
Abstract
Study Design
Cross-sectional survey study.
Objectives
To provide a contemporary global overview of intra-operative neuromonitoring (IONM) practices, attitudes, and perceived barriers among spine surgeons.
Methods
A web-based questionnaire was distributed to AO Spine surgeon members worldwide between April and May 2025 to collect data on surgeon demographics, access to and utilization of IONM, models of service delivery, intra-operative responses to neuromonitoring alerts, attitudes toward IONM, and perceived limitations. Attitudes were assessed using 13 Likert-scale statements. Logistic regression analysis was performed to identify factors associated with a positive attitude toward IONM. Significance was set at p<0.05.
Results
A total of 529 spine surgeons responded to the survey. Consistent access to IONM was reported by 55.5% of respondents, occasional access by 35.7%, and no access by 8.8%. External service providers were the most used IONM model (59.5%). Neuromonitoring technicians most frequently interpret intraoperative data (63.6%). In response to unexpected signal loss, most surgeons reported using a standardized checklist (76.3%). Overall attitudes toward IONM were predominantly positive, with most respondents agreeing that IONM improves patient outcomes, provides medicolegal protection, and offers surgeon reassurance. Economic constraints (38.2%), logistical challenges (27.4%), and lack of training (25.6%) were the most reported barriers. Multivariate analysis identified geographic region, specialty, and access to IONM as independent predictors of a positive attitude.
Conclusions
This global survey demonstrates widespread acceptance of IONM among spine surgeons, particularly for high-risk procedures. However, disparities in access and persistent economic and logistical barriers remain, highlighting the need for strategies to improve equitable implementation worldwide.
Introduction
Intra-operative neuromonitoring (IONM) has become an important adjunct in modern spine surgery, aiming to reduce the risk of neurological injury through real-time assessment of spinal cord and nerve root function. Modalities such as somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and electromyography (EMG) are commonly used to detect impending neurological compromise and allow timely corrective action during surgery.1-3 Over the past two decades, advances in technology and technique have expanded the scope of IONM across a wide range of spinal procedures.
The clinical value of IONM has been most clearly demonstrated in complex and high-risk spinal surgeries, including deformity correction, tumor resection, trauma, and procedures involving the spinal cord.4-6 In these settings, IONM has been associated with earlier detection of neurological insults and, in some reports, a reduction in postoperative neurological deficits. 7 However, its role in lower-risk procedures remains controversial, with ongoing debate regarding cost-effectiveness, variable sensitivity and specificity, and inconsistent impact on outcomes.8-10
In addition to clinical considerations, medicolegal expectations have increasingly influenced the adoption of IONM. Many surgeons perceive IONM as an important protective measure, particularly in regions with higher litigation risk. 11 At the same time, access to IONM is not uniform worldwide. Economic constraints, logistical challenges, limited availability of trained personnel, and reliance on external service providers may limit routine use, particularly in low- and middle-income regions.12,13
While prior studies have evaluated the efficacy and indications for IONM, 14 limited contemporary data describe global practice patterns, surgeon attitudes, and perceived barriers to implementation. Understanding these factors is essential for informing policy, training initiatives, and future guideline development. The strength of this survey is that it is truly global and that surgeons from all specialties participated, in contrast to earlier surveys that were more SCI- or deformity-focused. Therefore, the purpose of this study was to provide a global perspective on IONM practices, attitudes toward its use, and perceived barriers among spine surgeons using data from an international survey of AO Spine members.
Methods
AO Spine represents a premier global academic community dedicated to advancing education and research in spine care. An English-language cross-sectional electronic questionnaire, developed in SurveyMonkey (San Mateo, CA), was distributed via email to spine surgeon members of AO Spine across five AO regions over one month, between 4th July and 1st August 2025. Questions were presented in various formats, including single and multiple-choice, and open-ended questions. Attitudes were assessed using 13 Likert-scale statements. Branching logic was applied to select questions as necessary. All responses were anonymous. All active on-duty surgeons at the time of the survey were eligible for inclusion. A total of 529 surgeons submitted valid, completed questionnaires. Questionnaires with incomplete responses or missing data were excluded.
Data Collection
An online survey generator (Survey Monkey) was used to create a web-based, cross-sectional survey informed by a comprehensive literature review and expert insights.14-17 A panel of experts performed a preliminary screening through consensus, followed by testing an initial version of the questionnaire on a pilot sample of 5 Orthopedic surgeons and 5 Neurosurgeons with diverse years of experience to address ambiguity, confirm comprehension, and assess completion time. In response to their feedback, specific questions were rephrased to enhance clarity. In developing the final questionnaire, we assessed the logical arrangement of items and the anticipated relationships between responses to ensure overall coherence. The tool demonstrated strong internal consistency, evidenced by an overall Cronbach’s alpha of 0.81. This survey was reviewed and approved by the AO Spine Degenerative Knowledge Forum. The e-questionnaire comprised four sections designed to gather data on demographics, current, global perspective on the practices, access, attitudes, and perceived barriers related to Intraoperative neuromonitoring (IONM) among spine surgeons,14-18 as outlined below:
Demographic and Work-Related Characteristics of the Study’s Spine Surgeons
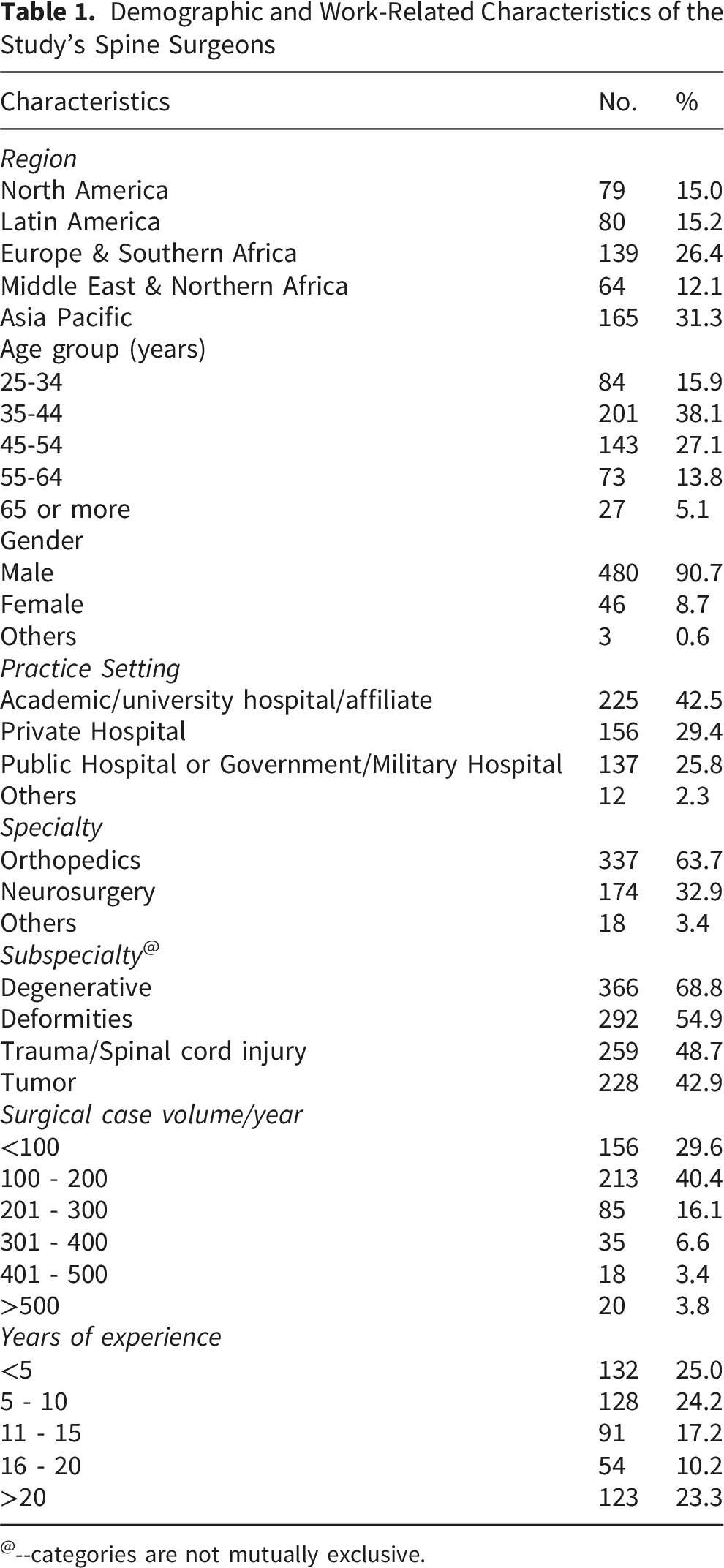
@--categories are not mutually exclusive.
Section (2) 115,17 Surgeons’ responses to IONM access [always, occasional, no access], models used [external company, In-house (internal)], who interprets the IONM data intra-operatively? [Self, neuromonitoring technician, neurologist, neurophysiologist, others], actions taken when facing unexpected loss of intraoperative potentials [Abort the surgery immediately, a neurophysiological problem, an anesthetic issue, use checklist], and Limitations to use include [economic, logistical, lack of trained neurophysiologists, others].
Section (3)14,16 discusses Attitude towards IOM. A total of 13 attitudinal statements were used to evaluate surgeons’ perspectives on the validity and importance of IOM in spine surgery. Agreement with eight statements and disagreement with five suggest a pro-IOM stance. Using a 1-5 scale, where 5 = strongly agree and 1 = strongly disagree, a score can be assigned to each respondent. For negative statements, the scoring was reversed, with 1 = strongly agree and 5 = strongly disagree. The total score ranged from 13 to 65 points, with 65 indicating a strong pro-IOM attitude. The total score for each participant was obtained by summing the scores across all 13 statements, and a percentage score was then calculated. A positive attitude was defined as PMS < 50%, a negative attitude as PMS > 75%, and a neutral attitude as PMS between 50% and 75%.
Finally, demographic information was collected from each surgeon, including age, specialty (neurosurgery or orthopedic surgery), subspecialty (degenerative, trauma, tumors, deformity), years of experience, annual case volume, practice setting (private, public, or academic/university hospital), and region.
Data Analysis
Variables were coded and analyzed using IBM SPSS Statistics version 30 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize respondent characteristics and survey responses. Categorical variables were reported as frequencies and percentages, while continuous variables were summarized using means and standard deviations or medians and interquartile ranges, as appropriate. Attitudes toward intra-operative neuromonitoring (IONM) were assessed using 13 Likert-scale statements. Responses were scored on a 5-point scale (1 = strongly disagree to 5 = strongly agree). For negatively worded statements, scores were reverse-coded. A total attitude score was calculated by summing responses across all items, yielding a possible range of 13 to 65 points. A percentage mean score (PMS) was then derived for each respondent. Attitude was then categorized as positive (>75 PMS), neutral (50-75 PMS), or negative (<50 PMS).
A multivariate logistic regression analysis was conducted to identify independent predictors of a positive attitude toward IONM. Variables entered the model included geographic region, specialty, years of experience, practice setting, annual case volume, and access to IONM. Results were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). All statistical tests were two-tailed, and a p-value ≤ .05 was considered statistically significant.
Results
Demographic and Professional Characteristics of Spine Surgeons
Table 1 summarizes the demographic and professional characteristics of the surveyed spine surgeons. Respondents were globally distributed, with the largest proportion practicing in the Asia-Pacific region (31.3%), followed by Europe & Southern Africa (26.4%). Most participants were aged 35-54 years (65.2%) and predominantly male (90.7%). Orthopedic surgeons accounted for the largest proportion of respondents (63.7%). Nearly half practiced in academic or university-affiliated hospitals (42.5%), and most reported moderate (100-200 cases/year) to high (201-300 cases/year) annual surgical volumes. Degenerative spine surgery (68.8%) was the most commonly reported subspecialty, followed by deformity (54.9%), trauma (48.7%), and tumor surgery (42.9%). About one-half of the participants (50.8%) reported more than 10 years of experience.
Access to IONM, utilization patterns, and perceived limitations
Surgeons’ Responses to IONM Access, Models Used, Actions Taken When Facing Unexpected Loss of Intraoperative Potentials, and Limitations of Use
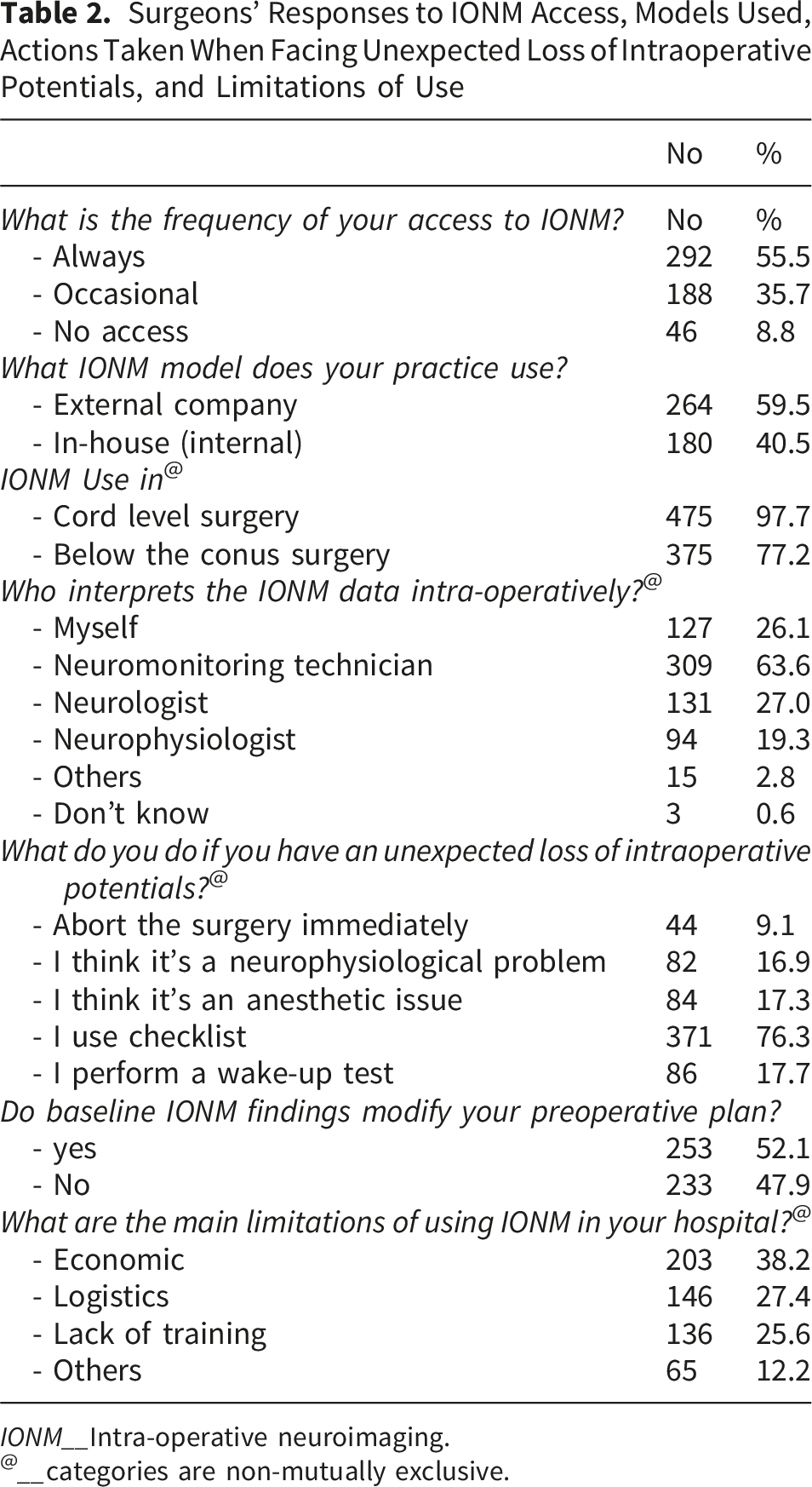
IONM__Intra-operative neuroimaging.
@__categories are non-mutually exclusive.
Surgeons’ Attitudes toward IONM
Surgeons’ Attitudes to IONM Use in Spine Operations
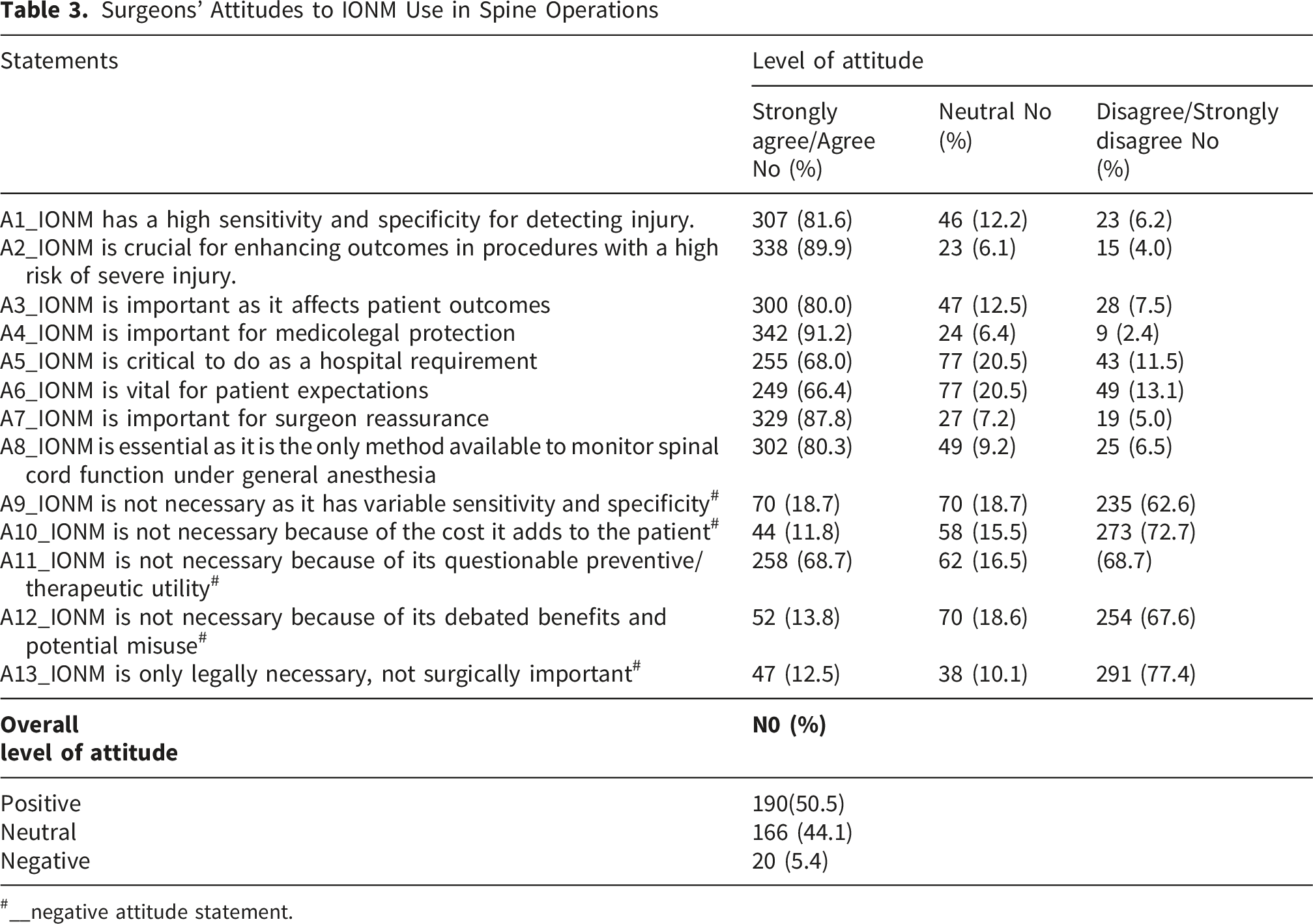
#__negative attitude statement.
Factors Associated With a Positive Attitude Toward IONM
Logistic Regression Analysis of Positive Attitude Towards IONM
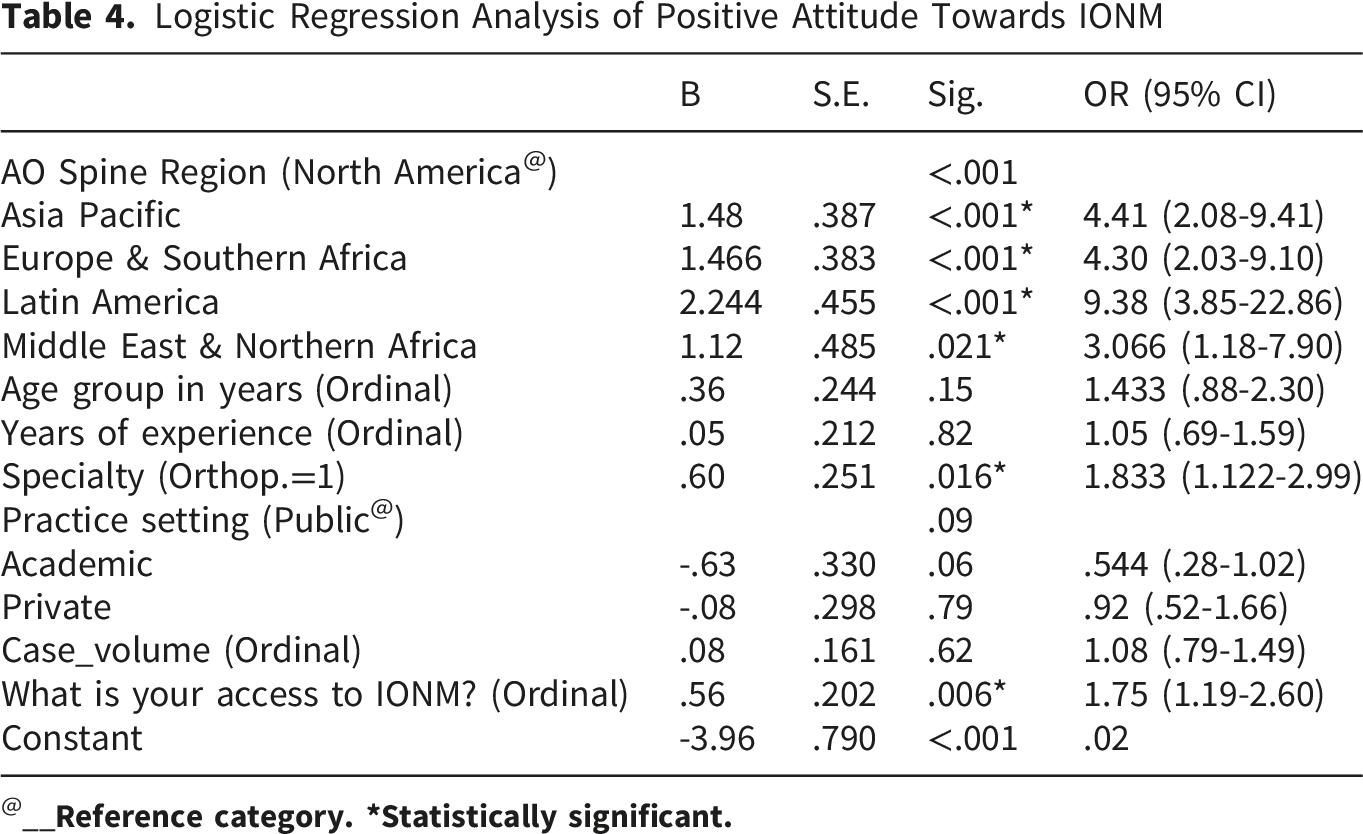
@__
IONM Modalities Routinely Utilized
Figure 1 illustrates the neuromonitoring modalities routinely used during spine surgery by survey respondents, demonstrating the widespread use of multiple IONM techniques in contemporary practice. All modalities were practiced more commonly at the cord level than below the conus. This reflects the differential use of IONM based on the perceived neurological risk of the procedure. IONM modalities routinely utilized for spine surgery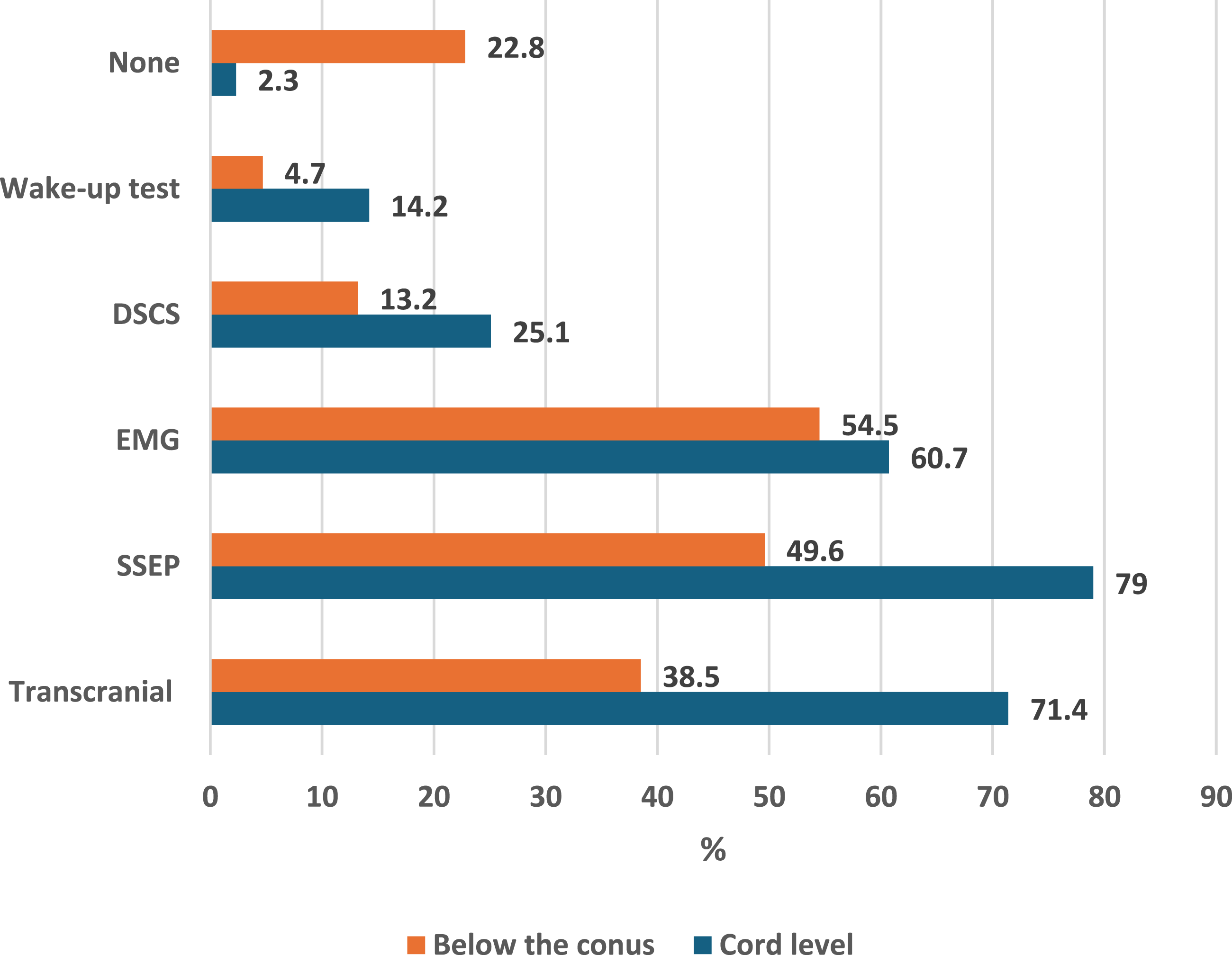
IONM Utilization Across Surgical Procedures
Figure 2 shows the rate of IONM use in different procedures among those who perform these procedures. It demonstrates that the utilization of IONM is strongly procedure-dependent. Almost all respondents (97.7%) reported using IONM during spinal cord–level procedures, underscoring its perceived necessity when the spinal cord is directly at risk. In contrast, the use of IONM declined to 77.2% for procedures performed below the conus, indicating that nearly one in four surgeons (22.8%) do not routinely employ neuromonitoring in these lower-risk operations. This approximately 20.5% absolute difference between cord-level and sub-conus procedures underscores a deliberate, risk-stratified approach to IONM use. While cord-level surgery is almost universally monitored, the reduced—but still substantial—use below the conus suggests that factors such as case complexity, surgeon preference, institutional policy, and medicolegal considerations influence decision-making beyond anatomical risk alone. Surgeons’ performance of IONM during different procedures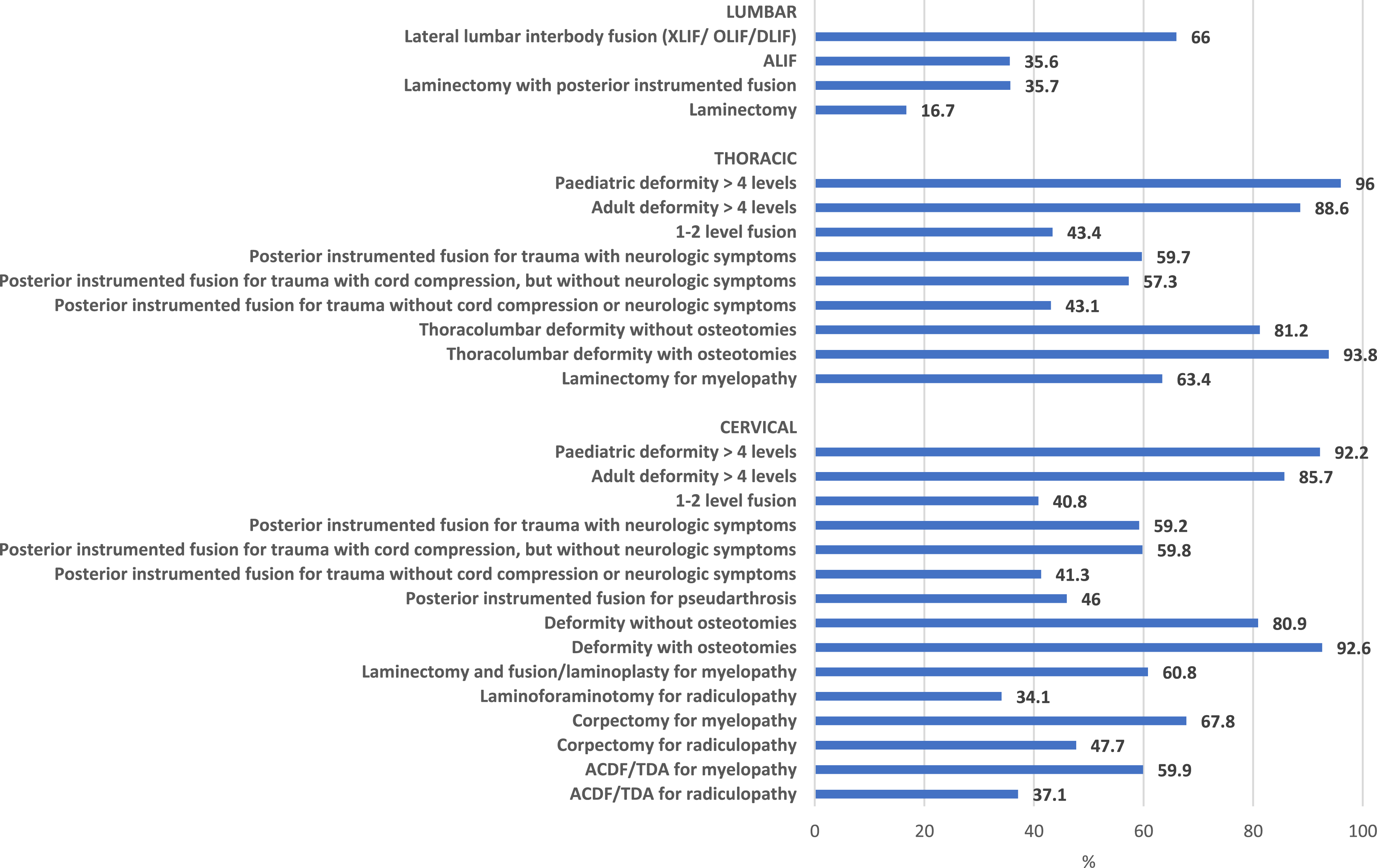
Perceived Importance of IONM by Surgical Condition
Figure 3 demonstrates a clear, risk-stratified pattern in surgeons’ opinions regarding the importance of intra-operative neuromonitoring (IONM). For high-risk procedures involving the spinal cord, such as deformity correction, intradural tumor surgery, and trauma-related spinal cord injury, IONM was rated as “necessary” by most respondents (approximately 80–90%), indicating strong consensus on its essential role in these settings. In intermediate-risk procedures, including complex degenerative surgery and revision operations, surgeons’ opinions were more distributed. In these categories, approximately 60–70% of respondents considered IONM essential, whereas a smaller proportion considered it unnecessary. For lower-risk procedures, particularly those performed below the conus, IONM was more frequently rated unnecessary, with only 30–40% of surgeons considering it essential. Surgeons’ beliefs about the importance of IONM use in different surgical conditions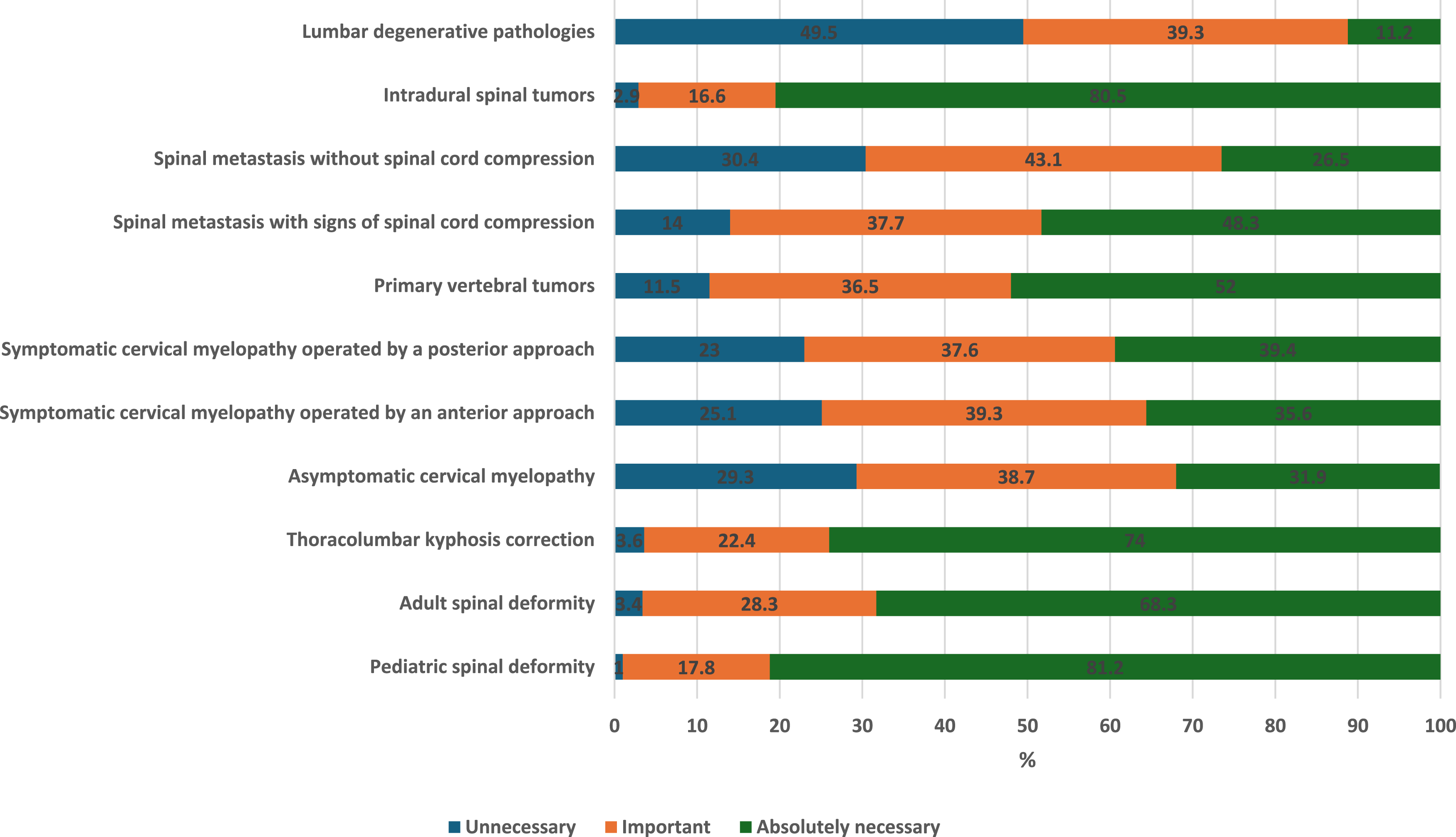
Overall, the percentages shown in Figure 3 indicate that surgeons’ perceptions of the importance of IONM are closely aligned with procedural risk. The data support a selective, indication-driven approach, with near-universal endorsement of IONM for high-risk spinal cord procedures and progressively lower perceived necessity as neurological risk decreases.
Discussion
This global survey provides a contemporary overview of intra-operative neuromonitoring (IONM) practices, attitudes, and perceived barriers among spine surgeons. The findings demonstrate that most respondents have regular access to IONM and hold predominantly positive attitudes toward its use, particularly regarding its role in improving patient outcomes, enhancing surgeon confidence, and providing medicolegal protection. These results align with prior reports indicating increasing acceptance of IONM as an adjunct for neurological safety in spine surgery.1,2,4
Despite generally favorable perceptions, access to IONM was not universal. While more than half of surgeons reported consistent availability, a substantial proportion reported only occasional or no access. This variability likely reflects differences in healthcare infrastructure, reimbursement models, and regional resource allocation. Previous studies have similarly highlighted disparities in IONM availability across institutions and geographic regions, particularly in low- and middle-income settings.1,5 The predominance of external service providers over in-house neuromonitoring models observed in this study may further exacerbate cost and logistical challenges, as outsourced models are often associated with higher procedural costs and scheduling constraints. 9
IONM utilization patterns in this cohort were largely risk-adapted. Our data showed nearly universal use during spinal cord–level surgery and reduced utilization for procedures below the conus, suggesting selective application based on perceived neurological risk. This finding is consistent with published guidelines and consensus statements that advocate the targeted use of IONM in complex deformity correction, tumor surgery, trauma, and other high-risk procedures.4,13 Surgeons’ reported beliefs regarding the importance of IONM across different surgical conditions further support this selective approach and reflect a nuanced understanding of its clinical value rather than routine, indiscriminate use.
Even though our survey covered lateral approaches, where 66% of participants reported using IONM during lateral lumbar interbody fusion, the specific dynamics of these procedures warrant special attention. IONM plays a highly specialized role in lateral surgeries, particularly sophisticated minimally invasive techniques, endoscopic procedures, and approaches such as anterior to psoas (ATP) and oblique lumbar interbody fusion (OLIF). Neuromonitoring is often used during these procedures to navigate the intricate retroperitoneal anatomy and reduce lumbar plexus risks. To maximize safety during changes in surgical corridors, this is a focused, risk-stratified application of neuromonitoring that goes beyond conventional spinal cord-level protection. In the end, prospective studies that evaluate various unimodal or multimodal IONM techniques and provide precise criteria of postoperative neurologic damage are required. 19
The evidence on the relative benefits and drawbacks of various therapeutic approaches in response to an IONM alert and potential acute spinal cord injury (SCI) is scarce. 20 The routine use of neuromonitoring in acute trauma is still a complicated and contentious topic that is regularly discussed at clinical conferences, even though a sizable section of our response pool consisted of surgeons who subspecialize in trauma and SCI (48.7%). Nearly two-thirds of surgeons preferred to use IONM in posterior instrumented fusion for cervical and thoracic injuries, as indicated by its use across various procedures in the current study (Figure 2). Pre-existing neurological impairments and spinal shock can significantly impair the capture of trustworthy baseline signals in acute SCI situations, making intraoperative interpretation more difficult. To prevent and reduce the risk of postoperative neurologic sequelae, a standardized checklist and treatment pathway are urgently needed. 20
However, the lack of agreement on monitoring indications is reflected in the variation among surgeons’ opinions on the requirement for IONM across various spine surgeries. The significance of IONM in high-risk spinal cord treatments, such as intradural tumor surgery and deformity repair, was almost universally acknowledged; however, opinions became significantly more divided in intermediate- and lower-risk procedures. 4 Variations in training background, regional practice patterns, medicolegal contexts, resource availability, institutional protocols, and interpretation of the current body of research are all likely contributing causes to this variation. Significantly, there is still debate in the literature about the usefulness and affordability of IONM for lower-risk degenerative treatments, which could lead to further disagreements among surgeons. 13 IONM was not helpful in a previous retrospective study 21 on the use of IONM during lumbar anterior approach surgery; many surgeons might feel compelled to employ IONM for medicolegal reasons. Future research is required to identify situations in which IONM is helpful and the type of monitoring, if any, that should be used for particular types of spine surgery.
Intra-operative interpretation of neuromonitoring data was most commonly performed by neuromonitoring technicians, with surgeons interpreting signals in approximately one-quarter of cases. This distribution reflects the multidisciplinary nature of IONM and mirrors findings from prior surveys. 3 However, reliance on non-physician interpreters underscores the importance of effective communication and standardized response protocols. The widespread use of checklists in response to unexpected signal changes observed in this study suggests increasing adoption of structured intra-operative algorithms, which have been shown to improve team communication and patient safety.7. Even though the majority of responders (76.3%) said they used a checklist approach, significant percentages completed wake-up tests, cancelled surgery right away, or attributed signal loss solely to neurophysiological or anesthetic factors. Rather than the result of mere ignorance, this heterogeneity most likely reflects variations in surgeon training, institutional culture, prior clinical experience, the availability of interdisciplinary IONM teams, and familiarity with troubleshooting methods. Evidence-based indications for IONM must be available to balance patient safety, medicolegal considerations, and healthcare costs.
Attitudinal analysis revealed strong agreement that IONM improves patient outcomes, provides medicolegal protection, and reassures surgeons intra-operatively. These findings are consistent with previous studies demonstrating that surgeons perceive IONM as both a clinical safeguard and a risk-management tool.1,6 Conversely, most respondents disagreed with statements questioning the necessity, cost-effectiveness, or preventive value of IONM, indicating that skepticism toward its utility is relatively uncommon among contemporary spine surgeons, despite ongoing debate in the literature regarding its role in lower-risk procedures. 8
Multivariate regression analysis identified geographic region, specialty, and access to IONM as independent predictors of a positive attitude toward its use. Notably, our data revealed a distinct divergence in perspectives between surgical specialties, with orthopedic surgeons showing a significantly more positive attitude toward IONM than neurosurgeons (OR=1.83). This difference in attitude may relate to fundamental variations in training paradigms or exposure to specific case mixes. For instance, orthopedic surgeons may manage a higher volume of complex, high-risk deformity corrections—where IONM is nearly universally endorsed—whereas neurosurgical training may foster different approaches to intraoperative risk assessment and medicolegal management. Furthermore, greater access to IONM was independently associated with a positive attitude, suggesting that familiarity, institutional culture, and routine use may reinforce confidence in its perceived clinical and protective benefits.
Economic constraints were the most frequently cited limitation to IONM use, followed by logistical barriers and lack of training. Cost has consistently been identified as a major impediment to the wider adoption of IONM, particularly in regions with limited reimbursement or bundled payment models.5,9 These findings underscore the need for cost-effective implementation strategies, expanded training opportunities, and clearer evidence-based guidelines to support appropriate use.
Limitations
This study has several limitations. Because this is a self-reported survey, the findings are subject to recall and response bias. Participation was limited to AO Spine members, which may limit generalizability. Further, the survey was distributed in English, which may not have been the primary language of many in this global audience. Additionally, reported practices may not reflect actual intraoperative behavior. Nonetheless, the large sample size and broad global representation provide valuable insight into current IONM practices and perceptions.
Conclusion
In conclusion, this global survey demonstrates that spine surgeons largely view IONM as a valuable adjunct in modern spine surgery, particularly for high-risk procedures. While access to and utilization of IONM vary across regions, positive attitudes toward IONM are widespread. Addressing economic, logistical, and training-related barriers may further facilitate the equitable and effective integration of IONM into spine care worldwide. Although IONM is valued for added safety and reassurance, its use is more discretionary and influenced by case complexity, surgeon experience, and institutional practice. However, the persistence of a sizable minority favoring IONM highlights the influence of non-clinical factors, such as medicolegal concerns, local protocols, and availability of neuromonitoring services.
Crucially, our results also imply that surgeons use IONM in a risk-stratified way, with spinal cord-level and deformity surgeries having the highest perceived necessity. However, ongoing efforts may be needed to establish evidence-based indications for IONM to balance patient safety, medicolegal considerations, and healthcare costs.
Therefore, the current findings highlight the significance of promoting global educational platforms, multicenter outcome studies, consensus conferences, and international collaboration through organizations such as AO Spine. Increased exchange of management algorithms, outcomes data, and procedural indications may help minimize unnecessary variation in practice and promote more evidence-based, risk-stratified IONM use globally.
Supplemental Material
Supplemental material - A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons
Supplemental material for A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons by Sameh Abolfotouh, Mason Alnouri, Stephen Lewis, Krishna Kumar and Mostafa A. Abolfotouh in Global Spine Journal.
Supplemental Material
Supplemental material - A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons
Supplemental material for A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons by Sameh Abolfotouh, Mason Alnouri, Stephen Lewis, Krishna Kumar and Mostafa A. Abolfotouh in Global Spine Journal.
Supplemental Material
Supplemental material - A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons
Supplemental material for A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons by Sameh Abolfotouh, Mason Alnouri, Stephen Lewis, Krishna Kumar and Mostafa A. Abolfotouh in Global Spine Journal.
Supplemental Material
Supplemental material - A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons
Supplemental material for A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons by Sameh Abolfotouh, Mason Alnouri, Stephen Lewis, Krishna Kumar and Mostafa A. Abolfotouh in Global Spine Journal.
Supplemental Material
Supplemental material - A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons
Supplemental material for A Global Survey on Intra-operative Neuromonitoring (IONM) Practices, Attitudes Towards Its Use, and Barriers Among Spine Surgeons by Sameh Abolfotouh, Mason Alnouri, Stephen Lewis, Krishna Kumar and Mostafa A. Abolfotouh in Global Spine Journal.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Deformity. AO Spine is a clinical specialty of the AO Foundation, which is an independent, medically guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and/or publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.