
Abstract
Study Design/Setting
Systematic review and meta-analysis.
Objectives
Anterior cervical discectomy and fusion (ACDF) is a well-established treatment for degenerative cervical pathology. Although outcomes following 1- and 2-level ACDF are favorable, increasing construct length has been associated with worse outcomes. Despite this, 3- and 4-level ACDF are often grouped as “multilevel” constructs, though emerging evidence suggests 4-level ACDF may carry greater risk. This study systematically reviewed the literature and performed a meta-analysis comparing outcomes between 3- and 4-level ACDF.
Methods
A systematic search of MEDLINE, Embase, and Cochrane databases was performed per PRISMA guidelines. Studies reporting outcomes following three- or four-level ACDF were included.
Results
Both 3- and 4-level ACDF improved pain, disability, and neurologic function. Meta-analysis showed 4-level ACDF had less improvement in axial neck pain, with similar arm pain improvement. Fusion rates were lower with 4-level ACDF. Perioperative outcomes favored 3-level constructs, with 4-level ACDF associated with longer operative time, greater blood loss, and longer hospital stay. No significant differences were observed in complication or revision rates, though confidence intervals were wide.
Conclusions
Both procedures improved pain and function. However, 4-level ACDF showed less neck pain improvement, lower fusion rates, and greater perioperative morbidity. Meta-analysis reveals clinically meaningful differences that should inform surgical planning and patient counseling.
Introduction
Anterior cervical discectomy and fusion (ACDF) is a well-established surgical treatment for degenerative cervical spine pathology resulting in radiculopathy and myelopathy.1-4 By achieving neural decompression and interbody fusion, ACDF improves radicular symptoms, prevents neurologic deterioration associated with cervical myelopathy, and restores spinal stability.5-7 While outcomes following one- and two-level ACDF are generally favorable, increasing construct length has been associated with higher complication rates, diminished improvement in patient-reported outcomes (PROs), and lower rates of fusion.8-12
As construct length increases, ACDF is associated with greater operative morbidity, including longer operative time, increased estimated blood loss, higher rates of dysphagia, and increased risk of pseudoarthrosis and revision surgery.8,9,13-15 Despite this, 3- and 4-level ACDF are often grouped together as “multilevel” constructs in both clinical practice and literature, which implicitly suggests equivalence in outcomes.16,17 However, emerging evidence suggests that this assumption may be invalid. Recent large administrative database studies have demonstrated higher rates of adverse events, reoperation, and dysphagia following 4-level ACDF compared to shorter constructs, whereas 3-level ACDF does not show such differences. 18
Although a prior meta-analysis has compared 3- and 4-level ACDF in patients with cervical spondylotic myelopathy, a comprehensive systematic review of patient-reported outcomes, fusion success, and perioperative morbidity across the broader spectrum of degenerative cervical pathology has not been performed.
19
As such, the primary objective of this study was to systematically evaluate outcomes following 3- and 4-level ACDF, with secondary aims including meta-analysis of directly comparative cohorts to clarify clinically meaningful difference between these constructs and better define the risks associated with increasing construct length.
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was not prospectively registered in PROSPERO; however, the research question, inclusion and exclusion criteria, search strategy, and outcome measures were defined a priori prior to data extraction.
Search Strategy
Three online databases (PubMed, Ovid Medline, and EMBASE) were queried for articles discussing clinical outcomes following 3- or 4-level anterior cervical discectomy and fusion (ACDF) from database inception to August 2024.
Study Screening
Study screening for the titles, abstracts, and full-text articles was performed by three independent reviewers (R.P., R.S., A.B.) and in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines.
Assessment of Study Eligibility
The research question and criteria for eligible studies were established a priori. The inclusion criteria were: English language studies, human studies, level of evidence I to IV, and studies investigating clinical outcomes in patients following 3- or 4- level ACDF. Studies that combined data for 3- or 4-level ACDF with 1- or 2-level surgeries were excluded. Studies that did not report clinical outcomes were excluded. Studies with cohorts that contained revision surgeries, surgery for traumatic injury, and surgery for infectious or oncologic etiologies were excluded.
Data Abstraction & Statistical Analysis
Data was collected by two reviewers and recorded using Microsoft Excel (Version 2019, Microsoft, Redmond, WA, USA). Author information, year of publication, study design, and sample sizes were abstracted. Demographics, clinical outcome scores, complication data, and fusion rates were collected.
Data were extracted and reported as means, ranges, and percentiles, directly from the results of each individual study. Meta-analysis was performed to compare several outcome measures between the 3- and 4-level ACDF cohorts: a) Overall VAS, b) NDI, c) JOA, d), fusion rate, e) LOS, f) EBL, and g) operative time. Studies were included in the meta-analysis if they directly compared 3- and 4-level ACDF, and if data were provided in an appropriate format for statistical analysis. Specifically, continuous variables were required to be presented with a mean, a measure of variability (i.e. standard deviation or standard error), and sample size.
For continuous variables, a random-effects, inverse-variance weighted model was used to generate a pooled effect size across studies. A restricted maximum-likelihood (REML) estimator was used to assess heterogeneity variance. Pooled effect size was reported as Cohen’s d value. For categorical variables, a random-effects, inverse-variance model was used to generate pooled effect size across studies. An REML estimator was again used to assess heterogeneity across studies. Pooled effect size was reported as log risk ratio. Egger’s regression test and Funnel plots were used to assess for presence of publication or other systemic bias across studies. Statistical significance was defined as p<0.05. All statistical analyses were completed using IBM SPSS Version 24.0 (IBM Corp).
Results
Study Characteristics
An initial 1047 publications were identified across the electronic database search. A total of 65 cohorts across 49 studies were included in the final quantitative analysis (Figure 1), comprising 27 cohort studies, 21 case series, and 1 randomized control trial (Supplemental Table 1). Of the included studies, 44 were retrospective and 5 were prospective. Publication years ranged from 1997 to 2022. The systematic review included 41 3-level ACDF cohorts and 24 4-level ACDF cohorts. Among these, 6 studies directly comparing 3- and 4-level constructs were eligible for inclusion in meta-analysis. Prisma flowchart of study eligibility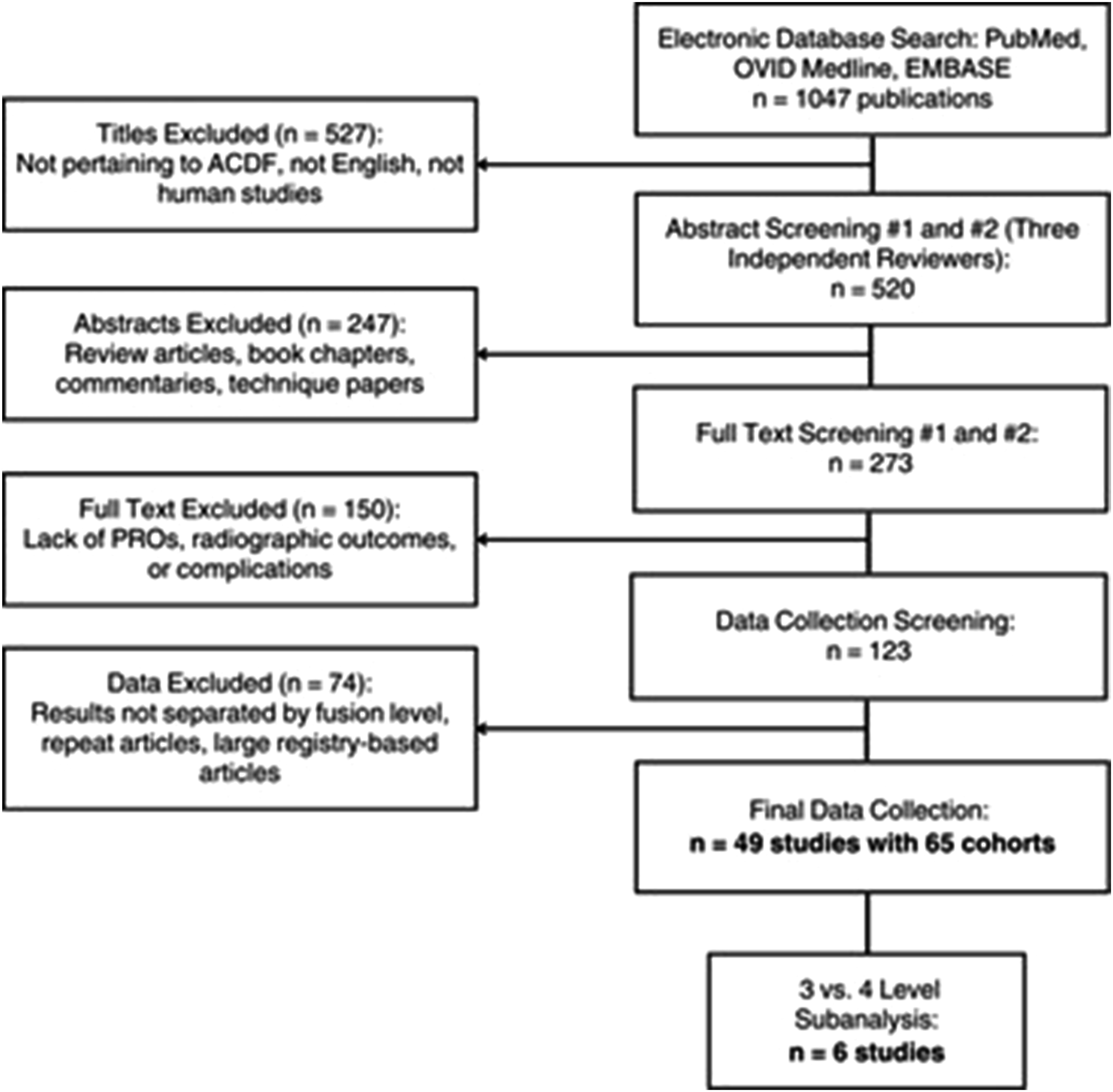
Patient Demographics and Pathology
Baseline Demographic Characteristics of Included Cohorts
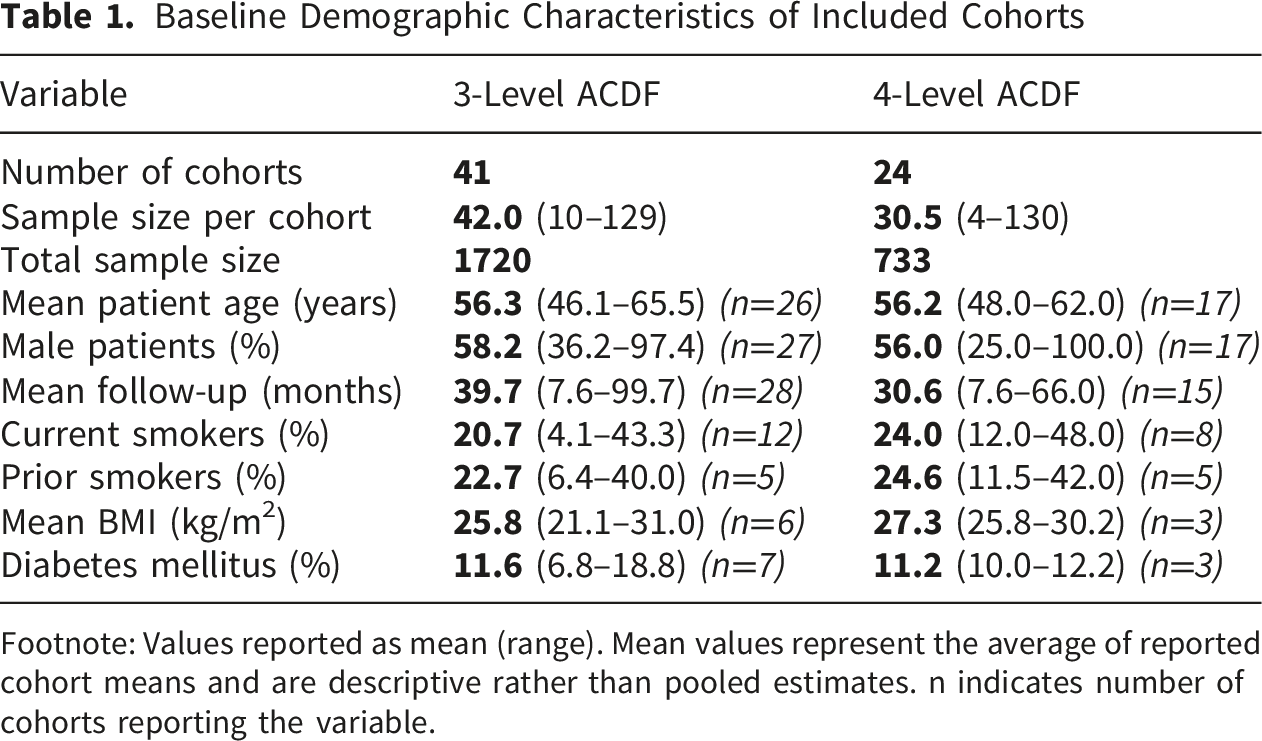
Footnote: Values reported as mean (range). Mean values represent the average of reported cohort means and are descriptive rather than pooled estimates. n indicates number of cohorts reporting the variable.
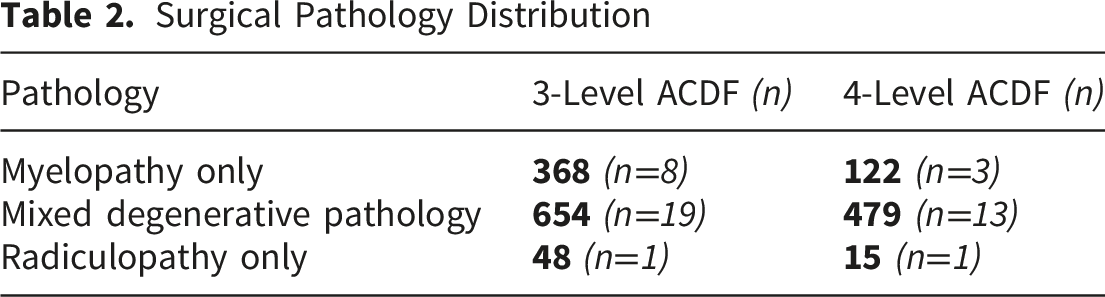
Surgical Pathology Distribution
Surgical Technique and Construct
All studies evaluated anterior cervical discectomy with a fusion construct length of 3 or 4 levels. Hybrid surgery procedures and posterior approaches were excluded. Surgical constructs varied and included cage-half plate constructs (5 cohorts), cage–full plate constructs (20 cohorts), plate-and-screw constructs (2 cohorts), and stand-alone cages (15 cohorts).
Cage materials included PEEK cages (32 cohorts) and titanium cages (4 cohorts). Graft materials consisted of allograft (20 cohorts) and autograft (18 cohorts). Cortico-cancellous (3 cohorts) and cadaveric (2 cohorts) were specified in allograft. Iliac crest (15 cohorts) and local bone graft (4 cohorts) were specified in autograft. Bone morphogenic protein (BMP) was reportedly used in 2 cohorts.
Patient Reported Outcomes
Patient-Reported Outcomes Across Included Cohorts
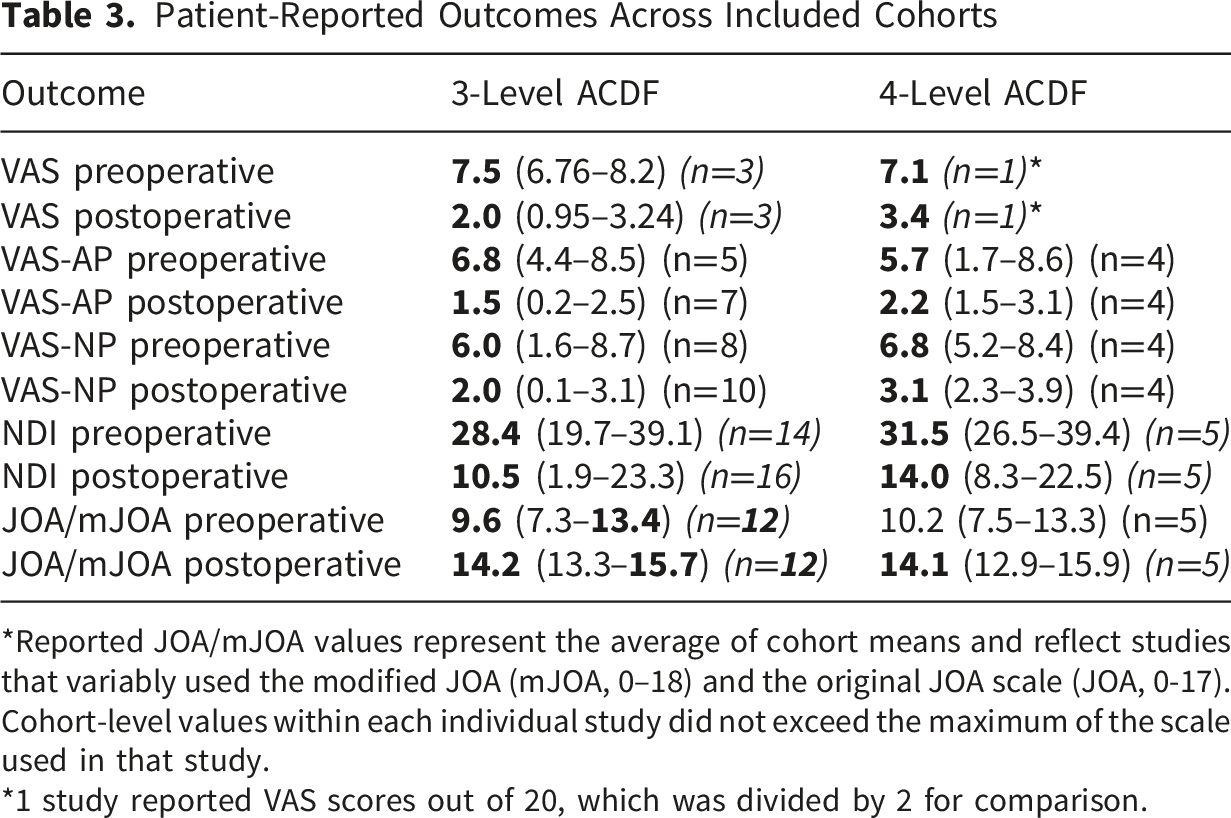
*Reported JOA/mJOA values represent the average of cohort means and reflect studies that variably used the modified JOA (mJOA, 0–18) and the original JOA scale (JOA, 0-17). Cohort-level values within each individual study did not exceed the maximum of the scale used in that study.
*1 study reported VAS scores out of 20, which was divided by 2 for comparison.
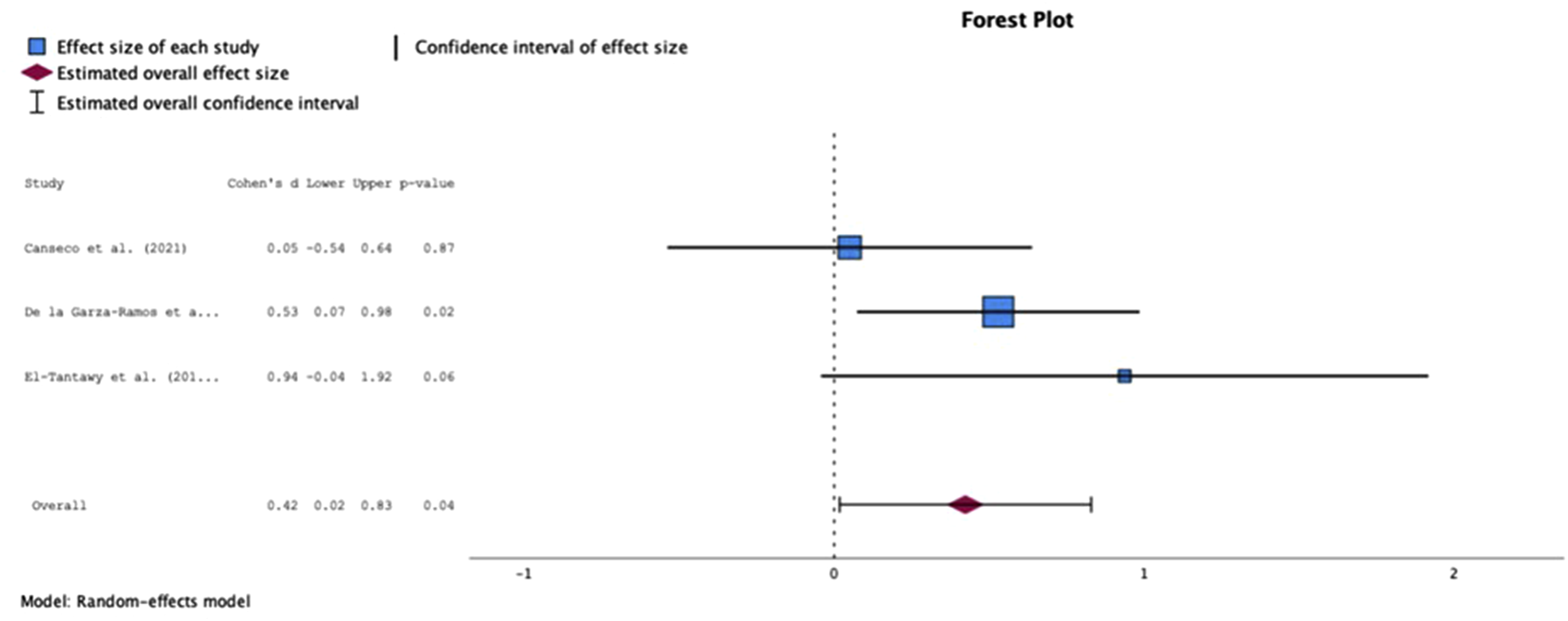
Forest plot of VAS-NP for three-level ACDF compared with four-level ACDF (derived from meta-analysis of three studies). VAS-NP, visual analog score-neck pain; ACDF, anterior cervical discectomy and fusion
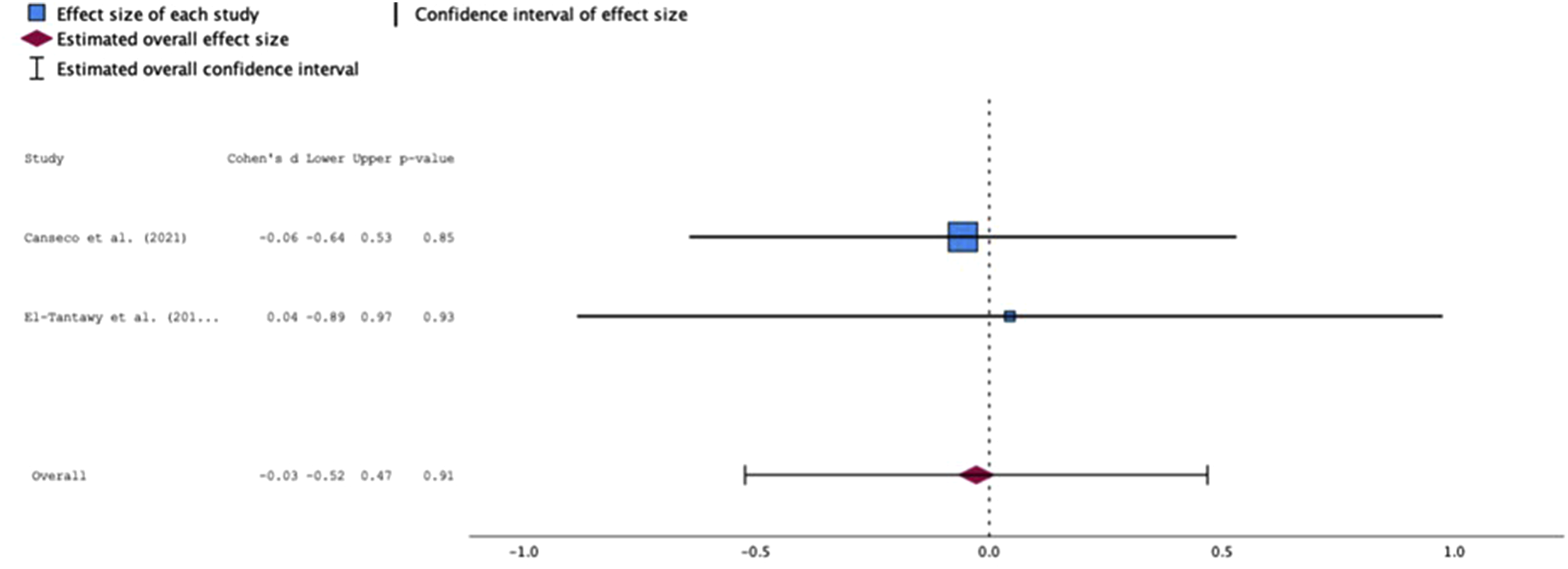
Forest plot of VAS-AP for three-level ACDF compared with four-level ACDF (derived from meta-analysis of two studies). VAS-AP, visual analog score-arm pain; ACDF, anterior cervical discectomy and fusion
While descriptive data demonstrated higher mean preoperative and postoperative pain and disability scores among 4-level cohorts, these findings were primarily descriptive and reflect cohort-level averages rather than pooled comparative estimates. However, among studies directly comparing 3- and 4-level ACDF, meta-analysis demonstrated significantly less improvement in VAS-NP following 4-level ACDF (Cohen’s d −0.42; 95% CI −0.83 to −0.02; p=0.041) (Figure 2). In contrast, no significant difference in improvement of VAS-AP was observed between 3- and 4-level ACDF on meta-analysis (Cohen’s d −0.03; 95% CI −0.53 to 0.47; p=0.913) (Figure 3).
Fusion Outcomes
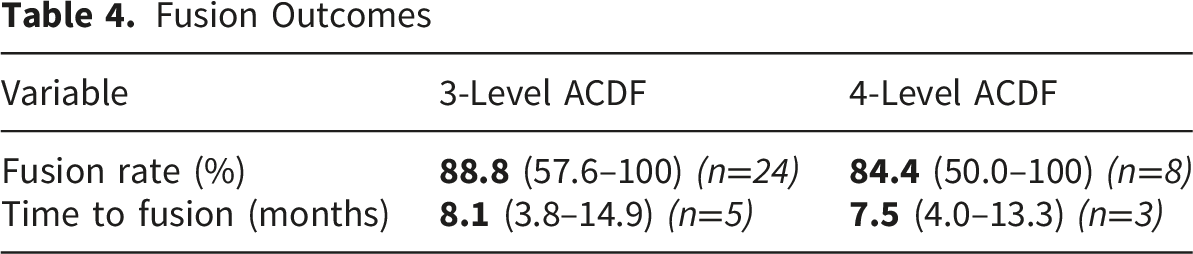
Fusion Outcomes
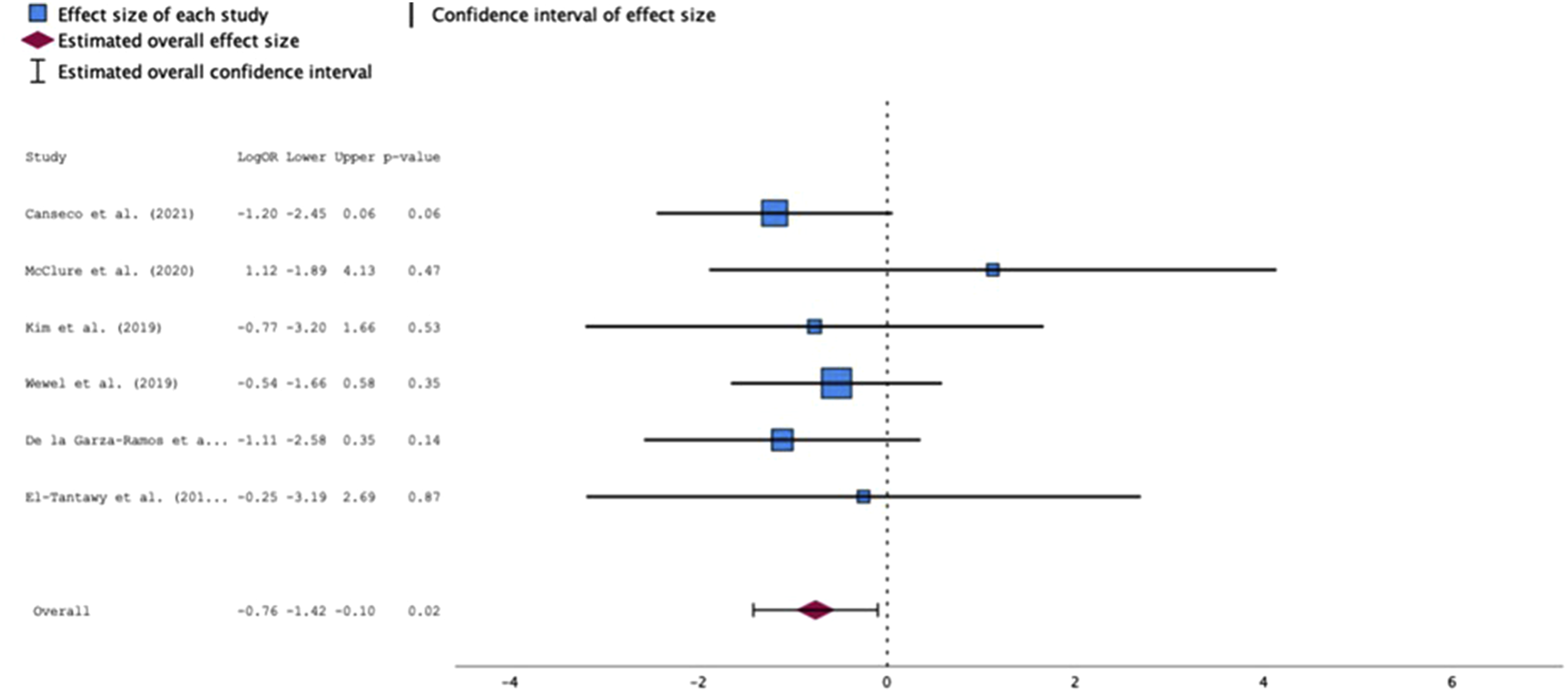
Forest plot of fusion rate for three-level ACDF compared with four-level ACDF (derived from meta-analysis of six studies). ACDF, anterior cervical discectomy and fusion
Fusion Outcomes by Construct Type

Complications
Complication Outcomes
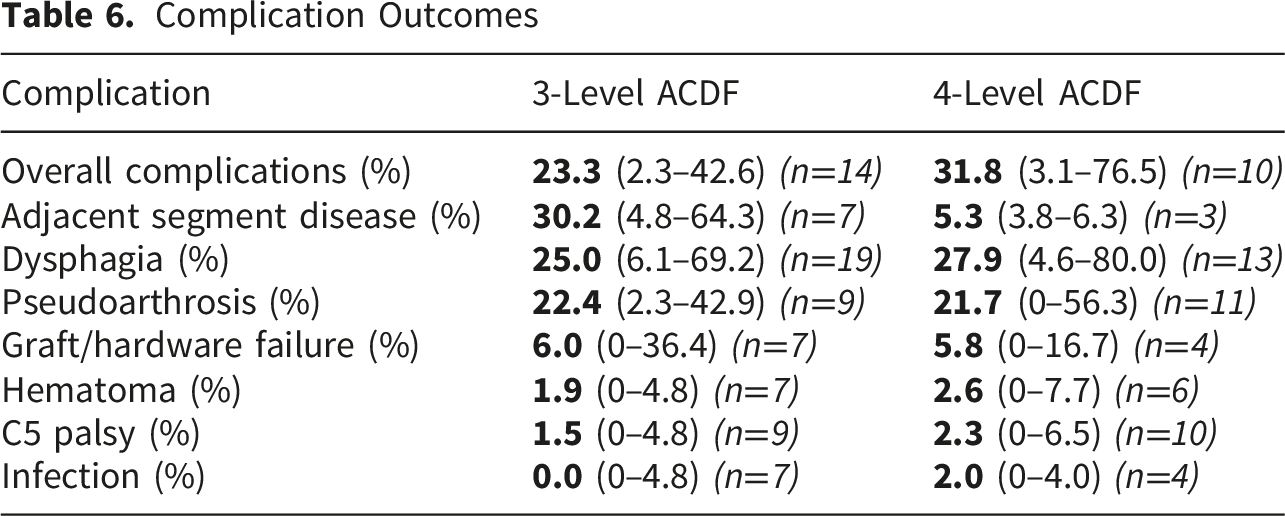
Meta-analysis of overall complication rates did not demonstrate a statistically significant difference between construct lengths, although confidence intervals were wide and the number of comparative studies was limited (log odds ratio 1.37, 95% CI −1.10 to 3.85; p=0.28) (Figure 5). Forest plot of total complication rate for three-level ACDF compared with four-level ACDF (derived from meta-analysis of two studies). ACDF, anterior cervical discectomy and fusion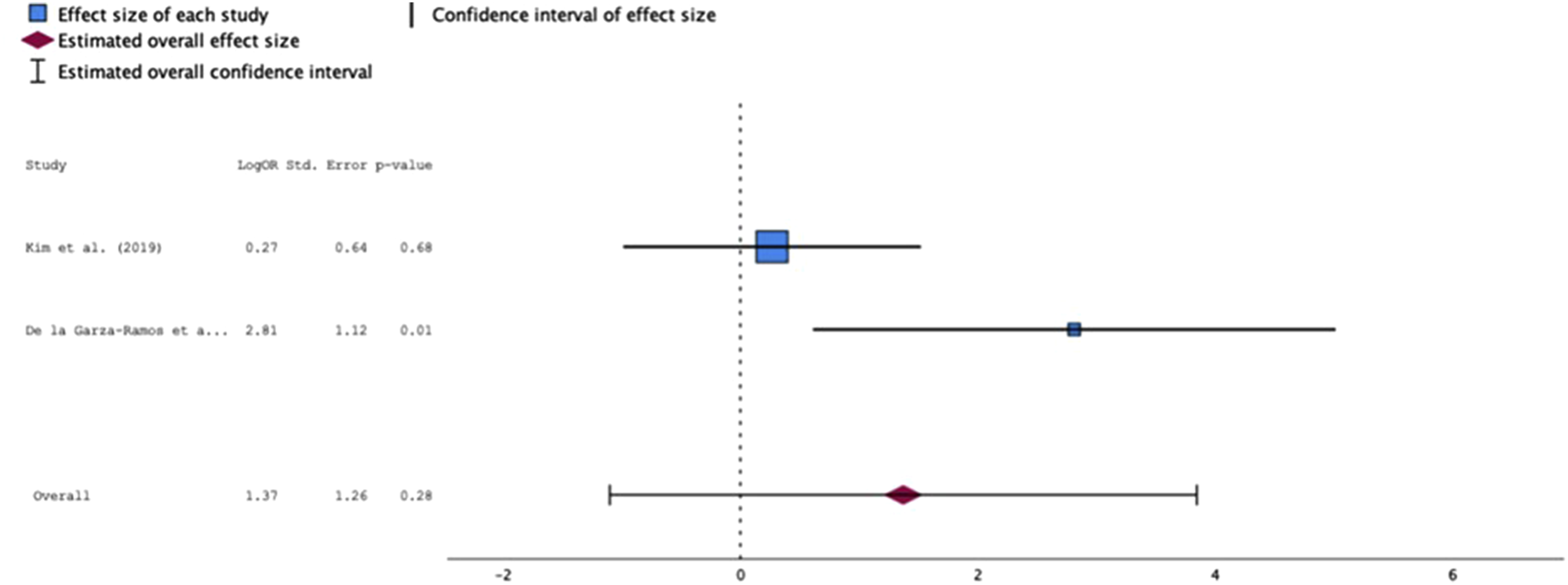
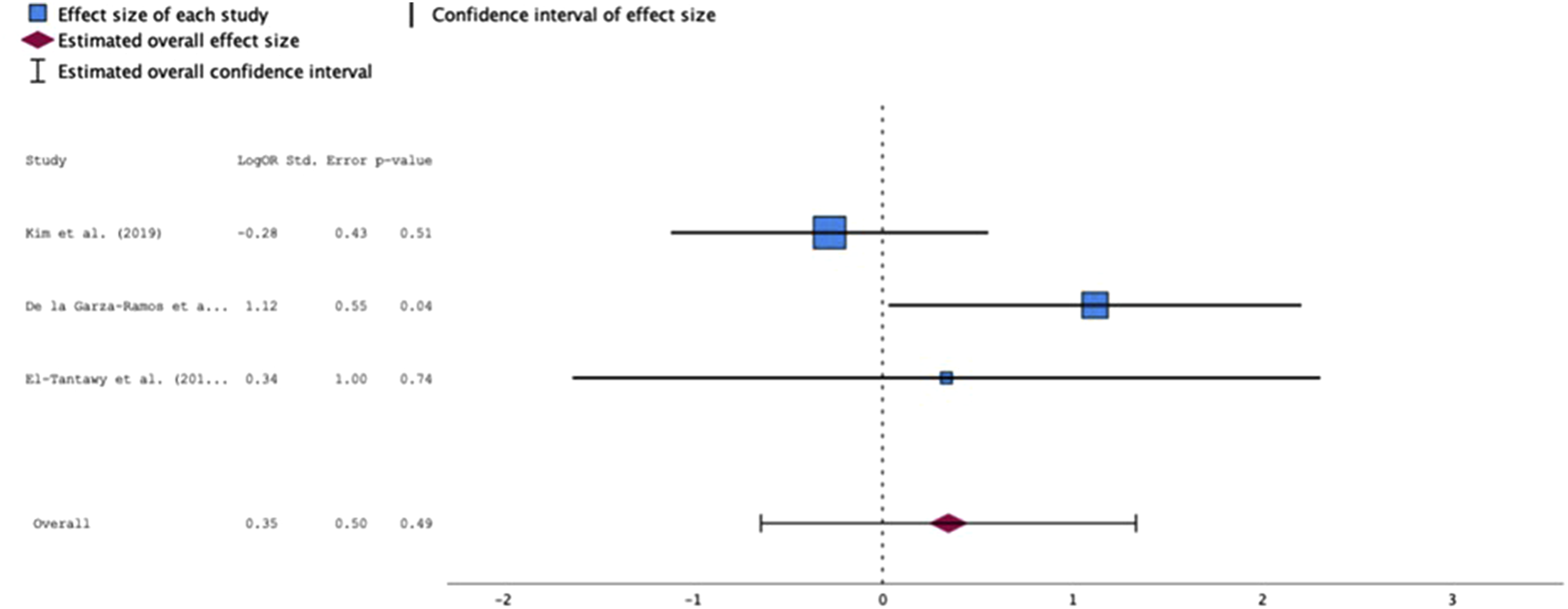
Among studies directly comparing 3- and 4-level ACDF, meta-analysis demonstrated no statistically significant difference in revision rates between groups (log odds ratio 0.08, 95% CI −0.70 to 0.86; p=0.84) (Figure 6). Similarly, no significant difference in postoperative dysphagia rates was observed between 3- and 4-level constructs (log odds ratio 0.35, 95% CI −0.64 to 1.34; p=0.49) (Figure 7). Forest plot of revision rate for three-level ACDF compared with four-level ACDF (derived from meta-analysis of five studies). ACDF, anterior cervical discectomy and fusion Forest plot of dysphagia rate for three-level ACDF compared with four-level ACDF (derived from meta-analysis of three studies). ACDF, anterior cervical discectomy and fusion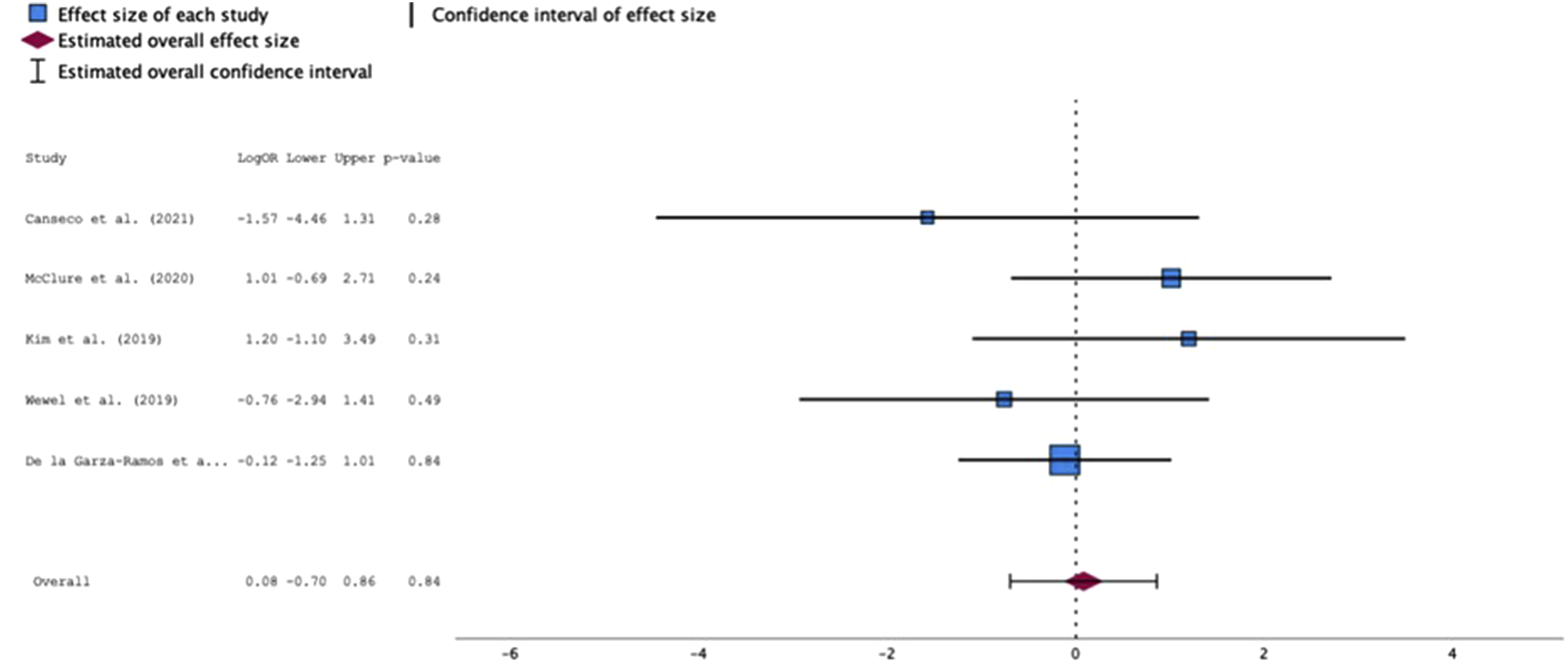
Perioperative Outcomes
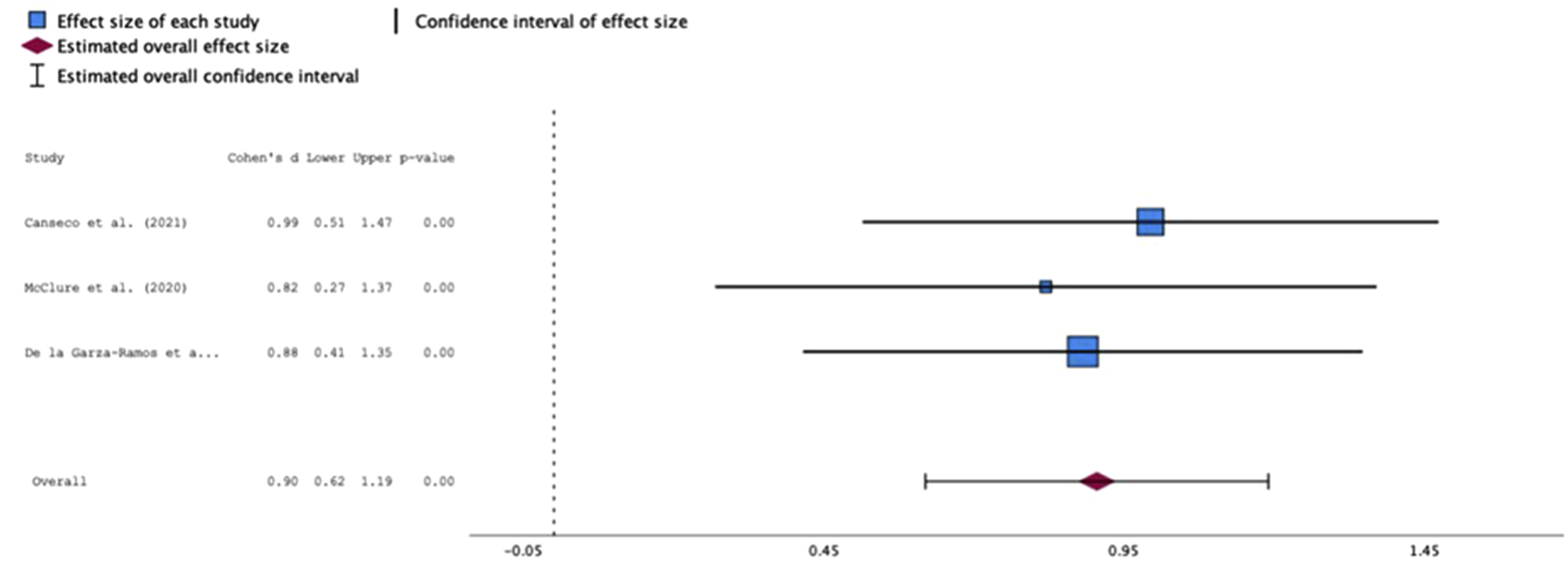
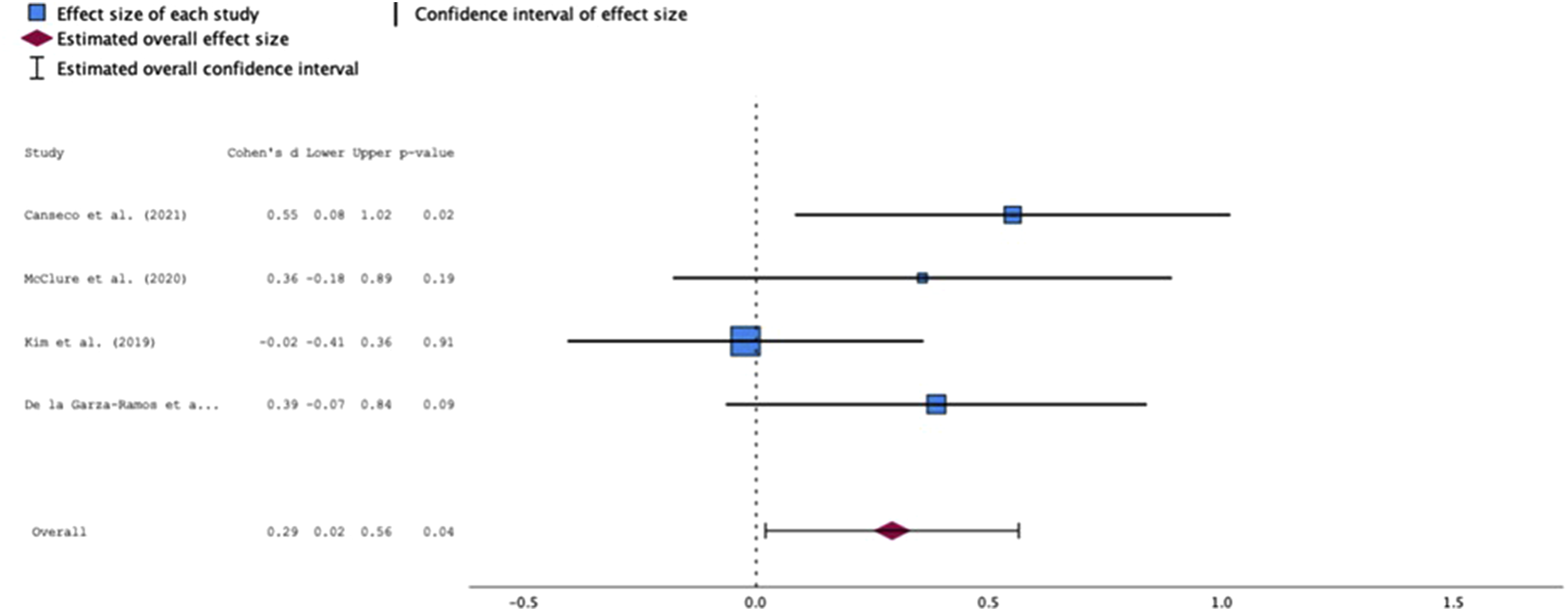
Across studies directly comparing 3- and 4-level ACDF, meta-analysis demonstrated that 4-level ACDF was associated with significantly longer operative time compared with 3-level constructs (Cohen’s d 1.19, 95% CI 0.81 to 1.58; p<0.001) (Figure 8) and significantly greater estimated blood loss (Cohen’s d 0.91, 95% CI 0.62 to 1.19; p<0.001) (Figure 9). Similarly, 4-level ACDF was associated with a modest but statistically significant increase in hospital length of stay compared with 3-level constructs (Cohen’s d 0.29, 95% CI 0.02 to 0.56; p=0.04) (Figure 10). Forest plot of operative time for three-level ACDF compared with four-level ACDF (derived from meta-analysis of four studies). ACDF, anterior cervical discectomy and fusion Forest plot of EBL for three-level ACDF compared with four-level ACDF (derived from meta-analysis of three studies). EBL, estimated blood loss; ACDF, anterior cervical discectomy and fusion Forest plot of hospital length of stay for three-level ACDF compared with four-level ACDF (derived from meta-analysis of three studies). ACDF, anterior cervical discectomy and fusion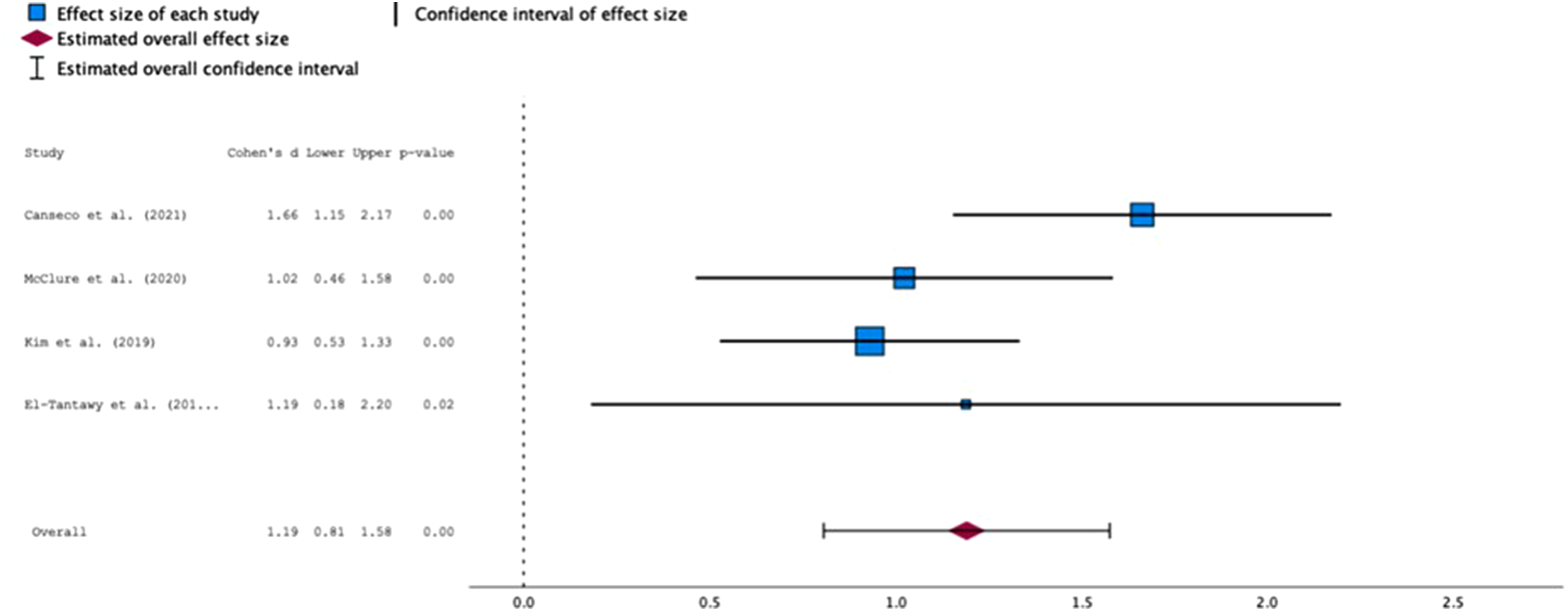
Discussion
This systematic review and meta-analysis provides a focused synthesis evaluating outcomes following 3- and 4-level ACDF, with particular emphasis placed on studies directly comparing these constructs. Both 3- and 4-level ACDF resulted in meaningful improvements in pain, disability, and neurologic function, reinforcing the role of multilevel ACDF as an effective treatment option for appropriately selected patients with degenerative cervical pathology. However, when outcomes were directly compared through meta-analysis, increasing construct length was associated with significantly less improvement in neck pain, lower fusion rates, and increased perioperative morbidity.
Findings from the systematic review component of our study demonstrate that patients undergoing both 3- and 4-level ACDF experience substantial reductions in pain and disability, consistent with prior studies evaluating multilevel anterior constructs.13,14,20 Across cohorts, mean postoperative VAS, VAS-neck pain, VAS-arm pain, NDI, and JOA/mJOA scores significantly improved from preoperative values in both groups. However, 4-level ACDF cohorts tended to have higher preoperative disability and pain scores and, despite improvement, higher postoperative scores compared with 3-level cohorts. This pattern suggests that while both constructs provide clinically meaningful benefit, patients requiring 4-level fusion represent a population with greater baseline disease burden.
These descriptive systematic review findings are supported by the meta-analysis of directly comparative studies, which demonstrated that 4-level constructs were associated with significantly less improvement in axial neck pain compared with 3-level constructs, while no difference was observed for radicular arm pain. This distinction aligns with the systematic-review data, where postoperative VAS-neck pain values remained higher in 4-level cohorts, whereas improvements in arm pain were comparable. Taken together, these findings suggest that while neural decompression achieved through ACDF is effective regardless of construct length, axial neck pain may be more sensitive to increasing fusion length and greater associated biomechanical stresses.
Conversely, several individual cohort studies, including Kim et al. and Canseco et al., reported postoperative improvement in PROs without statistically significant differences between construct length.21,22 However, these studies were limited by modest sample sizes and variability in follow-up length, potentially limiting their ability to detect smaller effect sizes.
One of the most clinically relevant findings of our meta-analysis was the significantly lower fusion rate observed in 4-level ACDF compared with 3-level constructs, supporting findings from previous studies that fusion rates decrease with increasing construct length. Wewel et al. reported decreased segmental fusion rates with longer constructs, while De la Garza-Ramos et al. found higher pseudoarthrosis rates in 4-level ACDF, although these findings did not always reach statistical significance in isolation.20,23 In contrast, the meta-analysis published by Wang et al. did not identify a statistically significant difference in fusion rates between 3- and 4-level ACDF.
19
This discrepancy likely reflects the lower number of studies included in the meta-analysis of fusion rate in the Wang et al. study (two cohorts), versus six in the present analysis, suggesting that increasing construct length from three to four levels may impose biomechanical demands that meaningfully affect fusion success.
Regarding fusion outcomes by construct type, the systematic review demonstrated higher reported fusion rates for cage–plate constructs compared with stand-alone cages in both 3- and 4-level ACDF. Fusion rates within each construct type were similar between 3- and 4-level procedures, though data for 4-level stand-alone cage constructs were limited. These findings are consistent with prior literature suggesting slightly higher fusion rates with supplemental anterior plating. 24 When considered alongside the lower fusion rates observed with increasing construct length in the present meta-analysis, these descriptive results suggest that construct selection may become increasingly relevant as the number of fused levels increases.
Meta-analysis of perioperative outcomes demonstrated a consistent and intuitive pattern. 4-level ACDF was associated with significantly longer operative time, greater estimated blood loss, and increased length of hospital stay. These findings align with previous individual comparative cohort studies and meta-analyses, all of which reported increased operative burden with 4-level ACDF when comparted to 3-level constructs.19,21,23,25
Meta-analysis of perioperative complication rates did not demonstrate a statistically significant difference between 3- and 4-level constructs. However, confidence intervals were wide, and the number of comparative studies was limited, suggesting that this analysis may be underpowered to detect differences in relatively infrequent adverse events. Prior large database studies have reported higher short-term complication and reoperation rates with increasing fusion length, particularly in 4-level ACDF. While such studies offer improved statistical power, they lack the clinical and radiographic detail available in cohort-level investigations and were therefore excluded from the present analysis.
Overall, the findings of this meta-analysis complement those reported in large national database analyses. Joo et al. demonstrated that 4-level ACDF was associated with higher rates of 90-day adverse events, reoperation, and dysphagia compared with lower-level constructs, while 3-level ACDF did not consistently demonstrate increased risk when compared to shorter constructs. 18 Although administrative database studies may overestimate complication rates due to coding limitations and lack of clinical granularity, the directionality of their findings aligns with the present pooled analysis; namely, that 4-level ACDF represents a distinct risk category relative to 3-level constructs.
This study has several limitations. The majority of included studies were retrospective, and there was heterogeneity in fusion definitions, outcome measure, complication reporting, and follow-up duration.
Conclusion
In summary, both 3- and 4-level ACDF were associated with significant postoperative improvement in pain and function. However, meta-analysis revealed that 4-level ACDF demonstrated significantly less improvement in neck pain, lower rates of fusion, and greater perioperative morbidity when compared with 3-level constructs. While individual cohort studies may not consistently detect such differences, meta-analysis reveals clinically significant distinctions that should inform surgical planning and patient counseling regarding outcomes following 4-level ACDF. Future prospective, adequately powered studies are needed to better define the long-term clinical implications of multilevel anterior cervical discectomy and fusion.
Supplemental Material
Supplemental material - Clinical Outcomes Following Three- and Four-Level Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis
Supplemental material for Clinical Outcomes Following Three- and Four-Level Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis by Tyler M. Compton, Ravi A. Patel, Mark A. Plantz, Rohan M. Shah, Theodore A. Joaquin, Jacob R. Staub, Daniel E. Herrera, Cade F. Bennett, Anitesh Bajaj, Abhinav R. Balu, Matthew W. Colman, Wellington K. Hsu, Alpesh A. Patel, Srikanth N. Divi in Global Spine Journal
Supplemental Material
Supplemental material - Clinical Outcomes Following Three- and Four-Level Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis
Supplemental material for Clinical Outcomes Following Three- and Four-Level Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis by Tyler M. Compton, Ravi A. Patel, Mark A. Plantz, Rohan M. Shah, Theodore A. Joaquin, Jacob R. Staub, Daniel E. Herrera, Cade F. Bennett, Anitesh Bajaj, Abhinav R. Balu, Matthew W. Colman, Wellington K. Hsu, Alpesh A. Patel, Srikanth N. Divi in Global Spine Journal
Footnotes
Ethical Considerations
This study is IRB exempt due to its design. No patient data was accessed.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data was accessed from current medical literature. The collection of studies investigated can be accessed per reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.