
Abstract
Study Design
Umbrella systematic review.
Objective
To critically appraise and synthesise the existing systematic review evidence regarding incidence, risk factors, management strategies, and prognostic impact of dysphagia in patients undergoing anterior cervical spine surgery(ACSS), with interpretation explicitly weighted by methodological confidence.
Methods
A systematic search (inception-November 2025) of PubMed, Embase, Scopus, Web of Science, and the Cochrane Database identified systematic reviews and meta-analyses evaluating dysphagia after ACDF, ACCF, CDA, or multilevel ACSS. Two reviewers independently screened and extracted data. Methodological quality was appraised using AMSTAR-2. Findings were synthesised narratively at the umbrella level and interpreted proportionate to the confidence of evidence.
Results
Thirty-two systematic reviews (>3.6 million patients) were included. Dysphagia incidence ranged from 1%-79% (variations largely driven by heterogeneous definitions and timepoints). Early postoperative (≤2 weeks) dysphagia was common (up to 71%); whereas persistent dysphagia (≥12 months) was reported in 12-14% in selected analyses. Female sex, multilevel procedures, C3-C4 involvement, anterior plating, and rhBMP-2 exposure were recurrently associated with increased risk. In contrast, zero-profile implants, cuff-pressure control, and perioperative steroids were associated with reduced early dysphagia in low-confidence reviews. However, 31/32 reviews were rated critically low confidence by AMSTAR-2 grading, limiting certainty. Only one RCT-based steroid meta-analysis achieved low confidence.
Conclusion
Dysphagia is frequently reported following ACSS, particularly in the early postoperative period. No preventive or therapeutic strategy can currently be recommended as standard of care based on high-certainty evidence. Most findings remain hypothesis-generating and require validation in high-quality prospective studies.
Introduction
The anterior approach to the cervical spine was initially described by Cloward, Robinson and Smith1–3 in the 1950s. Since then, it has become a widely employed approach for central and foraminal decompressions. Since the overall morbidity rates for anterior cervical spine surgery (ACSS) are acknowledged to be relatively low, 4 surgeons have been considering the safety and efficacy of performing this approach on an outpatient basis.5–7 Given the complex vascular, neural, and aerodigestive anatomy, the anterior approach carries a diverse array of potential complications; some of which (such as vertebral artery pseudoaneurysm and oesophageal perforation) can be fatal, if not correctly identified. 3
Among the diverse complications, dysphagia remains a poorly understood and underappreciated consequence following ACSS. 8 The etiopathogenesis of this condition is still largely unclear and has been purported to be multifactorial in nature.9–11 Esophageal denervation, prevertebral soft tissue edema, nerve root injuries [such as hypoglossal nerve injury at spinal levels proximal to C3, superior laryngeal nerve (SLN) injury at C3-C4, pharyngeal plexus injury at levels C2-C5, and recurrent laryngeal nerve (RLN) injury during surgery between C5 and T1 levels]; and hematoma formation are some of the causes potentially associated with this condition.12–16 Despite being a well-recognised clinical problem, there has been no universally accepted definition or technique to identify the presence of post-surgical dysphagia.8,17 Partly attributable to the lack of a clear definition (or criteria for diagnosis), the incidence of dysphagia in the literature has been reported to vary between 1 and 79%.18–21 Some of the risk factors for the development of post-surgical dysphagia include use of plate fixation, plate design or its physical prominence, revision surgery, female sex, multilevel procedures, pain severity and use of recombinant human bone morphogenetic protein-2 (rh-BMP-2).8,22–24 Prior studies have recommended the use of peri-operative corticosteroids, endotracheal tube (ETT) cuff pressure monitoring, use of favourable or low-profile plate designs, use of anchored spacers (instead of traditional cage plate constructs); and diverse modifications to surgical techniques as preventative strategies to reduce the incidence as well as mitigate the severity of this potentially debilitating post-operative adverse event after ACSS.16,25 However, with such a significant variation in the reported incidence and prevalence of dysphagia, lack of a clear definition, and often contradictory conclusions (from a relatively large-volume, yet lower-quality evidence) regarding the risk factors and preventative measures, the need for a clearer perspective on our current understanding of this significant clinical problem cannot be understated.3,16,26,27
The current umbrella review was thus planned to comprehensively summarise the systematic reviews hitherto published on this subject, and attempt to answer the following critically important questions: a. What is the incidence or prevalence of post-operative dysphagia after ACSS? b. What are the predisposing factors (modifiable versus non-modifiable) for the development of this complication, and what is the underlying pathophysiology? c. What are the recommendations to mitigate the incidence (or prevalence) or reduce the severity of this relatively common adverse event? d. What are the management strategies, and how do they impact the overall outcome and surgical prognosis?
Methods
Study Design
This study was conducted as an umbrella systematic review synthesising evidence from published systematic reviews and meta-analyses on dysphagia following ACSS. The primary objective was to provide a comprehensive overview of the incidence, risk factors, management strategies, and prognostic impact of dysphagia in ACSS. The methodology adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 28 Although a protocol was not prospectively registered, the review question, eligibility criteria, and analytic framework were established before data extraction. To minimize post hoc decisions, eligibility criteria and analytic framework established prior to data extraction were consistently adhered at all stages of review.
Search Strategy
A systematic search was performed across PubMed, Embase, Scopus, Web of Science, and Cochrane Database of Systematic Reviews from inception to November 2025. Reference lists of included reviews were hand-searched to identify additional eligible studies. The search terms combined controlled vocabulary and keywords related to “anterior cervical spine surgery,” “ACDF,” “cervical disc arthroplasty,” “corpectomy,” “zero-profile,” “plate,” “BMP,” “steroids,” and “dysphagia.” We used the following search strategy for the PubMed database: [(“Anterior Cervical Discectomy and Fusion”[MeSH] OR “ACDF” OR “Anterior Cervical Corpectomy” OR “ACCF” OR “Cervical Disc Arthroplasty” OR “CDA” OR “Anterior Cervical Spine Surgery” OR “ACSS”) AND (“Dysphagia”[Mesh] OR “Swallowing Disorders” OR “Swallowing Difficulty” OR “Bazaz” OR “SWAL-QOL” OR “MDADI” OR “EAT-10”) AND (“Systematic Review” OR “Meta-Analysis” OR “Review”)]. A similar search strategy was used for other databases with database-specific search parameters.
Eligibility Criteria
We followed the PICOS strategy for inclusion of reviews into the analysis. The criteria were as follows: Population: Patients undergoing anterior cervical spine surgery (ACDF, ACCF, CDA, multilevel procedures); Intervention/Exposure: Surgical techniques, implant types, biologics (BMP), perioperative measures (steroids, cuff pressure control); Comparator: Alternative surgical techniques or perioperative strategies; Outcomes: Dysphagia incidence, severity, risk factors, management efficacy, and long-term prognosis; Study type: Systematic reviews, and meta-analyses. Case reports, individual primary studies of prospective and retrospective nature, along with their narrative reviews, were excluded.
Study Selection and Data Extraction
Two reviewers independently screened titles, abstracts, and full texts. Discrepancies were resolved through consensus. Data were extracted into a structured spreadsheet capturing: author, year, number of studies, sample size, study designs and surgery types, dysphagia definitions and assessment tools, incidence rates and subgroup analyses, key findings and limitations. For consistency, dysphagia incidence was categorised into three time-windows: early (≤2 weeks post-surgery), intermediate (2 weeks-3 months), and persistent (≥12 months).
Quality Assessment
The methodological quality of included systematic reviews was assessed using the AMSTAR-2 (A Measurement Tool to Assess Systematic Reviews) instrument. 29 This tool evaluates 16 critical domains, including protocol registration, comprehensiveness of the search, duplicate study selection and data extraction, justification of exclusions, risk-of-bias assessment, funding transparency, heterogeneity, and publication bias. Each domain was judged as Yes, Partial Yes, No, or Not Applicable. Based on critical flaws, overall confidence in each review was categorised as High, Moderate, Low, or Critically Low. Two reviewers independently applied AMSTAR-2, with disagreements resolved by consensus. It is important to note that AMSTAR-2 evaluates methodological rigour of systematic reviews, but does not directly assess certainty of evidence for specific outcomes (as GRADE does). Our interpretations are therefore limited to review-level confidence rather than outcome-level certainty.
Interpretation Framework and Methodological Considerations
Interpretation of findings in this umbrella review was explicitly weighted according to AMSTAR-2 confidence ratings. Reviews rated as critically low confidence were considered hypothesis-generating and were not used to support definitive clinical recommendations. Findings supported by higher methodological confidence, specifically the RCT-based meta-analysis of perioperative corticosteroid use, were given proportionately greater interpretive emphasis. Although a protocol was not prospectively registered, the review question, eligibility criteria, and analytic framework were established before data extraction. The absence of protocol registration is acknowledged as a limitation.
Given the umbrella design, overlap of primary studies across included systematic reviews was anticipated. However, formal quantification of overlap (e.g., corrected covered area) was not feasible because most reviews did not provide complete lists of included primary studies. This limitation may inflate the denominator of reported patient entries and lead to overrepresentation of certain large registry studies, thereby biasing pooled incidence and effect estimates. We therefore interpret these figures cautiously as approximate patient entries rather than unique individuals.
Data Synthesis
Given the umbrella review design and substantial heterogeneity in definitions, outcome measures, and overlapping primary studies, quantitative aggregation was not appropriate. We therefore employed a narrative synthesis to preserve methodological transparency. Where available, pooled incidence and risk ratios were extracted. Subgroup analyses were summarised by surgical technique, implant type, biologic use, and perioperative interventions.
Results
Study Selection and Characteristics
The systematic search identified 425 records. After screening, 32 systematic reviews and meta-analyses published between 2010 and 2025 were included, as shown in Figure 1. The characteristics of the reviews included in the study are given in Table 1. These reviews encompassed diverse study designs: randomised controlled trials (RCTs), prospective and retrospective cohort studies, and extensive database analyses, with sample sizes ranging from a small case-series of 31 patients to registry-based studies involving more than 3.6 million individuals. Due to the overlap of primary studies, this figure should be interpreted as approximate aggregated entries rather than unique individuals. While the reviewed surgical procedures included anterior cervical discectomy and fusion (ACDF), anterior cervical corpectomy and fusion (ACCF), cervical disc arthroplasty (CDA), and multilevel procedures, diverse implant systems such as zero-profile constructs (or other anchored spacers), cage-plate systems, and stand-alone cages were compared. PRISMA flow diagram of inclusion of studies Characteristics of Reviews Included in the Study ACCF: Anterior Cervical Corpectomy and Fusion; ACDF: Anterior Cervical Discectomy and Fusion; ACSS: Anterior Cervical Spine Surgery; ADR/CDA/CDR: Artificial Disc Replacement/Cervical Disc Arthroplasty/Cervical Disc Replacement; BMP/rhBMP‑2: Bone Morphogenetic Protein/Recombinant Human Bone Morphogenetic Protein‑2; BSS: Bazaz Dysphagia Score; COI: Conflict of Interest; CR/CS: Case Report/Case Series; DBS: Database Study; EAT‑10: Eating Assessment Tool‑10; FOSS: Functional Outcome Swallowing Scale; MDADI: MD Anderson Dysphagia Inventory; MDSS: Modified Dysphagia Symptom Score; NRS: Numeric Rating Scale; PCS: Prospective Cohort Study; PROM: Patient‑Reported Outcome Measure; PSTS/PSTSI: Prevertebral Soft Tissue Swelling/Prevertebral Soft Tissue Swelling Index; RCS: Retrospective Cohort Study; RCT: Randomized Controlled Trial; RoB: Risk of Bias; SWAL‑QOL: Swallowing Quality of Life Questionnaire; VAS: Visual Analog Scale.
Methodological Quality of Included Reviews
Methodological Quality of the Included Reviews Based on AMSTAR-2 Grading (Confidence Ratings: High, Moderate, Low, or Critically Low)
AMSTAR‑2: A Measurement Tool to Assess Systematic Reviews, version 2; COI: Conflict of Interest; MA: Meta‑analysis; N/A: Not Applicable; PICO: Population, Intervention, Comparator, Outcome; RoB: Risk of Bias.
Incidence of Dysphagia
Dysphagia was reported as the most frequent complication following ACSS, though the incidence varied widely. Dysphagia incidence ranged from 1%-79%, reflecting highly heterogeneous definitions, timepoints, and assessment tools across anterior cervical spine surgery (ACSS) procedures. When applying standardised time-windows, early dysphagia (≤2 weeks) was reported in up to 71% of patients, while persistent dysphagia (≥12 months) was reported in 12-14%. These figures should be interpreted cautiously, given definitional heterogeneity and potential inflation of denominators due to unquantified overlap of primary studies across reviews.3,16,26,27 The variability in incidence was primarily attributable to differences in definitions and assessment tools [ranging from patient-reported symptoms to validated instruments such as the Bazaz Dysphagia Score (BDS), Swallowing Quality-of-Life (SWAL-QOL), Dysphagia Disability Index (DDI), Dysphagia Numerical rating Scale, MD Anderson Dysphagia Inventory (MDADI), Functional Outcome Swallowing Scale (FOSS), and Eating Assessment Tool (EAT-10)].8,22–24,31 In addition, radiographic indices like prevertebral soft tissue swelling (PSTS) and prevertebral soft tissue index (PSTSI), as well as video-fluoroscopic evaluations, were also employed. 16 Rates were most frequently reported for ACDF, but broader ACSS procedures (ACCF, CDA, multilevel constructs) demonstrated similar heterogeneity. Distinguishing ACDF-only data from broader ACSS findings is important.
Risk Factors for Dysphagia
Risk factor analyses identified both patient-related and surgical determinants.8,16,22–24,31 Female sex was associated with a higher risk [with odds ratios (OR)˷2.3]. While multilevel procedures were associated with a 2-fold greater risk of dysphagia (as compared with single-level surgeries), involvement of the C3-C4 level carried a particularly enhanced risk (OR>3.0).23–25,31 Prolonged operative time was also associated with increased dysphagia risk. Based on our analysis, implant design may be associated with differences in dysphagia rates: while anterior cage-plate constructs (CPC) were associated with higher dysphagia rates (OR = 1.66), use of zero-profile (or anchored spacer) constructs may be associated with reduced risk.32–37 Biologic use, especially recombinant human bone morphogenetic protein-2 (rhBMP-2), was associated with increased dysphagia risk [relative risk (RR): 1.43 and OR: 5.52].38–40 Peri-operative factors such as high endotracheal cuff pressure and excessive changes in cervical alignment (C2–C7 lordosis>9°) were also implicated in the occurrence of dysphagia.3,8,22–25 These associations were primarily reported in observational meta-analyses and registry data, and therefore must be interpreted with caution compared to the limited RCT-based evidence. Further, these associations should be interpreted cautiously, as they are derived predominantly from critically low-confidence reviews and may reflect confounding rather than causal relationships.
Management (Preventive) Strategies
Among several preventive and therapeutic measures that were evaluated, perioperative corticosteroids were the most consistently studied intervention.30,41–48 Both intravenous and local administrations were associated with reduced early postoperative dysphagia incidence and severity, particularly in multilevel ACDF. Local depo-medrol® (methyl-prednisolone acetate injectable suspension) administration was associated with reduced dysphagia in patients exposed to rhBMP-2; while retropharyngeal steroid application was associated with reduced PSTSI and improved Bazaz scores at 2 weeks without increasing complications. Steroid use was associated with reduced early dysphagia and shorter hospital stay in one RCT-based meta-analysis (low confidence). Findings from other reviews were critically low in confidence and therefore remain hypothesis-generating. However, this represents the only RCT-based meta-analysis available, and its findings carry greater evidentiary weight than observational syntheses.
Implant design modifications may also be associated with differences in dysphagia rates. Zero-profile constructs were associated with lower dysphagia rates compared with cage-plate systems. Still, these observations arise from critically low-confidence reviews and should be interpreted as hypothesis-generating signals [relative risk (RR) ranging between 0.19 and 0.76 across different timepoints].32–37 Anchored spacers were associated with lower dysphagia rates and operative time. Still, these findings are derived from critically low-confidence reviews and should be interpreted as preliminary, hypothesis-generating signals rather than definitive recommendations. On a similar note, stand-alone cages were associated with lower dysphagia incidence (than cage-plate constructs), with OR: 0.32 during the early postoperative period and 0.27 beyond 3 months. Cervical disc arthroplasty (CDA) was associated with potentially lower dysphagia rates compared with ACDF (9.5% vs 12.1%), possibly attributable to limited oesophageal retraction and avoidance of anterior plating (inherent to fusion procedure).9,49,50
Prognostic Impact and Outcomes
Although dysphagia was common, most cases were transient. Persistent dysphagia (beyond 12 months) affected 12 to 14% patients, impairing the quality of life (QoL) and functional recovery.3,8,16,22–24,26,27,42 Severe dysphagia correlated with prolonged hospital stays, higher readmission rates, and reduced patient satisfaction. Despite its frequency, dysphagia seldom influenced fusion rates or long-term surgical outcomes; however, chronic cases exerted a meaningful negative influence over postoperative recovery trajectories.
Discussion
Structured Umbrella-Level Synthesis of Evidence on Dysphagia After Anterior Cervical Spine Surgery, Stratified by AMSTAR-2 Confidence Rating and Evidence Type (Observational vs. RCT-Based), Distinguishing Hypothesis-Generating From More Reliable Findings
Note. All findings are weighted by AMSTAR‑2 confidence. Critically low confidence findings are hypothesis‑generating only and should not be interpreted as practice‑changing recommendations.
Definition and Measurement Heterogeneity as a Driver of Incidence Variability
It is important to distinguish that most incidence estimates arise from observational reviews and registry data, whereas the few RCT-based syntheses provide more reliable but narrower insights. The wide range in the reported dysphagia incidence across the literature may be attributed to definitional and measurement heterogeneity, rather than true epidemiological divergence. For structured synthesis, dysphagia time windows were categorised as early (≤2 weeks), intermediate (2 weeks-3 months) and persistent (≥12 months). However, many included reviews did not standardise the time points, and primary studies frequently used inconsistent follow-up intervals.
Additionally, diagnoses varied considerably, including clinician-reported symptoms, retrospective registry coding and validated patient-reported outcome measures such as the Bazaz score, EAT-10, SWAL-QOL, MDADI, and FOSS. Reviews incorporating structured PROMs generally reported higher dysphagia detection rates compared with those relying on unstructured chart documentation. This heterogeneity in definitions and assessment methods substantially limits comparability across reviews and contributes to imprecision in pooled incidence estimates.
Risk Factors
Yee et al 3 observed that the occurrence of dysphagia was a predictor of a longer hospital stay and multiple readmissions. Among the different risk factors considered, they observed that use of BMP, multi-level (≥3) ACDF, female sex, and revision surgery were associated with higher dysphagia. These risk factors are supported predominantly by low-quality observational evidence. In contrast, RCT-based analyses remain scarce, underscoring the need for higher-quality trials.
Cho et al 16 demonstrated that prevertebral soft tissue swelling (secondary to haemorrhage, iatrogenic peri-oesophagal trauma), cervical plate prominence, impingement secondary to fibrosis, adhesions or osteophytes, and prolonged oesophagal retraction (causing high intraluminal pressures, ischemia-reperfusion injury) could be associated with the etiopathogenesis of dysphagia. They demonstrated that female sex, older age, severe neck pain, multilevel/revision surgeries, longer operative time, prominent cervical plate, and rhBMP-2 use were significant risk factors. In the meta-analysis by Liu et al, 23 female sex (P < 0.001), use of anterior cervical plate (P < 0.001), multi-level (≥2 levels) surgery (P < 0.001), upper surgical level at C3-C4 (P = 0.004) and rhBMP-2 (P < 0.001) were correlated with dysphagia.
Biologic use
Among the biologics, BMP has been most commonly correlated with increased dysphagia. In the meta-analysis by Martin et al, 40 While rhBMP-2 was associated with improved arthrodesis, dysphagia and anterior soft tissue complications were enhanced. In another review, 25 based on data from 4 studies (level II-IV evidence),10,51–53 BMP was correlated with significantly enhanced risk of dysphagia. Shriver et al 26 demonstrated statistically insignificant difference in dysphagia rate between autograft and allograft implantation during ACDF.
Prominence of cervical plates
Zeng et al 54 observed a higher dysphagia rate with a prominent plate profile (thickness>1.4 mm). Similarly, Lee et al 55 demonstrated a lower incidence of early and persistent dysphagia with plates carrying a smoother and smaller profile. On the other hand, studies by Liu et al, 24 Jain et al 56 and Chin et al 11 reported an unclear correlation between the profile prominence of the plate and dysphagia.
Multilevel surgery
Generally, multi-level surgeries have been correlated with higher dysphagia rates. The meta-analysis by Oh et al 27 showed statistically higher dysphagia rate for multilevel ACDF (6.6% versus 4% at 12-24 months follow-up). However, studies have not demonstrated any significant difference in dysphagia between ACCF and ACDF surgeries in multilevel pathologies.3,31,41
Screw migration
Although usually self-limiting, dysphagia can be associated with serious pathologies. Carr et al 57 described dysphagia and pharyngoesophageal injury rates of 52% and 61%, respectively, following screw migration. A proportion of these patients required implant removal and surgical oesophageal or hypopharyngeal repair.
Yee et al 3 reported an incidence of oesophageal injury in 0.46% (pooled incidence: 0.2%). Such patients presented with dysphagia, odynophagia, sepsis, wound drainage, implant failure and neurological deficits. The timing of recognition of injury ranged from intraoperative to delayed discovery at 20 years, and mortality ranged between 0 and 33%.
Preventive Measures
Jaoquim et al 25 evaluated the role of diverse pre- and intra-operative preventive measures [such as tracheal traction exercises (TTE), avoidance of prolonged operative time, avoidance of BMP, considering CDA in appropriate situations, using modified retractors, control of tracheal cuff pressures, modifying dissection planes, use of plates with smaller profile, use of anchored spacers, and local steroid use] to mitigate dysphagia. They concluded that although evidence regarding these preventive measures was limited, these interventions did not appear to increase complications; however, their incorporation into routine surgical practice should be considered cautiously, pending validation in higher-quality prospective studies.
Anchored cages
In the study by Shao et al, 34 the zero-profile cage (ZPC) was associated with a lower dysphagia rate at 2 weeks (P = 0.0002), 6 months (P = 0.008), and 1 year (P = 0.001), as compared with the cage-plate construct (CPC). On a similar note, studies by Yin 33 , Gabr, 32 Xiao et al, 35 Yang et al 36 and Cheung 37 also reported lower dysphagia rates with stand-alone anchored spacers compared with CPC at different postoperative time points.
Cervical disc arthroplasty (CDA)
There have been contrasting reports regarding the association between CDA and dysphagia. While Anderson et al9,49 did not observe any significant correlation; Yang et al 36 and Zhong et al. 50 reported statistically significant associations with reduced dysphagia rates (P = 0.022 and 0.01, respectively) after CDA.
Corticosteroid use
Among the diverse preventive measures, the impact of corticosteroid administration (systemically or locally) on dysphagia has remained the most widely assessed. In the meta-analysis by Liu,23,24,42 perioperative intravenous (dexamethasone/methylprednisolone) and local steroid use were associated with reduced incidence and severity of early dysphagia (especially for multilevel surgeries). In the meta-analysis by Adenikinju, 47 patients receiving systemic and local steroids had better reductions in the severity of postoperative dysphagia (with no added risk of infections or pseudoarthrosis). In a meta-analysis of RCTs (Zhang et al 30 ), steroids administered locally or systemically were associated with reduced dysphagia (within 1 year), VAS (2 weeks) and length of hospital stay.
A majority of other reviews have focused on the effectiveness of local steroid application. Yu et al 41 demonstrated that perioperative retropharyngeal steroid administration mitigated the severity of postoperative dysphagia (P < 0.0001), ameliorated PSTSI (P < 0.0001), and improved VAS score (P < 0.001). In patients undergoing revision surgery or those requiring BMP application for pseudoarthrosis, locally-administered depomedrol on collagen sponge was shown to reduce dysphagia. On a similar note, reviews by Song et al, 43 Cheng et al, 44 and Shen et al 46 also reported the beneficial effect of local steroid application (in different formulations and dosages) in mitigating dysphagia-related complications. Among these, only perioperative corticosteroid use has been evaluated in an RCT-based meta-analysis, which provides relatively stronger evidence compared to the critically low-confidence observational reviews.
Endotracheal cuff pressure
The evidence regarding the role of endotracheal tube cuff pressure (ETTCP) and preoperative TTE is still largely unclear. Yee et al 3 observed that by limiting or monitoring endotracheal tube cuff pressure (ETTCP) to 15 mmHg, there was no change in dysphagia rates. In contrast, they observed that preoperative TTE significantly mitigated dysphagia (especially after multilevel ACDF). On the other hand, the meta-analysis by Cho et al 16 also did not demonstrate any significant benefit of ETTCP control or reduction in postoperative dysphagia incidence.
Quality of Evidence and Limitations
A significant finding of this umbrella review is the uniformly low methodological quality of existing systematic reviews. Overall, 31/32 reviews were rated as critically low on AMSTAR-2. The key recurring flaws included: a. lack of protocol registration, b. inadequate search strategies, c. absence of duplicate screening and extraction, d. inconsistent risk-of-bias assessment, e. failure to report excluded studies, f. inability to address publication bias. These flaws undermine confidence in pooled incidence estimates and effect sizes. Additionally, heterogeneity in dysphagia definitions, outcome time points, and assessment tools makes the comparison across studies challenging. Since most reviews synthesised retrospective data, under-reporting of dysphagia is likely, particularly in chronic cases or in registries lacking validated PROMs. Although the review question, eligibility criteria, and analytic framework were established before data extraction, the absence of formal registration of the study protocol may introduce bias by allowing post-hoc methodological decisions, particularly in study selection and synthesis. This limitation is acknowledged and underscores the need for protocol registration in future umbrella reviews.
How AMSTAR Ratings Informed Interpretation
Interpretation of the Evidence From the Structured Umbrella-Level Synthesis, Highlighting AMSTAR-2 Confidence Ratings, Distinctions Between Observational and RCT-Based Evidence, and Areas of Clinical Uncertainty
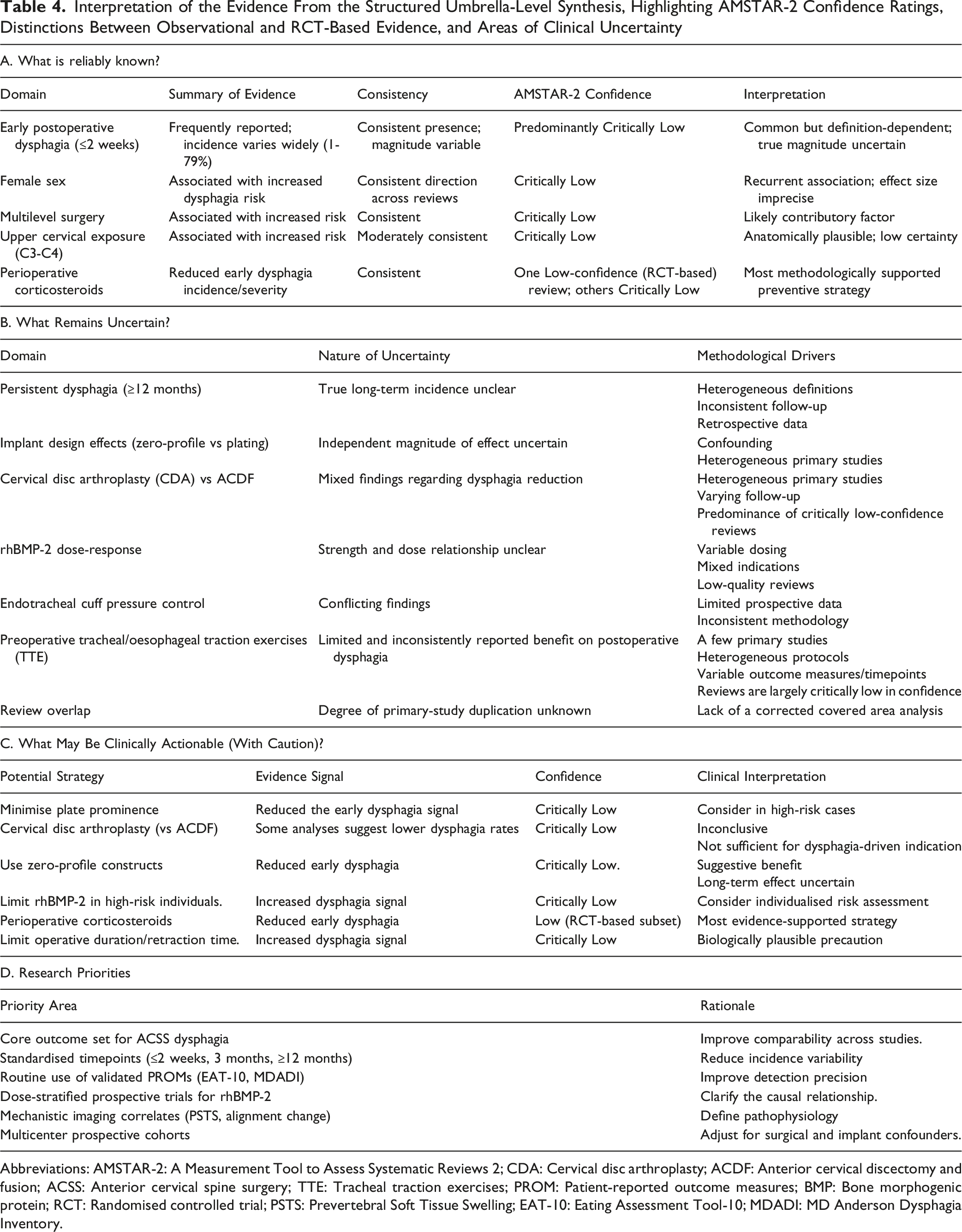
Abbreviations: AMSTAR-2: A Measurement Tool to Assess Systematic Reviews 2; CDA: Cervical disc arthroplasty; ACDF: Anterior cervical discectomy and fusion; ACSS: Anterior cervical spine surgery; TTE: Tracheal traction exercises; PROM: Patient-reported outcome measures; BMP: Bone morphogenic protein; RCT: Randomised controlled trial; PSTS: Prevertebral Soft Tissue Swelling; EAT-10: Eating Assessment Tool-10; MDADI: MD Anderson Dysphagia Inventory.
Evidence Certainty Statement
The overall certainty of evidence regarding dysphagia after ACSS is low. The predominance of critically low-confidence systematic reviews substantially limits confidence in pooled incidence estimates and effect size interpretations. Most identified associations, particularly those relating to implant design, rhBMP-2 exposure, and perioperative techniques, should therefore be interpreted as hypothesis-generating signals rather than definitive causal relationships.
Perioperative corticosteroid administration represents the most methodologically supported intervention, based on the only review synthesising RCTs; however, even this evidence is limited by heterogeneity in dosing, administration route, and follow-up duration. Accordingly, clinical decisions should be individualised, evidence-informed, and tempered by recognition of the current methodological constraints within the reviewed literature.
Future Research Directions
High-quality, prospective, standardised research is urgently needed. Priority areas include: a. Uniform definitions and validated assessment tools, including routine use of Bazaz scores, EAT-10, MDADI, and standardised radiographic markers, b. Prospective multicenter cohort studies: enabling robust adjustment for confounders and stratification by surgical approach, implant type, alignment correction, and intraoperative variables. Dose-response data for rhBMP-2 and optimised steroid protocols, d. Mechanistic imaging studies investigating PSTS, soft tissue oedema, cervical alignment shifts and pharyngeal biomechanics, etc. Development of individualised risk-prediction models, f. Long-term functional outcomes, including swallowing-related QoL, nutritional status, and health-care utilisation. These priorities are essential to move beyond hypothesis-generating signals toward reliable, practice-informing evidence.
Conclusion
Dysphagia is commonly reported after ACSS, particularly in the early postoperative period. However, the reported incidence substantially varies due to inconsistent definitions, assessment tools, and follow-up intervals. Female sex and multilevel surgery demonstrated association with increased risk, while perioperative corticosteroid administration represents the most methodologically supported strategy for reducing early dysphagia. However, no preventive or therapeutic strategy can currently be recommended as standard of care based on high-certainty evidence. Most findings remain hypothesis-generating and require validation in high-quality prospective studies. Future progress depends on standardised outcome definitions, validated patient-reported measures, and high-quality prospective multicenter studies capable of clarifying modifiable risk factors and preventive strategies.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data generated in the study will be made available upon reasonable request to the authors.