
Abstract
Background
Leg length discrepancy (LLD) remains a significant complication of total hip arthroplasty (THA), affecting patient's satisfaction and functional outcomes.
Methods
We have performed a prospective randomized control study to evaluate the efficacy of intraoperative technique with Steinmann pin as fixed supra-acetabular point to measure the leg length compared with preoperative planning with OrthoView digital software alone.
Results
Results showing that group A (Steinmann pin group) has a significantly lower postoperative LLD (p < 0.05) compared to group B (preoperative planning alone). There were no significant differences in operative time or blood loss between both groups.
Conclusion
The combination of preoperative digital imaging templating and intraoperative measurement using Steinmann pin as a fixed supra-acetabular marker for reference in THA can optimize leg length control on a posterolateral approach. The use of intraoperative measurement using Steinmann pin does not statistically increase the blood loss or operation time.
Keywords
Introduction
Leg length discrepancy (LLD) is considered to be one of the major problems after total hip arthroplasty (THA) and can adversely affect an otherwise excellent outcome. The amount of LLD after primary THA has been reported to range from 1% to 27%.1,2 LLD was reported to vary from 0 to 17 mm. 1 LLD is associated with lower back pain, limping, knees pain, instability symptoms, and loosening and nerve lesions. 3 These unfavorable outcomes often result in patient's dissatisfaction and is also the leading litigation after joint replacement in the United States. 4 Surgeons often put the stability of prosthetic hip joint as the top priority as THA dislocation could be disastrous. Therefore, correcting limb length inequality without compromising hip stability is definitely challenging. 5
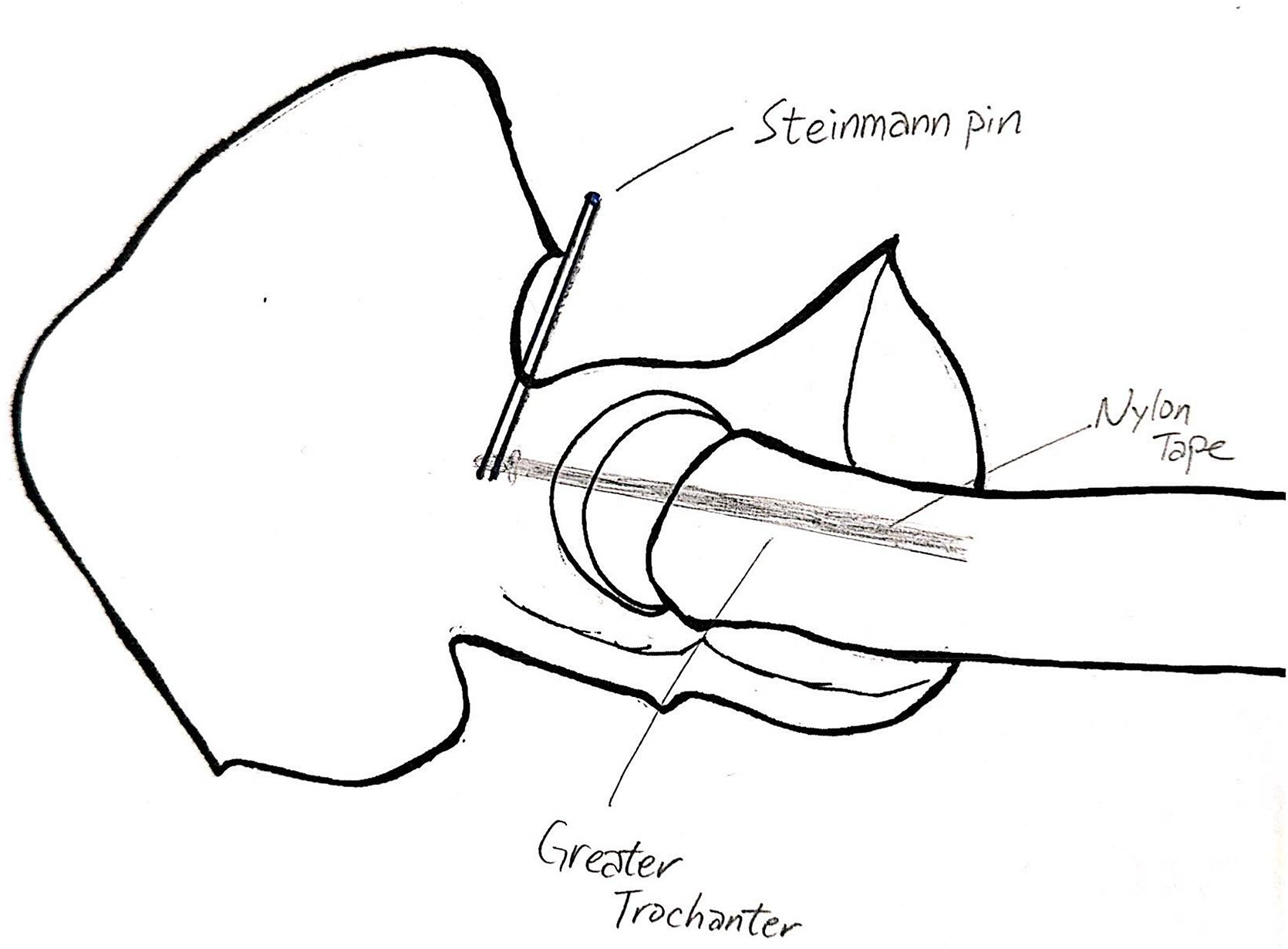
A schematic diagram showing the position of the Steinmann pin and nylon tape.
A piece of sterile nylon tape was tied to the Steinmann pin and the knot of nylon tape is pulled down along Steinmann pin at the level of greater trochanter (GT) surface. The first reference point at 5 cm was marked.
A permanent mark was made over greater trochanter (GT) with diathermy 5 cm below the Steinmann pin.
Methods and techniques to overcome LLD include preoperative and intraoperative measures. 2 The literature is replete with different techniques to overcome LLD during THA.2,6,7 However, some methods and devices manufactured are either too complicated or too expensive to be practical for routine use. 2
The use of intraoperative method of measurement using Steinmann pin as a fixed supra-acetabular marker for reference to measure leg length is first described in 2010. 8 However, there is lack of prospective study to review the effectiveness of this method in reducing LLD in THA.
Therefore, this prospective randomized study aims to evaluate effectiveness of this intraoperative method in reducing LLD in THA compared with only preoperative templating.
The hypothesis of our study is preoperative digital imaging templating and intraoperative Steinmann pin as a fixed supra-acetabular marker for reference in THA can reduce LLD during THA with a posterolateral approach.
Materials and methods
Study design
The study protocol was approved by our institution's research ethics committee (reference number: KCC/KEC-2019-0088). A prospective randomized control study was carried out in our institution from January 2020 until December 2022.
Inclusion and exclusion criteria
Twenty patients with THA in our institution, a district general hospital, were recruited.
The inclusion criteria including patients aged more than 40 years suffering from hip osteoarthritis, avascular necrosis, or hip dysplasia. Patients with severe spinopelvic deformity, contralateral hip arthritis which warrants future hip arthroplasty or contralateral hip being replaced, are all excluded from this study. Moreover, patient with the need of acetabular augmentation is also excluded.
Calculation of sample size
The calculation of sample size is based on a literature which had the very similar target groups and outcome measures. 9 Shiramizu's study in 2004 has the sample size of around 30 patients in each group with result showing the postoperative limb length inequality was reduced significantly in one group (p < 0.0001).
Based on the results of the literature, we used G Power software to calculate our sample size. The power was set at 0.8, alpha error 0.05. The effect size calculated was 2.11. It shows that sample size in each group is 5.
Although we anticipated that the drop-out rate was very minimal, we would like to ensure enough power for this study. Therefore, we decided the sample size of our study to about 20 patients (10 patients in each group).
Procedures
A pamphlet including the study information was given to all patients recruited. They will be asked to provide a written consent if they agreed to proceed with the study after reading the pamphlet. We will arrange radiograph of the pelvis with radiographic scaling marker for all patients and perform preoperative planning and templating. Their digitalized radiographs were processed using the OrthoView Orthopaedic Digital Imaging software (Version: REF 7.3.1) to approximate the size of modular femoral and acetabular components so as to restore normal geometry, including hip center of rotation, offset, and leg length. The digital planning was performed on a 17-inche LCD screen with a resolution of at least 1024 × 768 pixels. The patients were then randomized into 2 groups in a 1:1 ratio by drawing sequentially numbered sealed envelope. For group A, in addition to preoperative planning and templating, intraoperative method of measurement using Steinmann pin as fixed supra-acetabular marker are used to minimize LLD. For group B, only preoperative planning and templating will be performed as described.
Baseline evaluation
All patient's demographic data, blood loss, operation time, pre- and postoperative range of motion, pre- and postoperative radiologic LLD will be recorded.
Surgical technique
All total hip replacement surgeries are operated using the standard posterolateral approach. Patient is put in lateral decubitus position. A 10 cm curved incision is made posterior to greater trochanter (GT). Fascia lata is incised and gluteus maximus fibers are separated in usual manner to uncover vastus lateralis distally. The hip is then internally rotated to place short external rotators on stretch. Piriformis tendon and other short external rotators are cut close to femoral insertion.
For patients in group A:
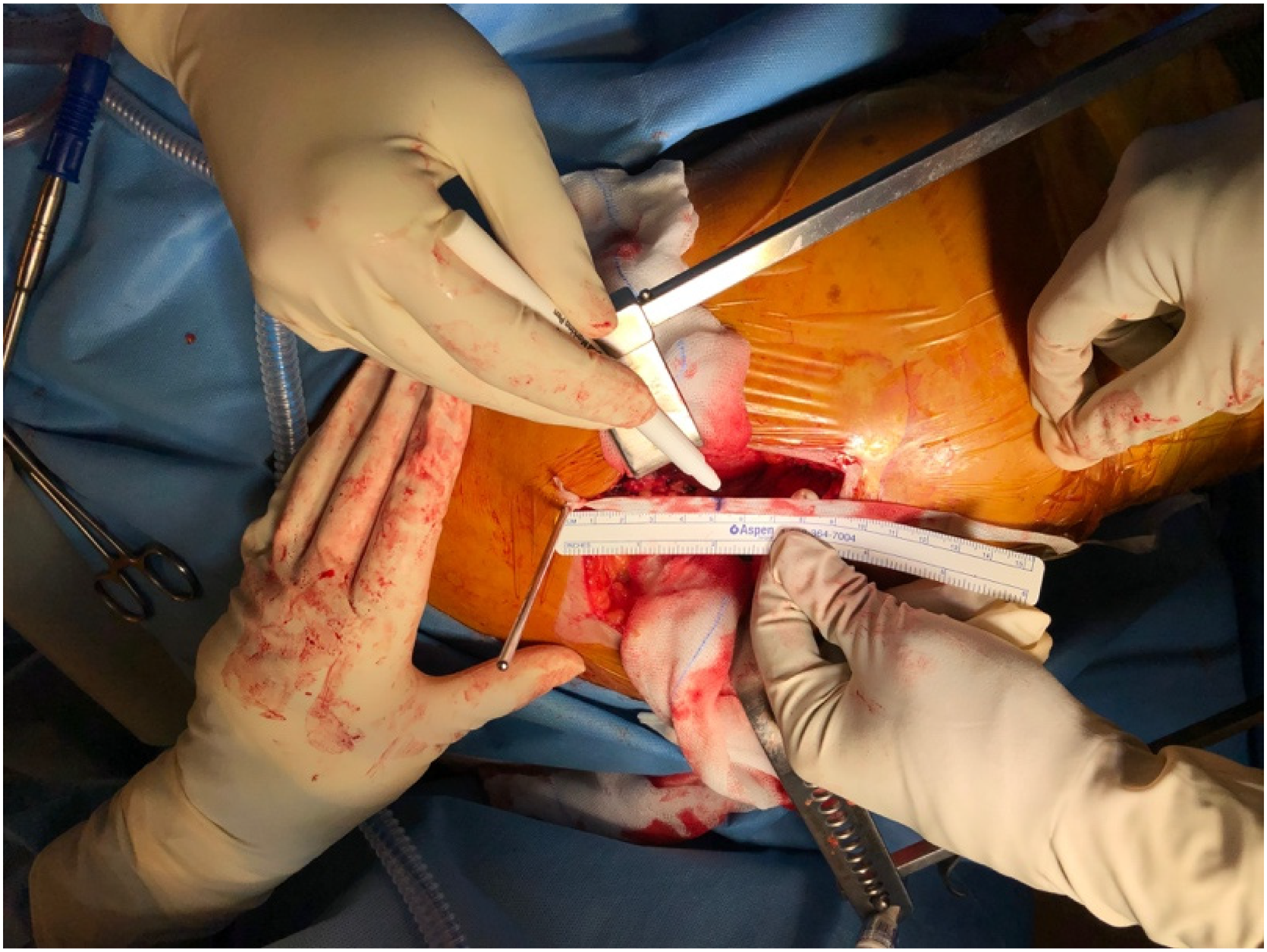
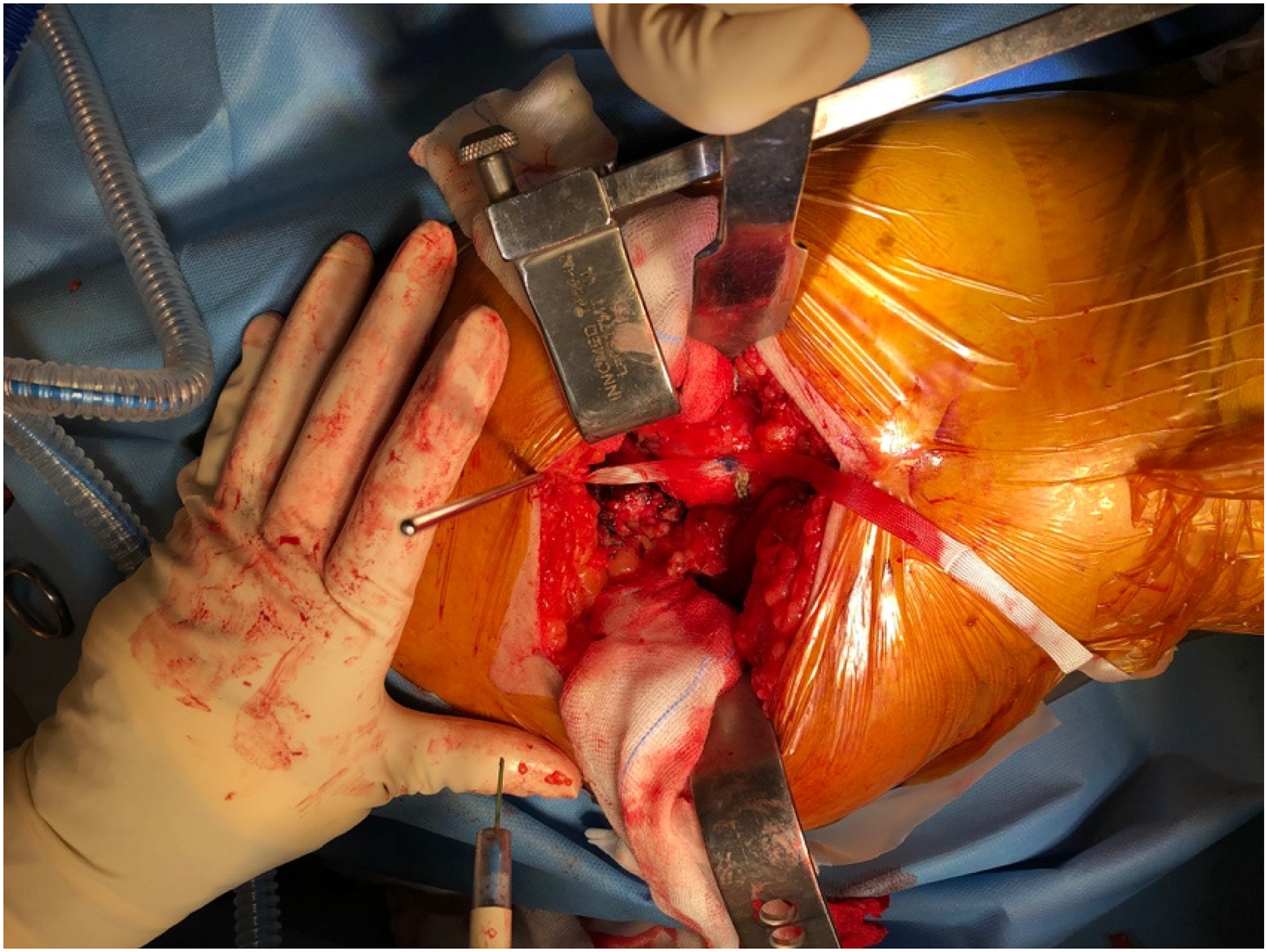
A 2.8 mm Steinmann pin was inserted into the supra-acetabular region of ilium 1 to 2 cm superior to the acetabulum dome level midway between anterior and posterior column after gluteus medialis is retracted anteriorly from the operative site and gluteus minimus muscle is released from supra-acetabular region if it is bulky to give better exposure. About 15 mm length Steinmann pin was inserted into the ilium to achieve stable anchor. A fixed stable pelvic reference point using Steinmann pin was formed (Figure 1). A piece of sterile nylon tape was tied to the Steinmann pin and the knot of nylon tape is pulled down along Steinmann pin at the level of GT surface then three reference points were marked on the nylon tape with sterile marker pen and ruler at 5, 6, and 7 cm distal to Steinmann pin to facilitate subsequent intraoperative judgment of leg length change (Figure 2). Before hip capsulotomy and dislocation, hip was positioned in full extension along the axis of the body and operated limb was parallel to the ground. If there was any hip flexion or adducted or abducted contracture of the hip, the contracted hip joint should be positioned as neutral as possible and the lower limb posture must be recorded and reproduced the same during each measurement of leg length. Next the marked tied nylon tape was pulled down and placed along the proximal femur. Then a permanent mark was made over GT with diathermy 5 cm below the Steinmann pin. The interval between the Steinmann pin and cauterized mark on GT is validated with ruler so that the cauterized mark over GT must correspond to the 5 cm mark on the nylon tape as well. The cauterized mark on GT will be highlighted with marker pen for easier identification (Figure 3). For every measurement, the same limb posture is reproduced first. The line between Steinmann pin and GT is usually parallel to the limb lengthening axis in ideal posture. The length of the tape between the Steinmann pin and the cauterized mark on GT is measured with ruler which is calibrated in millimeters. The measurements are recorded before hip dislocation and after trial implantation and final implantation. This is the intraoperative leg length, which can be used as reference intraoperatively to guide the surgeon to either lengthen, shorten or maintain the same length based on preoperative LLD measurement. Then femoral head component of different length options can be decided to match the target of leg length equality. After trial prosthesis and implantation of real prosthesis, the level of the cauterized mark on the GT distal or proximal to the 5 cm mark on the nylon tape will give an indication of lengthening or shortening. We have to pay attention that the lower limb is positioned in the same manner. After the implantation of THA prosthesis, the length between the Steinmann pin and the cauterized mark on GT is measured again and recorded. The perioperative target is to reproduce the leg length equality. The aim of intraoperative measurement allow surgeon to address the discrepancy by using appropriate modular implant to restore the leg length equality or minimize the LLD.
For patient in group B:
THA will be performed as usual manner based on the preoperative templating and planning. Intraoperatively, LLD will be minimized by judging the level of tibial tubercles of both legs with heels paired up at the same level after trial implantation and final implantation of prosthesis. Appropriate modular component will be chosen based on the judgment of LLD with this technique.
Outcome assessment
Radiologic assessment
All patients recruited into this study will have a standard digitalized anteroposterior (AP) radiograph of the pelvis with hip in neutral position preoperatively and 4 weeks after THA in our radiology department. Pre- and postoperative radiographs were evaluated on the Hospital Authority Clinical Management System via Hospital Authority image viewer.
All radiographs will be read by two members of the research team. These results will be reviewed if there are more than 1 mm discrepancies between the 2 results. They were both blinded from the patients’ grouping allocations.
For all the radiographs, LLD was assessed by the method described by Woolson. 10 Horizontal lines through the inferior aspect of the teardrop were drawn. The vertical distance between the most prominent point of the lesser trochanter and the trans-tear drop line is measured based on radiographic magnification by 10%.
Data collection
In group A, the perioperative measurement of the difference in length (mm) between the initial leg length and the final leg length after implantation of real prosthesis was recorded.
In both groups, the pre- and postoperative LLD, difference between intraoperative LLD and postoperative LLD, and the proportion of patients with less than 5 mm LLD were recorded.
Statistics
Demographic data were compared between two groups by nonparametric Mann–Whitney U test.
Dependent variables (change in length, LLD) were expressed as means and ranges, and analyzed on Fisher exact tests for inter-group comparison. The significance threshold was set at p≤ 0.05.
These results were analyzed using the student's t-test using online calculator. 11
Results
One of the patients from group A passed away due to medical illness unrelated to the surgery and therefore there were only nine valid samples in group A.
For the background demographics of both the groups, the mean age and standard deviation were 61.11 +/− 19.15 and 61.60 +/− 10.64, respectively. The mean and standard deviation of body mass index of group A and B were 23.13 +/− 4.88 and 24.50 +/− 4.59, respectively. Mann–Whitney U test for age and body mass index (BMI) both showing statistically insignificant between the groups with a p-value <0.05.
The mean operation time between the groups were 130 min in group A and 122 min in group B (p=0.24), which is statistically insignificant.
The mean blood loss for group A was 500 mL and group B 523 mL (p-value 0.44), which is also statistically insignificant.
The postoperative LLD is significantly reduced in group A, with mean 1.72 mm (range 0–4.5 mm), in contrast to group B, with mean 4.7 mm (range 0–11 mm) (p-value 0.026). The percentage of patients with postoperative LLD less than 5 mm was 100% (9/9) in group A and only 50% (5/10) in group B. Fisher's exact test on the postoperative LLD within 5 mm was statistically significant between the two groups with a p-value of 0.0325.
In group A, the difference between intraoperative LLD from target versus postoperative radiological LLD was only 1.39 mm (range 0–3 mm).
The use of OrthoView Orthopedic Digital Imaging software for preoperative planning also showed high accuracy in terms of the final size of the implant. 79% and 68% of our patients used the exact same size of final acetabular and femoral implants respectively as the preoperative plan.
Discussion
Previous studies had developed different methods to minimize LLD between preoperative planning and postoperative results, however most of the methods are quite complex and not user-friendly. 2
There are basically five categories of methods for this purpose. These include preoperative templating, intraoperative clinical test, intraoperative fluoroscopy imaging, computer-navigated robotic system, and intraoperative measurement of the distance between two fixed anatomical points.
The use of digital templating (i.e. Orthoview) is an essential part of preoperative planning in THA, however there are many factors affecting the accuracy of preoperative templating including patient's BMI, external rotation of the hip, and surgeon's experience. 12 Therefore, intraoperative measures are of utmost importance for a perfect THA.
The use of Steinmann pin as an intraoperative guide is a simple, safe, and reliable technique for posterolateral approach of total hip replacement in this study. It does not require any additional equipment, incision and preoperative radiographs when compared to standard total hip replacement technique. Our study had shown that the use of this method does not lengthen the operation time nor increase the blood loss when compared to the traditional THA.
Direct anterior approach (DAA) of THA is an approach that can use intraoperative X-ray to assess component position and leg length. Studies has shown that intraoperative imaging reduces the incidence of postoperative LLD >5 mm and improve the accuracy of cup positioning.13,14 However, DAA THA will increase radiation exposure to the patient as well as the surgical team. Other drawbacks for this approach are the false reassurance from single view imaging as pelvic tilt and limb positioning during imaging can lead to misinterpretation of the true leg length. 15
Our study results confirmed the usage of Steinmann pin intraoperatively together with preoperative OrthoView Orthopedic Digital Imaging planning significantly reduce the postoperative LLD when compared to preoperative planning alone. This technique is rather simple without the need of another wound over iliac crest compared with other intraoperative devices which have been used to assess intraoperative correction of LLD like “U-shaped bent guide wire, adjustable caliper, dual pin retractor, and compass device.16–19 The pelvic fixed point for our technique is at the supra-acetabular region, which is much closer to the center of hip rotation. It improves the accuracy of the leg length measurement. However, the accuracy of using intraoperative device to assess LLD is highly dependent on the reproducibility of femur position during each measurement in the lateral decubitus position. 20 This is a potential limitation of this technique to generate consistent result.
In the era of robotic surgery, robot-assisted THA is gaining more popularity over the past decade. Multiple researchers have found that the LLD is significantly smaller postoperatively with robotic THA than conventional THA. 21 No patients in the robotic group have LLD more than 10 mm comparing with 6% in the conventional group. 22 The patient reported that the outcomes were also superior in robotic THA. 23 There is no significant difference in revision rates comparing both groups. 21 The drawbacks of robot-assisted THA include high cost, preoperative computed tomography, and steep learning curve as well as limited long-term data.
For intraoperative clinical test, for example, Shuck test, which tests the soft tissue tension and length, is also a common practice to judge the leg length balance. However, it is not validated scientifically. It can be affected by many factors such as the amount of soft tissue release, the surgeons’ experience, force applied to distract the joint, muscle relaxation status as well as the type of anesthesia. 24
The intraoperative method we used to minimize LLD in group B is by judging the level of tibial tubercles of both legs with heels paired up at the same level. Although this method is relatively common in everyday practice, the authors acknowledged that this method may not be objective which may lead to false positive results.
In fact, LLD after THA is a significant cause of patient dissatisfaction and functional impairment.25–27 LLD alters the pelvic tilt, spinal alignment, and gait mechanics thus increasing the energy expenditure during walking. 25 A > 10 mm LLD leads to compensatory mechanism that may accelerate contralateral hip or knee arthritis causing patient's dissatisfaction. 17 Low back pain and sciatica are major complaints from patient with postoperative LLD as LLD >5 mm correlates with lumbar scoliosis and facet joint overload. Patients with post-THA LLD report 2.5 times higher odds of persistent back pain. 26 Knee pain is also another cause of patient's dissatisfaction after THA with excessive femoral lengthening as it increases patellofemoral joint reaction forces, leading the anterior knee pain. Jennings et al. 13 also suggests that patient with an LLD >5 mm is associated with lower Harris Hip Scores and Oxford Hip Scores. Moreover, LLD represents a significant medicolegal risk in THA, ranking as the second most common reason for litigation after nerve injury. 28 Linsen et al. analyzed 65 THA malpractice claims and revealed LLD accounted for 26% of cases. However, absolute equalization of leg length is difficult to be achieved after THA despite various methods available in the market.
In conclusion, LLD after THA remains a complex clinical problem. Treatment and revision surgery present with unique challenges. Despite advances in surgical techniques and technologies, achieving optimal limb length equality is often difficult due to anatomical constraints, such as soft tissue contractures 29 and pelvic obliquity. Scar tissue and altered anatomy will further add difficulty to the revision surgery. Removal of primary implants will cause bone loss which may require complex reconstructive techniques. 30 Even after revision surgery, some patients retain compensatory mechanism which leads to persistent gait abnormalities 17 and up to 40% patients will remain dissatisfied. 29 Higher re-revision rates due to instability or component loosening are also observed compared to primary THA. 29 On the other hand, nonsurgical treatments for LLD like shoe raise often causes gait asymmetry and patient dissatisfaction. 27 All in all, prevention is always better than remedial action when it happens. Once occurs, detailed discussion on the management of LLD after THA and pros and cons of revision surgeries with patient is imperative for patient's best interests.
Our study demonstrated that the surgical technique of using Steinmann pin as fixed supra-acetabular marker can definitely mitigate LLD in THA without additional risks.
Due to manpower arrangements in our district hospital, THA included in this study is not done by a single surgeon; however, each surgery will have at least one senior specialist participating. Although the same approach was used among all THA, minute difference in surgical skills may in turn affect the results.
Although every effort had taken place to ensure that the patient is positioned in a reproduced position (i.e. parallel to ground and hip in extension), there is still a minimal difference in position between pre- and postimplantation and between different patients due to human error.
One of the patients from group A passed away due to medical illness unrelated to the surgery and therefore there are only nine valid samples in group A. The author acknowledges the reduction in power due to this drop-out.
Due to the COVID pandemic, elective surgeries including total hip replacement was largely affected. The number of THA during the study period is greatly reduced. As the COVID restrictions are gradually lifted, the number of elective surgeries is resuming to normal capacity. The power of this study could be further improved by a larger sample size in the future. Moreover, we could cooperate this study with allied health professionals so as to explore whether the use of Steinmann pin could improve the Harris hip score and patient's satisfaction after THA.
Conclusion
The combination of preoperative digital imaging templating and intraoperative measurement using Steinmann pin as a fixed supra-acetabular marker for reference in THA can optimize leg length control on a posterolateral approach.
The use of intraoperative measurement using Steinmann pin does not statistically increase the blood loss or operation time.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tung Wah Group of Hospitals research fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.