
Abstract
Introduction
This study aimed to evaluate the reliability of online assessment tools for elbow and wrist function in civilian and military patients. In addition, functional outcomes were compared between cohorts to identify potential differences related to injury context and patient characteristics.
Methods
Two distinct cohorts participated: (1) military patients (MP), including 25 males from Ukraine (mean age 37.83 ± 6.97 years) with combat-related upper limb injuries, and (2) civilian patients (CP), comprising 28 males from Lithuania (mean age 39.33 ± 8.85 years) with noncombatant injuries. Four experienced physiotherapists (two per country), each with over 10 years of experience in musculoskeletal assessment, conducted evaluations using the Modified Mayo Wrist Score (MMWS) and the Mayo Elbow Performance Score (MEPS) both on-site and online.
Results
The intraclass correlation coefficients (ICCs) and kappa values exceeded 0.90 across both groups, indicating excellent reliability of online functional assessment. Significant differences were observed between the CP and MP groups in MEPS pain domain scores (P = 0.020) and MMWS domains of range of motion and grip strength (P < 0.001). A strong, statistically significant correlation was found between elbow and wrist function in the MP group (on-site rs = 0.848; online rs = 0.880; P < 0.001), whereas no significant correlation was observed in the CP group.
Discussion
The high inter-rater reliability supports the clinical use of MEPS and MMWS in online formats. Functional differences between cohorts highlight the impact of injury mechanism and rehabilitation context, emphasizing the importance of tailored assessment and intervention strategies in telerehabilitation.
Introduction
About 50% of fractures in combat trauma are upper extremities, while about 45% of upper-extremity injuries occur at home (wrist about 38%, elbow about 42%). 1 Although obvious differences exist, particularly regarding the mechanisms of injury, both civilian and military trauma can result in life-changing consequences. Although the literature highlights notable similarities in acute surgical management and early rehabilitation strategies in both types of injury, several context-specific differences have been described. For example, military casualties are typically younger, present a higher level of injury severity, and experience a greater incidence of amputations compared to civilian patients (CP). Despite the prevalence of more severe injury profiles, military patients (MP) consistently achieve superior mobility outcomes following rehabilitation. 2
In the countries involved in the ongoing war, such as Ukraine, has led to a significant rise in combat-related polytrauma injuries, including high-level multiple amputations, delayed evacuations, infectious complications, and limited access to rehabilitation services. 3 Frequently, it is a clinical challenge to provide long-term treatment for patients with combat-related injuries due to the logistics of health care services and high risk of complications. 4 Such complications are often associated with prolonged hospital stays and suboptimal anatomical and functional outcomes, primarily due to limited access to rehabilitation services and restricted healthcare human resources. Rehabilitation requires an interdisciplinary, multifaceted process that involves the coordinated integration of clinical decision-making, logistical infrastructure, and social support systems.
Clinical scoring systems, including patient-reported outcome (PRO) measures, have become increasingly utilized in evaluating the effectiveness of treatment interventions for wrist and elbow injuries. PRO measures offer valuable insights into how patients perceive the impact of their condition and treatment on their health status and quality of life, thereby complementing clinician-based assessments with patient-centered perspectives. For example, the Mayo Elbow Performance Score (MEPS) and Modified Mayo Wrist Score (MMWS) were designed to measure pain, range of motion (ROM), and the patient's ability to accomplish functional tasks.5,6 Both scales range from 0 to 100 points, with a higher score indicating a better outcome.7,8 While the two instruments have been used across different patient groups, there is no study describing the reliability of the MEPS and MMWS with MP.
MP typically undergo rehabilitation through structured cycles of intensive inpatient care, lasting several weeks, combined with periods of rehabilitation at home. This cyclical process continues until the patient achieves a high degree of functional independence and is either reintegrated into active military duty or formally discharged from service. 9 During the temporary rehabilitation periods at home, ongoing supervision and monitoring of the rehabilitation process remain essential to prevent complications such as joint contractures, muscle weakness, and functional regression. To support continuity of care, military rehabilitation frameworks increasingly emphasize the use of standardized assessment protocols, systematic follow-up procedures, and adaptable, supervised delivery formats applied on-site or via online platforms. However, it remains unclear whether the use of PRO instruments such as the MEPS and the MMWS, when administered remotely, can provide reliable assessments in military populations. Further investigation is needed to determine their applicability and psychometric robustness in online or telehealth contexts.
This study aimed to evaluate the reliability of the online assessment of elbow and wrist function in civilian and MP. In addition, comparison of functional assessment outcomes between the two cohorts was performed to identify potential differences related to injury context and patient characteristics.
Methods
The study protocol involved a comparative cross-sectional measurement design, and the Institutional Review Board at Lithuanian Sport University approved this protocol (Nr. 2024 05 08 BNL-FAV (B) – 2023-692).
Sample
The two distinct cohorts were involved in this study: (1) MP, including 25 males from Ukraine (mean age 37.83 years, SD = 6.97) with combat-related upper limb injuries undergoing rehabilitation in Ukraine (UA), and (2) CP of 28 males (mean age 39.33 years SD = 8.85) with noncombatant injuries receiving rehabilitation in Lithuania (LT).
Sample size calculations were done according to the previous studies revealing that the examination of test-retest (on-site vs online) reliability of the instruments required at least 41 patients (two observations, power 80%, α = 0.05, expected ICC 0.5) (Bujang et al., 2017). 8 All participants were 18 years or older and provided signed consent priori to their involvement in the study. Table 1 presents characteristics of participants. Inclusion criteria were history of traumatic injuries requiring physiotherapy assessment and treatment. Exclusion criteria were an immediate surgical indication, significant cardiac or neurological disease, limited legal capacity, psychiatric disorders, dementia, or other cognitive impairments.
Characteristics of the study participants.
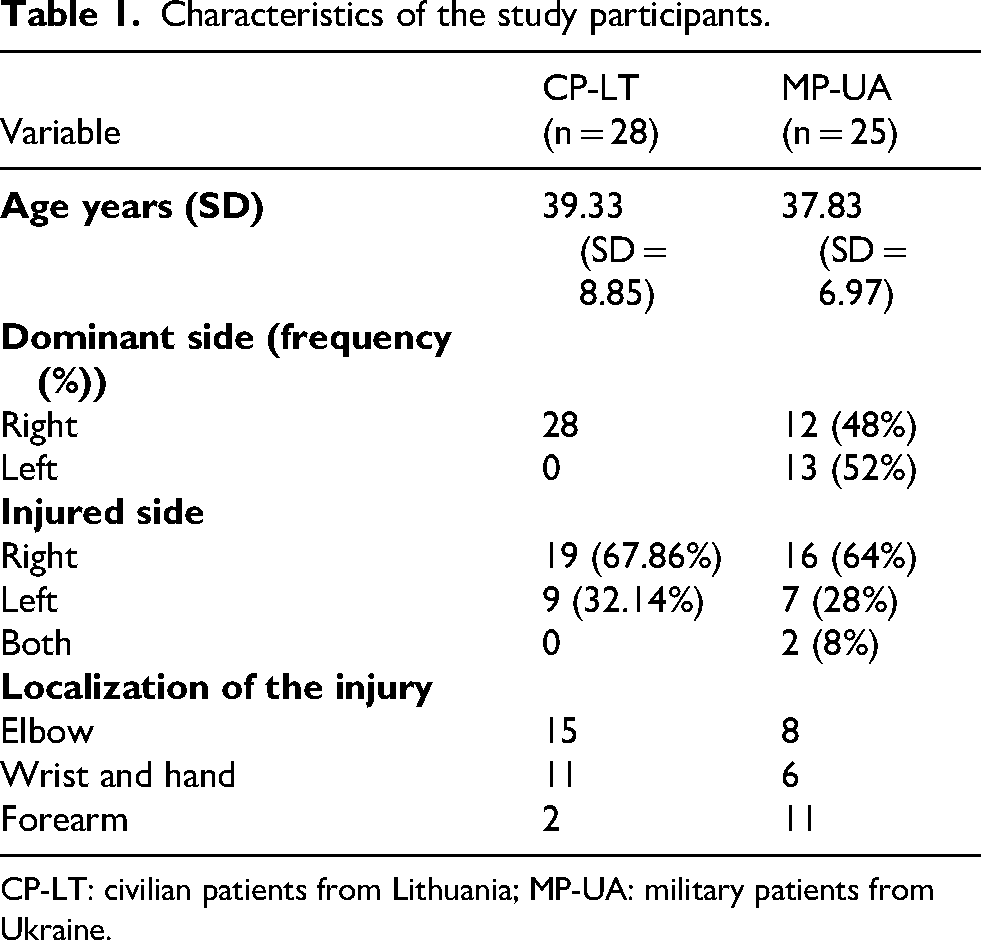
CP-LT: civilian patients from Lithuania; MP-UA: military patients from Ukraine.
Four qualified physiotherapists (two in Lithuania and two in Ukraine) with more than 10 years of working experience in traumatology and musculoskeletal physiotherapy assessment were trained and performed the MMWS and MEPS.
Instruments
The MEPS is a composite rating scale used to assess elbow function across four domains: (1) pain (45 points), (2) stability (10 points), (3) ROM (20 points), and (4) performance of daily functional tasks (25 points). The total score ranges from 0 (indicating worst function) to 100 (indicating normal elbow function). 10 The original version has been found to have good test-retest reliability (r = 0.82) and validity (r = 0.83). 8 Pain, stability, and ROM are each evaluated using a separate ordinal scale. The functional tasks domain is assessed based on the number of predefined activities the participant can perform.
The MMWS is a combined measure with a total score of 100 points, distributed across four domains: (1) pain (25 points), (2) active flexion/extension arc as a percentage of the contralateral side (25 points), (3) grip strength as a percentage of the contralateral side (25 points), and (4) the ability to return to regular employment or daily activities (25 points). Pain is rated by the evaluator based on the patient's subjective report as none (25 points), mild (20 points), moderate (10 points), or severe (0 points). The total MMWS ranges from 0 to 100, with higher scores reflecting better functional outcomes. A score of 90–100 is considered excellent, 80–89 good, 65–79 fair, and less than 65 poor (Green and Brien, 1978).
Testing procedure
Participants who met the eligibility criteria and agreed to participate in the study underwent two consecutive assessments (on-site and online) within a single clinic session with about 15 min rest between the two sessions. The sessions were conducted in the health care setting where the patients were treated. The EZ Read Jamar Goniometer, Patterson Medical, was used to measure the ROM at both locations. For the on-site session, the traditional physiotherapy room was used. The online physical assessments were conducted in the two separate rooms with the chair, desk, and computer using the ZOOM video-conferencing system. In preparation for conducting the online assessments, a pilot test was conducted in both research sites. This allowed physiotherapists from both countries to agree on the position of the videoconferencing platform and the assessment protocol alterations required to perform a physical examination via the Zoom platform. The MMWS and MEPS protocols were completed by physiotherapists on paper. The order of the assessments (on-site and online) was randomly assigned, and each examiner was blinded to the participants’ performance in the other assessment format and to the findings of other examiners. The researcher responsible for data entry was blinded to both the patients and the physiotherapists and entered the data into the designated data platform.
Data analyses
Data were analyzed using the SPSS software package, version 28 (IBM, Armonk, NY, USA).
The normality of the descriptive data, such as the participant demographics and the ROM values, was examined first using the Shapiro–Wilk test prior to conducting any other data analyses. 11 Paired t-tests were used to compare the ROM values assessed by each examiner in the online and on-site formats. A P-value of <0.05 was considered statistically significant. Intraclass correlation coefficients (ICCs) were calculated to test reliability with ICC values based on established criteria: moderate (0.50–0.75), good (>0.75), and excellent (>0.90). 12 Kappa statistics (κ) were used to assess the level of agreement between categorical ratings beyond chance. This statistic accounts for the proportion of agreement expected to occur randomly, providing a more accurate measure of inter-rater reliability. The strength of agreement, ranging from 0 to 1, is interpreted as follows: 0.00–0.20 = slight; 0.21–0.40 = fair; 0.41–0.60 = moderate; 0.61–0.80 = substantial; and 0.81–1.00 = almost perfect. 13 Values of k over 0.40 were considered to be clinically acceptable. The Spearman correlation coefficient between the total scores of MMWS and MEPS in online and on-site formats was used to analyze the association between the two contextual factors affecting joint recovery dynamics.
Results
Table 2 presents comparative analyses of on-site and online assessment outcomes between MP from Ukraine and CPs from Lithuania. In both assessment options, the MEPS scores demonstrated significant differences in the Pain intensity domain (P = 0.02) and MMWS scores in ROM and grip strength (P < 0.001).
Results for wrist and elbow functions measured on-site and online for UA and LT participants.
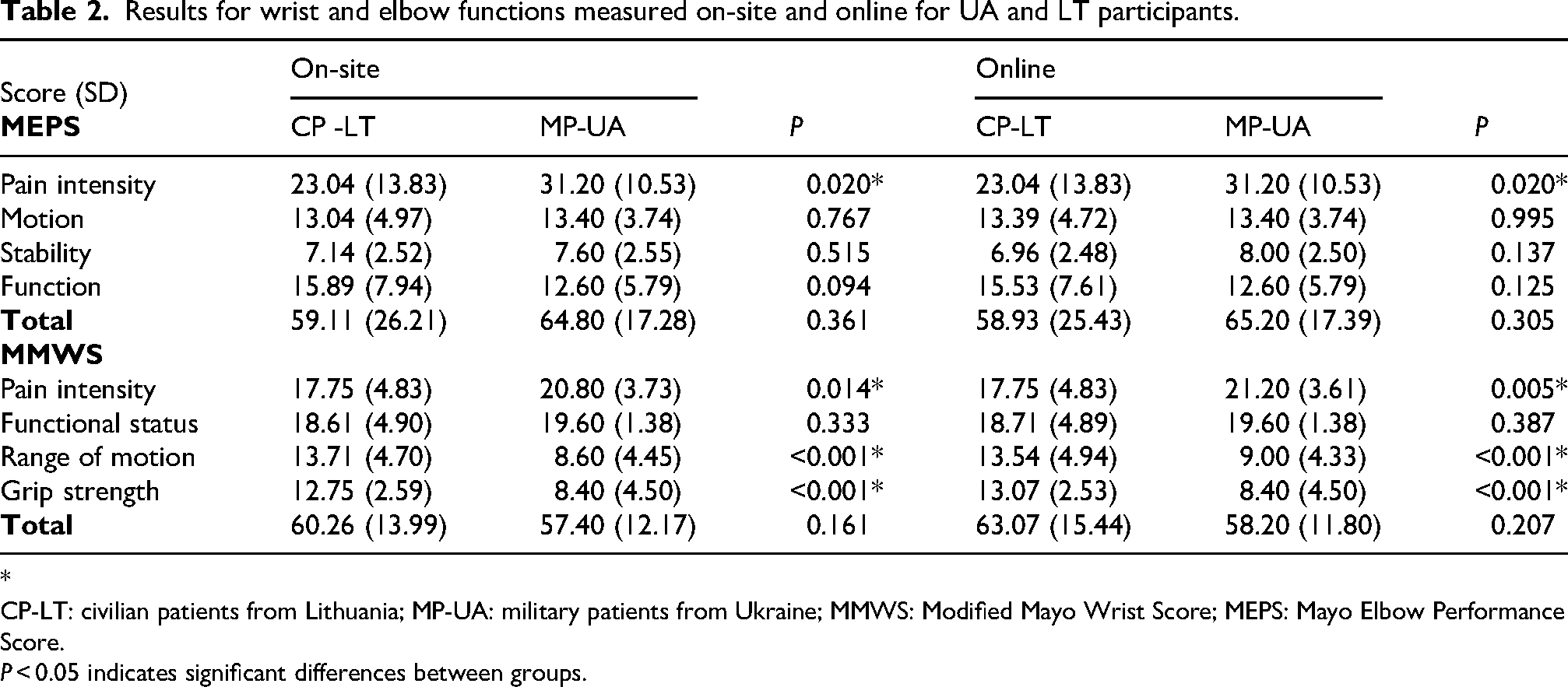
*
CP-LT: civilian patients from Lithuania; MP-UA: military patients from Ukraine; MMWS: Modified Mayo Wrist Score; MEPS: Mayo Elbow Performance Score.
P < 0.05 indicates significant differences between groups.
The results obtained by the two examiners from the two types of assessments did not present significant differences in any domains of both instruments. Table 3 shows the results of the interrater reliability between the two examiners of MEPS and MMWS total scores in online and on-site assessment. The ICC and kappa were high (above 0.09) for both samples, indicating excellent reproducibility in assessing elbow and wrist functions for CP and MP online.
Inter-rater reliability outcomes.
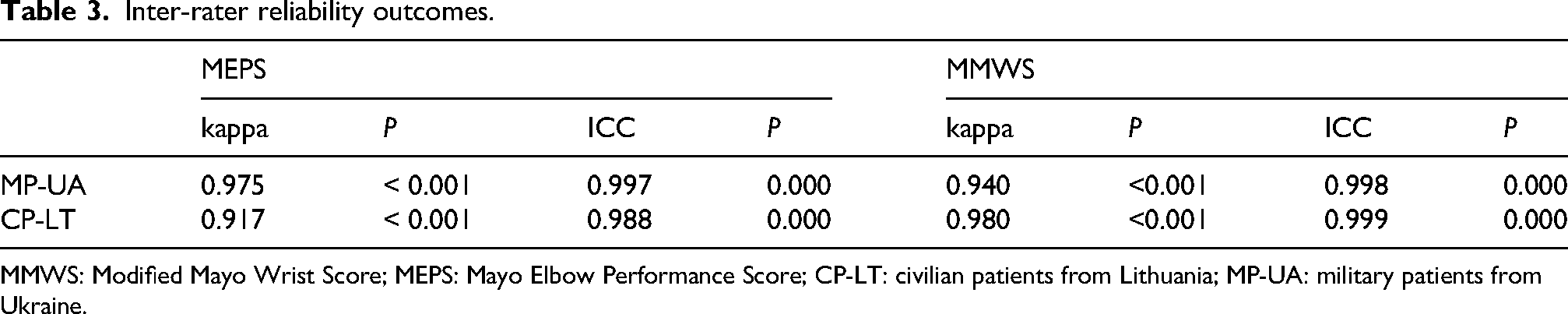
MMWS: Modified Mayo Wrist Score; MEPS: Mayo Elbow Performance Score; CP-LT: civilian patients from Lithuania; MP-UA: military patients from Ukraine.
The correlations between elbow and wrist function results presented high significant association in the UA group in both assessment sites (on-site rs = 0.848, online rs = 0.880, P < 0.001), while no significant association in LT group. The correlation results are presented in Table 4.
Correlation (rs) analyses of elbow and wrist total scores.
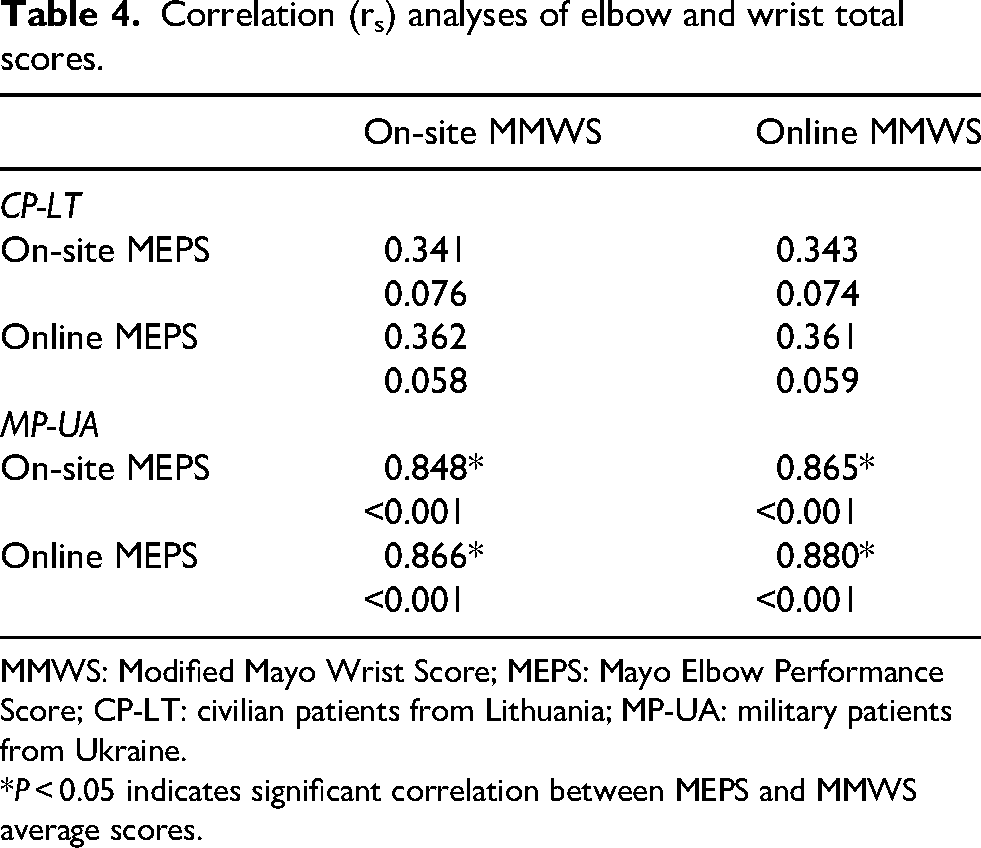
MMWS: Modified Mayo Wrist Score; MEPS: Mayo Elbow Performance Score; CP-LT: civilian patients from Lithuania; MP-UA: military patients from Ukraine.
*P < 0.05 indicates significant correlation between MEPS and MMWS average scores.
Discussion
The primary aim of this study was to assess whether the online application of the MEPS and MMWS is reliable in MP and CP. Scientific reports presenting the applicability of functional assessment instruments for upper extremity, particularly in combat patients, are very limited. Therefore, the current findings contribute to the existing literature with evidence by demonstrating the feasibility and reliability of online joint-specific functional assessment in military rehabilitation settings. In addition, since this study involved the two distinct cohorts, civilian from Lithuania and military from Ukraine, the comparative analyses of assessment outcomes provided further insight into inter-joint functional relationships. These findings will deepen knowledge on upper limb recovery patterns across different injury etiologies and rehabilitation contexts, and inform the development of more targeted, cohort-specific assessment and treatment strategies.
Reliability between the online and on-site assessment
The MEPS and MMWS have demonstrated acceptable inter and intra-rater reliability of on-site assessment in patients with impaired upper extremity joint functions.8,14,15 However, none of these studies used MEPS and MMWS in online mode. The recent review reported the validity and reliability of telerehabilitation assessment tools: out of 10 selected studies only one reported outcomes of real-time digital physiotherapy assessment of elbow function. 16 Researchers employed structured clinical diagnostic assessments (e.g. ROM, special orthopedic maneuvers) to compare examination findings obtained through face-to-face and remote tele-examination. The results indicated >68% agreement between on-site, remote, and repeated remote evaluations, suggesting that remote examination of the elbow is generally valid and reliable for clinical use. The present study demonstrated high inter-rater reliability between on-site and online assessment in both study groups (military and civilian) with ICC exceeding 0.90. These findings are consistent with prior research supporting the reliability of remote assessment in musculoskeletal conditions. For example, Palacin-Marin et al. 17 reported ICC scores above 0.80 between on-site and telerehabilitation evaluations for 7 of the 9 outcome measures in a small group of individuals with low back pain (n = 15, mean age 37 years). Similarly, Mani et al. 18 found excellent inter-rater reliability (ICC = 0.93–0.99) between face-to-face and tele-rehabilitation measures across the five assessment outcomes in patients with non-specific neck pain (n = 11, mean age 32.7 years). To our knowledge, the present study is the first to report the reliability of MEPS and MMWS in a synchronous online format for both civilian and military populations. These results support the feasibility and clinical utility of remote upper extremity assessment using standardized instruments and further justify their integration into telerehabilitation protocols for broader accessibility and continuity of care.
Comparative assessment of combat and civilian study groups
Previous studies describing combat and civilian injury treatment have reported significant differences, particularly related to the mechanism of injury (e.g. blasts or ballistic forces), whereas civilian injuries derive more commonly from low- to moderate-energy mechanisms. 2 Despite these differences, both cohorts experience a wide range of life-altering functional outcomes, and similar functional assessment instruments are frequently employed in their rehabilitation processes. In the present study, mean pain intensity outcomes were significantly lower in the military cohort from Ukraine, compared to the Lithuanian civilian cohort, indicating fewer pain complaints among combat-injured participants (P = 0.020 for MEPS, both online and on-site; P = 0.014 for MMWS on-site; P = 0.005 for MMWS online). In a recent observational study involving Ukrainian soldiers with extremity trauma, the average pain intensity on the Visual Analogue Scale was approximately 6/10, and neuropathic pain was reported in over half of the patients, indicating substantial symptom burden in this population. 19 No prior studies have directly compared pain intensity levels between combat and civilian upper-extremity injury patients. However, epidemiological evidence indicates that military veterans reported higher prevalence and severity of pain than civilians of comparable age and sex. For example, in U.S. veterans, the odds of suffering severe pain were approximately 40% higher. 20 Furthermore, experimental pain studies have demonstrated that combat veterans exhibited higher thermal pain thresholds and lower pain sensitivity compared to CPs, suggesting possible alterations in pain perception among military-experienced individuals. 21 Moreover, a significant between-groups difference (P < 0.001) was observed in ROM and grip strength with CPs (LT) consistently exhibiting higher functional scores than MP (UA) in both online and on-site assessments. This aligns with military evidence showing that combat injuries frequently result in more complex, multi-structure damage to the upper extremity, leading to more pronounced impairments in ROM and strength post-injury 22
Association between elbow and wrist function measures
The moderate and non-significant correlation observed in the LT study group between total MEPS and MMWS function scores demonstrated a relatively independent recovery course of these joints. This finding may be attributed to the heterogeneous nature of civilian injuries in this cohort, which likely included isolated or low-energy traumas (e.g. falls, workplace injuries, degenerative conditions), each requiring individualized treatment plans and rehabilitation protocols. Such injury-specific rehabilitation plans may result in variable recovery rates between the two joints, limiting functional interdependence. In contrast, the strong and statistically significant correlations between MEPS and MMWS scores in the Ukrainian cohort (rs = 0.84–0.88, P < 0.001) that included only combat patients indicated a more unified pattern of upper limb functional recovery. Combat injuries typically involve high-energy trauma, often affecting multiple anatomical regions of the limb simultaneously (e.g. blast or ballistic injuries), leading to complex soft tissue, neurovascular, and skeletal involvement of both the elbow and wrist.23,24 As a result, these patients may receive more intensive, multidisciplinary rehabilitation that targets the entire upper extremity, facilitating recovery of the elbow and wrist joint functions.
Furthermore, combat-injured patients may exhibit greater rehabilitation motivation and structured follow-up, often coordinated through military medical systems. 25 This function-oriented approach likely promotes coordinated improvements in wrist and elbow function, as reflected in the high inter-joint function correlation coefficients in the study outcomes.
Strengths
This was the first study involving both military and civilian cohorts from two different countries, which allowed for unique cross-population comparisons of upper extremity function. The use of standardized, validated instruments (MEPS and MMWS) in both on-site and online formats provided robust evidence of their reliability for implementing a telerehabilitation approach. Furthermore, the high inter-rater reliability and comprehensive assessment of pain, ROM, and grip strength strengthen the credibility of the findings and support the applicability of remote assessments across diverse rehabilitation contexts.
Limitations
This study has several limitations that should be considered when interpreting the findings. The sample size was relatively small and restricted to CPs from Lithuania and MP from Ukraine, which may limit the generalizability of the results. Moreover, although not intentional, the study included only male participants. The inclusion of female patients in future research may yield different outcomes in MEPS and MMWS domains, as sex-related differences in musculoskeletal function and pain perception could influence assessment results. Additionally, variability in healthcare systems, injury mechanisms, and rehabilitation protocols between the two countries might have influenced the functional outcomes in the upper extremity. Finally, the study design did not include long-term follow-up, limiting insights into the sustainability of remote assessment accuracy and recovery trajectories over time.
In addition, the study employed a non-randomized cross-sectional design, which may introduce selection bias. According to established evidence hierarchies, this design corresponds to Level III evidence. Furthermore, as the study was conducted across two countries with different native languages (Ukraine and Lithuania), potential language and cross-cultural differences may have influenced patient understanding of instructions and responses during both on-site and online assessments.
Conclusions
This study is the first to demonstrate that online application of the MEPS and MMWS is a valid and reliable method for assessing upper extremity function in both civilian and military populations. High inter-rater reliability across on-site and remote evaluations supports the integration of these tools into telerehabilitation programs. Comparative analysis between cohorts revealed meaningful differences in pain perception and functional outcomes, providing valuable insight into injury-specific recovery patterns. These findings contribute to the growing evidence base for digital rehabilitation and support the development of targeted, population-specific assessment strategies in diverse clinical settings.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to all the participants who contributed their time and effort to this study. The authors also acknowledge the support of the clinical and rehabilitation teams involved in the coordination and facilitation of the assessments in Lithuania and Ukraine.
Ethical approval and informed consent
The study protocol involved a comparative cross-sectional measurement design and the Institutional Review Board at Lithuanian Sport University approved this protocol (Nr. 2024 05 08 BNL-FAV (B) – 2023-692).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research study was conducted as a part of the project “Remote Functional Assessment: Innovative solution for rehabilitation of war victims in Ukraine” (nr. 2023-K-063) with the Central Project Management Agency of Lithuania.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.