
Abstract
Study Design
Systematic review.
Objectives
To synthesize outcomes, complications, and healthcare utilization after surgery for degenerative cervical myelopathy (DCM) in patients with Parkinson disease (PD).
Methods
PubMed/MEDLINE, EMBASE, and the Cochrane Library were searched from inception to March 2026. Eligible studies evaluated adults with PD undergoing cervical decompression with or without fusion for DCM; studies not specifically defining myelopathy but reporting cervical outcomes within broader PD spine cohorts were retained as indirect supportive evidence. Two reviewers independently screened studies, extracted data, and appraised quality using standard checklists. Because of marked heterogeneity, findings were synthesized narratively, with greater weight given to myelopathy-defined cohorts.
Results
Eleven studies were included: 5 myelopathy-defined cohorts and 6 supportive studies. In myelopathy-defined cohorts, PD patients improved after surgery, but some studies showed smaller gains in modified Japanese Orthopaedic Association (mJOA) or Nurick scores, lower odds of clinically important mJOA improvement, and less EQ-5D improvement compared with non-PD controls. Database studies showed higher complication rates, longer hospital stays, non-home discharge, and a dysphagia/aspiration signal. Supportive studies suggested similar increases in hospitalization and medical complications and raised concern for long-term mechanical failure or reoperation.
Conclusions
The most direct evidence suggests that patients with PD undergoing surgery for cervical myelopathy may improve neurologically, although functional recovery may be smaller or less clinically meaningful in some cohorts. Perioperative risk and healthcare utilization also appear higher. Indirect supportive evidence further suggests that dysphagia or aspiration-related events and long-term mechanical failure or reoperation are important concerns in this population.
Keywords
Introduction
Parkinson disease (PD) is a neurodegenerative disorder, with a rapidly rising incidence and a prevalence that increases sharply with age; an increasing number of patients live long enough to develop coexisting degenerative conditions of the spine.1-3 Motor features such as bradykinesia, rigidity, and postural instability, together with disease-associated frailty and impaired bone health, contribute to falls, abnormal spinal loading, and progressive degenerative or deformity-related changes. In clinical practice, degenerative cervical or lumbar pathology may also present with gait disturbance and postural imbalance, potentially obscuring the contribution of PD itself and delaying definitive diagnosis and treatment of structural cord or nerve root compression. 4
Degenerative cervical myelopathy (DCM), historically termed “cervical spondylotic myelopathy,” (CSM) represents a common cause of spinal cord dysfunction in older adults and is typically managed with surgical decompression, with or without fusion, to arrest neurological deterioration and, in many patients, improve function and health-related quality of life (QoL).5,6 Yet, when PD coexists, outcome assessment is challenging because gait dysfunction and balance impairment may reflect both central neurodegeneration and myelopathy. Moreover, compromised muscle control, osteopenia/osteoporosis, and progressive sagittal imbalance have been implicated as contributors to hardware-related failure, loss of alignment, and the need for revision surgery after spinal procedures in PD.7-10
Over the last decade, several literature reviews and systematic reviews/meta-analyses have attempted to synthesize evidence on spine surgery in PD, generally reporting heterogeneous indications, surgical strategies, and outcome measures across small case series and database studies.4,8,11,12 More recent work has further underscored that PD populations undergoing fusion are not uniform, and that construct characteristics and surgical intent may influence prognosis. 13 However, cervical myelopathy constitutes a distinct clinical entity in which timely decompression may prevent irreversible cord injury, and myelopathy-specific outcomes (e.g., neurological recovery scales) are not consistently captured in broader PD-spine syntheses. 14
Accordingly, we conducted a systematic review focusing on patients with PD undergoing surgery for degenerative cervical myelopathy. Our objectives were to summarize the available evidence on postoperative neurological and patient-reported outcomes (PROs), perioperative complications, and healthcare utilization, and to identify key gaps to guide future research and preoperative counseling.
Methods
Protocol and Registration
This systematic review evaluated outcomes of surgical treatment for degenerative cervical myelopathy in patients with PD. Reporting follows the PRISMA 2020 statement. 15 The protocol was registered on the Open Science Framework (OSF). 16 No substantive amendments were made after registration.
Information Sources and Search Strategy
We searched PubMed, EMBASE, and the Cochrane Library using controlled vocabulary (e.g., MeSH/Emtree) and free-text keywords related to PD, cervical myelopathy/cervical spondylotic myelopathy, and cervical spine surgery (decompression and fusion procedures). The final search was conducted on March 14, 2026. No language restrictions were applied. Reference lists of included studies were also screened. Full database-specific search strings are provided in Supplementary Table S1.
Eligibility Criteria
We included clinical studies of adult patients with PD undergoing cervical spine surgery for degenerative cervical myelopathy/cervical spondylotic myelopathy, or studies that allowed extraction of clinically relevant, myelopathy-supportive evidence for PD patients undergoing cervical procedures. Eligible designs included comparative observational studies (retrospective/prospective cohorts, registry analyses, and administrative database studies) and case series. We excluded studies without cervical surgery, purely technical reports without outcome data, and studies limited to non-degenerative etiologies (e.g., trauma, tumor, infection) unless degenerative subgroups were extractable.
To avoid conflation of distinct clinical questions, we prespecified an evidence-structuring framework based on “myelopathy specificity.” Studies were classified as tier A: myelopathy-defined cohorts reporting neurologic/functional recovery and/or patient-reported outcomes; tier B: myelopathy-defined cohorts reporting perioperative safety and resource utilization; and tier C: supportive evidence from mixed-indication cervical procedure cohorts or broader PD spine surgery series that included cervical procedures. This framework guided the narrative synthesis. Studies that did not explicitly define cervical myelopathy but included cervical procedures within broader PD spine surgery cohorts were considered indirect supportive evidence and were analyzed separately from myelopathy-defined studies.
Study Selection
After de-duplication, 2 reviewers independently screened titles/abstracts and subsequently assessed full texts for eligibility. Discrepancies were resolved by consensus, with third-reviewer adjudication when necessary. Reasons for exclusion at full-text review were recorded and are summarized in the PRISMA flow diagram (Figure 1). PRISMA 2020 flow diagram of study selection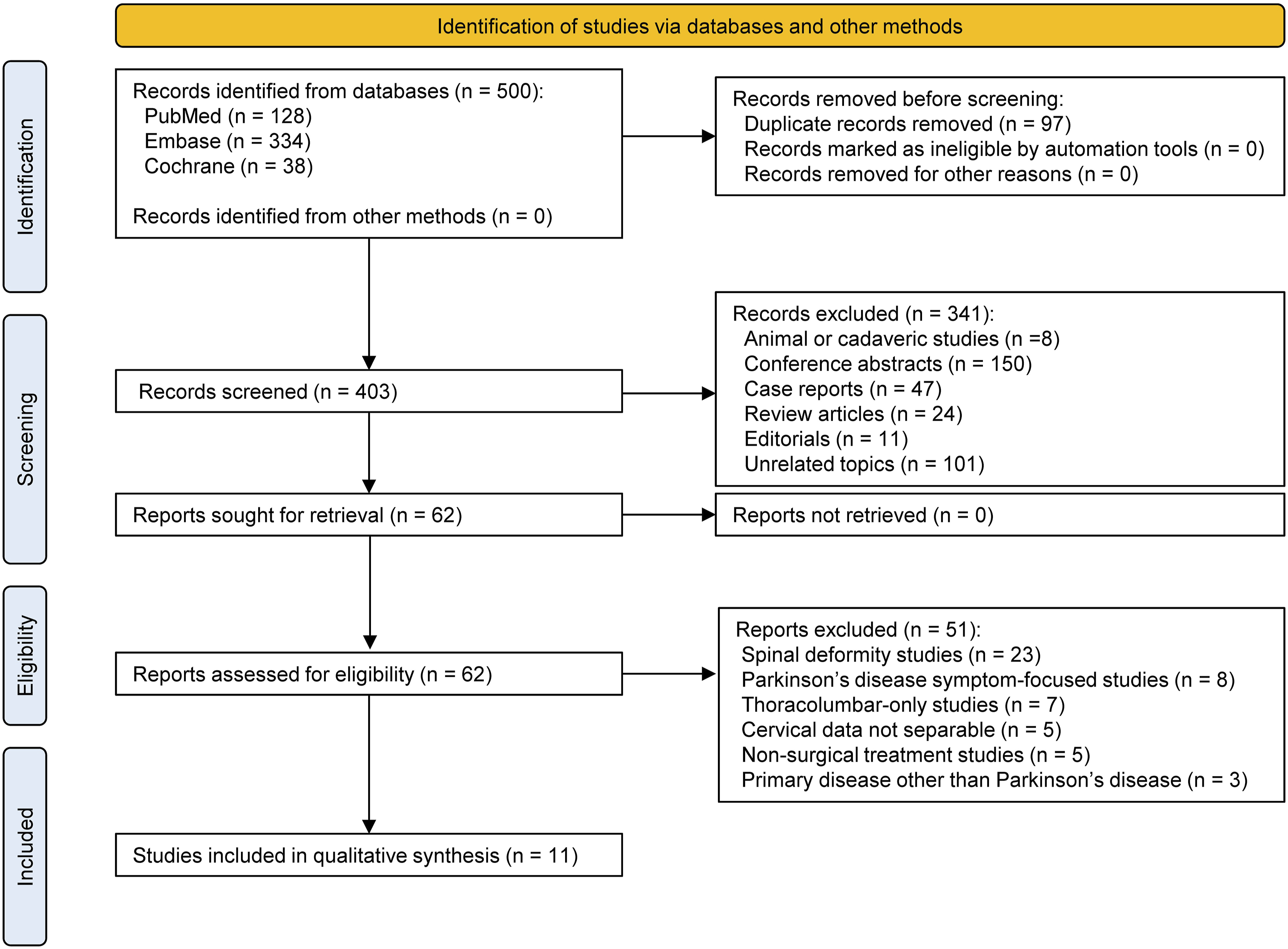
Data Extraction
Two reviewers independently extracted data from each included study using a standardized data-collection form. Extracted items included study design and data source; cohort definition and PD ascertainment; myelopathy definition; surgical approach/procedure category; follow-up duration; neurologic and functional outcomes (e.g., modified Japanese Orthopaedic Association [mJOA], Nurick); PROs (e.g., EQ-5D, Neck Disability Index [NDI], pain); perioperative complications (overall and system-specific); dysphagia/aspiration events; mortality; length of stay; discharge disposition; charges/costs; and reoperation/revision. When reported, we also extracted statistical adjustment methods (e.g., propensity matching, multivariable models). Disagreements in extraction were resolved by discussion and, when needed, adjudication by a third reviewer. We did not contact study authors for additional unpublished data.
When multiple timepoints were reported, we extracted the postoperative assessments as reported by the original study, with emphasis on clinically relevant early and late follow-up timepoints when available. When multiple analyses were presented for the same outcome, adjusted estimates were preferentially described over unadjusted comparisons. If key clinical details were unclear or not reported, they were recorded as not reported rather than imputed.
Critical Appraisal of Included Studies
Methodological appraisal of included studies was performed using the Joanna Briggs Institute (JBI) critical appraisal checklists for cohort studies and case series, as appropriate. 17 Two reviewers independently completed the appraisal, with disagreements resolved by consensus. Because the included evidence comprised heterogeneous observational designs and case series, JBI responses were summarized descriptively at the item level and were not converted into validated summary scores for study weighting or exclusion.
Effect Measures
For comparative studies, we extracted and reported effect estimates as presented by the original authors, including odds ratios, risk differences, beta coefficients, mean differences, and corresponding confidence intervals or P values when available. For non-comparative case series, we extracted descriptive event frequencies, proportions, and follow-up summaries. Because outcome definitions and reporting formats varied substantially across studies, no common effect measure was imposed across the full evidence base.
Synthesis Strategy
A quantitative meta-analysis was not performed because of substantial heterogeneity in cohort definitions (myelopathy-defined vs procedure-defined cohorts), outcome measures and follow-up timepoints, surgical strategies, and the possibility of overlapping patient capture across administrative databases. Accordingly, outcomes were synthesized narratively.
The narrative synthesis was prespecified to proceed in 2 steps. First, studies were grouped according to the prespecified myelopathy-specificity framework (tiers A to C) described above. Second, within each tier, findings were organized by outcome domain, including neurologic recovery, PROs/QoL, perioperative complications, dysphagia/aspiration-related events, length of stay/discharge disposition/costs, and revision or reoperation.
Because the included studies differed substantially in clinical directness to the primary review question, greater interpretive weight was assigned to myelopathy-defined evidence (tiers A and B). Tier C studies were used to contextualize patterns that were clinically relevant to PD patients undergoing cervical surgery, particularly perioperative morbidity and possible long-term construct-related failure, but were not used to override findings from myelopathy-defined cohorts. Emphasis was placed on the direction, consistency, and clinical relevance of findings rather than on vote counting alone.
Reporting Bias Assessment
We did not perform a formal assessment of reporting bias across syntheses, such as funnel plot analysis or small-study effect testing, because the evidence base was sparse, methodologically heterogeneous, and not amenable to quantitative meta-analysis.
Certainty Assessment
We did not perform a formal certainty-of-evidence assessment (e.g., GRADE). This decision was made because the included evidence consisted exclusively of heterogeneous observational studies and case series with substantial variation in directness, outcome definitions, and follow-up, such that outcome-level certainty judgments would have been difficult to apply consistently. Instead, certainty-related concerns were addressed qualitatively through the tiered evidence framework and item-level critical appraisal.
Results
Study Selection
The initial literature search identified 403 unique citations. After a preliminary screening of titles and abstracts, 341 records were excluded. Of the remaining 62 articles that underwent a comprehensive full-text review, 51 were excluded for failing to meet the eligibility criteria. Consequently, 11 studies were included in this review. The details of the screening and selection process are summarized in the PRISMA flow diagram (Figure 1).
Study Characteristics and Evidence Structure
Included Study Characteristics
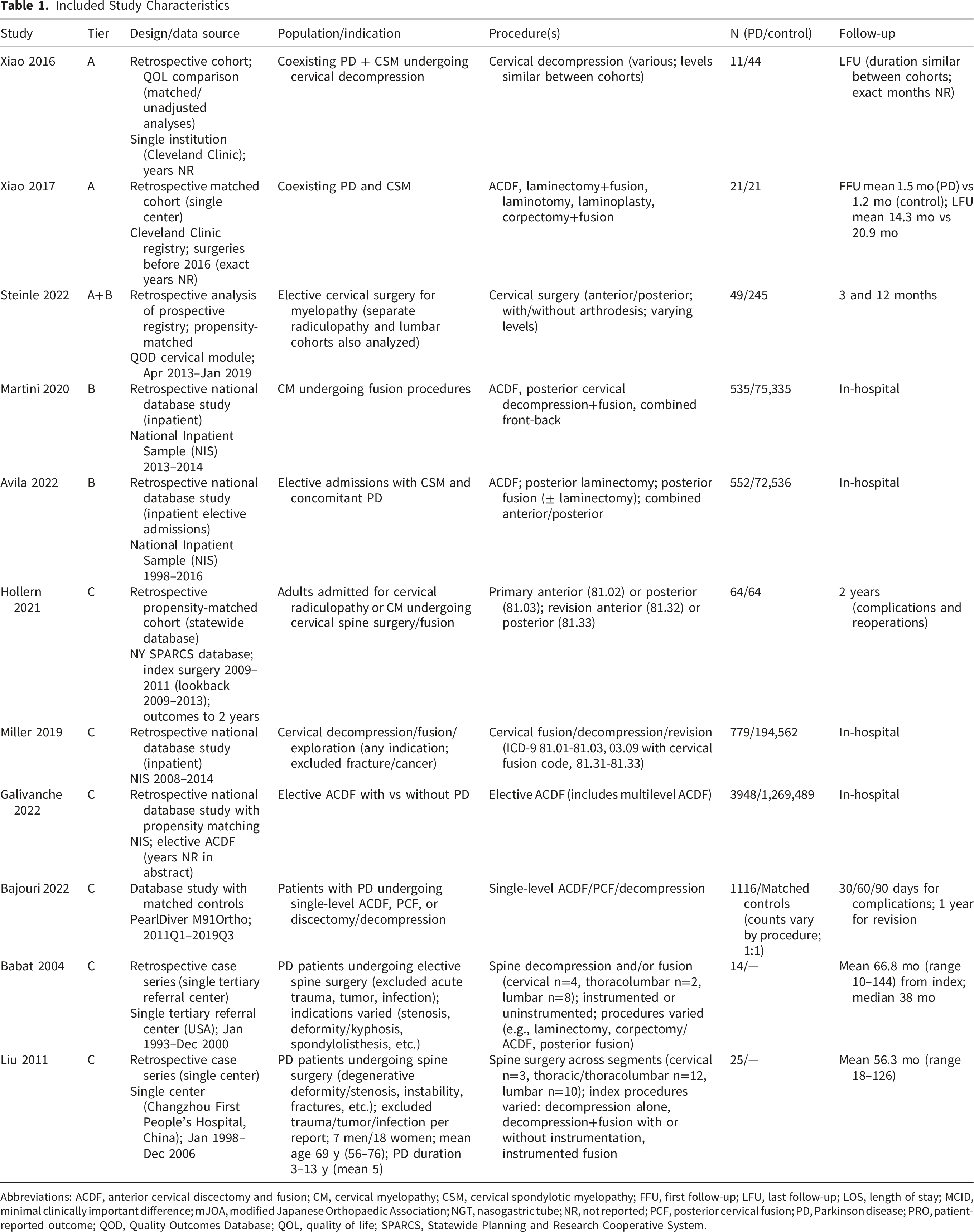
Abbreviations: ACDF, anterior cervical discectomy and fusion; CM, cervical myelopathy; CSM, cervical spondylotic myelopathy; FFU, first follow-up; LFU, last follow-up; LOS, length of stay; MCID, minimal clinically important difference; mJOA, modified Japanese Orthopaedic Association; NGT, nasogastric tube; NR, not reported; PCF, posterior cervical fusion; PD, Parkinson disease; PRO, patient-reported outcome; QOD, Quality Outcomes Database; QOL, quality of life; SPARCS, Statewide Planning and Research Cooperative System.
Summary of Key Extracted Findings by Outcome Domain
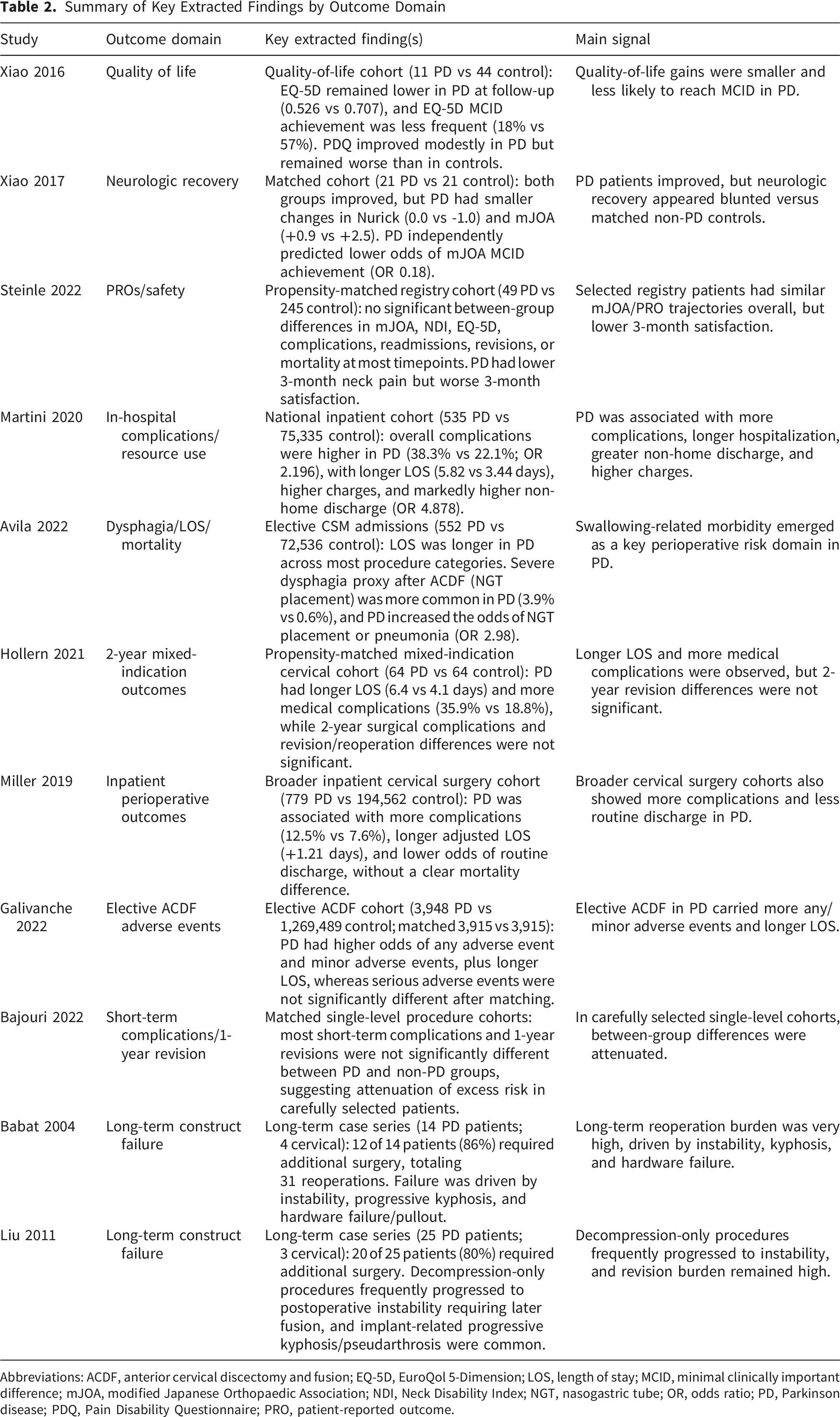
Abbreviations: ACDF, anterior cervical discectomy and fusion; EQ-5D, EuroQol 5-Dimension; LOS, length of stay; MCID, minimal clinically important difference; mJOA, modified Japanese Orthopaedic Association; NDI, Neck Disability Index; NGT, nasogastric tube; OR, odds ratio; PD, Parkinson disease; PDQ, Pain Disability Questionnaire; PRO, patient-reported outcome.
Within the myelopathy-specific evidence, 3 studies addressed neurologic recovery and/or PROs (tier A), while 3 reported perioperative safety and resource utilization (tier B), with 1 registry analysis contributing to both outcome domains. Supportive evidence (tier C) comprised 4 procedure-defined cervical cohorts with mixed indications and 2 case series focusing on long-term mechanical failure and revision patterns.
Methodological Appraisal
Joanna Briggs Institute (JBI) Critical Appraisal Results
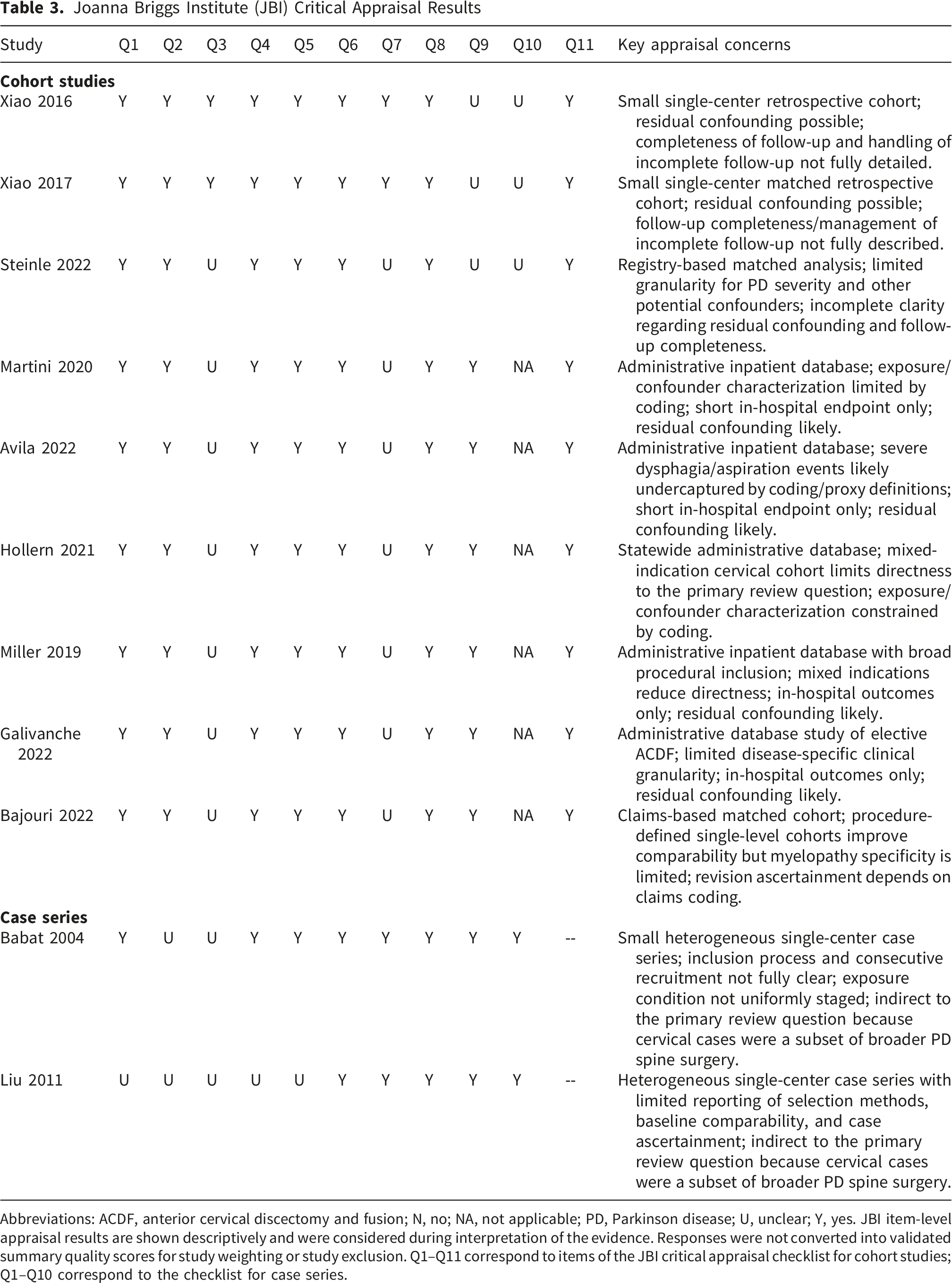
Abbreviations: ACDF, anterior cervical discectomy and fusion; N, no; NA, not applicable; PD, Parkinson disease; U, unclear; Y, yes. JBI item-level appraisal results are shown descriptively and were considered during interpretation of the evidence. Responses were not converted into validated summary quality scores for study weighting or study exclusion. Q1–Q11 correspond to items of the JBI critical appraisal checklist for cohort studies; Q1–Q10 correspond to the checklist for case series.
Myelopathy-specific Neurologic Recovery and Functional Outcomes
Two studies provided direct evidence regarding neurologic recovery after surgery for myelopathy-defined cohorts. In a single-center matched-cohort study of 21 PD patients with CSM and 21 non-PD CSM controls, Xiao and colleagues reported postoperative improvement in both groups but substantially smaller gains in the PD cohort. 18 The long-term follow-up change in Nurick grade was 0.0 in PD compared with -1.0 in controls, and the change in mJOA was +0.9 in PD compared with +2.5 in controls. In multivariable analysis, PD independently predicted less mJOA improvement (approximate β -0.89) and was associated with markedly lower odds of achieving the mJOA minimal clinically important difference (MCID; odds ratio [OR] 0.18). 18 Subscore patterns suggested relatively preserved improvement in upper-extremity and sphincter domains but limited improvement in lower-extremity motor performance. 18
In contrast, a registry-based analysis using the Quality Outcomes Database (QOD) identified a cervical myelopathy cohort in which 49 PD patients were propensity-matched 5:1 to 245 non-PD controls. In this matched myelopathy cohort, Steinle and colleagues found no significant between-group differences in mJOA at the reported timepoints. 19 Differences, when present, were more apparent in selected PROs, particularly lower 3-month neck pain and worse 3-month satisfaction in PD, whereas most other PROs were not significantly different. 19 Taken together, these findings suggest that PD may be associated with diminished neurologic recovery in some settings, although the magnitude and detectability of this effect may vary across cohorts and study design.18,19
Myelopathy-specific QoL and PROs
Two studies directly addressed PROs in myelopathy-defined cohorts. In a single-center cohort comparing 11 PD patients with CSM to 44 non-PD CSM controls, Xiao and colleagues reported that non-PD controls demonstrated significant improvements in QoL across measures, whereas PD patients showed minimal improvement. 20 At last follow-up, the EQ-5D index was lower in PD (0.526) than in controls (0.707; P = 0.01), and disability as measured by the Pain Disability Questionnaire (PDQ) remained worse in PD (PDQ total 80.7 vs 51.4; P = 0.03). Clinically meaningful improvement in EQ-5D was less frequent in PD, with MCID achievement of 18% compared with 57% in controls (P = 0.04), even though PDQ improved modestly within the PD cohort (89.9 to 80.7; P = 0.03). 20
In the QOD-matched cervical myelopathy cohort, Steinle and colleagues observed lower neck pain intensity at 3 months in PD (mean difference approximately -0.83 on a numeric rating scale (NRS); P = 0.005) but worse patient satisfaction at 3 months (risk difference approximately -0.262; P = 0.041). 19 At other reported timepoints, there were no significant differences between PD and non-PD patients in mJOA, NDI, EQ-5D, complications, readmissions, revisions, or mortality. Overall, the myelopathy-specific PRO literature suggests that PD patients can experience symptom and QoL improvement after surgery, but that they may be less likely to achieve clinically meaningful gains and may report lower satisfaction despite comparable scores on several standard instruments.19,20
Myelopathy-specific Perioperative Safety and Resource Utilization
Two large administrative database studies restricted to myelopathy-defined cohorts evaluated in-hospital outcomes. Using the National Inpatient Sample (NIS) and identifying cervical myelopathy patients undergoing fusion procedures, Martini and colleagues compared 535 PD patients with 75,335 non-PD patients. PD was associated with higher in-hospital complications (38.32% vs 22.05%; OR 2.196), markedly increased odds of non-home discharge (OR 4.878), longer length of stay (mean 5.822 vs 3.439 days), and higher hospital charges (mean $112,970 vs $87,408). 21 Procedure-stratified analyses suggested higher complication rates in PD after anterior cervical discectomy and fusion (ACDF) (29.09% vs 16.58%; OR 2.065), whereas differences across posterior or combined approaches were less consistent and, in some comparisons, not statistically significant. The study also reported increased odds of several systemic complications in PD, including thromboembolic and pulmonary events. 21
In an NIS study of elective admissions for cervical spondylotic myelopathy spanning 1998 to 2016, Avila and colleagues compared 552 PD patients with 72,536 non-PD patients and focused on dysphagia-related outcomes and aspiration risk. PD was associated with longer length of stay across several procedure categories, including ACDF (3.14 vs 2.04 days), laminectomy (4.25 vs 3.4 days), and posterior fusion (4.67 vs 3.65 days), with no difference in length of stay for combined anterior-posterior procedures. 22 Severe dysphagia as proxied by nasogastric tube placement after ACDF was more common in PD (3.9% vs 0.6%; P < 0.0001). PD was associated with increased odds of nasogastric tube placement or pneumonia (OR 2.98; 95% CI: 1.7-5.2). In-hospital mortality was also higher in PD in selected procedure subgroups, including ACDF (0.9% vs 0.2%; P = 0.011) and combined anterior-posterior procedures (6.1% vs 0.6%; P = 0.0001). Collectively, these myelopathy-specific database studies indicate that PD is associated with increased perioperative risk and substantially greater healthcare utilization, with dysphagia/aspiration-related complications emerging as a particularly prominent domain.21,22
Supportive Cervical Procedure Cohorts With Mixed Indications
Several studies evaluated broader cervical procedure cohorts that were not restricted to myelopathy-defined indications but provided context for perioperative risk and longer-term resource utilization in PD. In a propensity-matched cohort from the New York SPARCS database (64 PD vs 64 non-PD) including cervical surgery for radiculopathy and/or myelopathy, Hollern and colleagues found longer length of stay in PD (6.4 vs 4.1 days; P = 0.046) and higher medical complication rates (35.9% vs 18.8%; P = 0.029), while surgical complications and reoperation/revision rates over 2 years were not significantly different (15.6% vs 7.8% for revision; not significant). 23 In their multivariable models, PD was not a significant predictor of 2-year outcomes, whereas comorbidity burden predicted complications. 23
In other mixed-indication cohorts, Miller et al. reported higher in-hospital complications, longer adjusted stay, and lower odds of routine discharge after cervical decompression/fusion in PD. 24 Galivanche et al. found higher odds of any and minor adverse events and longer stay after elective ACDF, without a significant increase in serious adverse events after matching. 25 By contrast, a PearlDiver study of matched single-level procedures found no significant differences in most short-term complications or 1-year revisions. 26 Overall, mixed-indication cervical cohorts generally support longer hospitalization and more adverse events in PD, although differences may attenuate in carefully selected single-level populations.23-26
Supportive Evidence From PD Spine Surgery Case Series Including Cervical Procedures
Two long-term single-center case series provide indirect insight into mechanical failure, deformity, and reoperation in PD spine surgery, including cervical index cases. Babat et al. followed 14 PD patients for a mean of 66.8 months; 4 underwent cervical surgery. Twelve patients (86%) required additional surgery, totaling 31 reoperations, most often for instability at the operated or adjacent level, with hardware failure or pullout in 4 patients (29%). 10 Liu et al. followed 25 PD patients for 56.3 months, including 3 cervical cases, and reported 20 patients (80%) requiring 25 reoperations, driven by instability, progressive deformity, pseudarthrosis, and implant loosening or dislodgement. 27 Although these studies cannot quantify myelopathy-specific recovery, they highlight substantial long-term risk of mechanical failure and reoperation relevant to cervical surgical planning in PD.10,27
Discussion
This systematic review synthesized the available evidence on surgical outcomes for cervical myelopathy in patients with PD. The 11 included studies were heterogeneous: 5 directly evaluated myelopathy-defined cohorts, whereas 6 provided indirect supportive evidence from mixed-indication cervical cohorts or broader PD spine series including cervical procedures. Three themes emerged: First, PD patients may improve after surgery but recovery may be smaller or less clinically meaningful than in patients without PD.18,20 Second, perioperative risk and healthcare utilization appear higher, with dysphagia and aspiration-related events representing a particularly important complication domain.21,22 Third, long-term mechanical complications and reoperation appear common in PD spine surgery experience, suggesting the importance of durable alignment and fixation.10,27 Neurologic recovery, PROs, and perioperative risk were informed mainly by myelopathy-defined cohorts, whereas construct-related concerns were drawn primarily from indirect supportive evidence.
The most detailed neurologic-recovery Tier A cohort found smaller Nurick and mJOA improvements in PD than in controls, whereas the QOD cohort found no mJOA difference, underscoring heterogeneity.18,19 Locomotor outcomes require cautious interpretation because PD and DCM may both reduce walking speed through different mechanisms: PD gait is typically hypokinetic and cue-responsive, with reduced stride length and altered variability, whereas DCM gait more often reflects corticospinal and proprioceptive dysfunction with spastic or ataxic features.28-32 These mechanisms may mask or amplify one another, so postoperative gait change should be interpreted as recovery of cord-mediated components rather than global correction of mobility. This distinction may help explain inconsistent lower-extremity recovery and supports more granular gait assessment in future studies.18,19,28-32
Because most included studies lacked Hoehn and Yahr stage, Unified Parkinson’s Disease Rating Scale (UPDRS) or Movement Disorder Society-sponsored revision of the UPDRS (MDS-UPDRS) scores, and medication-state documentation, preoperative evaluation should explicitly address PD phenotype, disease duration, motor severity, medication schedule, levodopa response, cognition/non-motor burden, and myelopathy signs less attributable to PD.33,34 When gait attribution remains uncertain, neurology-supervised ON-medication assessment and, when clinically necessary, selective OFF-medication or levodopa-response assessment may help distinguish medication-responsive parkinsonian gait from cord-mediated myelopathic signs; routine OFF-medication testing is not recommended for every candidate.
PROs and QoL are important because PD can limit perceived benefit even when cord-related symptoms improve. Xiao et al. found less EQ-5D MCID achievement and persistent disability in PD, while the QOD cohort showed lower 3-month satisfaction despite broadly similar mJOA/PROs.19,20 This satisfaction gap may reflect PD non-motor symptoms, including mood, sleep, autonomic, cognitive, and swallowing burden, as well as expectation mismatch: decompression may improve hand function or selected myelopathic gait components but will not reverse bradykinesia, freezing, postural instability, or non-motor disability. Counseling should make this distinction explicit.35,36
Perioperative safety and resource utilization were addressed most consistently in Tier B database studies. PD was associated with higher complications, longer stay, higher charges, and greater non-home discharge; dysphagia/aspiration-related morbidity was prominent, including higher odds of nasogastric tube placement or pneumonia after cervical myelopathy surgery.21,22 Clinically, PD is not an absolute contraindication when DCM is clinically and radiographically concordant, but it should trigger a perioperative pathway emphasizing dopaminergic medication continuity, selective swallow-risk screening, speech-language pathology or diet modification when indicated, aspiration precautions, pulmonary optimization, and early discharge planning.21,22,37
Long-term case series provide additional perspective that is not captured in short-term administrative datasets. Both single-center series reported high reoperation rates related to progressive deformity, instability, pseudarthrosis, and implant-related complications, and both included cervical index cases.10,27 Although uncontrolled and heterogeneous, these studies suggest that PD-related factors such as neuromuscular imbalance, rigidity, postural instability, and impaired bone health may predispose patients to construct failure and progressive deformity. These signals support careful surgical planning in PD, with attention to alignment, fusion strategy, and longer postoperative surveillance than is typically required in non-PD populations.10,27
Limitations
Several limitations of the available evidence should be considered. Most included studies were retrospective and many relied on administrative coding without detailed information on PD severity (e.g., Hoehn and Yahr stage, UPDRS), medication response, frailty, bone health, or radiographic alignment.21-26 Outcome definitions and follow-up timepoints also varied substantially, particularly for complications and QoL measures, precluding quantitative pooling. In addition, several studies used large national databases with overlapping time periods, raising the possibility of partially overlapping patient capture; therefore, results were summarized study-by-study rather than aggregated. The literature on myelopathy-specific recovery also remains limited. The 2 single-center cohorts by Xiao and colleagues originated from the same institution and may overlap between the neurologic recovery and QoL cohorts.18,20 Finally, although we prespecified a structured narrative framework, inclusion of supportive mixed-indication cervical cohorts and broader PD spine surgery case series introduced variability in clinical directness to the primary review question. We also did not perform formal reporting-bias or certainty-of-evidence assessments.
Future Directions
Prospective cohorts of patients with PD and DCM should report PD phenotype and severity (Hoehn and Yahr stage, UPDRS/MDS-UPDRS, medication state), DCM severity, radiographic alignment, validated neurologic/PRO measures with MCID reporting, and longer-term follow-up. They should also incorporate quantitative gait metrics, somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), central motor conduction, and advanced spinal cord magnetic resonance imaging (MRI), including diffusion or quantitative techniques.31-34,38-40 These data would clarify which deficits are cord-mediated, medication-responsive, or related to fixed neurodegenerative disability, and would better define durability of neurologic recovery and construct-related failure.
Conclusion
In conclusion, the most direct available evidence suggests that PD is associated with higher perioperative risk and greater healthcare utilization after surgery for cervical myelopathy.18-22 Myelopathy-defined cohorts also suggest that functional recovery may be smaller or less clinically meaningful in some PD patients, although these findings remain heterogeneous.18-20 Evidence for long-term mechanical failure and reoperation is indirect and comes largely from supportive studies that included cervical cases within broader PD spine surgery populations.10,27 These findings support multidisciplinary decision-making: surgery may be considered for clinically and radiographically concordant DCM in PD, but counseling and perioperative planning should address limited recovery, persistent parkinsonian/non-motor disability, medication continuity, dysphagia/aspiration risk, discharge needs, and longer surveillance for construct-related failure.
Supplemental Material
Supplemental Material - Surgical Outcomes of Degenerative Cervical Myelopathy in Patients with Parkinson Disease: A Systematic Review
Supplemental Material for Surgical Outcomes of Degenerative Cervical Myelopathy in Patients with Parkinson Disease: A Systematic Review by Shota Takenaka, MD, DMSc, Hiroyuki Ishiguro, MD, PhD, Toshitaka Yoshii, MD, PhD, Kentaro Yamada, MD, PhD, Eiji Takasawa, MD, PhD, Satoshi Nori, MD, PhD, So Kato, MD, PhD, Kazuya Kitamura, MD, PhD, Takeo Furuya, MD, PhD, Hiroaki Nakashima, MD, PhD, Norimitsu Wakao, MD, PhD, Kazuyoshi Nakanishi, MD, PhD, Yasushi Fujiwara, MD, PhD, Masahiro Yoshida, MD, PhD, Masahiko Watanabe, MD, PhD, Hirotaka Chikuda, MD, PhD in Global Spine Journal
Supplemental Material
Supplemental Material - Surgical Outcomes of Degenerative Cervical Myelopathy in Patients with Parkinson Disease: A Systematic Review
Supplemental Material for Surgical Outcomes of Degenerative Cervical Myelopathy in Patients with Parkinson Disease: A Systematic Review by Shota Takenaka, MD, DMSc, Hiroyuki Ishiguro, MD, PhD, Toshitaka Yoshii, MD, PhD, Kentaro Yamada, MD, PhD, Eiji Takasawa, MD, PhD, Satoshi Nori, MD, PhD, So Kato, MD, PhD, Kazuya Kitamura, MD, PhD, Takeo Furuya, MD, PhD, Hiroaki Nakashima, MD, PhD, Norimitsu Wakao, MD, PhD, Kazuyoshi Nakanishi, MD, PhD, Yasushi Fujiwara, MD, PhD, Masahiro Yoshida, MD, PhD, Masahiko Watanabe, MD, PhD, Hirotaka Chikuda, MD, PhD in Global Spine Journal
Footnotes
Acknowledgments
The authors thank Chris Rowthorn Japan Co., Ltd. (Chris Rowthorn) for providing English language editing.
Ethical Considerations
This study was a systematic review of previously published literature and did not involve any direct interaction with human participants or access to identifiable personal data. Therefore, ethical approval and informed consent were not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: So Kato received research funding from Osferion Biomaterial. All other authors declare no conflicts of interest.
Data Availability Statement
The data supporting the findings of this study are available within the article and its supplementary materials. Further details regarding the extracted data are available from the corresponding author upon reasonable request.
Anonymized information for Peer Review
The protocol for this systematic review was prospectively registered in the Open Science Framework (OSF). To maintain double-blind peer review, the registration details and URL are temporarily anonymized in the manuscript. The full citation and link will be restored after peer review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.