
Abstract
Study Design
Retrospective Cohort Study.
Objective
To investigate whether patients with hip osteoarthritis (OA) who underwent sacroiliac joint (SI) fusion were at increased risk of subsequent total hip arthroplasty (THA) compared to matched controls.
Methods
This retrospective cohort study utilized the PearlDiver Mariner Database, a nationwide insurance claims dataset encompassing approximately 157 million patients. Patients with hip OA who underwent SI joint fusion were identified and propensity-matched 1:1 to controls with hip OA alone based on age, sex, and Elixhauser Comorbidity Index. A landmark analysis was employed to mitigate immortal time bias, with patients undergoing THA within two years of hip OA diagnosis excluded. Patients undergoing lumbar fusion surgery during this time period were also excluded. Univariable and multivariable logistic regression and Kaplan-Meier survival analyses were performed to assess the likelihood of subsequent THA.
Results
Following propensity matching, 4,383 patients per cohort were analyzed. SI fusion was independently associated with a significantly higher likelihood of subsequent THA on both univariable and multivariable analysis (OR: 2.18 [95% CI 1.60–2.96]; P < 0.001). THA-free survival at 10 years was 94.7% in the SI fusion group versus 96.8% in controls (p =0.007).
Conclusion
Patients with hip OA who underwent SI fusion demonstrated a significantly higher likelihood of requiring subsequent THA, suggesting that SI fusion may accelerate hip OA progression through adjacent segment biomechanical changes. These findings have important implications for preoperative counseling in patients with concomitant hip OA and SI dysfunction.
Introduction
Total hip arthroplasty (THA) is among the most frequently performed elective orthopaedic procedures, with projected utilization continuing to rise substantially in the United States over the coming decades. 1 As procedural volumes increase, there is growing interest in identifying risk factors that may accelerate hip degeneration and contribute to earlier need for arthroplasty. Sacroiliac joint (SI) dysfunction is a significant contributor to chronic low back pain, accounting for approximately 15–30% of cases, and represents a substantial source of disability and healthcare utilization. 2 When nonoperative treatments fail, SI fusion has emerged as an effective surgical option, demonstrating improvements in pain, function, and quality of life. 3 However, by eliminating motion at the SI joint, fusion alters the normal biomechanics of the lumbopelvic complex and redistributes mechanical loads to adjacent structures. This redistribution of forces is consistent with the well-described phenomenon of adjacent segment disease following spinal fusion, in which immobilization of one segment leads to increased stress and degeneration in neighboring joints. 4 Because the hip joint is anatomically and functionally linked to the spine and pelvis, it may be particularly susceptible to these biomechanical changes.
Prior studies have demonstrated that spinal fusion can decrease pelvic mobility and alter spinopelvic alignment, thereby influencing hip joint kinematics and loading patterns. 5 Biomechanical investigations provide further insight into this relationship. Finite element analyses have shown that lumbosacral fusion with sacroiliac fixation increases both angular motion and contact stress at the hip joint, with the greatest effects observed in constructs extending to the pelvis. 6 Similarly, gait-based modeling studies have demonstrated that SI fusion alters hip joint loading throughout the stance phase, with increases in contact stress during high-load phases such as foot-flat and heel-off. 2 Although these increases are relatively small in magnitude, the hip joint experiences millions of loading cycles annually, suggesting that even modest changes may have clinically meaningful long-term effects. 2
Clinical evidence also supports a potential association between fusion procedures and hip degeneration. Increased rates of hip joint-space narrowing have been observed following spinal fusion, particularly with longer fusion constructs, indicating a dose-dependent relationship between fusion extent and hip degeneration. 5 Furthermore, sacroiliac joint fixation itself has been implicated as a potential independent risk factor for the progression of hip osteoarthritis, leading to the proposed concept of “adjacent segment disease of the hip”. 7 Additional studies have suggested that extensive spinal fusion may increase the likelihood of subsequent THA, further highlighting the clinical importance of understanding this relationship. 5
Despite growing recognition of the hip–spine relationship, the specific impact of SI joint fusion on the risk of subsequent THA remains poorly understood. Conversely, a mechanistically distinct question arises: in patients who already carry a diagnosis of hip osteoarthritis, does SI joint fusion, performed for SI joint dysfunction, increase the risk of disease progression severe enough to require THA? The answer has potential implications for surgical decision-making and patient counseling. Improved ambulatory mechanics, pain reduction, and normalization of gait following SI joint fusion could theoretically alter the mechanical environment of the hip favorably, potentially slowing articular cartilage degeneration. Alternatively, changes in pelvic kinematics and load redistribution following SI joint fusion could increase hip joint contact forces, conceivably accelerating osteoarthritic progression.
To date, there is a paucity of large-scale study studies directly examining the relationship between SI joint fusion and the risk of subsequent THA in patients with pre-existing hip osteoarthritis. The present study sought to address this gap by leveraging a large nationwide insurance claims database to evaluate whether patients with hip osteoarthritis who underwent SI joint fusion had a higher or lower likelihood of subsequently requiring THA compared to matched controls with hip osteoarthritis alone.
Methods
Data Source and Study Population
This retrospective cohort study utilized the PearlDiver Mariner Database (PearlDiver Technologies, Colorado Springs, CO, USA), a large, national insurance claims dataset containing de-identified information on approximately 157 million patients across all payer types. The database includes demographic, diagnostic, and procedural information from inpatient and outpatient encounters between 2010 and 2022. As this study used anonymized data, institutional review board approval and informed consent were not required.
Study Endpoints
The primary aim of this study was to evaluate whether patients with hip osteoarthritis who underwent SI joint fusion for SI joint dysfunction were at increased risk of subsequent total hip arthroplasty compared to propensity-matched patients with hip osteoarthritis who did not undergo SI joint fusion over the study period.
Identification of Study Cohorts
Patients were identified using International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 and ICD-10), along with Current Procedural Terminology (CPT) codes. The complete list of diagnostic codes used for cohort identification is provided in Supplemental table 1.
Cohorts were limited to adults aged 18 years or older. Patients were excluded if they underwent total hip arthroplasty for trauma, malignancy, or infection during the study period.
Statistical Analysis
Statistical analyses were performed using RStudio (version 4.4.2) within the PearlDiver Mariner platform. Continuous variables were compared using Student’s t-test, and categorical variables were analyzed using Pearson’s chi-squared test. To control for confounding variables, the control cohort of patients with hip osteoarthritis but no SI joint fusion was propensity-matched to the SI joint fusion cohort at a 1:1 ratio based on age, sex, and ECI.
To evaluate the association between SI joint fusion and the likelihood of subsequent total hip arthroplasty, a univariate and multivariate logistic regression model adjusted for age, sex and ECI was used. Kaplan-Meier survival analysis was performed to assess THA-free survival. A p-value < 0.05 was considered statistically significant for all analyses.
Due to limitations of the integrated bellwether statistical software within PearlDiver, a time-dependent cox regression beginning at OA diagnosis could not be completed. To address time-dependent exposure and reduce immortal time bias, we instead performed a 2-year landmark analysis using the date of initial hip osteoarthritis diagnosis as time zero. Patients who underwent total hip arthroplasty or lumbar fusion within 2 years of diagnosis were excluded. Among patients who remained THA-free at 2 years, the exposed group consisted of those who underwent sacroiliac joint fusion during the 2-year landmark window, and the control group consisted of patients not receiving SI joint fusion during the window. Follow-up for risk of hip arthroplasty and Kaplan-Meier analysis began at 2 years.
Results
Baseline Demographic Characteristics of Propensity-Matched Patients With Hip Osteoarthritis With vs Without Sacroiliac Joint Fusion
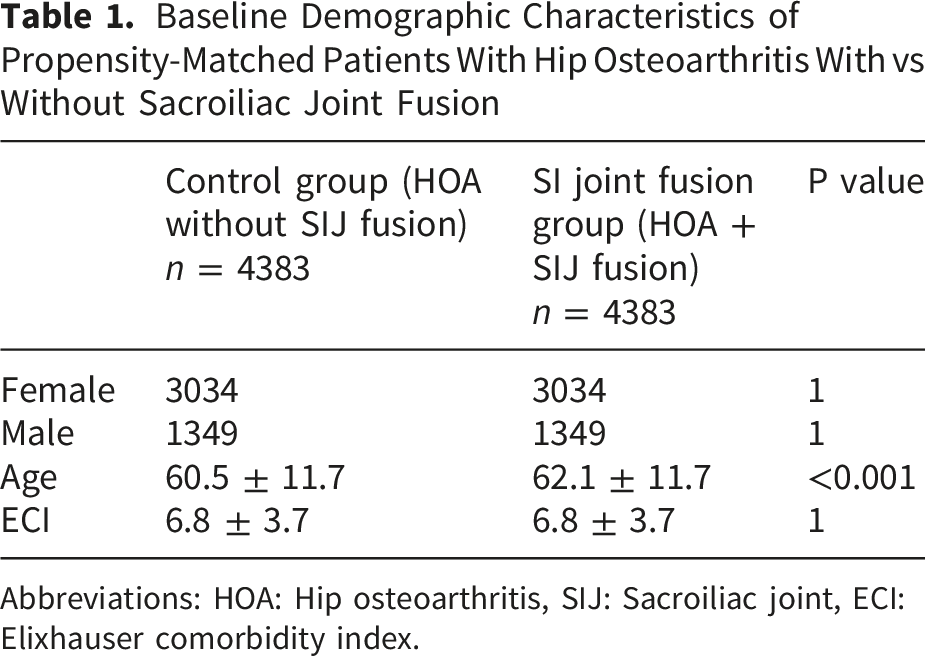
Abbreviations: HOA: Hip osteoarthritis, SIJ: Sacroiliac joint, ECI: Elixhauser comorbidity index.
Comparison of SI Joint Fusion vs Control Cohort
Odds of Subsequent THA in Patients With Hip Osteoarthritis Undergoing Sacroiliac Joint Fusion
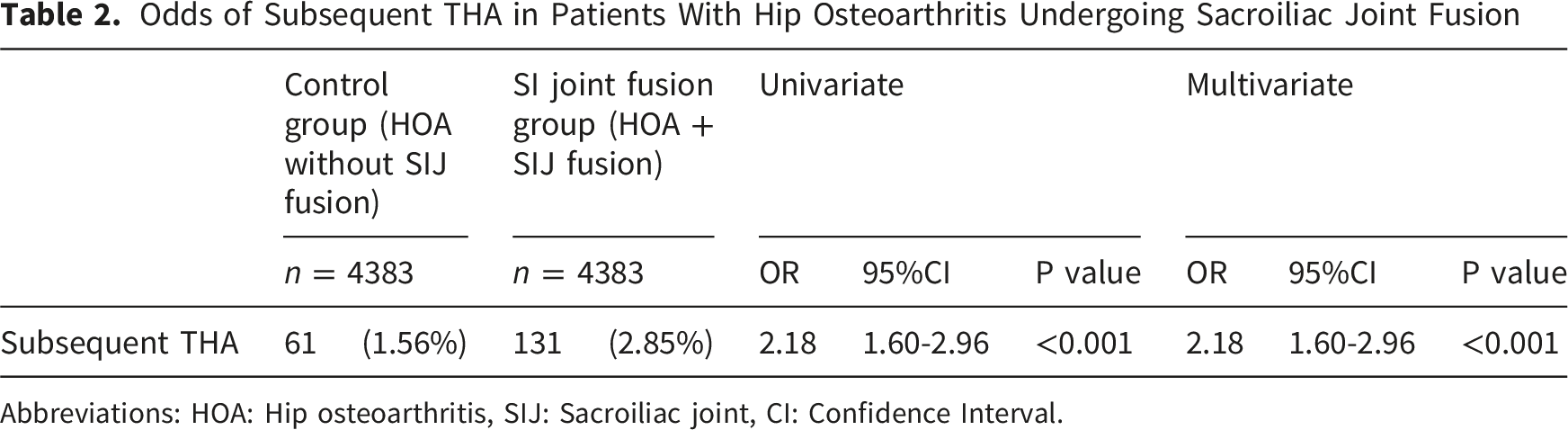
Abbreviations: HOA: Hip osteoarthritis, SIJ: Sacroiliac joint, CI: Confidence Interval.
Survival Analysis
Kaplan-Meier analysis demonstrated significant overlap between two cohorts. THA-free survival at 5 years was 97.9% (95% CI 97.4 – 98.5%) for the SIF cohort and 98.3% (95% CI 97.8% - 98.8%) in the control group. At 10 years, THA free survival was 94.7% (95% CI 93.7 – 95.8%) in the SIF group and 96.8% (95% CI 95.9% - 97.7%) in the control group. Log-rank testing showed no significant difference between groups (χ2 = 7.2, df = 1, p = 0.007).
Discussion
The primary finding of this large, propensity-matched nationwide cohort study is that patients with hip osteoarthritis who underwent SI joint fusion were significantly more likely to require subsequent THA compared to matched controls with hip osteoarthritis who did not undergo SI joint fusion (OR: 2.18 [1.60-2.96]; P < 0.001). This finding persisted on both univariate and multivariate analyses, suggesting a robust association between SI joint fusion and the likelihood of progressing to THA. These results suggest that SI joint fusion may accelerate hip degeneration. Kaplan-Meier survival analysis also demonstrated a statistically significant difference in THA-free survival between groups (Figure 1). Kaplan Meier survival curve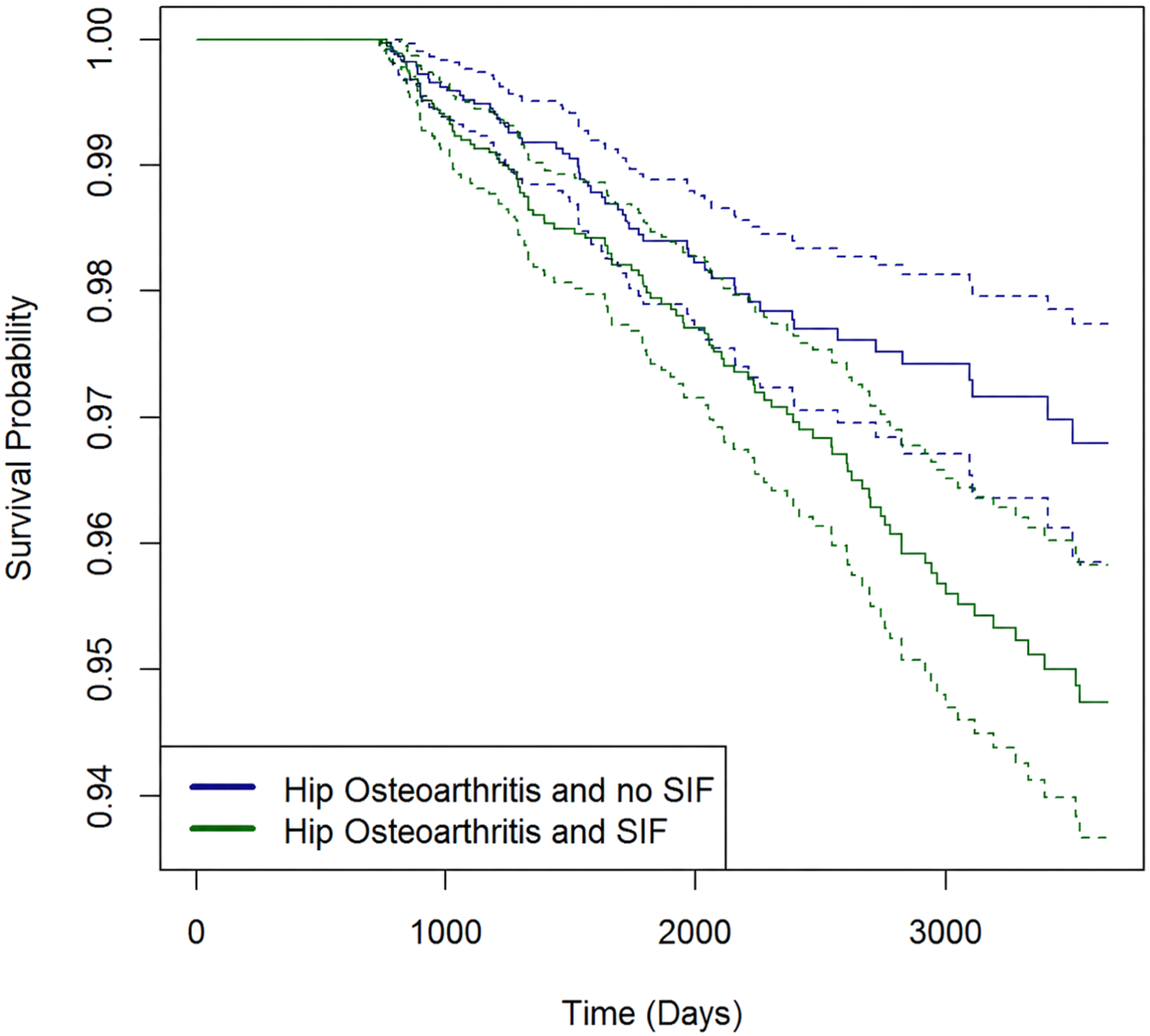
The relationship between SI joint surgery and hip pathology has been explored from several angles in the existing literature, though prior studies have largely focused on different populations or different directionalities of the hip-spine-SI joint relationship. Kozaki et al. conducted a retrospective cohort study of 118 patients who underwent adult spinal deformity surgery and found that sacroiliac joint fixation was the only variable independently associated with radiographic progression of hip OA on joint space width analysis (OR: 7.1; p = 0.0065). 7 The same group subsequently constructed a finite element model comparing four fusion configurations from L4 to the femoral bone and found that the S2F model, incorporating L4-S2 alar iliac screw fixation; produced the highest average and maximum hip joint contact stress of all configurations, leading to the conclusion that lumbosacral fusion including sacroiliac joint fixation places added stress on the hip joint. 8
It is essential to distinguish these findings from the clinical scenario studied in the present investigation. In both Kozaki studies, sacroiliac joint fixation was performed as part of long-segment adult spinal deformity surgery, in which the SI joint fixation serves as the distal anchor of a rigid multi-segment construct that eliminates both lumbar and pelvic mobility. In isolated SI joint fusion for SI joint dysfunction; as studied here; lumbar spinal mobility is preserved and fixation is limited to a single pathological joint. The kinematic consequences at the hip are therefore expected to differ substantially between these two surgical contexts.
An important related finding was reported by Ramamurti et al., who identified 197 patients with a history of isolated SI joint arthrodesis who subsequently underwent elective primary THA for osteoarthritis, and compared them to propensity-matched controls without prior arthrodesis using a national administrative database. They found a significantly higher incidence of THA dislocation in the SI joint arthrodesis group (OR: 2.06; 95% CI 1.04–4.04; p = 0.037). 9 This finding demonstrates that isolated SI joint fusion does alter spinopelvic mechanics in ways that are clinically detectable at the hip.
The reverse direction of this relationship has also been examined. Asada et al. performed preoperative CT scans of 31 female hip replacement candidates with hip OA and compared them to 34 age-matched controls, finding a significantly higher incidence of SI joint space narrowing and vacuum phenomena in the hip OA group. 10 The authors proposed that restriction of hip motion in advanced OA increases shear stress at the SI joint, drawing an analogy to the established relationship between hip arthrodesis and SI joint degeneration. This bidirectional relationship further highlights the mechanical interdependence of the hip and SI joint and provides context for interpreting why addressing SI joint dysfunction may, in turn, influence the mechanical environment of the hip. Haselhuhn et al. further inform the epidemiology of this relationship, reporting a low prevalence of preexisting THA (0.95%) among 105 SIJ fusion patients at a single academic institution, consistent with the estimated prevalence in the total US population. In their cohort, two SIJ fusion patients (1.9%) received subsequent THA at 8 and 16 months following SI fusion on the ipsilateral side. Both patients had hip OA diagnoses prior to SIJ fusion. 11
The finding that SI joint fusion was associated with a higher risk of subsequent THA warrants careful biomechanical interpretation. Kiapour et al. described the SI joint as transferring large bending moments and compressive loads to the lower extremities, while resisting shear through the tight wedging of the sacrum between the hip bones and the surrounding ligamentous structures. 12 When the SI joint is dysfunctional; whether due to hypermobility, instability, or aberrant mechanics; this load distribution is disrupted, with potential consequences for gait mechanics and force transmission throughout the lumbopelvic-hip kinetic chain.
Direct evidence for gait dysfunction in SI joint dysfunction patients comes from Mar et al., who evaluated 13 unilateral SI joint dysfunction patients using three-dimensional joint kinematics and kinetic ground reaction force analyses before and 6 months after unilateral SI joint fusion, comparing them to matched asymptomatic controls. 13 Preoperatively, patients exhibited significant deficits including elevated step width, reduced hip flexion/extension on the symptomatic side, and elevated pelvic obliquity and rotation. After SI joint fusion, significant improvements were observed, including normalization of step width between sides and improved hip flexion/extension range of motion, with overall function approaching levels comparable to matched asymptomatic controls, although elevated pelvic obliquity and rotation remained. 13 It is important to note that this was a small study of 13 patients and did not directly measure hip joint loading or cartilage stress, so a direct mechanical link to hip OA progression cannot be established from this study alone.
The clinical significance of hip loading in the context of OA progression was established by Tateuchi et al., who conducted a prospective cohort study of 50 patients with secondary hip OA and demonstrated that higher daily cumulative hip moment at baseline was independently associated with subsequent radiographic progression of hip OA; defined as joint space width reduction greater than 0.5 mm/year; over a 12-month follow-up period. 14 This finding establishes a mechanistic link between gait-related hip loading and articular degeneration. Taken together with the gait data from Mar et al., it is plausible; though not directly proven by either study; that the abnormal gait mechanics observed preoperatively in SI joint dysfunction patients may contribute to elevated hip loading, and that the gait improvements following fusion may unmask subclinical hip osteoarthritis, as patient regains ability to walk distance sufficient enough to produce hip symptoms, a phenomenon seen in adjacent segment disease. However, this remains a hypothesis that requires direct biomechanical investigation to confirm.
Kumaran et al. used a finite element model derived from CT scans of a healthy 55-year-old male to simulate unilateral and bilateral SI joint fusion using three triangular titanium alloy implants, applying pelvis and hip joint kinematics across key phases of the stance phase of the gait cycle; foot contact, foot flat, heel off, and toe off. 15 Their results demonstrated that hip joint contact stresses varied with both fusion configuration and gait phase. Unilateral right fusion reduced joint reaction forces by 2% but increased contact stress by 3.7%, while bilateral fusion increased joint reaction forces by 6.7% and contact stress by 3.25%, with the highest stresses occurring during the foot flat and heel off phases. 15 The study further found that with unilateral fusion, the hip contralateral to the fusion construct experienced larger joint reaction forces across all gait phases, whereas bilateral fusion produced the largest contact area and the highest maximum and average cartilage contact stresses across nearly all gait phases. 15 The authors attributed these findings to bilateral fusion increasing the rigidity of the sacropelvic complex to a greater degree than unilateral configurations, thereby reducing the joint’s capacity to dissipate forces and transferring greater load to the hip. 15 They concluded that these phase-specific loading alterations may necessitate fusion-specific rehabilitation protocols and warrant further investigation of long-term hip joint health outcomes. 15 Notably, the model was constructed from a single healthy male subject without SI joint dysfunction, and the authors themselves acknowledged that their findings should be interpreted as mechanical insights to guide future research rather than direct predictors of clinical outcomes. The modest magnitude of changes observed; 3–7% for most measures; must also be considered in the context of the approximately 1–2 million loading cycles the hip joint undergoes annually during walking alone, as highlighted by the authors. 15
Strengths and Limitations
This study benefits from the use of the PearlDiver Mariner database, a large nationwide claims dataset encompassing approximately 157 million patients across all payer types, providing sufficient sample size and statistical power to detect meaningful differences. The 1:1 propensity matching based on age, sex, and Elixhauser Comorbidity Index ensured well-balanced comparison groups, and the absence of significant between-group differences in baseline covariates following matching supports the validity of the comparison.
Several important limitations must be acknowledged. As a claims-based database study, our findings lack imaging data and granular patient data, precluding direct assessment of radiographic disease severity, functional status, or the specific indication, approach, or laterality of SI joint fusion, THA, or sidedness of hip osteoarthritis. Therefore our study is able to identify risk and trends, but lacks the ability to conclude a specific biomechanical mechanism or investigate ipsilateral vs contralateral SIJ-hip relationships. We cannot exclude the possibility that patients who underwent SI joint fusion had more severe hip OA at baseline, or that their clinical trajectory was influenced by factors not captured in claims data such as body mass index, physical activity level, leg length discrepancy, or the presence of inflammatory arthropathy. Our use of THA as a proxy for hip OA progression is an imperfect surrogate; patients may progress radiographically without reaching the threshold for surgery. Additionally, the biomechanical mechanisms proposed in this discussion are largely inferential, synthesizing findings from gait analysis, finite element modeling, and epidemiological data that were not designed to be analyzed in combination, and therefore require direct prospective validation.
Some additional confounding may be present relating to disease severity or socioeconomic status. Individuals willing to undergo SI joint fusion may be more comfortable with surgery, wealthier, or have better insurance, leading to greater rates of THA. Income and insurance status were not evaluated. Additionally, while a landmark analysis reduces immortal time bias, excluding patients operated during the first 2 years following osteoarthritis may selectively exclude the highest risk patients with accelerated hip disease, limiting the generalizability to hip OA patients who remain THA-free after 2 years.
Future studies incorporating radiographic outcomes, validated gait analysis, direct measurement of hip joint loading, and longer follow-up periods are needed to confirm these findings and elucidate the underlying mechanisms. Biomechanical simulation studies specifically modeled on patients with SI joint dysfunction; rather than healthy subjects; would more appropriately characterize the hip loading changes following SI joint fusion in this population.
Conclusion
In this large propensity-matched cohort study, patients with at least 2 years of non-operated hip osteoarthritis who underwent SI joint fusion for SI joint dysfunction were significantly more likely to require subsequent THA compared to matched controls who did not receive SI fusion. (OR: 2.18 [1.60-2.96]; P < 0.001). However, the absolute difference in THA-free survival at 10 years was modest: 94.7% in the SI fusion group versus 96.8% in controls, representing an absolute risk increase of approximately 2.1 percentage points. The observed association may reflect an adjacent segment phenomenon following modifications in gait mechanics and pelvic kinematics following SI joint fusion, though the precise biomechanical mechanisms remain to be directly established. This context is important for clinical communication; while a statistically robust relative association exists, the vast majority of patients with concomitant hip osteoarthritis and SI joint dysfunction who undergo SI fusion will not require THA solely as a consequence of that fusion over a 10-year horizon. These findings should not discourage SI joint fusion in appropriately selected patients, but do support incorporating the potential for accelerated hip OA progression into preoperative counseling. urther prospective research is needed to confirm these findings and determine whether surgical or rehabilitation strategies can mitigate the observed risk.
Supplemental Material
Supplemental material - Risk of Total Hip Arthroplasty after Sacroiliac Joint Fusion Surgery: A Nationwide Study
Supplemental material for Risk of Total Hip Arthroplasty after Sacroiliac Joint Fusion Surgery: A Nationwide Study by Ali Issani, Aidan Lindgren, Nathaneal Heckmann, Raymond J. Hah, Ram Kian Alluri, Jay R. Liebermann, Jeffrey Wang in Global Spine Journal
Footnotes
Consent to Participate
Informed consent and institutional review board approval were not required as this review did not include patient information.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ali Issani and Aidan Lindgren have nothing to disclose. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes, and stock options from Bone Biologics, Electrocore, PearlDiver, and Surgitech. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees and stock options from HIA Technologies, and payment from Eccential Robotics for lectures and presentations. Nathaneal Heckmann has received royalties from Corin USA, consulting fees from Intellijoint Surgical, Microport Orthopedics and Corin U.S.A Zimmer and stock options from Intellijoint Surgical. Jay R. Lieberman has received royalties from DePuy: A Johnson & Johnson company and Saunders/Mosby-Elsevier, consulting fees from DePuy: A Johnson & Johnson Company and stock options from BD Surgiphor and Hip innovations technologies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.