
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare clinical features and outcomes between culture-positive and culture-negative vertebral osteomyelitis (VO), describe empirical antimicrobial regimens used for culture-negative VO, and identify independent predictors of 1-year recurrence and mortality.
Methods
We retrospectively reviewed 252 consecutive patients treated for VO at a tertiary center (2010–2023). Finally, 206 patients were analyzed (173 culture-positive, 33 culture-negative). Demographics, comorbidities, laboratory and imaging findings, microbiology, antimicrobial regimens, and surgical treatment were collected. Antimicrobials were generally administered for ≥6 weeks. Primary outcomes were initial treatment failure, recurrence, 1-year all-cause mortality, and infection-related mortality.
Results
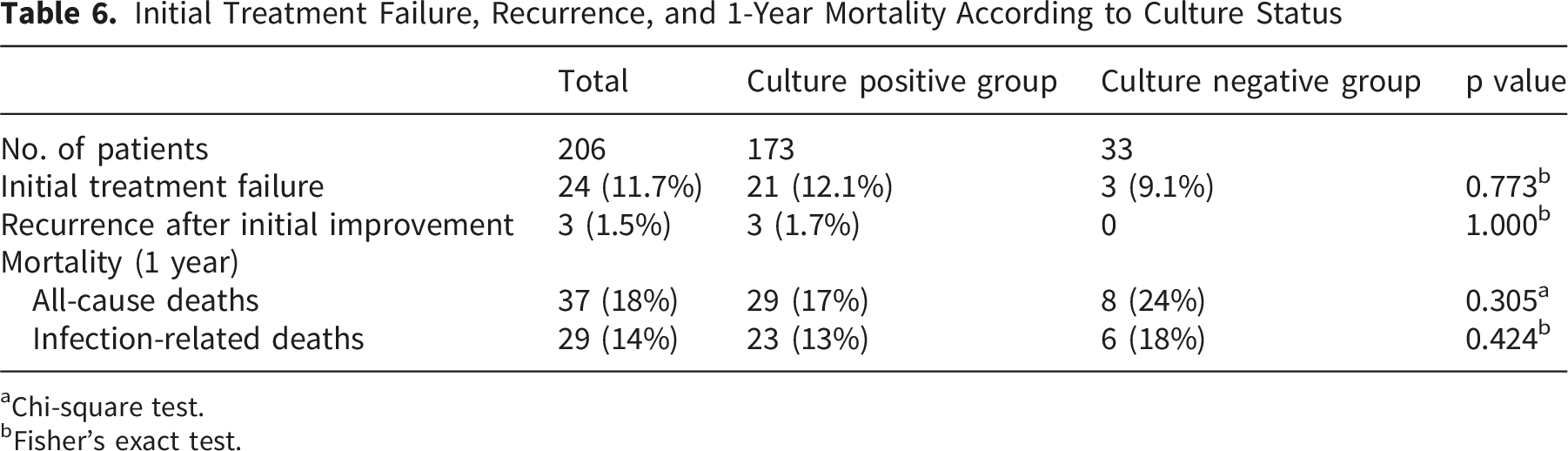
Culture-negative VO showed lower temperature, C-reactive protein, and white blood cell count; higher albumin; and fewer epidural abscesses than culture-positive VO, consistent with a milder phenotype. Initial treatment failure and recurrence occurred in 24/206 (11.7%) and 3/206 (1.5%) patients, respectively. All recurrences occurred in the culture-positive group. One-year all-cause mortality was 17% (29/173) in culture-positive and 24% (8/33) in culture-negative patients (p=0.305); infection-related mortality was 13% and 18%, respectively (p=0.424). Among culture-negative patients, outcomes did not differ between cefazolin-based versus other empirical regimens. Multivariable analysis identified older age, higher Charlson Comorbidity Index, hypoalbuminemia, and absence of surgery as independent predictors of mortality, whereas culture status was not.
Conclusions
In this cohort with high microbiological yield (84%), culture-negative VO presented with milder clinical features and had recurrence and 1-year mortality comparable to culture-positive VO when treated with ≥6 weeks of antimicrobials. Prognosis was driven primarily by host factors rather than culture status.
Introduction
Vertebral osteomyelitis (VO) is a rare but serious spinal infection predominantly affecting older adults and those with significant comorbidities. 1 Improvements in magnetic resonance imaging (MRI) and population aging have contributed to the increasing incidence of VO, which remains associated with prolonged hospitalization, neurological impairment, and substantial mortality. 1 Although establishing a definitive diagnosis of native vertebral osteomyelitis can be time-consuming in some patients, 2 it can often be achieved promptly with early use of advanced imaging and appropriate microbiological investigation. A microbiological diagnosis is central to VO management, as it allows targeted antimicrobial therapy and supports antimicrobial stewardship.2,3 Guidelines from the Infectious Diseases Society of America recommend performing multiple sets of blood cultures, and whenever feasible, conducting image-guided or open spinal biopsy before initiating antimicrobial therapy. 2
Despite these strategies, culture yield remains imperfect. In approximately 20–40% of VO cases, the causative organisms fail to be identified, often because of prior antibiotic exposure, low bacterial burden, or sampling limitations.2-5 In culture-negative VO, clinicians must rely on empirical regimens directed mainly against Staphylococcus aureus and common Gram-negative bacilli, tailored to the local epidemiology and host risk factors.2,5,6 Several observational studies have previously suggested that culture-negative VO presents with a less intense systemic inflammatory response and may have outcomes comparable to or even better than those of microbiologically confirmed infections when adequately treated.5,7-9 Conversely, other reports and reviews have emphasized the uncertainty surrounding empirical choices, the risk of overly narrow or unnecessarily broad coverage, and the potential for relapse or treatment failure in culture-negative VO.5,8,10 Consequently, there is currently no consensus regarding the optimal empirical strategy, particularly the balance between narrow-spectrum regimens targeting methicillin-sensitive S. aureus and streptococci versus broad-spectrum combinations with routine anti-MRSA coverage—and relatively few studies have examined how culture status relates to long-term outcomes, such as recurrence and mortality, or interacts with established prognostic factors.
To address these gaps, we conducted a single-center retrospective study of patients with VO to compare the clinical characteristics, imaging findings, antimicrobial use, and outcomes between culture-positive and culture-negative cases, focusing specifically on real-world empirical regimens for culture-negative VO (commonly based on first-generation cephalosporins in our center) and their association with recurrence and 1-year mortality. Therefore, this study addressed the following questions: (1) Do culture-negative and culture-positive VO differ in clinical presentation and outcomes, including recurrence and 1-year mortality? (2) What empirical antimicrobial regimens are used for culture-negative VO in routine clinical practice, and is empirical antimicrobial choice associated with prognosis? (3) Which factors independently predict 1-year all-cause and infection-related mortality in patients with VO?
Materials and Methods
Study Design and Setting
This study was a level IV retrospective cohort study conducted at a single tertiary medical center. We identified 252 consecutive patients who were diagnosed with and treated for VO between January 2010 and April 2023. We excluded patients with tuberculous spondylitis, postoperative spinal infection, isolated epidural abscesses without vertebral involvement, and those managed exclusively as outpatients.
Participants
Of the 252 patients initially diagnosed with VO during the study period, 46 were excluded because 1-year follow-up data were unavailable (those who died within 1 year were retained), leaving 206 patients for the analysis (173 culture-positive and 33 culture-negative). Thus, none of the patients included in the final cohort were lost to follow-up after the 1-year time point.
In this study, the term vertebral osteomyelitis (VO) was used broadly to include infectious involvement of the vertebral bodies, intervertebral discs, or both (i.e., spondylodiscitis/discitis and vertebral osteomyelitis). VO was suspected on the basis of new or worsening back or neck pain, fever, and laboratory evidence of inflammation. To facilitate early diagnosis, the initial evaluation included MRI, contrast-enhanced CT, and at least two sets of blood cultures. The diagnosis was confirmed by integrating the clinical, imaging, laboratory, and microbiological findings. MRI features consistent with VO include endplate destruction, increased T2-weighted signal intensity in the vertebral bodies and intervertebral discs, and epidural or iliopsoas abscesses. CT was used to evaluate the extent of endplate and vertebral body destruction. Imaging diagnoses were jointly confirmed by a senior spine surgeon with 30 years of experience in orthopedic and spine surgery and an experienced radiologist. In culture-negative cases, imaging was re-evaluated to exclude sacroiliitis and non-infectious conditions, such as ankylosing spondylitis or axial spondyloarthritis.
Overview of Treatment and Surgery
At the initial presentation, patients with suspected VO underwent at least two sets of blood cultures. When clinically indicated for microbiological diagnosis, percutaneous aspiration of the disc space or a vertebral body abscess was performed to identify the causative organism. CT-guided drainage was performed for psoas abscesses, and all specimens were cultured. Surgical intervention was indicated in patients with poor response to antimicrobial therapy, progressive neurological deficit, spinal instability or deformity, or extensive vertebral destruction. Poor response to antimicrobial therapy was defined as persistent or worsening pain, fever, inflammatory markers, or imaging findings despite appropriate antimicrobial treatment. Deformity was defined as progressive kyphotic or segmental alignment abnormality associated with infectious destruction. Meanwhile, vertebral destruction was defined as marked endplate or vertebral body destruction on CT or MRI judged to compromise spinal stability or risk progressive collapse. In such cases, debridement of the infection focus with decompression and/or spinal stabilization was conducted, and intraoperative specimens were obtained for culture. All microbiological results were reviewed by infectious disease specialists and any isolates judged to be affected by contamination were excluded from the analysis.
Antimicrobial regimens were selected by spine surgeons and infectious disease specialists based on each patient’s clinical presentation, culture results, and antimicrobial susceptibility testing. In principle, antibiotic therapy was administered for a total duration of at least 6 weeks, in accordance with the current guideline recommendations for VO, typically beginning with intravenous therapy.2,11,12 Oral antibiotic therapy was subsequently introduced in selected patients under infectious disease specialist supervision, based on the clinical course, including trends in inflammatory markers, overall clinical condition, and the presence of implanted foreign material such as spinal instrumentation or a prosthetic valve.
Patients underwent regular follow-up in the outpatient clinic with clinical assessment, laboratory tests (including C-reactive protein [CRP] and white blood cell count [WBC]), and imaging conducted as needed. Follow-up MRI or CT was conducted when clinical or laboratory improvements were insufficient, or when recurrence was suspected. Patients with at least 1 year of follow-up after diagnosis were included in the analysis; deaths occurring within 1 year were also recorded and classified as either infection-related or non-infection-related.
Variables, Outcome Measures, Data Sources, and Bias
Clinical data, including age, sex, body mass index (BMI), and medical history, were collected from the electronic medical records. Comorbidity burden was assessed using the Charlson Comorbidity Index (CCI) according to the original, non-age-adjusted Charlson method. 13 The maximum body temperature (°C) within 1 week of presentation was recorded as a clinical variable. Laboratory variables obtained within 1 week of presentation included white blood cell count (×109/L), C-reactive protein (mg/dL), and minimum serum albumin level (g/dL). Imaging studies were reviewed for the presence of epidural and iliopsoas abscesses, the site of vertebral involvement, as well as the number of infected intervertebral discs. When infection was confined to a single vertebral body without any apparent disc involvement, the number of infected discs was recorded as one. The presence of infective endocarditis (IE) and antibiotic exposure prior to culture sampling were also documented. The presence of infective endocarditis (IE) was determined by cardiology specialists using transthoracic echocardiography and/or transesophageal echocardiography, as clinically appropriate. Motor function was graded using the American Spinal Injury Association Impairment Scale (AIS), with AIS grades A–C indicating severe paralysis.
All patients were evaluated by spine surgeons and infectious disease specialists and classified as culture-positive when a causative organism was identified from any collected specimen, including blood cultures, disc space aspiration, CT-guided drainage, or intraoperative specimens. Patients were classified as culture negative only when no causative organism was identified from any of these microbiological specimens. The primary outcomes included initial treatment failure, infection recurrence, and 1-year all-cause and infection-related mortality. Treatment success was defined as clinical improvement or stabilization after the initial treatment course, without death due to uncontrolled vertebral osteomyelitis during that course. Initial treatment failure was defined as death due to uncontrolled vertebral osteomyelitis with sepsis progressing to multiple organ failure during the initial treatment course. Recurrence was defined as clinical and radiological deterioration requiring renewed or prolonged antimicrobial therapy and/or repeat surgery after initial improvement. Infection-related death was defined as death attributable to uncontrolled vertebral osteomyelitis, persistent or recurrent bloodstream infection associated with vertebral osteomyelitis, or infectious complications occurring during treatment. Deaths primarily attributable to non-infectious causes, such as malignancy, cardiovascular events, or senility, were classified as non-infection related.
To mitigate misclassifications, all imaging and microbiological results were jointly reviewed by spine surgeons, radiologists, and infectious disease specialists.
Ethical Approval
This study was approved by our institutional review board (approval number: zn231213). Participants’ notifications were managed using a general opt-out approach. The study complied with the institutional ethical guidelines and the Declaration of Helsinki, and the need for individual informed consent was waived.
Statistical Analysis
All statistical analyses were conducted using JMP 17.0 (JMP, Cary, NC, USA). Continuous variables were tested for normality and compared using Student’s t-test or the Mann–Whitney U test, as appropriate. Categorical variables were compared using the chi-square test or Fisher–Freeman–Halton exact test. Univariate logistic regression analyses were applied to investigate the variables associated with 1-year all-cause and infection-related mortality. Variables that were statistically significant in the univariate analysis, and judged to be clinically relevant, were entered into the multivariate logistic regression models. Collinearity among candidate variables was assessed using correlation matrices and variance inflation factors (VIFs), together with clinical judgment. A VIF of greater than 5 was considered to indicate potentially important multicollinearity. Variables identified as highly collinear were not included in the same multivariable model. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, and the level of significance was set at p < 0.05.
Results
Patient Characteristics and Antibiotic Treatment
Demographic and Clinical Characteristics of Patients With Vertebral Osteomyelitis According to Culture Status
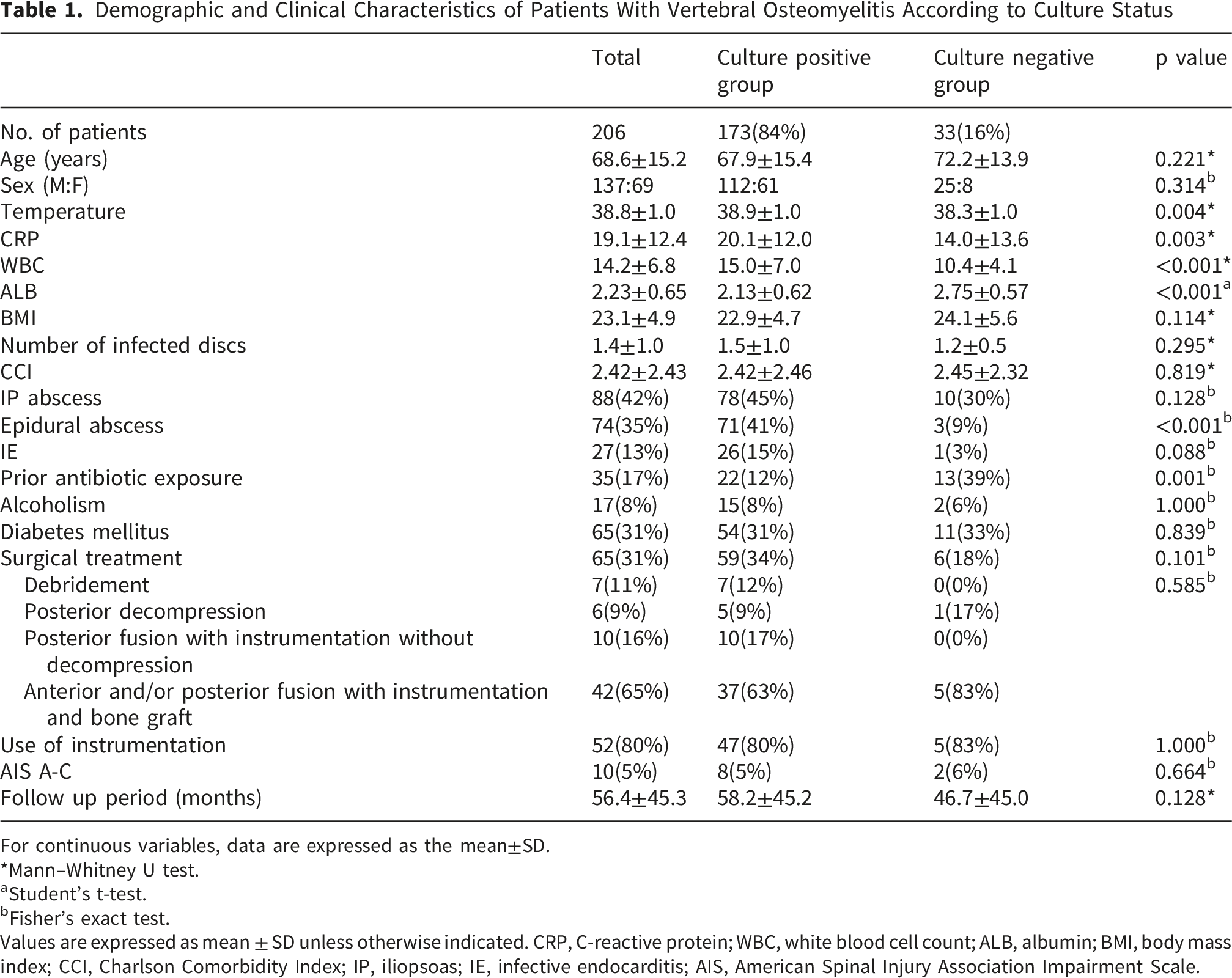
For continuous variables, data are expressed as the mean±SD.
*Mann–Whitney U test.
aStudent’s t-test.
bFisher’s exact test.
Values are expressed as mean ± SD unless otherwise indicated. CRP, C-reactive protein; WBC, white blood cell count; ALB, albumin; BMI, body mass index; CCI, Charlson Comorbidity Index; IP, iliopsoas; IE, infective endocarditis; AIS, American Spinal Injury Association Impairment Scale.
Distribution of Charlson Comorbidity Index Components by Culture Status
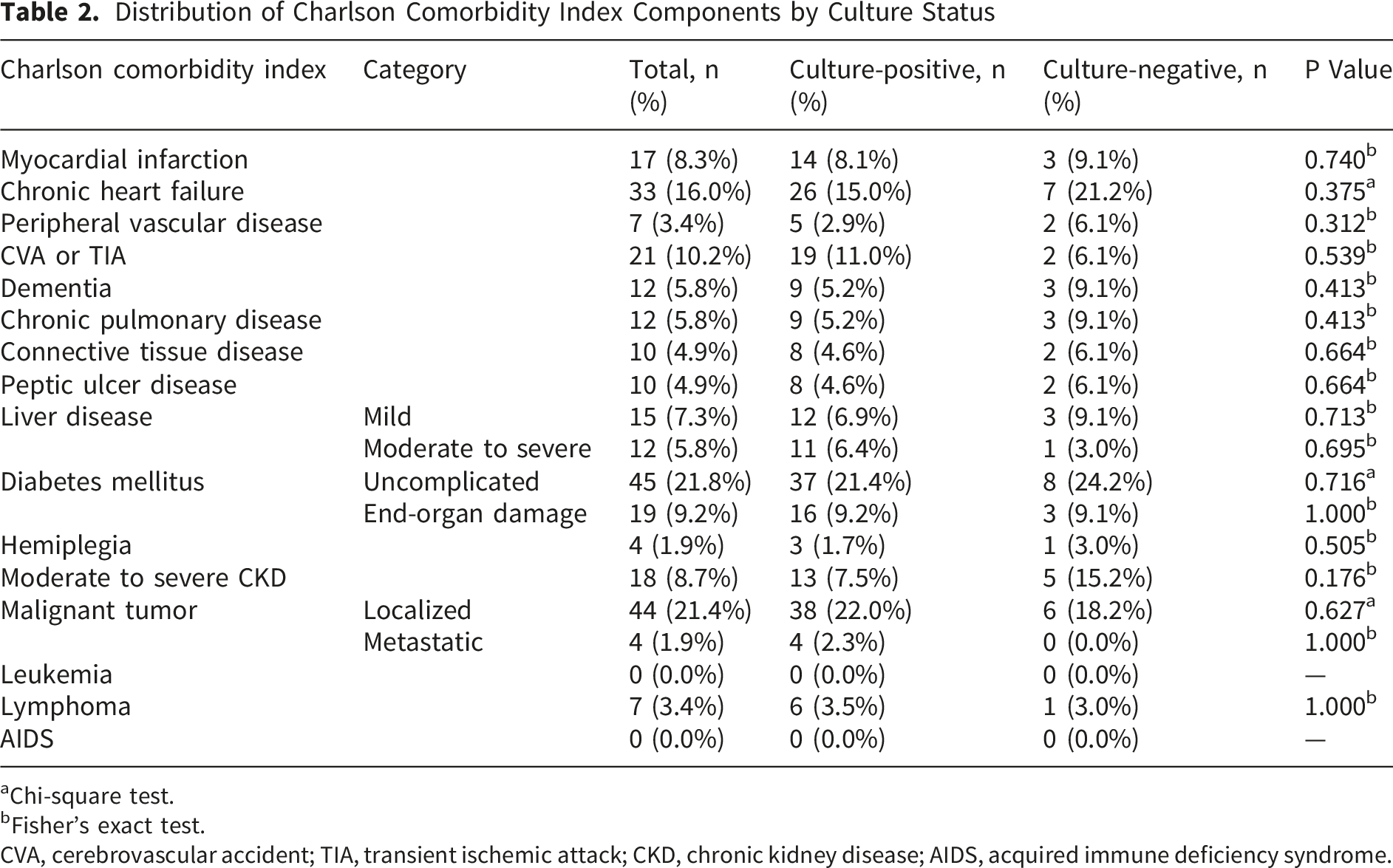
aChi-square test.
bFisher’s exact test.
CVA, cerebrovascular accident; TIA, transient ischemic attack; CKD, chronic kidney disease; AIDS, acquired immune deficiency syndrome.
Differences in Clinical Presentations and Prior Antibiotic Exposure Between Culture-positive and Culture-negative Vertebral Osteomyelitis
Impact of Prior Antibiotic Exposure on Culture Yield of Blood Culture and Biopsy, including Fluoroscopic Disc Biopsy, CT-Guided Drainage, and Intraoperative Specimen
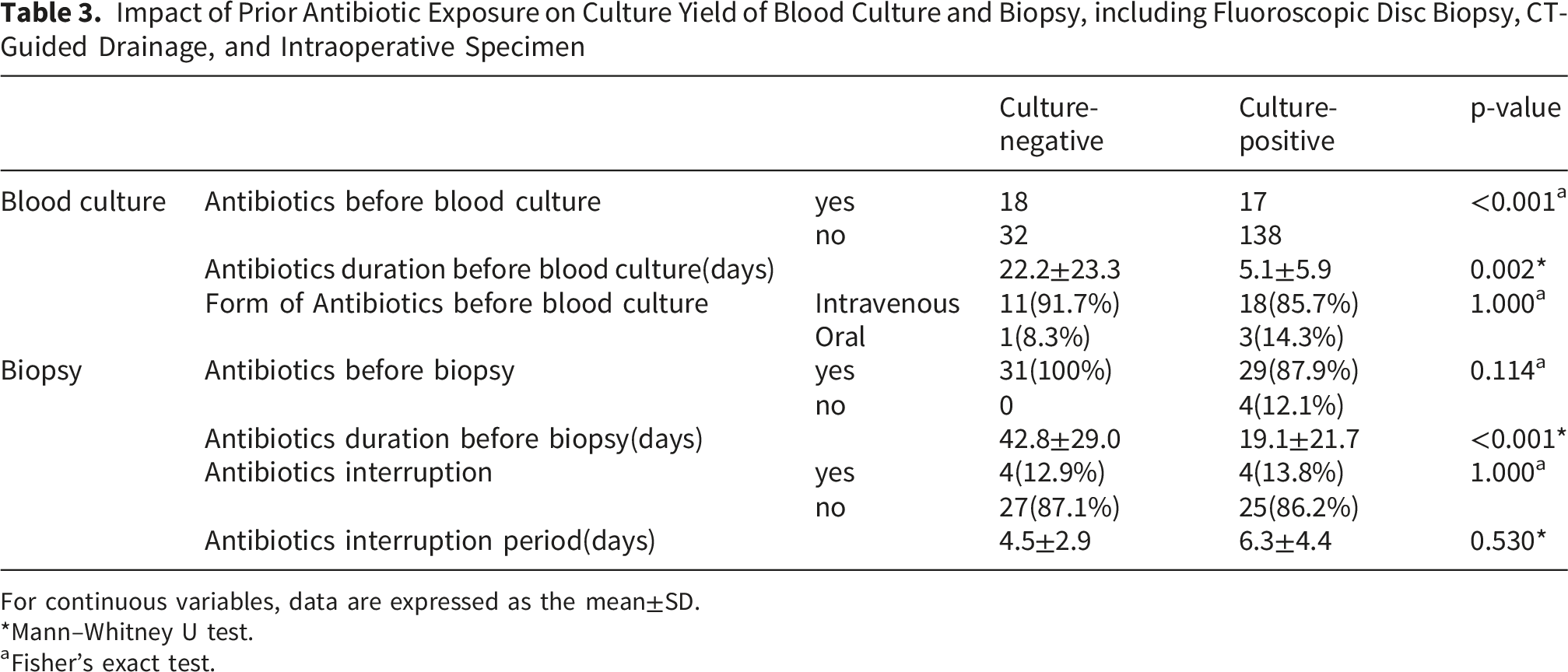
For continuous variables, data are expressed as the mean±SD.
*Mann–Whitney U test.
aFisher’s exact test.
What empirical antimicrobial regimens are routinely used for culture-negative VO in clinical practice, and is the treatment choice associated with prognosis?
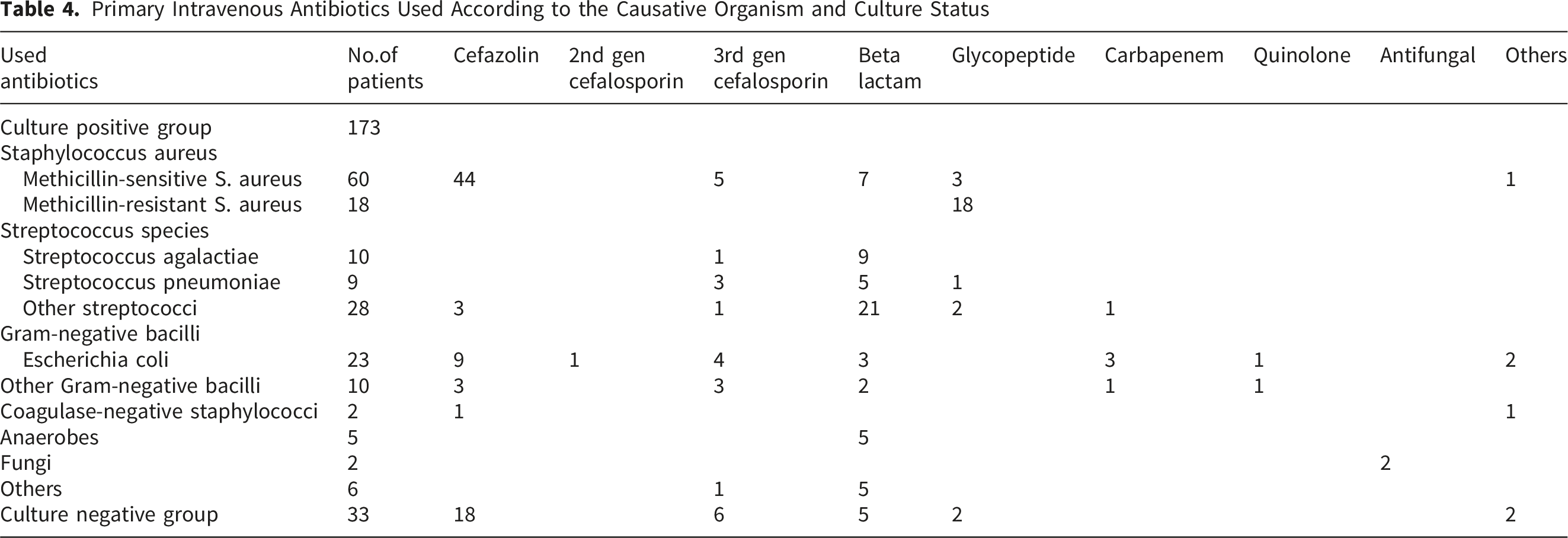
Primary Intravenous Antibiotics Used According to the Causative Organism and Culture Status
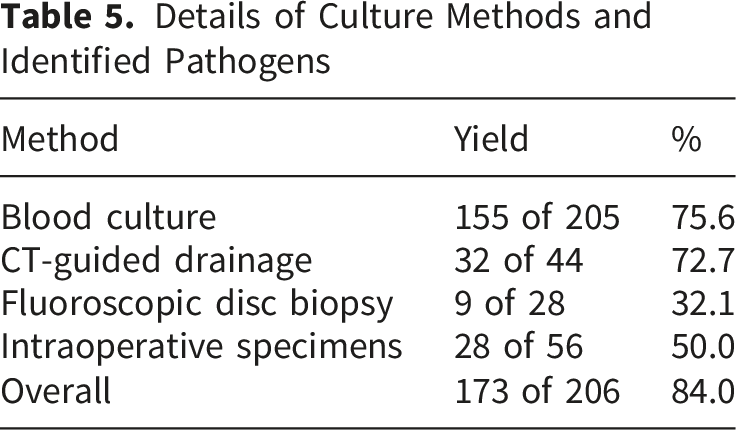
Details of Culture Methods and Identified Pathogens
Clinical Outcomes and Predictors of 1-year Mortality in Culture-positive and Culture-negative VO
Initial Treatment Failure, Recurrence, and 1-Year Mortality According to Culture Status
aChi-square test.
bFisher’s exact test.
Results of Univariate Analysis of Risk Factors for 1-Year All-Cause and Infection-Related Mortality
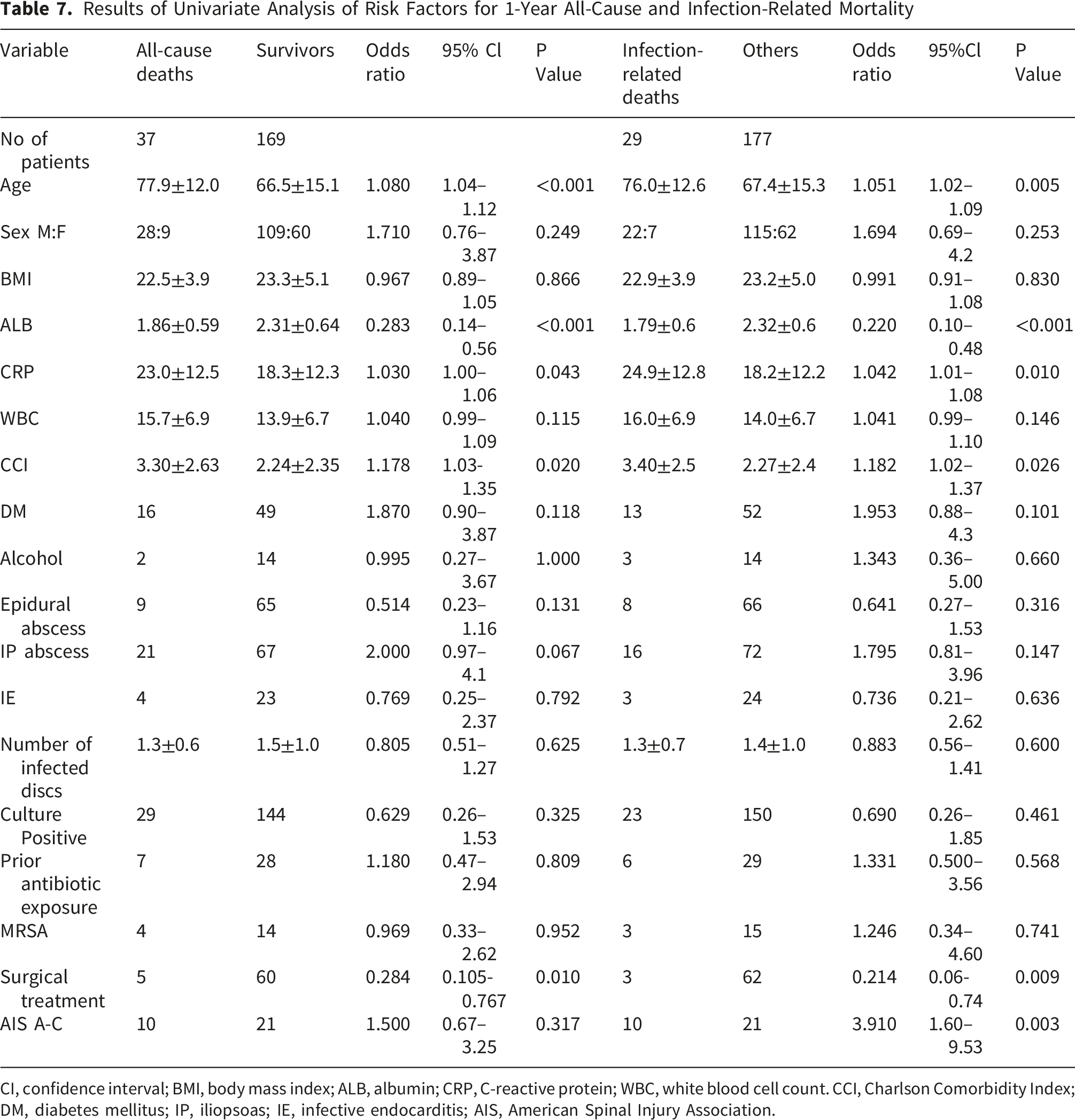
CI, confidence interval; BMI, body mass index; ALB, albumin; CRP, C-reactive protein; WBC, white blood cell count. CCI, Charlson Comorbidity Index; DM, diabetes mellitus; IP, iliopsoas; IE, infective endocarditis; AIS, American Spinal Injury Association.
Results of Multivariate Analysis of Risk Factors for 1-Year All-Cause and Infection-Related Mortality
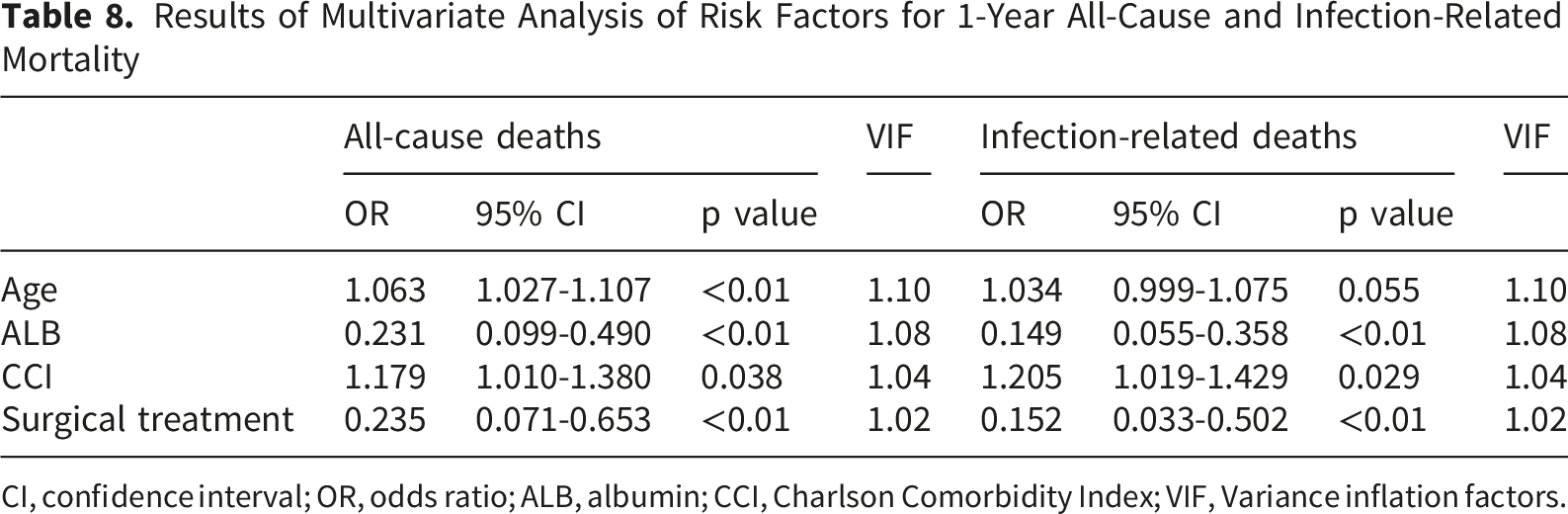
CI, confidence interval; OR, odds ratio; ALB, albumin; CCI, Charlson Comorbidity Index; VIF, Variance inflation factors.
Clinical Characteristics and Outcomes According to Surgical Treatment
Since multivariate analysis identified surgical treatment as an independent factor associated with better survival, baseline characteristics were further compared between surgically and non-surgically treated patients. No significant differences were observed in age, CCI, temperature, CRP, WBC count, albumin, or BMI. By contrast, epidural abscesses and severe neurological impairment were significantly more frequent in the surgically treated group (35/65 vs 39/141, p < 0.001, and 15/65 vs 16/141, p = 0.036, respectively), consistent with the clinical indications for surgery. Of the 65 surgically treated patients, 52 had instrumentation and 13 did not. In the surgically treated subgroup, comparison according to the use of instrumentation showed no significant differences in the duration of intravenous antibiotic therapy, the proportion of patients receiving intravenous therapy for more than 6 weeks, the use of oral suppressive antibiotic therapy, or recurrence risk. The mean duration of intravenous antibiotic therapy was 8.1 ± 4.2 weeks in the instrumentation group and 9.7 ± 4.6 weeks in the non-instrumentation group (p = 0.130). Intravenous therapy for more than 6 weeks was administered in 40 of 52 patients (76.9%) in the instrumentation group and 12 of 13 patients (92.3%) in the non-instrumentation group (p = 0.438). Oral suppressive antibiotic therapy was used in 46 of 52 patients (88.5%) and 13 of 13 patients (100%), respectively (p = 0.335). Recurrence was rare in both groups, occurring in 1 of 52 patients (1.9%) in the instrumentation group and in none of the 13 patients in the non-instrumentation group (0%, p = 1.000).
Discussion
Overall, we found that patients with culture-negative VO had milder inflammatory profiles but similar recurrence and mortality rates, while mortality was driven by age, comorbidity, albumin level, and surgery rather than culture status.
Clinical Significance of Culture-negative Vertebral Osteomyelitis
Several studies have examined the clinical significance of culture-negative VO and reported outcomes comparable to those of microbiologically confirmed diseases.5,7,9,15 Kim et al. found that culture-negative patients presented with lower inflammatory markers and achieved similar outcomes to culture-positive patients when treated with prolonged antimicrobial therapy, 7 while Yu et al. reported no significant differences in mortality or relapse between the two groups. 8 Our results are consistent with these observations; although culture-negative cases in our cohort represented a clinically milder phenotype, their recurrence rate was 0%, and their 1-year mortality was not higher than that of culture-positive patients. These data support the notion that host factors and infection severity are more important determinants of outcomes than culture status alone in cases of VO.
The more favorable inflammatory and radiologic profiles observed in our culture-negative group provide a plausible explanation for the non-inferior outcomes. Culture-negative patients presented with lower fever, CRP, and WBC counts, and higher serum albumin levels, suggesting a lower systemic inflammatory burden, which may also have contributed to relatively preserved serum albumin levels. This interpretation is also consistent with the report by Ghassibi et al., who showed that the responsiveness of routine diagnostic laboratory tests in VO may vary according to the infecting organism, with lower inflammatory marker values observed in culture-negative and other lower-virulence infections than in Staphylococcus aureus or antibiotic-resistant infections. 16 They were also less likely to have an epidural abscess, which is typically associated with a more extensive infection, as well as a higher risk of neurological compromise. 5 Antibiotic exposure prior to culture sampling was more common among culture-negative patients, which may have partially sterilized the bloodstream and reduced the culture yield.3,17,18 Additional analysis showed that antibiotic administration before blood culture was both more frequent and longer in culture-negative cases. Among patients who underwent biopsy, the duration of antecedent antibiotic administration before biopsy was also significantly longer in culture-negative cases, whereas biopsy interruption practices did not differ between groups. The low frequency of antibiotic interruption before biopsy may reflect the fact that, in many cases, microbiological diagnosis had already been established by blood culture and treatment was therefore continued without interruption. These findings suggest that prolonged antecedent antimicrobial exposure, rather than biopsy interruption practice itself, may have contributed to culture-negative results in some patients. Thus, in many culture-negative cases, failure to isolate a pathogen probably reflects a combination of earlier or partial treatment and an intrinsically milder disease, rather than an uncontrolled or atypical infection.
Our culture yield of 84% lies at the upper end of the contemporary VO series.3-5 This finding is consistent with our previous institutional study, in which higher inflammatory activity, lower serum albumin levels, the presence of an epidural abscess, and the absence of previous antibiotic exposure were associated with successful microbiological identification. Conversely, previous antibiotic exposure was the strongest factor associated with failure to identify the causative organism. 17 This interpretation is also supported by the recent study of Naganuma et al., who reported that pre-culture antimicrobial therapy was associated with a significantly lower proportion of positive blood and abscess cultures, although it did not significantly reduce bone culture positivity. 18 Kim et al. also demonstrated that, in patients undergoing needle biopsy, soft tissue specimens, including disc and paraspinal or psoas abscess samples, had a significantly higher microbiological yield than vertebral body specimens. 19 Achieving a microbiological diagnosis has been identified as an important predictor of successful treatment, as it allows for de-escalation from broad-spectrum empirical regimens to organism-directed therapies.4,10,20 In our study, the high culture yield may have facilitated timely targeted treatment in most patients, thus contributing to a low recurrence rate of 1.5%. Under such circumstances, culture status becomes a less dominant determinant of outcomes than host factors and the adequacy of medical and surgical management.
What empirical antimicrobial regimens are routinely used for culture-negative VO in clinical practice, and is the treatment choice associated with prognosis?
The antimicrobial strategy used at our center merits attention. Current guidelines recommend providing empirical regimens that combine anti-staphylococcal coverage, including MRSA, with activity against Gram-negative bacilli, such as vancomycin plus third- or fourth-generation cephalosporins, particularly in patients with severe sepsis or healthcare-associated infections.2,10 In contrast, most culture-negative patients in our cohort were treated empirically with cefazolin-based regimens, without the routine use of glycopeptides, carbapenems, or fluoroquinolones; however, they did not experience higher rates of recurrence or mortality than culture-positive patients. In our cohort, glycopeptide co-administration was used in a small subset of culture-negative patients, indicating that empirical therapy was not uniformly narrow-spectrum when resistant pathogens were a clinical concern. This selective escalation approach is also consistent with a pediatric osteomyelitis cohort in which MRSA-active coverage in culture-negative cases increased during treatment adjustment, although extrapolation to adult vertebral osteomyelitis should be made cautiously. 21 This likely reflects the relatively low prevalence of MRSA and multidrug-resistant Gram-negative bacilli in our setting and the milder profile of culture-negative cases. Our data extend the findings of Kim, Yu, Lee, Dai, and colleagues—who reported similar or non-inferior outcomes in culture-negative compared with culture-positive pyogenic vertebral osteomyelitis—to a setting with high culture yield and predominant use of cefazolin-based empirical therapy.7-9,22 Our findings suggest that cefazolin-based regimens represent a feasible empirical option for culture-negative VO in centers with similar epidemiological conditions and in clinically stable patients without risk factors for resistant organisms. However, these observations are hypothesis-generating rather than conclusive and should be interpreted cautiously, as they may not be generalizable to regions with high rates of MRSA or multidrug-resistant Gram-negative organisms or to settings with substantially different pathogen epidemiologies.
Which factors independently predict 1-year all-cause and infection-related mortality in patients with VO?
Importantly, our analysis indicates that 1-year mortality in VO is primarily driven by host-related factors rather than by culture status. A higher CCI score and hypoalbuminemia emerged as independent predictors of all-cause and infection-related mortality, whereas culture-negative status did not. These findings mirror those of previous studies demonstrating that older age, comorbidity burden, poor general condition, and neurological compromise are major determinants of VO outcomes.1,20,23-25 This is also consistent with the report by Vettivel et al., who found that increasing age was independently associated with 1-year mortality and that epidural abscess and spondylodiscitis were more common in surgically treated patients. 26 An apparent difference between all-cause and infection-related mortality was the role of age. In the multivariable analysis, advanced age remained independently associated with all-cause mortality, whereas for infection-related mortality it showed only a borderline association (OR 1.034, 95% CI 0.999–1.075, p = 0.055). This may reflect the fact that all-cause mortality is influenced not only by infection itself but also by age-related frailty, reduced physiologic reserve, and competing non-infectious causes of death. By contrast, infection-related mortality may be more directly determined by sepsis-related deterioration, comorbidity burden and nutritional status. We further observed that surgical intervention was independently associated with a lower risk of death, thus supporting earlier reports that timely decompression and stabilization can improve infection control and functional outcomes in appropriately selected patients, although a selection bias cannot be excluded.10,23,27,28 In the subgroup analysis of surgically treated patients, the presence of instrumentation was not associated with a longer intravenous antibiotic course, more frequent oral suppressive therapy, or a higher recurrence rate. These findings suggest that, in this cohort, surgical instrumentation itself did not clearly increase the risk of recurrence or mandate prolonged antimicrobial treatment. Recent systematic reviews have indicated that early surgery yields better overall clinical and neurological outcomes than conservative treatment in many patients with pyogenic spondylodiscitis. 29 In our cohort, surgical indications were determined primarily based on neurological impairment and structural factors, such as spinal instability or deformity, rather than age or general condition alone. Comparison between the surgically and non-surgically treated groups showed no significant differences in age, CCI, or systemic inflammatory markers. Conversely, epidural abscesses and severe neurological impairment were significantly more frequent in the surgically treated group, consistent with the established indications for operative management. Accordingly, these findings should not be interpreted as evidence of surgical superiority; rather, they suggest that surgical intervention may have contributed to improved outcomes in appropriately selected patients, although residual selection bias cannot be excluded.
Practical Approach in Suspected Culture-negative VO
Based on these findings, the following practical approach may help guide clinical decision-making in suspected culture-negative VO. 1. Obtain blood cultures before antibiotics whenever feasible. Pursue microbiological sampling when indicated, including image-guided biopsy, CT-guided drainage, or aspiration of the disc space or a vertebral body abscess. 2. In patients with sepsis, severe pain, neurological impairment, or structural instability, the risks of delaying treatment for an antibiotic holiday should be carefully weighed against the potential benefit of improving culture yield. 3. If blood cultures yielded negative results and the patient is systemically well, not in severe pain, and neurologically intact, further microbiological sampling should be pursued whenever feasible. A short antibiotic holiday before biopsy or drainage may be considered on an individual basis. 4. If no organism is identified, empirical therapy should be selected according to local epidemiology, disease severity, host factors, and the most likely pathogens, rather than using a single uniform regimen. 5. Clinical response should be reassessed continuously. Surgery should be considered when neurological deterioration, instability, deformity, or poor response to antimicrobial therapy is present.
Limitations
This study had several limitations. First, its retrospective, single-center design may have introduced selection and information biases; therefore, our findings may not be generalizable to settings with different pathogen distributions or antimicrobial resistance patterns. Second, antimicrobial regimens, treatment duration, and surgical indications were not fully standardized and were determined by the treating physicians. Although this approach reflects real-world practice, it may have introduced treatment-selection bias. The number of culture-negative cases was relatively small, thus limiting the statistical power to detect modest differences between the culture-positive and culture-negative groups. Third, molecular diagnostic techniques, such as broad-range PCR or metagenomic sequencing, are not routinely used and might have further increased the microbiological yield in culture-negative VO.3,5 In addition, no patients in this cohort had documented intravenous drug use. Although this likely reflects the characteristics of the local patient population, it may limit the generalizability of our findings to patients with vertebral osteomyelitis associated with intravenous drug use, which may differ in microbiology and clinical course. Prospective multicenter studies with standardized treatment algorithms and contemporary microbiological methods are required to refine empirical strategies for culture-negative disease and to clarify the relative contributions of microbiological, host-related, and surgical factors to prognosis.
Conclusion
Culture-negative cases (16%) presented with milder inflammation, higher serum ALB levels, and fewer epidural abscesses than those in culture-positive cases; however, infection recurrence was rare, and 1-year mortality did not differ according to culture status. Advanced age, greater comorbidity burden, hypoalbuminemia, and absence of surgical intervention were all identified independent predictors of mortality, whereas culture negativity was not. In a setting with a low prevalence of multidrug-resistant organisms, our findings support the feasibility of cefazolin-based empirical therapy for clinically stable culture-negative vertebral osteomyelitis and indicate that prognosis is determined primarily by host factors and the adequacy of surgical and medical management, rather than by culture status alone. These results will help inform other clinicians regarding the optimal treatment strategies for culture-negative VO.
Footnotes
Acknowledgments
The authors thank Editage for English language editing and proofreading.
Ethical Considerations
Approval for this study was received from the Ethics Committee of Kobe City Medical Center General Hospital (Approval Date: Dec 14, 2023; Approval Number: zn231213).
Consent to Participate
The need for informed consent was waived owing to the retrospective study design.
Author Contributions
D.S., E.O., and Y.S. designed the study, collected and analyzed the data, and drafted the manuscript. M.K. and M.T. collected the data. T.Y. supervised the study. All authors have read and approved the submitted version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Device Status/Drug Statement
The device in this manuscript is FDA-approved or approved by a corresponding national agency for this indication.