
Abstract
Study design
Systematic review and meta-analysis of randomized controlled trials and cohort studies directly comparing full-endoscopic posterior cervical decompression (PECD) with anterior cervical discectomy and fusion (ACDF) in adults with degenerative cervical disease.
Objective
To compare full-endoscopic posterior cervical decompression with anterior cervical discectomy and fusion for degenerative cervical disease.
Methods
PubMed, Embase, and CENTRAL were searched through September 2025 for randomized and cohort studies in adults with ≥ 6 months’ follow-up directly comparing PECD and ACDF. NDI, VAS neck/arm pain in short-term and long-term follow up, C2–C7 Cobb angle, peri-operative metrics, and adverse events were pooled using random-effects models with 95% confidence intervals.
Results
Ten studies (2 RCTs, 8 cohorts) comprising 862 patients (PECD 433; ACDF 429) with 6 months to 2.5 years of follow-up were included. NDI and VAS arm pain scores did not differ significantly at final follow-up. PECD showed greater short-term functional improvement (NDI MD 2.46, 95% CI 1.55–3.36), whereas ACDF achieved slightly greater long-term neck pain improvement (VAS neck MD −0.24, 95% CI −0.43 to −0.04). C2–C7 Cobb angle and operative time did not differ. PECD was associated with a shorter hospital stay (MD −1.64 days, 95% CI −2.31 to −0.97) and lower blood loss (MD −44.85 mL, 95% CI −79.8 to −9.89), though these perioperative outcomes demonstrated substantial heterogeneity. Additionally, PECD was associated with a significantly lower risk of postoperative complications (RR 0.53, 95% CI 0.34–0.81); whereas ASD and index-level re-operation rate did not differ.
Conclusions
PECD provides comparable mid-term disability and arm pain relief to ACDF with faster early recovery and lower perioperative morbidity, while ACDF offers marginally better long-term axial neck pain improvement.
Keywords
1. Introduction
Cervical degenerative disc disease (CDDD) is a prevalent cause of neck and arm pain in adults, with an annual incidence of approximately 85 per 100,000 individuals.1-3 For patients refractory to conservative management, surgical decompression is indicated.4 Anterior cervical discectomy and fusion (ACDF) has long been regarded as the recommended procedure, providing reliable nerve cord decompression and lordosis correction.5 However, its possible complications, including dysphagia, recurrent laryngeal nerve palsy, implant-misplacement, and accelerated adjacent segment degeneration (ASD), remain clinically significant.6-12 To avoid these fusion-related issues, posterior cervical decompression (PCD) including posterior cervical foraminotomy (PCF) and segmental laminectomy was developed as an alternative strategy.13,14 Although PCD yields comparable outcomes to ACDF in terms of radicular pain and neurological recovery, 15 PCD often requires extensive muscle dissection and partial facet resection. This can predispose to postoperative neck pain, segmental instability, and cervical kyphosis when more than 50% of the facet is removed.16-18 These biomechanical and anatomical concerns have driven the evolution toward less invasive, muscle-preserving posterior techniques.
In 2006, Ruetten et al first described a posterior endoscopic cervical decompression (PECD) technique, demonstrating its technical feasibility and safety in the treatment of cervical disc herniations.19,20 Subsequent investigations have emphasized the biomechanical advantages of PECD. The endoscopic approach allows precise decompression with higher facet joint preservation, thereby minimizing the risk of instability and postoperative kyphosis.21,22 Radiographic analyses have demonstrated that endoscopic decompression maintains cervical lordosis more effectively compared to traditional PCD. 23 Additionally, PECD minimizes paraspinal muscle injury by avoiding extensive detachment, leading to less postoperative neck pain, reduced blood loss, and shorter hospitalization.24,25 Collectively, by maintaining integrity of facet and related musculature, PECD may inherently reduce the risk of postoperative cervical kyphosis and chronic axial pain.
To our knowledge, this is among the first meta-analyses restricted to full-endoscopic posterior cervical decompression (PECD) that pre-specified and compared short-term functional endpoints with anterior cervical discectomy and fusion (ACDF). Despite growing clinical adoption, consolidated comparative evidence remains limited. Most prior syntheses examined open PCD or pooled posterior techniques24,26 and, in many cases, were single-arm meta-analyses without time-stratified early outcomes.27,28 To address this gap, we conducted the first pairwise meta-analysis directly comparing PECD and ACDF for cervical radiculopathy, with pre-specified short-term and longer-term endpoints. The present results clarify the relative efficacy and safety of these approaches and inform evidence-based decision-making in cervical spine surgery.
2. Materials and Methods
2.1. Study Registration
This systematic review and meta-analysis was conducted according to a pre-specified protocol registered in PROSPERO (CRD420261279853) and is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 29
2.2. Eligibility Criteria
2.2.1. Inclusion criteria
(1) Randomized controlled trials (RCTs) or cohort study comparing posterior endoscopic cervical decompression (PECD) with anterior cervical discectomy and fusion (ACDF) in adults with degenerative cervical disease presenting with radiculopathy or myelopathy, (2) Articles written exclusively in English, (3) Minimum follow-up of 6 months with clinical and radiographic assessment, (4) Reporting at least one prespecified outcome of interest.
2.2.2. Exclusion criteria
(1)Studies involving surgery at more than two cervical levels, (2)Duplicate or overlapping reports of the same cohort. When multiple reports described the same cohort, we included only the publication with the longest available follow-up to avoid double counting and reduce bias.
2.3. Information Sources and Search Strategy
A systematic search was conducted in PubMed, Embase, and CENTRAL (Cochrane Central Register of Controlled Trials) from database inception to September 2025, without time restrictions. Searches were limited to English language publications. The strategy combined controlled vocabulary and free-text terms, including “PECF,” “endoscopic foraminotomy,” “endoscopic cervical foraminotomy,” “endoscopic cervical laminectomy,” “endoscopic posterior cervical foraminotomy,” “posterior cervical decompression,” “posterior endoscopic cervical decompression,” “PECD,” “ACDF,” “anterior cervical discectomy and fusion.” Additional manual searches through cited references were performed.
2.4. Appropriate Outcome Measures
Eligible studies had to report at least one prespecified outcome, which was categorized as clinical, radiographic, perioperative or adverse events.
Clinical outcomes were the Neck Disability Index (NDI)30,31 and Visual Analog Scale (VAS) scores (separate neck and arm pain scores were extracted when available).32,33 For clinical outcomes, data were further stratified into short-term (≤3 months of follow-up) and long-term (≥12 months of follow-up) results. Radiographic outcome was C2 to C7 cobb angle (CA). Perioperative outcomes included operation time (OP time), blood loss (BL) and length of hospital stay (LOH). Adverse events included postoperative complication, adjacent segment degeneration (ASD) and reoperation at the index level.
2.5. Selection Process
All records were imported into Endnote for sorting and removal of duplicates. Two reviewers independently screened titles and abstracts for eligibility, followed by full-text review of potentially relevant studies. Disagreements were resolved by discussion, and unresolved conflicts were adjudicated by a third reviewer.
2.6. Data Collection Process
Data were independently extracted in duplicate using a standardized form. Extracted variables included study design, sample size, demographics, type of surgical intervention, levels, follow-up duration, and all prespecified outcomes. When dispersion measures were missing but ranges were reported, we estimated SDs from the minimum–maximum and sample size using established formulas.34,35 If results were only presented as figures, we digitized the data with WebPlotDigitizer 36 in duplicate and reconciled discrepancies. Units were harmonized a priori (e.g., VAS to 0–10, NDI to 0–50, time in minutes).
2.7. Risk of Bias Assessment
Risk of bias for randomized controlled trials was assessed using the Cochrane RoB 2.0 tool, while non-randomized cohort studies were evaluated using the ROBINS-I tool. Two reviewers independently assessed the risk of bias of included studies.
2.8. Statistical Analysis
A meta-analysis was conducted to compare posterior endoscopic cervical decompression (PECD) and anterior cervical discectomy and fusion (ACDF). Continuous outcomes measured on the same scale or after unit harmonization were synthesized as mean differences (MDs). When outcomes were assessed with different instruments or scales, we pooled standardized mean differences (SMDs) using Hedges’ g correction. All effect estimates are reported with 95% confidence intervals (CIs). For binary outcomes, effect sizes were expressed as relative risks (RRs) with 95% CIs. All analyses were conducted under a random-effects model using the meta package in R (version 2025.09.1+401). Forest plots were generated to summarize pairwise treatment effects with corresponding 95% CIs. All analyses followed a pre-specified protocol registered in PROSPERO. Statistical heterogeneity was quantified using the I2 statistic. Where appropriate, sensitivity analyses were conducted by excluding studies at high risk of bias. The pooled estimates and their uncertainty were compared with the primary analysis to assess robustness. Each included study was assigned a level of evidence according to the North American Spine Society (NASS) classification system. 37
2.9. Certainty of Evidence
The certainty of evidence for each outcome was assessed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework, and the overall certainty of evidence was classified as high, moderate, low, or very low according to the GRADE guidelines. 38
3. Result
3.1. Search Results and Study Characteristics
A total of 2820 records were identified through database searching (PubMed: 1350; Embase: 1358; Cochrane library: 112). After removing 1145 duplicates, 1675 records were screened by title and abstract. Of these, 136 full-text articles were assessed for eligibility, and 10 studies were ultimately included for quantitative synthesis39-48 (Figure 1). PRISMA 2020 flow diagram summarizing the study selection process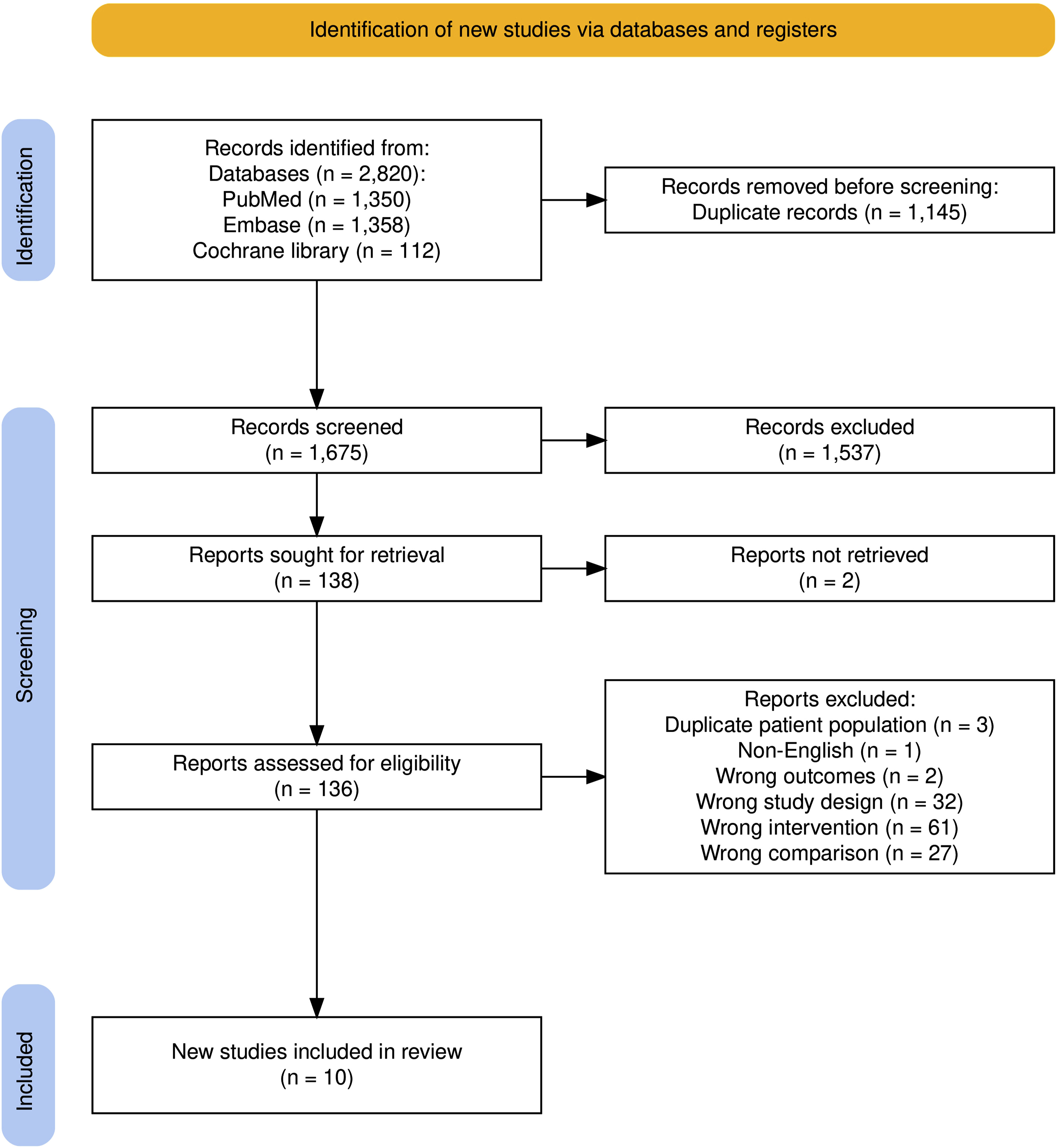
Studies Characteristics
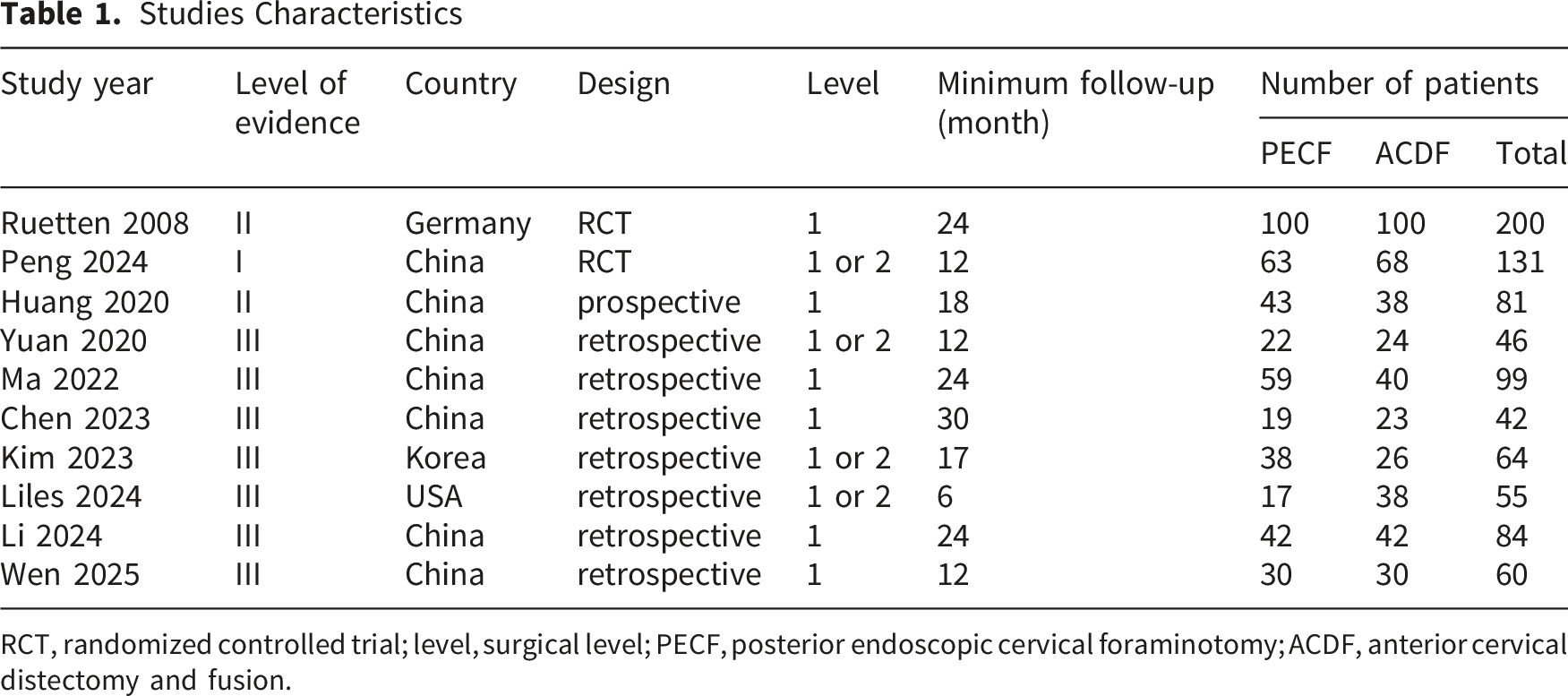
RCT, randomized controlled trial; level, surgical level; PECF, posterior endoscopic cervical foraminotomy; ACDF, anterior cervical distectomy and fusion.
3.2. Risk of Bias
Risk-of-bias assessment indicated that 6 studies had some concerns, and 4 were at high risk (Figure 2). Bias among the included studies was primarily attributed to the lack of randomization and blinding of patients and providers as many of the studies included were nonrandomized cohort studies. Further, three demonstrated differences in baseline age across the study populations among the included studies. Risk-of-bias plot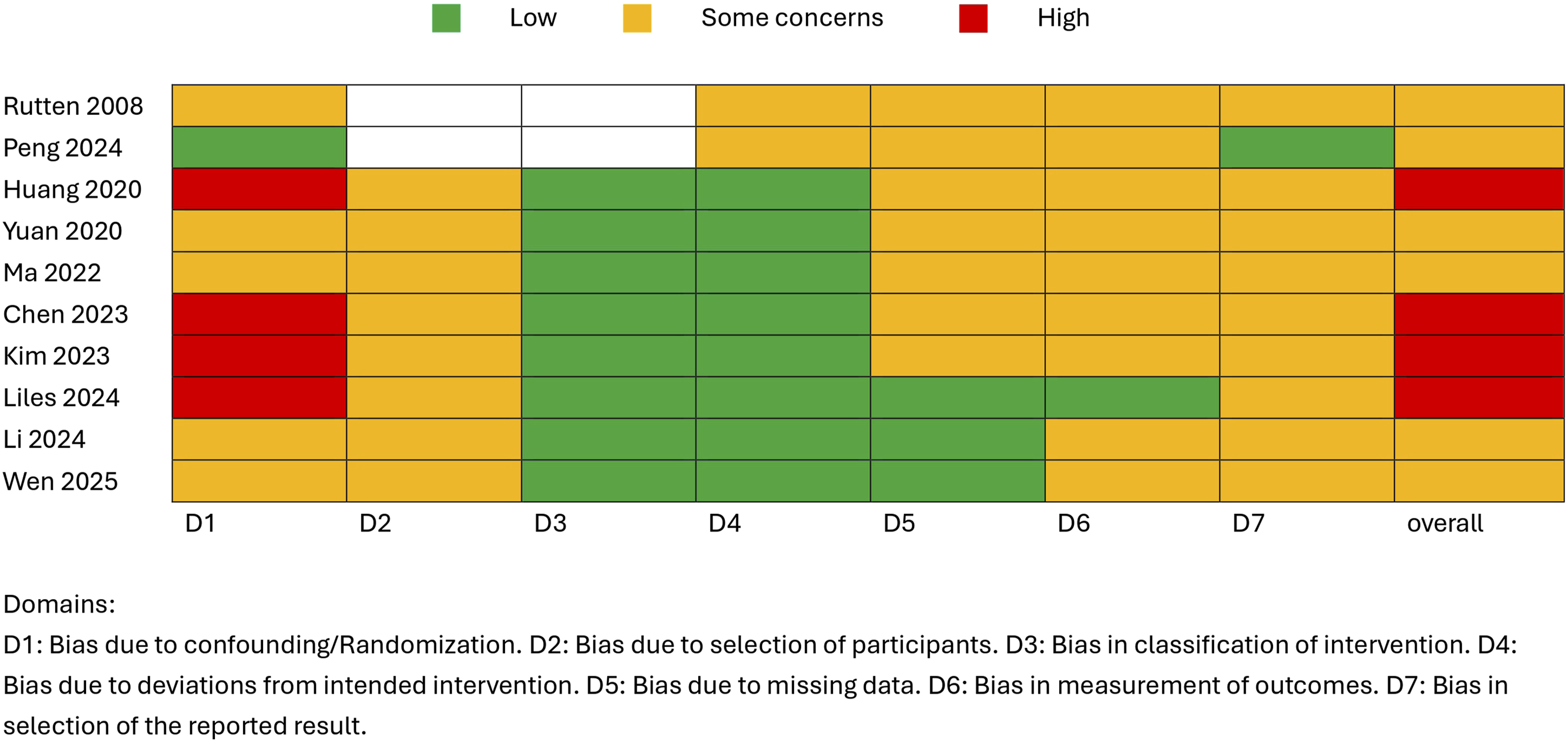
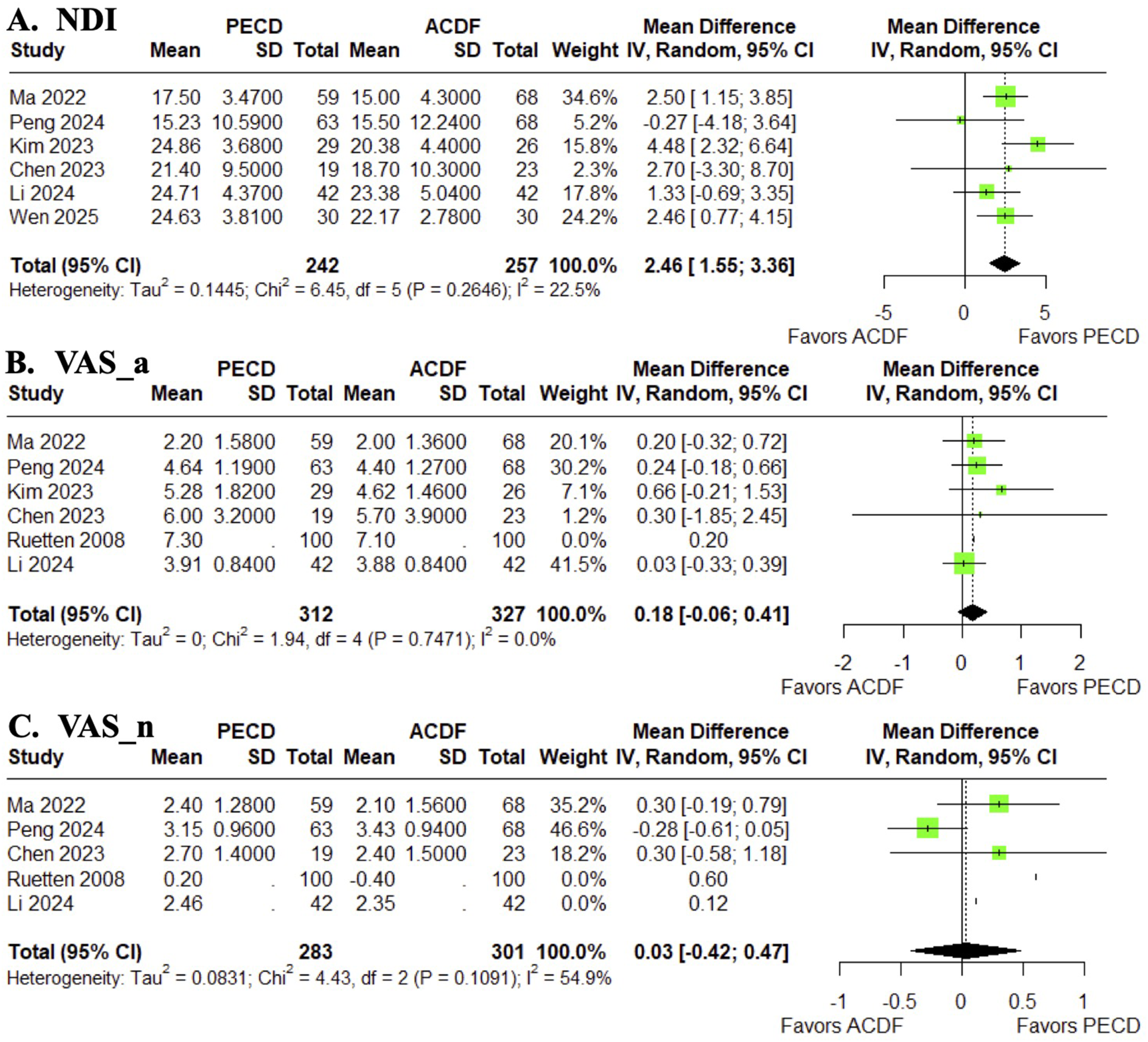
3.3. Clinical Outcomes
Although no significant difference in long-term NDI was observed between PECD and ACDF at final follow-up (Figure 3A), PECD showed a statistically greater improvement in short-term outcomes compared with ACDF (MD: Forrest plot of long-term clinical outcomes. (A) Neck disability index; (B) visual analog scale of arm pain; (C) visual analog scale of neck pain, ACDF showed significantly greater improvement than PECD at the final follow-up Forrest plot of short-term clinical outcomes. (A) Neck disability index, PECD showed a statistically greater improvement in short-term outcomes compared with ACDF; (B) visual analog scale of arm pain; (C) visual analog scale of neck pain
3.4. Radiographic Outcome
For the cobb angle measured from C2 to C7, no significant differences were observed between the two groups at the final follow-up (Figure 5). Forrest plot of C2-C7 cobb angle at the final follow-up. No significant differences were observed between the two groups at the final follow-up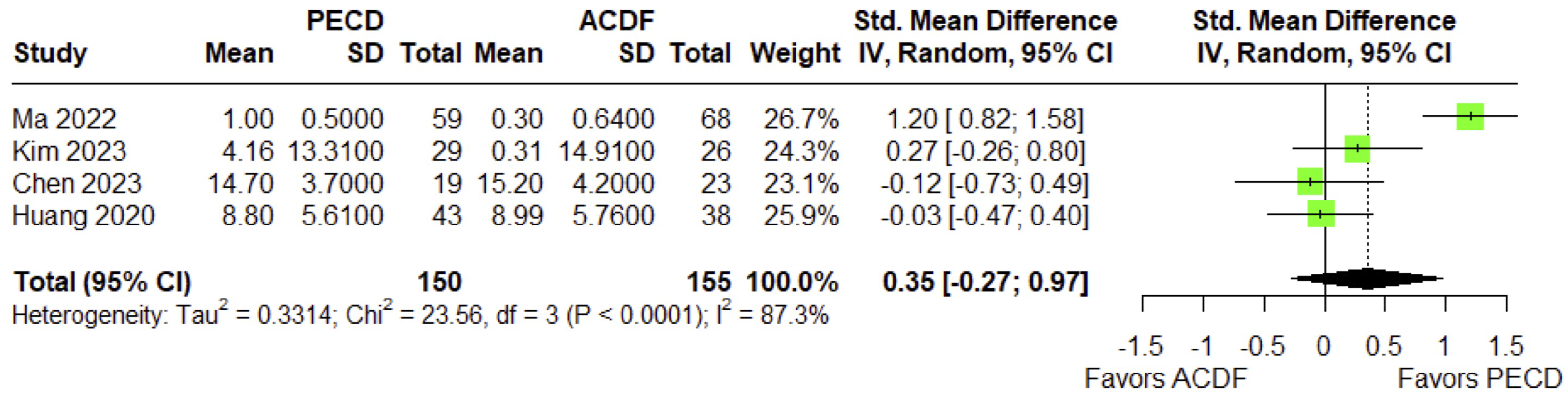
3.5. Perioperative Outcomes
PECD was associated with a shorter length of hospital stay compared with ACDF (MD: Forrest plot of perioperative outcomes. (A) Length of hospital stay, PECD was associated with a shorter length of hospital stay compared with ACDF; (B) operative time; (C) intra-operative blood loss, PECD was associated with lesser intraoperative blood loss compared with ACDF
3.6. Adverse Events
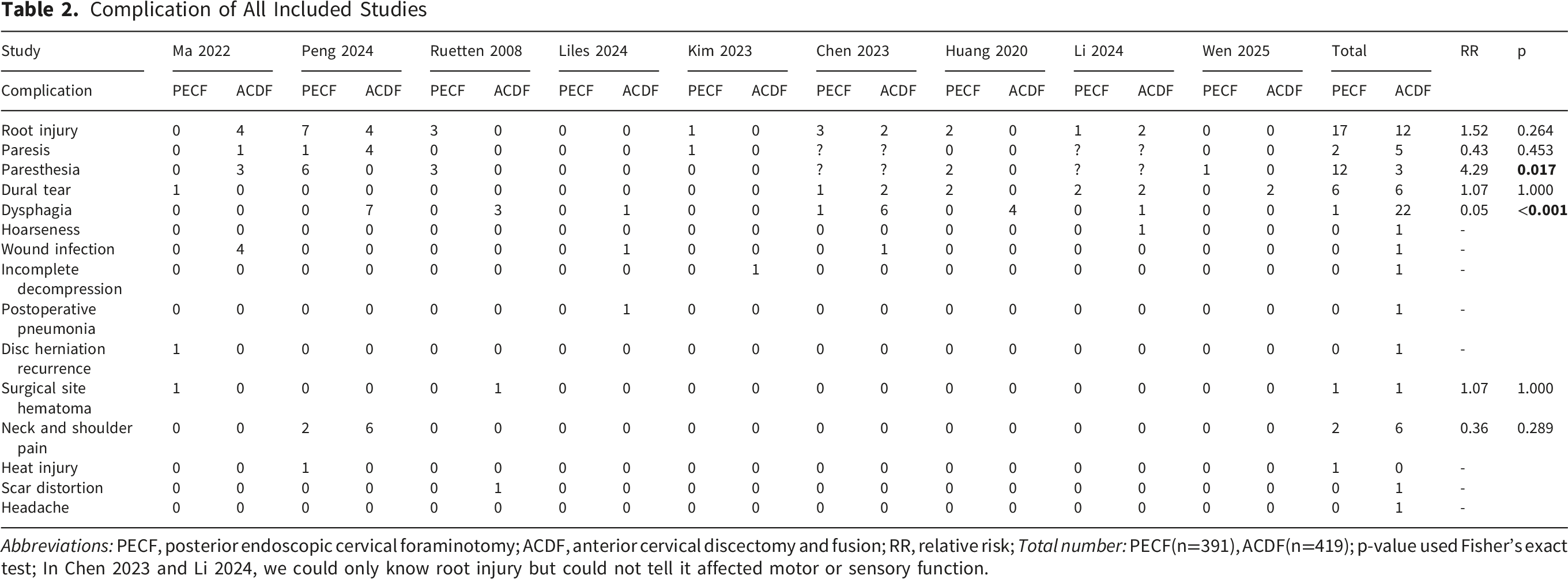
For postoperative complications, PECD showed a significantly lower incidence than ACDF after surgery (RR: Forrest plot of adverse events. (A) Ppostoperative complications, PECD showed a significantly lower incidence than ACDF after surgery; (B) adjacent segment degeneration;, (C) reoperation at the index level Complication of All Included Studies Abbreviations: PECF, posterior endoscopic cervical foraminotomy; ACDF, anterior cervical discectomy and fusion; RR, relative risk; Total number: PECF(n=391), ACDF(n=419); p-value used Fisher’s exact test; In Chen 2023 and Li 2024, we could only know root injury but could not tell it affected motor or sensory function.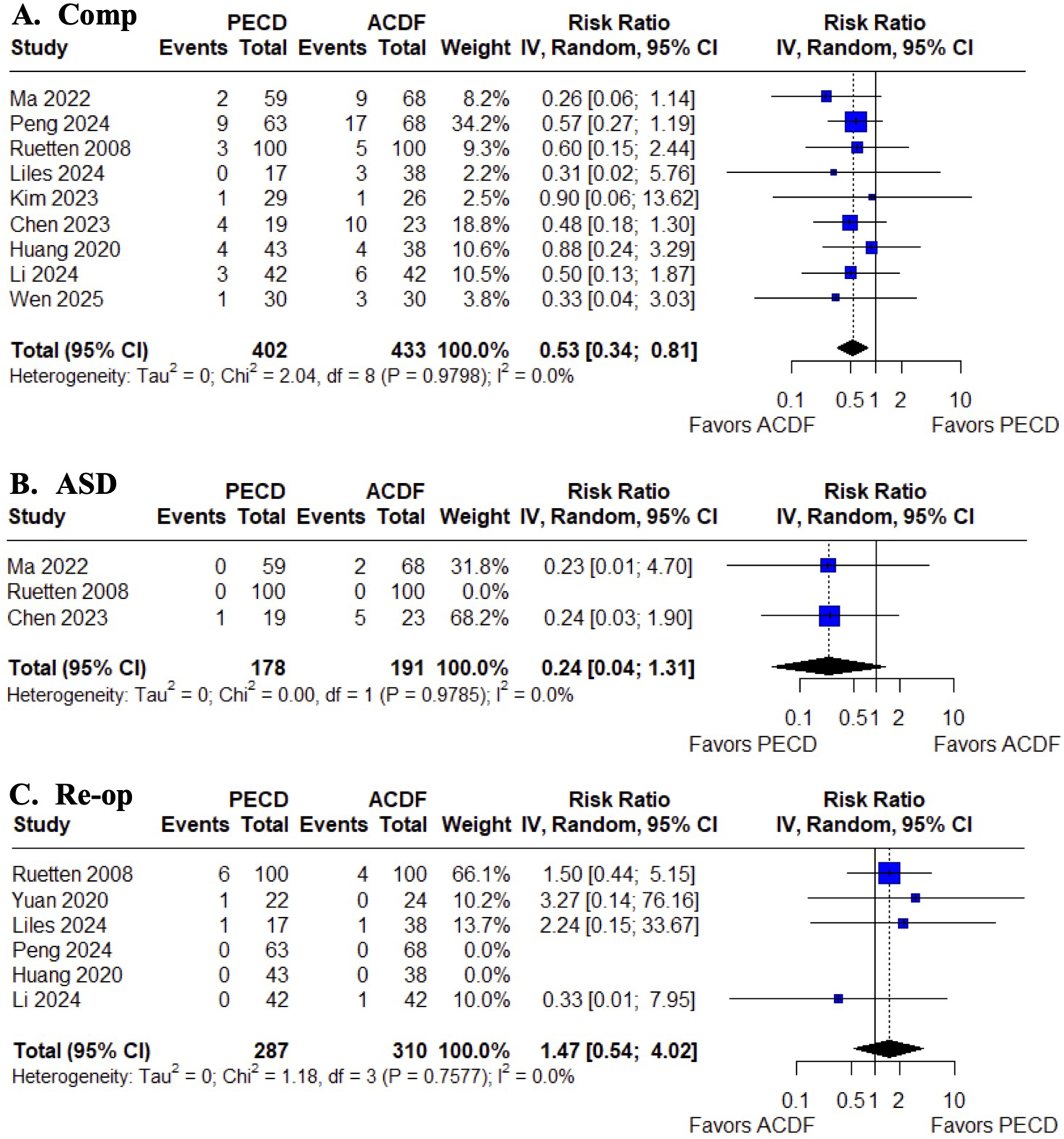
3.7. Subgroup and Sensitivity Analyses
Because Kim et al reported dispersion converted from the range, we performed a sensitivity analysis excluding this study. After exclusion of Kim et al, the pooled effect estimates remained directionally consistent, and their statistical significance was unchanged (Supplemental Figs. S1-S4). Given that some outcome data for Huang et al and Wen et al were obtained by digitizing published graphs (WebPlotDigitizer), we conducted a sensitivity analysis excluding this study. The direction of the pooled effects remained consistent following exclusion (Supplemental Figs. S1, 3, 5). Because Ruetten et al reported dispersion converted from the range, we performed a sensitivity analysis excluding this study and this interpretation was unchanged in sensitivity analysis (Supplemental Fig. S6).
3.8. Certainty of Evidence
Across the 12 prespecified outcomes, certainty ranged from very low to moderate. Seven outcomes achieved moderate certainty (long- and short-term clinical outcomes, C2–C7 Cobb angle). Length of hospital stay was low, and three outcomes were very low (operative time, adjacent segment degeneration, reoperation at the index-level). Downgrading was driven primarily by risk of bias (nonrandomized designs, lack of blinding), serious inconsistency (notably for operative time and length of stay), and imprecision for rare-event outcomes. Indirectness and publication bias were not judged serious. Detailed domain-level assessments and reasons for downgrading are provided in Supplemental Table S1.
4. Discussion
In this pairwise meta-analysis comparing PECD and ACDF, we found that both techniques achieve equivalent long-term outcomes in degenerative cervical diseases. Overall, functional improvement (NDI) and pain relief at arm (VAS) at final follow-up did not differ significantly. The long-term VAS in neck pain is lower in ACDF, indicating greater improvement in axial neck pain with fusion. However, PECD was associated with a faster early recovery, demonstrating significantly greater short-term improvement in NDI and a shorter hospital stay than ACDF, though the latter endpoint should be interpreted with caution due to substantial heterogeneity. The significantly shorter hospital stay with PECD (often allowing for ambulatory surgery) highlights its minimally invasive nature. Furthermore, PECD results in nearly half of the overall complication rate of ACDF, with no significant differences in reoperation rates, adjacent segment degeneration (ASD), operation time or radiographic cervical alignment observed between the two approaches.
Our results reinforce the growing evidence of which motion-preserving posterior decompression is as effective as ACDF in treating unilateral cervical radiculopathy or myelopathy.27,28,49-51 With lesser invasion, the PECD approach can attain equivalent symptomatic relief. Similarly, Gutman et al 52 likewise concluded that all three modern techniques (ACDF, cervical disc arthroplasty, and minimally invasive posterior cervical foraminectomy) achieve significant symptom improvements, with the posterior decompression yielding the lowest incidence of adverse events. The outcome differences identified in our meta-analysis closely reflect these theoretical advantages of PECD. Patients in the PECD group experienced superior early postoperative functional improvement, which is likely attributable to reduced muscle pain and soft tissue disruption. 53 Our pooled analysis showing a small but significant long-term advantage in VAS-neck with ACDF is biologically plausible. Fusion of spine vertebrae eliminates not only segmental motion and discogenic pain, but also improves sagittal alignment,54-56 both of which have been correlated with axial pain relief. On the other hand, posterior decompression, despite being muscle-sparing, can provoke posterior muscle or facet–related neck discomfort.57-60
Notably, we found no overall difference in operative duration between PECD and ACDF. Two pragmatic considerations may nevertheless explain case-level variability. First, in single-level disease, ACDF typically entails anterior exposure, disc-space preparation, graft selection, and plating steps that can prolong preparation time. By contrast, PECD requires a limited posterior corridor and may be finished sooner. Second, in multilevel pathology, PECD necessitates separate keyhole decompressions with repeated localization and docking at each level, which can offset the efficiency advantages compared to one single anterior exposure for multilevel management in ACDF. These mechanisms are only hypothetic interpretations and partly concordant with our subgroup results. Variability in how operative time was defined (skin-to-skin vs anesthesia time or inclusion of positioning and fluoroscopic localization) and unadjusted learning-curve effects likely contributed to imprecision. 61 We proposed that an universal definition of operation time, such as the adaptation of scope recording time, could provide better comparison results for future studies.
The learning curve of PECD should be considered when interpreting the present findings. Because the included studies span from 2008 to 2025, differences in surgeon experience may have affected perioperative outcomes, particularly operative time and complication profiles, and may partly explain the heterogeneity observed among studies. Compared with ACDF, PECD requires familiarity with endoscopic anatomy, working-channel orientation, neural decompression, and bleeding control. During the early learning phase, longer operative times, incomplete decompression, residual disc fragments, epidural bleeding, and transient neural irritation have been reported more frequently than after proficiency is achieved.62-65 Several studies have shown that surgical efficiency improves with increasing case experience. Koh et al. 64 reported that the learning curve for endoscopic lumbar discectomy is overcome after approximately 20 cases, mastery may require nearly 60 cases. In cervical endoscopy, Sun et al. 65 found substantial improvement in operative efficiency after 20–25 PECD cases, whereas Kang et al. 63 reported that approximately 20 cases were required to achieve 90% procedural proficiency in biportal endoscopic posterior cervical foraminotomy. Importantly, unlike many early lumbar endoscopic studies involving surgeons without prior endoscopic experience, many reported learning-curve studies of endoscopic cervical surgery have been conducted by surgeons already familiar with endoscopic spinal techniques. Therefore, the frequently cited threshold of 20–30 cases may not fully represent the learning process for surgeons transitioning directly from conventional ACDF practice. This should be considered when interpreting the favorable outcomes reported in the present meta-analysis, as these results may largely reflect the performance of experienced endoscopic surgeons. While complication and failure rates generally decrease with experience, careful case selection, mentorship, and structured training remain important during the early adoption phase. With the growing role of endoscopic techniques in contemporary spine surgery, continued development of standardized training programs may help facilitate broader implementation while maintaining patient safety. 66
Full-endoscopic cervical decompression (PECD) arose to address the limitations of both ACDF and traditional open PCD. While ACDF remains a workhorse for cervical degenerative disc disease, it carries well-recognized risks, including dysphagia, recurrent laryngeal nerve palsy, implant-related events, and motion-related adjacent segment degeneration.
67
Open posterior keyhole decompression preserves motion but relies on broader paraspinal muscle detachment and partial facetectomy or laminectomy, which can increase muscle morbidity and, when excessive, iatrogenic instability.16,51,52,68-70 Modern endoscopic techniques were designed to retain the motion-sparing advantages of PCD while minimizing soft-tissue trauma and maximizing facet preservation through precise and targeted decompression.
71
Consistent with this rationale, our meta-analysis showed a substantially lower postoperative complication risk with PECD (RR=
A key question in adopting PECD is whether avoiding fusion might sacrifice long-term stability or lead to higher recurrence rates. Our analysis provides encouraging evidence on this front. We detected no significant difference in the final alignment of cervical vertebra between PECD and ACDF patients, indicating that the motion-preserving procedure did not result in postoperative segmental kyphosis or loss of lordosis compared to fusion. This finding is noteworthy because it counters the historical concern that a posterior decompression (especially if aggressive) could induce spinal alignment changes.17,72,73 Biomechanical studies have shown that removal of more than half of the facet joint can destabilize the motion segment,18,74 but the endoscopic technique allows more targeted decompression with minimal bony resection. Our results support the notion that PECD maintains cervical stability consistent with prior radiographic analyses demonstrating preserved or improved lordosis after endoscopic decompression.23,75,76 In terms of durability, we found no statistical difference in reoperation rates at the index level between PECD and ACDF. This suggests that, within the available follow-up, the need for subsequent surgical intervention is comparable for the two approaches. Notably, earlier studies have reported mixed signals on reoperation. Fang et al observed a higher reoperation rate following PCD in a large meta-analysis, 49 whereas Guo et al reported similarly low reoperation frequencies for both ACDF and endoscopic groups. 27 In our study, the comparable reoperation risk may reflect the improved precision of modern PECD and thorough decompression under endoscopic visualization could reduce the likelihood of residual or recurrent stenosis that necessitates revision. It is also possible that the follow-up duration in current reports is insufficient for differences in adjacent segment disease to manifest, to which ACDF is known to predispose over the long term. Yet the incidence of radiographic ASD was similar between groups in our analysis, likely because the majority of included patients have not been observed beyond 2–5 years. Longer-term studies will be needed to determine if the motion preservation of PECD translates into a lower rate of adjacent segment disease and fewer secondary surgeries in the decade following treatment. For now, our findings indicate that at least in the mid-term, endoscopic foraminotomy does not incur an excess risk of reoperation.
5. Limitation
When interpreting the findings of this meta-analysis, several limitations must be acknowledged. First, the available evidence base is a mixture of study designs and quality. There have been only a few randomized controlled trials directly comparing PECD to ACDF. Second, although our focus was full-endoscopic posterior cervical decompression, technique and population heterogeneity still remained. The inclusion of both uniportal and biportal variants, alongside mixed cohorts of radiculopathy and myelopathy, may constrain the generalizability of our results. Third, several outcomes required secondary data handling. Although we performed sensitivity analyses excluding such studies, these procedures can introduce measurement error. Fourth, extreme statistical heterogeneity was observed for perioperative endpoints, including length of hospital stay and intraoperative blood loss. This variability is driven by profound clinical, methodological, and systemic confounding factors across the historical cohorts. Regarding hospitalization duration, variations in global healthcare delivery models create substantial baseline divergence. For instance, the aggressive transition toward outpatient ambulatory surgical centers in the United States contrasts sharply with multi-day inpatient observation protocols dictated by cultural expectations and insurance reimbursement frameworks in East Asian centers.8,43,45,47 Furthermore, institutional discharge criteria (e.g., drain removal thresholds vs. pain score minimums) remain unstandardized globally. Regarding intraoperative blood loss, the technical nature of full-endoscopic surgery introduces a severe measurement artifact. PECD relies on continuous fluid irrigation, meaning that true hemorrhage is heavily diluted and mathematically obscured. Consequently, estimating blood loss in PECD relies on highly volatile institutional methods (e.g., visual colorimetric estimation or subtraction of irrigation volume) compared to the direct suction and sponge-weight measurements used in ACDF.24,27 This is further compounded by the retrospective nature of the majority of included studies, which rely on subjective entries in operative logs rather than standardized, formula-based hidden blood loss calculations based on pre- and post-operative hemoglobin fluctuations. Furthermore, unadjusted surgeon experience and evolving endoscopic systems across the historical timeline compound this inconsistency.61-65 These unadjusted systemic variances necessitate caution when generalizing pooled perioperative metrics. Fifth, follow-up was predominantly mid-term, which may be insufficient to detect differences in ASD or late reoperations. Finally, a fundamental finding in surgical decision-making is that ACDF and PECD are not universally interchangeable. While PECD offers distinct advantages for select candidates, ACDF remains the gold standard for complex cases requiring broader clinical indications.
6. Conclusion
Posterior endoscopic cervical decompression emerges from this analysis as a compelling alternative to ACDF for cervical radiculopathy or myelopathy. It achieves comparable long-term success in functional improvement but less neck pain reduction. Clinically, PECD patients recover faster, with shorter hospital stays and reduced perioperative pain, and they avoid many fusion-related complications. Meanwhile, no compromises in neurological outcome, spine stability, or mid-term reoperation rates were observed.
Supplemental Material
Supplemental Material -Full-Endoscopic Posterior Cervical Decompression Versus Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis
Supplemental Material for Full-Endoscopic Posterior Cervical Decompression Versus Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis by Chi-Chin Huang, Yu-San Chen, Yueh-Ying Hsieh, Chang-Jung Chiang, Lien-Chen Wu, Yen-Hsiang Wang and Ting-Shuo Hsu in Global Spine Journal.
Supplemental Material
Supplemental Material -Full-Endoscopic Posterior Cervical Decompression Versus Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis
Supplemental Material for Full-Endoscopic Posterior Cervical Decompression Versus Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis by Chi-Chin Huang, Yu-San Chen, Yueh-Ying Hsieh, Chang-Jung Chiang, Lien-Chen Wu, Yen-Hsiang Wang and Ting-Shuo Hsu in Global Spine Journal.
Footnotes
Ethical Considerations
Not applicable. This study is a systematic review and meta-analysis of previously published studies and did not involve new human or animal participants.
Author Contributions
Conceptualization: Ting-Shuo Hsu. Data curation: Chi-Chin Huang, Yen-Hsiang Wang. Formal analysis: Chi-Chin Huang, Yu-San Chen. Funding acquisition: Not applicable. Methodology: Yueh-Ying Hsieh. Project administration: Not applicable. Visualization: Not applicable. Writing - original draft: Chi-Chin Huang, Yu-San Chen, Yen-Hsiang Wang. Writing - review & editing: Yueh-Ying Hsieh, Chang-Jung Chiang, Lien-Chen Wu, Ting-Shuo Hsu.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.