
Abstract
Study Design
Retrospective Cohort.
Objective
To investigate whether the timing of surgery, defined by admission-to-surgery intervals, influences short-term in-hospital outcomes and motor recovery in adult patients with Central Cord Syndrome (CCS). This single-center study aimed to investigate the optimal timing for surgery in patients with CCS by using a new categorization of surgical timing.
Methods
This study includes adult patients with clinically and radiologically confirmed traumatic CCS who received surgical care at a tertiary academic center between March 2012 and July 2022 (n = 70). Patients were classified by time of surgery as ultra-early (<24 h, n = 11), early (24-48 h, n = 33), late (48 h-14 days, n = 22), or ultra-late (>14 days, n = 4). The studied outcomes were in-hospital mortality, mechanical ventilation requirement, ventilation duration, intensive care unit (ICU) length of stay, ambulatory status at last follow-up, and changes in motor score in each group. Chi-square and Kruskal-Wallis tests were used to compare groups. The correlation between surgical timing and motor improvement was identified using correlation analysis.
Results
The four timing subgroups showed no significant differences in in-hospital mortality, ambulatory status, need for mechanical ventilation, ventilation duration, or ICU length of stay (p = 0.7, 0.4, 0.6, 0.8, and 0.3, respectively). Moreover, although there was a notable postoperative improvement in the total (four limbs), bilateral upper extremity (BUE), and bilateral lower extremity (BLE) motor scores, these improvements were not significantly different across subgroups (p = 0.7, 0.7, and 0.6, respectively). There was no significant correlation between surgery time and motor improvement (p = 0.63).
Conclusions
In this single-center study, the timing of surgery after admission did not appear to influence short-term in-hospital outcomes or early motor recovery in adult patients with CCS. Key limitations of this study include the retrospective design, the small sample sizes in some surgical timing subgroups, and the reliance on admission-to-surgery timing rather than injury-to-surgery intervals. Furthermore, long-term follow-up data were not consistently available.
Introduction
Central Cord Syndrome (CCS) is the most common type of incomplete cervical spinal cord injury, typically resulting in greater weakness in the arms and hands than in the legs. 1 Overall, CCS commonly happens when a hyperextension injury impacts a narrowed cervical spinal canal. This may result in contusion or compression of the spinal cord’s central region. 2 In addition to motor deficits, patients frequently experience sensory disturbances and may have autonomic dysfunction such as impaired bladder control, reflecting damage to central spinal pathways.1,3 For a long time, researchers believed that the upper-extremity weakness in CCS was mainly due to the neural organization of the spinal cord. Recently, emerging evidence has challenged the traditional view of isolated central cord damage, suggesting instead that central cord syndrome (CCS) is primarily driven by a disproportionate vulnerability of upper-extremity motor pathways to injury, alongside mechanisms of diffuse axonal injury and microvascular damage.4-6
CCS occurs more in older adults who are more prone to degenerative cervical changes and minor trauma mechanisms that precipitate the syndrome. 7 Beyond age, several additional patient- and injury-related variables influence both overall prognosis and the potential benefits of early surgical intervention. For example, baseline neurological severity significantly shapes recovery, with individuals presenting with severe deficits showing different improvement patterns than those with milder injuries. 8
Surgical decompression, with or without stabilization, is recommended in cases of cord compression or progressive neurological deterioration. 9 Despite the growing trend toward recommending earlier decompression, evidence remains conflicting when individual studies are compared directly. 2 Badhiwala et al demonstrated that early (<24 h) surgery was associated with superior upper-extremity motor recovery in a propensity-matched study of 186 patients with CCS. 10 In a meta-analysis of a large sample (8424 patients) by Xu et al, patients receiving early surgical treatment showed improved ASIA motor scores and fewer complications, but there was no benefit in survival. 11 However, other studies have shown no significant differences in mortality or neurological outcomes based on timing.12,13 In a nationwide trauma database study in Japan encompassing 236,698 patients, the early (within 24 hours) and late (25 hours- 7 days) surgical interventions were investigated, and they found no significant difference in in-hospital mortality between early and late surgery. In line with the previous study, a randomized trial reported no significant neurologic benefit of early versus delayed decompression, randomizing patients to the early period (less than 72 hours) and the late period (after that).14,15 It is notable that the approaches to classifying patients by surgery timing and the designs of these studies differed markedly, which may have led to these heterogeneous results. Despite the variation in reported results, 2025 AO Spine recommends that patients with AIS grade C CCS may benefit from early intervention, although the benefit for patients with less severe injury remains an area of debate. 16
Hence, we aimed to conduct a single-center study to explore whether a different and new categorizations of surgical timing may affect patient outcomes within specific time periods, with the goal of identifying differences that prior studies may have overlooked.
Material and Methods
Study Design and Setting
This is a retrospective observational study conducted in a tertiary academic hospital (University of Kentucky Albert Chandler Hospital, USA). The patients included in this study were obtained from the institutional electronic medical records.
Eligibility Criteria
This study focused exclusively on all adult patients admitted to our center between March 2012 and July 2022 with a definitive diagnosis of traumatic CCS, characterized by marked upper-limb weakness relative to the lower limbs, confirmed by Magnetic Resonance Imaging (MRI), and who underwent surgical treatment. In this study, the level of spinal cord injury was defined strictly by structural neuroimaging rather than by clinical motor or sensory levels, because clinical examinations are often confounded in the acute post-trauma phase by spinal shock and altered patient consciousness. The exclusion criteria for this study included prior spinal surgery, presence of any vertebral fracture or dislocation, complete spinal cord injury (ASIA Impairment Scale Grade A), non-traumatic etiologies of CCS (such as those arising from spondylosis, osteoporosis, spinal instability, or spinal arthropathies), lack of adequate imaging, physical exam, or follow-up data, and any other missing data that could interfere with reporting the study outcomes.
Definition of Exposure: Timing of Surgery
Based on current literature and our database, patients were divided into four main groups according to the timing of surgery after admission: ultra early, defined as surgery within 24 hours; early, between 24 and 48 hours after admission; late: from 48 hours up to 14 days; and ultra late, performed after 14 days. These times were determined based on the admission times available in patients’ records and our database.
Data Collection and Variables
Clinical data from patients, along with demographic indices and surgery-related variables, were extracted from patient records and compiled into our dataset. The primary outcomes of this study were in-hospital mortality, ambulatory status at follow-up, length of Intensive Care Unit (ICU) stay, need for ventilation, and, if required, length of assisted ventilation, and change in muscle power. For analysis purposes, muscle power was assessed by measuring the combined power of five muscles in each extremity and dividing it by 5 (resulting in a score between 0-5 for each limb). Accordingly, the change in power for each extremity was determined by comparing pre- and postoperative measurements. Additionally, composite indices were developed to provide a more objective comparison of power changes across the upper and lower extremities, as well as all four limbs. Regarding patient characteristics, data on age, gender, Body Mass Index (BMI), smoking status, underlying diseases such as Diabetes Mellitus (DM), Chronic Heart Failure (CHF), and hypertension (HTN), level of CCS, and admission time were recorded. Also, data on the surgical approach were exported for comparison across patient groups.
Statistical Analysis
Descriptive analyses were conducted to characterize patient demographics and summarize clinical outcomes. Patients were stratified into three groups based on surgical timing: <24 hours, 24–72 hours, and >72 hours. Inferential analyses were performed to compare outcomes across these surgical timing groups and to evaluate pre-versus postoperative changes. Categorical variables—including in-hospital mortality, ambulation at discharge, and ventilator use—were compared across groups using Fisher’s exact test. Baseline characteristics, including sex (male vs. female), smoking status, diabetes mellitus, hypertension, and heart failure, were also analyzed using Fisher’s exact test. For continuous variables, normality was assessed using the Shapiro–Wilk test and Q–Q plots. As most variables were not normally distributed, the Kruskal–Wallis H test was used to compare age, body mass index (BMI), ventilator duration, ICU length of stay, and highest injury level across the surgical timing groups. To evaluate changes in continuous outcomes before and after surgery, the Wilcoxon signed-rank test was applied, specifically for motor score improvements (total improvement, upper extremity (BUE) improvement, and lower extremity (BLE) improvement). Finally, Pearson’s correlation analysis was used to assess the relationship between time to surgery and motor improvement outcomes (total, BUE, and BLE improvement). Scatter plots were generated to visually depict these relationships. A significant p-value was considered to be less than 0.05, two-tailed. When a variable contained missing patient data, these values were excluded, and the analysis was conducted using only the available patient data. The analyses were performed using R.
This study was approved by the Institutional Review Board (IRB) of the University of Kentucky (approval number 79735).
Results
In total, 70 patients met our criteria, with a mean age of 56.64±15.78 years, a mean BMI of 29.97±9.51, and a mean follow-up of 371.4± 487.3 days. Most patients in this cohort were male (48 of 70, 68%) and non-smokers (36 patients, 51.4%). The most common underlying diseases were HTN (in 39 patients, 55.7%) and diabetic mellitus (in 19 patients, 27.1%). The highest level of injury was determined through imaging studies, and C3 and C4 injuries were the most frequent, each affecting 18 patients (25.7%). To assess the effect of surgical timing, patients were divided into four subgroups based on the time of surgery after admission. The ultra-early intervention group included 11 patients, the early group 33 patients, the late group 22 patients, and the ultra-late window group 4 patients. Comparing the baseline characteristics of these four groups showed no significant differences. The patients in each timing window were compared to each other in terms of in-hospital mortality, ambulation at discharge, need for ventilator-assisted respiration and days on ventilation, and ICU length of stay. The analysis of patient data revealed no statistically significant difference between patients (p-values 0.7, 0.4, 0.6, 0.8, and 0.3, respectively) (Figure 1). Frequency of different outcomes based on desirable time windows. (A) ICU admission, (B) in-hospital mortality, (C) Ambulation at the time of discharge, (D) Ventilator use. Note that the incongruence between the reported number of patients and the total sample is due to missing data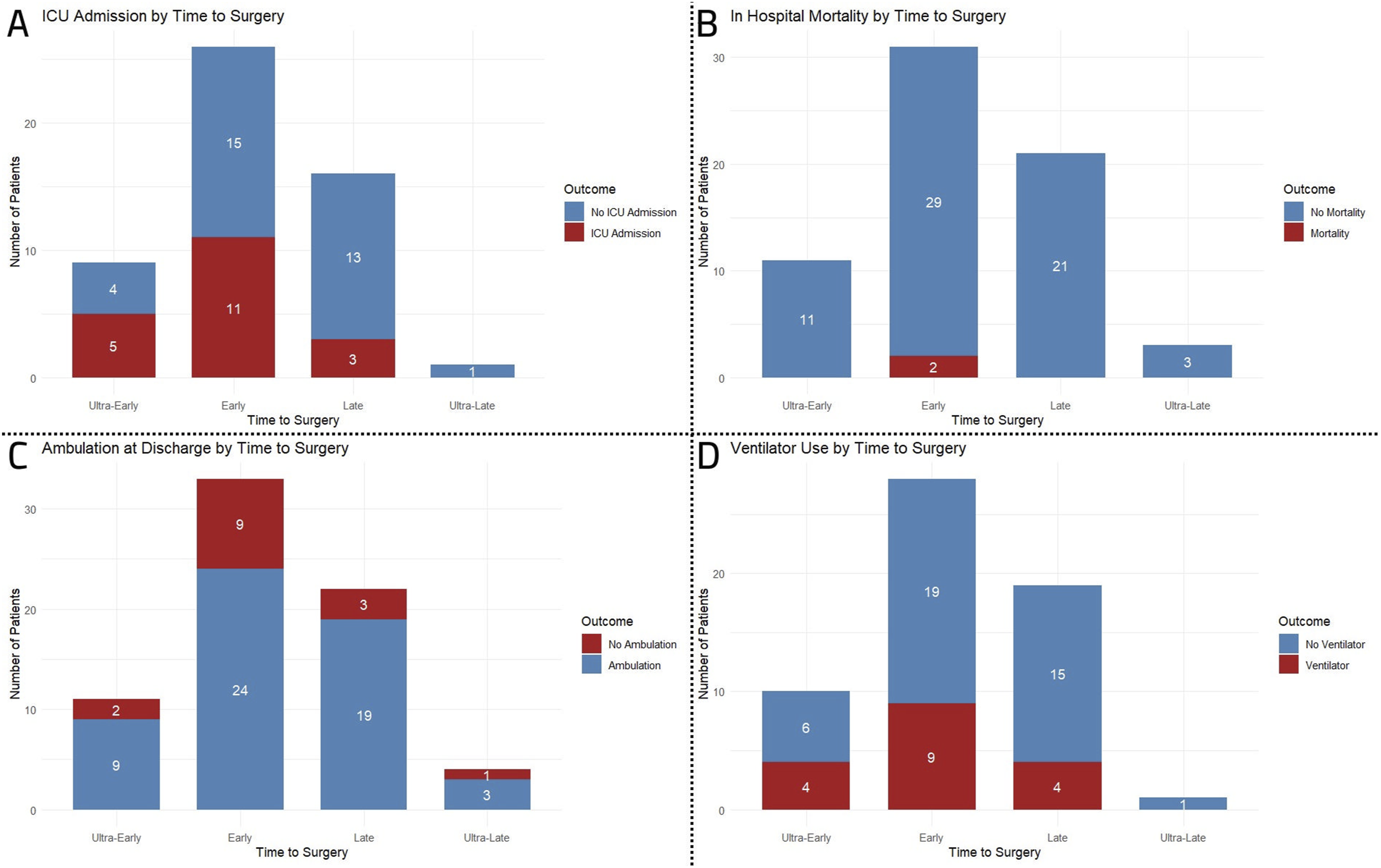
Demographic Characteristics and Clinical Outcomes According to Surgical Timing
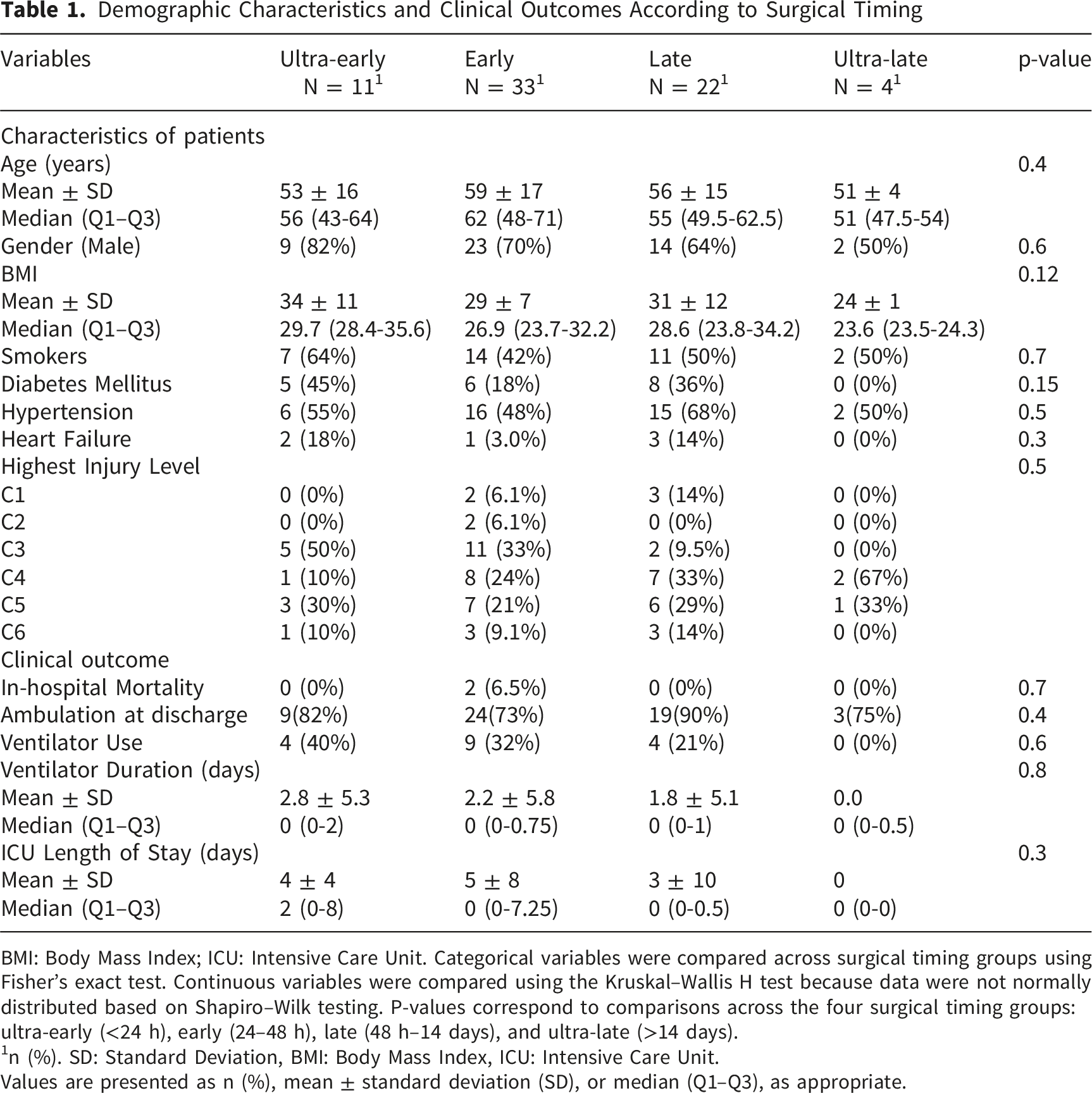
BMI: Body Mass Index; ICU: Intensive Care Unit. Categorical variables were compared across surgical timing groups using Fisher’s exact test. Continuous variables were compared using the Kruskal–Wallis H test because data were not normally distributed based on Shapiro–Wilk testing. P-values correspond to comparisons across the four surgical timing groups: ultra-early (<24 h), early (24–48 h), late (48 h–14 days), and ultra-late (>14 days).
1n (%). SD: Standard Deviation, BMI: Body Mass Index, ICU: Intensive Care Unit.
Values are presented as n (%), mean ± standard deviation (SD), or median (Q1–Q3), as appropriate.
Overall Motor Improvement Outcomes Across Surgical Timing Groups
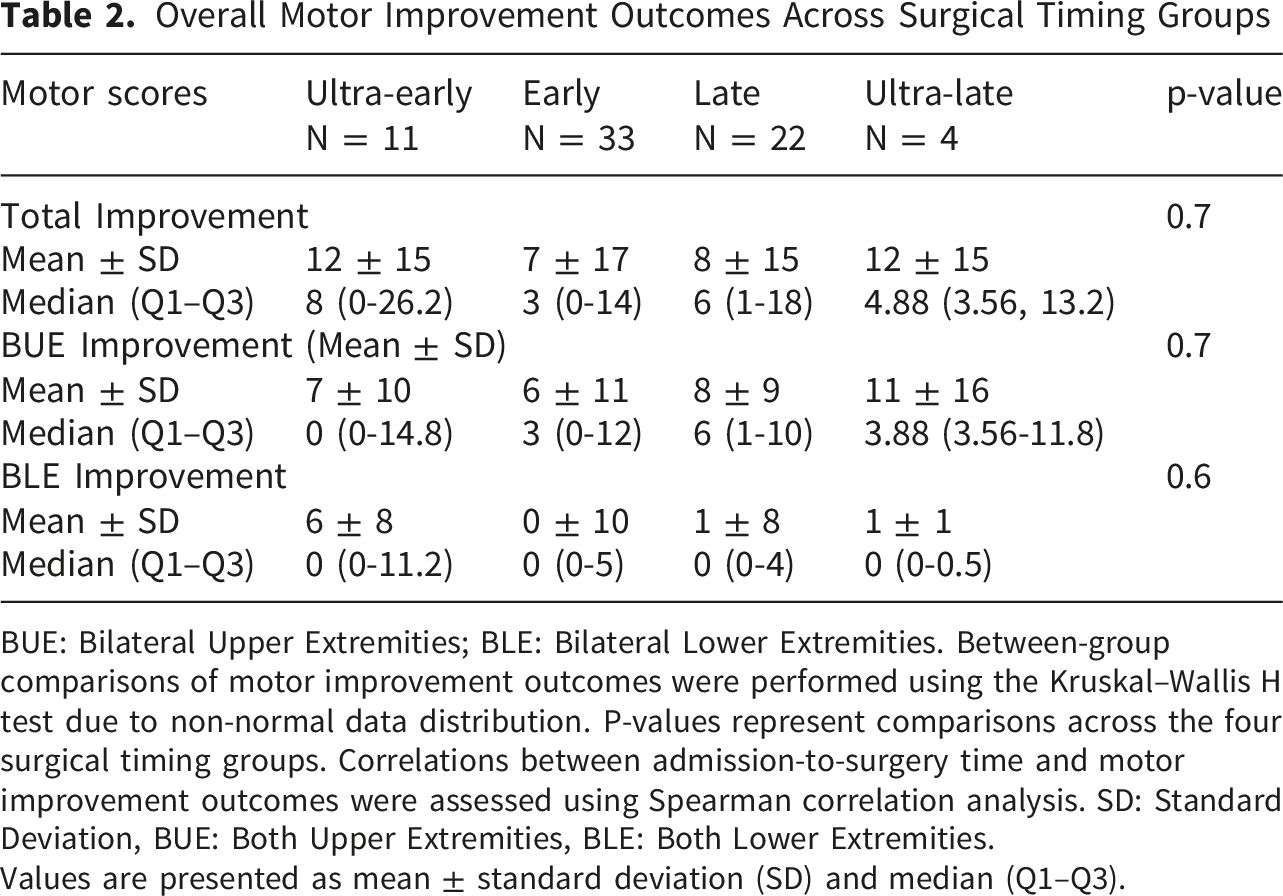
BUE: Bilateral Upper Extremities; BLE: Bilateral Lower Extremities. Between-group comparisons of motor improvement outcomes were performed using the Kruskal–Wallis H test due to non-normal data distribution. P-values represent comparisons across the four surgical timing groups. Correlations between admission-to-surgery time and motor improvement outcomes were assessed using Spearman correlation analysis. SD: Standard Deviation, BUE: Both Upper Extremities, BLE: Both Lower Extremities.
Values are presented as mean ± standard deviation (SD) and median (Q1–Q3).
Segmental Upper- and Lower-Extremity Motor Scores Before and After Surgery
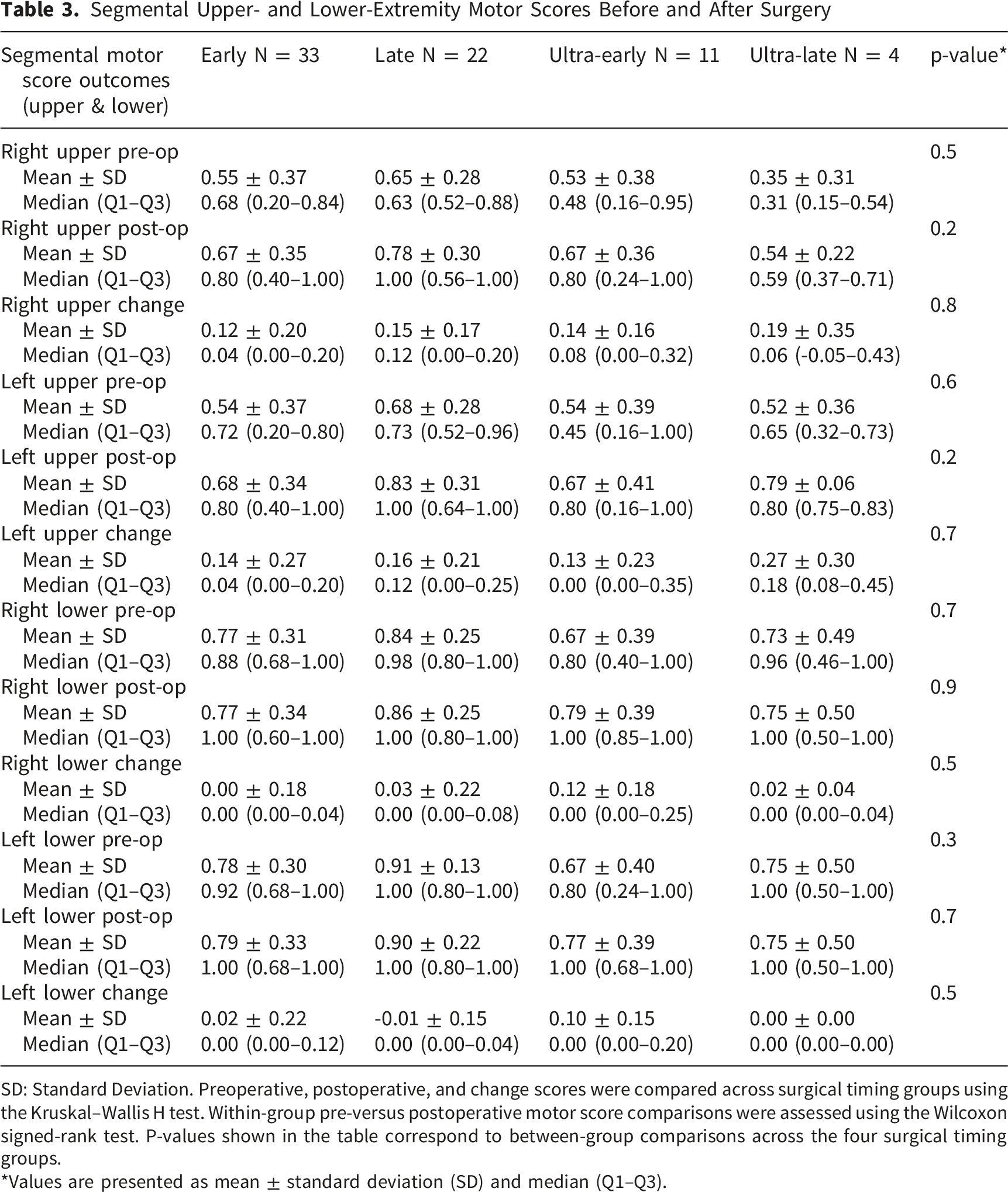
SD: Standard Deviation. Preoperative, postoperative, and change scores were compared across surgical timing groups using the Kruskal–Wallis H test. Within-group pre-versus postoperative motor score comparisons were assessed using the Wilcoxon signed-rank test. P-values shown in the table correspond to between-group comparisons across the four surgical timing groups.
*Values are presented as mean ± standard deviation (SD) and median (Q1–Q3).
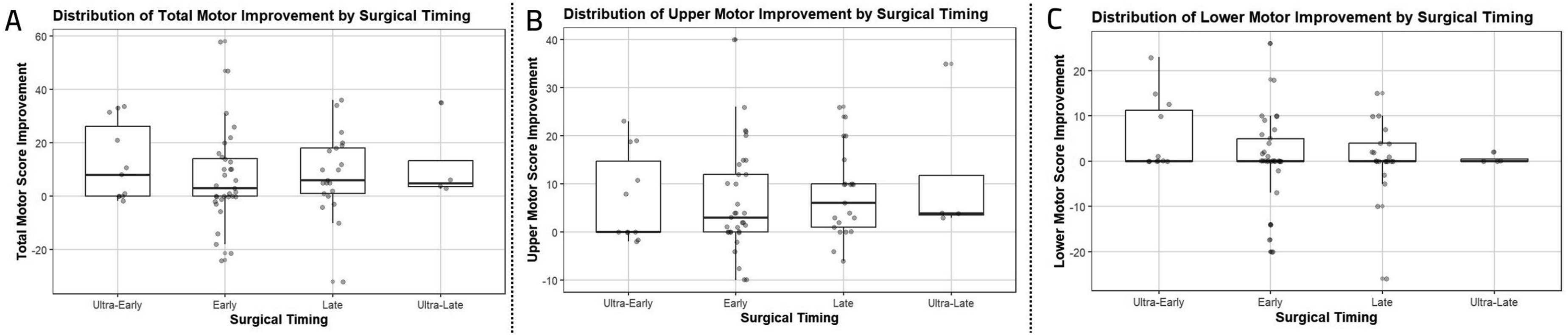
Motor improvement by the time of surgery. (A) Total motor improvement, (B). Upper motor improvement, (C) Lower motor improvement
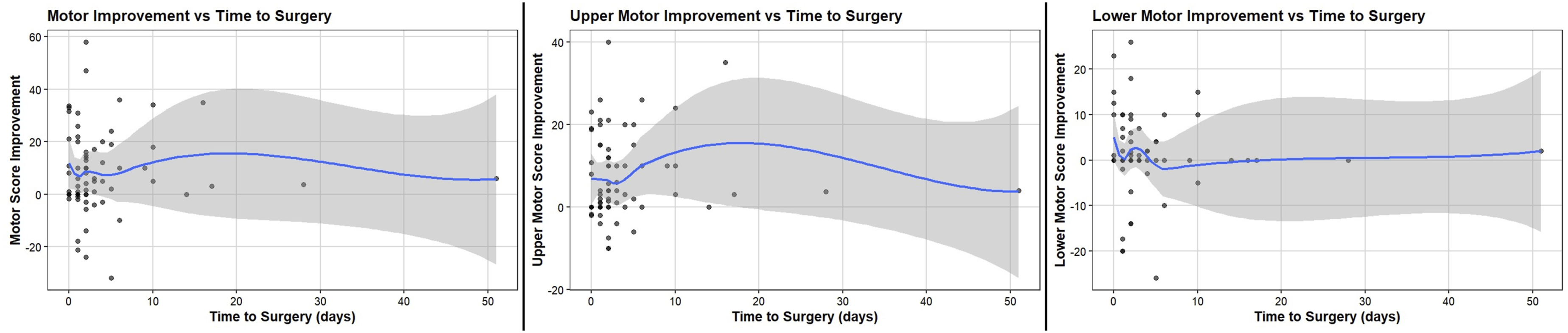
Motor improvement, considering the time of surgery, regardless of time period classification, is demonstrated as a scattered plot
Furthermore, Spearman’s rank correlation analysis was conducted to examine the relationship between admission-to-surgery time, treated as a continuous variable, and motor improvement outcomes. No significant correlations were identified between surgical timing and total motor improvement (ρ = 0.079, p = 0.521), BUE improvement (ρ = 0.149, p = 0.223), or BLE improvement (ρ = −0.060, p = 0.623).
Discussion
This single-center retrospective cohort included 70 adults with traumatic CCS who underwent surgery. We found no statistically significant differences between the surgical timing subgroups (ultra-early, early, late, or ultra-late) regarding in-hospital mortality, ICU length of stay, ventilator requirement or ventilator days, and ambulatory status. Total motor scores improved after surgery, regardless of timing, and BUE and BLE improvement scores did not differ between subgroups. When time-to-surgery was examined as a continuous variable, there was no significant correlation with motor improvement either.
Our main outcomes were measured during hospitalization. These endpoints are influenced by several factors, such as perioperative course, in-hospital medical complications, rehabilitation planning, and discharge logistics.8,17 Because of this, an actual timing effect on neurological recovery can be harder to detect with short-term outcomes. CCS is also heterogeneous. Definitions have been broad and variable, resulting in a wide spectrum of impairments and injury types being grouped under the same label, which complicates outcomes research. 18 Patients differ in baseline impairment, degenerative stenosis, instability, and cord contusion severity.8,19 Such variation, together with unmeasured differences in injury burden, can reduce the ability to detect differences between timing groups. Surgical timing is also affected by clinical decision-making. 19 Surgery can be delayed because of medical optimization, anticoagulation, transfer delays, or operating room availability. Earlier surgery can be selected for patients with concerning imaging or clinical features.19-21
Motor improvement after surgery was observed across the cohort, which is consistent with neurological recovery during hospitalization in surgically treated CCS. The absence of between-group differences suggests that, within these timing ranges, early inpatient motor change did not differ across timing categories. This finding is consistent with previous retrospective cohorts that have shown that the timing of surgery has no effect on the final neurologic outcome.22-25 Kepler et al evaluated surgically treated Acute Traumatic CCS (ATCCS) by timing, comparing surgery within 24 hours of injury with surgery performed more than 24 hours after injury. They found no short-term differences in neurologic status at 7 days and no differences in hospital length of stay or intensive care unit length of stay between cohorts. 24 Chen et al also stratified ATCCS patients by timing, including surgery within 24 hours, surgery beyond 24 hours, and surgery during a subsequent admission; no statistically significant differences were observed between the early and late subgroups. 26 Chen et al compared two cohorts based on time to surgery: one treated within 4 days of injury and the other more than 4 days after injury. At 6 months, neurologic function improved in both cohorts, without a statistically significant difference between groups. 27 Aarabi et al grouped ATCCS patients by time to surgical intervention, defined as within 24 hours, 24 to 48 hours, or more than 48 hours from injury; neurologic outcomes did not differ significantly across these cohorts. 28
Early decompression is expected to reduce ongoing compression and secondary injury processes, including edema and ischemia. At the same time, CCS includes contusion and microstructural injury, which are not reversed by short-term decompression. A systematic review by Karen et al reported improved total ASIA motor scores after very early surgery at 6 months and 1 year. The review also reported greater recovery among patients who underwent surgery within 2 weeks compared with those treated more than 2 weeks after injury, while ICU length of stay and hospital length of stay did not differ between these groups. 29 In a systematic review of observational studies, Brian et al reported that surgery within 24 hours in stable CCS with spondylosis was associated with greater improvement in total motor score than later surgery at 6- and 12-month follow-up. 30 A cohort study by Jetan et al reported that surgery within 24 hours was associated with improved upper-limb motor function at 1 year among patients with ASIA grade D injuries, whereas patients with ASIA grade C injuries showed improvement in overall motor scores. 10 A randomized clinical trial including 70 patients with traumatic spine injury reported higher motor scores at 2 weeks, 3 months, and 6 months in the early surgery group compared with delayed surgery performed 2 weeks after injury. 31 Another study reported that early surgery improved ASIA motor scores and reduced complication rates compared with delayed surgery, while mortality did not differ between groups. 11 Direct comparison across studies is limited by variation in how early surgery is defined. In our study, timing was defined from admission time, and the late category extended to 14 days, with an additional ultra-late category beyond 14 days. The motor score in this study was based on averaged strength across five muscle groups per extremity rather than standardized ASIA motor scoring. This approach supports retrospective data collection, but it can be less sensitive to small changes and reduces comparability with studies reporting ASIA motor point changes. Timing was calculated from admission rather than injury time. This is important, where admission-based timing can differ from injury-to-surgery time. This mismatch can weaken the association between timing and neurological outcomes.
The surgical approach was associated with upper-extremity motor improvement. However, Anderson et al revealed that the surgical approach in CCS appears to have no effect on motor recovery. 25 Approach selection reflects the underlying pathology, the number of compressed levels, and alignment goals.32,33 For example, an anterior surgical approach is preferred in cases of myelomalacia. 33 Therefore, this association likely reflects both treatment effect and patient selection. The associations between lower-extremity motor improvement and ultra-early timing, DM, and HF need cautious interpretation. Age was associated with ambulation at discharge. Age is also an important prognostic factor in patients with spinal cord injury. 34 This supports the role of age as an important factor for functional recovery and discharge mobility after neurological injury. 35
This study reports a single-center surgical cohort with consistent institutional practices. We assessed clinically relevant outcomes, including ICU course, ventilator outcomes, ambulation at discharge, and extremity-specific motor changes. The inclusion of multiple timing strata describes a broad range of admission-to-surgery intervals seen in clinical practice. Moreover, one important strength of the study was its robust inclusion and exclusion criteria to avoid pooling CCS with other types of spinal cord injury (in which the effects of early surgery are more established). However, the retrospective design increases the risk of selection bias and residual confounding, especially for timing decisions. The ultra-late group was small, which limits statistical power and precision. Missing outcome data for some variables can also introduce bias. Admission-based timing does not capture the actual injury-to-surgery interval, particularly in transferred patients.
Furthermore, motor outcomes were assessed using retrospectively derived extremity-specific motor strength averages rather than standardized ASIA motor scores, limiting direct comparison with prior studies and preventing the application of validated ASIA motor improvement thresholds. Finally, we focused on in-hospital outcomes and early motor change, and we did not include standardized long-term neurological and functional follow-up.
Future studies should use prospective or multicenter designs, measure true injury-to-surgery time, and apply standardized ASIA grading and ASIA motor scoring. Studies should also include imaging markers of compression and instability, and longer follow-up focused on functional outcomes and quality of life. Larger samples are also needed for more reliable subgroup analyses to confirm the findings of this study, as there was a shortage of study participants.
Conclusion
In this single-center retrospective cohort of 70 adults with CCS treated surgically, admission-to-surgery timing was not associated with in-hospital mortality, ICU length of stay, ventilator outcomes, ambulation at discharge, or early motor change, when analyzed by timing strata or as a continuous measure. Motor scores improved after surgery across the cohort. The retrospective design, admission-based timing, the small ultra-late group, and the lack of standardized long-term follow-up limit this study. Prospective multicenter studies should use injury-to-surgery intervals, standardized ASIA scoring, imaging markers, and functional outcomes.
Supplemental Material
Supplemental Material - Surgical Timing and Neurological Outcomes in Traumatic Central Cord Syndrome: A Single-Center Retrospective Cohort Study
Supplemental material for Surgical Timing and Neurological Outcomes in Traumatic Central Cord Syndrome: A Single-Center Retrospective Cohort Study by Rachel Crasta, Saeed Abdollahifard, Tyler Barnes, Mehrdad Behboodi Fahimeh Golabi, Erfan Sanaei, Ali Razmkon, Rouzbeh Motiei-Langroudi in Global Spine Journal.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of the University of Kentucky (approval number 79735).
Consent to Participate
As this is a retrospective cohort study, the IRB waived informed consent.
Author Contributions
All authors participated in drafting, reviewing, and finalizing the manuscript. SA, MB, ES, and RML contributed to analysis and data curation. RC, TB, and RBL handled data gathering and investigation. SA, FG, and AR worked on data visualization and interpretation. RML, RC, and SA contributed to conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.