
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Cervical disc arthroplasty (CDA) and anterior cervical discectomy and fusion (ACDF) are both safe and effective surgical options for cervical spine pathologies such as myelopathy and radiculopathy. Comparative outcomes data for CDA versus ACDF in osteoporotic female patients remain limited despite this population’s increased vulnerability to postoperative complications. This study compares postoperative outcomes and healthcare utilization between single-level ACDF and CDA in this patient group.
Methods
Adult female patients aged ≥55 years with osteoporosis who underwent single-level CDA or ACDF between 2010 and 2022 were identified using the PearlDiver national database. A one-year washout period for prior cervical surgeries was applied, and patients receiving both procedures simultaneously were excluded. Eligible patients were matched three-to-one on age, Elixhauser Comorbidity Index (ECI), and smoking history. Outcomes included 90-day medical and surgical complications and 30-day, 90-day, and 2-year healthcare utilization metrics. Welch’s t-tests and Pearson χ2 tests were used for all comparisons. Statistical significance was set at p < .05.
Results
678 female patients with osteoporosis underwent CDA (n = 170) or ACDF (n = 508). No baseline comorbidities differed significantly between groups. Incidences of 90-day medical and surgical complications and all healthcare utilization metrics were comparable between groups.
Conclusions
Our findings suggest CDA can be performed safely in female patients with an administrative diagnosis of osteoporosis, warranting further investigation with stratified bone-density–specific analyses.
Keywords
Introduction
Osteoporosis is a progressive skeletal disorder characterized by decreased bone mass and deterioration of the bone microarchitecture, causing increased fragility and a higher risk of fractures. 1 Given the increasing prevalence of osteoporosis in the aging global population, osteoporosis represents a significant public health concern. Approximately 42% of postmenopausal women worldwide are affected by osteoporosis, with 1 in 3 women over the age of 50 projected to experience an osteoporosis-related fragility fracture at some point in their lifetime.1,2
Osteoporosis sensitizes patients to degenerative cervical pathology, such as radiculopathy or myelopathy, via heightened vertebral fracture and segmental instability secondary to compromised bone quality.3,4 To surgically address single-level anterior cervical pathology, the anterior cervical discectomy and fusion (ACDF) has been considered the gold standard procedure. 5 However, ACDF has been associated with complications such as hardware failure and adjacent segment disease due to increased mechanical load on adjacent vertebrae. 6 Moreover, fusion surgeries carry the risk of pseudarthrosis, which is especially prevalent in osteoporotic patients. 7
To mitigate fusion-related complications, cervical disc arthroplasty (CDA) has emerged as a noninferior, motion-preserving alternative to ACDF. 5 However, osteoporosis has been historically regarded as a contraindication to CDA. In contrast to fusion constructs, CDA relies on preserved vertebral endplate integrity and sufficient osseous support to maintain long-term stability and motion, features that may be compromised in osteoporotic bone. 8 Nevertheless, as implant design, surgical technique, and patient selection criteria have evolved, CDA is increasingly being performed in patients with osteoporosis, including postmenopausal women. 9 To clarify the contemporary safety and efficacy of CDA, we compared postoperative outcomes between osteoporotic postmenopausal women undergoing CDA versus ACDF.
Methods
Data Source
The PearlDiver (PearlDiver Inc., Colorado Springs, Colorado, USA) database contains deidentified and aggregated records from over 170 million patients in the United States. The database was queried using the International Classification of Diseases (ICD)-9/10th edition and Current Procedural Terminology (CPT) codes. This study was exempt from the Institutional Review Board approval process, as records are Health Insurance Portability and Accountability Act (HIPAA)-compliant and deidentified.
Study Population and Data Collection
Adult female patients aged 55 and above with a prior diagnosis of osteoporosis who underwent single-level ACDF or single-level CDA between 2010 and 2022 were identified from the PearlDiver database. Those with a recent diagnosis of metastasis, trauma, or infections to the spine within 90 days of surgery and those with database inactivity longer than 90Please note that “bold” should not allowed and therefore it was removed. Please confirm.days after surgery were excluded. Patients who received both a CDA and an ACDF at different cervical levels during the same surgical encounter were also excluded to minimize exposure misclassification. Additionally, a one-year washout period for prior cervical surgeries was applied before the index procedure date to reduce the risk of treatment contamination. Eligible patients were matched in a three-to-one ratio on age range, gender, the Elixhauser Comorbidity Index (ECI), and smoking history within two years of surgery. Baseline demographics and medical comorbidities were assessed. The primary outcomes included 90-day medical and surgical complications as well as 30-day, 90-day, and 2-year healthcare utilization metrics - measured by emergency department visits, readmissions, and cervical reoperation rates. Informed consent was not required for this study.
Statistical Analysis
Welch’s t-tests were performed to compare baseline age and ECI. Pearson χ2 tests were performed to analyze demographic comorbidities and postoperative outcomes. As no baseline comorbidities reached statistical significance following cohort matching, confounding-adjusted regression modeling was not indicated, and unadjusted chi-square analyses were used for all outcome comparisons. Multivariate logistic regression was utilized to analyze medical and surgical complications as well as healthcare utilization metrics, controlling for age, ECI, and medical comorbidities. Statistical significance was defined as p < 0.05.
Results
Summary of Baseline Demographics and Comorbidities for Matched Patients With Osteoporosis Undergoing Single-Level ACDF or Single-Level CDA
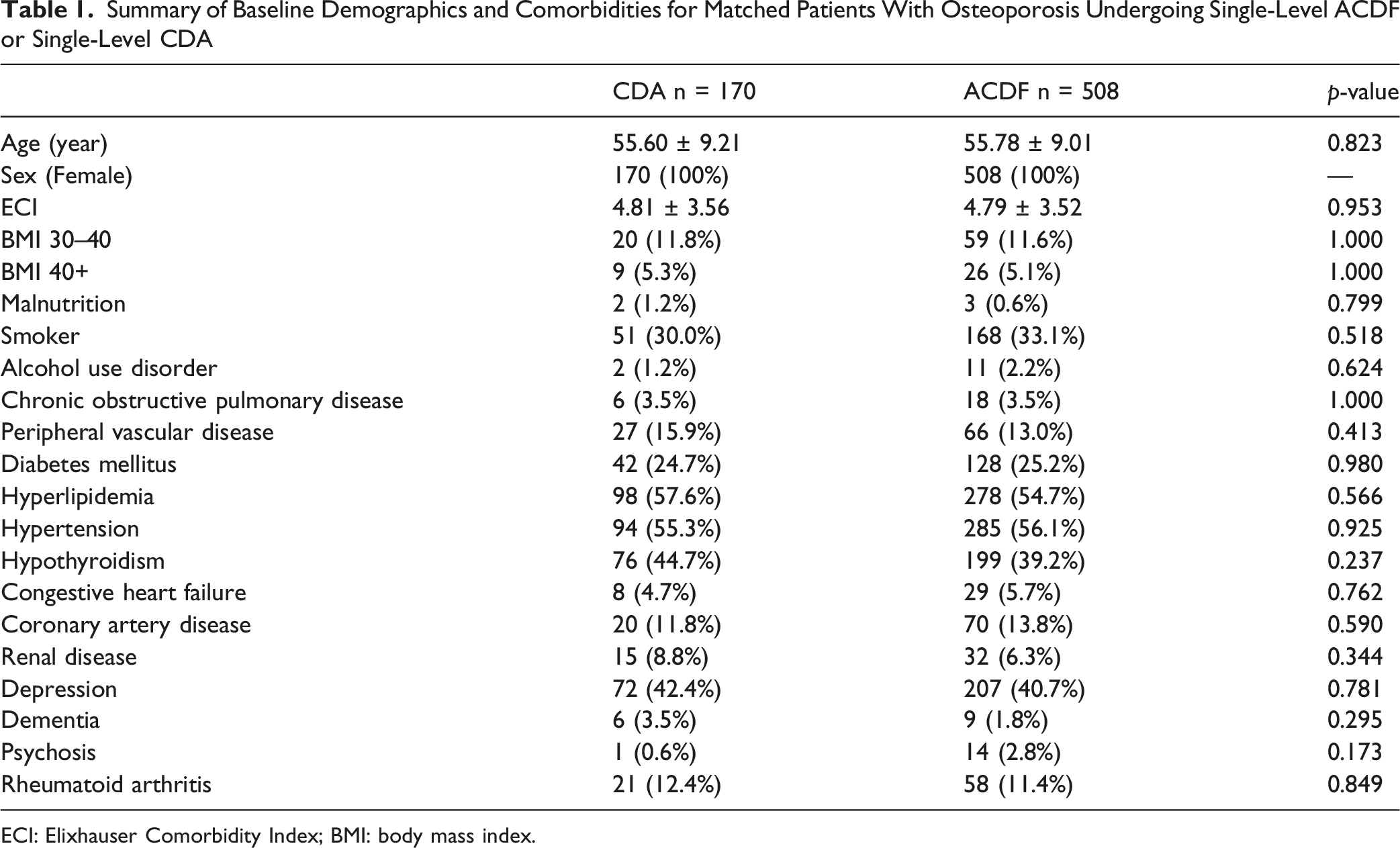
ECI: Elixhauser Comorbidity Index; BMI: body mass index.
90-Day Medical Complications for Matched Patients With Osteoporosis Undergoing Single-Level ACDF or Single-Level CDA
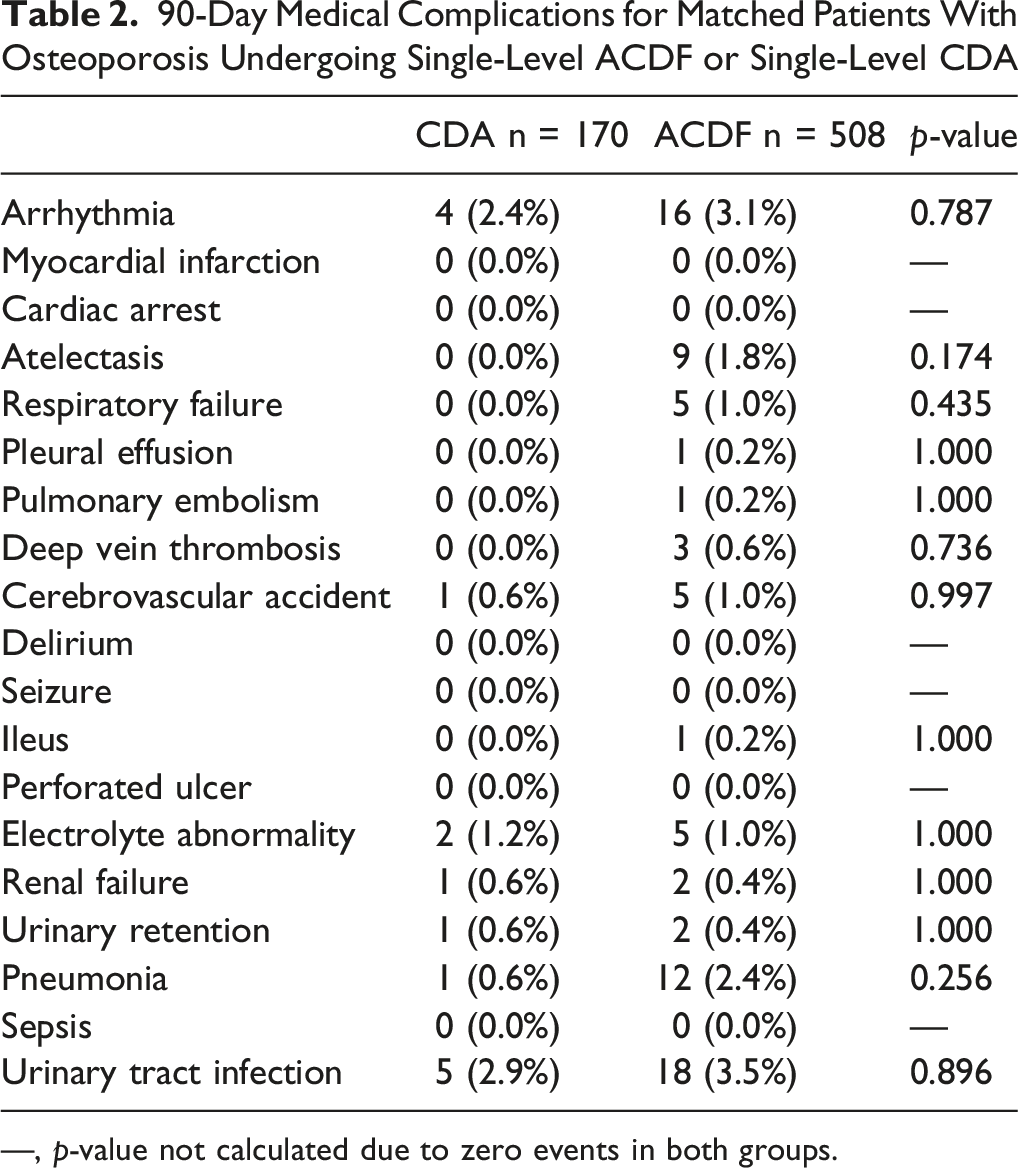
—, p-value not calculated due to zero events in both groups.
90-Day Surgical Complications for Matched Patients With Osteoporosis Undergoing Single-Level ACDF or Single-Level CDA
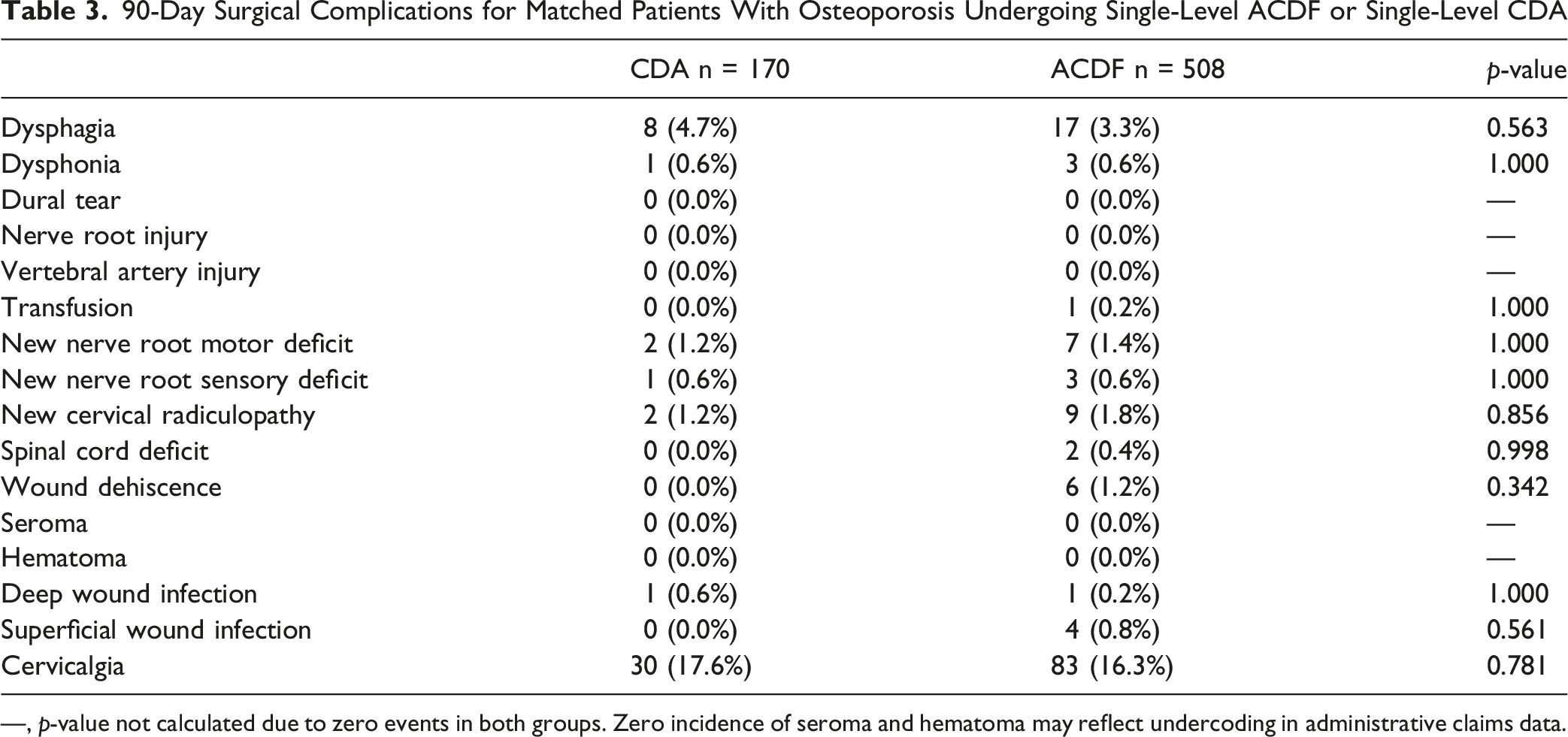
—, p-value not calculated due to zero events in both groups. Zero incidence of seroma and hematoma may reflect undercoding in administrative claims data.
Healthcare Utilization and Perioperative Complication Rates Across 30-Day, 90-Day, and 2-Year Follow-Up
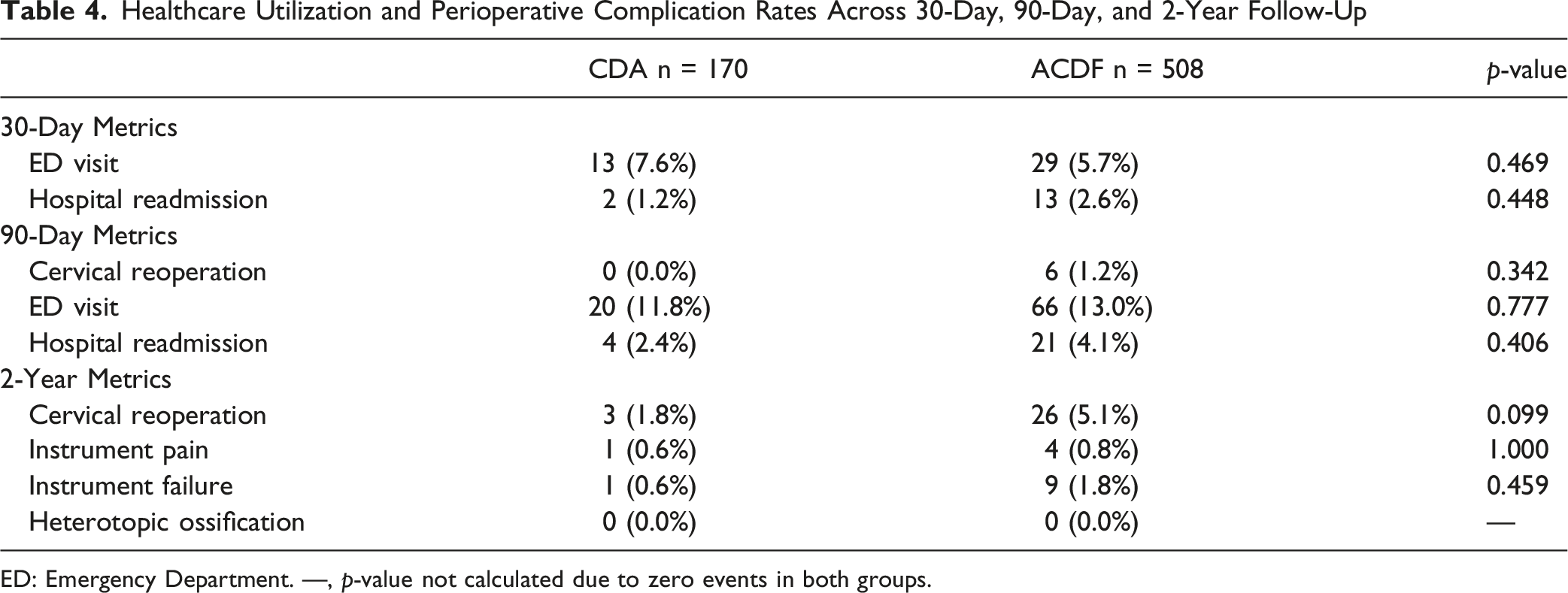
ED: Emergency Department. —, p-value not calculated due to zero events in both groups.
Discussion
Clinical Context of Osteoporosis in Cervical Spine Surgery
The intersection of cervical degenerative disease and osteoporosis creates a complex clinical scenario that challenges conventional surgical planning. While osteoporosis has historically been viewed as a contraindication to cervical disc arthroplasty (CDA) due to concerns regarding implant subsidence and long-term device stability, this assumption has not been well validated in contemporary osteoporotic populations.10–12 In this context, the present retrospective cohort study evaluated perioperative and long-term outcomes in female patients with osteoporosis undergoing single-level CDA versus ACDF using a large national claims database. After rigorous cohort matching, we observed no statistically significant differences in surgical and medical complications, short-term healthcare utilization, or reoperation-free survival rates. Accordingly, these findings challenge the traditional view of osteoporosis as an absolute contraindication to CDA and suggest that, in appropriately selected patients, CDA may offer a safety profile comparable to ACDF.
Perioperative Complications and Healthcare Utilization
In the general patient population, several prior studies have reported that ACDF and CDA produce comparable rates of short-term complications. Large-scale retrospective cohort studies have uniformly concluded that, while CDA may offer advantages in motion preservation and reduced adjacent segment disease, its perioperative risk profile is noninferior to that of ACDF.13,14 Our findings reflect a similar pattern within a female osteoporotic population: rates of complications such as arrhythmia (2.7% vs. 4.2%, p = 0.179), urinary tract infection (4.1% vs. 3.7%, p = 0.823), and dysphagia (4.9% vs. 3.2%, p = 0.180) were not significantly different between the CDA and ACDF groups. This consistency suggests that osteoporosis, specifically in single-level disease, may not substantially affect the comparative short-term complication profile of either procedure. Interestingly, healthcare utilization outcomes further support this analysis, as we found no significant differences in 30-day (6.1% vs. 5.8%, p = 0.782) and 90-day emergency department visits (11.5% vs. 13.4%, p = 0.410) or 30-day (1.7% vs. 2.4%, p = 0.465) and 90-day inpatient readmissions (3.4% vs. 4.1%, p = 0.638).
Long-Term Outcomes and Reoperation Risk
Beyond the perioperative period, long-term durability and the risk of reoperation are critical considerations when selecting a surgical strategy for patients with diminished bone quality. Randomized controlled trials conducted by Coric et al and Heller et al have demonstrated comparable safety and functional outcomes between ACDF and CDA over time; however, these studies systematically excluded patients with osteoporosis, limiting their generalizability.15,16 By focusing exclusively on osteoporotic patients, our study addresses this gap. Despite osteoporosis being a concern for nonunion or subsidence, especially in the setting of arthroplasty, we did not observe increased complication or reoperation rates. 90-day (1.4% ACDF vs. 1.0% CDA, p = 0.485) and 2-year (7.0% vs. 4.4%, p = 0.088) cervical reoperation remained infrequent, and no individual complication was disproportionately represented. Our findings support the possibility that osteoporosis alone may not uniformly increase the long-term risk of complications or reoperation following either surgical approach in carefully selected patients.
Our findings are further contextualized by a recent 2025 single-center study demonstrating that patients with osteopenia undergoing single-level CDA achieved clinical outcomes comparable to those with normal bone mineral density (BMD). 17 Although osteopenia and osteoporosis represent distinct degrees of bone loss, these data suggest that reductions in systemic BMD may not independently predispose patients to worse long-term outcomes after CDA.
Reconciling the Influence of Patient Selection and Osteoporosis Diagnosis
An important interpretive consideration is the likelihood of residual selection bias in this cohort, which warrants emphasis when drawing conclusions from these findings. One possible confounding variable is patient selection bias. In clinical practice, CDA is typically preferentially reserved for patients with favorable anatomies and milder spondylotic changes, which could result in the exclusion of patients with advanced osteoporosis. 11 Consequently, outcomes reported in broader population studies may disproportionately reflect the success of CDA in already healthier individuals, thus overstating its comparative advantages. 18 Though this cannot be confirmed with our dataset, it is a plausible explanation that aligns with known surgical decision-making practices.
Furthermore, a key consideration when interpreting our findings is the limitation of conventional bone mineral density assessment in reflecting true cervical spine bone quality. To diagnose osteoporosis, Dual-energy X-ray absorptiometry (DEXA) is typically performed at the hip and lumbar spine, providing a measure of systemic bone density. 19 Accordingly, osteoporosis diagnosis by DEXA does not capture regional bone density or endplate integrity in the cervical spine: biomechanical properties paramount to implant fixation and long-term stability in CDA.11,20,21 As a result, DEXA-defined osteoporosis may imperfectly correlate with cervical vertebral bone quality, introducing additional anatomical variance within our osteoporotic cohort. This discordance may partially explain the absence of increased complications or reoperation rates observed in CDA, as osteoporotic candidates selected for arthroplasty may retain sufficient cervical bone integrity despite reduced systemic BMD. 22 Accordingly, our findings should be interpreted as assessing outcomes among patients with administrative diagnosis of osteoporosis. More granular, single-center studies with access to radiographic data such as Vertebral Body Hounsfield Units are required to further investigate candidacy for CDA across individuals with low cervical spine bone density.23–25
Bone Health Optimization and Evolving Surgical Approaches
While our data demonstrate comparable outcomes between CDA and ACDF in osteoporotic patients, the broader literature suggests that perioperative bone health optimization may play an important role in shaping surgical outcomes in this population. Pharmacologic agents such as teriparatide have demonstrated beneficial effects on fusion biology, with multiple studies reporting improved fusion rates in patients undergoing spinal arthrodesis.26,27 Furthermore, recent single-center analyses suggest that the majority of osteoporotic patients undergoing spine surgery are already receiving pharmacologic therapy aimed at improving bone quality perioperatively. 28 We therefore hypothesize that structured bone health optimization protocols may further influence comparative outcomes between CDA and ACDF in osteoporotic patients, though this relationship could not be assessed with the present dataset. Prospective studies incorporating verified bone density assessments and perioperative treatment data are needed to clarify this question.29,30
Limitations
As a retrospective analysis using the PearlDiver administrative database, our findings are limited by potential inaccuracies in coding, missing data, lack of radiographic measures, and absence of granular clinical information such as BMD, implant type, and spinal level addressed. 31 In particular, the inability to account for specific cervical levels precludes level-specific matching between cohorts and may introduce residual confounding, as surgical level can influence complication profiles and biomechanical outcomes. Additionally, osteoporosis was defined using administrative diagnosis codes, and its duration, timing of diagnosis, and treatment response cannot be determined, as claims are limited to the observable enrollment window and do not reflect true disease chronicity or resolution (e.g. osteoporosis treated to osteoporosis), potentially resulting in misclassification of bone health status at the time of surgery or during follow-up. Claims-based analyses are also unable to capture patient-reported outcome measures such as pain severity, functional improvement, quality of life, or patient satisfaction, which are increasingly recognized as essential endpoints for assessing the effectiveness of cervical spine interventions.32,33 The relatively smaller number of CDA cases likely reflects historical exclusion of osteoporotic patients from seminal FDA trials and subsequent surgical decision-making, which may have introduced selection bias despite our cohort matching strategy. Future research using single-institution or multicenter clinical data with verified BMD measurements and radiographic validation could mitigate these limitations, provide greater clinical granularity, and validate the generalizability of our results.
Conclusion
This study found no statistically significant differences in postoperative complications, healthcare utilization, or long-term reoperation rates between ACDF and CDA among female patients with osteoporosis undergoing single-level anterior cervical surgery. While osteoporosis has historically been viewed as a contraindication to arthroplasty, our findings demonstrate comparable outcomes among osteoporotic patients undergoing either procedure. Particularly patients receiving an administrative diagnosis of osteoporosis and considered optimal surgical candidates. Future studies incorporating verified bone density assessments, radiographic parameters, and multicenter clinical outcomes are needed to refine surgical decision-making and optimize patient selection in this growing demographic.
Footnotes
Author Contributions
Kikelola Afolabi-Brown, Harshit Polavarapu, Joyce En-Hua Wang, and Nicholas Cormas contributed to the study design, data analysis, and manuscript drafting. Joshua Li conceived the study. Joyce En-Hua Wang and Nicholas Cormas generated the data, created the tables, and performed statistical analysis. Wendy Novicoff contributed to study design and statistical analysis. Joshua Li and Stephen Lockey supervised data analysis and manuscript drafting. All authors read and approved the final manuscript. Authors Kikelola Afolabi-Brown and Harshit Polavarapu had an equal contribution and should be considered co-first authors. Kikelola Afolabi-Brown and Joshua Li share corresponding authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Status
This study did not require Institutional Review Board approval.