects systemic vulnerability to physiological stressors, whereas sarcopenia reflects skeletal muscle impairment and may independently influence postoperative outcomes. 15 Although the prognostic utility of frailty index has been elucidated in spine surgery cohorts,8,16 this clinical index inherently lacks the ability to capture morphological and physical depletion. Consequently, investigating the synergistic predictive value of combining a comorbidity-based frailty index (mFI-5) with an objective, imaging-based morphometric tool remains a critical gap in the current literature. Furthermore, while previous research has predominantly focused on short-term morbidity, the longitudinal trajectory of these highly vulnerable older adults warrants comprehensive evaluation.
Therefore, this study aimed to assess whether the mFI-5 and imaging-defined sarcopenia—both independently and in combination—are associated with a continuum of postoperative outcomes, ranging from immediate in-hospital complications to 1-year adverse events in adults aged ≥70 years undergoing spine surgery.
Methods
Study Design and Population
This study was approved by the Institutional Review Board of Yonsei University’s Gangnam Severance Hospital, Seoul, South Korea (Approval No. 3-2023-0353; approval date: November 21, 2023). The need for informed consent was waived given the retrospective design of the study. The study cohort included patients aged ≥70 years who underwent lumbar spine surgery at Gangnam Severance Hospital between January 1, 2020, and December 31, 2021. Although the World Health Organization and United Nations traditionally define the elderly as individuals aged 60–65 years, modern spine surgery literature indicates that age ≥70 years is a more clinically critical threshold for physiological decline. Previous studies stratifying patients by decade cohorts have demonstrated that patients in their 60s often maintain sufficient physiological reserves to tolerate lumbar fusion similar to the younger population and that the incidence of adverse postoperative events and systemic complications increases exponentially from the seventh decade of life. 17 Furthermore, age over 70 years has been established as a robust independent risk factor for perioperative morbidity in large-scale spine registries. 18 Accordingly, we have defined our geriatric cohort using the age cut-off of 70 years to specifically focus on this highly vulnerable population. 5
Eligible participants were followed for 1 year postoperatively, with follow-up completed by December 31, 2022. Surgical interventions included discectomy, laminectomy, decompression, laminoplasty, spinal fusion, and other spinal reconstructive procedures. Patients with missing data or who were lost to follow-up were excluded from the analysis. All patients received standardized perioperative care incorporating key principles of Enhanced Recovery After Surgery (ERAS), 19 including multimodal analgesia, prevention of postoperative nausea and vomiting, and early mobilization, aiming to minimize physiological stress in this vulnerable geriatric cohort. The study complied with the 1964 Declaration of Helsinki and its 2013 revision.
Data Collection and Definitions
Information was extracted from an institutional observational registry established to evaluate postoperative outcomes in geriatric patients undergoing spine surgery. Additional demographic and clinical data were obtained from electronic medical records. The study variables included age, sex, body mass index (BMI), preoperative anticoagulant use, comorbidities, American Society of Anesthesiologists Physical Status (ASA-PS), primary diagnosis, lesion location, and surgical technique. Additionally, intraoperative data, including surgical duration, estimated blood loss, fluid administration, transfusion volume, and urine output, were obtained from anesthesia records. The transfusion threshold was typically set at a hemoglobin level of 8.0 g/dL and adjusted on a case-by-case basis depending on intraoperative blood loss and hemodynamics.
Frailty was quantified using the mFI-5, which assesses five variables: diabetes mellitus, hypertension requiring medications, chronic obstructive pulmonary disease, congestive heart failure, and functional dependence. The mFI-5 score ranges from 0 to 5, with higher scores indicating greater frailty. For this study, patients with a score ≥3 were classified as having severe frailty. 8 Following initial automated query from the registry, authors manually verified the data against electronic medical records to ensure the completeness of mFI-5 scores and surgical outcomes. Any cases with missing or ambiguous data were excluded from the final analysis to maintain the robustness of the cohort.
Sarcopenia was evaluated preoperatively on computed tomography (CT) by measuring the total psoas area (TPA), defined as the combined cross-sectional area of the left and right psoas muscles. Following established protocols, TPA was measured on axial CT images at the L3 and L4 vertebral levels using the first slice moving in the craniocaudal direction on which both transverse processes were clearly visible.13,14 Measurements were performed using a semi-automated method consisting of manual delineation of the margins of the bilateral psoas muscles with attenuation thresholds from –30 to 110 Hounsfield units to exclude non-muscle tissue. The psoas muscle index (PMI) was calculated by dividing TPA by height squared (cm2/m2). For inter-rater reliability assessment, two evaluators independently measured the bilateral psoas areas in consecutive subjects. For intra-rater reliability assessment, each evaluator repeated the measurements after an interval of at least 2 weeks.
Outcome Assessment
The primary outcome was in-hospital complications. This outcome included any of the following events that occurred after surgery and before discharge: surgical complications (such as hematomas or wound infections); ileus; and cardiovascular, neurological, or pulmonary complications. These complications were diagnosed by attending physicians based on clinical presentation, laboratory findings, electrocardiography, and radiological imaging.
The secondary outcome was 1-year adverse events. Patients were followed up for 1 year or until they died, whichever occurred first. This outcome included all-cause mortality, as well as any hepatic, renal, pulmonary, neurological, cardiovascular, or other unspecified medical conditions. We also aimed to identify prognostic factors related to in-hospital complications and 1-year adverse events, including sarcopenia.
Statistical Analysis
Sample size was determined by data availability given the retrospective design of the study. The patients were divided into two groups based on an mFI-5 score of 3. A post hoc power analysis was conducted using PASS version 15 (NCSS, LLC, Kaysville, UT, USA) based on logistic regression models to assess the association between the mFI-5 score and the primary and secondary outcomes. The resulting post hoc statistical powers for these outcomes were 80% and 94%, respectively.
Continuous variables were analyzed using an independent two-sample t-test and presented as mean ± standard deviation for normally distributed data. Categorical variables were compared using the χ2 or Fisher’s exact test, as appropriate, and presented as counts and percentages.
IPTW was performed using propensity scores estimated from age, gender and the underlying spinal pathology to minimize confounding. In the IPTW set, continuous variables were presented as weighted means with standard errors, and categorical variables were presented as weighted frequencies and percentages. Following IPTW, covariate balance between the two groups was assessed using standardized mean differences (SMD). An absolute standardized difference of less than 0.1 was considered to indicate negligible imbalance.
Potential risk factors for outcomes were identified using univariate logistic regression analysis. Variables with P < 0.05 were included in a multivariable logistic regression model with stepwise variable selection. IPTW was additionally used as a sensitivity analysis to assess the robustness of the association with the study outcomes.
Statistical analyses were conducted using SAS software (version 9.4; SAS Institute, Cary, NC, USA) and R version 4.3.2 (The R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was considered at two-tailed P < 0.05.
Results
Among 3,399 consecutive surgical candidates screened during the study period, 2,207 were excluded by age. Among the remaining 1,192 geriatric patients, 225 were excluded because they had not undergone lumbar spine surgery and therefore did not have lumbar CT images available for analysis. Ultimately, the cohort comprised 967 participants. The overall 1-year mortality rate for the entire cohort was 0.3% (3 patients). Using an mFI-5 score of 3, the cohort was stratified into a severe frailty group (mFI-5 ≥ 3; n = 132, 13.6%) and a comparison group (mFI-5 < 3; n = 835, 86.4%; Figure 1). Flowchart of patient selection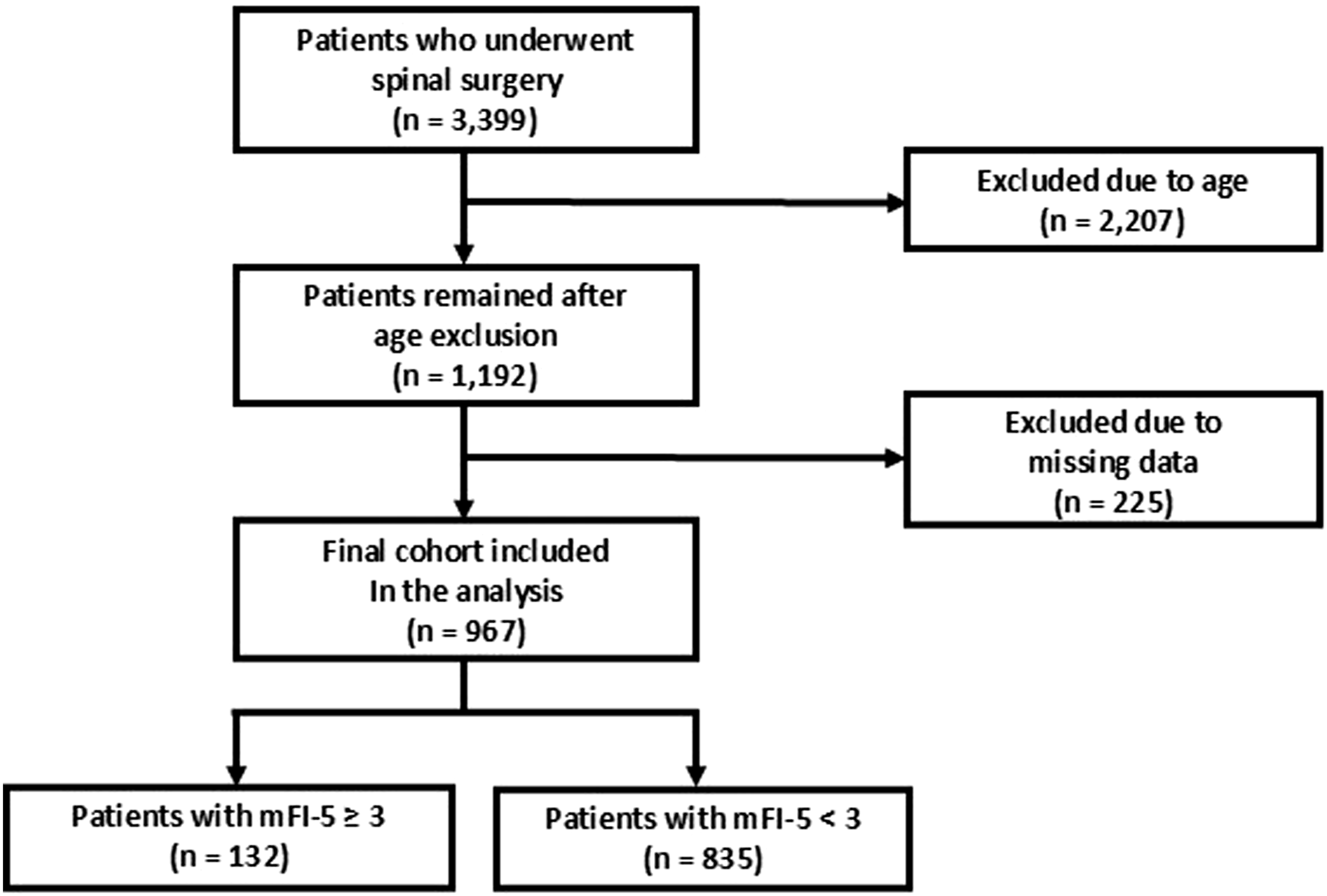
Baseline Demographic and Clinical Characteristics After Inverse Probability of Treatment Weighting (IPTW)
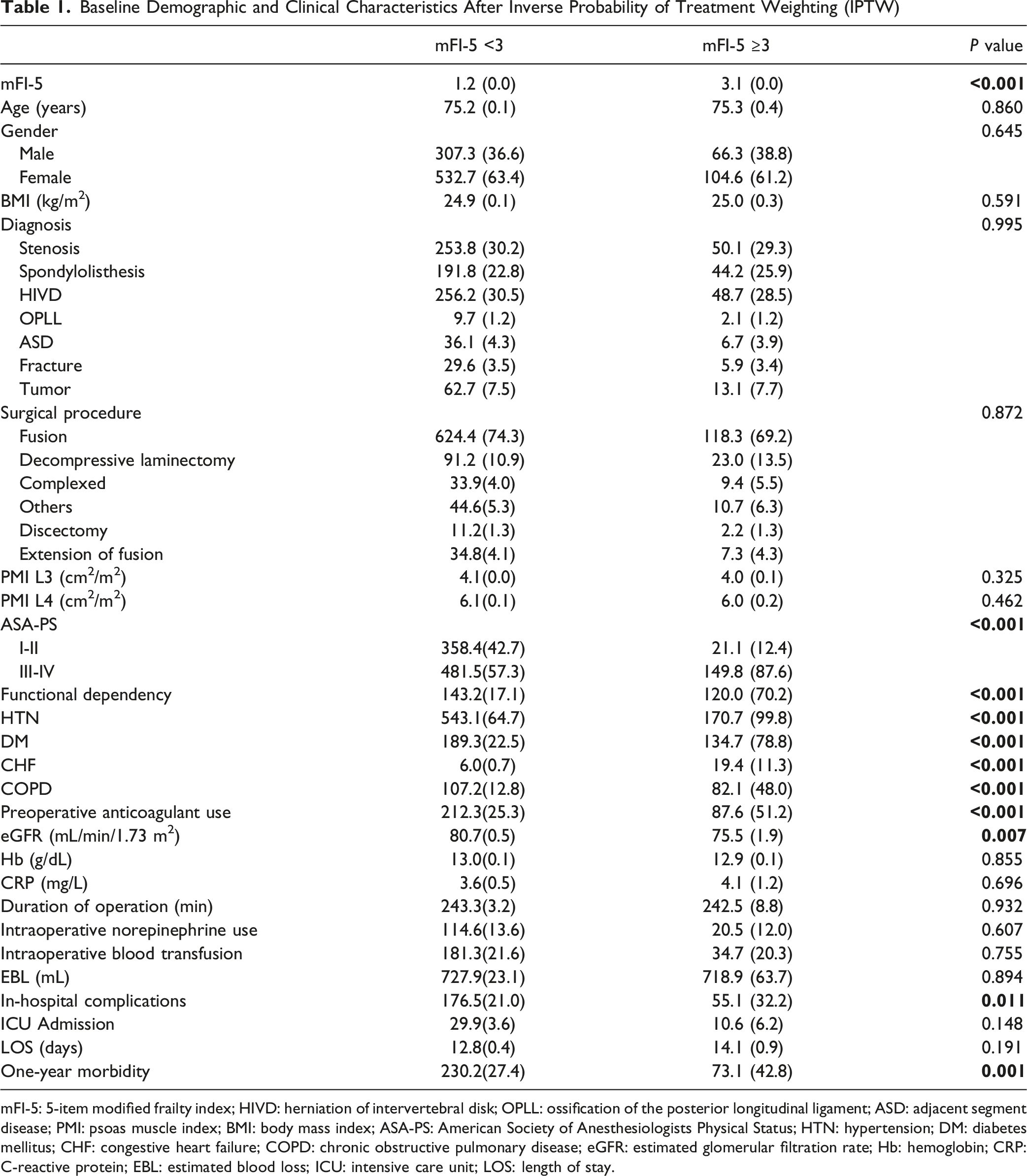
mFI-5: 5-item modified frailty index; HIVD: herniation of intervertebral disk; OPLL: ossification of the posterior longitudinal ligament; ASD: adjacent segment disease; PMI: psoas muscle index; BMI: body mass index; ASA-PS: American Society of Anesthesiologists Physical Status; HTN: hypertension; DM: diabetes mellitus; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; eGFR: estimated glomerular filtration rate; Hb: hemoglobin; CRP: C-reactive protein; EBL: estimated blood loss; ICU: intensive care unit; LOS: length of stay.
Independent Risk Factors for In-Hospital Complications: Multivariable Logistic Regression Analysis With and Without Inverse Probability of Treatment Weighting
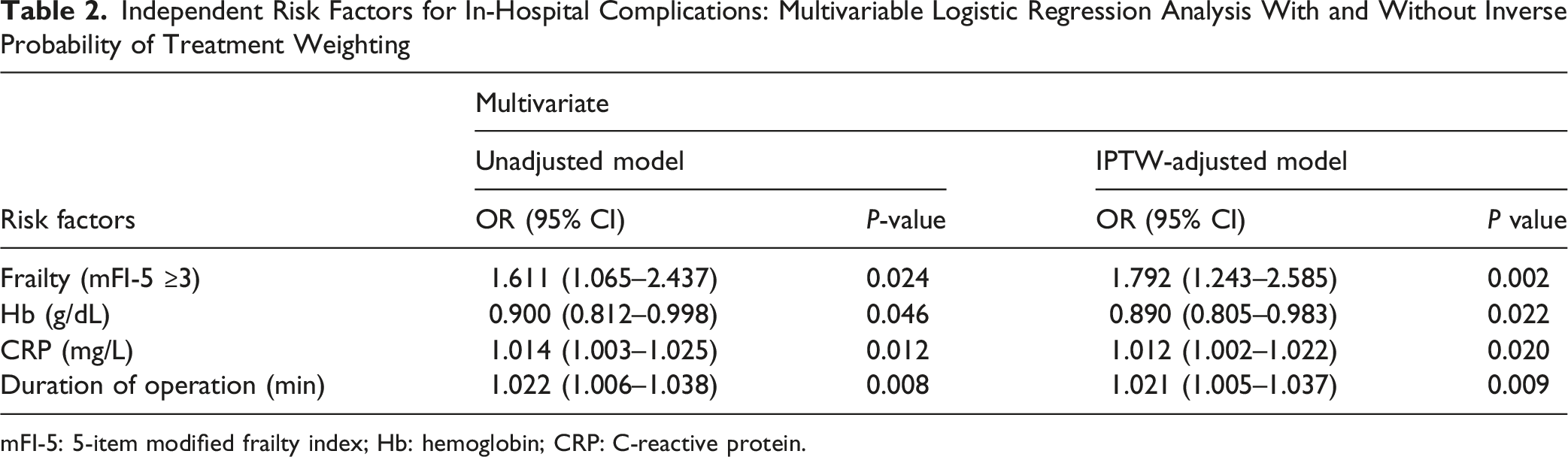
mFI-5: 5-item modified frailty index; Hb: hemoglobin; CRP: C-reactive protein.
Independent Risk Factors for 1-Year Adverse Events After Lumbar Spine Surgery: Multivariable Logistic Regression Analysis With and Without Inverse Probability of Treatment Weighting
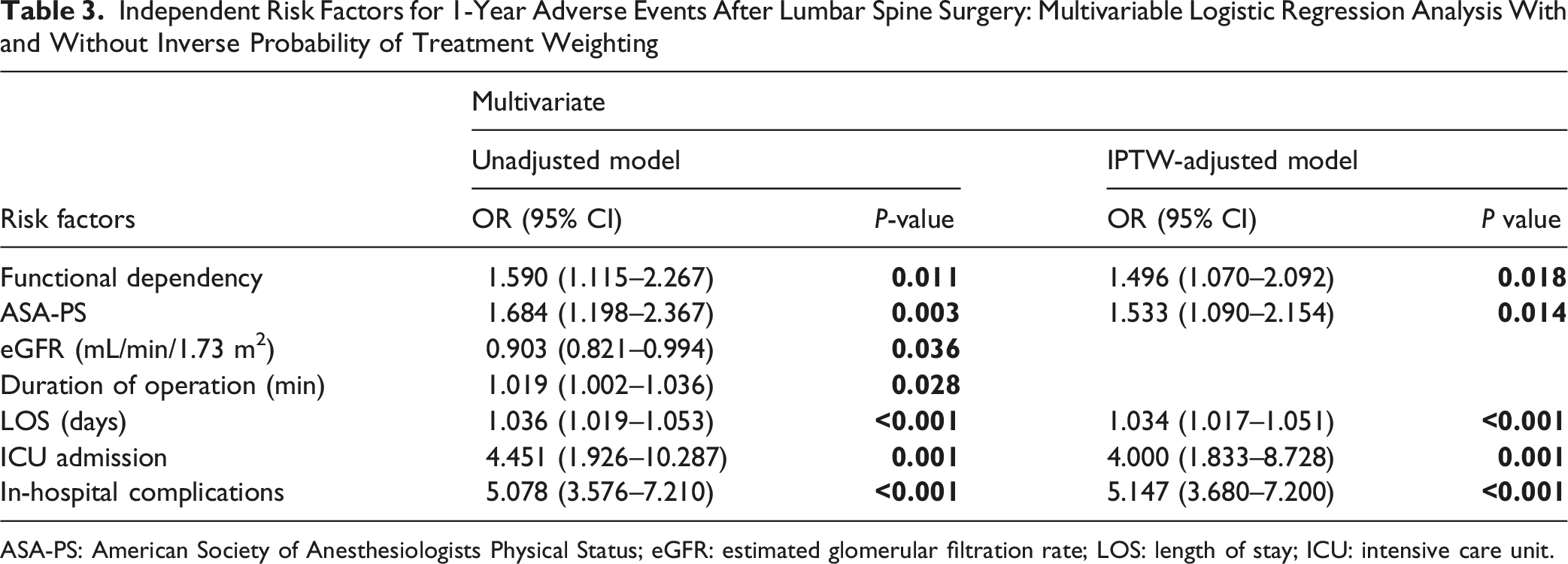
ASA-PS: American Society of Anesthesiologists Physical Status; eGFR: estimated glomerular filtration rate; LOS: length of stay; ICU: intensive care unit.
Association of mFI-5 and Its Individual Components With In-Hospital Complications and 1-Year Morbidities
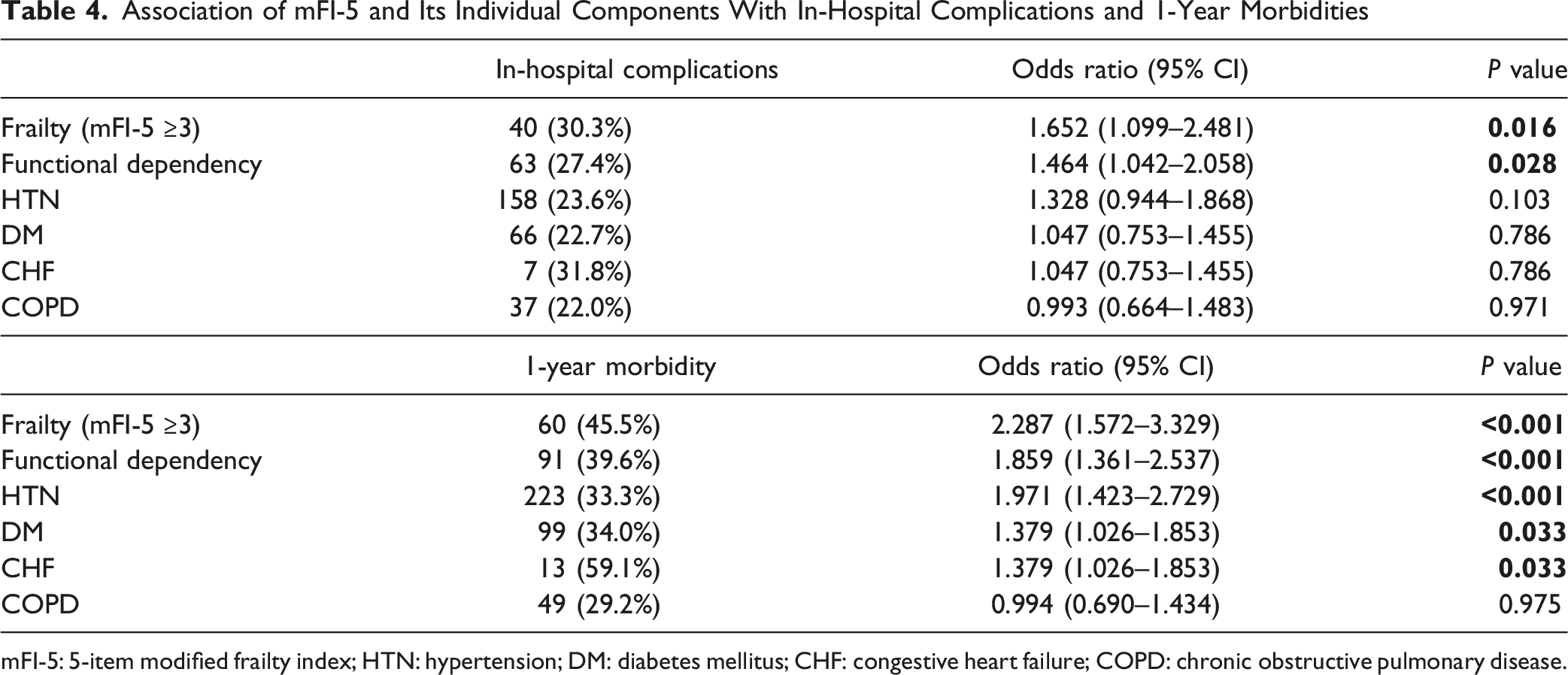
mFI-5: 5-item modified frailty index; HTN: hypertension; DM: diabetes mellitus; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease.
Risk of In-Hospital Complications and 1-Year Morbidities According to mFI-5 Scores
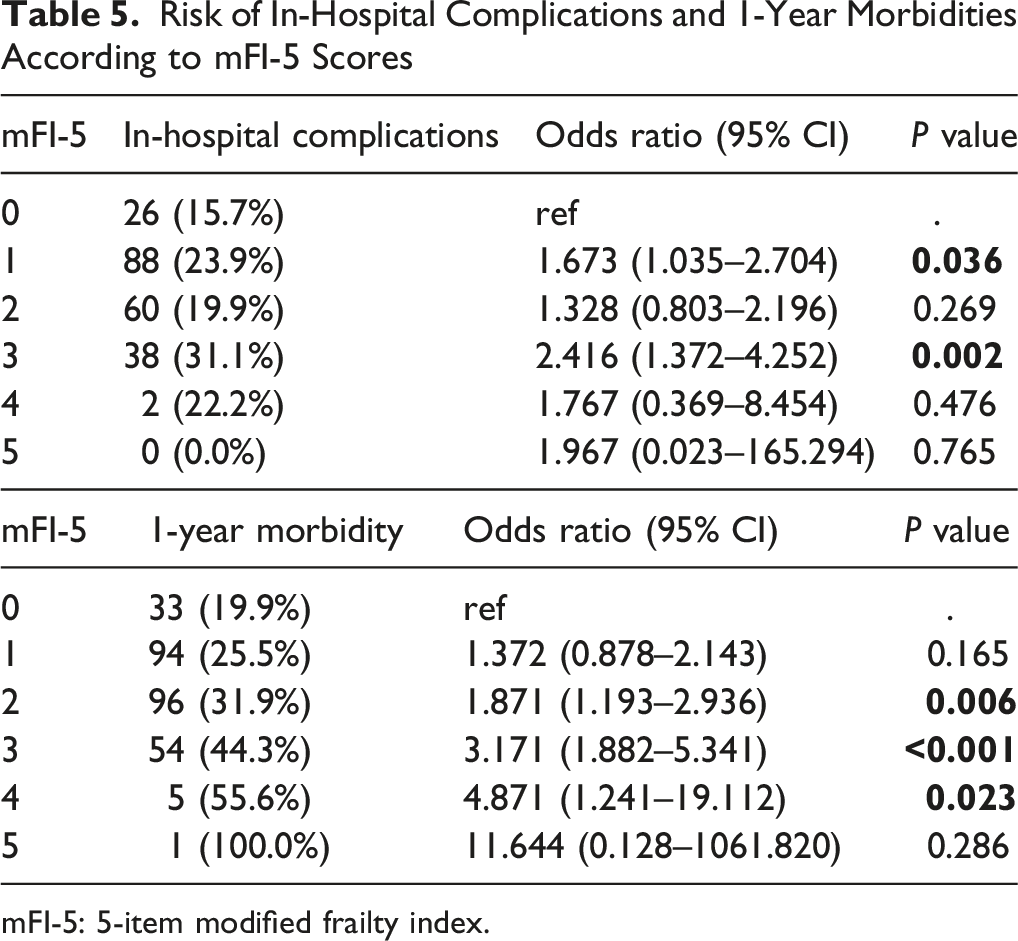
mFI-5: 5-item modified frailty index.
Discussion
Our findings indicated that geriatric patients aged ≥70 years undergoing lumbar spine surgery with an mFI-5 score of 3 or higher had increased odds of in-hospital complications. Specifically, severe frailty was associated with an approximately 1.8-fold increase in the odds of in-hospital complications compared with mFI-5 scores <3. Pre-existing functional dependence within the mFI-5 framework correlated with a 1.6-fold higher probability of negative events at one year. Especially, the most profound detriment was observed in patients who developed in-hospital complications, which amplified this risk five-fold. Contrary to expectations, the present cohort failed to establish a clear association between sarcopenia and elevated postoperative risk.
Frailty indices have been used to estimate vulnerability to adverse postoperative outcomes across surgical populations.20,21 Higher frailty burden is associated with worse postoperative outcomes. 22 Comprehensive models, such as the original 70-item Canadian Study of Health and Aging Frailty Index (CSHA-FI), offer a granular assessment of cumulative deficits. However, these exhaustive models require extensive data collection, which limits their clinical feasibility and rapid integration into routine surgical workflows.9,23,24 To address this issue, streamlined indices like the modified Frailty Index (mFI) have been widely adopted.
Subramaniam et al introduced the mFI-5, which provides an efficient and objective framework for preoperative screening. 21 The primary advantage of the mFI-5 lies in its clinical feasibility; by including only five readily available variables, it allows for rapid preoperative screening without inadvertently oversimplifying the patient’s physiological status. 8 The mFI-5 yielded comparable statistical performance and prognostic accuracy for predicting severe adverse events following instrumented spine surgery compared with th mFI-11 25 as well as in general surgery cohorts.8,26 The main advantage of the mFI-5 is its rapid integration into clinical workflows, supported by a growing body of evidence demonstrating its efficacy in preoperative risk stratification. 27 Using this streamlined metric, it has been reported that a higher frailty burden was associated with increased rates of postoperative complications, severe life-threatening complications, longer hospital stay, and adverse discharge outcomes after vertebral kyphoplasty. 28
Risk assessment in older surgical patients increasingly considers frailty alongside chronological age. Frailty, defined as the multisystem deterioration of physiological reserves, has been associated with adverse postoperative outcomes after neurological and spine surgery.29,30 While their comparative performance may fluctuate based on the specific pathology, surgical approach, and frailty assessment tool utilized, frailty indices offer clinically significant prognostic insights that extend beyond chronological age in spine surgery cohorts. 27 Indeed, relying solely on chronological age is often inadequate for robust perioperative risk stratification. 17 Given that frailty may increase susceptibility to adverse postoperative outcomes, including infection, mortality, and revision surgeries, 31 frailty assessment has become an important component for risk stratification before lumbar fusion and similar procedures.24,32–36 In the present investigation, severe frailty was defined as an mFI-5 score ≥3, and this threshold was associated with higher odds of in-hospital complications, whereas the odds of 1-year adverse events increased significantly at a score ≥2.
Furthermore, it is imperative to contrast frailty-specific indices with traditional comorbidity scoring systems, such as the Charlson Comorbidity Index (CCI). While the CCI is a well-established metric for predicting long-term mortality, it often fails to capture the immediate systemic vulnerability to surgical stress. 11 While the CCI remains a well-established metric for predicting long-term mortality based on cumulative comorbidity burden, it often fails to capture the immediate physiological vulnerability inherent in frailty.11,34 In contrast, the mFI-5 offers superior predictive utility for acute postoperative complications because it incorporates functional dependence—a critical domain that reflects an individual’s diminished physiological reserve more accurately than a simple count of chronic diseases. 35 As previously noted, the mFI-5 was inherently developed as a streamlined alternative to the 11-item modified frailty index (mFI-11). 8 Despite the reduction in the number of variables, the mFI-5 has demonstrated a strong correlation with the original 11-item index and provides comparable predictive validity across various surgical subspecialties, including spine surgery.3,16 By focusing on five readily available clinical factors, the mFI-5 enhances clinical feasibility and allows for rapid risk stratification in high-volume surgical settings without sacrificing the prognostic accuracy of more comprehensive tools or cumulative deficit models.12,37 Thus, our findings support that mFI-5 serves as a highly efficient and potent predictor of acute outcomes in geriatric patients undergoing lumbar surgery.
Sarcopenia is conceptually intertwined with frailty, a state characterized by increased vulnerability to stressors resulting from diminished physiological reserve and impaired homeostasis. 38 In older surgical patients, this systemic vulnerability may not be fully captured by chronological age alone. 6 Given the substantial perioperative morbidity and mortality associated with major spine surgery, both frailty and sarcopenia were evaluated in the present study as candidate prognostic markers.39-41 Although previous studies have demonstrated the independent predictive value of frailty for adverse postoperative outcomes, including after elective spine surgery,33,42,43 the prognostic value of sarcopenia in spine surgery remains unclear. Accordingly, our findings showed that baseline sarcopenia which was determined by the total psoas area on CT imaging at L3 and L4 was not significantly associated with the postoperative outcomes evaluated in this study.
An apparent contradiction in our data was the observation that the in-hospital complication rate peaked in the mFI-5 score 3 cohort (31.1%) rather than in the extreme frailty groups (mFI-5 scores 4 and 5). We attribute this finding to a strong preoperative selection bias and surgeon-patient shared decision-making dynamics, a well-recognized phenomenon in retrospective surgical registries.24,44 Patients presenting with exceptionally high frailty scores (mFI 4 and 5) represent an extremely high-risk demographic population. In our cohort, the sample size for these extreme populations was exceptionally small (n = 9 for mFI-5 score 4, and n = 1 for mFI-5 score 5). In clinical practice, spine surgeons are likely to manage these highly vulnerable patients conservatively, effectively excluding them from the operative cohort. When surgery is performed, it is often limited to less invasive, palliative-intent decompressive procedures with a lower baseline complication risk. Conversely, patients with an mFI-5 score of 3, while severely frail, are often deemed considerably physiologically fit to undergo standard or more extensive decompression and fusion procedures. 45 Consequently, they are exposed to a higher magnitude of surgical stress, thus probably resulting in the highest observed complication rates in our study. Therefore, outcomes in the extreme frailty tiers should be interpreted with caution due to these inherent selection biases.16,33
When evaluating the variable that exerts the highest impact on postoperative outcomes, our data revealed a critical timeline-dependent relationship. For acute in-hospital complications, severe frailty (mFI-5 score ≥3) emerged as the most robust preoperative predictor. This finding aligns with those of previous studies, demonstrating that cumulative physiological deficits rather than chronological age alone dictate immediate surgical resilience. 12 However, with respect to 1-year adverse events, the occurrence of an in-hospital complication superseded all baseline characteristics, amplifying the risk of long-term morbidity more than five-fold. Among preoperative factors, functional dependence and higher ASA-PS scores were the strongest indicators of the 1-year declines. These findings highlight a critical “cascade effect” in geriatric spine surgery: severe preoperative frailty predisposes older adults to immediate postoperative complications, which subsequently act as a profound catalyst for long-term physiological decline and adverse events. 46 Therefore, identifying and mitigating frailty prior to surgery is paramount not only to prevent immediate morbidity but to avoid this unfavorable cascade.
This study has some limitations. First, the retrospective design is inherently susceptible to selection bias and residual confounding, even with IPTW. Second, the mFI-5 is practical but may not fully capture other clinically relevant domains of frailty, including nutritional, psychosocial, and cognitive vulnerabilities. Third, sarcopenia was assessed solely by psoas morphometry and therefore did not fully reflect contemporary consensus frameworks, which define sarcopenia using measures of muscle strength and quantity or quality, with physical performance used to stage severity. Fourth, the requirement for preoperative lumbar CT may have selected a specific subgroup of patients, and the single-center design may limit the generalizability of these findings to other institutions or healthcare systems. Fifth, while we categorized the types of complications in detail, the severity of these in-hospital complications was not stratified using a formal grading system such as the Clavien-Dindo classification. Given the retrospective design, retroactively assigning severity grades could introduce misclassification bias; thus, the lack of severity weighting remains a limitation when interpreting the clinical burden of these events. To address these limitations, specific areas of future study are required. Follow-up research should aim to prospectively replicate this experiment by incorporating direct clinical measures of skeletal muscle mass and physical function (e.g., grip strength or gait speed) as comprehensive indices of sarcopenia. Moreover, while our analysis focused on outcomes up to 1 year, extended long-term follow-up studies reaching well past 1 year are needed to fully elucidate the enduring prognostic impact of sarcopenia and frailty on postoperative recovery and prognosis.
In conclusion, for geriatric patients undergoing lumbar spine surgery, severe frailty was independently associated with in-hospital complications. Furthermore, 1-year adverse events were more closely associated with functional dependence of the factors within the mFI-5, higher ASA-PS scores, and in-hospital complications. Consequently, assessing frailty, in addition to chronological age, can help predict outcomes in geriatric patients undergoing spine surgery. Conversely, our results yielded no discernible evidence linking baseline sarcopenia to an exacerbated risk of postoperative in-hospital complications or 1-year morbidity. Our findings support the clinical use of the mFI-5 for preoperative risk stratification, identifying patients with severe frailty as a high-risk group for postoperative adverse outcomes who may benefit from comprehensive preoperative functional evaluation as well as closer perioperative monitoring and management.
Supplemental Material
Supplemental Material - A High Frailty Burden is a Strong Predictor of Adverse Postoperative Outcomes in Geriatric Lumbar Spine Surgery: A Retrospective Cohort Study
Supplemental Material for A High Frailty Burden is a Strong Predictor of Adverse Postoperative Outcomes in Geriatric Lumbar Spine Surgery: A Retrospective Cohort Study by Jaein Cho, Hyun-Chang Kim, Do-Hyeong Kim, Hye Sun Lee, Hana Choe and Myoung Hwa Kim in Global Spine Journal.
Footnotes
Acknowledgements
We thank the Department of Neurosurgery at the Spine and Spinal Cord Institute, Gangnam Severance Spine Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea, for their invaluable cooperation.
Ethical Considerations
This study was approved by the Institutional Review Board of Yonsei University Gangnam Severance Hospital, Seoul, Republic of Korea (Approval No. 3-2023-0353; approval date: November 21, 2023). The requirement for informed consent was waived due to the retrospective design of the study.
Author Contributions
Jaein Cho: Concept and design, Acquisition and data, Analysis and interpretation of data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content. Hyun-Chang Kim: Concept and design, Analysis and interpretation of data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content. Do-Hyeong Kim: Concept and design, Acquisition and data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content. Hye Sun Lee: Analysis and interpretation of data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content, Statistical analysis. Hana Choe: Acquisition and data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content, Statistical analysis. Myoung Hwa Kim: Concept and design, Acquisition and data, Analysis and interpretation of data, Drafting of manuscript, Critical revision of the manuscript for important intellectual content, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated in and/or used for this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.