
Abstract
Study Design
Retrospective Cohort study.
Objective
Posterior lumbar fusion (PLF) carries notable risks of bleeding and implant-related complications. Testosterone replacement therapy (TRT) has been associated with a myriad of medical and postsurgical-related complications in orthopedic procedures, but its impact on PLF outcomes remains unclear.
Methods
Using the TriNetX Research Network, adults undergoing PLF were identified and grouped by perioperative TRT use. After 1:1 propensity score matching demographics, comorbidities, and 3,380 patients remained per cohort. Outcomes included acute postoperative events and long-term surgical sequelae, assessed through 2 years. Risk ratios (RR), 95% confidence intervals (CI), and p-values were calculated; Kaplan–Meier curves assessed long-term event incidence.
Results
The TRT cohort had lower rates of readmission (2.07% vs. 3.05%; RR 0.69, 95% CI 0.51-0.94; p=0.016) and ED visits (2.66% vs. 4.26%; RR 0.64, 95% CI 0.49-0.83; p=0.001). There were no statistically significant differences between cohorts for DVT intensive care unit admission, PE, wound dehiscence, SSI, or AKI at 90 days. TRT use was associated with increased revision PLF (8.05% vs. 6.15%; RR 1.31, 95% CI 1.10-1.56; p=0.002). No statistically significant differences were observed for implant displacement or pseudoarthrosis.
Conclusions
Perioperative TRT exposure is associated with a favorable immediate postoperative recovery timeline, with subsequent increased revision surgery. Recognition of these risks should inform preoperative counselling, postoperative surveillance, and multidisciplinary care planning for patients undergoing PLF.
Introduction
Testosterone replacement therapy(TRT) is an emerging therapy for a variety of disease processes, such as hypogonadism, gender affirming care, and congenital disorders. 1 Hypogonadism is the most common diagnosis resulting in TRT utilization, defined as a clinical condition in which low serum testosterone is found in association with specific clinical symptoms such as decreased muscle mass and libido, along with insomnia and depression.2,3 Awareness and treatment for this pathologic state has seen a significant rise in recent years with a concomitant rise in TRT prescriptions which have expanded by more than 300% in the United States since 2001.4,5 However, TRT has been associated with a myriad of serious adverse reactions, such as increased risk of cardiovascular events, stroke, venous thromboembolism (VTE), and mortality. 6
While there is literature to suggest increased risk of adverse events with this intervention, there simultaneously exists a multitude of positive effects. TRT utilization has been shown to increase bone mineral density (BMD), lean body mass, and muscular strength, theoretically yielding positive effects in the perioperative period and subsequent rehabilitation.7,8 Despite these data, scant literature exists on the effects that TRT may have in the perioperative setting. While past investigations have demonstrated that testosterone levels decrease in the postoperative state and supplementation can assist in preventing critical muscle loss, alternative investigations have associated TRT utilization with increased medical expenditures, prosthetic joint infection, and revision surgery.9-11 Additionally, there has been an association with increased surgical site infection (SSI) and deep implant infection noted in TRT users following total shoulder and hip arthroplasty, suggesting that testosterone may play a role in immune suppression. 12
Posterior lumbar fusion (PLF) remains one of the most commonly performed lumbar spine surgeries in the United States of America and shows no signs of slowing down.13,14 Current projections suggest that by 2050, the number of single-level lumbar fusions done annually will double. 15 With the aforementioned rise in awareness surrounding adult male hypogonadism and subsequent implementation of TRT to combat this issue, it follows that in time a larger proportion of patients undergoing PLF will be prescribed these medications. Although advances in surgical technique and perioperative care have improved outcomes in the last 20 years, complication rates following PLF remain substantial, particularly regarding bleeding events, pseudoarthrosis, and postoperative infections, all of which may theoretically be impacted by TRT usage.5,16,17 Given these aforementioned trends and complications, further clarification of the interplay between TRT and perioperative outcomes in those patients undergoing PLF is crucial for clinical decision-making and preoperative risk stratification.
The primary focus of the present investigation was to clarify the interplay between TRT usage and postoperative outcomes in patients undergoing single-level PLF. We hypothesize that preoperative exposure to TRT would be associated with higher postoperative complications, including SSI, readmission, and medical complications.
Methods
Study Design and Data Source
This retrospective cohort study was conducted via the TrinetX Global Research Network (TriNetX LLC, Cambridge, MA, USA). This federated, de-identified electronic health record database is an aggregation of inpatient and outpatient data from participating healthcare organizations worldwide. TrinetX provides longitudinal information, including demographics, diagnoses, procedures, medications, and mortality outcomes, all of which are de-identified in accordance with the Health Insurance Portability and Accountability Act (HIPAA). Institutional review board approval was not obtained. To the best of the authors’ abilities and TriNetX’s capabilities, the methods in the present study were conducted most consistently in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines. 18
Patient Selection and Cohort Construction
Adult patients (≥18 years) who underwent primary, single-level PLF were identified using the Current Procedure Terminology (CPT) code. Patients were excluded if they had multi-level PLF and/or primary surgical indications for spinal cord injury (ICD10: S34) and/or spinal neoplasms (ICD10: C41.2 or C72.0). Patients with concomitant thoracic or cervical fusion procedures during the index hospitalization were also excluded to ensure cohort homogeneity.
Primary Exposure and Covariates
Exposure was defined as preoperative TRT, identified using RxNorm code 10379. Patients were classified into the TRT cohort if they had documentation of TRT use within one year before the index PLF procedure. Patients without any documented TRT exposure before surgery served as the control cohort.
Baseline demographic variables included age, sex, race, ethnicity, and body mass index (BMI). Medical comorbidities were identified using ICD-10 diagnostic codes and included diabetes mellitus (DM), hypertension, chronic obstructive pulmonary disease (COPD, chronic kidney disease (CKD), liver disease, peripheral vascular disease (PVD), coagulation disorders, smoking history, opioid dependence, dementia, benign and malignant neoplasms, testicular hypofunction, and hypopituitarism.
Outcomes
Outcomes included 30- and 90-day all-cause readmissions and ED visits following PLF. Additionally, 30- and 90-day risk of DVT, intensive care unit (ICU) admission, pulmonary embolism (PE), wound dehiscence, surgical site infection (SSI), and acute kidney injury (AKI) were also assessed. Long-term outcomes included opioid use, new onset lumbar pain, new lumbar disc herniation, implant displacement, pseudarthrosis, and revision PLF assessed at six months, one year, and two years following surgery. Outcomes were identified using ICD-10 diagnosis codes and procedural codes within the TriNetX platform.
Statistical Analysis
Baseline characteristics were summarized using descriptive statistics, with categorical variables reported as counts and percentages and continuous variables reported as means with standard deviations. Propensity score matching was performed to account for baseline differences between TRT and non-TRT cohorts. Patients were matched using a 1:1 nearest-neighbor approach incorporating demographic variables and relevant comorbidities. Balance between cohorts was assessed using standardized mean differences. Postoperative outcomes were compared between matched cohorts using risk ratios (RRs) with 95% confidence intervals (CIs). Statistical significance was defined as a two-sided p-value <0.05. All analyses were conducted using the TriNetX built-in statistical framework.
Results
Cohort Characteristics and Propensity Score Matching
Patient Demographics for Unmatched and Matched Cohorts
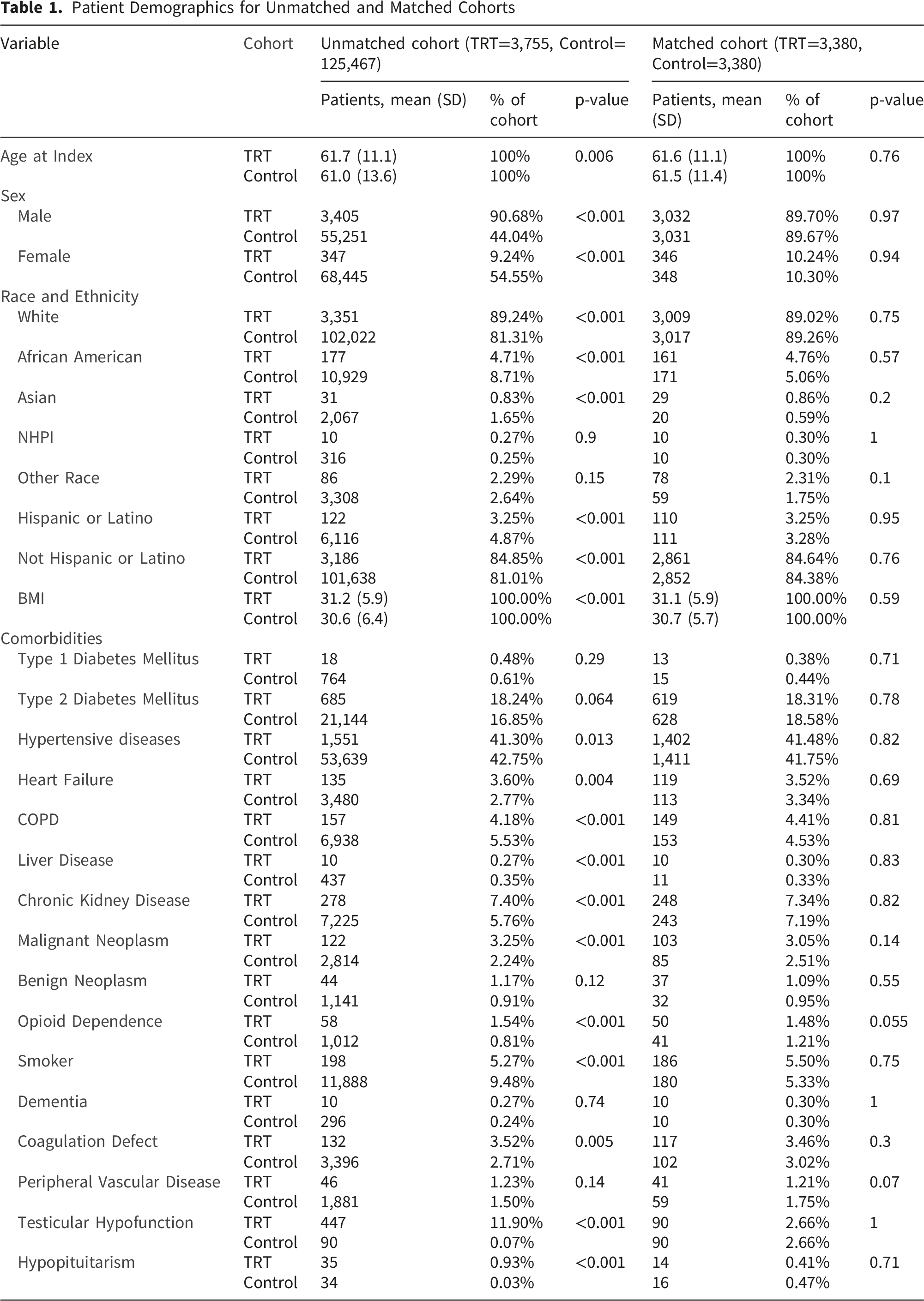
Mean body mass index was comparable between groups after adjustment (31.1 vs. 30.7 kg/m2; p=0.59). Comorbid conditions were well matched, including rates of type 1 diabetes mellitus (0.38% vs. 0.44%; p=0.71), type 2 diabetes mellitus (18.31% vs. 18.58%; p=0.78), hypertension (41.48% vs. 41.75%; p=0.82), chronic obstructive pulmonary disease (4.41% vs. 4.53%; p=0.81), heart failure (3.52% vs. 3.34%; p=0.69), and chronic kidney disease (7.34% vs. 7.19%; p=0.82). Additional comorbidities, including liver disease, malignant and benign neoplasms, opioid dependence, smoking history, dementia, coagulation defects, peripheral vascular disease, testicular hypofunction, and hypopituitarism, were also balanced between cohorts following matching [Table 1].
Short-Term Outcomes
Postoperative Complications for TRT Versus Non-TRT Cohorts Following PLF
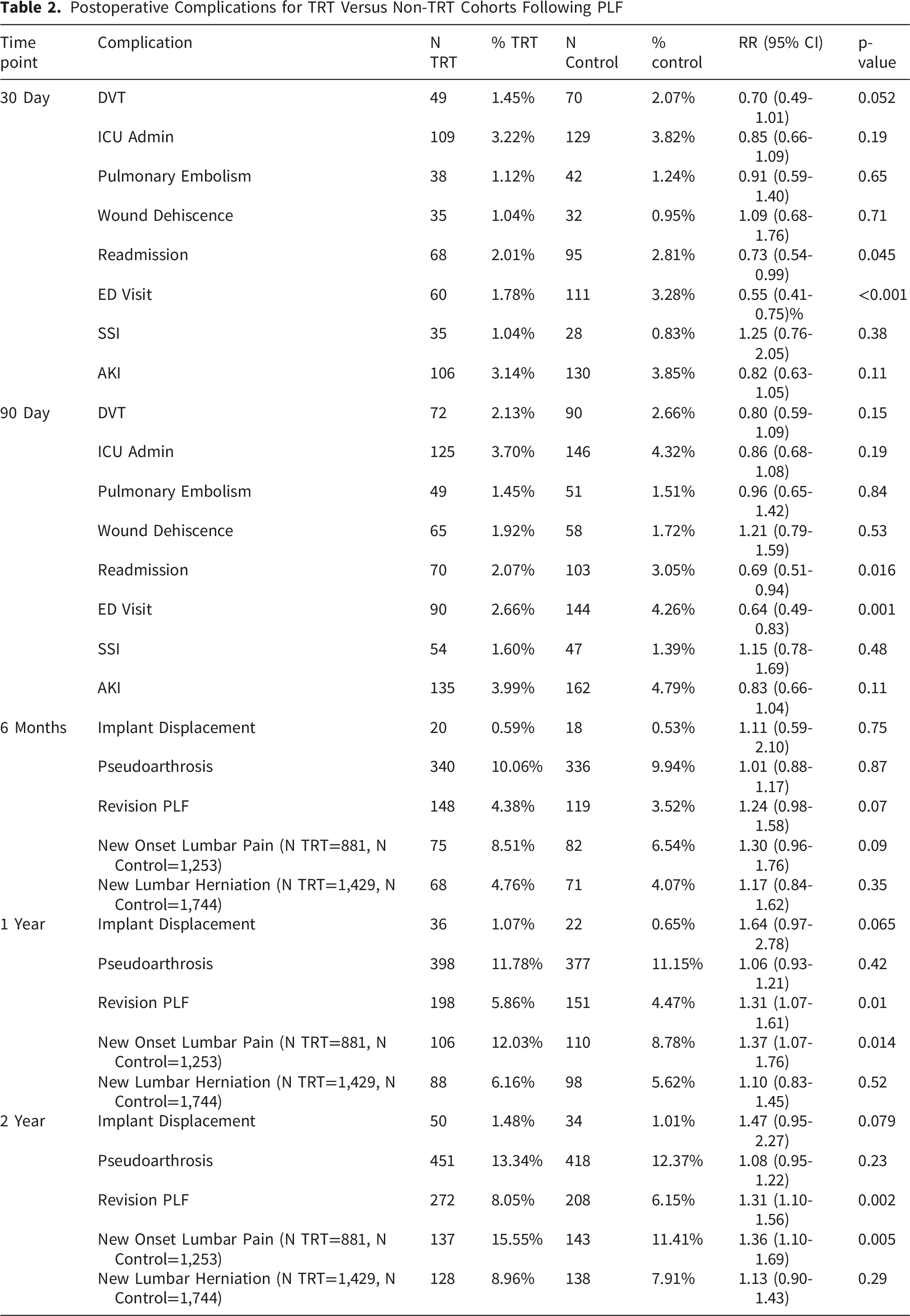
At 90 days, similar patterns persisted. The TRT cohort had lower rates of readmission (2.07% vs. 3.05%; RR 0.69, 95% CI 0.51-0.94; p=0.016) and ED visits (2.66% vs. 4.26%; RR 0.64, 95% CI 0.49-0.83; p=0.001). There were no statistically significant differences between cohorts for DVT intensive care unit admission, PE, wound dehiscence, SSI, or AKI at 90 days [Table 2].
Long-Term Outcomes
At six months following PLF, no statistically significant differences were observed at this time point in implant displacement, pseudarthrosis, revision PLF, new onset lumbar pain, or new onset lumbar disc herniation [Table 2, Figure 1]. Cumulative incidence of revision posterior lumbar fusion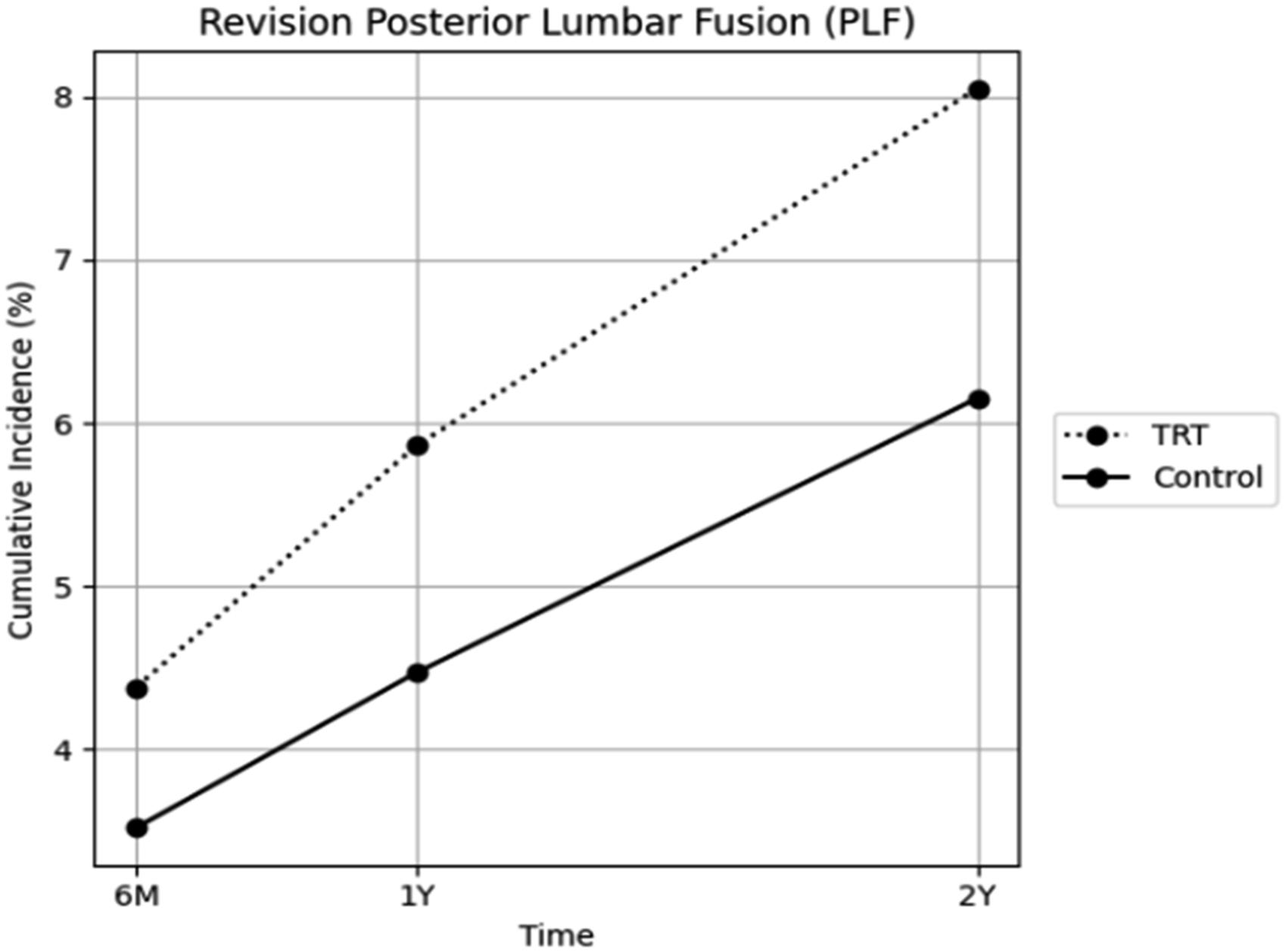
At one year postoperatively, the TRT cohort demonstrated higher rates of revision PLF (5.86% vs. 4.47%; RR 1.31, 95% CI 1.07-1.61; p=0.010), and new-onset lumbar pain (12.03% vs. 8.78%; RR 1.37, 95% CI 1.07-1.76; p=0.014). No differences were observed in implant displacement, pseudarthrosis, or new lumbar disc herniation.
Two years following the index, primary PLF, these differences persisted. Patients in the TRT cohort continued to demonstrate higher rates of revision PLF (8.05% vs. 6.15%; RR 1.31, 95% CI 1.10-1.56; p=0.002), and new-onset lumbar pain (15.55% vs. 11.41%; RR 1.36, 95% CI 1.10-1.69; p=0.005). No statistically significant differences were observed for implant displacement, pseudarthrosis, or new onset lumbar disc herniation at long-term follow-up [Table 2].
Discussion
Exogenous testosterone use in musculoskeletal surgery historically garnered popularity via purported postoperative recovery benefits; however, more contemporary trends show a significant rise in utilization for treatment of acquired hypogonadism.3,19 This investigation represents the first large-scale analysis to evaluate the association between TRT use and postoperative complications following PLF. Our findings demonstrate that preoperative TRT exposure was independently associated with decreased postoperative ED utilization and readmission, suggesting beneficial effects on immediate postoperative recovery trajectories. However, TRT exposure was associated with increased long-term revision rates, suggesting a lack of long-term protective benefit.
In the perioperative period, TRT exposure was associated with a significantly decreased risk of readmission and ED visits. Given that TRT is associated with increased skeletal muscle mass, exercise capacity, and self-reported function and mobility, it is plausible that these findings could be the result of an improvement in functional activity profiles in patients on TRT.20,21 Previous literature has demonstrated that increased postoperative activity and ambulation have been associated with decreased risk of readmission after surgery. 22 Additionally, TRT usage has been associated with a litany of medical complications and major postoperative adverse events, attributed to testosterone’s direct stimulation of erythropoiesis, with resultant increase in overall blood viscosity, theoretically increasing thrombogenesis. 6 However, despite the physiologic implications of TRT usage on blood viscosity, the present investigation failed to demonstrate any significant differences in clinical outcomes including PE, DVT, AKI, or ICU admission, within the 90-day postoperative period. These findings lend credence to the growing body of literature suggesting that TRT supplementation in the perioperative period may be safer than once thought. A recent high-powered investigation by Lincoff et al highlighted the cardiovascular safety of TRT, demonstrating no increase in major cardiac adverse events compared to placebo. 23 Similarly, a variety of recent evidence has also demonstrated that TRT can be continued perioperatively without increased risk for VTE.24-26
Furthermore, there was no significant difference in those patients with TRT exposure and resultant SSI or wound dehiscence following PLF. This finding contrasts with previous orthopaedic literature, which demonstrated that TRT was associated with an increased risk of periprosthetic joint infections after total joint arthroplasty.10,11,27 It is integral to note that the previous investigations often cited Cultibacterium acnes (C. acnes) as the primary infectious organism in these cases, with subsequent literature demonstrating a parallel association between serum testosterone levels and resultant C. acnes infection.11,28 While the cited incidence of C. acnes infection is notably increasing throughout the spine literature, it is most commonly associated with posterior cervical surgery, where there is a higher number of hair follicles.29,30 Furthermore, our reported rate of SSI of 1.6% is comparable to previous investigations reporting on rates of infection following PLF, further exemplifying that our large propensity-matched cohort accurately reflects the more general population.31,32 These findings provide further evidence that TRT exposure appears to be safe in the perioperative period without increased risk of significant medical events or increased risk of postoperative wound complications.
Extensive literature exists concerning the role of testosterone in the prevention of osteoporosis and bone loss in elderly males, with clinical studies demonstrating higher bone mineral density (BMD) in those patients exposed to TRT.33,34 Despite this, the role of pharmacologic exogenous testosterone application in relation to spinal fusion rates is nonexistent. Notably, the present investigation uncovered that preoperative TRT exposure was not associated with any observed differences in pseudoarthrosis or implant displacement at long-term follow-up. Future research is necessary to granularly characterize rates of fusion in those patients utilizing TRT. However, the present investigation lends credence to the notion that TRT use may not have detrimental effects on osseous integration or postoperative fusion status.
Despite these observations, those patients exposed to TRT were significantly more likely to undergo revision procedures at one and two-year time frames, coinciding with previous literature regarding total joint arthroplasty.27,35 While granular data concerning the indication for revision were not collected due to constraints of national database-driven data, the literature is well versed in the fact that revision lumbar fusions are most commonly performed predominantly for indications of adjacent segment disease (ASD), pseudoarthrosis, recurrent stenosis, implant-related issues, and infection.36,37 Given that no differences were observed in rates of pseudoarthrosis, implant-related issues, or SSI, it is reasonable to assume that many of these revisions may have been indicated for ASD or recurrent stenosis. TRT use is associated with improved exercise capacity and function, with resultant higher mechanical demand of the fusion construct, which may predispose TRT patients to ASD/recurrent stenosis and subsequent reoperation. 20 Although the specific indication for revision surgery could not be determined within the present database, revision lumbar fusion itself remains a clinically meaningful endpoint associated with increased morbidity, healthcare utilization, and cost. 17 Therefore, the observed association between TRT exposure and revision surgery remains relevant despite uncertainty regarding the underlying mechanism. Future prospective investigations incorporating operative reports, imaging findings, and patient-reported outcomes are needed to identify the specific drivers of reoperation in this population.
This study has multiple limitations. First, given the limitations of the database, the study was unable to capture potentially important clinical variables, such as the dose, route, duration, or resultant testosterone levels of TRT regimens during the preoperative and postoperative periods. With this, there was no differentiation between the indications for TRT. Furthermore, the present investigation was unable to characterize perioperative management of TRT medications, and thus, variability was likely present concerning institutional protocols for preoperative TRT cessation and postoperative treatment resumption, which may add heterogeneity to the study population. Additionally, the lack of clinical granularity regarding documentation of preoperative symptom severity and duration may have played a role in reoperation rates. Also, given the nature of TriNetX, there may exist an underestimation of the true incidence of complications secondary to the database relying on procedure and diagnostic codes to identify complications. For example, some literature reports using diagnostic codes have the potential for misclassification of data, which could result in missed complications. 38 Similar to all observational analyses, which include retrospective cohort studies, this type of study is only able to provide associations rather than establish causality. 39 Also, given the lack of patient-reported outcome measures, it remains unknown whether patients on TRT derive the same clinical benefit from PLF compared to other populations. Finally, surgical details, techniques, and implants were not recorded, which may have influenced outcomes. Future institutional-level investigations are needed to provide clarity in the role that these variables may play in these perioperative recovery trajectories.
Conclusion
Perioperative TRT exposure is associated with a favorable immediate postoperative recovery timeline, transposed with subsequent increased revision surgery and concomitant long-term opioid utilization. These effects emerge in the long-term postoperative period, suggesting that TRT exposure may lack long-term protective benefits. Recognition of these risks should inform preoperative risk counselling, postoperative surveillance, and multidisciplinary care planning for patients undergoing PLF.
Footnotes
Consent to Participate
The use of entirely de-identified records qualified this study as non-human research and is therefore exempt from institutional review board oversight.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.