
Abstract
Study Design
Retrospective cross-sectional study.
Objective
To evaluate national trends in utilization and inflation-adjusted charges for single-level posterior cervical decompression and fusion (PCDF) performed in hospital-owned ambulatory surgery centers (ASCs).
Methods
The National Ambulatory Surgery Sample was queried from 2016 to 2022 for adult ASC encounters with CPT 22600, corresponding to single-level posterior cervical fusion. Survey-weighted methods estimated national volumes and modeled adjusted charges using generalized linear models. Statistical significance was set at P< 0.05.
Results
A weighted total of 8,609 single-level PCDF procedures were performed in hospital-owned ASCs from 2016 to 2022 (unweighted n = 6,505). Annual volume increased from 577 cases in 2016 to 3,307 cases in 2021 before declining to 1,586 cases in 2022. Median inflation-adjusted charges rose from $41,697 in 2016 to $69,255 in 2022 (P < 0.001). Adjusted mean charges varied significantly by payer and region, with higher charges for private insurance versus Medicaid ($62,621 vs $50,095, P < 0.001) and for the West versus the Northeast ($93,278 vs $19,847, P < 0.001), based on adequate regional sample sizes (unweighted n = 653 and n = 1,557, respectively). Medicare demonstrated the fastest annual charge growth, higher than Medicaid (+10.35%/year, P = 0.004), private (+12.31%/year, P < 0.001), and Other (+11.87%/year, P < 0.001).
Conclusions
Outpatient PCDF adoption in ASCs rose sharply from 2016 to 2021 with persistent, pronounced regional and payer-associated charge variation. These findings suggest that geographic pricing ecosystems and payer dynamics are key drivers of outpatient PCDF economics.
Keywords
Introduction
Posterior cervical decompression and fusion (PCDF) is a well-established treatment for cervical radiculopathy and myelopathy, and nationwide procedure rates have risen markedly in recent years.1,2 Compared with anterior cervical discectomy and fusion (ACDF) — the most commonly performed cervical spine operation — PCDF offers several advantages in appropriately selected patients, including lower reoperation rates, reduced postoperative dysphagia, and particular utility for multilevel fusion or extensive posterior decompression.3,4 However, PCDF requires substantial posterior dissection and muscle retraction, leading to greater postoperative pain and longer hospital stays relative to ACDF and other anterior approaches.5,6 Advanced imaging to delineate disc degeneration and nerve compression, especially the number of affected levels, guides the decision between PCDF, ACDF, and alternative techniques. 7 Despite its more demanding recovery profile, PCDF remains widely used because it can minimize long-term complications and repeat surgery, making it a valuable option for patients with complex cervical pathology. 1
As procedural volume and health-care expenditures continue to climb, characterizing PCDF utilization across payer groups, seasons, and geographic regions is increasingly important. For example, Lima et al. found that Medicare Advantage beneficiaries in Florida had significantly less access to spine surgeons than those with traditional Medicare or private insurance, highlighting payer-level disparities among older adults. 8 Wang et al. likewise documented marked geographic variation in cervical fusion rates, with the highest utilization in the Northwest and South Central United States (U.S.). 9 Concurrently, spine surgery is steadily migrating to outpatient venues, especially ambulatory surgery centers (ASCs). 10 Understanding how this shift affects PCDF adoption, costs, and payer mix will inform policy and clinical decision-making.
Because surgical choices are shaped by both clinical complexity and system-level factors — such as payer status, regional practice norms, and seasonal variation — examining PCDF through these lenses offers critical insight into evolving outpatient spine care. Focusing specifically on single-level PCDF further refines this analysis by isolating a more standardized, commonly selected outpatient fusion construct that remains technically demanding and implant-intensive, thereby providing a clearer understanding of utilization patterns and cost drivers in the ASC setting. Accordingly, this study aims to (1) evaluate temporal trends in procedure volume and facility-adjusted charges for single-level PCDF, (2) compare utilization and charge patterns across payer types, geographic regions, and seasons, and (3) determine how patient, hospital, and procedural factors influence charge and regional growth over time. We hypothesized that overall utilization and inflation-adjusted charges for PCDF would increase during the study period, particularly among privately insured patients and in high-income, urban regions.
Materials and Methods
Data Source
This retrospective cross-sectional study used data from the National Ambulatory Surgery Sample (NASS) for the years 2016 through 2022. Developed as part of the Healthcare Cost and Utilization Project (HCUP), NASS is a nationally representative database that captures encounter-level information from hospital-owned ASCs across the U.S., excluding physician-owned freestanding ASCs, which may differ in payer mix, patient selection, and practice patterns. 11 Discharge-level weights provided by HCUP were applied to generate national estimates using survey-weighted methods consistent with best practices.
Procedure Identification
Procedures were identified using Current Procedural Terminology (CPT) code 22600, which corresponds to single-level PCDF. To isolate standalone fusion cases, records were excluded if they contained CPT code 22614 (each additional posterior segment), any anterior cervical fusion codes (22551, 22552), or cervical disc arthroplasty codes (22856, 22858, 22861, 22864). Encounters containing CPT 22600 in combination with any excluded anterior fusion, multilevel posterior fusion, or cervical disc arthroplasty codes were removed to avoid inclusion of hybrid, multilevel, or otherwise non-standalone posterior cervical fusion cases.
Inclusion and Exclusion Criteria
Eligible patients were adults aged 18 years or older undergoing PCDF procedures in the outpatient setting during the study period. Encounters were excluded if they had missing or invalid discharge weights, missing data for sex, age, income quartile, hospital region, rural/urban status, or primary payer, or if total charges were zero or negative. All charge values were inflation-adjusted to 2022 U.S. dollars using year-specific Medical Consumer Price Index (CPI) multipliers. 12 Specifically, annual multipliers were derived by dividing the 2022 Medical CPI by the Medical CPI for each study year and then applying these factors to reported charges. To reduce the influence of extreme outliers, adjusted charges were winsorized at the 1st and 99th percentiles.
Decompression Subgroup Classification
Cases were further categorized based on the presence or absence of concomitant decompression. Posterior decompression was defined as any concurrent CPT code for cervical laminectomy, including 63001, 63015, 63020, 63030, 63035, 63040, 63045, or 63048. Encounters with any of these codes were classified as PCDF with decompression; all others were considered fusion alone. Of the included procedures, 4,003 (weighted n = 5,407) were performed without laminectomy and 2,502 (weighted n = 3,202) included concomitant decompression.
Variables and Outcomes of Interest
Patient-level variables included age, sex, and median household income quartile based on ZIP code of residence. Hospital characteristics included U.S. Census region (Northeast, Midwest, South, West) and rural versus urban location. Primary payer was categorized as Medicare, Medicaid, Private Insurance, or Other. Season of surgery was assigned using calendar month and grouped as Winter (December–February), Spring (March–May), Summer (June–August), or Fall (September–November). The primary outcomes of interest were inflation-adjusted total charges per encounter, total national procedure volume, and annual market share by payer, region, and season.
Statistical Analyses
All analyses were conducted using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). A survey design object was created using the survey package to account for the complex sampling structure of NASS, incorporating discharge weights as well as the dataset’s sampling strata and cluster design to generate nationally representative estimates. All descriptive analyses and generalized linear models were fit within this survey design framework so that design weights were incorporated directly into estimation. Descriptive statistics summarized patient, hospital, and procedural characteristics, with categorical variables compared using Rao–Scott chi-square tests and continuous variables compared using design-based Kruskal–Wallis tests. Statistical significance was defined as P < 0.05.
Adjusted charge analyses were performed using survey-weighted generalized linear models (GLMs) with a log-link and gamma distribution, modeling inflation-adjusted total charges as the dependent variable. Separate models evaluated charge differences by payer, region, and season. Marginal means were back-transformed from the log scale to yield geometric mean charges with 95% confidence intervals. Post hoc contrasts were Tukey-adjusted, with Bonferroni correction applied when appropriate. To assess robustness of regional charge differences, we additionally examined weighted median and interquartile range (IQR) by region.
To assess charge trends over time, year was modeled as a continuous variable to evaluate overall temporal trends, with interaction terms included to capture group-specific differences in annual growth. Pairwise comparisons of marginal slope estimates were conducted using Wald tests. Procedure volume trends were analyzed by estimating annual weighted totals and comparing group-specific linear trends over time. Market share was defined as the proportion of annual PCDF procedures attributable to each payer, region, or season and modeled using inverse-variance weighted linear regression to assess directional change over the study period.
Results
Patient Characteristics and Procedure Volume
Patient Demographics, Socioeconomic, and Payer Characteristics by Year (2016–2022)
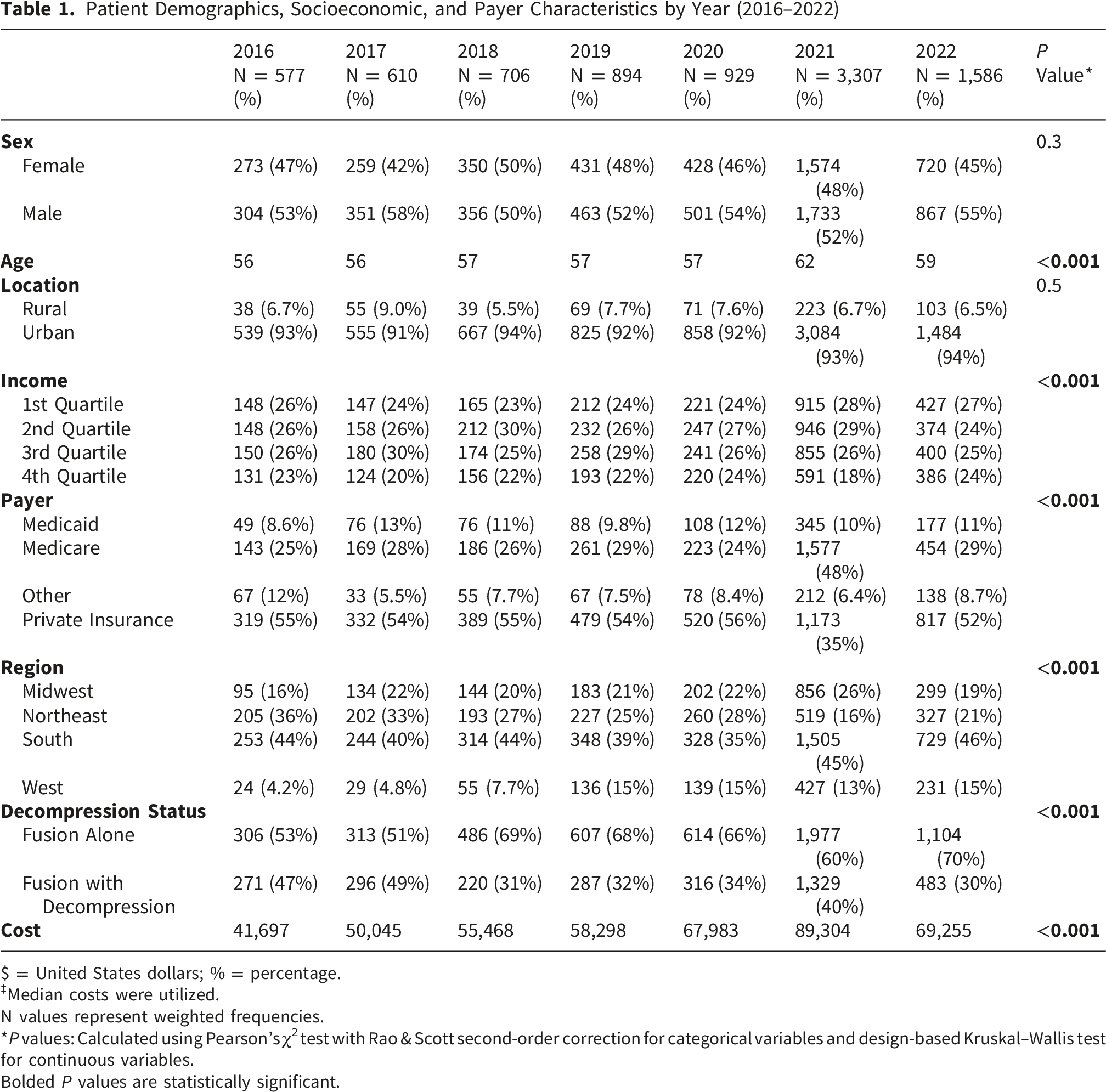
$ = United States dollars; % = percentage.
‡Median costs were utilized.
N values represent weighted frequencies.
*P values: Calculated using Pearson’s χ2 test with Rao & Scott second-order correction for categorical variables and design-based Kruskal–Wallis test for continuous variables.
Bolded P values are statistically significant.
Payer distribution shifted notably over time (P < 0.001), with Medicare utilization increasing from 25% in 2016 to 48% in 2021, before stabilizing at 29% in 2022. Conversely, the proportion of privately insured patients declined from 55% to 35% before rebounding to 52%. Regionally, the South consistently accounted for the largest share of procedures (39–46%), while the West experienced the greatest relative growth, increasing from 4.2% in 2016 to 15% by 2022 (P < 0.001). There was a significant increase in the proportion of cases performed as fusion alone rather than fusion with decompression (P < 0.001), alongside a nearly 66% increase in median adjusted charges, rising from $41,697 in 2016 to $69,255 in 2022 (Table 1).
Adjusted Procedure Charges by Payer, Region, and Season
Adjusted Mean Per-Procedure Charges for Single-Level PCF by Payer, Region, and Season, 2016–2022
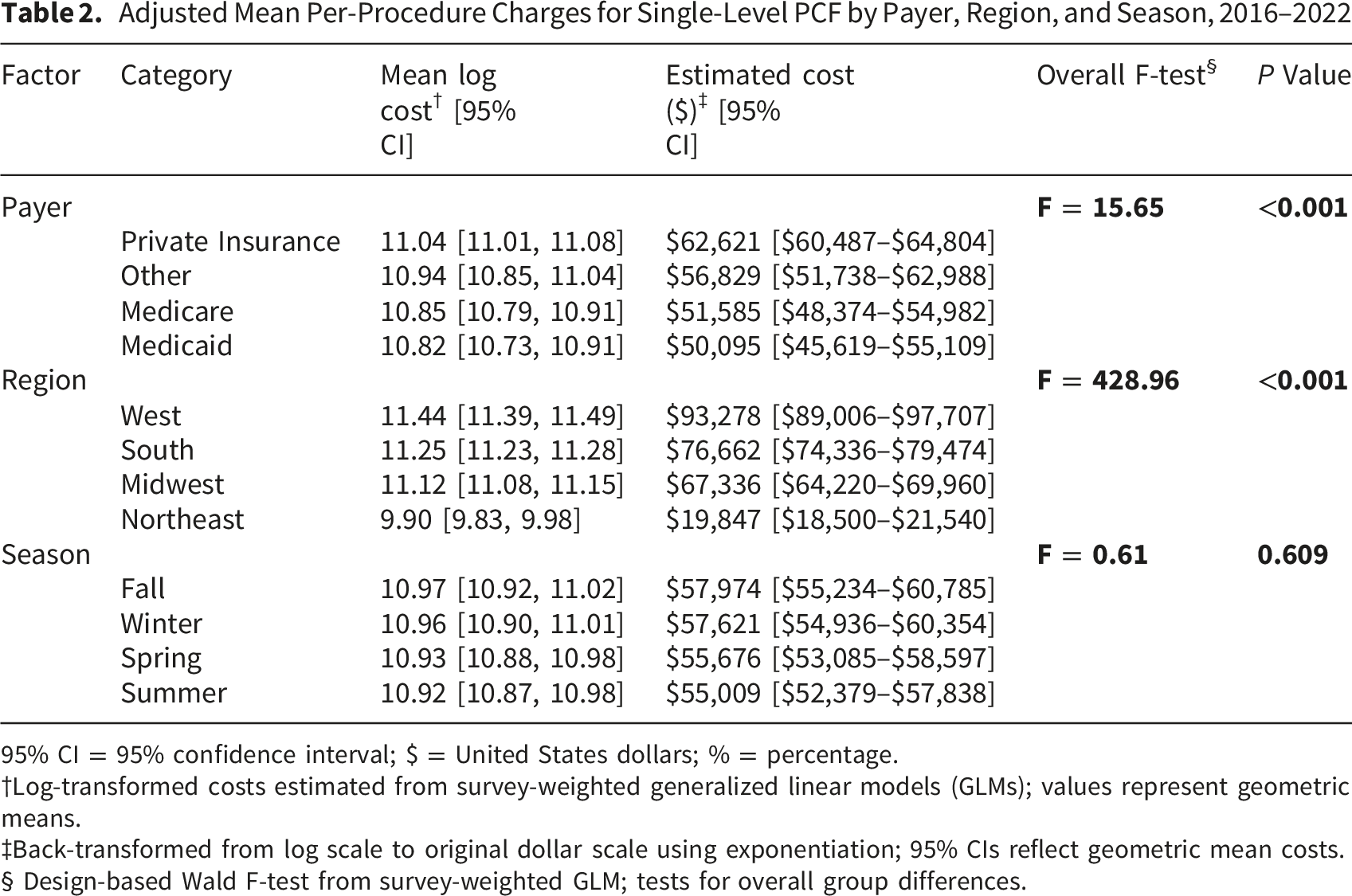
95% CI = 95% confidence interval; $ = United States dollars; % = percentage.
†Log-transformed costs estimated from survey-weighted generalized linear models (GLMs); values represent geometric means.
‡Back-transformed from log scale to original dollar scale using exponentiation; 95% CIs reflect geometric mean costs.
§ Design-based Wald F-test from survey-weighted GLM; tests for overall group differences.
Regional charge differences were pronounced (F = 428.96, P < 0.001). Procedures in the West had the highest adjusted mean charge ($93,278; unweighted n = 653), while those in the Northeast were substantially less expensive ($19,847; unweighted n = 1,557) (Table 2, Figure 1). Seasonal differences were not statistically significant (P = 0.609), with estimated mean charges ranging narrowly between $55,009 (Summer) and $57,974 (Fall) (Table 2). Adjusted mean charges for single-level PCF by U.S. Census region from 2016 to 2022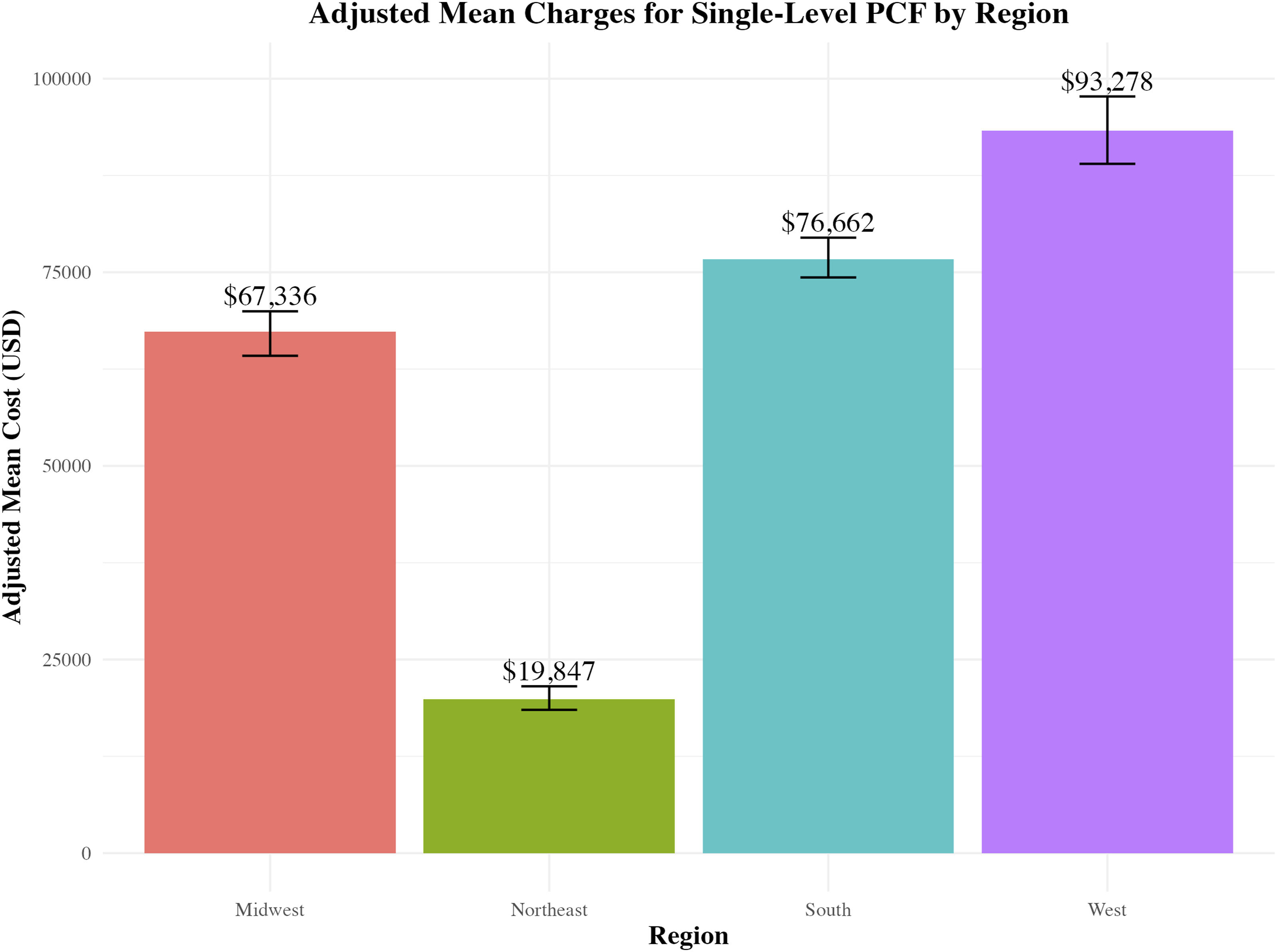
Pairwise Charge Comparisons
Significant Pairwise Comparisons of Adjusted Mean Costs for Single-Level PCF by Payer and Region (2016–2022)
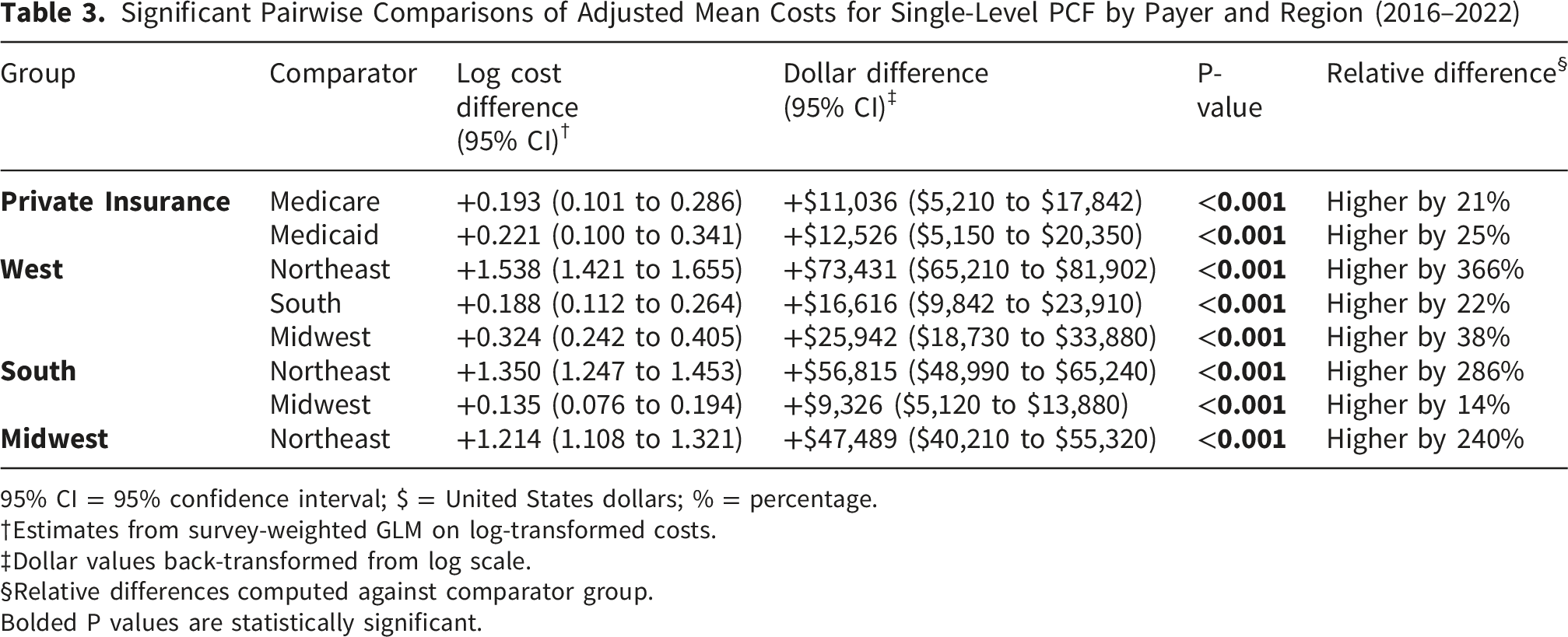
95% CI = 95% confidence interval; $ = United States dollars; % = percentage.
†Estimates from survey-weighted GLM on log-transformed costs.
‡Dollar values back-transformed from log scale.
§Relative differences computed against comparator group.
Bolded P values are statistically significant.
Regional contrasts were even more striking. Procedures in the West were associated with charges that were $73,431 (or 366%) higher than those in the Northeast (P < 0.001). The South and Midwest also had significantly higher charges than the Northeast by $56,815 (+286%) and $47,489 (+240%), respectively. The West remained significantly more costly than the South (+$16,616, +22%) and Midwest (+$25,942, +38%) (Table 3, Figure 1).
This regional gradient was also present in distribution-based summaries. Weighted median charges increased from $38,560 (IQR, $11,215–$81,495) in the Northeast to $95,549 (IQR, $62,275–$140,655) in the West, with the Midwest ($75,211 [IQR, $49,209–$107,077]) and South ($86,677 [IQR, $54,228–$132,325]) displaying intermediate values.
Differences in Charge Growth Trends
Significant Pairwise Comparisons of Annual Cost Growth Rates for Single-Level PCF Procedures by Payer and Region (2016–2022)
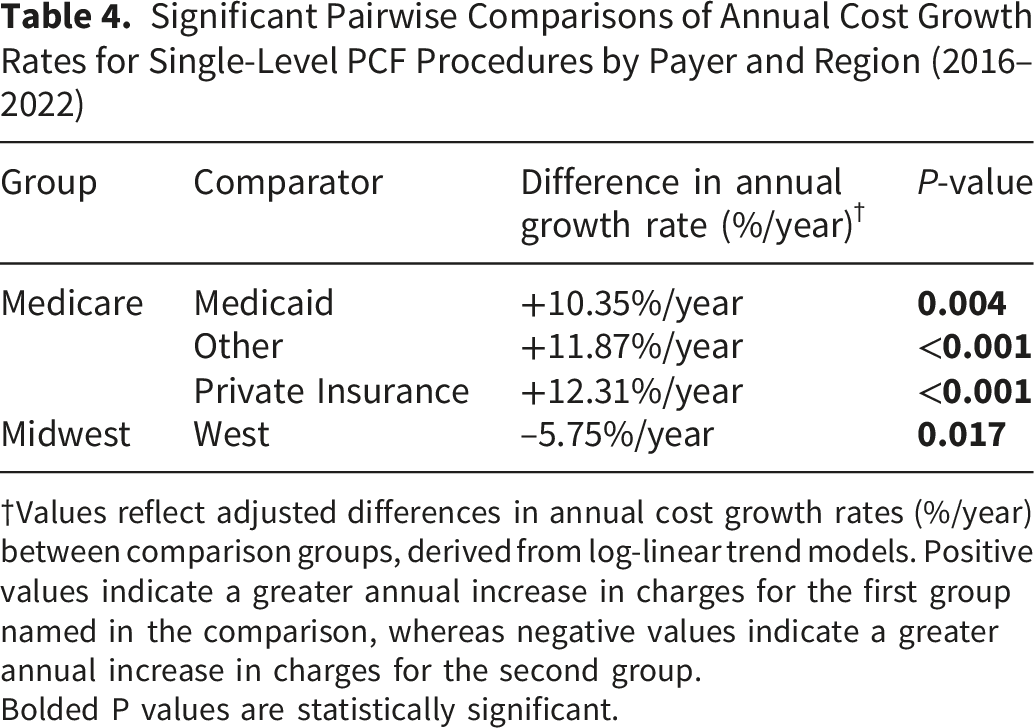
†Values reflect adjusted differences in annual cost growth rates (%/year) between comparison groups, derived from log-linear trend models. Positive values indicate a greater annual increase in charges for the first group named in the comparison, whereas negative values indicate a greater annual increase in charges for the second group.
Bolded P values are statistically significant.
Market Share and Utilization Trends
Market Share Trends in Single-Level PCF Procedures by Payer, Region, and Season (2016–2022)
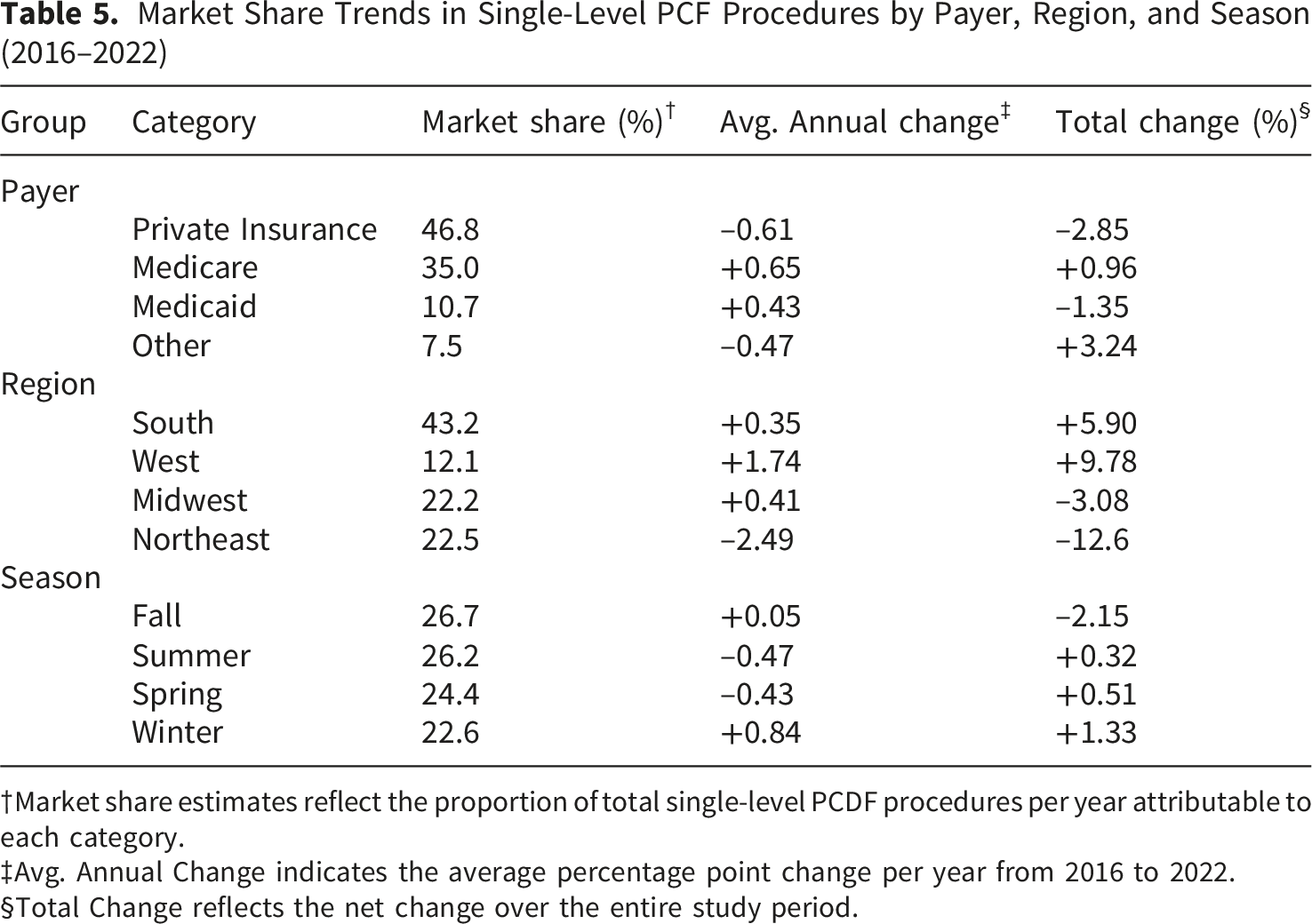
†Market share estimates reflect the proportion of total single-level PCDF procedures per year attributable to each category.
‡Avg. Annual Change indicates the average percentage point change per year from 2016 to 2022.
§Total Change reflects the net change over the entire study period.
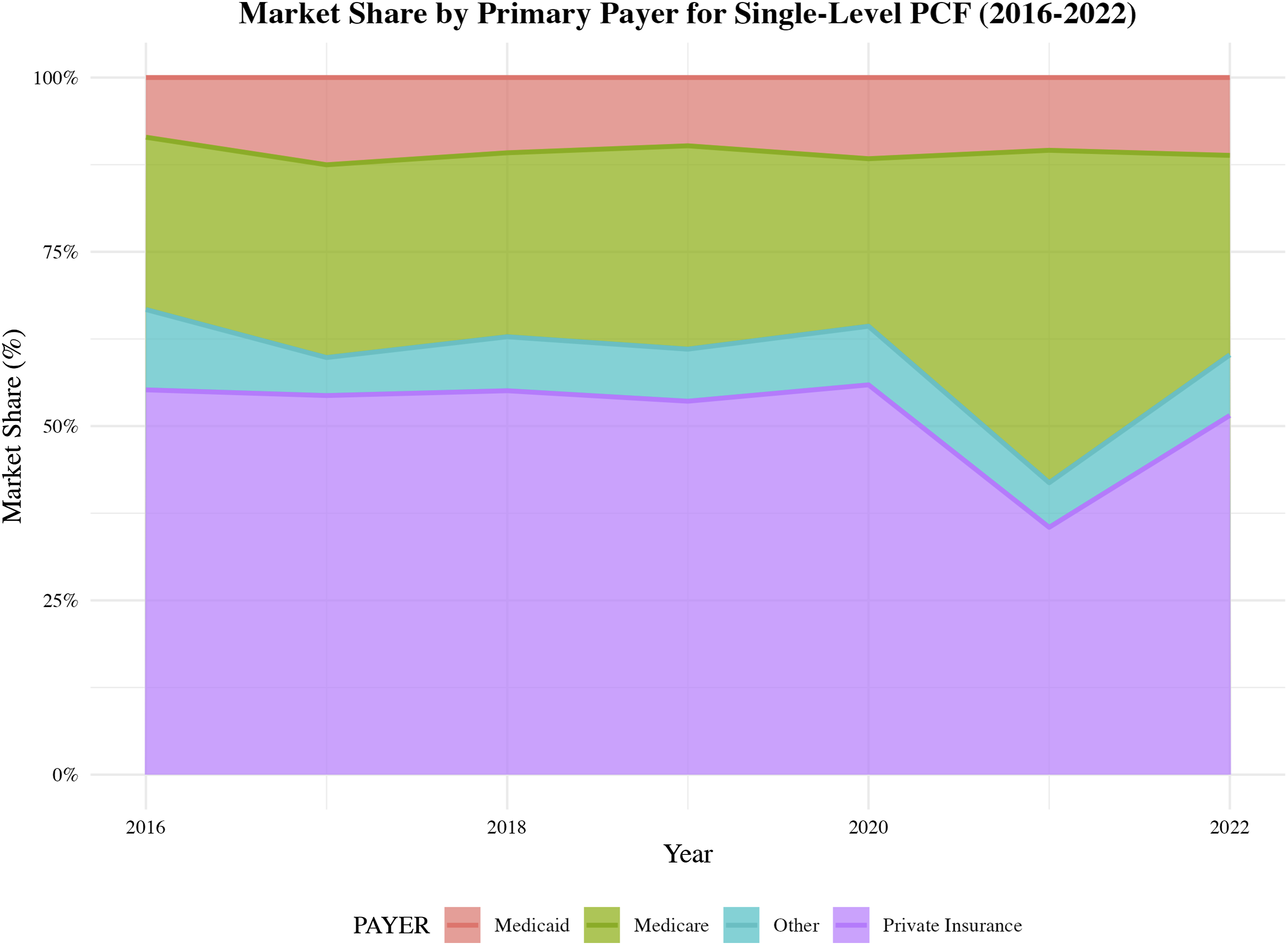
Market share trends by primary payer for single-level PCF procedures from 2016 to 2022
Seasonal variation in market share was minimal. Fall remained the most common season for PCDF procedures (26.7%), followed closely by Summer (26.2%), Spring (24.4%), and Winter (22.6%), with only minor changes over time (Table 5).
Top Diagnoses
The most common primary diagnosis code for single-level PCDF was spinal stenosis of the cervical region (M4802), followed by pseudarthrosis after fusion (M960) and cervical spondylosis with myelopathy (M4712), reflecting typical surgical indications in this cohort (Figure 3). Top 10 most frequent primary diagnosis codes for single-level PCF procedures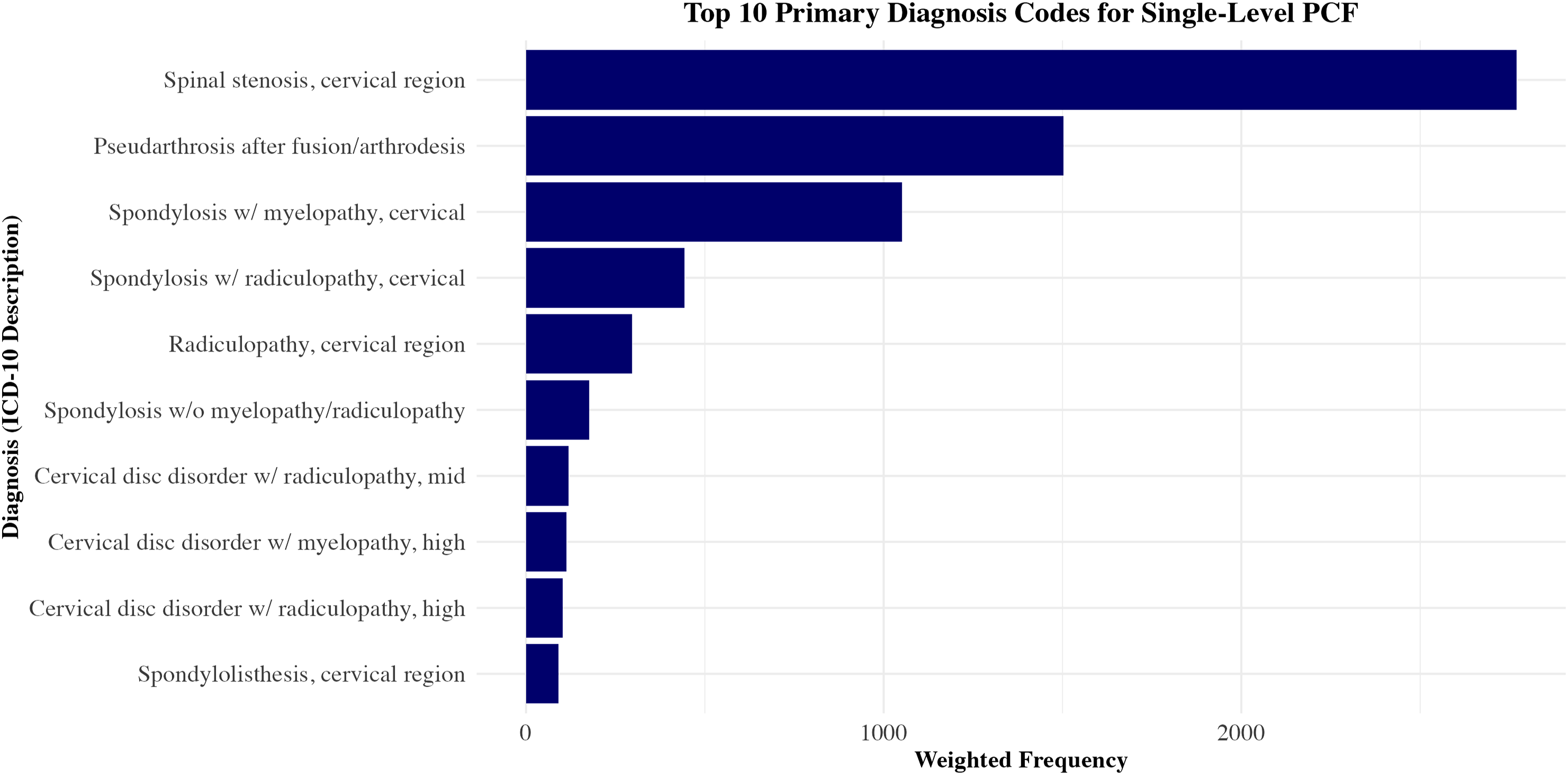
Discussion
In this national evaluation of single-level PCDF performed in hospital-owned ASCs from 2016 through 2022, we observed a rapid but uneven outpatient adoption, marked payer-mix shifts, and striking geographic charge variation. Weighted encounter volume climbed more than five-fold — from 577 cases in 2016 to a peak of 3,307 in 2021 — before contracting to 1,586 cases in 2022. During the same interval, median patient age increased by three years and Medicare’s share of ASC cases nearly doubled before settling at 29% in 2022, mirroring the transient pandemic-era push of older, frailer patients to outpatient sites. Despite inflation adjustment, geometric mean charges averaged $57,600, yet procedures in the West were almost four times costlier than those in the Northeast ($93,278 vs $19,847), and privately insured encounters out-priced Medicaid by approximately $12,500 per case. These patterns highlight both the momentum and the inefficiencies accompanying PCDF’s migration to ASCs.
Annual PCDF volume surged from 577 encounters in 2016 to 3,307 in 2021 before moderating in 2022, mirroring the early-pandemic shift of elective spine surgery to ASCs reported using the American College of Surgeons National Surgical Quality Improvement Program database. 13 During this interval, the median patient age rose by three years and the share of Medicare beneficiaries nearly doubled, underscoring that ASCs are increasingly managing older, more medically complex patients. Notably, Medicare share rose from 25% in 2016 to 48% in 2021 before declining to 29% in 2022, a pattern that may reflect pandemic-related shifts in outpatient case selection, recovery of elective surgical volume, and year-to-year variation in the composition of hospital-owned ASC encounters captured in NASS. Mean facility-adjusted charges climbed from $42,000 to $58,000, well above the CPI, and parallel the upward spending trajectory described for other outpatient cervical procedures. 14 This expansion coincided with a shift toward fusion-alone constructs and a five-fold increase in Western cases, developments that likely intensified implant and labor expenditures. Medicare encounters also showed the fastest year-over-year charge growth; however, this finding should be interpreted in the context of the marked fluctuation in Medicare case share over the study period, which may reflect changes in case mix, pandemic-related shifts in outpatient utilization, or year-to-year variation in reporting and dataset composition.
Charge inflation was steeper for Medicare cases by 10-12% per year than for commercially insured encounters. Geographically, the West remained the costliest region throughout the study window, with 2022 charges nearly four-times those in the Northeast; similar West-to-Northeast differentials have not been reported for inpatient PCDF and therefore appear amplified in the ASC setting. 15 Given the magnitude of these charge differences, these findings should be considered hypothesis-generating, reflecting structural and market-level variation in ASC charge practices, payer contracting, case selection, and regional healthcare pricing rather than a definitive causal regional effect. Seasonal analysis showed peak volumes and highest per-case charges in the fourth quarter, consistent with pre-deductible behavior in privately insured patients and end-of-year scheduling pressures in hospital-owned ASCs. Taken together, these findings highlight how payer behavior and local practice norms shape both access to and the pricing of outpatient PCDF. Future studies using reimbursement and resource utilization data are needed to identify the mechanisms underlying outpatient PCDF charge variation and determine whether these patterns affect healthcare efficiency and access to specialized spine care.
Shifts in patient demographics, such as the rise in median age from 56 to 59 years and a proportional increase in Medicare beneficiaries, were associated with the most pronounced annual charge inflation, consistent with registry evidence linking frailty indicators to higher resource utilization in outpatient PCDF.13,16 Market forces may also have shaped pricing, as even among predominantly urban facilities, Western sites demonstrated substantially higher charges; however, potential contributors such as regional labor costs, implant contracting, and payer negotiations should be regarded as hypotheses rather than directly measured drivers in the present dataset.14,15 Finally, the growing preference for fusion-alone techniques, although clinically aligned with current guidelines for the treatment of myelopathy, was associated with a 66% jump in median inflation-adjusted charges, underscoring the budgetary impact of implant-intensive strategies. 17 Collectively, these findings suggest that patient ageing, region-specific market forces, and evolving operative preferences may contribute to trends in outpatient PCDF charges.
This study is subject to several limitations common to large administrative datasets. The NASS database captures only hospital-owned ASCs, excluding physician-owned centers where adoption rates and cost structures may differ markedly. As a result, the findings from this study may only reflect a subset of patients undergoing outpatient PCDF and, therefore, may not be generalizable to private ASCs, inpatient hospitals, or other surgical settings, where higher-acuity patients may be treated. Reported charges, even after CPI adjustment, are list prices that do not reflect negotiated payments or patient out-of-pocket liability. We relied on geometric means to summarize highly skewed charge data; although this approach mitigates the influence of extreme values, it may obscure clinically meaningful charge outliers. Importantly, the economic outcomes captured in this study were limited to charges, which may not directly reflect true procedural costs, reimbursements, or underlying resource utilization. Rather, these values represent billed amounts and may vary substantially across hospitals, regions, and payer-specific contracting arrangements. Accordingly, the observed differences should be interpreted as variation in charges rather than direct measures of economic value or efficiency. The markedly lower charges observed in the Northeast should therefore be interpreted cautiously, as they may reflect geographic differences in billing practices, coding patterns, payer contracting, and outpatient site-of-service composition rather than true differences in procedural complexity or resource utilization. Exclusion of encounters with zero or negative reported charges, while necessary to ensure data validity, may introduce bias if such values are differentially distributed across payer, region, or time. The dataset also lacks granular clinical details, precluding evaluation of fusion levels, implant selection, radiographic alignment, operative time, surgeon experience, or post-discharge complications beyond 30 days. Analyses were restricted to single-level PCDF, limiting generalizability to multilevel constructs. Although a wide range of laminectomy codes were used to capture cases involving decompression, this approach may not fully identify patients who underwent foraminotomy or other limited decompressions, potentially leading to misclassification. In addition, regional variation in coding practices, including undercoding or overcoding of decompression-related procedures, may have influenced subgroup assignment and should be considered when interpreting stratified regional analyses. Potential miscoding and pandemic-related care disruptions introduce additional uncertainty. In addition, year-to-year changes in the composition of hospitals and hospital-owned ASCs contributing to NASS may have influenced observed temporal trends independent of true changes in procedure utilization or charges. Because year was modeled as a continuous variable, trend estimates should be interpreted as average annual changes and may not fully capture non-linear patterns, including the increase in outpatient PCDF volume through 2021 followed by the decline in 2022. Although CPT 22600 was used to identify single-level PCDF and concurrent multilevel or anterior fusion codes were excluded, coding variation may still have resulted in occasional misclassification of combined or multilevel procedures as single-level cases. Residual confounding is inevitable despite survey weighting and model adjustment; consequently, causal inferences should be interpreted with caution.
Conclusions
Outpatient single-level PCDF volumes grew five-fold from 2016 to 2021 while the case mix aged and Medicare’s share nearly doubled, yet charges diverged dramatically — reaching a four-to-one difference between Western and Northeastern markets. These findings underscore that the migration to ASCs is being driven as much by payer dynamics and regional pricing ecosystems as by clinical demand. To ensure the transition improves value rather than inflating list prices, stakeholders should target modifiable levers such as implant contracting, labor costs, and regional payment policies, with particular attention to high-charge Western centers. Future research incorporating physician-owned ASC data, longer-term outcomes, and real-world reimbursement figures is essential to refine patient selection and guide cost-containment strategies.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.