
Abstract
Study Design
Retrospective Study.
Objective
To identify clinical risk factors for symptomatic epidural hematoma (SEH) following posterior lumbar decompression and fusion, with a particular focus on paraspinal muscle parameters.
Methods
We retrospectively analyzed data from 105 patients who underwent transforaminal lumbar interbody fusion (TLIF) between January 2016 and January 2025, including 21 patients in the SEH group and 84 in the normal group. General information, surgical-related parameters, routine laboratory parameters, preoperative coagulation-related parameters, spinal imaging-related parameters, and muscle-related parameters were collected. Univariate analysis and binary multivariate logistic regression were performed to identify independent risk factors for SEH.
Results
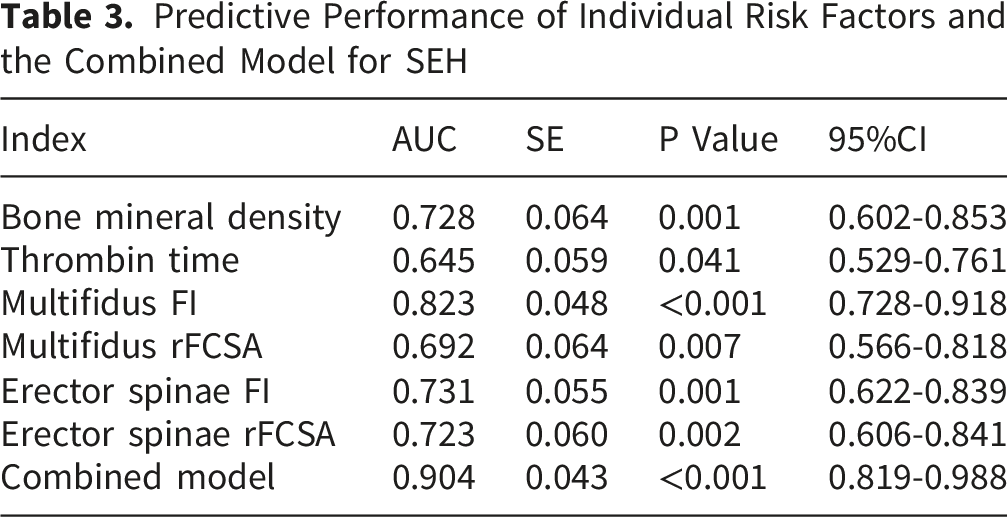
Multivariate logistic regression identified prolonged thrombin time (OR = 1.780, P = 0.043) and increased multifidus fatty infiltration (FI) (OR = 1.116, P = 0.012) as independent risk factors for SEH following TLIF. Higher bone mineral density (BMD) was a protective factor (OR = 0.527, P = 0.023). No other variables showed significant associations in the regression model.
Conclusion
Preoperative evaluation of coagulation status, BMD, and paraspinal muscle quality—particularly multifidus FI, is clinically important for predicting and preventing SEH following lumbar spine surgery.
Keywords
1. Introduction
Symptomatic epidural hematoma (SEH) is one of the most serious complications that may occur after lumbar spine surgery. The clinical manifestations of spinal SEH were first described by Jackson R in 1869. 1 Studies have shown that among patients undergoing lumbar decompression surgery, 33–100% develop asymptomatic epidural hematoma postoperatively, whereas the incidence of SEH ranges from 0.1% to 0.24%. 2 Furthermore, the incidence of postoperative hematoma is higher in posterior spinal procedures than in anterior approaches. 3 Although SEH is relatively rare, once it occurs after lumbar decompression, it may cause progressive and potentially permanent neurological deficits by compressing the cauda equina and nerve roots, manifesting as sensory impairment, pain, and decreased muscle strength. 4 Once SEH is diagnosed, prompt surgical evacuation should be performed. Decompression within 6 hours is associated with improved neurological recovery, 5 delayed evacuation beyond 24 hours may result in poor outcomes. 6 Given the potentially serious consequences of SEH, it is particularly important to investigate the risk factors and preventive strategies for postoperative SEH following lumbar spine surgery. Previous studies have indicated that advanced age, obesity, hypertension, hypocalcemia, coagulation dysfunction, a lumbar lordosis angle of less than 25°, multilevel surgery, increased intraoperative blood loss, prolonged operative time, the use of gelatin sponge during surgery, and poor postoperative drainage may increase the risk of SEH after lumbar procedures.2,4,7-9 However, due to variations in evaluation criteria and inconsistent findings across studies, the current understanding of postoperative SEH following lumbar spine surgery remains limited and requires further investigation.
Paraspinal muscles play a critical role in the development of spine-related disorders, and alterations in their structure and function appear to have a direct impact on spinal health. 10 Parameters of the paraspinal muscles, such as cross-sectional area (CSA) and fatty infiltration (FI), are closely associated with the presence and severity of low back pain. 11 Atrophy of the multifidus muscle and increased FI have been implicated in the progression of lumbar disc degeneration.12,13 In patients with chronic low back pain, the multifidus muscle exhibits a reduced CSA and an increased degree of FI. 14 The condition of the paraspinal muscles also plays a significant role in lumbar spine surgery. Some studies have suggested that degeneration of these muscles is associated with distal pedicle screw loosening following corrective surgery for degenerative lumbar scoliosis. 15 A reduction in the functional cross-sectional area (FCSA) of the paraspinal muscles, along with increased FI, has been associated with the development of proximal junctional kyphosis. 16 Due to the surgical approach and prolonged retraction inherent to posterior decompression procedures, paraspinal muscles inevitably sustain injury, with the multifidus muscle typically being more severely affected than other paraspinal muscles. 17 Moreover, sarcopenia diagnosed based on the psoas muscle index has been found to be associated with adverse outcomes following complex thoracolumbar revision surgery. 18 Although previous studies have demonstrated a relationship between paraspinal muscle condition and adverse outcomes after lumbar spine surgery, research specifically examining the association between paraspinal muscles and postoperative SEH is still lacking. This study incorporated relevant factors, including the psoas and paraspinal muscles, with the aim of identifying risk factors for SEH following posterior lumbar decompression and fusion.
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
Inclusion Criteria (1) To minimize the potential confounding effect of surgical technique, only patients who underwent transforaminal lumbar interbody fusion (TLIF) were included. The study population comprised patients with degenerative lumbar conditions, including lumbar disc herniation and lumbar spinal stenosis, who underwent TLIF at our institution. (2) Had no evidence of epidural hematoma on preoperative imaging. (3) Had routine placement of a surgical drain during the procedure, which was removed when postoperative drainage was less than 50 mL within 24 hours. (4) Completed all examinations at our hospital, with comprehensive and accessible medical records. (5) Provided informed consent and voluntarily agreed to undergo surgery.
Exclusion Criteria (1) Surgery involved thoracic spinal segments. (2) Presence of other spinal disorders, including ankylosing spondylitis, spinal infection, or spinal tumors. (3) Development of other postoperative complications. (4) History of previous spinal surgery.
2.2. General Information
Based on the above criteria, a total of 21 patients who underwent TLIF at our institution between January 2016 and January 2025 were included in the SEH group. These patients required surgical evacuation due to the development of SEH within 72 hours postoperatively. Hospitalization records of all patients who underwent TLIF at our institution during the same period and did not develop SEH were extracted and reassigned identification numbers. Using a random number table, 84 patients were then selected at a 1:4 ratio to serve as the normal group. All surgeries were performed by surgeons with comparable experience and expertise, following the same standardized operative protocol. This study was approved by the Ethics Committee, and written informed consent was obtained from all participants.
2.3. Surgical Procedure
After induction of general anesthesia, patients were positioned prone, and the surgical area was prepared and draped in a sterile manner. A posterolateral incision was made on the affected side, and the skin and subcutaneous tissues were incised layer by layer down to the deep fascia. The paraspinal muscles on the affected side were carefully dissected to expose the facet joints, where pedicle screws were inserted. The inferior articular process and a portion of the lamina on the affected side were removed to expose the intervertebral foramen, and the nerve root was gently retracted to achieve decompression until the dural sac and nerve root were free from compression. The nucleus pulposus was then excised, and autologous or allogeneic bone grafts were implanted. An appropriately sized interbody fusion cage was inserted, followed by placement of titanium rods connecting the bilateral pedicle screws. After securing the top set screws, the surgical site was thoroughly irrigated, a drain was placed, and the incision was closed in layers.
2.4. Outcome Measures
In this study, the diagnostic criteria for SEH were as follows: (1) Development of neurological deficits or persistent pain within 72 hours postoperatively; (2) Postoperative MRI axial images showing a dural sac area of less than 75 mm 19 . The need for hematoma evacuation following the initial surgery was identified in accordance with the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), using the code G97.51.
General information included sex, age, body mass index (BMI), and bone mineral density (BMD), as well as blood pressure at admission, history of hypertension, and postoperative use of anticoagulants. Bone mineral density was assessed using T-scores obtained by dual-energy X-ray absorptiometry.
Surgical-related parameters included the surgical segments, surgical duration, and intraoperative blood loss.
Routine laboratory parameters included red blood cell count, hemoglobin, white blood cell count, sodium, calcium, potassium, erythrocyte sedimentation rate, C-reactive protein, alanine aminotransferase, aspartate aminotransferase, the aspartate/alanine aminotransferase ratio, albumin, globulin, and the albumin/globulin ratio.
Preoperative coagulation-related parameters included D-dimer, international normalized ratio, prothrombin time, prothrombin activity, activated partial thromboplastin time, plasma fibrinogen levels, thrombin time (TT), and platelet count.
Spinal imaging-related parameters included lumbar lordosis angle, preoperative segmental lordosis angle and postoperative segmental lordosis angle at the surgical level, and the degree of correction of segmental lordosis angle.
Muscle-related parameters included the CSA of the vertebral body, psoas major, multifidus, and erector spinae muscles. In addition, the relative cross-sectional area (rCSA) of the psoas major, multifidus, and erector spinae, as well as the FCSA, relative functional cross-sectional area (rFCSA), and FI of the multifidus and erector spinae were evaluated. The delineation of each region is illustrated in Figure 1. By calculating the rCSA, the influence of individual factors such as height and body weight on muscle CSA can be effectively minimized.
20
The rCSA was defined as the ratio of muscle CSA to vertebral body CSA, whereas the FCSA represented the CSA of lean muscle tissue after excluding fat CSA.
16
The rFCSA was defined as the ratio of muscle FCSA to vertebral body CSA, while FI was calculated as the percentage of fat tissue CSA relative to the total muscle CSA.
21
Magnetic resonance imaging (MRI) has increasingly gained popularity in recent years as a noninvasive modality for evaluating the structural characteristics and composition of paraspinal muscle tissue.
22
Therefore, MRI was used in this study to quantify the CSA and FI of the paraspinal muscles. Previous studies have shown that the paraspinal muscle CSA reaches its maximum at the L3–L4 level, accordingly, axial MRI images at the superior endplate of L4 were selected for CSA measurements.
23
All muscle-related parameters were measured using ImageJ software (National Institutes of Health, USA). Measurements were performed using T2-weighted MRI. In accordance with methodologies described in previous studies, a fixed grayscale thresholding technique was employed to extract lean muscle characteristics.
24
Based on standardized MRI scanning parameters, distinct muscular and vertebral tissues were delineated into separate regions of interest. By normalizing the grayscale distribution curves of each tissue, a universally applicable grayscale threshold interval for lean muscle was established. This boundary was defined by the critical intersection point between the descending curve of muscle pixels and the ascending curve of adipose pixels. In the current study, the critical threshold differentiating lean muscle from adipose tissue was ultimately set at 80. When measuring the area metrics for the multifidus, erector spinae, and psoas major, the bilateral muscle areas on both sides of the vertebra were summed in this study. To ensure consistency of the measurement standards, axial MRI images at the level of the L4 superior endplate were uniformly selected for patients undergoing multi-segment surgery, with the measured paraspinal muscle parameters serving as representative indicators of the patient’s overall paraspinal muscle status. All measurements were independently performed by three experienced physicians who were blinded to the clinical data. Each parameter was measured twice by each observer, and the mean value was used for statistical analysis. The intraobserver and interobserver reliabilities for the measurements were assessed using the intraclass correlation coefficient (ICC). The results demonstrated excellent reliability, with an intraobserver ICC of 0.91 and an interobserver ICC of 0.84. In this study, rCSA, FI, and rFCSA were all expressed as percentages. Anatomy of the vertebral body and paraspinal muscles. A: vertebral body; B: multifidus; C: erector spinae; D: psoas major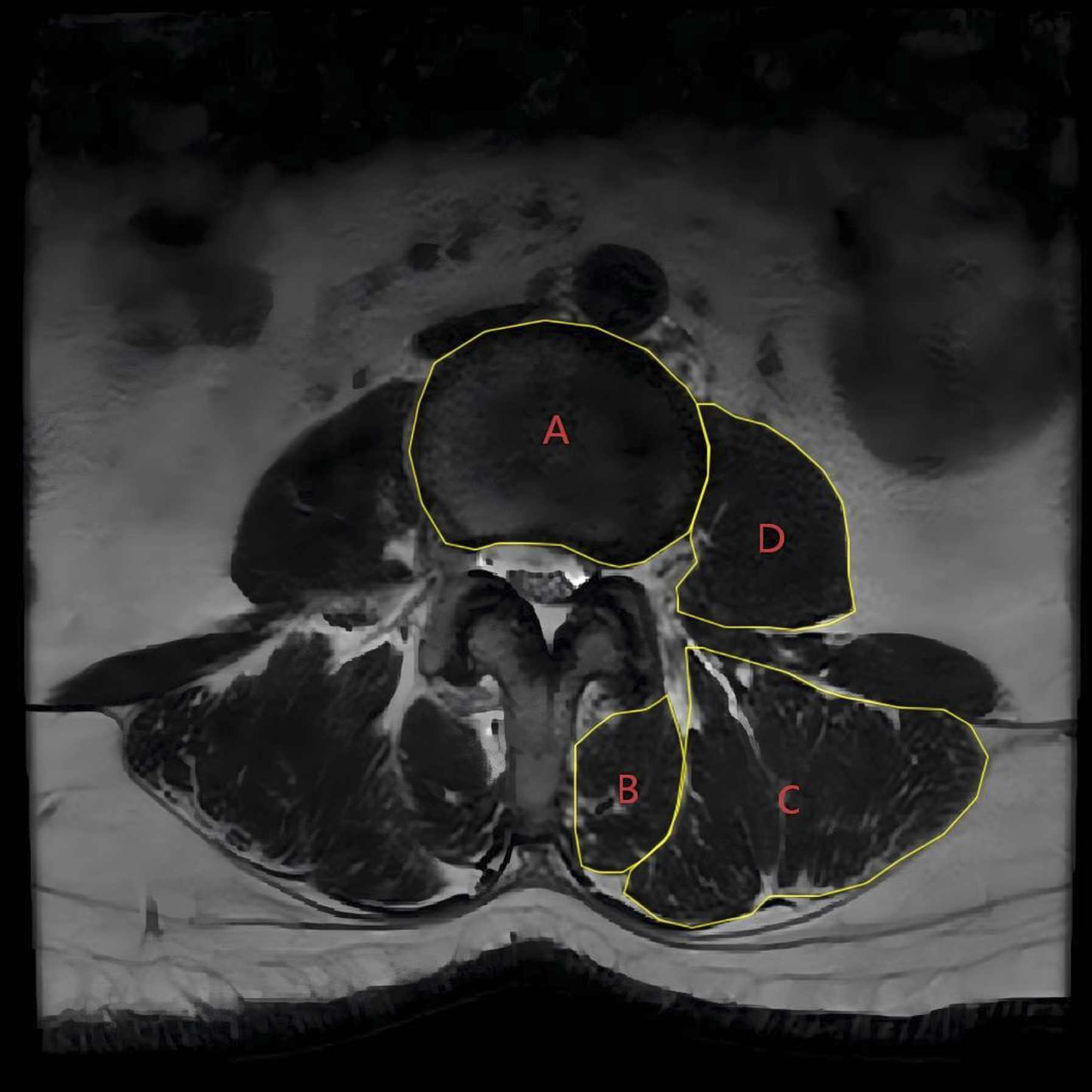
2.5. Statistical Analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables were first assessed for normality using the Shapiro–Wilk test. Variables with a normal distribution were expressed as the mean ± standard deviation (mean ± SD), whereas non-normally distributed variables were presented as the median (interquartile range, IQR). Homogeneity of variance was evaluated using Levene’s test.
For continuous variables satisfying both normality and homogeneity of variance, intergroup comparisons were conducted using the independent-samples t-test. Non-normally distributed variables or those failing the homogeneity assumption were analyzed with the Mann–Whitney U test. Categorical variables were compared using the chi-square (χ2) test or Fisher’s exact test when expected cell counts were less than 5. Ordinal data were analyzed with the Mann–Whitney U test.
Binary multivariate logistic regression analysis was performed to identify predictors of SEH, with the occurrence of SEH as the dependent variable. Variables with P < 0.05 in the univariate analysis were included in the multivariate model. A two-tailed P value < 0.05 was considered statistically significant.
3. Results
3.1. Clinical Outcomes
A representative case of SEH following TLIF is shown in Figure 2. Among the 21 patients with SEH, neurological recovery was evaluated at 12 months after reoperation using the Frankel grading system (grades A–E). Eleven patients recovered to grade E, eight to grade D, and two to grade C. The two patients classified as grade C had concomitant sphincter dysfunction, whereas no sphincter dysfunction was observed in the remaining patients. Representative MRI of postoperative hematoma following TLIF. A 43-year-old female underwent L5/S1 TLIF for lumbar disc herniation and developed right lower limb weakness 12 hours postoperatively. MRI revealed abnormal signal in the right posterolateral recess of the L5/S1 disc and the upper portion of the S1 vertebral body, with associated spinal canal stenosis. Panels A, B, and C show MRI images at different axial levels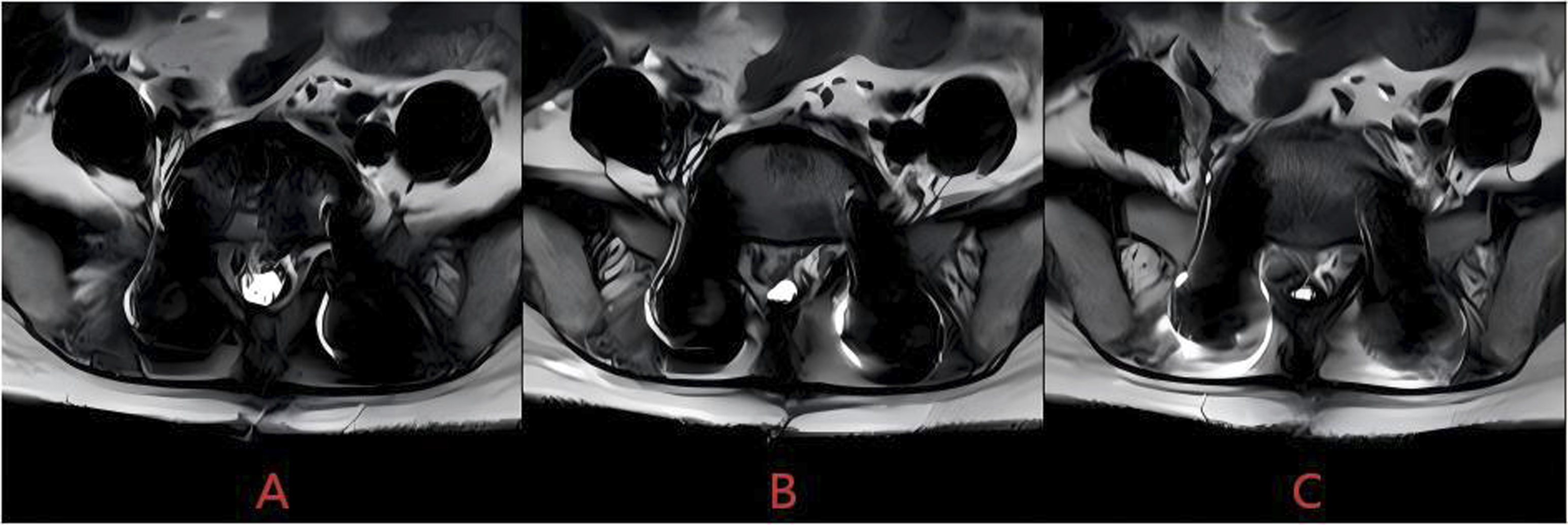
3.2. Univariate Analysis Results
Univariate Comparison Between Patients With and Without SEH
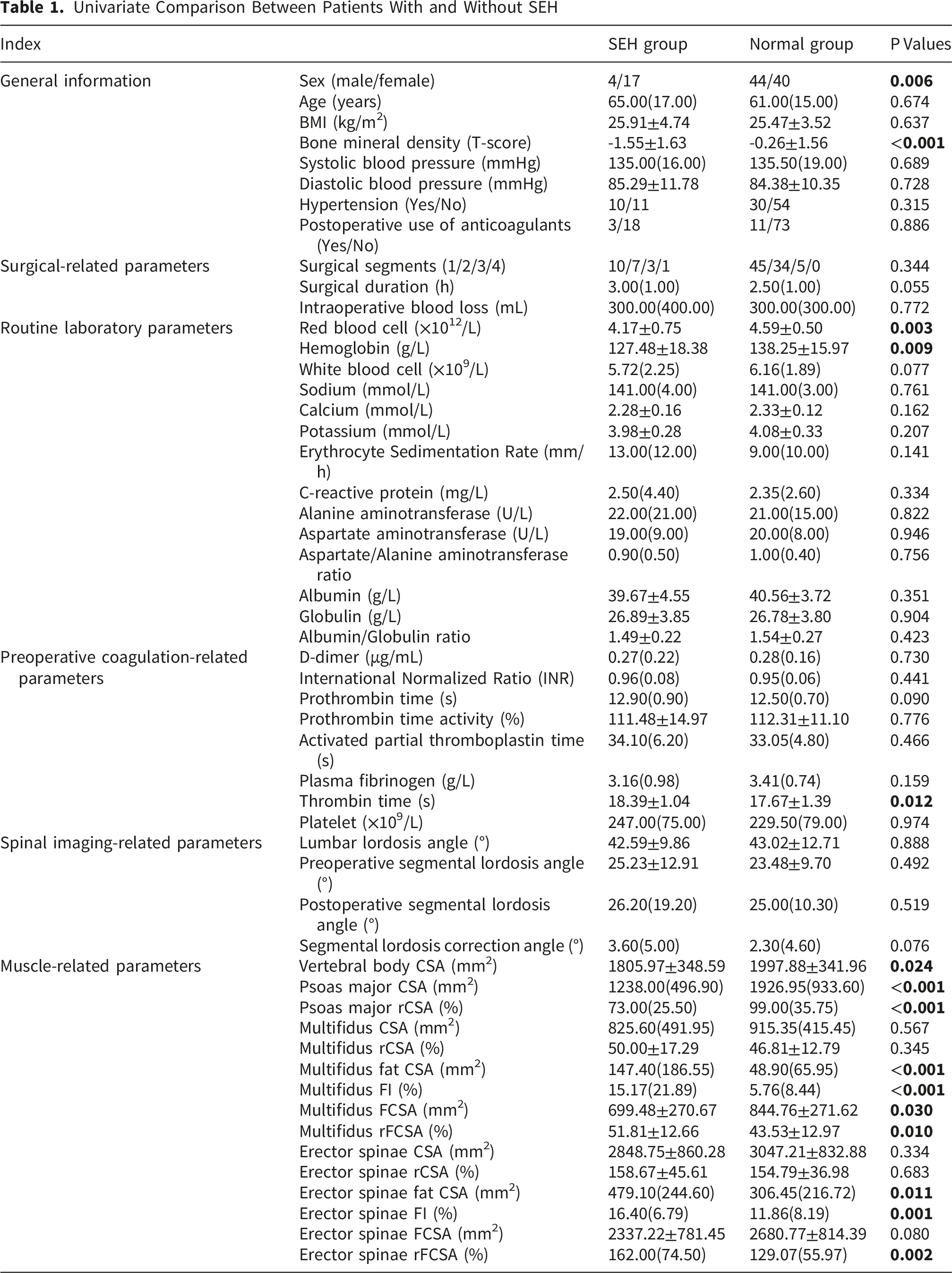
Regarding general information, significant differences were observed between the two groups in sex (P = 0.006) and BMD (P < 0.001). The proportion of female patients was higher in the SEH group, and the T-scores were lower compared with the normal group. No significant differences were found in other general information (P > 0.05).
For surgical information, surgical duration, surgical segments, and intraoperative blood loss showed no statistically significant differences between the groups (P > 0.05).
Among routine laboratory parameters, RBC (P = 0.003) and Hb level (P = 0.009) were significantly lower in the SEH group than in the normal group, while no significant differences were observed in the remaining indices.
For preoperative coagulation-related parameters, TT was significantly different between the two groups (P = 0.012), with a longer TT observed in the SEH group; no other coagulation indices showed statistical significance (P > 0.05).
No significant differences were identified in the spinal imaging-related parameters included in this study (P > 0.05).
Regarding muscle-related parameters, significant intergroup differences were observed in vertebral body CSA (P = 0.024), psoas major CSA (P < 0.001), psoas major rCSA (P < 0.001), multifidus fat CSA (P < 0.001), multifidus FI (P < 0.001), multifidus FCSA (P = 0.03), multifidus rFCSA (P = 0.010), erector spinae fat CSA (P = 0.011), erector spinae FI (P = 0.001), and erector spinae rFCSA (P = 0.002). Specifically, vertebral body CSA, psoas major CSA, psoas major rCSA, and multifidus FCSA were significantly lower in the SEH group, whereas multifidus fat CSA, multifidus FI, multifidus rFCSA, erector spinae fat CSA, erector spinae FI, and erector spinae rFCSA were significantly higher compared with the normal group. No significant differences were observed in the remaining muscle-related parameters (P > 0.05).
3.3. Multivariate Logistic Regression Analysis Results
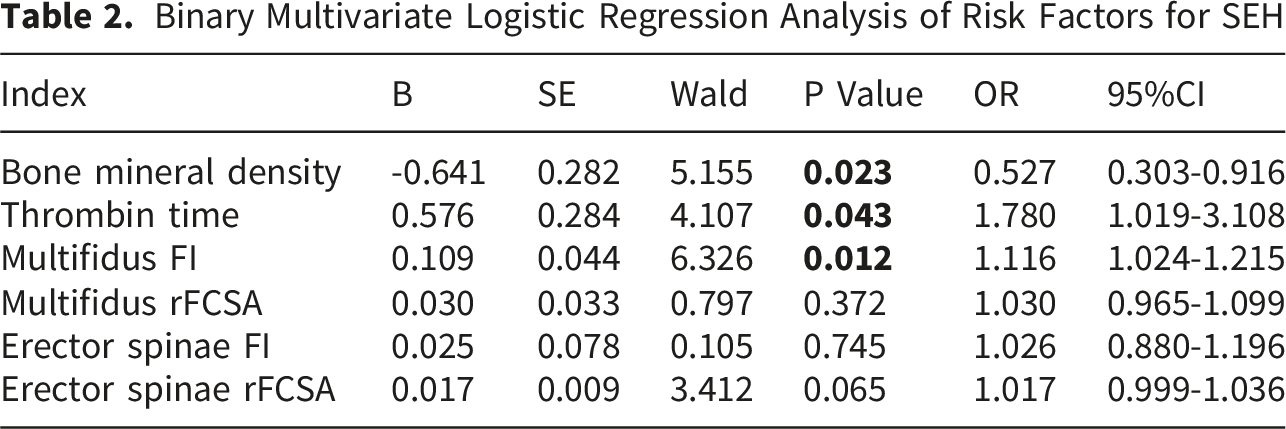
Binary multivariate logistic regression analysis was performed using variables that were statistically significant in the univariate analysis. Prior to the regression analysis, multicollinearity diagnostics were conducted for variables that showed significant differences between the two groups. In general, a variance inflation factor (VIF) greater than 5 was considered indicative of a high likelihood of multicollinearity in the model. 25 The results indicated potential multicollinearity among vertebral body CSA (VIF = 17.028), psoas major CSA (VIF = 67.667), psoas major rCSA (VIF = 51.597), multifidus fat CSA (VIF = 18.816), multifidus FI (VIF = 21.569), multifidus FCSA (VIF = 12.853), multifidus rFCSA (VIF = 12.465), erector spinae fat CSA (VIF = 17.230), erector spinae FI (VIF = 22.901), and erector spinae rFCSA (VIF = 7.506). The remaining variables showed tolerance values greater than 0.1 and VIF values less than 5, indicating no significant multicollinearity. Considering that psoas major rCSA, multifidus FI, multifidus rFCSA, erector spinae FI, and erector spinae rFCSA better account for inter-individual variability, vertebral body CSA, psoas major CSA, multifidus fat CSA, multifidus FCSA, and erector spinae fat CSA were excluded, and multicollinearity diagnostics were repeated. The repeated diagnostic analysis showed that all variables had tolerance values greater than 0.1 and VIF values less than 5, indicating the absence of multicollinearity among the included variables.
Binary Multivariate Logistic Regression Analysis of Risk Factors for SEH
Predictive Performance of Individual Risk Factors and the Combined Model for SEH
4. Discussion
Studies have reported that following the occurrence of SEH after lumbar spine surgery, approximately 81.6% of patients require reoperation. 4 This undoubtedly increases patient suffering and may result in serious sequelae; therefore, a thorough preoperative evaluation is essential to identify and mitigate potential risk factors for SEH.
In this study, significant differences in sex and BMD were observed between the two groups in the univariate analysis. However, in the multivariate logistic regression analysis, only BMD remained significantly associated with the occurrence of SEH following TLIF (P < 0.05), whereas sex was not significantly associated (P > 0.05). Previous studies have reported inconsistent findings regarding the association between sex and postoperative SEH. Some studies suggest that sex is not related to the incidence of SEH following spinal surgery, 3 whereas others indicate that female sex may be a risk factor for SEH in certain types of spinal procedures. 26 In this study, no significant difference in age was observed between the two groups. However, some studies have identified advanced age as a risk factor for SEH, 4 whereas others have reported no association between age and the occurrence of SEH. 2 Additionally, Yamada K et al reported that a high BMI may be a risk factor for SEH following spinal surgery. 27 Poor bone quality has been associated with an increased risk of postoperative complications following spinal surgery, including cage subsidence and pedicle screw loosening after TLIF.19,28 Studies have reported that nearly half of patients undergoing TLIF have undiagnosed osteopenia or osteoporosis. 29 In patients undergoing spinal procedures, osteoporosis plays a critical role in preoperative evaluation, perioperative management, and postoperative outcomes. 30 In this study, higher BMD was identified as a significant protective factor against postoperative SEH (OR = 0.527, P = 0.023), further highlighting the importance of preoperative assessment of bone quality.
Although none of the three surgical related parameters included in this study reached statistical significance, previous studies have suggested that prolonged surgical duration, multilevel surgical segments, and increased intraoperative blood loss may be risk factors for SEH following lumbar decompression surgery.4,7,8 Therefore, during surgery, surgeons should aim to minimize operative time and ensure meticulous hemostasis, and patients scheduled for multilevel procedures should undergo comprehensive preoperative evaluation. Although preoperative blood pressure and a history of hypertension were not statistically significant in this study, previous research has suggested that hypertension at admission may be a risk factor for SEH following lumbar decompression surgery. 31 Furthermore, no significant differences were observed between the two groups in postoperative anticoagulant use, which is consistent with the findings of Crawford AM et al. 32 However, it is noteworthy that some researchers have found an association between the use of anticoagulants and antiplatelet agents and the development of chronic SEH. 33 Therefore, the potential correlation between anticoagulants and postoperative SEH also warrants attention.
Among the general laboratory parameters included in this study, only RBC and Hb showed significant differences between groups (P < 0.05). Previous studies have suggested that in adult patients undergoing spinal surgery, preoperative Hb and hematocrit are important clinical indicators for predicting postoperative outcomes. Reduced Hb and hematocrit levels have been associated with an increased risk of cardiac events, higher transfusion requirements, and prolonged hospital stay following posterior lumbar fusion. 34 Although RBC and Hb were not included in the binary logistic regression model due to concerns regarding model stability in this study, preoperative levels of Hb and related parameters should still be considered key reference indicators for preoperative risk assessment and patient optimization in spinal surgery.
Among the coagulation-related parameters included in this study, the analysis indicated that prolonged TT was a risk factor for SEH (OR = 1.78, P = 0.043), which is consistent with previous research. 35 Prolonged TT typically reflects potential coagulation dysfunction, and abnormal coagulation has long been recognized as one of the risk factors for SEH following lumbar spine surgery.9,36 Notably, although no other coagulation parameters besides TT reached statistical significance in this study, previous research has suggested that other coagulation indices, such as the international normalized ratio, may also be associated with the occurrence of SEH following lumbar spine surgery. 4 In summary, during preoperative evaluation, clinicians should comprehensively assess all relevant coagulation parameters to ensure a thorough understanding of the patient’s coagulation status.
Currently, research on the relationship between spinal imaging parameters and postoperative SEH remains limited. Fujita N et al reported that a lumbar lordosis angle of less than 25° is a risk factor for SEH following posterior decompression surgery for lumbar spinal stenosis. 8 Wang LJ et al reported that an increased thoracic kyphosis angle is a risk factor for SEH following posterior decompression surgery of the thoracic spine. 37 In this study, none of the included imaging parameters reached statistical significance. Given the limited and inconsistent findings in the current literature, further research is warranted to clarify the impact of spinal imaging parameters on the occurrence of SEH following spinal surgery.
Imaging parameters of the paraspinal muscles, such as muscle CSA and FI, serve as important indicators for assessing paraspinal muscle atrophy, with MRI providing superior accuracy over CT for measuring FI. 38 An increase in paraspinal muscle FI often reflects degenerative atrophy and is closely associated with spinal disorders. Studies have shown that symptomatic spinal stenosis leads to more severe paraspinal muscle atrophy compared with isolated low back pain. 39 In patients with unilateral lumbar disc herniation, changes in the multifidus muscle on the affected side are also commonly observed. 12 Some researchers have suggested that the multifidus muscle plays a key role in lumbar segmental stability, whereas the erector spinae primarily functions to maintain sagittal balance of the spine. 40 Higher levels of FI in the multifidus, longissimus, and psoas muscles are associated with poorer functional outcomes. 41 FI is also closely related to spinal surgery outcomes. Studies have shown that patients with lower multifidus FI achieve better recovery following artificial disc replacement surgery, 42 and the degree of paraspinal muscle fatty degeneration is also associated with postoperative outcomes following microdiscectomy. 43 Furthermore, studies have indicated that following posterior lumbar fusion, the multifidus muscle volume decreases significantly, and the erector spinae also shows a trend of volume reduction within the first postoperative year. 44 Paraspinal muscle atrophy is more pronounced following lumbar fusion, open posterior approaches, and non-minimally invasive fusion procedures. 45 Moreover, patients undergoing conventional open surgery experience greater postoperative FI and increases in FI compared with those receiving modified minimally invasive approaches. 17 In this study, the higher multifidus FI (OR = 1.116, P = 0.012) was identified as a risk factor for SEH. Increased FI of the multifidus reflects muscle degeneration and reduced functional capacity, which weakens its protective role during surgery and may render intramuscular microvasculature more vulnerable to intraoperative injury, thereby increasing bleeding risk. Additionally, in this study, the psoas muscle CSA and rCSA differed significantly between the two groups. Previous studies have shown that the psoas muscle is closely related to spinal physiological function, and the psoas muscle index can predict perioperative outcomes in elderly patients undergoing spinal surgery. 46 A lower standardized total psoas muscle area at L3–L4 has been associated with a higher incidence of perioperative adverse events in adult patients undergoing scoliosis surgery. 47 Therefore, although psoas major parameters were not included in the multivariable logistic regression model, preoperative assessment of the psoas major remains clinically significant. Furthermore, although the FCSA of the multifidus and erector spinae was smaller in the SEH group than in the normal group, their rFCSA was actually larger in the SEH group. This discrepancy may be attributed to the higher proportion of female patients in the SEH group, as females generally possess a smaller vertebral cross-sectional area compared with males.
To our knowledge, this is one of the first studies to investigate the association between paraspinal muscle characteristics and SEH following lumbar spine surgery. However, this study also has several limitations. First, as a single-center retrospective study with a relatively small sample size, the variables included were limited, only patients undergoing TLIF were enrolled, and the follow-up period was relatively short. Second, due to the limited number of positive events, there is a risk of overfitting, which may lead to unstable model estimates. Furthermore, due to the limited availability of comprehensive clinical data, several key variables were not fully considered. These include antiplatelet therapy, the timing of anticoagulant resumption, the use of NSAIDs and tranexamic acid, intraoperative hemostatic agents, drain output and duration, as well as postoperative blood pressure spikes. Third, potential measurement errors may exist, as muscle CSA and FI measurements were obtained using software-based image analysis. Therefore, further large-scale, multicenter, prospective studies incorporating multiple surgical approaches are warranted.
5. Conclusion
This study demonstrates that prolonged TT and increased multifidus FI are independent risk factors for SEH following TLIF, whereas higher BMD serves as a significant protective factor. These findings underscore the importance of comprehensive preoperative assessment. Clinicians should pay particular attention to patients’ coagulation status, bone quality, and the degree of paraspinal muscle degeneration. Precise preoperative evaluation of muscle quality via MRI can help identify high-risk patients and guide preventive strategies, thereby reducing the risk of postoperative SEH and improving outcomes after lumbar spine surgery.
Footnotes
Ethical Considerations
This study was approved by the Ethics Committee [Approval No. (2025) Lunshen 53-KY], and written informed consent was obtained from all participants.
Author Contributions
Luming Kong: Conceptualization, Methodology, Software, Writing-Original draft preparation; Songlin Liang, Renchang Chen, Xintian Qu, Moji Wangchen, Zelin Yue: Data curation, Investigation; Huapeng Guan, Nianhu Li: Writing- Reviewing and Editing. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Administration of Traditional Chinese Medicine, Science and Technology Department Co-constructed Project (GZY-KJS-SD-2023-042), the Natural Science Foundation of Shandong Province (ZR2023MH063), and the Natural Science Foundation of Shandong Province (ZR2023LZY012).
Declaration of Conflicting Interests
The Authors declares that there is no conflict of interest.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.