
Abstract
Study Design
Experimental ex vivo biomechanical cadaver study.
Objectives
Thoracic pedicle screws are essential for stabilizing spinal injuries, but misplacement remains a frequent complication. While many studies focus on neurovascular injuries, the impact of the degree of lateral misplacement (offset) on the biomechanical stability of thoracic pedicle screws has not been examined. Therefore, this study aimed to evaluate the influence of lateral offset on pullout force (POF) and peak insertion torque (PIT), and to analyse additional factors such as screw diameter, screw length, and bone quality.
Methods
In this ex vivo cadaveric study, 61 thoracic vertebrae (T1–T12) from seven human cadavers were instrumented using pedicle screws placed with predefined lateral offsets via 3D-printed templates. Each vertebra received one optimal and one offset screw for pairwise comparison. Biomechanical testing included cyclic loading followed by axial pullout testing. Linear mixed-effects models assessed the influence of offset, screw diameter, screw length, and bone density on POF and PIT.
Results
Lateral offset significantly reduced POF and PIT. Each millimeter of offset decreased POF by 41.1 N (−9.2%; p<0.001) and PIT by 0.079 Nm (−5.9%; p=0.002). Larger screw diameter significantly increased both POF and PIT (p=0.020; p<0.001). Screw length and bone quality showed no significant independent effects. POF and PIT were strongly correlated (r=0.637, p<0.001).
Conclusions
Lateral offset significantly reduced both pullout force and peak insertion torque of thoracic pedicle screws, demonstrating a progressive loss of biomechanical stability with increasing misplacement. These findings underline the biomechanical relevance of accurate thoracic pedicle screw placement.
Background Context
Dorsal fixation with pedicle screws (PS) is a frequently used procedure for stabilizing unstable spinal injuries.1-3 Due to the small diameter of the pedicles, there is an increased risk of PS malposition and pedicle cortical breaches in the thoracic spine. 4 There are various classification systems for quantifying these malpositions. The most commonly used classification, according to Gertzbein and Robbins, defines screw perforations ≥2 mm as misplaced. 5
In the upper thoracic spine, malpositions with a breach of ≥2 mm are described in up to 36.1% of fluoroscopy-assisted PS implantations. 6 A meta-analysis by Perdomo-Pantoja et al reports misplacements in 0.8%–12.1% of PS throughout the thoracic spine, depending on the insertion technique, and identifies publication bias, suggesting that these misplacement rates are likely underestimated. The same meta-analysis further indicates that the use of 3D navigation and robot-assisted pedicle screw insertion can improve the accuracy of PS placement. 7
Complications of these misplaced PS can include injury to neurovascular structures,3,8 although such injuries are rare. 9 At the same time, however, the position of the PS also affects biomechanical stability.
Screw loosening and the resulting failure of internal fixation are major complications, particularly in elderly patients with osteoporotic bone.10,11 In addition to bone quality, pedicle breach has also been shown to be a risk factor for PS loosening in a retrospective analysis. 12
While most studies and classification systems on screw malposition generally focus on injury to neurovascular structures, the influence of varying degrees of screw perforation and pedicle breach on the biomechanical stability of thoracic PS has not been extensively investigated.
So far, 3D-printed templates for positioning PS have primarily been used to achieve optimal screw placement.13-15 When applied to the application of controlled perforation, new challenges arise for the templates, as a deviation of the screws includes transcortical trajectories through solid cortical bone. Accordingly, in addition to drill guidance, rigid screw guidance is required to achieve precise control of PS position in breaching trajectories.
In this study, exact screw misplacement in the thoracic spine was planned using CT imaging and CAD planning. Subsequently, rigid guidance for drilling and screw insertion was implemented using a new methodology with 3D-printed templates specific to the vertebral body and the planned offset.
Objectives
The primary objective of this study is to investigate the influence of the degree of lateral offset of pedicle screws in the thoracic spine on the biomechanical stability. Therefore, this study hypothesized that a higher degree of lateral offset reduces the biomechanical stability of thoracic pedicle screws.
Secondary objectives are to evaluate the influence of screw diameter, screw length, and bone quality on the biomechanical stability of the pedicle screw and to determine what information the peak torque applied during pedicle screw insertion can provide regarding the biomechanical stability.
Methods
This study is an experimental ex vivo biomechanical cadaver study. The study was approved by the ethics committee of the responsible state medical association (application number 2024-17723). All procedures were conducted in accordance with the ethical standards of the institutional and national research committees, as well as the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards.
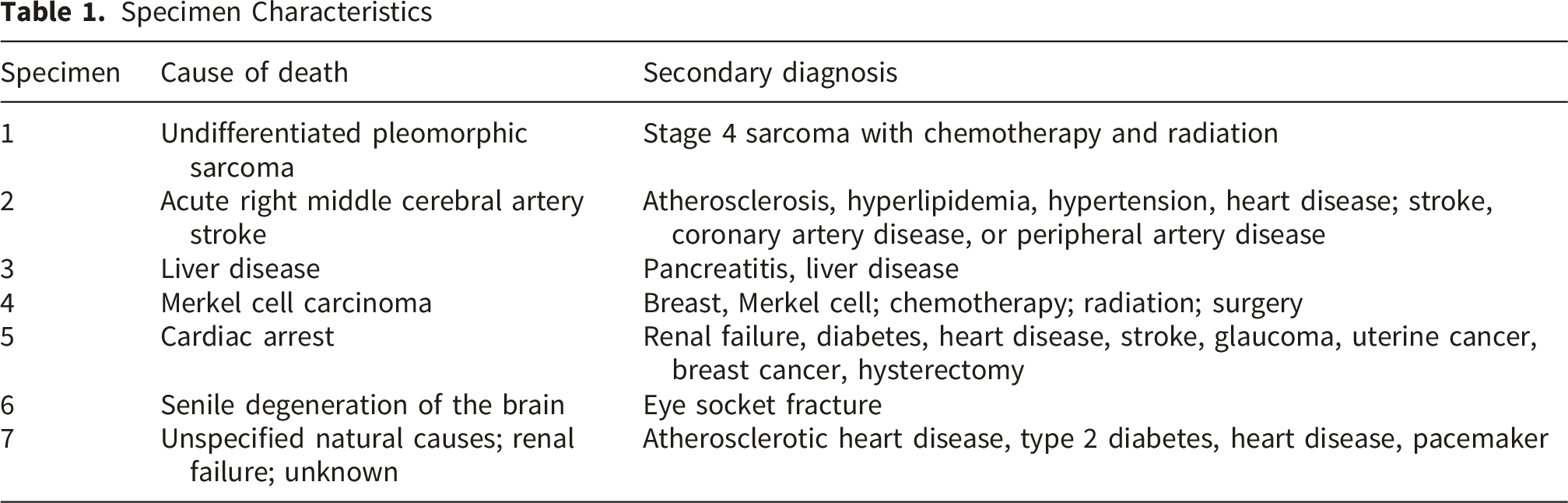
Specimen
A total of seven cadaveric specimens were used in this study. The thoracic spine from T1 to T7 was obtained from four specimens, and the thoracic spine from T1 to T12 from three specimens. In total, 64 human vertebral bodies were prepared. The bone density of each vertebral body was determined by analysing the Hounsfield units (HU) on CT scans, following the methodology of Lee et al. 16 HU measurements were obtained from the trabecular bone of the vertebral body using three axial slices, while avoiding cortical bone. The mean value of these three measurements was used for further analysis. The specimens were fresh-frozen and stored at -20°C between the experimental steps. Before PS implantation and biomechanical testing, the specimens were thawed for 24 hours.
The thoracic vertebral bodies were initially dissected free from the spine. During this process, the ribs were transected at 10 cm from the vertebral body. Subsequently, the vertebral bodies were carefully cleared of surrounding soft tissue, except for the region around the costovertebral joints, where the soft tissues were preserved to protect the ligamentous structures. Each vertebral body was then embedded in a standardized 3D-printed mold using polyurethane (PU) resin (GP 010, Gößl+Pfaff, Karlskron, Germany). The vertebral bodies were embedded so that approximately 50% of their height was enclosed within the resin, with the superior and inferior endplates aligned parallel to the outer edges of the mold. After embedding, CT imaging (slice thickness: 0.5 mm; Aquilion Lightning, Canon Medical Systems, Ōtawara, Japan) of the embedded vertebral bodies was acquired.
Pedicle Screw Planning
First, the vertebrae in the CT datasets were segmented and then exported as stereolithography (STL) files using 3DSlicer. 17 Subsequent CAD post-processing was performed in Fusion 360 (Autodesk, San Francisco, California, USA).
Based on the CT data, the placement of the PS and the systematic offset trajectory were planned. For this purpose, both PS were first planned in a correct intrapedicular position (a + b; Figure 1). The PS convergence was planned along the axis of the pedicles. The craniocaudal angle was selected to position the screw tip centrally within the vertebral body. Schematic illustration of offset planning. (A) Optimal intrapedicular trajectory; (B) Optimal intrapedicular trajectory; (C) Offset trajectory (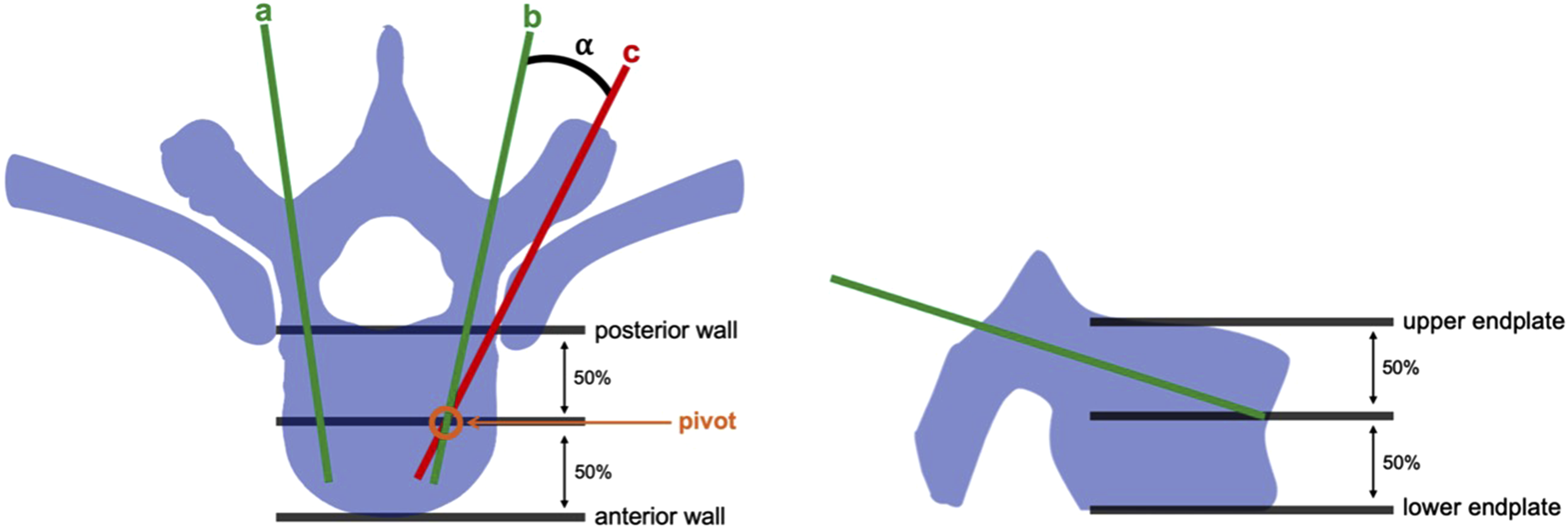
To achieve the maximum diameter of the PS, a cylinder with the largest possible diameter was positioned along the planned trajectory within the vertebral body. A screw diameter-to-pedicle width ratio greater than 0.8 was targeted.
Subsequently, the trajectory was rotated around the constructed pivot (Figure 1) in the axial plane until a fully extrapedicular position at the isthmus of the pedicle was achieved. The required angle CAD-based planning of screw trajectories. Green indicates the optimal trajectory, and red indicates an offset trajectory (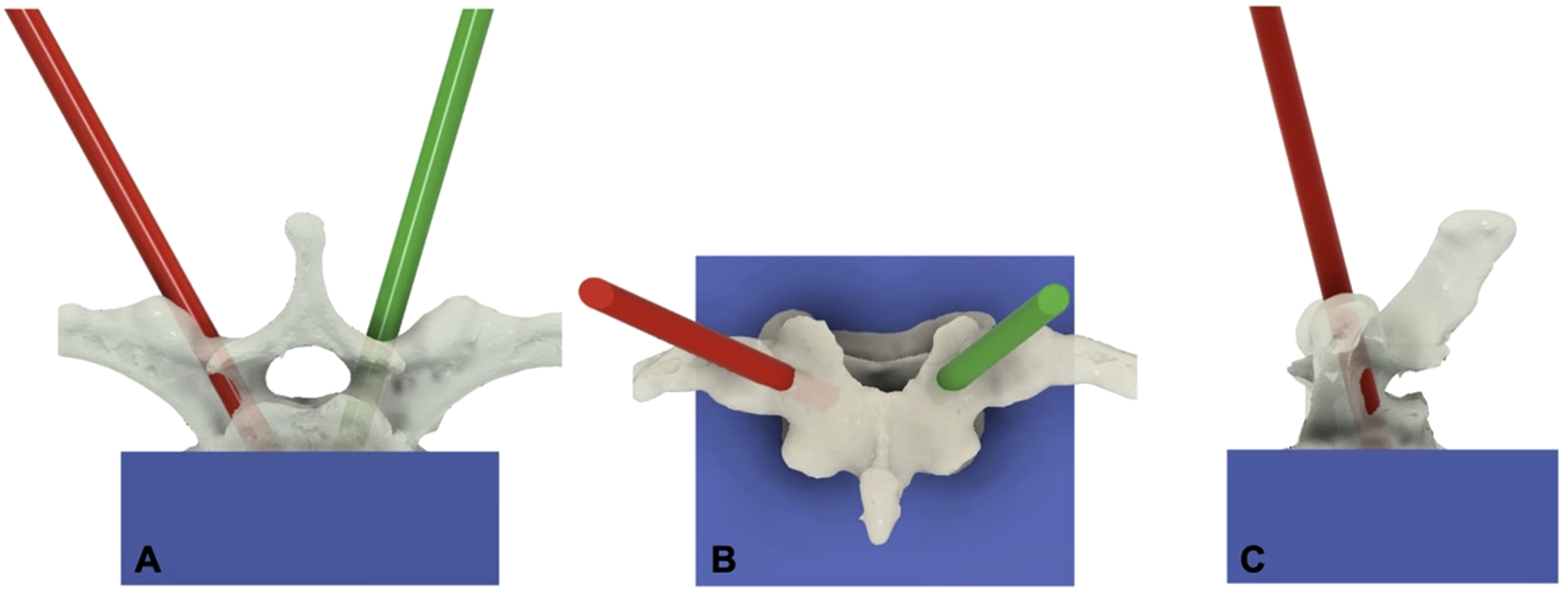
Importantly, offset planning was performed using normalized offset ratios relative to the individual screw diameter. This approach enabled a fine-grained, standardized grading of lateral screw malposition up to the maximum extrapedicular position, independent of the absolute screw diameter.
The side receiving the offset trajectory was randomly assigned. Consequently, each vertebral body was instrumented with one optimally placed intrapedicular screw and one offset screw, allowing for a direct paired comparison within the same vertebra.
Implantation of Pedicle Screws
A specific template was then created for each vertebral body, referenced at the mold cup, which contained the two planned trajectories (Figure 3). Together with a mold adapter and guiding sleeves for drilling and PS implantation (Figure 4), the instrumentation of the vertebral bodies could then be performed. Vertebral body–specific template and mold adapter. The vertebral body–specific template (yellow), referenced at the mold cup and containing the two planned trajectories, is shown in panels (A) and (B). Panel (C) illustrates the assembly with the mold adapter (grey) Mold adapter with vertebral body–specific guidance template. The CAD-planned and 3D-printed mold adapter is shown in combination with a vertebral body–specific guidance template, providing rigid guidance for drilling (green) and pedicle screw insertion (purple)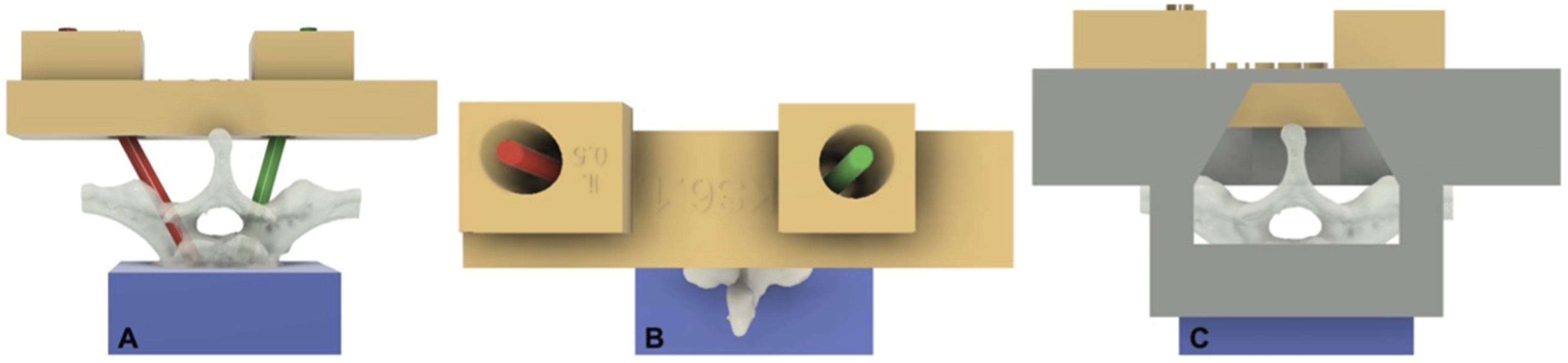

The polyaxial PS system used in this study was Reline MAS (Globus Medical Inc., Audubon, PA, USA). For PS implantation, the trajectory was initially predrilled with a 3.5 mm drill bit to a depth equal to the planned screw length minus 10 mm. A K-wire was then inserted into the drill hole, and the planned PS was placed over it. No pre-tapping was performed. During screw insertion, the peak insertion torque (PIT) was measured (Nm). Following instrumentation, a second CT scan was performed to assess the actual screw position achieved. The measured offset (mm) at the pedicle isthmus was used for the statistical analysis.
Biomechanical Testing
Subsequently, biomechanical testing of the PS was performed. For this purpose, a rod (5 mm diameter, titanium alloy) was inserted into the screw tulip and aligned in a cranio-caudal position. The rod was secured using an insert with a manufacturer-recommended torque of 10 Nm. The mold was then secured in a vice, and the rod was mounted to the force transducer of a universal testing machine (UTM) (Z005, ZwickRoell GmbH & Co. KG, Ulm, Germany) at a distance of 50 mm from the center of the screw head.
Force-controlled cyclic loading was applied to the rod at room temperature to simulate flexion and extension of the thoracic spine. This standardized cyclic preloading was performed to precondition the screw–bone interface and to unmask potential biomechanical weaknesses prior to axial pullout testing. Cyclic loading of the PS was started at a bending moment of 0.5 Nm, with subsequent increments of 0.5 Nm up to a maximum of 2.5 Nm. At each loading level, the PS were subjected to 100 cycles at approximately 0.1 Hz, resulting in a total of 500 cycles per PS (Figure 5A). Experimental biomechanical setup. (A): Force-controlled cyclic loading setup simulating flexion–extension moments applied via a rod connected to the pedicle screw head. (B): Axial pullout testing configuration with load applied along the screw axis until failure.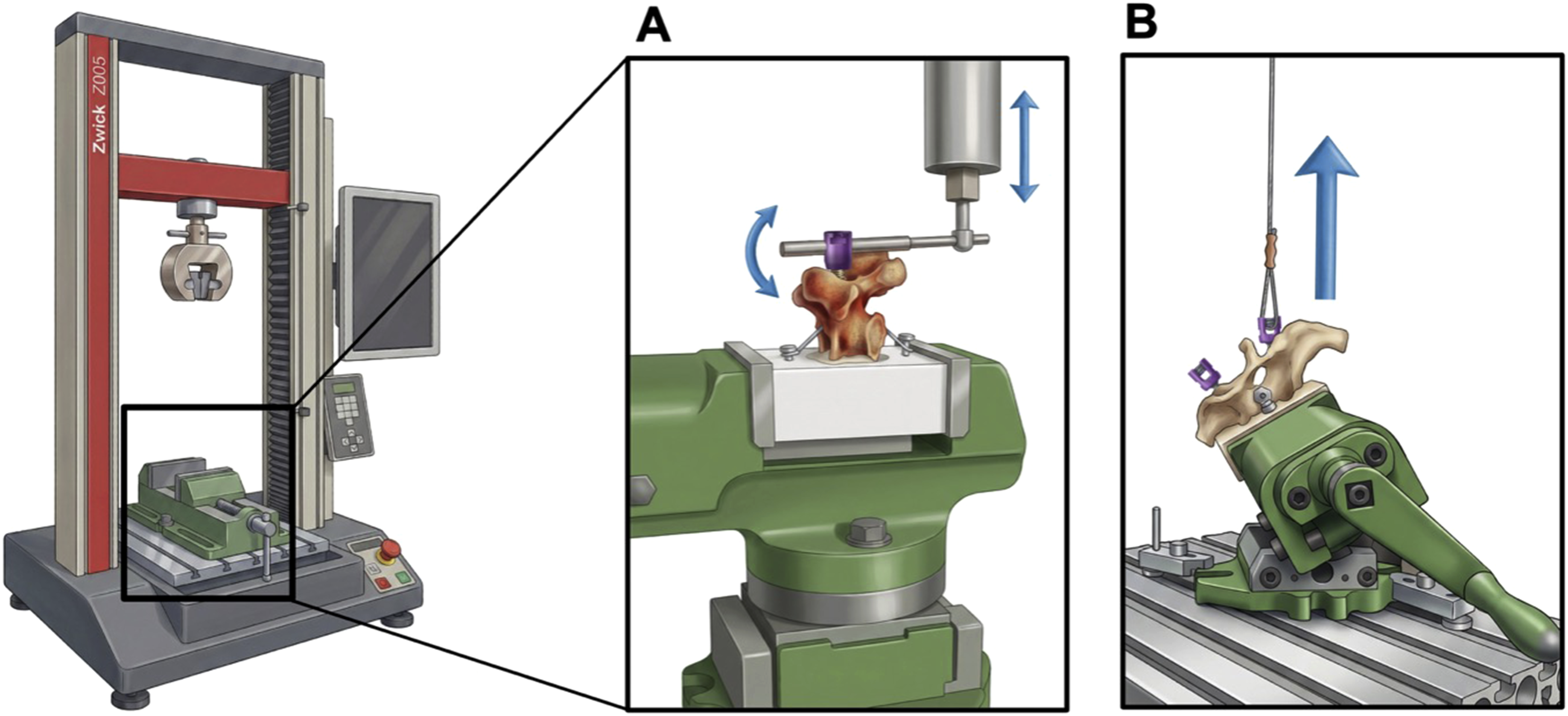
After cyclic loading, the axial pullout force was tested. A transverse force compensation plate was attached to the UTM, and the vice was mounted on top of it. This ensured that the PS pullout occurred along the screw’s axis without introducing shear forces. A wire loop was attached to the UTM hook and to the tulip via the insert.
The hook was then raised to create pretension in the wire rope, keeping the initial pulling force below 0.5 N. The PS was then pulled at a rate of 5 mm/min.18,19 Testing stopped when an 80% drop in force was reached, and the maximum pullout force was recorded (Figure 5B).
The side and sequence of implantation, cyclic loading, and pullout tests (using optimal and offset PS) were randomized. Groups were assigned to ensure a balanced distribution of starting conditions across all five groups (optimal plus four offsets), with similar numbers of tests beginning with each group (range 12–14 PS per group).
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics Version 30 (IBM Corp., Armonk, NY, USA). Quantitative data are expressed as mean ± standard deviation (SD). No a priori sample size calculation was performed due to the lack of prior data on the continuous effect of graded lateral offset on thoracic PS stability. To account for the paired design and subject-specific variability, linear mixed-effects models were employed, with screw parameters (lateral offset, screw diameter, screw length) and bone density as fixed effects, and random intercepts for each vertebral body. The results of the linear mixed-effects models are reported as regression coefficients with standard errors, 95% confidence intervals, and p values. Model diagnostics were performed by visual inspection of Q-Q plots to assess approximate normality of residuals and residual plots to identify obvious systematic patterns. The diagnostic plots did not indicate major violations of the model assumptions. The correlation was calculated using Pearson’s correlation coefficient. A significance level of p<0.05 was set.
Results
Specimen Characteristics
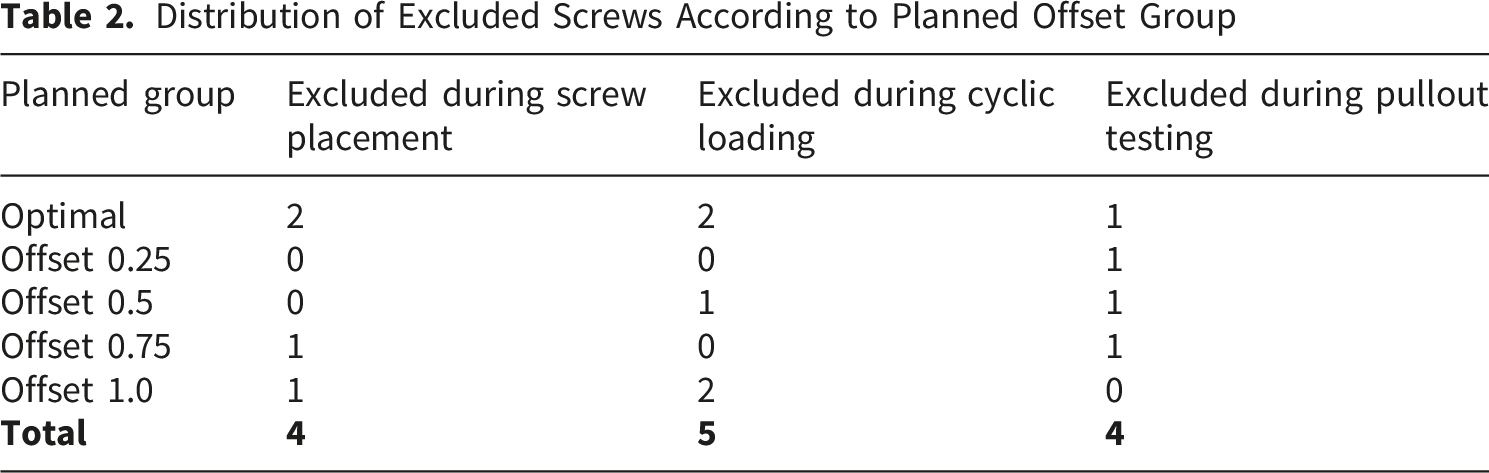
A total of 122 PS were placed in the thoracic spines. After exclusions during PS placement and cyclic loading, 113 PS underwent pullout testing. Of these, 109 PS were included in the POF analysis, whereas 4 PS were excluded during pullout testing because pullout of the contralateral screw had already destroyed the vertebral body. The reasons for excluding the PS are shown in Figure 6, and the distribution of exclusions according to planned offset group is summarized in Table 2. This resulted in 51 vertebrae and 102 PS (84%), of which both screws were included in the pairwise comparisons. Exclusion of vertebrae and pedicle screws Distribution of Excluded Screws According to Planned Offset Group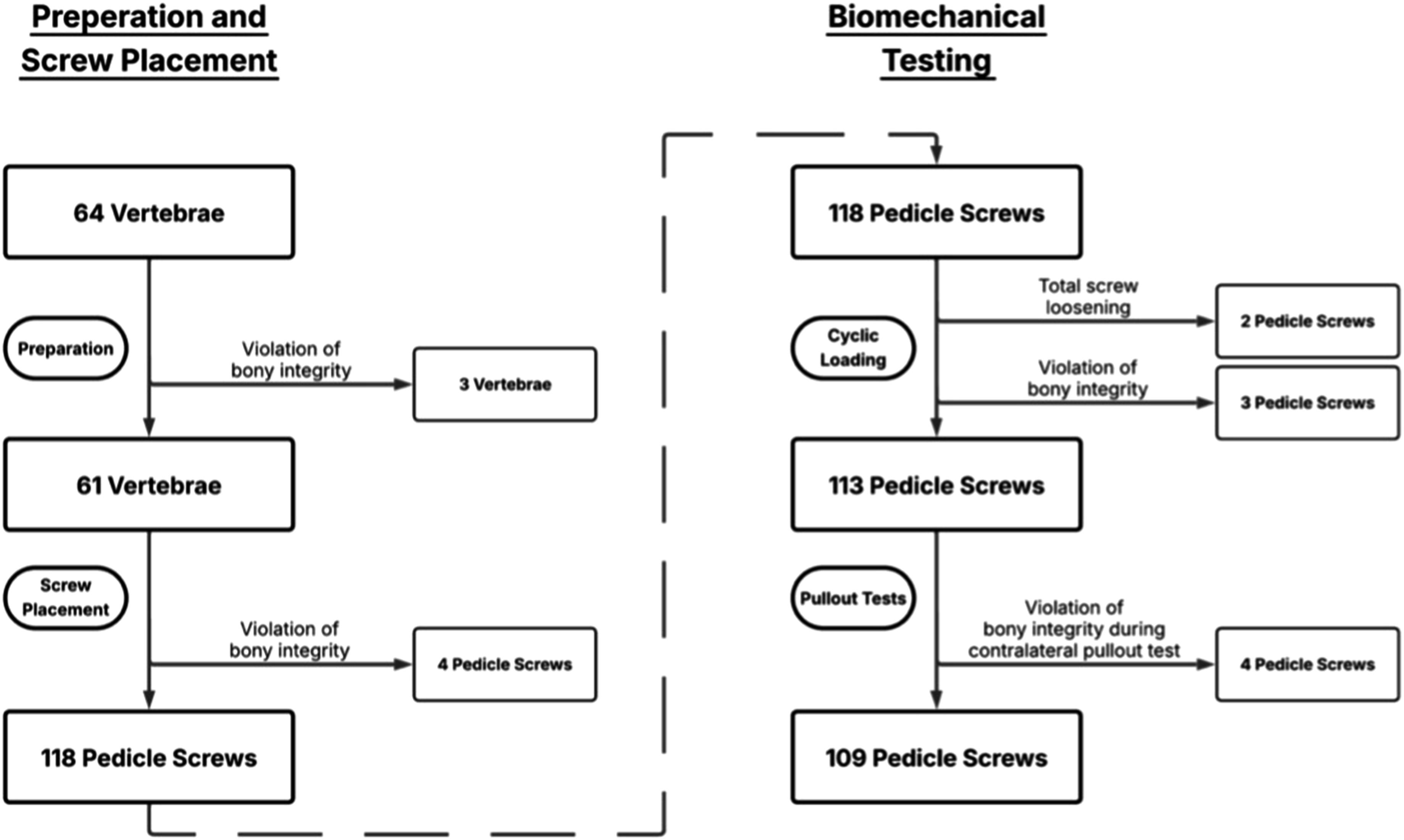
In the final pairwise analysis, the mean HU value of the included vertebral bodies was 186.4 ± 73.1 HU (range: 14.3–300.5 HU).
Across all included PS, a deviation of 0.71 ± 1.20 mm was measured between the planned and actual trajectories. The distribution of the differences between the planned and achieved trajectories is presented in Figure 7. For the statistical analysis, the measured postoperative lateral offset in millimeters was used rather than the planned offset category. Comparison of planned vs. achieved offset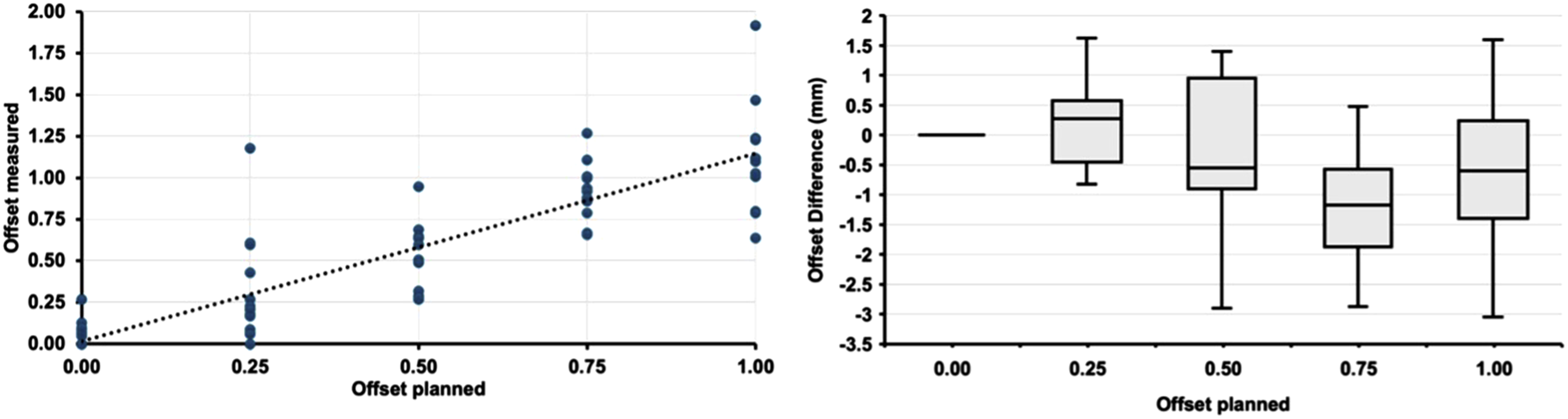
Linear Mixed-Effects Model on Pullout Force (POF)
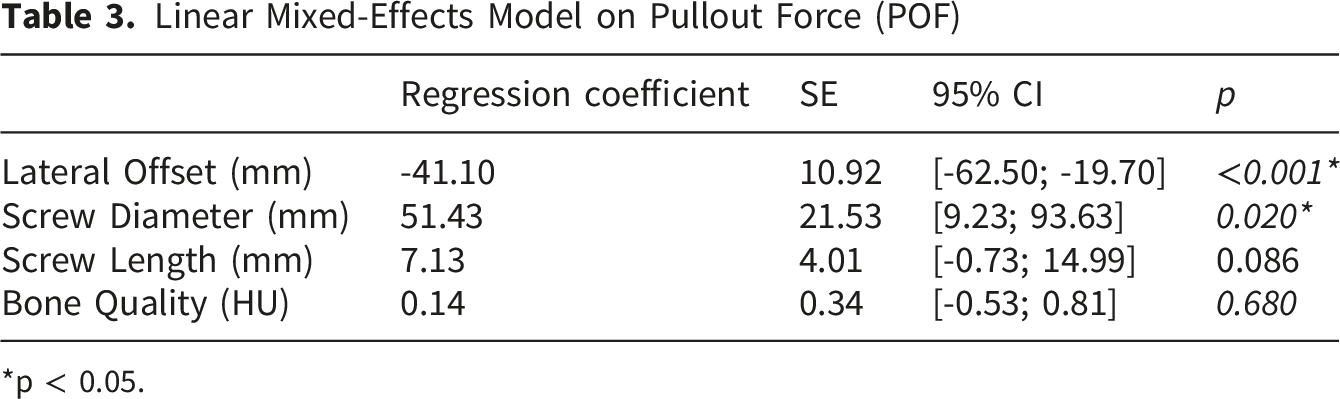
*p < 0.05.
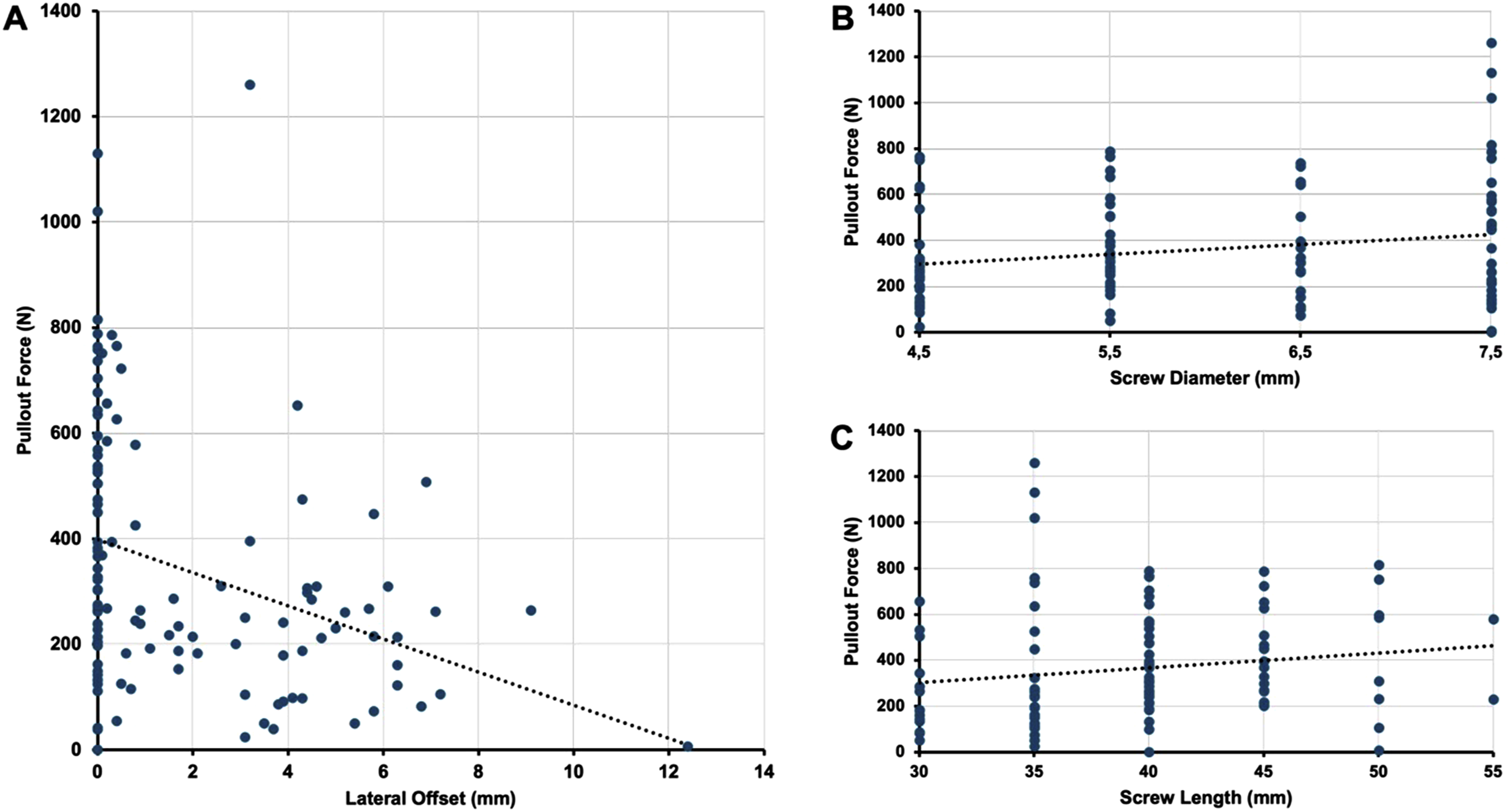
Effects on pullout force. (A): Pullout force vs. lateral offset. (B): Pullout force vs. screw diameter. (C): Pullout force vs. screw length
Additionally, the analysis showed that screw diameter had a significant positive effect on POF, with an estimated increase of 51.4 N per millimeter in diameter (95% CI: [9.23; 93.63]; p=0.020) (Figure 8B). Although screw length demonstrated a positive trend, the association was not statistically significant (p=0.086) (Figure 8C). Bone quality, assessed in Hounsfield Units, did not significantly affect POF (p=0.680).
Linear Mixed-Effects Model on Peak Insertion Torque (PIT)
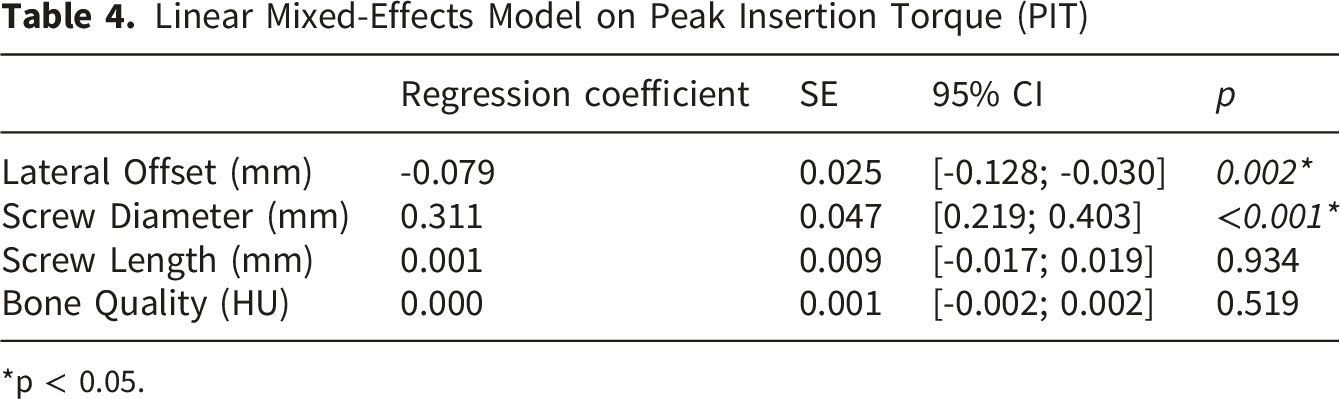
*p < 0.05.
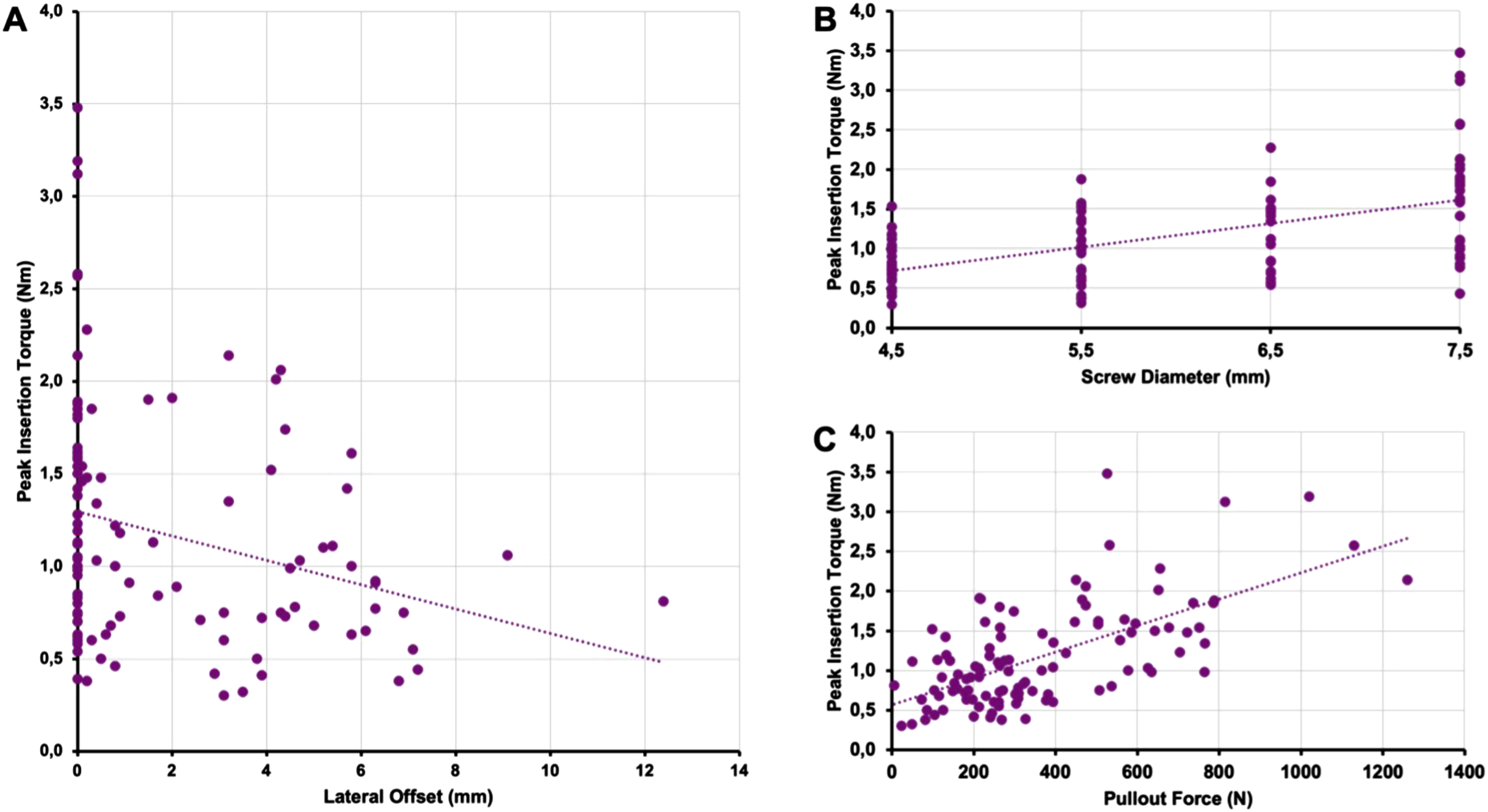
Effects on peak insertion torque. (A): Peak insertion torque vs. lateral offset. (B): Peak insertion torque vs. screw diameter. (C): Peak insertion torque vs. pullout force
A comparison between the two main parameters, POF and PIT, revealed a strong and statistically significant correlation (r=0.637, p<0.001) (Figure 9C).
In a subgroup analysis of optimally placed PS (n=58) (Figure 10), a weak correlation of 0.331 was found between POF and screw diameter (p=0.017). The correlations between POF and screw length (r=0.163, p=0.222) and between POF and bone quality (r=0.224, p=0.091) were not statistically significant. Subgroup analysis of optimally placed screws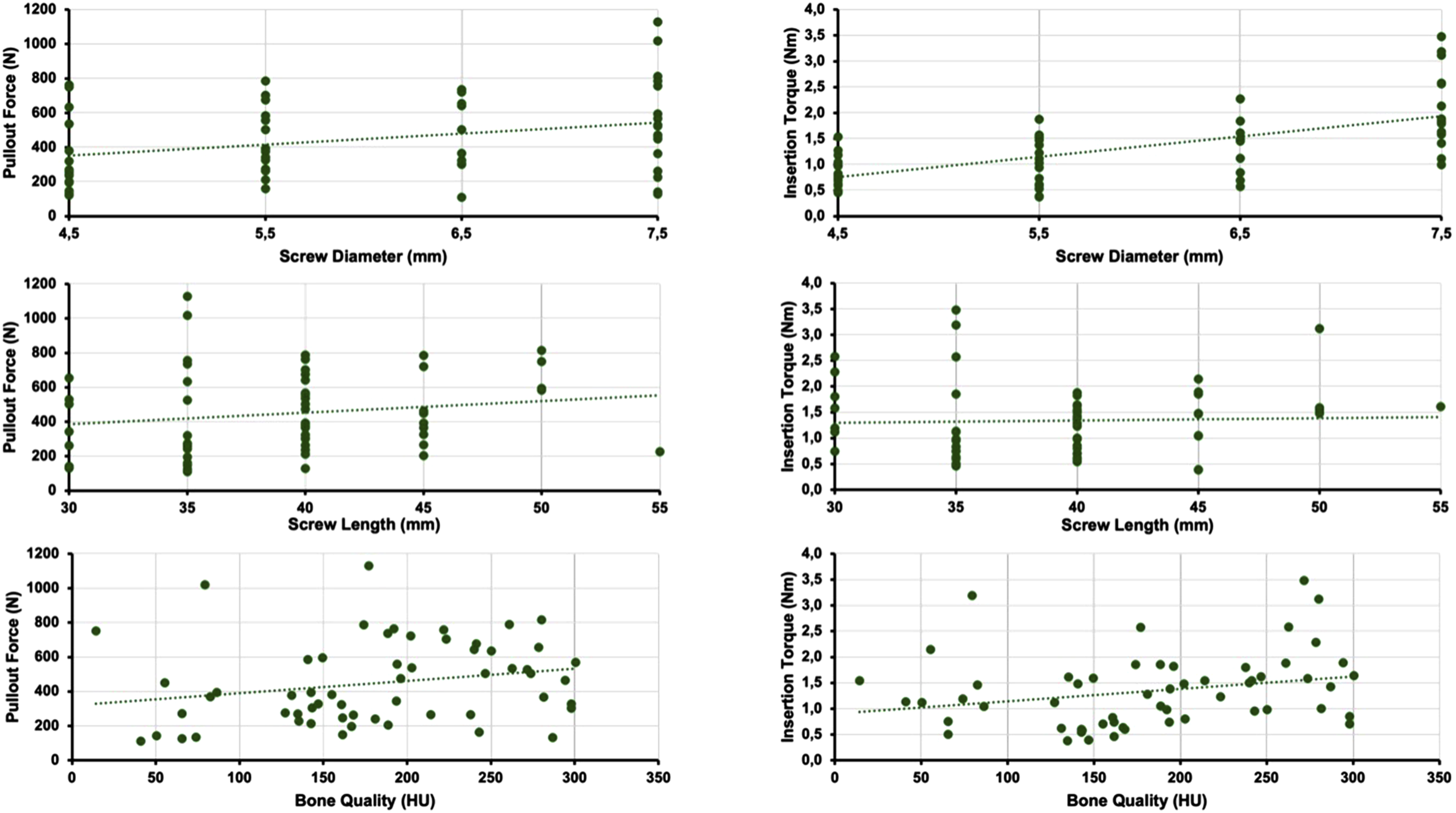
Regarding PIT, a strong correlation was observed with screw diameter (r=0.647, p<0.001), whereas screw length (r=0.036, p=0.790) and bone quality (r=0.255, p=0.055) did not reach statistical significance.
Discussion
Pedicle screws (PS) are commonly used for dorsal instrumentation of the thoracic spine. While advanced technologies such as 3D navigation and robot-assisted surgery have been shown to improve placement accuracy,20,21 their limited availability means that screw misplacements remain a clinically relevant issue. Existing classification systems predominantly focus on the proximity to neurovascular structures,5,22 yet significant complications in this regard remain rare. 23 However, particularly in elderly patients with compromised bone quality, accurate placement is crucial to ensure biomechanical stability.
To address this, the present study systematically investigates the effect of varying degrees of lateral offset on the biomechanical stability of thoracic PS, with the primary objective of quantifying how lateral misplacement influences biomechanical stability as measured by pullout force (POF).
Lateral offset of PS in the thoracic spine showed a significant negative influence on POF, indicating that each millimeter of lateral misplacement decreased biomechanical stability by approximately 9.2%.
Studies on lateral perforation of PS in the thoracic spine have thus far primarily employed a binary experimental design (optimal vs. perforated). For example, a study by Brasiliense et al demonstrated that laterally perforated PS in the thoracic spine exhibited lower biomechanical stability compared to optimally placed PS. 24
In contrast, more studies exist for the lumbar spine. Costa et al investigated the influence of perforations on biomechanical stability in porcine lumbar vertebrae, 25 showing a significant reduction in stability with increasing perforation. Due to the randomized malpositioning, this study included various directions and degrees of perforation, which resulted in a reduced sample size in each subgroup. Another cadaver study demonstrated that isolated perforation of the lateral pedicle cortex resulted in a reduction of POF. 26
Tsagkaris et al examined the influence of perforation extent on the biomechanical stability of lumbar pedicle screws using template-guided misplacement, in a methodological approach related to that of the present study. 27 They found that lateral perforation, created by parallel displacement of the screw trajectory, led to reduced POF. This effect increased with the extent of the perforation, which was performed in 2 mm increments up to a maximum of 6 mm.
However, lateral pedicle perforations in the lumbar and thoracic spine should be considered separately. While lateral perforation in the lumbar spine is commonly defined as PS malposition, there is no such consensus in the thoracic spine. Due to the frequently small diameter of the thoracic pedicles, alternative PS trajectories have been established in the thoracic spine, such as the “costovertebral” 28 or “in-out-in” 29 techniques, both of which involve an intentional lateral breach. These PS can nevertheless be classified as clinically acceptable. 30 According to the evaluation system of Zdichavsky et al for thoracic PS, these lateral PS are also considered optimal. 31
The biomechanical analysis of these alternative trajectories has already been conducted in several studies. One study of the thoracic spine demonstrated comparable decreases in spinal mobility and resistance to cyclic loading between intra-pedicular screws and those positioned in the costovertebral joint. 32 A detailed biomechanical study by Little et al, which included cyclic loading followed by pullout testing, demonstrated that the costovertebral screw position was inferior to the intrapedicular position and should be considered a salvage option rather than a primary trajectory. After cyclic loading, the POF in the intrapedicular trajectory was 62% higher than in the costovertebral trajectory. 33
Hirano et al also showed that approximately 60% of the POF depends on the structural characteristics of the pedicle, while only about 40% is attributable to the vertebral body. 34 This finding implies that in cases of complete extrapedicular placement at the pedicle isthmus, a loss of approximately 60% of the POF might be expected. However, it should be noted that this investigation was conducted in the lumbar spine.
Screw diameter showed a significant positive effect on both POF and PIT, suggesting that larger screw diameters enhance biomechanical stability.
This finding is consistent with existing literature. Several biomechanical studies have reported a correlation between screw diameter and pullout force.35,36
Our data indicate that, per millimeter, increasing screw diameter improves stability more than lateral offset reduces it. However, pairwise comparisons within each vertebral body involved screws of identical diameter. Screw diameter effects were therefore assessed across specimens, which should be considered when interpreting diameter-specific effects.
With increased lateral offset, PIT was significantly reduced. Furthermore, this study demonstrated a strong and statistically significant correlation between POF and PIT, highlighting a biomechanical link between these parameters.
Zdeblick et al previously demonstrated the relationship between these parameters. 37 Additional factors that can influence PIT, such as screw design 38 and bone quality, 39 have been described in the literature.
Overall, PIT appears to be a promising indicator for the biomechanical stability of a PS. However, to achieve clinical relevance intraoperatively, it would be essential to calibrate this parameter at least against bone quality, screw diameter, and screw design.
Alternatively, intraoperative comparison of PIT values between all screws inserted during the same procedure may represent a more feasible strategy. This approach may allow the identification of potential outliers, particularly since other influential factors, such as patient-specific anatomy, are difficult to generalize and therefore challenging to incorporate into a reliable model. Identifying such outliers could lead to targeted verification of individual screws, for example, through focused intraoperative 3D imaging. This would enable immediate intraoperative revision if required, thereby improving surgical accuracy and outcomes.
Bone quality, as measured by Hounsfield Units (HU), did not significantly affect either POF or PIT in this study. However, in the subgroup of optimally placed PS, a trend was observed. This finding should be interpreted cautiously, as the relationship between bone quality and pedicle screw fixation strength has been described in the literature. 39 Therefore, the absence of a statistically significant effect in the present models should not be interpreted as evidence that bone quality is not relevant. Rather, it indicates that an independent effect of HU-based bone quality could not be demonstrated under the specific experimental conditions of this study.
One possible explanation is that the present study was primarily designed to investigate the influence of lateral offset, whereas HU-based bone quality was analysed as a secondary objective. Accordingly, the study was not specifically powered to detect an independent effect of HU. In addition, HU was measured on post-mortem CT scans of the vertebrae in this study. Due to post-mortem changes in bone tissue and the absence of perfusion, the HU values obtained may not be fully comparable to those measured in living patients. As a result, HU-based assessments of bone quality in this study should be interpreted with caution, as they may not accurately reflect in vivo bone density or structural integrity. Nevertheless, a comparison between specimens remains valid, as all HU measurements were obtained using the same standardized procedure.
From a clinical perspective, the present findings suggest that lateral thoracic pedicle screw breaches should not be regarded as purely radiographic deviations without potential mechanical relevance. However, as this was an ex vivo cadaveric study, the results should be interpreted as evidence of a biomechanical principle rather than as a direct prediction of clinical screw loosening or construct failure. Even when a lateral breach may appear clinically acceptable because of the lower immediate risk to neurovascular structures, increasing lateral offset was associated with progressive loss of fixation strength in this study. This may be particularly relevant in patients at increased risk of mechanical failure, such as elderly individuals or those with reduced bone quality, in whom even moderate reductions in screw stability could contribute to loosening or construct failure. Accordingly, accurate intraoperative screw placement remains important, and suspicious lateral trajectories may warrant targeted verification and, if necessary, immediate correction.
In this study, only the effect of lateral perforation on biomechanical stability was tested. This focus was chosen because previous studies have shown that medially perforated PS, which are associated with increased cortical contact, demonstrate superior biomechanical results. 27 Additionally, lateral perforations occur more frequently in clinical settings, are often considered less critical from a neurovascular standpoint, and are intentionally used in some surgical techniques.29,40 Taken together, these factors make lateral perforation a clinically relevant focus for biomechanical analysis.
Furthermore, a pairwise comparison of two identical PS was performed, even though a trajectory with a lateral offset would often have permitted the use of longer, thicker PS. This decision was made because the primary aim of this study was to analyse the biomechanical impact of unintended lateral misplacement of thoracic PS. Specifically, the study aimed to simulate a scenario in which a screw that was initially planned and dimensioned for an intrapedicular position was inadvertently placed laterally.
As this was a cadaver study, the generalizability of the results to patients is limited due to differences in tissue properties and biomechanical conditions. Furthermore, one limitation of this study is that the vertebral bodies used for biomechanical testing were removed from both the surrounding soft tissues and the rib cage. Watkins et al have demonstrated the importance of an intact rib cage for the biomechanical stability of the thoracic spine. 41 However, the extent to which the POF of PS in the costovertebral joint depends on the stability provided by the rib cage has not yet been investigated. It may be hypothesized that the reduced holding strength of the rib might result in falsely low POF values for PS placed in the costovertebral joint.
Moreover, the study design focused on pairwise comparisons of lateral offsets, thereby maximizing data quality and minimizing the influence of potential covariates on the primary objective. However, the additional factors analysed as secondary objectives could not be fully accounted for in the methodology and should therefore be interpreted with caution in this context. In addition, thoracic level and cadaver clustering were not included as additional covariates or random-effects levels to avoid further increasing model complexity. Although level-related anatomical differences may partly be reflected by screw diameter and screw length, and donor-related differences in bone quality may partly be reflected by HU-based bone density, residual level- and donor-specific effects cannot be fully excluded.
Conclusions
This study demonstrated that increasing the lateral perforation of pedicle screws in the thoracic spine progressively reduces pullout force, underscoring the importance of precise screw placement. Ensuring optimal screw positioning within the pedicle appears essential for maintaining the biomechanical integrity of the construct. Moreover, the observed decrease in stability was progressive, indicating that increasing lateral misplacement led to greater biomechanical compromise. These findings emphasize the importance of reliable intraoperative techniques to minimize lateral misplacement.
Footnotes
Ethical Considerations
The study was reviewed and approved by the responsible Ethics Committee (Application No. 2024-17723). The legal and ethically correct handling of the human cadavers was reviewed by the ethics committee and confirmed by a positive vote. All procedures were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to Participate
The cadavers were obtained from Science Care (Science Care, Phoenix, AZ). Consent from the body donors for use in medical research was obtained during the donor’s lifetime.
Author contributions
Benno Bullert contributed to the conceptualization and design of the study, data acquisition, statistical analysis, and drafting of the manuscript, and supervised the project. Viktor Gupta contributed to the conceptualization and design of the study, data acquisition, statistical analysis, and revision of the manuscript. Mareike Schonhoff contributed to the conceptualization and design of the study, data analysis and interpretation, and critical revision of the manuscript. Sebastian Jaeger contributed to the conceptualization and design of the study and critical revision of the manuscript. J. Philippe Kretzer and Paul A. Gruetzner contributed to the conceptualization and design of the study, funding acquisition, supervision, and critical revision of the manuscript. Sven Y. Vetter contributed to funding acquisition, supervision, and critical revision of the manuscript. Jula Gierse contributed to the conceptualization and design of the study, statistical analysis, supervision, and critical revision of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The research group MINTOS had grants/grants pending and technical support from Siemens Healthineers AG (Erlangen, Germany) and Globus Medical Inc. (Audubon, Pennsylvania, USA). The funders had no involvement in the study conceptualization, design, data collection, analysis, nor the decision to publish or the preparation of the manuscript. SJ reports institutional research support from Johnson & Johnson DePuy, Ceramtec GmbH, Implantcast GmbH, Heraeus Medical, Peter Brehm GmbH, Förderkreis Orthopädie e.V. and the BMFTR – Federal Ministry of Research, Technology and Space. JPK reports institutional research support from AQ Solutions GmbH, Ceramtec GmbH, Implantcast GmbH, Innoproof GmbH, SINTX Technologies, Inc., Permedica S.P.A., Questmed GmbH, and Back to mobility GmbH; personal payments/honoraria from Meril GmbH, Permedica S.P.A., Falcon Medical GmbH, and DePuy Synthes/Johnson & Johnson Medical GmbH; and leadership roles on the boards of the German Society of Biomechanics and Förderkreis Orthopädie e.V. The remaining authors declare no additional competing interests.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the author(s) used DeepL (DeepL SE, Cologne, Germany) and ChatGPT-5.5 (OpenAI, San Francisco, California, USA) to check for spelling and grammar. In addition, Illustrae (Illustrae Ltd, Eastbourne, United Kingdom) was used as the basis for figure creation. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the publication’s content.