
Abstract
Study Design
Systematic Review.
Objectives
Lumbar foraminal stenosis (LFS) is a common finding on spine imaging. While surgery is indicated for symptomatic LFS, the clinical impact of incidentally found asymptomatic LFS (aLFS) on surgical outcomes remains unclear. This study aims to evaluate the influence of aLFS on reoperation rates and functional outcomes following lumbar spine surgery.
Methods
A systematic search of PubMed, Embase, MEDLINE, and the Cochrane Library was conducted. Eight of 795 records met inclusion criteria and encompassed 1,744 adult patients undergoing lumbar spinal surgery, of whom 468 (26.8%) had aLFS. Due to heterogeneity in LFS classification, surgical procedures, follow-up duration, and patient-reported outcome measures (PROMs), quantitative pooling was not feasible and a structured narrative synthesis was performed. Study characteristics, patient demographics, surgical details, LFS classification methods, PROMs, and reoperation events were assessed.
Results
aLFS was associated in some studies with less postoperative improvement in Oswestry Disability Index and greater residual back and leg pain. Several studies suggested that preoperative aLFS at the surgical level was associated with increased index-level reoperations following decompression (low-moderate certainty). However, no association was found at adjacent levels or with fusion procedures.
Conclusions
Evidence regarding the prognostic significance of incidental aLFS remains limited, heterogeneous, and low certainty. Association between index-level aLFS and later reoperation should be interpreted cautiously because instability-related factors may be stronger drivers of failure than stenosis severity alone. Current evidence does not support prophylactic treatment of radiographically asymptomatic foraminal stenosis, particularly at adjacent levels in the absence of instability or symptom correlation.
Introduction
Lumbar foraminal stenosis (LFS) is defined as radiographic narrowing of the intervertebral foramen beneath the lamina and facet joints, often causing radiculopathy in the legs or back. 1 Diagnosis typically relies on clinical symptoms and radiographic assessments such as magnetic resonance imaging (MRI), and severity can be graded morphologically. Although symptomatic LFS is a well-recognized indication for surgical treatment, 2 incidental LFS is frequently detected in patients undergoing evaluation for other degenerative spinal pathologies, such as central canal stenosis or lateral recess stenosis.3-6 Many of these patients undergo spinal surgery for their primary diagnosis, leaving surgeons to question whether coexisting asymptomatic LFS (aLFS) defined clinically as radiographic foraminal narrowing without attributable dermatomal radicular symptoms or focal neurologic findings, should be observed or addressed by extending decompression at the index level or fusion to an adjacent level.
There is currently no consensus on the optimal management of aLFS when spinal surgery is indicated for other symptomatic pathology. A conservative approach is to leave aLFS unaddressed, following the idea that intervention is not justified without clear corresponding symptoms. However, some studies have found the presence of aLFS to be linked to poorer clinical outcomes and higher reoperation rates following decompression surgery.7-11 This discrepancy has led surgeons to consider prophylactically addressing aLFS, despite the absence of definitive supporting data.2,12 Interpretation of these findings is further complicated by heterogeneity in radiographic definitions of aLFS and inconsistent handling of subtle or equivocal symptoms across studies.
Given these uncertainties, clarifying the clinical impact of aLFS is necessary to help guide surgical decision-making and patient counseling. To address this gap, we conducted a systematic review to evaluate whether preoperative aLFS influences postoperative outcomes following lumbar spine surgery and to highlight priorities for future research.
Methods
Design and Search Strategy
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, and the study selection process is illustrated in a PRISMA flow diagram (Figure 1). This review was not prospectively registered. We searched PubMed, Embase, The Cochrane Library (CENTRAL), and OVID Medline for eligible publications using words including “asymptomatic foraminal stenosis,” “foraminal stenosis,” and “foraminal narrowing,” along with any combinations of words indicating a different primary surgical indication. For example, keywords including “spinal stenosis,” “foraminal stenosis,” “lumbar stenosis,” “foraminal narrowing,” “fusion,” and “decompression” were combined with Boolean operators to ensure a comprehensive search strategy of relevant literature. The last search was conducted on May 4, 2025; no language other than English was included by design. The detailed search terms can be found in Supplemental Table 1. Prisma flowchart for manuscript selection. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.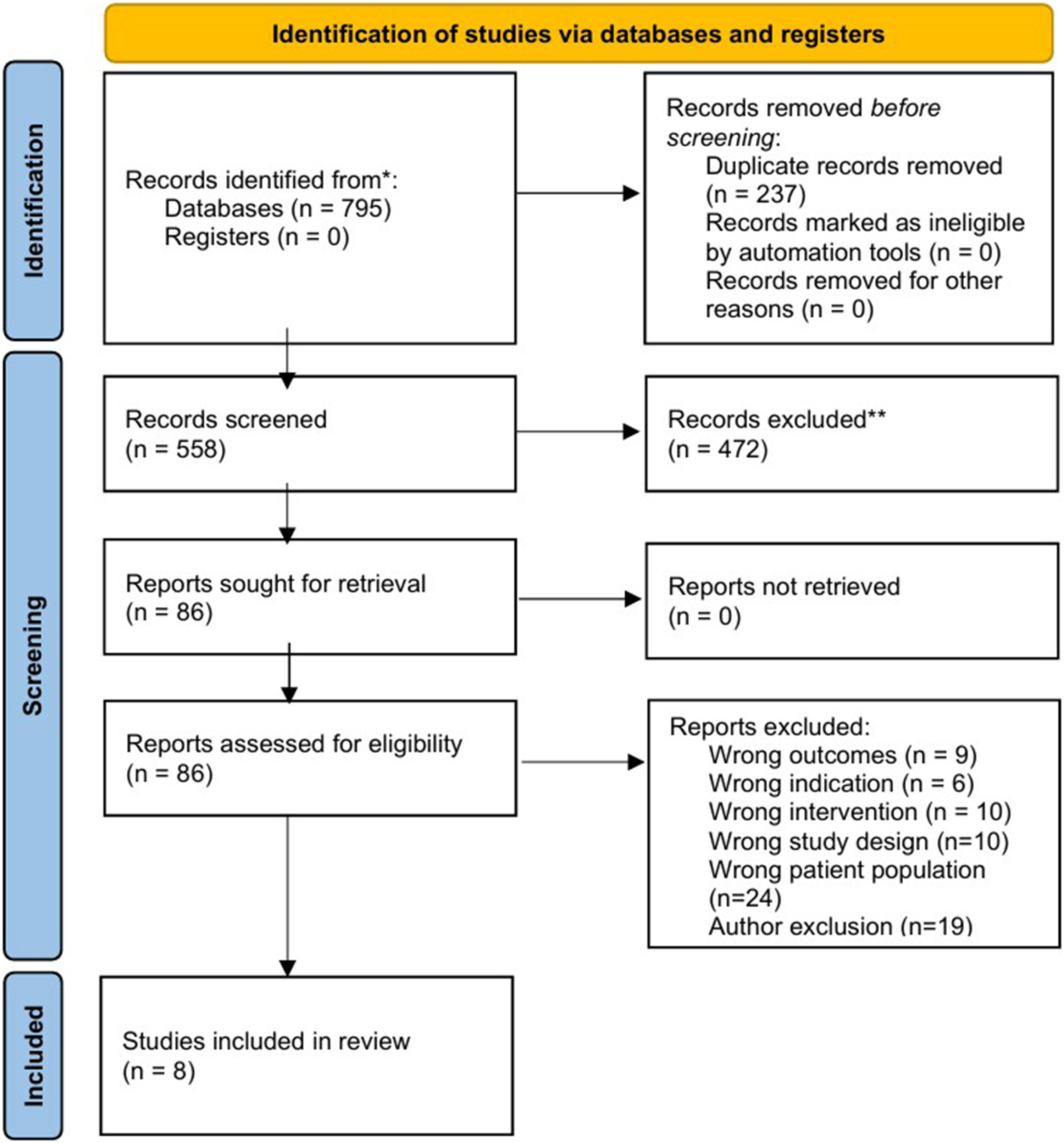
Eligibility Criteria
All Level I–IV evidence studies, as defined by the Center for Evidence-Based Medicine (CEBM) system, that involved adult patients (aged >18 years) who (1) underwent lumbar spine surgery and (2) had aLFS identified preoperatively were included. 13 Studies that reported aLFS status in patients undergoing surgery for a different indication were included. Exclusion criteria were: (1) pediatric patients (aged < 18 years), (2) non-surgical studies, (3) single case reports, (4) non-English studies, (5) studies not primarily focused on the lumbar region, (6) studies only assessing symptomatic LFS, and (7) studies limited to postoperative-onset aLFS.
Study Selection, Data Extraction, and Risk-of-Bias Assessment
Titles/abstracts and full texts were screened independently by two reviewers, with disagreements resolved by a senior author. The following data points were collected and extracted for analysis independently by two reviewers: (1) study details including author, date, and type of study, (2) population details (sample size, demographics, and number of aLFS patient), (3) intervention details, (4) radiographic assessment methods for aLFS, (5) patient-reported outcomes and measures (PROMs: ODI, VAS, JOA, EQ-5D, others), (6) reoperation or additional surgery events (at index and adjacent level), (7) complications (cerebrospinal fluid leakage, implant failure, nonunion, infection, thromboembolism, cardiovascular events, respiratory complications, ASD development), and (8) radiographic outcomes (pelvic incidence-lumbar lordosis mismatch, sagittal vertical axis, foraminal measurements, disc height, extension-neutral transition, and posterior slip). Risk of bias was assessed using the ROBINS-I tool. Methodological quality was graded using the Modified Coleman Methodology Score (MCMS), and the level of evidence was assigned using the CEBM system.
Synthesis Approach
Because of anticipated heterogeneity in study design, definitions of aLFS, surgical procedures, follow-up durations, and outcome measures, a quantitative meta-analysis was not considered feasible. We therefore planned a structured narrative synthesis in accordance with the SWiM (Synthesis Without Meta-analysis) reporting guideline. 14 Studies were to be grouped by surgical strategy (decompression alone vs fusion), classification method of LFS, and outcome domain. PROMs were synthesized with ODI as the primary metric when available, while other validated scales (VAS, NRS, JOA, EQ-5D) were considered for direction of effect. Reoperations/additional surgeries were categorized as index- or adjacent-level. Synthesis relied on structured tabulation and vote counting by direction of effect, prioritizing the longest available follow-up and the most widely used outcome measures when multiple time points or scales were reported. Heterogeneity was examined narratively with attention to variability in aLFS definitions (e.g., Lee grading vs perineural fat obliteration), surgical strategies, and reported outcomes. Certainty of evidence was judged qualitatively using ROBINS-I risk-of-bias assessments, methodological quality scores, and study design. These decision rules were established to improve consistency of synthesis across heterogeneous observational studies. Results are presented in summary tables ordered by outcome domain and study design, with effect direction indicated.
Results
Study Selection and Quality Assessment
Study Characteristics
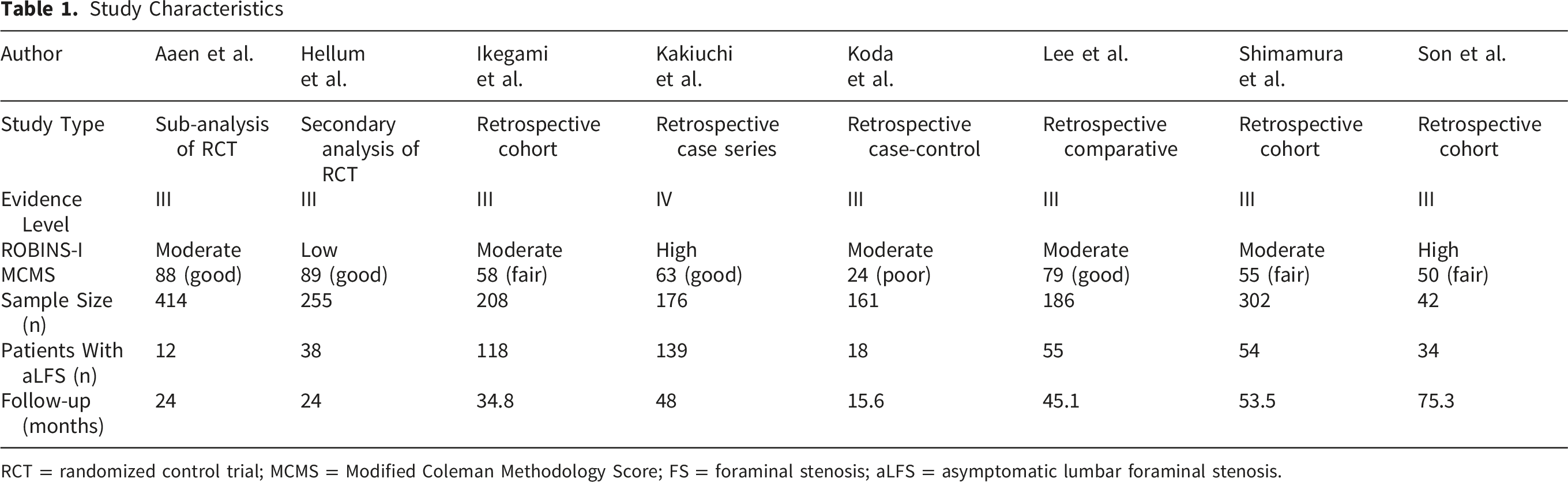
RCT = randomized control trial; MCMS = Modified Coleman Methodology Score; FS = foraminal stenosis; aLFS = asymptomatic lumbar foraminal stenosis.
Demographic Data and Surgical Strategies
The eight studies analyzed 1,744 patients, of whom 26.8% had asymptomatic LFS.11,15-22 Four studies compared baseline demographics between patients with and without asymptomatic LFS. Two studies (Lee et al., and Ikegami et al.) reported that those with LFS were older than those without. In contrast, Aaen et al. found no difference in age between groups, but of their included 12 patients with aLFS (2.9% of this study cohort), a greater proportion were female. 18
Demographic Data and Surgical Strategies
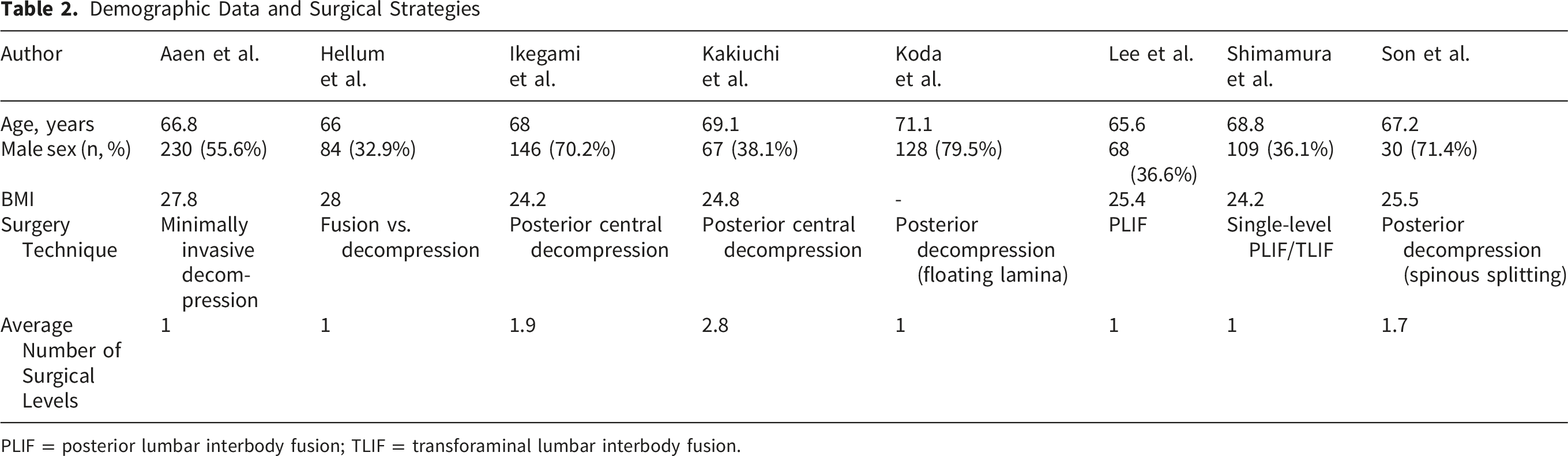
PLIF = posterior lumbar interbody fusion; TLIF = transforaminal lumbar interbody fusion.
LFS Assessment
Foraminal Stenosis Classification
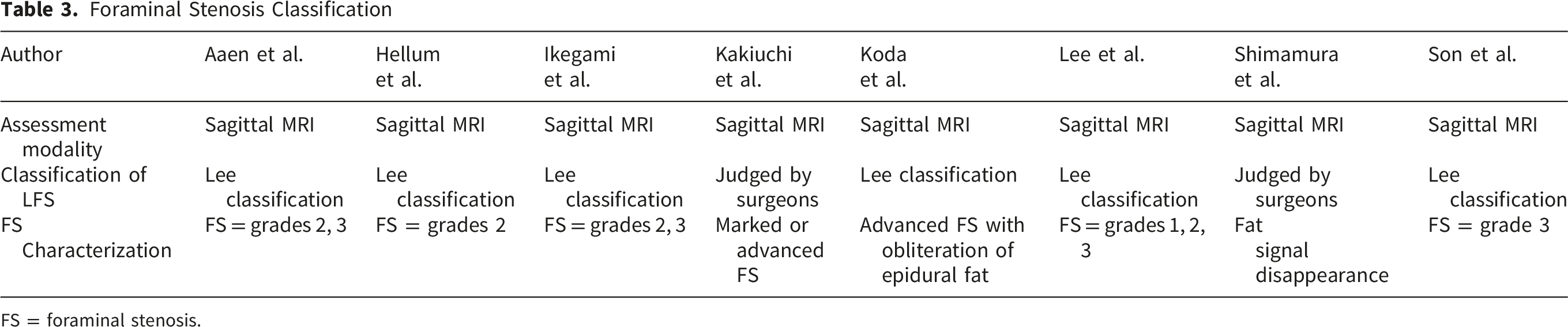
FS = foraminal stenosis.
PROMs
Summary of Outcomes
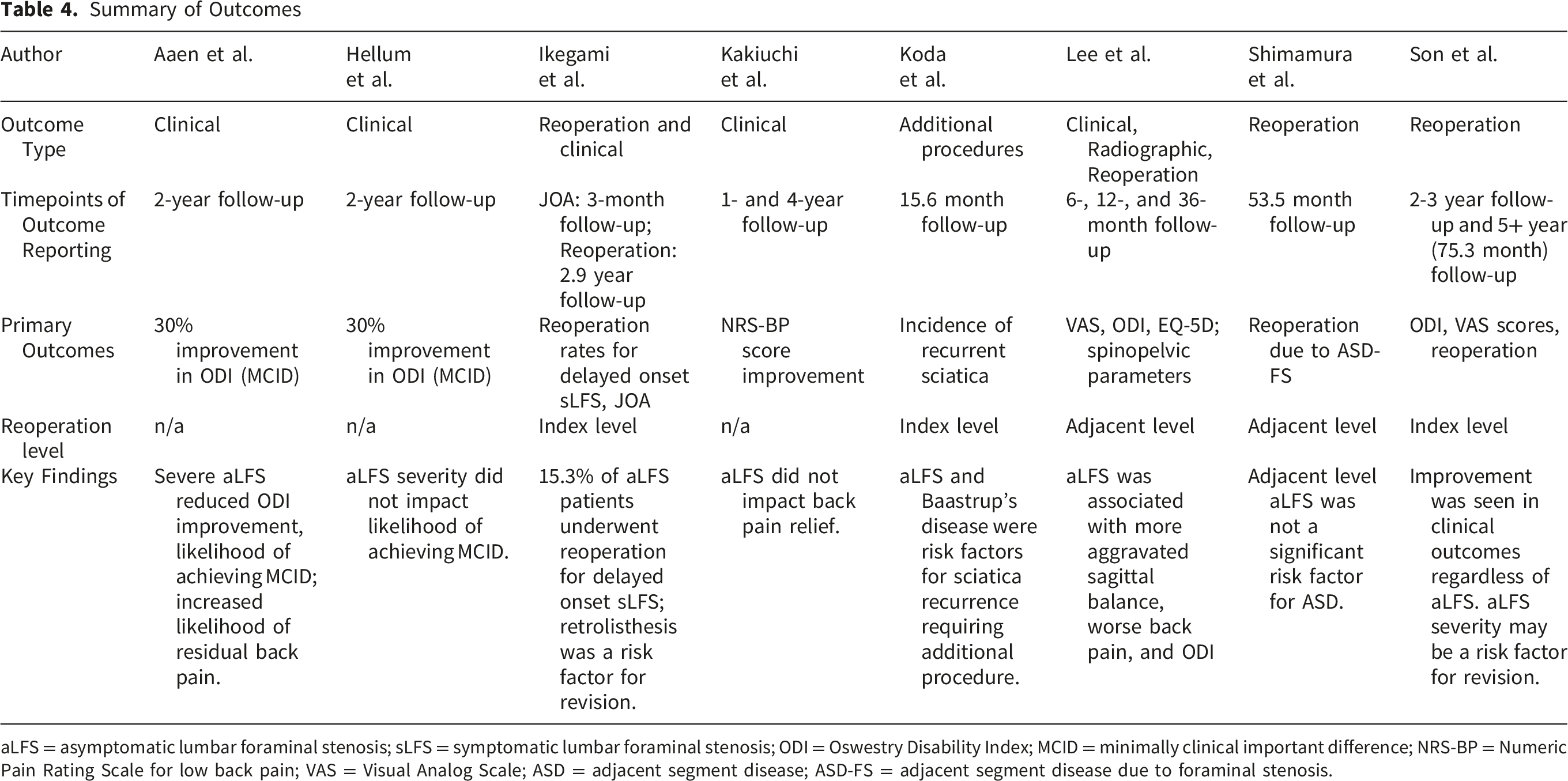
aLFS = asymptomatic lumbar foraminal stenosis; sLFS = symptomatic lumbar foraminal stenosis; ODI = Oswestry Disability Index; MCID = minimally clinical important difference; NRS-BP = Numeric Pain Rating Scale for low back pain; VAS = Visual Analog Scale; ASD = adjacent segment disease; ASD-FS = adjacent segment disease due to foraminal stenosis.
Direction of Effect Summary for aLFS
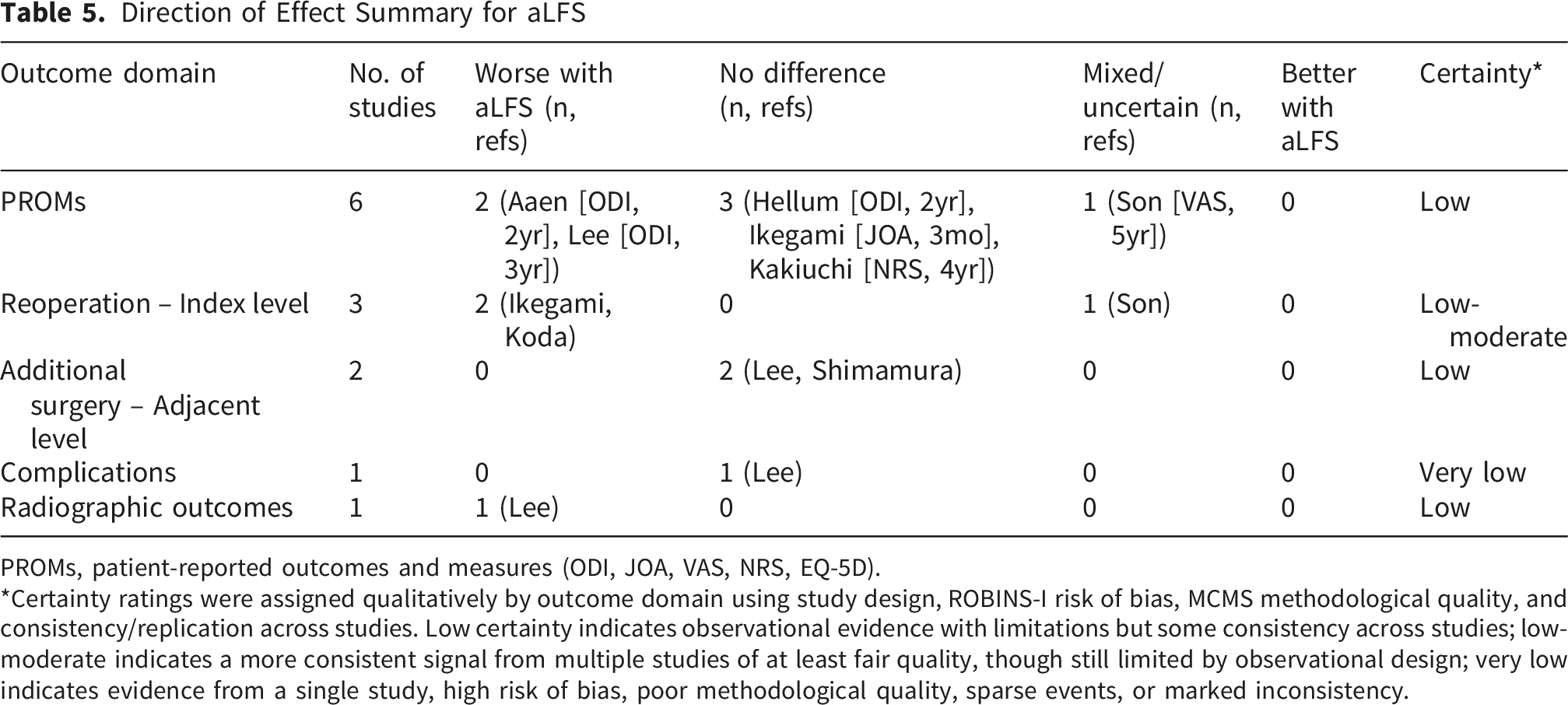
PROMs, patient-reported outcomes and measures (ODI, JOA, VAS, NRS, EQ-5D).
*Certainty ratings were assigned qualitatively by outcome domain using study design, ROBINS-I risk of bias, MCMS methodological quality, and consistency/replication across studies. Low certainty indicates observational evidence with limitations but some consistency across studies; low-moderate indicates a more consistent signal from multiple studies of at least fair quality, though still limited by observational design; very low indicates evidence from a single study, high risk of bias, poor methodological quality, sparse events, or marked inconsistency.
In contrast, longer-term outcomes showed signals of worse results in the aLFS group. Aaen et al. reported that patients with severe aLFS were less likely to achieve the MCID of ODI (36% vs 71%) and had greater residual back pain (mean NRS 5.6 vs 3.6). 18 Likewise, Lee et al. noted that ODI scores worsened at 24 months in patients with aLFS (32 vs 16 in non-aLFS). 20 In contrast, Hellum et al. found no association between aLFS and ODI improvement or MCID achievement, and ZCQ improvement at 2 years did not differ by aLFS status. 17 Kakiuchi et al. also concluded no significant association between aLFS and postoperative back pain at 4 years postoperatively. 21
Overall, short-term PROMs were generally comparable between groups. At longer follow-up, two studies and one mixed report suggested that aLFS may be associated with less favorable outcomes, particularly regarding ODI improvement and residual back pain, whereas several others found no difference. Certainty of evidence was low, limited by heterogeneity of outcome measures, moderate risk of bias, and inconsistency across studies.
Reoperations at Index Level
Three studies evaluated reoperation at the index level (Ikegami et al., Koda et al., and Son et al.). Direction-of-effect synthesis indicated a consistent signal toward higher revision rates among patients with preoperative aLFS (Table 5). Ikegami et al. reported that 15.3% of patients with preoperative aLFS at the index level eventually required additional surgery and preoperative retrolisthesis was an independent predictive factor of these additional surgeries. 11 Son et al. similarly found that dynamic radiographic factors such as posterior translation and slip were strongly associated with reoperation, while the severity of foraminal stenosis showed a marginal trend (OR: 7.56, p = 0.064). 16 Koda et al. also reported that preoperative aLFS was associated with recurrent sciatica requiring additional procedures (OR: 17.9, p < 0.01). Overall, the evidence suggests that aLFS may be associated with a risk of reoperation at the index level following decompression. Certainty of evidence was judged as low–moderate, limited by observational study design and potential residual confounding.
Additional Surgeries at Adjacent Level
Two studies assessed adjacent-level surgeries related to ASD or foraminal stenosis (Shimamura et al., and Lee et al.). Both found no significant association between preoperative aLFS and adjacent-level reoperation risk (Table 5). Shimamura et al. reported that only 9.3% of patients with preoperative aLFS developed ASD, and that sagittal alignment parameters, rather than aLFS, were the primary predictors of reoperation. 15 Lee et al. likewise observed no additional adjacent-level reoperations among patients with coexisting asymptomatic L5–S1 stenosis. 20 Overall, the evidence indicates that aLFS does not substantially increase adjacent-level reoperation risk. Certainty of evidence was rated as low, reflecting the small number of available studies and limited event rates.
Complications
Perioperative and postoperative complications were inconsistently reported across studies, and few analyses stratified outcomes by aLFS status. Lee et al. reported that surgical and medical complication rates were similar between groups: 10.9% and 6.1% in those with and without adjacent aLFS, with no significant differences in cerebrospinal fluid leakage, implant-related events, nonunion, infection, or systemic complications. Given the small number of studies, low event rates, and heterogeneous definitions, the current evidence is insufficient to establish whether aLFS influences complication risk. Certainty of evidence was graded as very low.
Radiographic Outcomes
Radiographic findings were limited and heterogeneous. In the only study that reported detailed spinopelvic parameters, patients with aLFS showed worse preoperative alignment and higher foraminal stenosis grades at both the index L4–5 level (mean Lee grade 1.2 vs 0.7; p<0.001) and the adjacent asymptomatic L5–S1 level (0.9 vs 0.0; p<0.001). 20 Although sagittal alignment improved postoperatively in both groups, alignment at final follow-up remained less favorable in those with adjacent-level aLFS. Foraminal height decreased in both groups after PLIF (Δ−1.7 mm in aLFS vs Δ−2.2 mm in non-aLFS; p=0.020 and p=0.004, respectively). Overall, current evidence suggests a possible association between aLFS and unfavorable radiographic parameters; however, certainty of evidence was graded as low, reflecting reliance on a single cohort and lack of replication.
Discussion
Summary of Findings
This systematic review summarized current literature regarding the impact of preoperative aLFS on post-surgical outcomes after lumbar spine decompression and fusion. Eight studies including 1,744 patients (468 with aLFS) were identified, but their small number, heterogeneous designs, and inconsistent findings preclude definitive conclusions. Demographic data suggested that patients with aLFS tended to be older and showed more advanced degeneration, whereas other baseline characteristics were largely comparable. The most common radiographic assessments were Lee’s classification and perineural fat assessment. Short-term clinical outcomes were generally comparable between patients with and without aLFS, whereas long-term follow-up suggested less favorable outcomes in those with preoperative aLFS group, particularly in ODI and its MCID achievement (low certainty). For reoperation, two of three studies reported higher revision rates at the index level while adjacent-level additional surgery showed no association with aLFS; certainty was low-moderate and low, respectively. Complications were rarely stratified by aLFS status and showed no differences (very low certainty), while radiographic outcomes suggested more severe preoperative alignment issues in aLFS patients but were based on a single cohort (low certainty).
LFS Radiographic Assessment
The first knowledge gap involves the definition and diagnosis of aLFS. Standardizing what qualifies as “asymptomatic LFS” remains challenging. In three studies, diagnosis relied on interview-based symptom screening, which is practical in routine clinical care but may allow patients with subtle symptoms to be misclassified, biasing intervention effects.11,15,20 Although more objective tests, such as preoperative selective nerve root block could theoretically help exclude symptomatic involvement, interview-based screening cannot be dismissed from a clinical utility standpoint. 23
For radiographic assessment methods, this review identified two approaches: Lee’s grading system and foraminal fat disappearance. Studies using the Lee scale generally demonstrated good to excellent reliability; for example, nearly perfect agreement was reported between two experienced radiologists and Ikegami et al. also confirmed high interobserver consistency.11,22 Even so, Lee-based studies applied different grade thresholds to define the aLFS group (e.g., grades 1–3 vs ≥2), creating variability in case definition. Because morphological changes of the intervertebral foramen correlate, at least to some extent with radicular symptoms, inconsistent grouping criteria likely contribute to between-study heterogeneity and limit comparability. 24 Future prospective studies should pre-specify a symptom-screening protocol, adopt a uniform imaging definition with blinded readers and report inter/intra-rater reliability, and declare an a priori threshold for Lee grades or perineural fat obliteration.
PROMs and Associated Factors With Poorer Outcomes
Six studies evaluated patient-reported outcomes, with overall mixed results. Short-term outcomes within 1-year were generally comparable, but long-term follow-up later than 2 years after lumbar decompression with or without fusion suggested possible differences. Two studies18,20 reported less ODI improvement in patients with aLFS, while others11,17 found no association. These discrepancies may partly reflect differences in grading criteria: for example, Lee et al. defined aLFS as grade 2–3, whereas Hellum et al. excluded patients with grade 3 disease.
Beyond grading definitions, several studies suggest that the impact of aLFS may be amplified by changes in mechanical loading that elicit dynamic instability. Examples include posterior slip, kissing spinous processes, or retrolisthesis.11,19 Similarly in fusion surgery, increased load transfer to adjacent segments can convert aLFS into symptomatic LFS. 25 These observations indicate that mechanical loading, whether due to intrinsic instability or surgically induced redistribution, may represent a plausible pathway through which aLFS influences long-term outcomes. Dynamic imaging studies support this concept: foraminal area varies by position 26 with kinetic MRI demonstrating 30% reduction in extension 27 and dynamic tomosynthesis showing narrower foramina in the upright position. 28 These findings highlight the importance of identifying radiographic markers of instability, such as kissing spinous processes, retrolisthesis, facet joint morphology, coronal deformity, or excessive facet joint resection, rather than relying solely on static MRI.11,19,29-32
Interpretation of reduced ODI improvement requires caution. Lee et al. observed that patients with LFS demonstrated worse sagittal malalignment, potentially due to compensatory forward leaning to avoid stenosis in the upright position. Whether sagittal malalignment is a cause or a marker remains unclear, but it may be influenced by age and the degree of degeneration to influence outcomes. 11 Furthermore, excessive facet joint resection may contribute to the segmental instability. 32 Future studies should systematically evaluate segmental instability markers, investigate their interaction with aLFS, and determine which factors provide the strongest predictive value for long-term functional decline or conversion to symptomatic LFS. 31
Reoperation at the Index Level
Across three studies, there was a consistent signal that preoperative aLFS is associated with higher revision rates after decompression at the index level, but the magnitude and independence of this association remain uncertain.11,15,16 This outcome helps to address one of the primary questions underlying this review: should prophylactic repair of aLFS be performed when performing spinal surgery for other indications? Taken together with the observation that radiographic markers of segmental instability (e.g., retrolisthesis, posterior translation/slip) predicted reoperation, these findings suggest that aLFS may be a marker of segments more vulnerable to dynamic narrowing and recurrent symptoms after decompression. Clinically, this data does not justify prophylactic intervention of aLFS, but does support risk stratification by using similar findings related to PROMs. Future studies should therefore evaluate whether targeted surgical strategies in patients with both aLFS and instability markers, rather than all patients with incidental aLFS, can reduce revision risk and improve long-term outcomes.11,19
Additional Surgery at Adjacent Levels
By contrast, two studies did not show an increased risk of adjacent-level additional surgery in the presence of preoperative aLFS. Predictors of adjacent procedures were instead sagittal alignment parameters (e.g., sacral slope, lumbar lordosis, pelvic tilt), consistent with the broader literature on adjacent segment disease after fusion. These findings suggest that incidentally detected aLFS at an adjacent level should not prompt prophylactic extension of surgery. Rather, prevention efforts should prioritize alignment goals and load redistribution rather than prophylactically extending surgery to incidentally detected aLFS at the adjacent level.33,34
Limitations
This systematic review has several inherent limitations. The exclusion of non-English studies may have omitted relevant research in other languages, and the inclusion criteria may have introduced selection bias by prioritizing studies that explicitly differentiated between symptomatic and aLFS. Additionally, heterogeneity among studies, such as LFS diagnostic criteria, severity classification, surgical technique, and patient populations, limits the generalizability of conclusions and our ability to perform subgroup analyses between clinical outcomes of decompression versus fusion patients. Standardization among LFS grading and patient populations would be required to make direct comparisons among the articles. The reliance on published studies also introduces potential publication bias, as studies with negative or inconclusive findings may be underrepresented in published literature. This review was not prospectively registered in PROSPERO or another database, which reduces transparency regarding protocol deviations and may introduce reporting bias; however, the scope of this review (observational risk factor synthesis) lies partly outside PROSPERO’s main registration categories. To mitigate this limitation, eligibility criteria, synthesis methods, and outcome domains were defined a priori, and the review process adhered to PRISMA and SWiM frameworks. Because of the substantial heterogeneity of included studies, only narrative synthesis with vote counting was feasible. While this approach increases the risk of interpretive bias, it provides structured transparency when meta-analysis is not possible. We did not perform a formal GRADE assessment because the included evidence was heterogeneous, prognostic in nature, and not amenable to pooled effect estimation. A source of heterogeneity was the definition of aLFS. Most included studies did not explicitly screen for subclinical or equivocal radicular symptoms, while others used variable clinical exclusion rules. Misclassification of symptoms is possible as a result. The certainty ratings used throughout this review (low, low–moderate, very low) are qualitative descriptors assigned by the authors based on ROBINS-I risk of bias, methodological quality, and consistency across studies, and should not be interpreted as formal GRADE evidence ratings.
Despite these limitations, this review employed a broad search strategy, rigorous study selection, and structured synthesis to provide the most comprehensive summary currently available.
Conclusion
This systematic review clarifies that current evidence does not support prophylactic surgery for incidental aLFS. Although some studies suggest that index level aLFS may be associated with higher longer-term reoperation risk after decompression, this assessment is based on low-moderate certainty, heterogeneous observational evidence and may be confounded by coexisting instability and alignment related factors. Conversely, available evidence does not suggest that asymptomatic adjacent-level foraminal stenosis alone predicts adjacent-level reoperation. Overall, incidental aLFS should be interpreted in clinical and mechanical context rather than as an isolated indication to extend decompression or fusion.
Supplemental Material
Supplemental material - Impact of “Asymptomatic,” Radiographic Foraminal Stenosis on Lumbar Spine Surgery Outcomes: A Systematic Review
Supplemental material for Impact of “Asymptomatic,” Radiographic Foraminal Stenosis on Lumbar Spine Surgery Outcomes: A Systematic Review by Rebecca L. Boyle, Tim Xu, Zora C. Hahn, Tomoyuki Asada, Ted Shi, John E. Lama, Arsen M. Omurzakov, Evan D. Sheha, Sheeraz A. Qureshi, MD, MBA, Sravisht Iyer in Global Spine Journal
Footnotes
Ethical Considerations
Not applicable. This study is a systematic review of previously published data and does not involve human subjects, identifiable data, or new patient information.
Author Contributions
All authors contributed to the design, data extraction, analysis, drafting, and revision of the manuscript. All authors approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sheeraz A. Qureshi has or may receive payments or benefits from the following commercial entities: Tissue Differentiation Intelligence (Ownership/Equity/Investment); Stryker K2M (Royalties from Intellectual Property, Designer, Consultant); SpineGuard, Inc. (Consultant); Globus Medical, Inc. (Royalties from Intellectual Property, Speakers’ Bureau, Consultant); Simplify Medical, Inc. (Clinical Event Committee); AMOpportunities (Honoraria); Surgalign (Consultant); Viseon, Inc. (Research Support either personally or through HSS, Consultant); HS2, LLC (Ownership/Equity/Investment); ![]() Inc. and Spinal Simplicity, LLC (Medical or Scientific Advisory Board Membership). The author also serves in editorial or leadership roles at: Contemporary Spine Surgery (Editorial Board); North American Spine Society (NASS) (Political Engagement Committee, Payor Policy Review Committee, SpinePAC Advisory Committee, CME Committee); Annals of Translational Medicine (ATM) (Editorial Board); Hospital for Special Surgery Journal (Editorial Board, Senior Associate Editor, 2021–2024); Society of Minimally Invasive Spine Surgery (SMISS) (Program Committee, 2018 Annual Meeting Program Chair, Board of Directors, 2021–2024); Lumbar Spine Research Society (LSRS) (Website Committee, 2022, Member at Large); Cervical Spine Research Society (CSRS) (Publications Committee, 2019–2022); Minimally Invasive Spine Study Group (Board of Directors – Treasurer); Association of Bone and Joint Surgeons (ABJS) (Program Committee); and International Society for the Advancement of Spine Surgery (ISASS) (Education and Program Committees, 2021 Annual Meeting Program Chair). Sravisht Iyer has or may receive payments or benefits from the following commercial entities: Globus Medical and Stryker (Paid presenter or speaker); Vertebral Columns/International Society for the Advancement of Spine Surgery (ISASS) (Editorial or Governing Board). HS2, LLC Innovasis HSS ASC Development Network, LLC Globus Medical, Inc. Joint Effort Administrative Services Organization Intrinsic Therapeutics.
Inc. and Spinal Simplicity, LLC (Medical or Scientific Advisory Board Membership). The author also serves in editorial or leadership roles at: Contemporary Spine Surgery (Editorial Board); North American Spine Society (NASS) (Political Engagement Committee, Payor Policy Review Committee, SpinePAC Advisory Committee, CME Committee); Annals of Translational Medicine (ATM) (Editorial Board); Hospital for Special Surgery Journal (Editorial Board, Senior Associate Editor, 2021–2024); Society of Minimally Invasive Spine Surgery (SMISS) (Program Committee, 2018 Annual Meeting Program Chair, Board of Directors, 2021–2024); Lumbar Spine Research Society (LSRS) (Website Committee, 2022, Member at Large); Cervical Spine Research Society (CSRS) (Publications Committee, 2019–2022); Minimally Invasive Spine Study Group (Board of Directors – Treasurer); Association of Bone and Joint Surgeons (ABJS) (Program Committee); and International Society for the Advancement of Spine Surgery (ISASS) (Education and Program Committees, 2021 Annual Meeting Program Chair). Sravisht Iyer has or may receive payments or benefits from the following commercial entities: Globus Medical and Stryker (Paid presenter or speaker); Vertebral Columns/International Society for the Advancement of Spine Surgery (ISASS) (Editorial or Governing Board). HS2, LLC Innovasis HSS ASC Development Network, LLC Globus Medical, Inc. Joint Effort Administrative Services Organization Intrinsic Therapeutics.
Data Availability Statement
All data included in this systematic review are derived from previously published studies. No new raw data were generated. Extracted data used in the analysis are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.