
Abstract
Study Design
Retrospective cohort study.
Objectives
To evaluate patient, injury, and hospital-level predictors of in-hospital mortality following operative management of cervical spinal cord injury (cSCI) using a national trauma registry.
Methods
A retrospective cohort study was performed using the National Trauma Data Bank (NTDB) from 2021 to 2023. Adult patients with cSCI were identified using ICD-10-CM diagnosis codes and included if they underwent operative treatment at the cervical spine level. Patient and injury characteristics were assessed using the Abbreviated Injury Scale (AIS) and Injury Severity Score (ISS). Hypotension and Glasgow Coma Scale (GCS) were used to characterize arrival physiology. Multivariable logistic regression identified independent predictors of in-hospital mortality, with significance set at the P < 0.05 level.
Results
Among 18,401 operatively managed cSCI patients, 1,222 (7.1%) died in-hospital, with no variation across years (P = 0.827). Compared with survivors, decedents were older, more often male, and more frequently injured by falls (all P ≤ 0.007). Polytrauma and hypotension were more common among in-hospital deaths (both P < 0.001), and decedents demonstrated higher injury severity and worse presenting neurologic status (both P < 0.001). In adjusted analyses, mortality was independently associated with older age, higher ISS, worse GCS, hypotension, critical spine AIS severity, and polytrauma. Key comorbidity predictors included advanced directives limiting care, functional dependence, congestive heart failure, chronic renal failure, cirrhosis, diabetes mellitus, and anticoagulant therapy.
Conclusions
In-hospital mortality after operative cSCI was 7.1% and was driven by initial physiology, neurologic status, injury severity, and comorbidity burden.
Keywords
Introduction
Cervical spinal cord injuries (cSCI) are a leading traumatic cause of death and disability and represent a major cause of early postoperative mortality. 1 Inpatients require acute specialized care and constant monitoring, as well as advanced measures such as respiratory support. Cervical SCIs are expensive to hospitals and patients alike. Surviving patients are frequently disabled, resulting in loss of independence and productivity, as well as psychological burden.2-5 The cervical spine is injured in 52-54% of all spine injuries worldwide. 6 Though global and regional patterns of cSCI are variable, males represent between 68.3 to 82.2% of cSCI patients and elderly patients are also affected more often with worse outcomes.3,7 As the median ages of cSCI cohorts increases, falls have emerged as a major etiology, supplanting motor vehicle accidents and other causes such as sports injuries which disproportionately affect younger patients.8,9
In-hospital mortality after cSCI ranges from 5.6 to 38% in some cohorts, though most large studies place the figure between 5 and 12%.10,11 Single and multi-center studies have elucidated important predictors of in-hospital complications and mortality. Increased age, polytrauma, neurological severity at presentation, and respirator dependence are commonly cited as factors that increases risk of in-hospital mortality.9,12,13 Charlson comorbidity index (CCI) and pre-existing organ dysfunction are also associated with poor outcomes and mortality.9,14
Given the clinical complexity and resource intensity of acute in-hospital care after cSCI, contemporary population-level data are needed to support early risk stratification, triage, and resource allocation. Therefore, this study aimed to: (1) characterize contemporary patient demographics, injury severity profiles, comorbidity burden, and treating hospital characteristics among adults undergoing operative management for cSCI using the National Trauma Data Bank (NTDB); (2) describe national patterns and rates of in-hospital mortality following operative cSCI; and (3) identify independent patient, injury, and hospital-level predictors of in-hospital mortality using multivariable regression. We hypothesized that in-hospital death would be primarily driven by worse presenting physiology and neurologic status, greater overall injury burden, and greater comorbidity/frailty markers.
Methods
Data Source
This was a retrospective cohort study analyzing patients undergoing operative management of cSCI using the NTDB from 2021 to 2023. The NTDB is the largest aggregation of U.S. trauma registry data, maintained by the ACS as part of its Trauma Quality Programs. 15 Institutional Review Board (IRB) approval was not required, and informed consent was deemed exempt due to the use of a publicly available, de-identified dataset.
Cohort Identification and Exclusion Criteria
The NTDB was queried for adult patients presenting with a cSCI using ICD-10-CM diagnosis codes starting with S14.1. These SCI encounters were merged with the NTDB trauma, Abbreviated Injury Scale (AIS), preexisting condition, hospital-event, and ICD-10-PCS procedure files using unique patient identifiers. Patients were excluded if they did not undergo surgical treatment at the level of the cervical spine, were aged less than 18 years, contained missing sex, died in the emergency department, lacked spine AIS information, or contained missing Glasgow Coma Scale (GCS) scores at presentation. A variable indicating the presence of hypotension (systolic blood pressure <90 mm Hg) upon admission to the emergency department (ED) was created. Patients were stratified by in-hospital mortality.
Injury Severity, Polytrauma, and Mechanism of Injury
Injury severity was assessed using both the Injury Severity Score (ISS) and AIS, each treated as categorical variables in all descriptive statistics and models. ISS was categorized as mild (<16), moderate (16-24), or severe (≥25). Similarly, spine AIS scores were grouped as minor (1-2), serious (3), severe (4), or critical (5-6). A maximum non-spine AIS severity score variable was generated to identify polytrauma, defined as a non-spine AIS score greater than or equal to 3, indicating serious trauma outside the cervical spine region. Mechanism of injury was also captured from each encounter, which was derived from ICD-10-CM external cause-of-injury codes recorded in the NTDB PUF. Encounters were categorized as relating to falls (W00–W19), motor vehicle/transport-related mechanisms (V00–V99), intentional self-harm (X60–X84), or other (all remaining external-cause codes, including assault, undetermined intent, and other specified mechanisms).
Demographics, Comorbidities, and Hospital Characteristics
Patient demographics and presentation included age, sex, race, and GCS upon admission. Several clinically relevant comorbidities were extracted from the database and are presented both descriptively and as predictors of in-hospital mortality following operative management of cSCI. These comorbidities include alcohol use disorder, bleeding disorder, receiving chemotherapy for cancer, congestive heart failure, current smoker, chronic renal failure, cerebrovascular accident, diabetes mellitus, disseminated cancer, advanced directive limiting care, functionally dependent health status, hypertension, chronic obstructive pulmonary disease (COPD), steroid use, cirrhosis, dementia, anticoagulant therapy, myocardial infarction, peripheral arterial disease, and substance abuse disorder.
Hospital bed size was categorized as ≤200, 201–400, 401–600, or >600 beds. Teaching status was grouped as community, non-teaching, or academic, taken directly from the NTDB facility teaching variable per NTDS definitions. Trauma center verification level was also extracted.
Outcomes
The primary outcome of this study was to identify independent predictors of in-hospital mortality following operative management of cSCI. Secondary outcomes were to observe the differences in patient and hospital demographics, comorbidities, and injury-related severity metrics across mortality cohorts. In addition, the mechanism of injury across age groups (18 to 39, 40 to 64, and ≥65) was recorded to describe age-related differences in injury mechanisms contributing to cSCI.
Statistical Analysis
Continuous variables were summarized using means with standard deviations and compared between mortality groups using Student’s t tests or Wilcoxon rank-sum tests, as appropriate based on distribution and sample size. Categorical variables were summarized as frequencies with percentages and compared using χ2 tests or Fisher’s exact tests when expected cell counts were small.
Multivariable logistic regression was performed to identify independent predictors of in-hospital mortality following operative management of cSCI. Covariates were selected a priori based on clinical relevance and included age, sex, race, year of admission, mechanism of injury, ISS, GCS on presentation, maximum spine AIS score, presence of severe non-spine injury (non-spine AIS ≥ 3), presence of hypotension, hospital teaching status, hospital bed size, trauma center level, and pre-existing comorbidities. Multicollinearity among covariates in the multivariable model was also assessed. All adjusted generalized variance inflation factor (GVIF) values were low, with the highest values observed for ISS category (1.55), spine AIS category (1.32), and severe non-spine injury (1.24), supporting simultaneous inclusion of these injury severity variables.
Complete-case analysis was used for multivariable modeling; encounters with missing data for any covariate included in the regression were excluded. Missingness was assessed for all variables included in the multivariable model. Trauma center verification level demonstrated the highest rate of missingness (21.6%), while missingness was low for hypotension on presentation (1.2%), spine AIS category (1.2%), and teaching status (0.2%). Model results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was defined as P < 0.05. All analyses were performed using R statistical software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Demographics, Injury Characteristics, and Hospital Factors
Patient, Injury, and Hospital Characteristics by Mortality Status
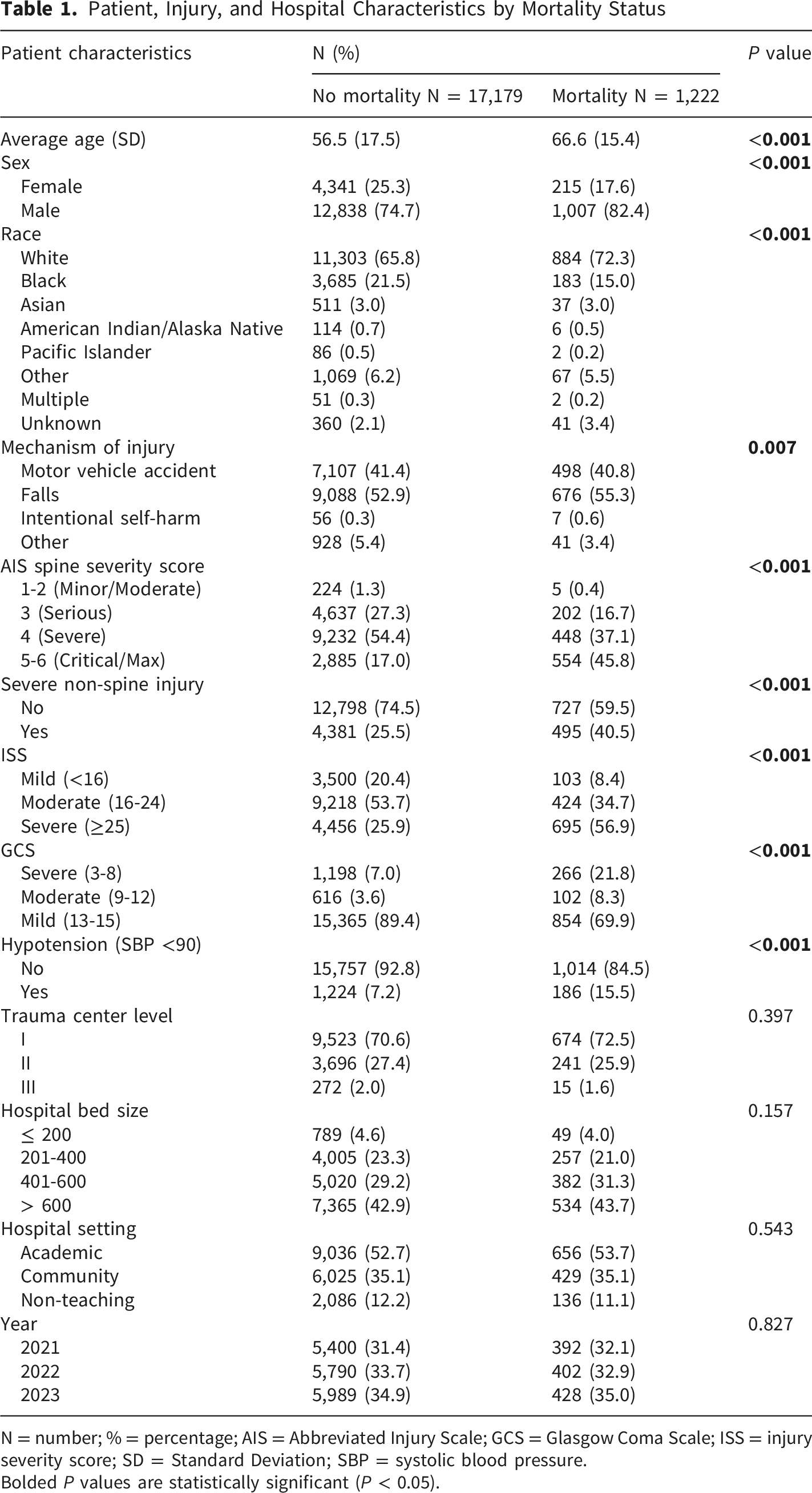
N = number; % = percentage; AIS = Abbreviated Injury Scale; GCS = Glasgow Coma Scale; ISS = injury severity score; SD = Standard Deviation; SBP = systolic blood pressure.
Bolded P values are statistically significant (P < 0.05).
Mechanism of injury varied across groups, with injuries more frequently coming from falls in the mortality cohort (55.3% vs 52.9%, P = 0.007; Table 1). In patients aged 65 years and older, approximately 70% of injuries were due to falls. In contrast, the predominant mechanism of injury in the youngest cohort (18 to 39 years of age) was a motor vehicle accident, underscoring age-related differences in injury mechanisms contributing to cSCI (Figure 1). Distribution of mechanism of injury by age group among operative cervical spine injury admissions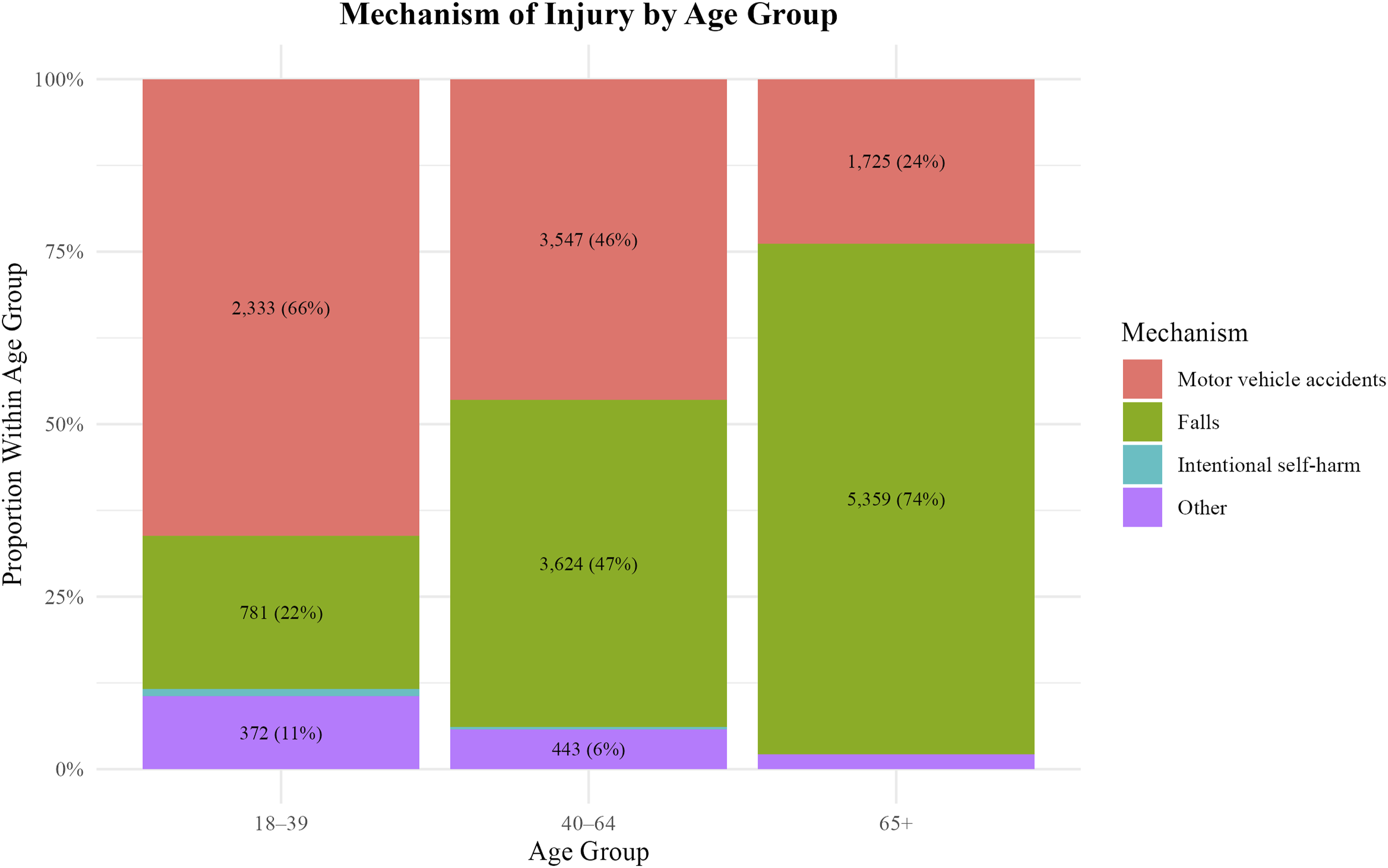
Polytrauma, as defined by a severe non-spine AIS score, was significantly more likely in those experiencing in-hospital death (40.5% vs 25.5%, P < 0.001). Hypotension on presentation (SBP <90 mmHg) was also more common among in-hospital deaths (15.5% vs 7.2%, P < 0.001). Injury severity was significantly worse in the mortality cohort, with a higher proportion of severe ISS (≥25: 56.9% vs 25.9%) and lower proportion of mild ISS (<16: 8.4% vs 20.4%, P < 0.001). Similarly, patients who died were more likely to have critical/maximal spine AIS scores (5–6: 45.8% vs 17.0%). Presenting neurologic status was also poorer in the mortality group, with higher rates of severe GCS (3–8: 21.8% vs 7.0%) and moderate GCS (9–12: 8.3% vs 3.6%), and lower rates of mild GCS (13–15: 69.9% vs 89.4%, P < 0.001; Table 1).
Bed size distributions were broadly similar across cohorts (P = 0.157), and there were no observed differences in the types of facilities at which these patients were treated with regard to trauma level (P = 0.397) or teaching status (P = 0.543; Table 1).
Prevalence of Comorbidities
Prevalence of Comorbidities by Mortality Status
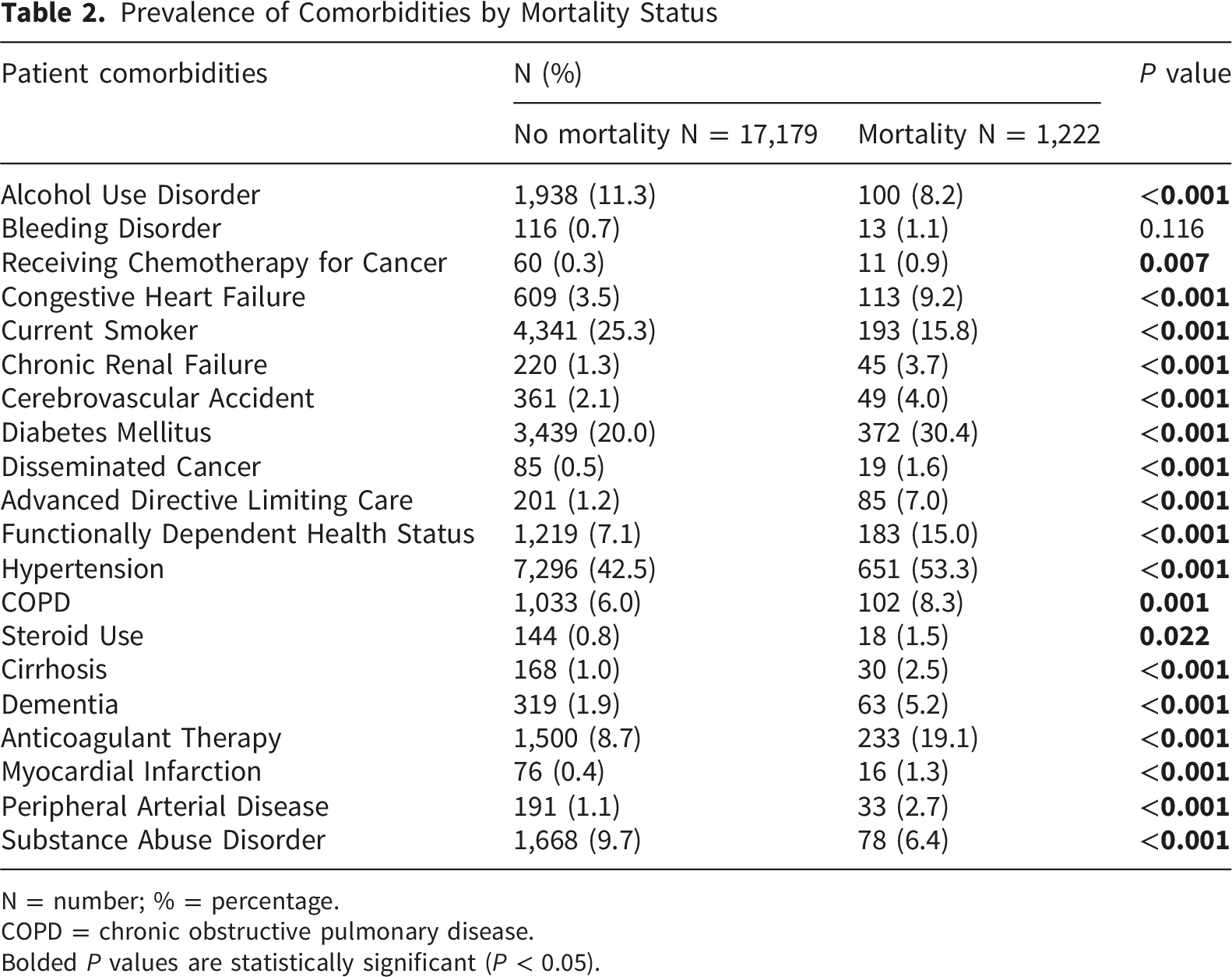
N = number; % = percentage.
COPD = chronic obstructive pulmonary disease.
Bolded P values are statistically significant (P < 0.05).
Adjusted Analyses
Predictors of In-Hospital Mortality
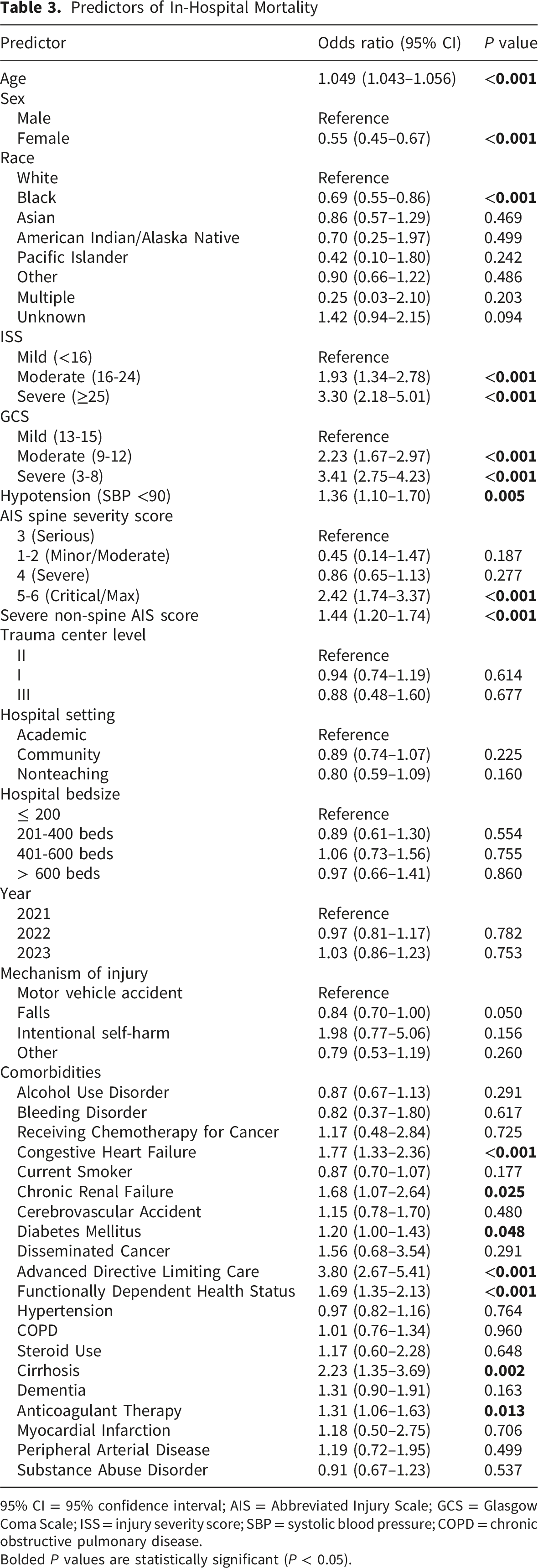
95% CI = 95% confidence interval; AIS = Abbreviated Injury Scale; GCS = Glasgow Coma Scale; ISS = injury severity score; SBP = systolic blood pressure; COPD = chronic obstructive pulmonary disease.
Bolded P values are statistically significant (P < 0.05).
Discussion
This retrospective study of the NTDB analyzed patient, hospital, and injury-related factors associated with in-hospital mortality among surgically treated cSCI patients. The findings showcase age-related differences in injury mechanisms, with a progressive transition from predominantly high-energy trauma in younger patients to lower-energy mechanisms in elderly patients. When stratified by mortality status, those suffering an in-hospital death experienced a greater comorbidity burden, higher rates of polytrauma and injury severity, and decreased neurological status on admission. Adjusted analyses revealed several clinically meaningful predictors of mortality, including older age, greater injury severity, lower presenting neurologic status and blood pressure, presence of polytrauma, and higher comorbidity burden — particularly advanced directives limiting care, functional dependence, congestive heart failure, cirrhosis, diabetes, renal failure, and anticoagulant use. Together, these findings may help guide early identification of high-risk patients requiring greater perioperative resources, including ICU-level monitoring, respiratory support, hemodynamic optimization, and multidisciplinary care coordination, while also underscoring the importance of age-informed prevention strategies, particularly fall prevention in older adults, and risk stratification that accounts for injury mechanism and frailty.
This study found a 7.1% rate of in-hospital mortality among operatively managed cSCI patients, aligning with rates reported throughout the literature.16,17 Mechanism of injury across age groups displayed considerable variation. The youngest cohort, aged 18 to 39 years, predominately presented because of a high-impact motor vehicle trauma, whereas the oldest cohort, aged 65 years and older, was most frequently admitted due to a fall. These age-related differences in injury mechanisms are supported by prior investigations, including a study that found falls to be responsible for nearly 75% of all SCIs in patients aged 76 years or older. 18 As the population continues to age, frailty measures are becoming more clinically relevant as a means of assessing overall perioperative risk. A retrospective multicenter cohort study conducted by Karthikeyan et al. categorized adult patients into robust, prefrail, and frail groups using a pragmatic tool. 19 The authors discovered a marked gradient across frailty strata, in which in-hospital mortality increased substantially from 6% in the robust group to 23% in the frail group. As such, the intersection of age, injury mechanism, and frailty should remain a central focus in improving surgical outcomes and guiding individualized care pathways for cSCI patients.
Patient and injury-related characteristics varied substantially across cohorts. Cervical SCI patients experiencing an in-hospital mortality were more likely to be male, present with worse neurologic status on admission, have greater spine and non-spine injury severity scores, and arrive to the ED with hypotension. The predominance of males experiencing an SCI in this study aligns with prior investigations.20,21 In this study, decedents were, on average, approximately 10 years older than survivors, and age was noted as an independent predictor of mortality status on multivariable analysis. A registry-based study with longitudinal outcomes among surgically treated traumatic SCI patients corroborates the observed influence of age on survival. 22 Specifically, the authors noted a six-fold increase in the odds of mortality within 50 days postoperatively in patients ≥77 years of age versus those 65-76 years of age. Interestingly, female sex and Black race were independently associated with lower odds of in-hospital mortality. While prior studies have reported demographic differences in outcomes following traumatic spinal cord injury, the mechanisms underlying these associations remain incompletely understood and may reflect differences in injury patterns, comorbidity profiles, social determinants of health, or unmeasured confounding factors not captured within the NTDB. Trauma center verification level and hospital size were not independently associated with in-hospital mortality, which may be explained by residual case-mix differences, whereby more severely injured patients are preferentially triaged or transferred to larger and higher-level centers, as well as unmeasured institutional factors not captured within the NTDB. Arrival physiology has been extensively researched regarding its impact on outcomes in SCI patients. A meta-analysis conducted by Tanvir et al. analyzed the effect of mean arterial pressure on functional recovery in acute SCI patients, highlighting the association of hypotension with worse outcomes across all subgroups analyzed. 23 Our findings add to this work by suggesting 36% increased adjusted odds of mortality in cSCI patients presenting to the ED with low blood pressure. In addition, high cervical spinal cord injuries may be complicated by autonomic dysfunction, including thermoregulatory disturbances such as quad fever, further highlighting the physiologic vulnerability of this patient population and the need for close inpatient monitoring. Coupled with the increased rates of polytrauma, higher injury severity scores, and impaired presenting neurological status observed in the mortality group, these findings reveal a high-risk presentation profile that may help identify patients vulnerable to early in-hospital death.
Comorbidity burden was substantially elevated in the group suffering an in-hospital mortality. While the unadjusted rates of most comorbidities met the criteria for statistical significance, multivariable adjustment identified several key predictors, including advanced directives limiting care, functional dependence, congestive heart failure, cirrhosis, diabetes, renal failure, and anticoagulant use. Taken together, these predictors define a high-risk profile for in-hospital mortality, in which multisystem comorbidity may limit physiologic reserve – a relationship that may be partially mediated or reflected by the functional dependence observed in the mortality group. Consistent with our findings, a study conducted by Blex et al. identified pre-existing kidney and liver disease as predictors of in-hospital mortality following traumatic SCI. 17 Approximately 2.2 million adults in the United States suffer from cirrhosis, and chronic kidney disease affects an estimated 10% of the global population.24,25 As such, comorbid liver and kidney disease represent common, clinically meaningful risk factors that should be incorporated into early prognostication and perioperative planning for traumatic cSCI. The increased odds of in-hospital mortality in patients undergoing anticoagulation therapy may reflect an elevated risk of bleeding and other perioperative complications in this cohort, as highlighted in prior studies. 26 Nevertheless, this remains an area of extensive debate within the spine surgery literature, with many other well-designed studies illustrating no additional detrimental effect.27-29 For instance, a single-center study conducted by Camil et al. found that among 63 trauma patients requiring cervical spine decompression and fusion, anticoagulation therapy was not associated with increased rates of perioperative complications or a decline in ASIA scores postoperatively. 27 Overall, these findings support early, structured risk stratification and multidisciplinary perioperative planning — particularly for patients with renal/hepatic disease, heart failure, functional dependence, or advanced directives limiting care — to better guide prognostication, surgical decision-making, and family counseling after traumatic cSCI.
The current study is not without limitations. The retrospective design inherently limits our ability to establish causality and introduces the potential for selection bias. The NTDB does not capture cause-of-death detail; therefore, in-hospital mortality is interpreted as a surrogate endpoint that may encompass both direct injury-related and secondary medical causes. Similarly, the strong association observed for advanced directives limiting care should be interpreted cautiously, as this variable may capture patients in whom treatment limitations or withdrawal of life-sustaining measures contributed to mortality independent of injury severity. The NTDB is also subject to billing and coding errors that may result in misclassification of injury severity, comorbidities, or procedural details. This study was limited to mortality occurring at the index admission; longitudinal follow-up could not be carried out and, thus, mortality rates may be underestimated due to the inability to capture deaths occurring after discharge or during subsequent hospitalizations. Detailed neurological examination findings, including International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) assessments, American Spinal Injury Association (ASIA) Impairment Scale grades, injury completeness, and motor and sensory examination data, are not available in the database and therefore could not be assessed. In addition, the NTDB does not provide granular data on the specific surgical technique used, including the number of levels fused or construct characteristics. Although operative timing is a well-established determinant of outcomes in spine trauma, the available NTDB timing fields may not reliably capture the interval from injury to surgical decompression. Therefore, this variable was not included in the analysis and may represent a source of residual confounding. Other intraoperative factors, such as blood loss, operative time, and surgeon experience, were also unavailable. The absence of these variables may also introduce unmeasured confounding and limit the generalizability of the present findings. Additionally, multivariable analyses were performed using a complete-case approach. Although missingness was low for most variables, exclusion of incomplete encounters may have introduced selection bias. Despite these limitations, this study highlights key predictors of in-hospital mortality among cSCI patients, showcasing the multifactorial nature of outcomes in this population and the importance of comprehensive risk stratification in guiding early management decision.
Conclusions
The in-hospital mortality rate following surgically treated cSCI in this study was 7.1%. Compared to survivors, patients in the mortality group had worse presentation upon admission, including higher rates of hypotension, lower GCS scores, more frequent polytrauma, and increased injury severity scores. Mechanism of injury varied across age groups, with the oldest cohort of patients admitted due to a fall. After multivariable adjustment, key comorbidities were associated with increased odds of mortality following operatively managed cSCI, including advanced directives limiting care, functional dependence, congestive heart failure, cirrhosis, diabetes, renal failure, and anticoagulant use. Future studies should aim to incorporate standardized measures of frailty, detailed operative variables, and timing to decompression or stabilization to better delineate modifiable risk factors and optimize perioperative outcomes in this vulnerable population.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.